Embed Size (px)
Citation preview
pharmacoepidemiology and drug safety 2009; 18: 235–239w.interscience.wiley.com) DOI: 10.1002/pds.1707
Published online 14 January 2009 in Wiley InterScience (wwORIGINAL REPORT
Magnitude of QT prolongation associated with a higher riskof Torsades de Pointesy
Yeong-Liang Lin MD* and Mei-Fen Kung PhD
Center for Drug Evaluation, Taiwan
SUMMARY
Purpose Drug induced Torsades de Pointes (TdP) is a major concern for new drugs seeking regulatory approval. Prolongation of QTintervals greater than 60millisecond or to longer than 500millisecond in an individual patient has been considered to be associated with ahigher risk. The purpose of this study is to identify values inferred from a population that predict a stronger potential for TdP.Methods Prolongation data of 30 non-antiarrhythmic QT prolonging drugs were analysed. Depending on how strong the drugs wereassociated with TdP, they were categorized as strong or borderline torsadogens. The differences in mean QTc increases between the twogroups were compared and cut-off values that distinguished strong from borderline drugs were searched for.Results The average QTc increase of 19.3millisecond of strong torsadogens was significantly greater than the 8.0millisecond of borderlinetorsadogens. Prolongation greater than 12millisecond in the context of monotherapy or 25millisecond in the presence of metabolic inhibitionand an upper bound of 95% confidence interval (CI) for the mean QTc increase greater than 14millisecond in monotherapy or30.1millisecond in combination therapy with metabolic inhibitors favoured a stronger association with TdP.Conclusions Drugs strongly associated with TdP have greater QTc increases than those with less concern. Several cut-off values havebeen noted to distinguish between them. These values may be helpful for evaluation of TdP risk for future QT prolonging drugs.Copyright # 2009 John Wiley & Sons, Ltd.
key words—QT prolongation; Torsades de Pointes; cut-off value
Received 11 September 2008; Revised 8 December 2008; Accepted 8 December 2008
INTRODUCTION
Drug-induced QT prolongation and Torsades dePointes (TdP) are major concerns facing the develop-ment, approval and clinical use of new drugs. Toaddress these concerns, several guidelines have beendeveloped, which provide recommendations for thedesign, conduct, analysis and interpretation of clinicaland non-clinical studies that assess the potential ofdelayed ventricular repolarization.1–4
In assessing prolongation data, the guideline statesthat the threshold level of regulatory concern is around5millisecond, as evidenced by an upper bound of the95% confidence interval (CI) around the mean effect on
*Correspondence to: Y.-L. Lin, Center for Drug Evaluation 1F, No 15-1,Section 1, Hangjou S Road, Taipei 100, Taiwan. E-mail: [email protected] declare that we have no conflict of interest.
Copyright # 2009 John Wiley & Sons, Ltd.
QTc of 10millisecond in healthy volunteers.3 If thestudy result is positive, i.e. the upper bound of the95%CI includes 10millisecond, further evaluation inthe target patient population with particular attention todose and concentration effects should be performed.3
Although an increase below than 10millisecond isconsidered relative safe, small increases can stillsometimes lead to TdP in circumstances where theconcerning drug is a potent Ikr blocker or the drug isgiven to patients with reduced repolarization reserve.5,6
Consequently, it is difficult to define a value that is sosmall as to be of no consequence.3
In this study, we examined whether cut-off values ofQT prolongation can be identified that distinguisheddrugs strongly associated with TdP from those withless concern. To achieve the goal, we compared thedifference in the values of QT prolongation and usedthe receiver operating characteristic (ROC) analysis to

236 y.-l. lin and m.-f. kung
identify threshold values that distinguished betweenthe two groups. We hypothesized that drugs withstronger TdP concern would have larger values and,despite some overlapping between the two groups,there would be cut-off values abovewhich a higher riskof TdP would be expected.
METHODS
To collect non-antiarrhythmic QT prolonging drugseligible for this study, we systemically searched thepublished literature and the drug approval packages onthe regulatory websites, including the US Food andDrug Administration and EuropeanMedicines Agency,for drugs that had warning of QT prolongation in druglabels, had adequate drug-induced QT prolongationdata available for analysis and were well recognized tohave this cardiotoxic property in the literature.7,8 Afterthe list was compiled, we divided the drugs into twogroups based on the following criteria. If the evidenceof association with TdP was strong and overwhelming,e.g. the drugs had been withdrawn from the marketbecause of this side effect, or there had been warningsof TdP in drug labels and vivid discussions in theliterature that they caused TdP, they were categorizedas strong torsadogens. In contrast, if the drugs had hadonly rare, limited case reports of this side effect, theywere categorized as borderline torsadogens.Next, we reviewed the data on QT prolongation and
extracted the values reported in the literature, i.e. meanchanges from baseline QTc and their 95%CI, in thecontext of monotherapy as well as in the presence ofmetabolic inhibition. If CI was not available in thereference literature, we constructed it based on thereported sample size and standard deviation or standarderror (SE), using the formula 95%CI¼Mean� tdf, 0.05�SE, where df represented degrees of freedom. If morethan one study reported prolongation data of the samedrug, we used those generated in a clinical pharma-cology study, which, in contrast to a clinical efficacystudy, accounted for drug exposure levels.Finally, we compared the mean QTc increases and
upper bounds of 95%CI between the two groups. Thevalues were averaged for each group and thesignificance of the difference was evaluated by a t-test. We constructed the ROC plot to identify cut-offvalues that distinguished strong from borderlinetorsadogens.9
RESULTS
A total of 30 non-antiarrhythmic drugs, including13 strong torsadogens and 17 borderline torsadogens,
Copyright # 2009 John Wiley & Sons, Ltd.
were identified. Table 1 summarized their prolongationdata.10–34 The strong torsadogenic group was comprisedof drugs that had beenwell recognized in the literature tocause TdP, e.g. terfenadine, thioridazine and astemizole,or drugs that had been withdrawn from the marketbecause of an association with TdP, e.g. cisapride andsparfloxacin. The borderline torsadogenic group con-sisted of drugs that had limited case reports of anassociation with TdP, e.g. erythromycin and clarithro-mycin, drugs that were frequently used as control drugsin QT studies, e.g. moxifloxacin, or drugs that under-went several QT studies and were eventually determinedto have minimal TdP concern, e.g. ziprasidone.As noted in Table 1, most prolongation data were
obtained from patients in clinical pharmacologystudies. The mean changes from baseline QTc ofstrong torsadogens were greater than those of border-line torsadogens. Their averages were 19.3millisecond(ranging from�16.0 to 46.6millisecond) and 8.0milli-second (ranging from �2.3 to 20.0millisecond),respectively (p¼ 0.013). The upper bounds of95%CI of strong torsadogens also seemed greaterthan those of borderline torsadogens. Their averageswere 32.9millisecond (range 14.0–57.4millisecond)and 13.8millisecond (range 1.7–36.1millisecond),respectively. Of note, 11 of 13 upper bounds of strongtorsadogens were greater than 20millisecond, incontrast to 5 of 17 of borderline torsadogens. Usingthe ROC analysis, we identified two cut-off values. Formean changes, an increase of 12millisecond differ-entiated strong torsadogens from borderline torsado-gens with a sensitivity of 85% and specificity of 71%.For the upper bound, an increase of 14milliseconddistinguished with a sensitivity of 100% and specificityof 67%.Table 2 summarized the changes of QT intervals in
the presence of metabolic inhibition.10,14,18,22,26
Because of study complexity, only 10 drugs had thedata. As noted, the mean changes from baseline QTc ofstrong torsadogens were greater than those of border-line torsadogens. Their averages were 35.9millisecond(range 12.0–82.0millisecond) and 8.7millisecond(range 2.4–16.5millisecond), respectively (p¼0.058). The upper bounds of 95%CI of strongtorsadogens were also larger than those of borderlinetorsadogens. Their averages were 46.7millisecond(range 30.1–97.1millisecond) and 14.7millisecond(range 8.3–19.4millisecond), respectively. Based onthe ROC analysis, we noted that a mean increase of25.0millisecond differentiated strong from borderlinetorsadogens with 80% sensitivity and 100% specificityand an upper bound of 30.1millisecond distinguishedwith 100% sensitivity and 100% specificity.
Pharmacoepidemiology and Drug Safety, 2009; 18: 235–239DOI: 10.1002/pds
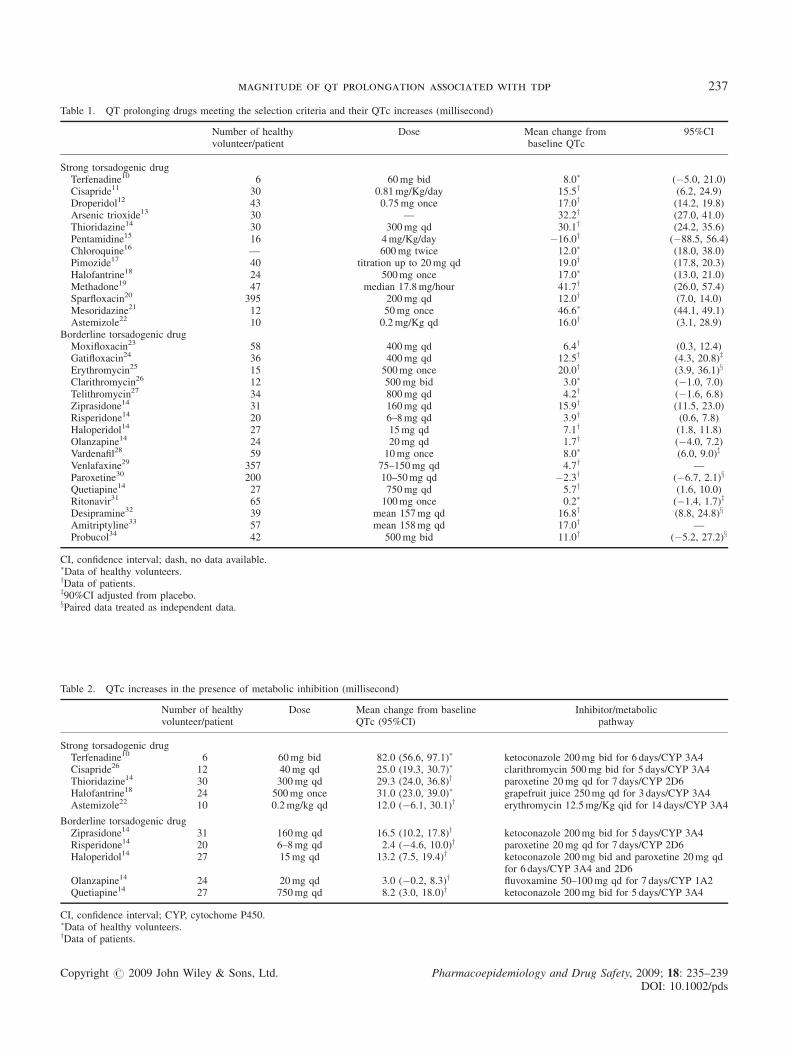
Table 1. QT prolonging drugs meeting the selection criteria and their QTc increases (millisecond)
Number of healthyvolunteer/patient
Dose Mean change frombaseline QTc
95%CI
Strong torsadogenic drugTerfenadine10 6 60mg bid 8.0� (�5.0, 21.0)Cisapride11 30 0.81mg/Kg/day 15.5y (6.2, 24.9)Droperidol12 43 0.75mg once 17.0y (14.2, 19.8)Arsenic trioxide13 30 — 32.2y (27.0, 41.0)Thioridazine14 30 300mg qd 30.1y (24.2, 35.6)Pentamidine15 16 4mg/Kg/day �16.0y (�88.5, 56.4)Chloroquine16 — 600mg twice 12.0� (18.0, 38.0)Pimozide17 40 titration up to 20mg qd 19.0y (17.8, 20.3)Halofantrine18 24 500mg once 17.0� (13.0, 21.0)Methadone19 47 median 17.8mg/hour 41.7y (26.0, 57.4)Sparfloxacin20 395 200mg qd 12.0y (7.0, 14.0)Mesoridazine21 12 50mg once 46.6� (44.1, 49.1)Astemizole22 10 0.2mg/Kg qd 16.0y (3.1, 28.9)
Borderline torsadogenic drugMoxifloxacin23 58 400mg qd 6.4y (0.3, 12.4)Gatifloxacin24 36 400mg qd 12.5y (4.3, 20.8)z
Erythromycin25 15 500mg once 20.0y (3.9, 36.1)x
Clarithromycin26 12 500mg bid 3.0� (�1.0, 7.0)Telithromycin27 34 800mg qd 4.2y (�1.6, 6.8)Ziprasidone14 31 160mg qd 15.9y (11.5, 23.0)Risperidone14 20 6–8mg qd 3.9y (0.6, 7.8)Haloperidol14 27 15mg qd 7.1y (1.8, 11.8)Olanzapine14 24 20mg qd 1.7y (�4.0, 7.2)Vardenafil28 59 10mg once 8.0� (6.0, 9.0)z
Venlafaxine29 357 75–150mg qd 4.7y —Paroxetine30 200 10–50mg qd �2.3y (�6.7, 2.1)x
Quetiapine14 27 750mg qd 5.7y (1.6, 10.0)Ritonavir31 65 100mg once 0.2� (�1.4, 1.7)z
Desipramine32 39 mean 157mg qd 16.8y (8.8, 24.8)x
Amitriptyline33 57 mean 158mg qd 17.0y —Probucol34 42 500mg bid 11.0y (�5.2, 27.2)x
CI, confidence interval; dash, no data available.�Data of healthy volunteers.yData of patients.z90%CI adjusted from placebo.xPaired data treated as independent data.
Table 2. QTc increases in the presence of metabolic inhibition (millisecond)
Number of healthyvolunteer/patient
Dose Mean change from baselineQTc (95%CI)
Inhibitor/metabolicpathway
Strong torsadogenic drugTerfenadine10 6 60mg bid 82.0 (56.6, 97.1)� ketoconazole 200mg bid for 6 days/CYP 3A4Cisapride26 12 40mg qd 25.0 (19.3, 30.7)� clarithromycin 500mg bid for 5 days/CYP 3A4Thioridazine14 30 300mg qd 29.3 (24.0, 36.8)y paroxetine 20mg qd for 7 days/CYP 2D6Halofantrine18 24 500mg once 31.0 (23.0, 39.0)� grapefruit juice 250mg qd for 3 days/CYP 3A4Astemizole22 10 0.2mg/kg qd 12.0 (�6.1, 30.1)y erythromycin 12.5mg/Kg qid for 14 days/CYP 3A4
Borderline torsadogenic drugZiprasidone14 31 160mg qd 16.5 (10.2, 17.8)y ketoconazole 200mg bid for 5 days/CYP 3A4Risperidone14 20 6–8mg qd 2.4 (�4.6, 10.0)y paroxetine 20mg qd for 7 days/CYP 2D6Haloperidol14 27 15mg qd 13.2 (7.5, 19.4)y ketoconazole 200mg bid and paroxetine 20mg qd
for 6 days/CYP 3A4 and 2D6Olanzapine14 24 20mg qd 3.0 (�0.2, 8.3)y fluvoxamine 50–100mg qd for 7 days/CYP 1A2Quetiapine14 27 750mg qd 8.2 (3.0, 18.0)y ketoconazole 200mg bid for 5 days/CYP 3A4
CI, confidence interval; CYP, cytochome P450.�Data of healthy volunteers.yData of patients.
Copyright # 2009 John Wiley & Sons, Ltd. Pharmacoepidemiology and Drug Safety, 2009; 18: 235–239DOI: 10.1002/pds
magnitude of qt prolongation associated with tdp 237

238 y.-l. lin and m.-f. kung
DISCUSSION
QTc duration has been recognized as a usefulparameter for evaluating the risk of drug-inducedventricular arrhythmia. Its upper limit of normal is450millisecond for males and 460millisecond forfemales. Previous studies have found that prolongationof QTc intervals greater than 60millisecond or tolonger than 500millisecond in an individual patientpredicts a higher risk of TdP, in randomized controlledtrials, an increase larger than 10% baseline QT durationsuggests the need for further study, and a peak placebo-corrected increase in QTc interval greater than26millisecond definitely predicts the risk.35–38
In this study, 30 drugs were collected, exclusive ofseveral other well-recognized QT prolonging drugs,e.g. chlorpromazine, sertindole, doxepin, indinavir,sertraline, tacrolimus and ciprofloxacin, because ofinadequate data available for analysis. To correctlycategorize the selected drugs and therefore minimizethe risk of misclassification, which would be the keystep for obtaining valid results, we sought to employobjective criteria for defining strong torsadogens.Accordingly, drug withdrawal from the market becauseof TdP concern and warning of an association with TdPin a drug label were used which should bring aboutminimal ambiguity.The results showed that there was a significant
difference in the values of mean QTc changes betweenthe two groups. Because there was a significantoverlapping of mean QTc changes between the twogroups in monotherapy, the sensitivity and specificityobtained from the 12-millisecond cut-off value weremediocre. However, in the presence of metabolicinhibition, the 25-millisecond cut-off value almostperfectly discriminated between the two groups.Consequently, prolongation data derived from combi-nation therapy with metabolic inhibitors are moreutilizable for distinguishing strong from borderlinetorsadogens.Furthermore, the study showed a mean QTc change
of 19.3millisecond for strong torsadogens and8.0millisecond for borderline torsadogens as well asa cut-off value of 12millisecond that distinguishedbetween the two groups of QT prolonging drugs. Thefindings were consistent with previously reportedprognostic values, 6–10, 11–15 and 16–20millisecond,which predicted an unlikely, possible and probablerisk, respectively.38
As we know, QT prolongation enhanced bymetabolic inhibition is determined by the inhibitors’potency, which is defined by factors including theinhibitors’ bioavailability, mechanism of inhibition and
Copyright # 2009 John Wiley & Sons, Ltd.
the administered dose. Among the 10 drugs that hadprolongation data with metabolic inhibition, themajority were metabolized primarily by cytochromeP450 3A4 and 2D6. The inhibitors used wereketoconazole and paroxetine, respectively, in standarddoses. An exception was astemizole, which usederythromycin for inhibition. There were several factorsthat explained why astemizole had a relatively smallQTc increase, including the less inhibitory potency oferythromycin.39
As for upper bounds of 95%CI for mean QTcincreases, strong torsadogens also had greater valuesthan borderline torsadogens. In addition, a valuegreater than 14millisecond in monotherapy or30.1millisecond in the presence of metabolic inhi-bition was found to distinguish strong from borderlinetorsadogens, which supports the rule stated in theguideline that an upper bound larger than 10milli-second in healthy volunteers suggests the need forfurther study in patients.3 The study results providemore precise values needed for such studies in patients.The study has several limitations. First, the number
of eligible drugs is limited, especially that usingmetabolic inhibitors. It makes inferences based onstatistics difficult. Second, the prolongation data aregenerated in different population, which makes head-to-head comparison difficult. Third, many unknownpharmacological factors including electrophysiologi-cal activities at the molecular level significantlyinfluence the potential of QT prolongation andtherefore the ultimate risk of TdP, for example, theancillary pharmacologic characteristics that modulatethe risk of TdP including adenoreceptors or calciumchannel-blocking properties, down regulation ofpotassium channels in cardiac failure or increasedsusceptibility in autonomic neuropathy.6 Fourth, someof the sensitivity and specificity data generated by thecut-off values are not high enough, meaning thatoptimal cut-off values have not been identified yet. Inaddition, the scientific merit of the study relies verymuch on correct categorization of eligible drugs.Although objective criteria are used to minimizemisclassification, there is no assurance that no drug isincorrectly categorized. After all, actions to withdraw adrug from the market or to issue a warning in a druglabel are sometimes taken before a causal relationshipis established.
CONCLUSION
This study demonstrates that drugs strongly associatedwith TdP have greater QTc increases than those withless TdP concern. Mean QT prolongation greater than
Pharmacoepidemiology and Drug Safety, 2009; 18: 235–239DOI: 10.1002/pds
magnitude of qt prolongation associated with tdp 239
12millisecond in the context of monotherapy or25millisecond in the presence of metabolic inhibitionand an upper bound of 95%CI for the mean QTcincrease greater than 14millisecond in monotherapy or30.1millisecond in combination therapy with meta-bolic inhibitors favour a stronger association with TdP.These values could be used as a helpful guide to predicta higher risk of TdP (for future QT prolonging drugs).
REFERENCES
1. Haverkamp W, Breithardt G, Camm AJ, et al. The potential for QTprolongation and proarrhythmia by non-arrhythmic drugs: clinical andregulatory implications: report on a policy conference of the EuropeanSociety of Cardiology. Eur Heart J 2000; 21: 1216–1231.
2. AndersonME, Al Khatib SM, Roden DM, et al. Cardiac repolarization:current knowledge, critical gaps and new approaches to drug devel-opment and patient management. Am Heart J 2002; 144: 769–781.
3. International Conference on Harmonisation of Technical Requirementsfor Registration of Pharmaceuticals for Human Use. ICH HarmonisedTripartite Guideline: The Clinical Evaluation of QT/QTc IntervalProlongation and Proarrhythmic Potential for Non-antiarrhythmicDrugs. Geneva, Switzerland: International Conference on Harmonisa-tion, 2005.
4. International Conference of Harmonisation of Technical Requirementsfor Registration of Pharmaceuticals for Human Use. ICH HarmonisedTripartite Guideline: The Nonclinical Evaluation of the Potential forDelayed Ventricular Repolarization (QT Interval Prolongation) byHuman Pharmaceuticals. Geneva, Switzerland: International Confer-ence on Harmonisation, 2005.
5. Roden DM. Drug-induced prolongation of the QT interval. N Eng JMed 2004; 350: 1013–1022.
6. Lin YL, Chan K. Pharmacokinetic and pharmacodynamic character-ization of Non-antiarrhythmic QT-prolonging drugs associated withTorsades de Pointes. Drug Inf J 2008; 42: 211–219.
7. FDA. Drugs@FDA. FDA CDER, Rockville. http://www.accessdata.f-da.gov/scripts/cder/drugsatfda [accessed 28 August 2008].
8. European Medicines Agency. Authorized medicinal products forhuman use. http://www.emea.europa.eu/htms/human/epar/eparin-tro.htm [accessed 28 August 2008].
9. Zweig MH, Campbell G. Receiver operating characteristic (ROC)plots: a fundamental evaluation tool in clinical medicine. Clin Chem1993; 39: 561–577.
10. Honig PK, Wortham DC, Zamani K, et al. Terfenadine-ketoconazoleinteraction. Pharmacokinetic and electrocardiographic consequences.JAMA 1993; 269: 1513–1518.
11. Khongphatthanayothin A, Lane J, Thomas D, et al. Effects of cisaprideon QT interval in children. J Pediatr 1998(133): 51–56.
12. Charbit B, Albaladejo P, Funck-Brentano C, et al. Prolongation of QTcinterval after postoperative nausea and vomiting treatment by droper-idol or ondansetron. Anesthesiology 2005; 102: 1094–1100.
13. Zhou J, Meng R, Li X, et al. The effect of arsenic trioxide on QTinterval prolongation during APL therapy. Chin Med J 2003; 116:1764–1766.
14. Harrigan EP, Miceli JJ, Anziano R, et al. A randomized evaluation ofthe effects of six antipsychotic agents on QTc, in the absence andpresence of metabolic inhibition. J Clin Psychopharmacol 2004; 24:62–69.
15. Girgis I, Gualberti J, Langan L, et al. A prospective study of the effectof iv pentamidine therapy on ventricular arrhythmias and QTc pro-longation in HIV-infected patients. Chest 1997; 112: 646–652.
16. Mzayek F, Deng H, Mather FJ, et al. Randomized dose-rangingcontrolled trial of AQ-13, a candidate antimalarial and chloroquinein healthy volunteers. PLoS Clin Trials 2007; 2: e6.
Copyright # 2009 John Wiley & Sons, Ltd.
17. Fulop G, Phillips RA, Shapiro AK, et al. ECG changes during halo-peridol and pimozide treatment of Tourette’s disorder. Am J Psychiatry1987; 144: 673–675.
18. Charbit B, Becquemont L, Lepere B, et al. Pharmacokinetic andpharmacodynamic interaction between grapefruit juice and halofan-trine. Clin Pharmacol Ther 2002; 72: 514–523.
19. Kornick CA, Kilborn MJ, Santiago-Palma J, et al. QTc intervalprolongation associated with intravenous methadone. Pain 2003;105: 499–506.
20. DeAbate CA, Henry D, Bensch G, et al. Sparfloxacin vs ofloxacin in thetreatment of acute bacterial exacerbations of chronic bronchitis. Amulticenter, double-blind, randomized, comparative study. Chest 1998;114: 120–130.
21. Salih ISM, Thanacoody RHK, McKay GA, et al. Comparison of theeffects of thioridazine and mesoridazine on the QT interval in healthyadults after single oral doses. Clin Pharmacol Ther 2007; 82: 549–554.
22. Delgado LF, Pferferman A, Sole D, et al. Evaluation of the potentialcardiotoxicity of the antihistamines terfenadine, astemizole, loratadineand cetirizine in atopic children. Ann Allergy Asthma Immunol 1998;80: 333–337.
23. Morganroth J, DiMarco JP, Anzueto A, et al. A randomized trialcomparing the cardiac rhythm safety of moxifloxacin vs levofloxacinin elderly patients hospitalized with community acquired pneumonia.Chest 2005; 128: 3398–3406.
24. FDA. Review of Tequin. FDA CDER, Rockville; 2002. http://www.fda.gov/cder/foi/nda/2002/021061s010_s016_Tequin_MedR.pdf[accessed 28 August 2008].
25. Mishra A, Friedman HS, Sinha AK. The effects of erythromycin on theelectrocardiogram. Chest 1999; 115: 983–986.
26. van Haarst AD, van’t Klooster GA, van Gerven JM, et al. The influenceof cisapride and clarithromycin on QT intervals in healthy volunteers.Clin Pharmacol Ther 1998; 64: 542–546.
27. Demolis JL, Vacheron F, Cardus S, et al. Effect of single and repeatedoral doses of telithromycin on cardiac QT interval in healthy subjects.Clin Pharmacol Ther 2003; 73: 242–252.
28. Levitra. Physician’s Desk Reference, (61th edn), Thomson PDR:Montvale, NJ, 2007; 3034–3038.
29. Effexor. Physician’s Desk Reference, (61th edn), Thomson PDR:Montvale, NJ, 2007; 3411–3417.
30. Krulewicz S, Carpenter D, Fong R, et al. Analysis of electrocardio-graphic data following use of paroxetine in pediatric depression andobsessive-compulsive disorder. J Am Acad Child Adolesc Psychiatry2006; 45: 422–430.
31. Sarapa N, Nickens DJ, Raber SR, et al. Ritonavir 100mg does not causeQTc prolongation in healthy subjects: a possible role as CYP 3Ainhibitor in thorough QTc studies. Clin Pharmacol Ther 2008; 83:152–159.
32. Leonard HL, Meyer MC, Swedo SE, et al. Electrocardiographicchanges during desipramine and clomipramine treatment in childrenand adolescents. J Am Acad Child Adolesc Psychiatry 1995; 34: 1460–1468.
33. Claghorn JL, Schroeder J, Goldstein BJ, et al. Comparison of theelectrocardiographic effect of dothiepin and amitriptyline. J Clin Psy-chiatry 1984; 45: 291–293.
34. Dujovne CA, Atkins F, Wong B, et al. Electrocardiographic effects ofprobucol. A controlled prospective clinical trial. Eur J Clin Pharmacol1984; 26: 735–739.
35. Haddad PM, Anderson IM. Antipsychotic-related QTc prolongation,torsade de pointes and sudden death. Drugs 2002; 62: 1649–1671.
36. Moss AJ. Measurement of the QT interval and the risk associated withQTc interval prolongation: a review. Am J Cardiol 1993; 72: 23B–25B.
37. Welch R, Chue P. Antipsychotic agents and QT changes. J PsychiatryNeurosci 2000; 25: 154–160.
38. Shah RR. The significance of QT interval in drug development. Br JClin Pharmacol 2002; 54: 188–202.
39. Dana G, Descatoire V, Pessayre D. Self-induction by erythromycin ofits own biotransformation into a metabolite forming an inactive com-plex with reduced cytochrome P450. J Pharmacol Exp Ther 1981; 218:509–515.
Pharmacoepidemiology and Drug Safety, 2009; 18: 235–239DOI: 10.1002/pds