-
7/22/2019 Magnesium for Depression
1/9
-
7/22/2019 Magnesium for Depression
2/9
population is affected by depression at any givenmoment. The
World Health Organization showedthat unipolar major depression was
the leadingcause of disability globally in 1990, and suggeststhat
depression and heart disease will be the mostcommon diseases on
Earth by 2020 [1], with both ofthese diseases having strong
magnesium deficiency
components.Contemporary approaches to treating unipolarmajor
depression and manic depression (bipolardisorder) utilize a wide
variety of drugs that in-clude monoamine oxidase (MAO) inhibitors,
tricy-clic compounds, selective serotonin reuptakeinhibitors
(SSRIs), and lithium (for bipolar disor-der). These drugs need
several weeks to becomefully functional.
Varley [2] and many others have shown concernthat some
antidepressant drugs promote suiciderather than prevent it,
particularly in childrenand adolescents, wherein adverse
mood-related ef-
fects, including suicide attempts is 4% in activedrug versus 2%
in placebo-treated patients. Thiswide-spread concern has resulted
in Black Boxwarnings by the United States Food and
DrugAdministration and outright declarations of contra-indications
for the United Kingdom for most antide-pressants. This led Varley
to ask, What optionsnow?.
In answer to Varleys question, magnesiumshould again become the
treatment of choice dueto its: (1) wide role in brain biochemistry,
(2)safety, (3) long history in treating depression and
other mental health issues. Depression appears tobe a magnesium
deficiency disorder especially inmajor and suicidal depression, but
not necessarilyin simple melancholy or depression caused byother
factors such as underlying disease (particu-larly hepatitis C),
hormonal imbalance (particularlyhypothyroidism and low
testosterone), low choles-terol, Wilsons Disease, food allergy
(particularlygluten intolerance), and adverse reaction
tomedications.
The benefit of magnesium to treat agitateddepression was first
published in 1921 by Weston[3]. Magnesium sulfate (10% elemental
magnesium)was injected in doses of one to two CCs of a 25% or50%
solution resulting in nearly all of his fifty pa-tients relaxing
and sleeping from 4 to 6 h.
Magnesium is recognized in homeopathic medi-cine for the
treatment of depression. For example,magnesium chloride (Magnesia
Muriatica) has beenused for many decades to relieve various
emotionalproblems including anxiety, apathy, aversions, des-pair,
depression, discontent, headaches, insecu-rity, irritability, over
sensitiveness, restlessness,sulkiness, talkativeness and
uncertainty.
Wacker and Parisi [4] reported in 1968 that mag-nesium
deficiency could cause numerous neuro-muscular symptoms including
hyperexcitability,depression, behavior disturbances, tetany,
head-aches, generalized tonic-clonic as well as focal sei-zures,
ataxia, vertigo, muscular weakness,tremors, irritability, and
psychotic behavior, each
of which were reversible by magnesium repletion.According to
Durlach and Bac [5], the mentalhealth pattern induced through
simple magnesiumdeficiency is always neurotic and never
psychotic,for example: generalized anxiety, panic attack
dis-orders, and depression. Other psychiatric symp-toms from
magnesium deficiency consisted ofhyperemotionality, asthenia,
headache, insomnia,dizziness, nervous fits, lipothymias (repeated
faint-ing), and sensations of a lump in the throat andof blocked
breathing, all of which can be effec-tively treated with magnesium.
Although a neurosispattern due to magnesium deficiency is
frequently
observed and simply cured through oral supplemen-tation,
neuroses are preeminently conditioningfactors for stress.
Cernak et al. [6] showed that chronic stress de-creases both
free and total plasma ionized magne-sium and simultaneously
increased oxidative stressin humans. These findings support the
need formagnesium supplementation for people living inconditions of
chronic stress. However, about 70%of United States and the West
have diets containingless than the recommended 400 mg of
magnesiumper day and up to 20% have diets with less than
one-half the recommended intake. Increased stressbuilds up
further worsening magnesium deficiency,with health issues such as
depression and cardio-vascular disease resulting.
Magnesium deficiency symptoms are non-spe-cific due to its
necessity in over 325 enzymes. Withmost of these enzymes being
brain-related, thepossibility that magnesium deficiency is
involvedin a variety of neurosis can be safely assumed.
Opportunity arose to test the hypothesis thatmagnesium would be
helpful in subjects with majordepressive disorders. After
explaining the possiblerisks and benefits, and obtaining informed
consent,the subjects proceeded to treat their depressionwith
magnesium.
Methods and procedures
A non-drinking, 59-year old hypomanic-depressivemale, having had
a long history of mild depressiontreatable with antidepressants,
suddenly becameextremely anxious, insomniac, tetanic and
suicid-ally depressed after a year of extreme personal,
2 Eby and Eby
ARTICLE IN PRESS
-
7/22/2019 Magnesium for Depression
3/9
business and noise stress and poor dietary habits(fast food). He
was not responsive to treatmentwith a number of antidepressants and
lithium car-bonate. After reviewing the report of Durlach
con-cerning magnesium and depression [5], he wastreated with
magnesium. He was given 300 mg ofmagnesium, as glycinate and later
as taurinate,
to take orally with each meal and at bedtime.A 23-year-old
woman, who had 5 years previ-ously suffered traumatic brain injury
and lost muchof her short term memory and some of her IQ, sud-denly
became severely depressed after experienc-ing long-term stress due
to several stressorsrelated to diet (fast food), work, constant
noise,and especially because of very poor academic per-formance
after having had excellent grades prior toher brain injury.
Antidepressants had beneficial ef-fects, but her concern about side
effects causedher to switch to magnesium. She was given200 mg of
magnesium (as taurinate) to take with
each meal and at bedtime.A 35-year old woman, having had three
children
followed by severe postpartum depression (PPD) ineach case, was
given 200 mg of magnesium (as gly-cinate) to take each meal during
her pregnancy toprevent PPD during her fourth pregnancy.
Antide-pressants had previously had some beneficial ef-fects, but
side effects were worrisome to her.Part of her decision to take
magnesium was her de-sire to prevent preeclampsia, a known but
often ig-nored magnesium deficiency condition [7].
A 40-year old man, irritable, anxious, extremely
talkative, moderately depressed, and heavily intouse of food,
tobacco (smoking and chewing), alco-hol and cocaine, took 125 mg of
magnesium (astaurinate) with each meal and at bedtime in an ef-fort
to relieve his symptoms.
Results
The 59-year old man experienced life-saving bene-fit from
magnesium. The first night after startingmagnesium, sleep was
restored essentially to nor-mal. Within the following 4 days,
depression wasgreatly reduced for 46 h after each magnesiumdosage.
Anxiety steadily disappeared. Tetany andheadaches rapidly
disappeared. On occasion,2:00AM doses were also required to
maintain afeeling of wellness. Over the following months,normalcy
was maintained only by frequent magne-sium ingestion. In this
patient, depression alwaysoccurred 1 h after taking a 500 mg
calcium (carbon-ate) dietary supplement, which was
extinguishablewithin 1 h only by administration of 400 mg of
mag-nesium. This man was extremely sensitive to cal-
cium, and elimination of all dairy andsupplemental forms of
calcium was mandatory formental stability. Osteoporosis due to low
calciumintake was feared, but a high magnesium and lowcalcium diet
did not have an adverse effect on hisbone density over a 5-year
observation period. Nor-mal life free of depression was difficult
to maintain
without frequent magnesium treatment, until Ke-fir, a rich
source of beneficial intestinal flora andinulin (vital for
magnesium absorption [8]), andindole-3-carbinol (200 mg per meal)
were addedto his diet. These nutrients seemed to stabilizethe
beneficial effect of magnesium, perhaps byimprovements in
intestinal absorption, digestionand immunity. After incorporation
of these agentsinto his diet, total wellness occurred, which
waseasily maintained with much less magnesium.
After 1 week of magnesium treatment, the 23-year old woman
became free of depression. Unex-pectedly, her short term memory and
IQ also
returned, benefits only previously shown in rats[9] when
immediately treated with magnesiumafter traumatic brain injury.
However, her mentalacuity returned nearly immediately upon
magne-sium treatment, even though the trauma had oc-curred 5 years
earlier.
The 35-year old woman delivered her baby onschedule without
developing any aspect of postpar-tum depression, preeclampsia or
any other illnessassociated with pregnancy. The baby was
healthy,full weight and quiet.
The 40-year old man found himself free of his
symptoms within a week, and unexpectedly foundhis craving for
smoking, dipping, cocaine and alco-hol to disappear also. It seemed
that magnesiumdeficiency caused his habituation. He also notedthat
his ravenous appetite was suppressed, andbeneficial and desired
weight loss ensued.
Discussion
We have shown efficacy, as have others, in treatingdepression
and some related mental disorders withmagnesium. We suggest that
magnesium treatmentwill be found effective in future clinical
trials, atleast to an extent equivalent to antidepressantdrugs, and
perhaps more effective.
The occurrence of depression 100 years ago wasrare, occurring
primarily in the elderly. Only 1% ofAmericans born before 1905
developed depressionbefore they were 75 years old, while 6% of
Ameri-cans born in 1955 developed depression by the timethey were
24 years old. [10] Previous to 1905,grains were not refined and
there was adequatemagnesium (over 400 mg per day) in the diet.
At
Rapid recovery from major depression using magnesium treatment
3
ARTICLE IN PRESS
-
7/22/2019 Magnesium for Depression
4/9
that time, refining was necessary to prevent spoil-age. One
hundred years later, only 16% of the mag-nesium found in whole
wheat grain remains inrefined flour, [11] lowering dietary intake
of mag-nesium in some severe cases by 250 mg per dayand setting the
stage for magnesium deficiency.Additionally, we often rely on diets
containing
too much calcium, while taking on more
stressfulactivities.Inadequate dietary magnesium in todays diet
is clearly evident from a 4-min 16-mb videoproduction titled,
Foods Containing 400 mgof Magnesium located on the Internet
at:http://coldcure.com/gif/foods-containing-400mg-magnesium.wmv.
Further, some city and residen-tial water treatment systems remove
all mineralsfrom drinking water, and bottled beverages nolonger
contain nearly as much minerals as theydid 100 years ago.
Consequently, due to wide-spread removal of magnesium from human
food
and drink, we hypothesize that most cases of ma-jor depression,
including postpartum depression,may be related to magnesium
deficiency.
Not only has the incidence of depression in-creased greatly in
the last 100 years, but the ageof onset has also fallen greatly.
Depression wasessentially unheard of in children in 1906.
Today,children in the United States are taking four timesthe amount
of psychiatric medications as childrenin the rest of the world
combined [12], with essen-tially no emphasis being placed on
magnesium intheir food. For example, we were not able to find
magnesium listed as an ingredient on any packagedfood, except
Planters Peanuts, in grocery storesin the United States.
Consequently, what used tobe a disease risk primarily for the
elderly is nowcommon in all ages including children.
Some dietary supplements sold in the UnitedStates and the West
contain magnesium, althoughthe ligand of choice for large-scale
manufacturersis oxide due to its compactness and ease ofuse in
manufacturing. Unfortunately, magnesiumoxide is not biologically
available in the humanbody [1315]. Other magnesium ligands
includingchloride, sulfate (Epsom Salts), citrate, lactate,malate,
glycinate and taurinate produce highly bio-logically available
magnesium complexes.
Taurine, Gamma-aminobutyric (GABA) acid andglycine are major
inhibitory neurotransmitters inthe central nervous system,
predominantly activein the spinal cord and brain stem. Taurineand
glycine also act as a modulator of excitatoryamino acid
transmission (glutamate) mediated byN-methyl-D-aspartate (NMDA)
receptors. Shealyet al. [16] found that magnesium and taurine
weredeficient in nearly all depressed patients.
Magnesium glutamate and magnesium aspartategreatly worsened the
59-year old mans depres-sion. A possible reason for this
observation is thatexcess glutamate is more cytotoxic than
cyanideto neurons in bringing into neurons toxic levels ofcalcium
ions [17]. These magnesium compoundsshould be considered as
neurotoxic to depressives,
and perhaps all people, and should not be used dur-ing treatment
of depression, anxiety or similarhyperemotional disorders. Food and
drink productscontaining monosodium glutamate and aspartateshould
not be used by depressives.
This report is based on internet page
http://coldcure.com/html/dep.html (Rapid RecoveryFrom Depression
Using Magnesium Treatment), a135 page report that receives a
quarter millionaccesses per year. This page is permanently
ar-chived on the WayBack machine at http://archive.org. Most
correspondence reported that the pageviewers depression was
effectively treated with
high-dose magnesium. Viewers were pleased to findsomething
natural that helped them instead ofusing prescription drugs. Most
reported havinghad treatment-resistant depression, while otherswere
simply reluctant to use psychiatric, antide-pressant drugs due to
their fear of side effects.While over 60,000 Internet pages were
foundusing the search terms major depression andmagnesium, there
were only 11 medical journalarticles found with the same search
terms. Thissuggests that the public is far more interested
inmagnesium for depression than is medical science.
The single largest obstacle to viewers success intreating
depression appeared to be continued,excessive intake of dietary
calcium. Some viewerswere found to have kidney or digestive
diseasesthat impaired magnesium metabolism, forestallingtheir
recovery from depression until those condi-tions were corrected.
Apparently, the use of in-dole-3-carbinol to improve magnesium
utilizationis new.
One physician-viewer, having suffered from se-vere depression
for two decades, reported thathe had found the above web page
several years ear-lier and totally dismissed it as being overly
simplis-tic, recounting that scientists are not so stupid asto have
overlooked magnesium. In total despera-tion, he finally tried
magnesium treatment and itcured his depression. Later, he became
verballyabusive with the writer because the page made itseem too
simple, and because of that, he had dis-missed the idea as
preposterous and continued tosuffer. Irritability is a sign of
modest magnesiumdeficiency, consequently this physician could
bediagnosed as needing more dietary magnesium.Although irritability
can cause violence, no clinical
4 Eby and Eby
ARTICLE IN PRESS
http://coldcure.com/gif/foods-containing-400mg-magnesium.wmvhttp://coldcure.com/gif/foods-containing-400mg-magnesium.wmvhttp://coldcure.com/html/dep.htmlhttp://coldcure.com/html/dep.htmlhttp://archive.org/http://archive.org/http://archive.org/http://archive.org/http://coldcure.com/html/dep.htmlhttp://coldcure.com/html/dep.htmlhttp://coldcure.com/gif/foods-containing-400mg-magnesium.wmvhttp://coldcure.com/gif/foods-containing-400mg-magnesium.wmv
-
7/22/2019 Magnesium for Depression
5/9
data has been published about the ability of mag-nesium to
prevent violence, although we hypothe-size that a magnesium-replete
population wouldbe less violent.
The main side effect reported from high-dosemagnesium and low
calcium intake as treatmentfor depression was diarrhea. This
results mainly
from the attachment of each magnesium ion toabout 800 molecules
of water in the intestinaltract. Any treatment to terminate
diarrhea,including lowering magnesium intake, was deemedessential
to promote proper absorption of nutri-ents. One gram of arginine
with each meal helpedprevent magnesium-induced diarrhea, while 3
gper meal caused severe constipation, perhapsdue to the effect of
excessive arginine-induced ni-tric oxide on nonadrenergic,
noncholinergic inhib-itory nerves of the colon [18]. Methods
ofintroducing magnesium to treat depression with-out causing
diarrhea were by injection, by rectum
and topical. Of these alternatives, daily topicalapplication to
the chest and back using 25% mag-nesium chloride solutions as
described by Shealy
[16] was preferred due to simplicity and apparentlack of side
effects.
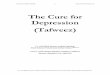
Fig. 1, by the University of California, San Diego Department of
Cognitive Science, shows magne-sium ion involvement in nerve cell
electrical con-duction activity in a regulatory fashion forcalcium
ions. Magnesium ions normally block cal-
cium ions within the N-methyl-D-aspartate (NMDA)receptor
channel. When magnesium ions are miss-ing, the channel is unblocked
and calcium ionsand sodium ions enter the postsynaptic neuron
aspotassium exits. Sapolsky [19] suggested that mag-nesium
depletion was likely to be deleterious toneurons possibly by
causing NMDA-coupled calciumchannels to be biased towards opening.
From ourobservations, Sapolsky is correct with the damageto neurons
appearing to the individual as depres-sion and related mood
disorders.
Paul [20] suggested that any means of reducingpathological
neuronal calcium ion flow to reduce
resulting pathological nitric oxide neuronal out-put would have
antidepressant effects. Durlachand Bac [5] reported that magnesium
deficiency
Figure 1 Magnesium has a role in regulating calcium ion flow in
neurons.
Rapid recovery from major depression using magnesium treatment
5
ARTICLE IN PRESS
-
7/22/2019 Magnesium for Depression
6/9
increased nitric oxide production. Too much cal-cium ion and
glutamate with insufficient magne-sium ion, particularly in the
hippocampus, playsa vital role in brain cell synaptic
dysfunctionleading to depression and other mood and behav-ioral
disorders. These observations help explainwhy the 59-year old man
was highly sensitive to
calcium and mono-sodium-glutamate, makinghim nearly immediately
depressed upon theirconsumption.
Murck [21] showed many actions of magnesiumions supporting their
possible therapeutic potentialin affective disorders. Examinations
of the sleep-electroencephalogram (EEG) and of the endocrinesystem
points to the involvement of the
limbichypothalamuspituitaryadrenocortical axis be-cause magnesium
affects all elements of thissystem. Magnesium has the property to
suppresshippocampal kindling, to reduce the release
ofadrenocorticotrophic hormone (ACTH) and to af-
fect adrenocortical sensitivity to ACTH. The roleof magnesium in
the central nervous system couldbe mediated via the
N-methyl-D-aspartate-antago-nistic, g-aminobutyric acid A-agonistic
or theangiotensin II-antagonistic property of this ion. Adirect
impact of magnesium on the function ofthe transport protein
p-glycoprotein at the levelof the blood-brain barrier has also been
demon-strated, possibly influencing the access of cortico-steroids
to the brain. Furthermore, magnesiumdampens the calcium ion-protein
kinase C relatedneurotransmission and stimulates the NaK-ATP-
ase. All these systems have been reported to be in-volved in the
pathophysiology of depression.Singewald et al. [22] also
demonstrated inducedmagnesium deficiency in mice to produce
depres-sion-like behavior which was beneficially influ-enced with
antidepressants.
What remains to be explained is exactly whycontrol of calcium
ions is lost in depression,although depletion of magnesium ions
certainlycould cause it by impairing control of calciumions in
neuronal channels resulting in calciumion cascades that are
pathological (excitotoxic).A compelling argument for the use of
calciumchannel blockers, such as therapeutic doses ofmagnesium, is
that the influx of calcium ionsfrom the extracellular fluid to the
cytosol of cellsthrough calcium channels is important for theproper
release of neurotransmitters from presyn-aptic neurons [23].
Interestingly, some calciumchannel blocking drugs used in
cardiology havebeen reported to increase depression and
suiciderisk.
Seelig and Rosanoff [24] reviewed the evidencethat chronic
stress depletes magnesium reservoirs,
increasing the risk of depression. Elevated cortisolin a subset
of depressives is an enduring and well-replicated finding [25].
Papadopol et al. [26] in Romania compared theIntelligence Quota
(IQ) of children growing up athome compared with the IQ of children
growingup in a stressful orphanage. Stress from orphanage
living drove down intracellular magnesium so se-verely that
orphans lost much of their IQ (seeFig. 2). Attention, memory,
psychoticism and neu-roticism were also similarly, but less,
affected.Magnesium deficit caused a number of neuropsy-chological
disorders including, agitation, anxiety,depression, irritability,
weakness, fatigue, confu-sion, asthenia, sleeplessness, headache,
convulsiveand nervous attacks, delirium, hallucinations
andhyperexcitability [26]. Nothing could be moreharmful to the
minds of children than stress-in-duced magnesium deficiency. Yet,
in search of aca-demic excellence increasingly more stress is
applied to children. Their diets are often insuffi-cient in
magnesium to protect them from stress,consequently they are treated
with antidepressantsand other drugs.
There are reports that there was no differencein the serum
concentration of magnesium ion orcalcium/magnesium ratios [27], and
that magne-sium was higher in serum of depressives [28], how-ever,
these observations do not represent what is
Figure 2 Distortion in childrens IQ attributed tostress-induced
damage to intracellular magnesium ininstitutionalized homes vs.
home living fromPapadopol.
6 Eby and Eby
ARTICLE IN PRESS
-
7/22/2019 Magnesium for Depression
7/9
going on inside the central nervous system. Bankiet al. [29]
showed that both cerebrospinal fluid 5-hydroxyindoleacetic acid
(5-HIAA) and magnesiumions are low in suicidal depressives. Levine
et al.[30] showed that there were high serum and cere-brospinal
fluid calcium to magnesium ratios in re-cently hospitalized acutely
depressed patients.
Kalinin et al. [31] using magnesium lactate andvitamin B-6
(required for absorption of magnesium)showed benefit in anxiety and
depression treat-ment in patients with epilepsy. There are
numerousreports showing magnesium to be extremely bene-ficial in
treating attention deficit hyperactivity dis-order (ADHD),
suggesting that ADHD is a symptomof magnesium deficiency [32].
Hypothyroidism, a known cause of depression, isassociated with
low magnesium with circulating T4levels being directly correlated
with magnesiumserum levels [33]. The depression attributable
tohypothyroidism is hypothesized to be caused by
resultant low magnesium, which is restored to nor-mal only by
proper treatment of hypothyroidism.
Several secondary injury factors have been iden-tified in
traumatic brain injury including oxidativestress, changes in blood
flow, neurotransmittersand metal ionic changes, edema and energy
fail-ure. Of these, magnesium ion decline has beenidentified as
playing a crucial role in the secondaryinjury process [34].
Postpartum depression can be much more se-vere than clinical
depression. The fetus and pla-centa absorb enormous amounts of
nutrients
(especially magnesium) from the mother and lossof magnesium to
the fetus coupled with insufficientintake of magnesium by the
mother is hypothesizedto be the cause of postpartum depression.
Lacta-tion is also known to deplete maternal magnesium[4]. Our
observations support this otherwise unre-ported concept.
Consistent with our observations, elimination ofcravings by
magnesium for tobacco, alcohol andcocaine has been separately
observed. For exam-ple, Nechifor et al. [35] found that magnesium
sup-plements reduced the number of cigarettessmoked. Margolin et
al. [36] demonstrated utilityof magnesium in reducing the craving
for cocaine.Murray and Berger [37] showed that magnesiumwas helpful
in alcohol withdrawal. The Alturas[38] showed that alcohol greatly
lowered serummagnesium, raising the potential for headaches,strokes
and brain injury.
The process of normal aging is accompanied bychanges in
sleep-related endocrine activity, and indepression sleep is often
highly disturbed. Duringaging an increase in cortisol and a
decrease in re-nin and aldosterone concentration occur. In aged
subjects more time is spent awake and slow-wavesleep is reduced.
The natural NMDA antagonistand GABA agonist, magnesium ion, plays a
keyrole in the regulation of sleep and endocrine sys-tems such as
the HPA system and renin-angioten-sin-aldosterone system. Magnesium
ion partiallyreverses sleep EEG and nocturnal neuroendocrine
changes occurring during aging [39]. The similari-ties of the
effect of magnesium ion and lithiumion furthermore support the
efficacy of magne-sium ion as a mood stabilizer, and one may
showthat lithium ions play some of the roles normallyperformed by
magnesium ions in the brain.Clearly, magnesium (200400 mg) is
extremelyeffective in promptly inducing sleep when takenat bedtime,
and sleep is vital to recovery fromdepression.
Even national security issues may result frommagnesium
deficiency. Consider that Saudi Arabia,in its modernization
process, removes most magne-
sium and other minerals, such as boron (necessaryfor magnesium
absorption and proper brain func-tion [40,41]), from drinking water
processed by re-verse osmosis. Reliance on refined grain
products,rather than whole grain products, results in inade-quate
dietary magnesium. Inadequate magnesiumintake may be the cause of
the 40% depression rateamong the elderly [42], and the nearly 25%
depres-sion rate in the 1529 year old group [43], an agegroup that
is the main source of suicidal bombers.Consider that stress
depletes magnesium and in-creases oxidative stress in soldiers
during military
combat [6]. If all other factors between engagedarmies are
similar, surely the army having the mostresistance to stress via
adequate brain magnesiumwill prevail.
Low calcium and high magnesium (1:2 ratio) in-take is vastly
more beneficial to overall health,including depression,
cardiovascular disease andosteoporosis than high calcium and low
magnesium(2:1 ratio). The old 2:1 ratio worked well at a
muchearlier time when we were getting enough magne-sium from food
and water. Nevertheless, officialgovernmental and highly scholarly
dietary recom-mendations remain backward. Excessive calciumintake
prevents absorption of magnesium in theintestinal tract, adversely
affecting health[4,5,12,24,44].
The only bone and joint effect of the lowcalcium and high
magnesium diet on the 59-yearold man was complete elimination of
all joint andback pain. This observation reflects
terminatinghyperalgesia in rats via sensitization of
nociceptivepathways in the spinal cord involving NMDA andnon-NMDA
receptors by administration of magne-sium [45], which also explains
why most of Shealys
Rapid recovery from major depression using magnesium treatment
7
ARTICLE IN PRESS
-
7/22/2019 Magnesium for Depression
8/9
patients having depression with chronic pain weremagnesium
deficient [16].
Since magnesium has sedative properties, cau-tion is advised
when administering anesthesia andmagnesium, or anesthesia to
magnesium-repletepatients, as less anesthesia will be required
[46].
This report supports the overall hypothesis that
magnesium is therapeutic for depression and re-lated mental
disorders. However, in the UnitedStates, it is effectively illegal
to market nutrientsto treat, cure, and prevent diseases. This
discon-nect between policy and reality creates artificial,insidious
illnesses which are frustratingly hard toaddress at the policy
level, as was found by Aaserudet al. [7] in 2005 in their efforts
to promote magne-sium for the prevention of preeclampsia,
somethingthat was first demonstrated in 1925 by Lazard [47].
It is likely that magnesium deficiency causesmost major
depression and related mental healthillnesses, IQ loss and
addictions. We suggest that
magnesium deficiency as cause of these disordersis enormously
important to public health and is rec-ommended for immediate,
wide-spread furtherstudy. The public should be advised to obtain
morethan 600 mg of dietary magnesium a day to enablethem to
adequately handle stress and prevent neu-ronal calcium ion injury.
Fortifying refined grainand drinking water with biologically
available mag-nesium is recommended.
References
[1] World Health Organization. The World Health Report.Making a
Difference. Geneva: World Health Organization;1999.
[2] Varley CK. Treating depression in children and adolescents
:what options now?. CNS Drugs 2006;20:113.
[3] Weston PG. Magnesium as a sedative. Am J
Psychiat1921;78:6378.
[4] Wacker WE, Parisi AF. Magnesium metabolism. N Engl J
Med1968;278:7127. On Internet at
http://coldcure.com/html/magnesium-metabolism.html.
[5] Durlach D, Bac P. Chapter 20, Mechanisms of Action on
theNervous System in Magnesium Deficiency and Dementia. In:Yasui M,
Strong MJ, Ota K, Verity MA, editors. Mineral andmetal
neurotoxicology. Boca Raton, New York, London,Tokyo: CRC Press;
1997. On Internet at http://www.mgwa-ter.com/dur30.shtml.
[6] Cernak I, Savic V, Kotur J, Prokic V, Kuljic B, Grbovic D,et
al. Alterations in magnesium and oxidative status duringchronic
emotional stress. Magnes Res 2000;13:2936.
[7] Aaserud M, Lewin S, Innvaer S, Paulsen EJ, Dahlgren
AT,Trommald M, et al. Translating research into policy andpractice
in developing countries: a case study of magne-sium sulphate for
pre-eclampsia. BMC Health Serv Res2005;5:68.
[8] Coudray C, Demigne C, Rayssiguier Y. Effects of
dietaryfibers on magnesium absorption in animals and humans. JNutr
2003;133:14.
[9] Fromm L, Heath DL, Vink R, Nimmo AJ. Magnesiumattenuates
post-traumatic depression/anxiety followingdiffuse traumatic brain
injury in rats. J Am Coll Nutr2004;23:529S33S.
[10] Meyer JS, Linda F, Quenzer LF. Psychopharmacology, Drugsthe
Brain and Behavior. Sunderland, Maryland: SinauerAssociates; 2005.
p. 386.
[11] Anon.. Heart gains from whole grains. Harvard Heart
Lett.2002:24.
[12] Dean C. The miracle of magnesium. New York:
BallantineBooks; 2003.
[13] Firoz M, Graber M. Bioavailability of US
commercialmagnesium preparations. Magnes Res 2001;14:25762.
[14] Walker AF, Marakis G, Christie Byng M. Mg citrate foundmore
bioavailable than other Mg preparations in a random-ised,
double-blind study. Magnes Res 2003;16:18391.
[15] Lindberg JS, Zobitz MM, Poindexter JR, Pak CY.
Magnesiumbioavailability from magnesium citrate and magnesiumoxide.
J Am Coll Nutr 1990;9:4855.
[16] Shealy NC, Cady RK, Veehoff D, Houston R, Burnette M,
CoxRH, et al. The neurochemistry of depression. AJPM1992;2:136. On
the Internet at http://coldcure.com/html/shealy13.html.
[17] Mark LP, Prost RW, Ulmer JL, Smith MM, Daniels DL,
Strottmann JM, et al. Pictorial review of glutamate
excito-toxicity: fundamental concepts for neuroimaging. Am
JNeuroradiol 2001;22:181324.
[18] Tomita R, Fujisaki S, Ikeda T, Fukuzawa M. Role of
nitricoxide in the colon of patients with slow-transit
constipa-tion. Dis Colon Rectum 2002;45:593600.
[19] Sapolsky RM. Stress the aging brain and the mechanisms
ofneuron death. Cambridge, MA: A Bradford Book, The MITPress; 1992.
page 192.
[20] Paul IA. Antidepressant activity and calcium
signalingcascades. Hum Psychopharmacol 2001;16:7180.
[21] Murck H. Magnesium and affective disorders. Nutr
Neurosci2002;5:37589.
[22] Singewald N, Sinner C, Hetzenauer A, Sartori SB, Murck
H.Magnesium-deficient diet alters depression- and anxiety-
related behavior in mice influence of desipramine andHypericum
perforatum extract. Neuropharmacology2004;47:118997.
[23] Hollister LE, Trevino ESG. Calcium channel blockers
inpsychiatric disorders: a review of the literature. Can
JPsychiatry 1999;44:65864.
[24] Seelig MS, Rosanoff A. The magnesium factor. New
York:Penguin Group; 2003.
[25] Brown ES, Varghese FP, McEwen BS. Association of
depres-sion with medical illness: does cortisol play a role?.
BiolPsychiat 2004;55:19.
[26] Papadopol V, Tuchendria E, Palamara I. Magnesium andsome
psychological features in two groups of pupils(magnesium and
psychic features). Magnes Res 2001;14(1/2):2732. On the Internet at
http://coldcure.com/html/mag-iq.html.
[27] Young LT, Robb JC, Levitt AJ, Cooke RG, Joffe RT. SerumMg2+
and Ca2+/Mg2+ ratio in major depressive disorder.Neuropsychobiology
1996;34:268.
[28] Imada Y, Yoshioka S, Ueda T, Katayama S, Kuno Y,Kawahara R.
Relationships between serum magnesiumlevels and clinical background
factors in patients withmood disorders. Psychiat Clin Neurosci
2002;56:50914.
[29] Banki CM, Arato M, Kilts CD. Aminergic studies
andcerebrospinal fluid cations in suicide. Ann N Y Acad
Sci1986;487:22130.
[30] Levine J, Stein D, Rapoport A, Kurtzman L. High serum
andcerebrospinal fluid Ca/Mg ratio in recently hospitalized
8 Eby and Eby
ARTICLE IN PRESS
http://coldcure.com/html/magnesium-metabolism.htmlhttp://coldcure.com/html/magnesium-metabolism.htmlhttp://www.mgwater.com/dur30.shtmlhttp://www.mgwater.com/dur30.shtmlhttp://coldcure.com/html/shealy13.htmlhttp://coldcure.com/html/shealy13.htmlhttp://coldcure.com/html/mag-iq.htmlhttp://coldcure.com/html/mag-iq.htmlhttp://coldcure.com/html/mag-iq.htmlhttp://coldcure.com/html/mag-iq.htmlhttp://coldcure.com/html/shealy13.htmlhttp://coldcure.com/html/shealy13.htmlhttp://www.mgwater.com/dur30.shtmlhttp://www.mgwater.com/dur30.shtmlhttp://coldcure.com/html/magnesium-metabolism.htmlhttp://coldcure.com/html/magnesium-metabolism.html
-
7/22/2019 Magnesium for Depression
9/9
acutely depressed patients. Neuropsychobiology 1999;39:6370.
[31] Kalinin VV, Zheleznova EV, Rogacheva TA, Sokolova
LV,Polianskii DA, Zemlianaia AA, et al. [A use of Magne-B6 inthe
treatment of anxiety-depressive states in patients withepilepsy].
Zh Nevrol Psikhiatr Im S S Korsakova 2004;104:515.
[32] Mousain-Bosc M, Roche M, Rapin J, Bali JP. MagnesiumVitB6
intake reduces central nervous system hyperexcit-
ability in children. J Am Coll Nutr 2004;23:545S8S.[33] Joffe
RT, Levitt AJ, Young LT. The thyroid, magnesium and
calcium in major depression. Biol Psychiat 1996;40:4289.[34] van
den Heuvel C, Vink R. The role of magnesium in
traumatic brain injury. Clin Calcium 2004;14:914.[35] Nechifor
M, Chelarescu D, Mandreci I, Cartas N. Magnesium
influence on nicotine pharmacodependence and smoking.Magnes Res
2004;17:17681.
[36] Margolin A, Kantak K, Copenhaver M, Avants SK. A
pre-liminary, controlled investigation of magnesium
L-aspartatehydrochloride for illicit cocaine and opiate use in
metha-done-maintained patients. J Addict Dis 2003;22:4961.
[37] Murray TD, Berger A. Alcohol withdrawal. Va Med
Q1997;124:1847. 189.
[38] Altura BM, Altura BT. Association of alcohol in brain
injury,
headaches, and stroke with brain-tissue and serum levels
ofionized magnesium: a review of recent findings andmechanisms of
action. Alcohol 1999;19:11930.
[39] Held K, Antonijevic IA, Kunzel H, Uhr M, Wetter TC,
GollyIC, et al. Oral Mg (2+) supplementation reverses age-related
neuroendocrine and sleep EEG changes in humans.Pharmacopsychiatry
2002;35:13543.
[40] Meacham SL, Taper LJ, Volpe SL. Effect of boron
supple-mentation on blood and urinary calcium, magnesium,
andphosphorus, and urinary boron in athletic and sedentarywomen. Am
J Clin Nutr 1995;61:3415.
[41] Penland JG. Quantitative analysis of EEG effects
followingexperimental marginal magnesium and boron
deprivation.Magnes Res 1995;8:34158.
[42] Al-Shammari SA, Al-Subaie A. Prevalence and correlates
ofdepression among Saudi elderly. Int J Geriatr Psychiat
1999;14:73947.[43] Al-Khathami AD, Ogbeide DO. Prevalence of
mental illness
among Saudi adult primary-care patients in Central SaudiArabia.
Saudi Med J 2002;23:7214.
[44] Seelig MS. Magnesium deficiency in the pathogenesis
ofdisease: early roots of cardiovascular, skeletal and
renalabnormalities. 1980, Goldwater Memorial Hospital, NewYork
University Medical Center, New York, New York.(On Internet at:
http://www.mgwater.com/Seelig/Mag-nesium-Deficiency-in-the-Pathogenesis-of-Disease/jacket.shtml).
[45] Begon S, Pickering G, Eschalier A, Mazur A, Rayssiguier
Y,Dubray C. Role of spinal NMDA receptors, protein kinase Cand
nitric oxide synthase in the hyperalgesia induced bymagnesium
deficiency in rats. Br J Pharmacol 2001;134:
122736.[46] Dube L, Granry JC. The therapeutic use of magnesium
in
anesthesiology, intensive care and emergency medicine: areview.
Can J Anaesth 2003;50:73246.
[47] Lazard EM. A preliminary report on the intravenous use
ofmagnesium sulfate in puerperal eclampsia. Am J ObstGynec
1925;9:17888.
Rapid recovery from major depression using magnesium treatment
9
ARTICLE IN PRESS
http://www.mgwater.com/Seelig/Magnesium-Deficiency-in-the-Pathogenesis-of-Disease/jacket.shtmlhttp://www.mgwater.com/Seelig/Magnesium-Deficiency-in-the-Pathogenesis-of-Disease/jacket.shtmlhttp://www.mgwater.com/Seelig/Magnesium-Deficiency-in-the-Pathogenesis-of-Disease/jacket.shtmlhttp://www.mgwater.com/Seelig/Magnesium-Deficiency-in-the-Pathogenesis-of-Disease/jacket.shtmlhttp://www.mgwater.com/Seelig/Magnesium-Deficiency-in-the-Pathogenesis-of-Disease/jacket.shtmlhttp://www.mgwater.com/Seelig/Magnesium-Deficiency-in-the-Pathogenesis-of-Disease/jacket.shtml