Embed Size (px)
Citation preview

Br Heart J 1986;56:455-62
Magnetic resonance assessment of aortic and mitralregurgitationS R UNDERWOOD, R H KLIPSTEIN, D N FIRMIN, K M FOX,P A POOLE-WILSON, R S 0 REES, D B LONGMORE
From the National Heart and Chest Hospitals, London
SUMMARY Magnetic resonance imaging provides an accurate method for the measurement of leftand right ventricular volume. The ratio of left ventricular stroke volume to right ventricular strokevolume was calculated from contiguous transverse magnetic resonance images and was used tomeasure the severity of regurgitation in 18 patients with aortic regurgitation and 10 with mitralregurgitation. Cardiac anatomy was well demonstrated, allowing an assessment of relative cham-ber volumes and associated abnormalities, although valve abnormality was not well seen. Therewas a weak correlation between magnetic resonance measurements of left ventricular end diastolicvolume and stroke volume ratio. The stroke volume ratio differed significantly in four groups withincreasing angiographic severity of regurgitation, and all but the group with trivial regurgitationdiffered significantly from normal. There was good correlation between magnetic resonance andradionuclide measurements of left ventricular ejection fraction and stroke volume ratio, althoughthe stroke volume ratio was consistently overestimated by radionuclide ventriculography.Correlation was less good for the right ventricular ejection fraction, which was underestimatedby radionuclide ventriculography.
It is concluded that magnetic resonance imaging provides valuable information in patients withvalvar regurgitation, and serves as a suitable standard by which to judge conventional techniques.
Magnetic resonance imaging now has an establishedplace in diagnostic imaging of the brain and spinalcord. Its value lies in high soft tissue contrast andhigh resolution and in the fact that contrast is deter-mined partly by the biochemical environment of theprotons forming the image. Moving organs in thethorax and abdomen require special techniques tominimise artefact, but images ofthe heart with excel-lent anatomical definition can be produced with elec-trocardiographic gating alone.' 3 Contrast mediaare not required because of the natural contrastbetween myocardium and flowing blood whichusually gives no magnetic resonance signal.
Functional and anatomical information areobtained, and we have previously demonstrated thatcardiac chamber volumes can be measured with anaccuracy of approximately 2%.4 Ventricular volumemeasurements allow an assessment of systolic ven-
Requests for reprints to Dr S R Underwood, Magnetic ResonanceUnit, The National Heart and Chest Hospitals, 30 Britten Street,London SW3 6NN.
Accepted for publication 10 June 1986
tricular performance (end systolic volume and ejec-tion fraction), and the ratio of left ventricular strokevolume to right ventricular stroke volume gives ameasure of valvar regurgitation and atrial shunting.'In this study we have used measurements of left andright ventricular stroke volume to quantify theseverity of aortic and mitral regurgitation and wehave compared these findings with measurementsmade by radionuclide ventriculography and cardiaccatheterisation.
Patients and methods
PATIENTSWe studied 28 patients (17 male, 1 1 female, mean age53 5 (range 18-75)). Eighteen had isolated aorticregurgitation and 10 had isolated mitral regur-gitation. The aetiology of aortic valve disease wasunknown in nine, a bicuspid valve in two, Marfan'ssyndrome in one, ankylosing spondylitis in one,rheumatic valve disease in one, leaking homograftsin three, and a leaking pulmonary valve autograft inone. The aetiology of mitral regurgitation was valve
455
on 22 May 2018 by guest. P
rotected by copyright.http://heart.bm
j.com/
Br H
eart J: first published as 10.1136/hrt.56.5.455 on 1 Novem
ber 1986. Dow
nloaded from

Underwood, Klipstein, Firmin, Fox, Poole- Wilson, Rees, Longmoreprolapse in seven, Marfan's syndrome in one, hyper-trophic cardiomyopathy in one, and coronary arterydisease in one. All patients were in sinus rhythmexcept four with mitral regurgitation who were inatrial fibrillation.
All patients were studied by magnetic resonance,26 underwent cardiac catheterisation, and 26 equi-librium radionuclide ventriculography, investi-gations in each patient being completed within 8weeks.
MAGNETIC RESONANCEA Picker International Vista MR2055 magnetic res-onance scanner operating at 0 5 T was used toacquire multiple 10mm contiguous sections in thetransverse plane at end diastole and at end systole.The images were reconstructed by two dimensionalFourier transformation from two averages of 128spin echo sequences (echo time 24ms). Diastolicimages were acquired immediately after the R waveof the electrocardiogram, and systolic images weretimed to coincide with the end of the T wave.Diastole at one level was acquired at the same timeas systole at another, and each pair of images tookbetween 3 and 4 minutes to acquire, depending uponheart rate. Preliminary coronal images were acquiredin the plane of the aortic valve and sagittal images inthe plane of the pulmonary valve; 12 transverseimages were usually sufficient to cover both ventri-cles. Total imaging time was between 40 and 60minutes.
Left and right ventricular endocardial contourswere assigned manually by use of a Nodecrest V77computer, and diastolic and systolic volumes weremeasured by summing the areas of the chambers ineach transverse image. The left and right ventricularstroke volumes, ejection fractions, and the left toright ventricular stroke volume ratio were derivedfrom the volumes.
RADIONUCLIDE VENTRICULOGRAPHYEquilibrium radionuclide ventriculography wasperformed after in vivo erythrocyte labelling with740MBq of technetium-99m sodium pertech-netate.6 Sixteen frames were acquired in the leftanterior oblique projection with 300 of caudal tilt bymeans of a Siemens gamma camera (200mm field ofview) and a Medical Data Systems "A2" computer.Fourier phase and amplitude images wereconstructed7 and used together with the enddiastolic and end systolic images to assign left andright ventricular regions of interest. Counts withinthese regions were used to calculate left and rightventricular ejection fractions and the left to rightventricular stroke volume ratio. Background counts
were estimated from a crescentic region inferior andlateral to the left ventricle.
CARDIAC CATHETERISATIONMitral and aortic regurgitation were assessed froman x ray contrast left ventriculogram and aortogramrespectively by one of three consultant radiologistswithout knowledge of the magnetic resonance orradionuclide findings. Aortic regurgitation wasclassified as trivial (I), mild (II), moderate (III), orsevere (IV) according to whether regurgitant con-trast opacified the left ventricle incompletely and wascleared at end systole (I), failed to be cleared at endsystole (II), accumulated within the left ventriclewith complete opacification (III), or filled the ven-tricle completely at the end of the first diastole fol-lowing injection (IV).89 Mitral regurgitation wasclassified into the same grades according to the sizeof the regurgitant jet and the degree of left atrialopacification, taking into account the size of the leftatrium.10 l
STATISTICAL ANALYSISThe Wilcoxon rank-sum test was used to comparemeasurements between groups and to compare witha group of normal subjects previously studied by thesame methods.4
Results
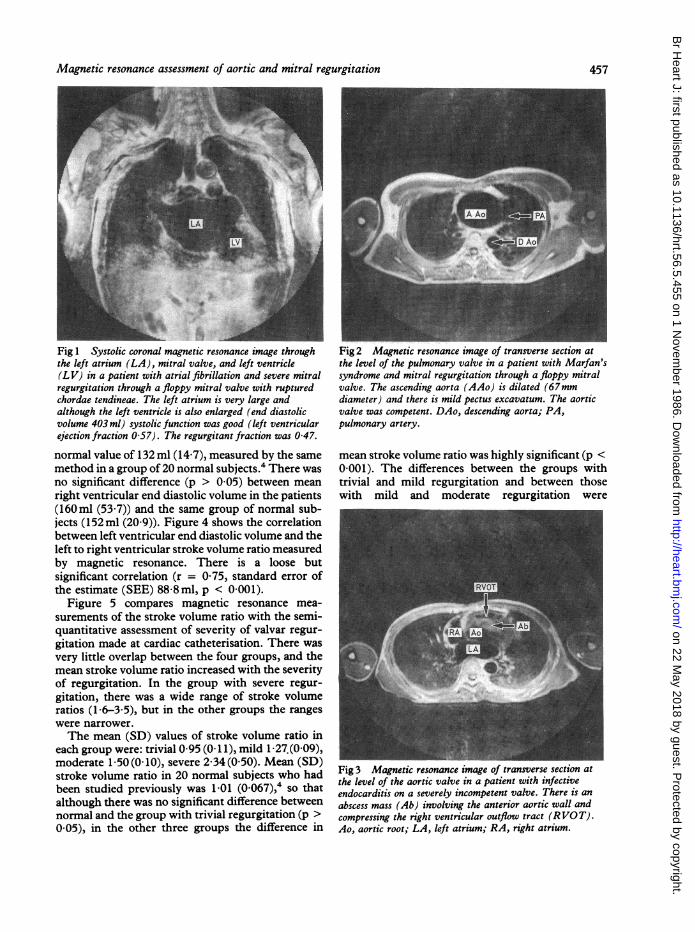
Magnetic resonance image quality depended mainlyupon the ability of the patient to keep still duringacquisition and upon the cardiac rhythm. In the fourpatients with atrial fibrillation the images were ofpoorer quality but it was still possible to measureventricular volume. Figure 1 shows a coronal imagein one of the patients with atrial fibrillation andmitral regurgitation due to valve prolapse.
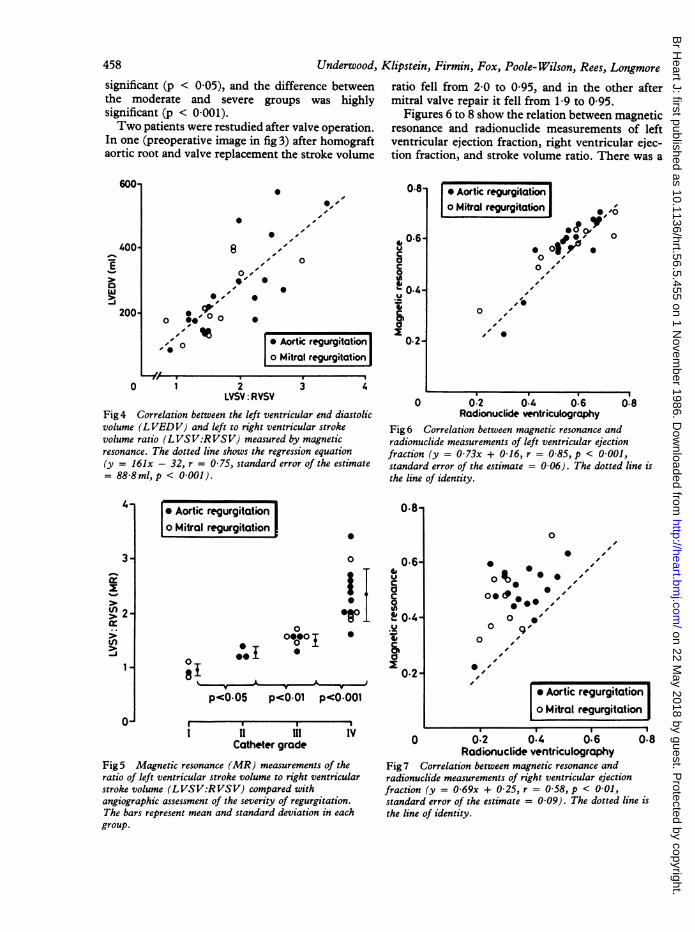
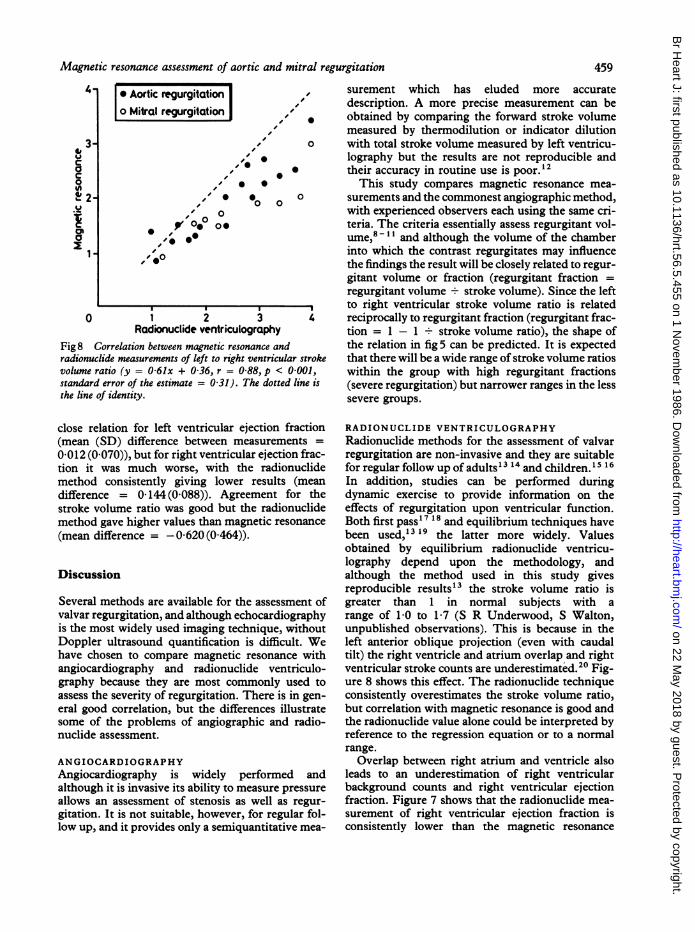
Cardiac anatomy was easily judged from theimages, giving an estimate of relative chamber sizes,myocardial hypertrophy, and aortic dilatation. Fig-ure 2 shows the dilated ascending aorta in a patientwith Marfan's syndrome and mitral valve prolapse.In one patient with aortic regurgitation studied dur-ing an episode of infective endocarditis, an abscessmass was seen involving the anterior aortic wall com-pressing the right ventricular outflow tract (fig 3).This abnormality was also shown by echo-cardiography. The aortic and mitral valves were vis-ible in many of the patients, particularly the mitralvalve in the systolic images, but resolution was notsufficient to identify valve abnormalities.Mean (SD) left ventricular end diastolic volume in
the whole group of patients was 262 ml (131.5),which is significantly higher (p < 0-001) than the
456
on 22 May 2018 by guest. P
rotected by copyright.http://heart.bm
j.com/
Br H
eart J: first published as 10.1136/hrt.56.5.455 on 1 Novem
ber 1986. Dow
nloaded from
Magnetic resonance assessment of aortic and mitral regurgitation
Fig 1 Systolic coronal magnetic resonance image through Fig 2 Magnetic resonance image of transverse section atthe left atrium (LA), mitral valve, and left ventricle the level of the pulmonary valve in a patient with Marfan's(LV) in a patient with atrial fibrillation and severe mitral syndrome and mitral regurgitation through a floppy mitralregurgitation through a floppy mitral valve with ruptured valve. The ascending aorta (AAo) is dilated (67mmchordae tendineae. The left atrium is very large and diameter) and there is mild pectus excavatum. The aorticalthough the left ventricle is also enlarged (end diastolic valve was competent. DAo, descending aorta; PA,volume 403 ml) systolic function was good (left ventricular pulmonary artery.ejection fraction 057). The regurgitant fraction was 0 47.
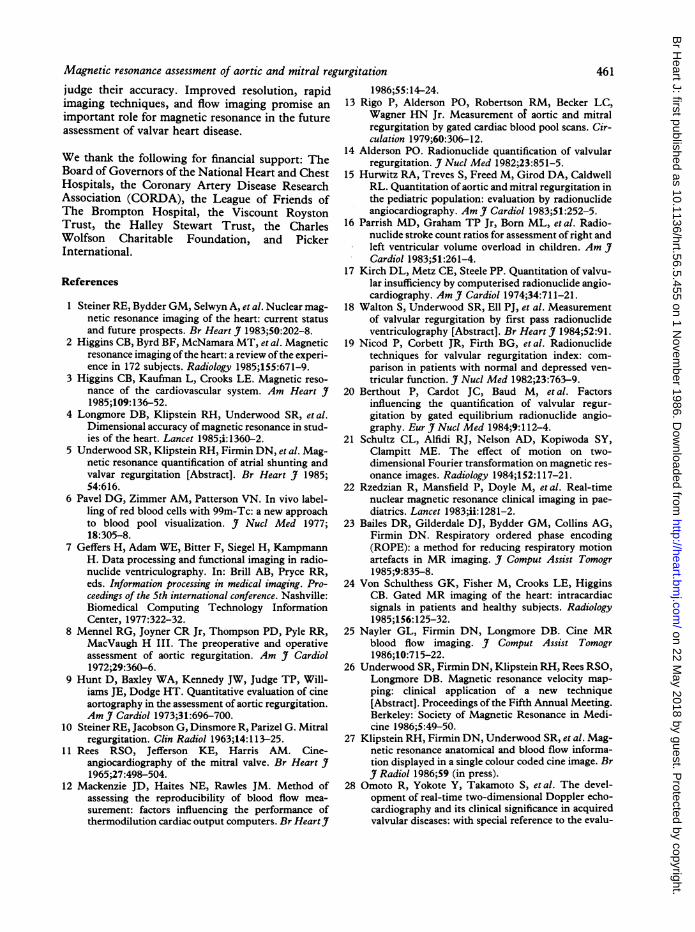
normal value of 132 ml (14 7), measured by the samemethod in a group of 20 normal subjects.4 There wasno significant difference (p > 0 05) between meanright ventricular end diastolic volume in the patients(160ml (53.7)) and the same group of normal sub-jects (152 ml (20 9)). Figure 4 shows the correlationbetween left ventricular end diastolic volume and theleft to right ventricular stroke volume ratio measuredby magnetic resonance. There is a loose butsignificant correlation (r = 0 75, standard error ofthe estimate (SEE) 88-8 ml, p < 0-001).
Figure 5 compares magnetic resonance mea-surements of the stroke volume ratio with the semi-quantitative assessment of severity of valvar regur-gitation made at cardiac catheterisation. There wasvery little overlap between the four groups, and themean stroke volume ratio increased with the severityof regurgitation. In the group with severe regur-gitation, there was a wide range of stroke volumeratios (1 6-3 5), but in the other groups the rangeswere narrower.The mean (SD) values of stroke volume ratio in
each group were: trivial 0 95 (0 11), mild 127.(0-09),moderate 1-50(0-10), severe 2-34(0 50). Mean (SD)stroke volume ratio in 20 normal subjects who hadbeen studied previously was 1 01 (0-067),4 so thatalthough there was no significant difference betweennormal and the group with trivial regurgitation (p >0 05), in the other three groups the difference in
mean stroke volume ratio was highly significant (p <0 001). The differences between the groups withtrivial and mild regurgitation and between thosewith mild and moderate regurgitation were
Fig 3 Magnetic resonance image of transverse section atthe level of the aortic valve in a patient with infectiveendocarditis on a severely incompetent valve. There is anabscess mass (Ab) involving the anterior aortic wall andcompressing the right ventricular outflow tract (RVOT).Ao, aortic root; LA, left atrium; RA, right atrium.
457
on 22 May 2018 by guest. P
rotected by copyright.http://heart.bm
j.com/
Br H
eart J: first published as 10.1136/hrt.56.5.455 on 1 Novem
ber 1986. Dow
nloaded from
Underwood, Klipstein, Firmin, Fox, Poole- Wilson, Rees, Longmoresignificant (p < 0 05), and the difference betweenthe moderate and severe groups was highlysignificant (p < 0 001).Two patients were restudied after valve operation.
In one (preoperative image in fig 3) after homograftaortic root and valve replacement the stroke volume
ratio fell from 2-0 to 0-95, and in the other aftermitral valve repair it fell from 1 9 to 0 95.
Figures 6 to 8 show the relation between magneticresonance and radionuclide measurements of leftventricular ejection fraction, right ventricular ejec-tion fraction, and stroke volume ratio. There was a
* - n.A.8 ,0 ,
leol0-0
0.1-., 0 4L._
*0 9~~~~~
. Aortic regurgitation| 0.2-o Mitral regurgitation
2LVSV: RVSV
3 4
Fig 4 Correlation between the left ventricular end diastolicvolume (LVEDV) and left to right ventricular strokevolume ratio (LVSV:RVSV) measured by magneticresonance. The dotted line shows the regression equation(y = 161x - 32, r = 0 75, standard error of the estimate= 88 8 ml, p < 0 001) .
* Aortic regurgitationo Mitral regurgitation *,o
0o{>o
0 '
I.
- 0
0 0-2 0.4 0.6 0-8Radionuclide ventriculography
Fig6 Correlation between magnetic resonance andradionuclide measurements of left ventricular ejectionfraction (y = 0 73x + 0 16, r = 0-85, p < 0 001,standard error of the estimate = 0-06). The dotted line isthe line of identity.
0.8-Aortic regurgitationlo Mitral regurgitation
0
0 0-6-
0~~~~~~~4J00T0o 0Y
0o0o I 0* X
o *I *c
0i 009
81 0.2'
p<0.05 p<0.01 pC<0.00
I Ii I~I 11ICeCatheter grcade
1V
Fig 5 Magnetic resonance (MR) measurements of theratio of left ventricular stroke volume to right ventricularstroke volume (LVSV:RVSV) compared withangiographic assessment of the severity of regurgitation.The bars represent mean and standard deviation in eachgroup.
0
0
0
0 -
o 0.-.0.0 - --~~~~~~.
0 *'o 9,
0 -
0'*
Aortic regurgitation|o Mitral regurgitation|
** .~~~~~~~~~~~~~~~
0.2 0.4 0.6Radionuclide ventriculography
Fig 7 Correlation between magnetic resonance andradionuclide measurements of right ventricular ejectionfraction (y = 0O69x + 0-25, r = 0-58, p < 0 01,standard error of the estimate = 0-09). The dotted line isthe line of identity.
458
600-
400OE
2000*
0 ,o 00
.1%I.0
0 1
4-
3-
~I-
1-
0-0.8
- x
I I I a
v I I I
0-8-
on 22 May 2018 by guest. P
rotected by copyright.http://heart.bm
j.com/
Br H
eart J: first published as 10.1136/hrt.56.5.455 on 1 Novem
ber 1986. Dow
nloaded from
Magnetic resonance assessment of aortic and mitral regurgitation
4- Aortic regurgitationo Mitral regurgitaition
3-toU
5c0
1 2-
1-
0
*0
, '0 0-1 0
* , 00~. .
.0.00
0
1 2 3Radionuclide ventriculograph
Fig 8 Correlation between magnetic resonanceradionuclide measurements of left to right ventrivolume ratio (y = 0 61x + 0-36, r = 0-88, pstandard error of the estimate = 0 31). The dothe line of identity.
close relation for left ventricular ejection fraction(mean (SD) difference between measurements =0 012 (0 070)), but for right ventricular ejection frac-tion it was much worse, with the radionuclidemethod consistently giving lower results (meandifference = 0-144 (0 088)). Agreement for thestroke volume ratio was good but the radionuclidemethod gave higher values than magnetic resonance(mean difference = - 620 (0 464)).
Discussion
Several methods are available for the assessment ofvalvar regurgitation, and although echocardiographyis the most widely used imaging technique, withoutDoppler ultrasound quantification is difficult. Wehave chosen to compare magnetic resonance withangiocardiography and radionuclide ventriculo-graphy because they are most commonly used toassess the severity of regurgitation. There is in gen-eral good correlation, but the differences illustratesome of the problems of angiographic and radio-nuclide assessment.
ANGIOCARDIOGRAPHYAngiocardiography is widely performed andalthough it is invasive its ability to measure pressureallows an assessment of stenosis as well as regur-gitation. It is not suitable, however, for regular fol-low up, and it provides only a semiquantitative mea-
- - surement which has eluded more accurate,' description. A more precise measurement can be
, * obtained by comparing the forward stroke volumemeasured by thermodilution or indicator dilution
o with total stroke volume measured by left ventricu-lography but the results are not reproducible and
0* their accuracy in routine use is poor.'2This study compares magnetic resonance mea-
0 ° surements and the commonest angiographic method,with experienced observers each using the same cri-teria. The criteria essentially assess regurgitant vol-ume,8 -11 and although the volume of the chamberinto which the contrast regurgitates may influencethe findings the result will be closely related to regur-gitant volume or fraction (regurgitant fraction =regurgitant volume - stroke volume). Since the left
- , to right ventricular stroke volume ratio is related4. reciprocally to regurgitant fraction (regurgitant frac-
lY tion = 1 - 1 + stroke volume ratio), the shape ofand the relation in fig5 can be predicted. It is expectedicular stroke that there will be a wide range of stroke volume ratios< 0001, within the group with high regurgitant fractionstted line is (severe regurgitation) but narrower ranges in the less
severe groups.
RADIONUCLIDE VENTRICULOGRAPHYRadionuclide methods for the assessment of valvarregurgitation are non-invasive and they are suitablefor regular follow up of adults'3 14 and children.'5 16In addition, studies can be performed duringdynamic exercise to provide information on theeffects of regurgitation upon ventricular function.Both first pass' 7 18 and equilibrium techniques havebeen used,'3 19 the latter more widely. Valuesobtained by equilibrium radionuclide ventricu-lography depend upon the methodology, andalthough the method used in this study givesreproducible results'3 the stroke volume ratio isgreater than 1 in normal subjects with arange of 1-0 to 1-7 (S R Underwood, S Walton,unpublished observations). This is because in theleft anterior oblique projection (even with caudaltilt) the right ventricle and atrium overlap and rightventricular stroke counts are underestimated.20 Fig-ure 8 shows this effect. The radionuclide techniqueconsistently overestimates the stroke volume ratio,but correlation with magnetic resonance is good andthe radionuclide value alone could be interpreted byreference to the regression equation or to a normalrange.
Overlap between right atrium and ventricle alsoleads to an underestimation of right ventricularbackground counts and right ventricular ejectionfraction. Figure 7 shows that the radionuclide mea-surement of right ventricular ejection fraction isconsistently lower than the magnetic resonance
459
.1
.1 -.
on 22 May 2018 by guest. P
rotected by copyright.http://heart.bm
j.com/
Br H
eart J: first published as 10.1136/hrt.56.5.455 on 1 Novem
ber 1986. Dow
nloaded from

Underwood, Klipstein, Firmin, Fox, Poole- Wilson, Rees, Longmoremeasurement but, more importantly, correlationbetween the two is not as good as for the left ven-tricle. This implies that the contribution of the rightatrium to background is very variable, and right ven-tricular ejection fraction measured by this techniqueshould be interpreted with caution.
MAGNETIC RESONANCEVolume measurements by magnetic resonance arevery simple but there are several points to considerin achieving accurate results. Most important isimage quality and patient cooperation is essential forthis.2' In future imaging times will be reduced,simplifying the imaging of sick or uncooperativepatients: real time imaging is already possible.22Respiratory gating can be used to eliminate respira-tory motion artefact, but imaging time is unaccept-ably prolonged and alternative techniques such asrespiratory ordered phase encoding23 are moresuitable.
Irregular rhythms also degrade image qualitybecause the size and position of the heart may varywith each heart beat. Many patients with mitral valvedisease are in atrial fibrillation, but satisfactoryimages are still obtained (fig 1). Because there is lessvariation in end systolic size of the ventricles thesystolic images are better than diastolic. It is tech-nically possible to reject data from beats with lengthsoutside a predetermined range if the aquisition timeis extended. This is particularly helpful in patientswith extrasystoles or profound sinus arrhythmia, butwas not necessary in any of the patients in this study.Accuracy in outlining the endocardium is also
important and some experience is needed to achievereproducible results. Visual methods are adequatefor edge detection in these high resolution, high con-trast images, but automatic edge detection wouldspeed up the process. An automatic programmewould need to be complex, since it can often bedifficult to distinguish between signals from themyocardium and from static blood within the ven-tricle,24 particularly under the anterior cusp of thetricuspid valve. In addition, criteria must be definedfor the inclusion or exclusion of trabeculae andpapillary muscles. We excluded papillary musclesbut included small trabeculae in the cavity becausethe latter may not occupy the whole of a 10mm slice,and we found that exclusion gave low values for rightventricular stroke volume.4 Thinner slices are moreaccurate but they increase the acquisition time ordecrease the signal to noise ratio.An important limitation of the use of the stroke
volume ratio for the measurement of regurgitation isthat in the presence of multiple valve disease orshunting the ratio reflects the sum of all effects. Withequally severe mitral and tricuspid regurgitation for
instance the ratio will be 1. More accurate assess-ment of multiple lesions will be possible by magneticresonance flow imaging.25 26 A colour coded cinedisplay of blood velocity within the cardiac cham-bers and arteries may be superimposed upon theanatomical images,27 allowing an assessment ofregurgitation in the same way as two dimensionalDoppler flow imaging,28 although with greater ver-satility.Some patients with valvar heart disease may have
prosthetic valves but this is not a contraindication tomagnetic resonance imaging.29 Virtually all modernvalves are non-ferromagnetic and their workings arenot affected by either static or changing magneticfields. They may cause loss of magnetic resonancesignal and hence a "black hole" in the image, but thearea affected is small and does not prevent assess-ment of the rest of the heart.
ECHOCARDIOGRAPHYBoth M mode and cross-sectional echocardiographyare widely used in the assessment of patients withvalvar heart disease. The presence and type of dis-ease are seen and the severity of stenosis can beassessed. Valvar regurgitation is less easy to quan-tify, however, and reliance is usually placed on indi-rect observations such as relative chamber sizes anddiastolic fluttering of the mitral valve. Continuouswave and pulsed Doppler echocardiography are sen-sitive and specific in the detection of valvar regur-gitation, 3031 and they allow an assessment of theseverity of regurgitation in various ways.32 -34 Twodimensional Doppler flow imaging is also of poten-tial value, although it is not yet widely practised andits clinical role is still to be established.28 3538Although cross-sectional echocardiography was
performed on all the patients in this study, withDoppler velocity measurements in some, we did notcompare the magnetic resonance results with echo-cardiography because reliable quantitative informa-tion was not always achieved.
Conclusion
Magnetic resonance imaging allows an assessment ofcardiac anatomy and ventricular function in patientswith isolated aortic and mitral regurgitation. Itprovides an accurate measure of ventricular volume,ejection fraction, and the left to right ventricularstroke volume ratio, which can be used to quantifythe severity of regurgitation. Associated anatomicalfeatures may be seen, but details of valve disease arenot well shown. Although it is unlikely to displaceconventional methods of assessment in the shortterm, magnetic resonance imaging is a valuable addi-tion and serves as a suitable standard by which to
460
on 22 May 2018 by guest. P
rotected by copyright.http://heart.bm
j.com/
Br H
eart J: first published as 10.1136/hrt.56.5.455 on 1 Novem
ber 1986. Dow
nloaded from
Magnetic resonance assessment of aortic and mitral regurgitation 461judge their accuracy. Improved resolution, rapidimaging techniques, and flow imaging promise animportant role for magnetic resonance in the futureassessment of valvar heart disease.
We thank the following for financial support: TheBoard of Governors of the National Heart and ChestHospitals, the Coronary Artery Disease ResearchAssociation (CORDA), the League of Friends ofThe Brompton Hospital, the Viscount RoystonTrust, the Halley Stewart Trust, the CharlesWolfson Charitable Foundation, and PickerInternational.
References
1 Steiner RE, Bydder GM, Selwyn A, et al. Nuclear mag-netic resonance imaging of the heart: current statusand future prospects. Br Heart J 1983;5O:202-8.
2 Higgins CB, Byrd BF, McNamara MT, et al. Magneticresonance imaging of the heart: a review of the experi-ence in 172 subjects. Radiology 1985;155:671-9.
3 Higgins CB, Kaufman L, Crooks LE. Magnetic reso-nance of the cardiovascular system. Am Heart J1985;109:136-52.
4 Longmore DB, Klipstein RH, Underwood SR, etal.Dimensional accuracy of magnetic resonance in stud-ies of the heart. Lancet 1985;i:1360-2.
5 Underwood SR, Klipstein RH, Firmin DN, et al. Mag-netic resonance quantification of atrial shunting andvalvar regurgitation [Abstract]. Br Heart J 1985;54:616.
6 Pavel DG, Zimmer AM, Patterson VN. In vivo label-ling of red blood cells with 99m-Tc: a new approachto blood pool visualization. J Nucl Med 1977;18:305-8.
7 Geffers H, Adam WE, Bitter F, Siegel H, KampmannH. Data processing and functional imaging in radio-nuclide ventriculography. In: Brill AB, Pryce RR,eds. Information processing in medical imaging. Pro-ceedings of the 5th international conference. Nashville:Biomedical Computing Technology InformationCenter, 1977:322-32.
8 Mennel RG, Joyner CR Jr, Thompson PD, Pyle RR,MacVaugh H III. The preoperative and operativeassessment of aortic regurgitation. Am J Cardiol1972;29:360-6.
9 Hunt D, Baxley WA, Kennedy JW, Judge TP, Will-iams JE, Dodge HT. Quantitative evaluation of cineaortography in the assessment of aortic regurgitation.Am Jf Cardiol 1973;31:696-700.
10 Steiner RE, Jacobson G, Dinsmore R, Parizel G. Mitralregurgitation. Clin Radiol 1963;14: 113-25.
11 Rees RSO, Jefferson KE, Harris AM. Cine-angiocardiography of the mitral valve. Br Heart J1965;27:498-504.
12 Mackenzie JD, Haites NE, Rawles JM. Method ofassessing the reproducibility of blood flow mea-surement: factors influencing the performance ofthermodilution cardiac output computers. Br HeartJ
1986;55:14-24.13 Rigo P, Alderson PO, Robertson RM, Becker LC,
Wagner HN Jr. Measurement of aortic and mitralregurgitation by gated cardiac blood pool scans. Cir-culation 1979;60:306-12.
14 Alderson PO. Radionuclide quantification of valvularregurgitation. Jf Nucl Med 1982;23:851-5.
15 Hurwitz RA, Treves S, Freed M, Girod DA, CaldwellRL. Quantitation of aortic and mitral regurgitation inthe pediatric population: evaluation by radionuclideangiocardiography. Am J Cardiol 1983;51:252-5.
16 Parrish MD, Graham TP Jr, Born ML, et al. Radio-nuclide stroke count ratios for assessment of right and
- left ventricular volume overload in children. Am JCardiol 1983;51:261-4.
17 Kirch DL, Metz CE, Steele PP. Quantitation of valvu-lar insufficiency by computerised radionuclide angio-cardiography. Am J Cardiol 1974;34:711-21.
18 Walton S, Underwood SR, Ell PJ, et al. Measurementof valvular regurgitation by first pass radionuclideventriculography [Abstract]. Br Heart J 1984;52:91.
19 Nicod P, Corbett JR, Firth BG, et al. Radionuclidetechniques for valvular regurgitation index: com-parison in patients with normal and depressed ven-tricular function. J7 Nucl Med 1982;23:763-9.
20 Berthout P, Cardot JC, Baud M, et al. Factorsinfluencing the quantification of valvular regur-gitation by gated equilibrium radionuclide angio-graphy. Eur Jf Nucl Med 1984;9:112-4.
21 Schultz CL, Alfidi RJ, Nelson AD, Kopiwoda SY,Clampitt ME. The effect of motion on two-dimensional Fourier transformation on magnetic res-onance images. Radiology 1984;152:117-21.
22 Rzedzian R, Mansfield P, Doyle M, et al. Real-timenuclear magnetic resonance clinical imaging in pae-diatrics. Lancet 1983;ii: 1281-2.
23 Bailes DR, Gilderdale DJ, Bydder GM, Collins AG,Firmin DN. Respiratory ordered phase encoding(ROPE): a method for reducing respiratory motionartefacts in MR imaging. J Comput Assist Tomogr1985;9:835-8.
24 Von Schulthess GK, Fisher M, Crooks LE, HigginsCB. Gated MR imaging of the heart: intracardiacsignals in patients and healthy subjects. Radiology1985;156:125-32.
25 Nayler GL, Firmin DN, Longmore DB. Cine MRblood flow imaging. Jf Comput Assist Tomogr1986;10:715-22.
26 Underwood SR, Firmin DN, Klipstein RH, Rees RSO,Longmore DB. Magnetic resonance velocity map-ping: clinical application of a new technique[Abstract]. Proceedings of the Fifth Annual Meeting.Berkeley: Society of Magnetic Resonance in Medi-cine 1986;5:49-50.
27 Klipstein RH, Firmin DN, Underwood SR, et al. Mag-netic resonance anatomical and blood flow informa-tion displayed in a single colour coded cine image. BrJ Radiol 1986;59 (in press).
28 Omoto R, Yokote Y, Takamoto S, et al. The devel-opment of real-time two-dimensional Doppler echo-cardiography and its clinical significance in acquiredvalvular diseases: with special reference to the evalu-
on 22 May 2018 by guest. P
rotected by copyright.http://heart.bm
j.com/
Br H
eart J: first published as 10.1136/hrt.56.5.455 on 1 Novem
ber 1986. Dow
nloaded from

462 Underwood, Klipstein, Firmin, Fox, Poole- Wilson, Rees, Longmore
ation of valvular regurgitation. Jpn Heart J1984;25:325-40.
29 Soulen R, Higgins CB, Budinger TF. Magnetic reso-nance imaging of prosthetic heart valves. Radiology1985;154:705-7.
30 Come PC. The optimal Doppler examination: pulsed,continuous wave or both? J Am Coll Cardiol1986;7:886-8.
31 Wilde P, Pitcher D. Pulsed doppler echocardiographyin cardiac diagnosis. Y R Coll Physicians Lond1986;20:25-31.
32 Pons-Llado G, Carreras-Costa F, Ballester-Rodes M,Auge-Sampera JM, Crexells-Figueras C, Oriol-Palou A. Pulsed Doppler patterns of left atrial flow inmitral regurgitation. Am J Cardiol 1986;57:806-10.
33 Masuyama T, Kodama K, Kitabatake A, et al. Non-invasive evaluation of aortic regurgitation bycontinuous-wave Doppler echocardiography. Circu-lation 1986;73:460-6.
34 Zhang Y, Nitter-Hauge S, Ihlen H, Rootwelt K, Myhre
E. Measurement of aortic regurgitation by Dopplerechocardiography. Br Heart J 1986;55:32-8.
35 Miyatake K, Izumi S, Okamoto M, et al. Semi-quantitative grading of severity of mitral regur-gitation by real-time two-dimensional doppler flowimaging technique. J Am Coll Cardiol 1986;7:82-8.
36 Suzuki Y, Kambara H, Kadota K, et al. Detection andevaluation of tricuspid regurgitation using a real-time, two-dimensional, color-coded, Doppler flowimaging system: comparison with contrast two-dimensional echocardiography and right ventricu-lography. Am J Cardiol 1986;57:811-5.
37 Nakagawa H, Yamamoto K, Takamiya M, SakakibaraH, Nimura Y. Semiquantitative grading of severity ofmitral regurgitation by real-time two-dimensionaldoppler flow imaging technique. J Am Coll Cardiol1986;7:82-8.
38 Goldman ME. Real-time two-dimensional doppler flowimaging: a word of caution. J Am Coll Cardiol1986;7:89-90.
on 22 May 2018 by guest. P
rotected by copyright.http://heart.bm
j.com/
Br H
eart J: first published as 10.1136/hrt.56.5.455 on 1 Novem
ber 1986. Dow
nloaded from





























