Embed Size (px)
Citation preview

Magnitude of Stromal Hemangiogenesis Correlates with HistologicSubtype of Non^Hodgkin’s LymphomaJia Ruan,1,2 Elizabeth Hyjek,3 Pouneh Kermani,2 PaulJ. Christos,4 Andrea T. Hooper,5 Morton Coleman,1,2
Barbara Hempstead,2 John P. Leonard,1,2 Amy Chadburn,3 and Shahin Rafii5,6
Abstract Purpose: Tumor stromal microenvironment promotes neoplastic growth and angiogenesis.We have previously shown that recruitment of marrow-derived vascular endothelial growth factorreceptor-1+ (VEGFR-1+) proangiogenic hematopoietic progenitors contributes instructivelyand structurally to neoangiogenesis in mouse models. Here, we investigated whether stromalincorporation of CD68+ hemangiogenic cells and a-smooth muscle actin+ (a-SMA+) stromal cellscorrelates withneoangiogenesis andprogression inhumannon ^Hodgkin’s lymphoma subtypes.Experimental Design: Spatial localizations of vascular and stromal cells expressing CD34,VEGFR-1, a-SMA, and CD68 were examined by immunohistochemistry in 42 cases of non ^Hodgkin’s lymphoma, including diffuse large B-cell lymphoma, Burkitt lymphoma, follicularlymphoma, and chronic lymphocytic leukemia/small lymphocytic lymphoma (CLL/SLL), andcompared with benign follicular hyperplasia.Results: Compared with indolent lymphomas, there was a profound increase in recruitment ofCD68+ cells andVEGFR-1+ neovessels in aggressive subtypes (including those transformed fromindolent subtypes), where CD68+ cells were localized to the perivascular region of neovessels aswell as the stromal compartment.The perivascular CD68+ cells expressedVEGFR-1andVEGF-A.In contrast, therewas a diffuse increase in a-SMA incorporation throughout the stromal compart-ment of indolent subtype of CLL/SLL comparedwith the scant perivascular pattern in aggressivesubtypes. Overall, there was no correlation between CD34+ microvessel density and lymphomahistologic subtype.Conclusions: Heightened stromal hemangiogenesis as marked by infiltration of proangiogenicVEGFR-1+CD68+VEGF-A+ cells and their paracrine cross-talk with neovasculature appears to bea distinct feature of aggressive lymphoma, providing novel targets for antiangiogenic therapy,whereas a-SMA+ stromal vascular network may be differentially targeted in CLL/SLL.
Despite the fact that multimodality treatment, includingcombination chemotherapy, radiation, and target-specificmonoclonal antibodies, such as rituximab, can induce highrate of remission in many subtypes of non–Hodgkin’slymphoma (NHL), significant proportions of patients relapsewith incurable disease (1, 2). Several clinical and diagnosticvariables have been developed to improve the prognosticstratification of clinical outcome, including the internationalprognostic index (IPI; ref. 3), tumor-specific markers, such asBCL-2 (4), BCL-6 (5), and p53 (6), and gene expressionprofiling signatures (7–9). However, very few studies haveaddressed the contribution of the stromal and vascular
microenvironment to the pathogenesis and clinical behaviorof lymphoma.Neoangiogenesis is essential for tumor growth and progres-
sion (10–12). Blockade in angiogenesis can lead to tumorregression in solid tumor models (13, 14). Targeting vascularendothelial growth factor (VEGF)-A with bevacizumab incombination with chemotherapy promotes progression-freesurvival in human patients with metastatic colorectal cancer,advanced stage non–small cell lung cancer, as well as breastcancer (15–17). Surprisingly, very few studies have addressedthe role of angiogenesis in the growth of human lymphomas,although several reports have implicated up-regulation of
Human Cancer Biology
Authors’ Affiliations: 1Center for Lymphoma and Myeloma, 2Division ofHematology-Oncology, Department of Medicine, 3Department of Pathology,4Division of Biostatistics and Epidemiology, Department of Public Health,5Department of Genetic Medicine, and 6Howard Hughes Medical Institute,WeillMedical College of Cornell University, New York, New YorkReceived 5/19/06; revised 7/7/06; accepted 7/17/06.Grant support: NIH grants HL075234, HL67839, and HL 59312 (S. Rafii),HL67839 (Histotechnology core; B. Hempstead), and K23RR016814 (J.P.Leonard); Leukemia and Lymphoma Society (S. Rafii); Lymphoma ResearchFoundation grant (J.P. Leonard and S. Rafii); and American Society of ClinicalOncology Young Investigator Award (J. Ruan). S. Rafii is an investigator of theHoward Hughes Medical Institute.
The costs of publication of this article were defrayed in part by the payment of pagecharges.This article must therefore be hereby marked advertisement in accordancewith18 U.S.C. Section1734 solely to indicate this fact.Requests for reprints: Shahin Rafii, Howard Hughes Medical Institute,Department of Genetic Medicine,Weill Medical College of Cornell University, 1300York Avenue, RoomA-863, New York, NY10021. Phone: 212-746-2070; Fax: 212-746-8481; E-mail: [email protected] and Jia Ruan, Division of Hematology-Oncology, Department of Medicine,Weill Medical College of Cornell University,520 East 70th Street, Starr 341, New York, NY10021. Phone: 212-746-2932; Fax:212-746-3844; E-mail: [email protected].
F2006 American Association for Cancer Research.doi:10.1158/1078-0432.CCR-06-1204
www.aacrjournals.orgClin Cancer Res 2006;12(19) October1, 2006 5622
Cancer Research. on September 21, 2020. © 2006 American Association forclincancerres.aacrjournals.org Downloaded from

VEGF-A and VEGF receptors (VEGFR) in mediating lymphoma-genesis (18–20).In search of the cellular and molecular mechanisms involved
in the assembly of tumor neovessels, our group and othershave shown that recruitment of marrow-derived VEGFR-1+
proangiogenic hematopoietic progenitors to the vascular micro-environment contributes instructively and structurally to neo-angiogenesis in mouse lymphoma models (21–23). Otherstudies have also set forth the concept that hematopoieticprogenitors and differentiated myeloid cells, including maturemonocytes/macrophages, can home to tumor tissue andpromote angiogenesis of the growing tumor via possibly twomechanisms. One is through the production of proangiogenicgrowth factors, such as VEGF-A, VEGF-C/VEGF-D, brain-derivedneurotrophic factor, and platelet-derived growth factor, as wellas matrix metalloproteinases, such as matrix metalloproteinase-9, to support endothelial proliferation and stromal remodeling
(24–26). Secondly, monocytes/macrophages seem to becapable of coexpressing vascular markers both in vitro andin vivo (27, 28), raising the possibility of direct participationin neoangiogenesis and vasculogenesis (29). In humansubjects, tumor-associated macrophages have been implicatedin aggressive disease and inferior outcome in several tumors,including breast, prostate, ovarian, cervical cancers andfollicular lymphoma (FL; ref. 30, 31). However, the contribu-tion of hemangiogenic progenitors to lymphoma angiogenesisin human subjects has not been studied.Other stromal components can be activated during tumor-
igenesis and express myofibroblastic markers, including a-smooth muscle actin (a-SMA; ref. 32). In breast epithelialcarcinoma model, carcinoma-associated a-SMA+ fibroblastshave been shown to promote tumor angiogenesis and growthvia recruitment of endothelial progenitors from the bonemarrow (33). Pericytes/smooth muscle cells have also beensuggested to play a role in regulation of endothelial survivaland vessel stability (34). However, it remains unclear whetherthe degree of the a-SMA+ stromal cell incorporation contributesto neovessel formation in human lymphoma as well.Based on these studies, we hypothesized that the magnitude
of recruitment of marrow-derived VEGFR-1+ hematopoieticprecursors and incorporation of proangiogenic CD68+ myelo-monocytic cells expressing VEGF-A may correlate with histo-logic subtypes of human lymphoma. Additionally, stromalproduction of the a-SMA may also define angiogenic propertiesof the respective subtypes. To test these hypotheses, wecharacterized the spatial localization of vascular and stromalcells on different subtypes of human NHL samples frompatients with previously untreated diseases and compared themwith benign follicular hyperplasia (FH).
Materials and Methods
Lymphoma specimens. Clinical diagnostic grade frozen and paraffinsections (5-Am thick) of untreated human NHL tissue specimens wereobtained from the pathology department at Weill Cornell MedicalCollege (New York, NY) according to Institutional Review Board–approved protocols and Health Insurance Portability and Accountabil-ity Act regulations. The specimens used in this study included theindolent subtypes of FL (n = 7) and chronic lymphocytic leukemia/small lymphocytic lymphoma (CLL/SLL; n = 5), and aggressive lym-phomas, including diffuse large B-cell lymphoma (DLBCL; n = 28) andBurkitt lymphoma (BL; n = 2). Tonsil and FH (n = 5) were used ascontrols. Clinical information was obtained for prognosis and survivalcorrelations.
Immunohistochemistry. Paraffin tissue sections were stained with
the following antibodies: anti-CD34 (QBEnd10, DAKO, Carpinteria,
CA), CD68 (KP1 and PGM1, DAKO), a-SMA (1A4, Sigma, St. Louis,MO), BCL-6 (PG-B6, DAKO), MUM1 protein (MUM1p, DAKO), CD10
(56C6, Novocastra Laboratories, Newcastle upon Tyne, United
Kingdom), CD138 (BB4, Serotec, Raleigh, NC), podoplanin (AngioBio
Co., DelMar, CA), and VEGF-A (VG1 and Z-CVF3, Zymed, Carlsbad,
CA). Frozen tissue sections were stained with anti-CD68 (KP1), CD34
(QBEnd10), VEGFR-1 (FB5, ImClone, New York, NY), VEGFR-2 (1121,
ImClone), and VEGF-A (VG1 and Z-CVF3). Double staining was done
on paraffin and frozen tissue sections with the following antibodies:
a-SMA/CD34, CD34/CD68, VEGFR-1/CD68 (frozen section only),
VEGFR-2/CD68 (frozen section only), and VEGF-A/CD68. Thesecondary antibodies were biotinylated using ARK kit (DAKO)
followed by alkaline phosphatase ABC kit. Alkaline phosphatase
reaction was developed using BT Red from ChemMate kit (Ventana,
Table 1. Clinical characteristics of the lymphomacases
Category DLBCL FL* CLL/SLLc BL
No. patients 28 7 5 2Median age (range), y 60 (29-83) 62 (45-81) 60 (53-61) 72Gender
Male 14 3 5 2Female 14 4 0 0
IPI scoreb
0-1 4 2 NA NA2 8 23 16 3>3 0 0
StageI 3 0 ND 0II 0 0 0III 7 0 0IV 18 7 2
LDHNormal 14 3 ND 0Elevated 14 4 2
Extranodal site0-1 17 7 ND 0>1 11 0 2
Survival statusAlive 18 5 0 0Deceased 10 1 0 2Unknown 0 1 5 0
B-cell marker patternx
GBC 3 NA NA NAABC 22ND 3
Abbreviations: LDH, lactate dehydrogenase; GBC, germinal centerB-cell pattern; ABC, activated B-cell pattern; NA, not applicable;ND, not determined.*All FL cases are histologic grade 1 or grade 2 diseases.cZAP-70 expression was positive by immunohistochemistry inthree of five cases.bIPI scores were calculated for the DLBCL cases. FLIPI scores werecalculated for the FL cases. Neither IPI nor FLIPI was applicable forCLL/SLL or BL.xB-cell marker pattern assignment is based on the expressionprofile of the four markers (CD10, BCL6, MUM1, and CD138) byimmunohistochemistry (35). Some paraffin blocks were fixed inBouin’s solution, and consequently, antigens could not be ade-quately retrieved for immunohistochemistry.
Hemangiogenesis in Non ^ Hodgkin’s Lymphoma
www.aacrjournals.org Clin Cancer Res 2006;12(19) October1, 20065623
Cancer Research. on September 21, 2020. © 2006 American Association forclincancerres.aacrjournals.org Downloaded from

Tucson, AZ) or Vector Blue Substrate kit II (Vector Laboratories,
Burlingame, CA). Frozen sections were double stained using immuno-
fluorescence method. VEGFR-1/CD68 double staining was done with
anti-VEGFR-1 followed by Alexa Fluor 594 goat anti-mouse IgG2b and
anti-CD68 (KP1) followed by Alexa Fluor 488 goat anti-mouse IgG1.
VEGFR-2/CD68 double staining was done first with FITC-conjugated
anti-VEGFR-2 and then with mouse anti-FITC (DAK-FITC4, DAKO)
followed by Alexa Fluor 488 goat anti-mouse IgG, and biotinylated
anti-CD68 (KP1) followed by Alexa Fluor 594–conjugated streptavidin
(Molecular Probes, Carlsbad, CA). VEGF-A/CD68 double staining was
done with anti-VEGF-A followed by Alexa Fluor 488 goat anti-rabbit
IgG and anti-CD68 (KP1) followed by Alexa Fluor 594 goat anti-mouse
IgG. All staining experiments were done with appropriate positive and
negative controls.Imaging data analysis. A total of 4 to 10 fields with the highest
vessel density in the lymphoma-involved area was selected foranalysis. For lymphoma cases with relatively preserved follicularstructures, only areas with neoplastic involvement (i.e., follicularcenter in FL) were studied. For CD34 and CD68 double-stainedlymphoma sections, individual CD34-positive vessels and CD68-positive cells were counted manually. For VEGFR-1 and CD68 double-stained frozen sections, the percentage of the pixels covered by theVEGFR-1 and CD68 staining at �200 magnification was defined asthe hemangiogenic index of VEGFR-1 and CD68 and scored using theNIH ImageJ program. Similarly, for a-SMA and CD34 double-stainedsections, the percentage of the pixels covered by these markers wasdefined as the a-SMA index. The coexpression of VEGFR-1 and CD68
was studied using laser scanning confocal microscopy. For readout ofthe B-cell activation markers, the germinal center B-cell pattern isdefined if only CD10 and/or BCL6 are expressed without theexpression of the activation markers MUM1 or CD138. ABC patternis assigned if either MUM1 or CD138 is expressed regardless of theexpression status of CD10 and BCL6 (35).
Statistical analysis. All results are expressed as mean and SD.ANOVA models were done for comparing outcome variables (CD34,CD68, and VEGFR-1/CD68 hemangiogenic index) across the varioussubtype groupings. The nonparametric Kruskal-Wallis test was alsoused to confirm the ANOVA analyses. For specific pairwisecomparisons of interest, post hoc analyses were done with theTukey’s honestly significant difference adjustment. Ninety-five percentconfidence intervals for mean differences between subtype groupingswere calculated to assess the precision of the obtained estimates. Allp-values are two sided with statistical significance evaluated at the0.05 a level.
Results
Clinical characteristics of the lymphoma cases. Forty-twocases of NHL were studied (Table 1). The median age of theDLBCL patients at diagnosis was 60 years, with median follow-up of 40 months (range, 2-108 months). The genderdistribution was evenly divided. Fourteen percent of DLBCLpatients had low risk disease according to the IPI, whereas 28%
Fig. 1. Incorporation of CD68+ cells, butnot the number of CD34+ vessels (MVD),is increased in aggressive subtypes oflymphomas. A, representative case(paraffin section) each of BL (1), DLBCL(2), CLL/SLL (3), FL (4), and FH (5) at�400 magnification. Arrow, CD34+ vessel(brown); arrowhead, CD68+ cells (red).B, scatter graph of the CD34 vessel countsof the NHL subtypes. Magnification, �200.Points, mean; bars, SD. C, scatter graph ofthe CD68 cell counts of the NHL subtypes.Magnification, �200. Points, mean; bars,SD. Open symbols, values from a singlecase; solid symbols, means for individualsubtypes. D, coexpression of CD34 (red)and podoplanin (brown) on CLL/SLLvasculature. Representative case each of BL(1), DLBCL (2), CLL/SLL (3), FL (4), andFH (5) at �400 magnification. Arrow,CD34+ vessel; arrowhead, double-positiveCD34+podoplanin+ vessels.
Human Cancer Biology
www.aacrjournals.orgClin Cancer Res 2006;12(19) October1, 2006 5624
Cancer Research. on September 21, 2020. © 2006 American Association forclincancerres.aacrjournals.org Downloaded from

and 57% of patients had low-intermediate and high-interme-diate risk diseases, respectively. Twenty-five of 28 (89%)DLBCL patients had stage III or IV disease at diagnosis, and36% of DLBCL patients were deceased at the time of lastclinical follow-up. Five of the 28 cases of DLBCL weretransformed from prior existing indolent subtypes, includingFL, marginal zone lymphoma, and CLL/SLL, whereas theremainders of the DLBCL cases were de novo (n = 23). B-cellsurface markers CD10, BCL6, MUM1, and CD138 wereanalyzed by immunohistochemistry and used as surrogatemarkers to stratify the DLBCL samples into either germinalcenter B-cell (GBC) expression pattern or activated B-cell (ABC)expression pattern (35). Consistent with the clustering of high-risk clinical features in our patient cohort, 79% (22 of 28) ofDLBCL cases had the ABC pattern, which portends a lessfavorable prognosis, and only 11% (3 of 28) of cases had thegerminal center B-cell pattern. The remaining three DLBCLcases were not evaluable due to suboptimal tissue procure-ment. For the FL cases, only grade 1 or 2 diseases wereincluded. For CLL/SLL, three of five cases were ZAP-70 positiveby immunohistochemistry.Microvessel density as measured by CD34+ vessels does not
correlate with histologic subtype of lymphoma. We first exam-ined the vascular component within the tumor stroma byCD34 staining (Fig. 1A). The average CD34 counts fromindividual DLBCL cases displayed a wide range of distribution(15.60-84.50 per 200� field). Surprisingly, the means of theCD34+ microvessel density (MVD) did not differ significantlybetween DLBCL, indolent subtypes of FL and CLL/SLL, and thebenign control of FH (37.10 F 16.24 versus 41.88 F 18.65versus 47.92 F 13.05; Fig. 1B; Table 2). Although not statis-tically significant, the de novo DLBCLs showed a trend towardhigher MVDs compared with the transformed cases and FL(38.55 F 17.04 versus 30.42 F 10.74 versus 29.52 F 3.19).Compared with the other indolent subtypes, CLL/SLL had ahigher mean MVD (CLL/SLL versus DLBCL versus FL: 59.18 F17.30 versus 37.10 F 16.24 versus 29.52 F 3.19; Table 2). Toexamine the possibility that some of the CD34+ vessels may beof lymphatic origin, we did CD34 and podoplanin costaining(Fig. 1D). Podoplanin is specifically expressed on lymphaticcapillaries but not in the blood vasculature. Up to 30% ofCD34+ vessels in CLL/SLL tumors expressed podoplanin. Incontrast, the benign control and the other NHL subtypes,including BL, DLBCL, and FL, had very few podoplanin/CD34double-positive vessels. When adjusted to exclude the lym-phatic vessels, the difference of the MVD of the CD34+ blood-specific vessels was less pronounced between the aggressivesubtype of DLBCL and the indolent subtypes of CLL and FL.Collectively, the means of the CD34+ MVD were comparablebetween the aggressive and indolent subtypes of lymphoma[aggressive (n = 30) versus indolent (n = 12) versus benignhyperplasia (n = 5): 39.29 F 18.71 versus 41.88 F 18.65 versus47.92 F 13.05; P = 0.61; Table 2]. These data suggest thatCD34+ MVD is not a sensitive biomarker for assessingneoangiogenesis in lymphoma and does not correlate withthe clinical aggressiveness and histologic subtype of humanlymphoma.Marked stromal and perivascular infiltration of CD68+
hematopoietic cells is present in aggressive subtypes of B-cellNHLs but not in indolent subtypes. To delineate the contribu-tion of the bone marrow–derived hemangiogenic cells present
in aggressive or indolent lymphomas, we quantified thenumber of hematopoietic cells expressing CD68 by immuno-histochemistry, which marks subsets of the hematopoieticprogenitors and mature cells of myeloid and monocytic originthat may contribute to lymphoma neoangiogenesis. In benigncontrols, such as tonsils and reactive lymph nodes, the CD68+
cells were limited to the parafollicular sinus area, where theywere closely associated with paracortical vasculature. Doublestaining with monoclonal antibodies against CD68 (hemato-poietic cells) and CD34 (vasculature) showed a dichotomouspattern of CD68+ hematopoietic cells in indolent versusaggressive NHL (Fig. 1A). In aggressive subtypes, includingBL and DLBCL, the tumor stroma was marked by intenseCD68+ myelomonocytic infiltration within the tumor stromaand perivascular regions. In some tumor-involved areas, theCD68+ cells were aligned side by side with the CD34+
neovessels. In contrast, there was a profound decrease in thenumber of infiltrating CD68+ cells within the stroma ofindolent subtypes. Additionally, the morphology of themyelomonocytic infiltrate was different. In aggressive lym-phomas, the intrastromal and perivascular CD68+ cells werelarger in size with ample cytoplasm, whereas in indolentlymphomas the CD68+ cells were small and often notassociated with the vasculature.The numbers of incorporated CD68+ cells were significantly
higher in aggressive subtypes than those in indolent subtypes[aggressive (n = 30) versus indolent (n = 12): 235.48 F92.63 versus 35.98 F 15.52 in 200� field; P < 0.0001;Fig. 1C; Table 2]. When the DLBCL cases were furthersegregated into de novo versus transformed cases, the averageCD68+ counts were comparable between the two groups(241.77 F 87.06 versus 193.97 F 129.91; P = 0.38; Table 2).Within the DLBCL subtype, no significant differences of theCD68+ counts were detected according to the followingvariables: GBC (n = 3) versus ABC (n = 22; 299.63 F 82.09versus 227.80 F 94.74); IPI 0 to 2 (n = 12) versus IPI >2 (n =16; 258.46 F 74.27 versus 216.10 F 103.24); and alive (n =18) versus deceased (n = 10; 227.83 F 101.78 versus 245.82F 77.94). These data implicate a fundamental difference inthe hemangiogenic switch between indolent and aggressivesubtypes of lymphoma. The aggressive subtypes are substan-tially more capable of recruitment and stromal incorporationof the marrow-derived CD68+ hematopoietic cells. The differ-ences of hemangiogenic activity within the DLBCL subtypemay be less pronounced compared with the differencesbetween the subtypes and could potentially be obscured bythe small sample size.
Stroma of aggressive NHL is characterized by increasedproliferation of VEGFR-1+ neovasculature and perivascularincorporation of VEGFR-1+CD68+ hematopoietic cells expressingVEGF-A. VEGFR-1 expression on the hematopoietic cellsidentifies a population of proangiogenic hematopoietic cellsthat contribute to neoangiogenesis in the primary tumors (21)and initiating the premetastatic niche (36, 37). Costainingwith CD68 and VEGFR-1 on frozen sections was used toidentify cells that could potentially participate in blood vesselassembly within the lymphoma stroma. In DLBCL, there wereincreased numbers of VEGFR-1+ vascular structures that weredecorated and infiltrated by CD68+ hematopoietic cells.Importantly, the majority of the CD68+ hematopoietic cellscoexpressed VEGFR-1 and seemed to be in close association
Hemangiogenesis in Non ^ Hodgkin’s Lymphoma
www.aacrjournals.org Clin Cancer Res 2006;12(19) October1, 20065625
Cancer Research. on September 21, 2020. © 2006 American Association forclincancerres.aacrjournals.org Downloaded from

with one or another VEGFR-1+ neovessels (Fig. 2F-I). TheCD68+VEGFR-1+ double-positive cells were localized eitherwithin intravascular space, transiting across the vascular walls,juxtapositioning endothelial cells, or scattered in a shortdistance away from the vessels. To compare the hemangio-genic activity among different subtypes, we developed theterm hemangiogenic index, which measures the percentage ofthe tumor-involved stromal area covered by the VEGFR-1+
vessels and VEGFR-1+CD68+ hematopoietic cells. In contrast
to the aggressive subtypes, the hemangiogenic index ofindolent subtypes of NHL, including CLL/SLL and FL, wassignificantly lower [DLBCL (n = 5) versus CLL (n = 4) versusFL (n = 5): 18.14 F 2.83% versus 3.39 F 1.95% versus 6.54F 2.82%; P < 0.0001; Fig. 2A-E]. No CD68+VEGFR-1+ double-positive cells were observed in indolent subtypes. Toinvestigate whether the CD68+ cells also coexpress othervascular markers, we did double staining of CD68 with eitherCD34 or VEGFR-2 on frozen sections of DLBCL and BL
Fig. 2. Enhanced colocalization ofVEGFR-1+CD68+ hematopoietic cells withVEGFR-1+ neovessels in aggressive but notindolent lymphoma subtypes. A toD,VEGFR-1+ vessels and cells (brown) andCD68+ cells (red) at �400 magnificationin a representative case (frozen section)each of DLBCL (A), CLL/SLL (B), FL (C),and tonsil (D). E, scatter graph ofhemangiogenic index ofVEGFR-1/CD68correlated to lymphoma subtypes. Points,mean; bars, SD. Sample sizes (n) forindividual subtypes. Openblack circle, indexfrom a single case; solid red circle, meansfor individual lymphoma subtypes.*, P < 0.0001, comparing DLBCL with CLLor FL. F to I, coexpression ofVEGFR-1and CD68 in DLBCL. F and G, confocalscanning microscopic analysis ofVEGFR-1(Alexa Fluor 594; red) and CD68 (AlexaFluor 488; green) expression on DLBCLfrozen sections.White arrowhead,VEGFR-1+ vessels and cells; yellowarrow, cells coexpressingVEGFR-1(red, membranous) and CD68 (green,cytoplasmic and membranous).V, vessel.H and I, light microscopic analysis ofVEGFR-1 (brown) and CD68 (blue)coexpression. Black arrowhead,VEGFR-1+
vessels and cells; black arrow, cellscoexpressingVEGFR-1and CD68.
Table 2. Correlation of the CD34 MVD and CD68 cell counts to NHL subtypes
Variables Aggressive subtypes
De novo DLBCL Transformed DLBCL DLBCL, total
Sample size 23 5 28CD34*
Range 15.60-84.50 17.25-44.50 15.60-84.50Mean 38.55 30.42 37.10SD 17.04 10.74 16.24SE 3.55 4.80 3.0795% Confidence interval 31.2-45.9 17.1-43.8 30.8-43.4
CD68c
Range 30.17-387.50 47.25-329.25 30.17-387.50Mean 241.77 193.97 233.24SD 87.06 129.91 94.99SE 18.15 58.10 17.9595% Confidence interval 204.1-279.4 32.7-355.2 196.4-270.1
*CD34 counts: aggressive (n = 30) versus indolent (n = 12) versus benign (n = 5), P = 0.61 by ANOVA test.cCD68 counts: aggressive (n = 30) versus indolent (n = 12) versus benign (n = 5), P < 0.0001 by ANOVA test. Pairwise comparisons for CD68counts (with Tukey’s honestly significant difference adjustment for multiple comparisons): aggressive (235.48 F 92.63) versus indolent (35.98F 15.52), P < 0.0001; aggressive (235.48 F 92.63) versus benign (79.06 F 27.76), P < 0.0001; indolent (35.98 F 15.52) versus benign(79.06 F 27.76), P = 0.54.
Human Cancer Biology
www.aacrjournals.orgClin Cancer Res 2006;12(19) October1, 2006 5626
Cancer Research. on September 21, 2020. © 2006 American Association forclincancerres.aacrjournals.org Downloaded from

(Fig. 3). Both CD34 and VEGFR-2 marked vasculature onlyand were not expressed in the CD68+ hematopoietic cells. Themajority of the perivascular CD68+ hematopoietic cellsexpressed VEGF-A. These data suggest that hemangiogenicindex as determined by the number of infiltrating VEGFR1+
and CD68+ cells provides a reliable means to assess thecontribution of the proangiogenic hematopoietic cells toneoangiogenesis in different histologic subtypes of lymphoma.In addition to providing structural support, perivascularpositioning of proangiogenic VEGF-A+VEGFR-1+CD68+ hema-topoietic cells in aggressive lymphoma subtypes argues for aparacrine role in neovessel formation, where neoangiogenesisis essential to sustain rapid tumor growth.Stroma of the indolent subtype of CLL/SLL is marked by
incorporation of a large numbers of a-SMA+ cells. Newlyformed neovessels within regenerating organs are stabilizedby incorporation of a-SMA+ cells to the perivascular zone. Inbenign nodal hyperplasia, the a-SMA+ stromal cells werelimited to the parafollicular sinus in association with para-cortical vasculature. Remarkably, despite the abundance of theCD68+ hematopoietic infiltrates, the stroma of aggressivesubtypes, such as DLBCL, was largely devoid of a-SMA+ cells.Most of the a-SMA+ cells detected in DLBCL were vascularsmooth muscle cells, which demarcated the CD34+ vasculature.By contrast, the stroma of indolent subtype of CLL/SLL, whichhad scant incorporation of CD68+ cells, was marked by diffuseinfiltration of a-SMA+ cells, which formed an elaboratemeshwork bridging CD34+ vessels within the parenchyma oflymphomas. The magnitude of incorporation of a-SMA+ cellsin CLL, which included both perivascular and intrastromalareas, was significantly higher than the other subtypes andbenign nodal hyperplasia (CLL/SLL versus DLBCL versus FLversus FH: 11.80% versus 2.22% versus 1.42% versus 2.70%;P < 0.0001; Fig. 4). These findings indicate that stromalcomposition of lymphomas is dictated by differential recruit-ment of either mesenchymal a-SMA+ or hemangiogenicCD68+VEGFR1+ cells. CLL/SLL stroma has scant infiltration ofCD68+VEGFR1+ cells but is populated by a large number ofa-SMA+ mesenchymal cells. In contrast, aggressive subtypesrecruit CD68+VEGFR1+ cells but lack incorporation of a-SMA+
stromal cells.
Fig. 3. PerivascularVEGFR-1+CD68+ hematopoietic cells are distinct from CD34+
andVEGFR-2+ endothelium and expressVEGF-A. All double stainings were done onfrozen sections of DLBCL and BL cases. A and B, coexpression of CD68 (AlexaFluor 488; green) andVEGFR-1 (Alexa Fluor 594; red).White arrowhead,VEGFR-1/CD68 double-positive cells.V, vessel. C and D, costaining of CD68 (Alexa Fluor594; red) andVEGFR-2 (Alexa Fluor 488; green).White arrow, single-positiveCD68 cells. E and F, costaining of CD68 (Alexa Fluor 594; red) and CD34 (AlexaFluor 488; green).White arrow, single-positive CD68 cells.G and H, coexpressionof CD68 (Alexa Fluor 594; red) andVEGF-A (Alexa Fluor 488; green). Asterisk,CD68/VEGF-A double-positive cells.
Table 2. Correlation of the CD34 MVD and CD68 cell counts to NHL subtypes (Cont’d)
Aggressive subtypes Indolent subtypes Benign
BL Subtype, total FL CLL/SLL Subtype, total FH
2 30 7 5 12 5
47.5-92.5 15.60-92.50 24.60-33.60 41.00-81.75 24.60-81.75 29.80-63.00NA 39.29 29.52 59.18 41.88 47.92NA 18.71 3.19 17.30 18.65 13.05NA 3.42 1.20 7.74 5.38 5.84NA 32.3-46.3 26.6-32.5 37.7-80.7 30.0-53.7 31.7-64.1
227.7-306.2 30.17-387.50 23.25-58.00 13.00-47.00 13.00-58.00 47.60-122.50NA 235.48 40.98 28.98 35.98 79.06NA 92.63 14.02 16.20 15.52 27.76NA 16.91 5.30 7.24 4.48 12.41NA 200.9-270.1 28.0-53.9 8.9-49.1 26.1-45.8 44.6-113.5
Hemangiogenesis in Non ^ Hodgkin’s Lymphoma
www.aacrjournals.org Clin Cancer Res 2006;12(19) October1, 20065627
Cancer Research. on September 21, 2020. © 2006 American Association forclincancerres.aacrjournals.org Downloaded from

Discussion
Non-Hodgkin’ lymphomas are a heterogenous group ofmalignancies. The contribution of neoangiogenesis to thepathogenesis of various human lymphoma subtypes remainspoorly defined. In preclicnical mouse models, it is wellestablished that neoangiogenesis and growth of murine lym-phomas is partially dependent on the recruitment of bonemarrow–derived proangiogenic hematopoietic population con-tributing to neovessel assembly either instructively by releasinggrowth factors, such as VEGF-A, or constructively by localizingperivascularly to stabilize newly formed vessels (21, 24, 38). Inthis study, we show that there is a statistically significantcorrelation between hemangiogenic index, as measured by thedifferential stromal recruitment of either hemangiogenicCD68+VEGFR-1+ cells or mesenchymal a-SMA+ cells, andhistologic subtype of human NHL (Fig. 5). In aggressivesubtypes of lymphoma, there is increased proliferation ofVEGFR-1+ neovasculature and enhanced recruitment and peri-vascular incorporation of VEGF-A-producing CD68+VEGFR-1+
hematopoietic cells, which provide paracrine support toneovasculature. Remarkably, the aggressive subtypes weredepleted of a-SMA+ stromal cells. In contrast, the stroma ofindolent subtype of CLL/SLL has a profound increase in thenumber of a-SMA+ mesenchymal cells both perivascularlyand diffusely, which presumably enhance vascular stabilityand may contribute to chemotherapy resistance. Importantly,there is no correlation between the CD34+ microvessel
densities in aggressive versus indolent lymphomas. These datasuggest that the stromal hemangiogenic index, determined bythe magnitude of the incorporation of VEGFR-1+, CD68+, anda-SMA+ cells, provides a novel surrogate marker for assessingbone marrow–derived hematopoietic contribution to neo-angiogenesis in human NHL. As CD68+ hematopoietic and a-SMA+ stromal cells can directly be targeted by antiangiogenicagents, stromal hemangiogenic index may be used to predictresponse to antiangiogenic therapy.The evidence highlighting the importance of stromal micro-
environment during lymphomagenesis is emerging, mostrecently from large-scale gene expression array studies lookingat differential genetic signatures among different subtypes orwithin one specific subtype of NHL (7–9). For instance, inDLBCL, genetic signatures expressed by the stromal and infil-trating immune cells, including lymphocytes, macrophages, anddendritic cells, have been shown to form a distinct prognosticgroup, which identifies the tumor microenvironment for riskstratification (8, 39). In FL, clinical survival was correlated to thenontumor immune infiltrating cells alone (40). Indeed, thecontent of the lymphoma-associated macrophages is anindependent predictor of survival in FL (31). However, themechanisms underscoring the prognostic contribution of thehematopoietic immune cells remain poorly characterized.To characterize the tumor hematopoietic compartment, we
have used the hematopoietic marker CD68, which is expressedby hematopoietic cells, including proangiogenic VEGFR-1+
myelomonocytic progenitors, monocytes, macrophages, and
Fig. 4. Stromal a-SMA is absent in aggressive lymphomas butsignificantly increased in indolent subtype of CLL/SLL. a-SMA+
stroma cells (brown) and CD34+ vessels (red) in a representativecase (paraffin section) each of BL (A), DLBCL (B), CLL/SLL (C),FL (D), and FH (E). F, scatter graph of a-SMA+ stroma index of NHLsubtypes. Points, mean; bars, SD. Sample sizes (n) for individualsubtypes. w , index from a single case; x, means for individuallymphoma subtypes. *, P < 0.0001, comparing CLL/SLL withDLBCL or FL.
Human Cancer Biology
www.aacrjournals.orgClin Cancer Res 2006;12(19) October1, 2006 5628
Cancer Research. on September 21, 2020. © 2006 American Association forclincancerres.aacrjournals.org Downloaded from

dendritic cells. Our present study clearly shows a statisticallysignificant progressive increase in CD68 hematopoietic infil-trates within lymphoma stroma across different histologiesfrom indolent to aggressive subtypes. Within DLBCL subtype,the de novo DLBCL cases exhibit a wide range of CD68infiltrating cells, perhaps reflecting the underlying heterogene-ity of the pathogenic tumor cells. No significant correlation wasnoted between CD68 cell counts and the clinical outcomes inthe de novo DLBCL cohorts, although this may be masked byour sample size and the clustering of poor-risk features.Questions remain about the functional roles of the CD68+
hematopoietic infiltrates in the lymphoma stroma. CD68+ cellscomprise a heterogeneous population, including monocytes,tissue macrophages, and dendritic cells. Our costaining studieson the CD68+ cells have shown that majority of the CD68+ cellscoexpress VEGF-A and remain in close contact with the vascularendothelium, suggestive of paracrine support these cells mayhave on the developing neovasculature in aggressive lympho-ma. Indeed, emerging evidence has shown that bone marrow–derived hematopoietic cells critically contribute to neovesselformation by promoting vessel stability (38) and enhancingin situ endothelial proliferation (26).
To characterize the tumor vascular compartment, we haveused markers, including CD34 and VEGFR-1. Our studyhas shown that CD34 alone is not a sensitive biomarker forlymphoma neoangiogenesis, as it stains stable preexistingvessels and lymphatic structures as well. In contrast, VEGFR-1expression showed a clear difference of vascular distributionwith prominent microvascular staining in the aggressivesubtype of DLBCL. Both the VEGFR-1 staining intensityand the VEGFR-1+ microvessel counts were significantlydecreased in the indolent subtypes of FL and CLL/SLL. Assuch, the magnitude of VEGFR-1 expression either on theendothelial or hematopoietic cells provides a more sensitivemeans to assess the degree of neoangiogenesis in varioussubtypes of lymphomas. Recently, VEGFR-1+ hematopoieticprogenitors have been implicated in initiating the pre-metastatic niche, a tumor-directed process proceeding theinfiltration of actual tumor cells or tumor-associated neo-angiogenesis (37). This raises a provocative notion thatVEGFR-1+CD68+ hematopoietic cells may also direct themetastatic spread of lymphoma. Clearly, future in vivostudies in lymphoma mouse models are needed to furtherdelineate the functional contribution of VEGFR-1+CD68+
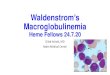
Fig. 5. Schema depicting the potential mechanism by which hemangiogenicVEGFR-1+CD68+ and a-SMA+ cells contribute to neoangiogenesis. Stromal composition oflymphomas is dictated by differential recruitment of either hemangiogenicVEGFR-1+CD68+ cells or mesenchymal a-SMA+ cells. A, aggressive subtypes (DLBCL/BL) recruitbone marrow ^ derived CD68+VEGFR-1+ cells but lack incorporation of stromal cells.Vascular composition is characterized by perivascular assembly ofVEGF-A-producingVEGFR-1+CD68+ hematopoietic cells. B, stroma of indolent subtype of CLL/SLL is populated by a large number of a-SMA+ mesenchymal cells, which presumablyenhance vascular stability. C, comparison of perivascular accessory cells between aggressive and indolent NHL. Bone marrow (BM)^ derivedVEGFR-1+CD68+VEGF-A+
hematopoietic cells are preferentially recruited to perivascular region of growing neovessels in aggressive NHL, whereas a-SMA+ mesenchymal stromal cells arepredominantly recruited to perivascular region in CLL/SLL.
Hemangiogenesis in Non ^ Hodgkin’s Lymphoma
www.aacrjournals.org Clin Cancer Res 2006;12(19) October1, 20065629
Cancer Research. on September 21, 2020. © 2006 American Association forclincancerres.aacrjournals.org Downloaded from

hematopoietic population in lymphoma angiogenesis andprogression.Remarkably, in indolent subtype of CLL/SLL, the tumor
stroma is marked by a-SMA+ stromal cells diffusely as well asperivascularly. a-SMA expression is up-regulated in fibroblastsin response to tumor stromal-specific growth factors, such asplatelet-derived growth factor and transforming growth factor-h, causing a unique phenotype of tumor-associated myofibro-blasts (32). a-SMA+ myofibroblasts have recently been shownto express high level of SDF-1a, a chemokine critical formobilization and recruitment of CXCR4-expressing vascularprogenitors (33). Alternatively, a-SMA+ pericytes/vascularsmooth muscle cells can be recruited and proliferate into theinterstitial stroma along with vascular endothelial cells underproangiogenic stimuli and regulate vessel stability (34, 41).Blood vessels with few pericytes coverage were more sensitiveto VEGF-A inhibition (42). Thus, targeting a-SMA+ perivas-cular cells may compliment endothelial cell inhibition foreffective antiangiogenic therapy in indolent subtypes of CLL/SLL (43).Our study has provided a novel perspective into the complex
interplay between several stromal and vascular componentswithin the lymphoma microenvironment and the potentiallydivergent pathogenic processes whereby the bone marrow–derived hemangiogenesis contributes to lymphomagenesis. Inaggressive subtypes, prominent incorporation of proangiogenic
VEGFR-1+CD68+ cells and diminished localization of a-SMA+
stromal cells to the perivascular zone may contribute toenhanced neoangiogenesis and chemosensitivity, whereasdecrease in CD68+ cells and increase in the a-SMA+ incorpo-ration may promote neovessel stability and chemoresistance inCLL/SLL. Identification of critical hemangiogenic componentsspecific to lymphoma subtypes will lay the foundation whereefficacy in blocking these factors alone or in combination canbe tested in clinical trials. In pilot studies, bevacizumab hasshown clinical activity both as a single agent in relapsedaggressive NHL setting (44) and in combination with rituximaband cyclophosphamide-Adriamycin-vincristine-prednisone(CHOP) in upfront setting (45), lending support to antiangio-genic development in NHL. It is tempting to speculate that anti-VEGF-A therapy may be an effective addition to the standardchemotherapy for aggressive subtypes of lymphoma, whichhave a significant VEGFR-1+ hemangiogenic stromal compo-nent, whereas disrupting mesenchymal-tumor interaction mayafford durable remission in the indolent subtypes.
Acknowledgments
We thank Dr. Sherry Ikalowych for assistance in patient data collection,Dr. LoicVincent for helpful discussion and critical review of the article, and ImClonescientists Drs. YanWu, Zhenping Zhu, and Dan Hicklin for kindly providing anti-humanVEGFR-1antibody FB5.
Human Cancer Biology
www.aacrjournals.orgClin Cancer Res 2006;12(19) October1, 2006 5630
References1. Coiffier B. Effective immunochemotherapy foraggressive non-Hodgkin’s lymphoma. Semin Oncol2004;31:7^11.
2. Fisher RI. Overview of non-Hodgkin’s lymphoma:biology, staging, and treatment. Semin Oncol 2003;30:3^9.
3. A predictive model for aggressive non-Hodgkin’slymphoma. NEngl JMed1993;329:987^94.
4. Yunis JJ, Mayer MG, Arnesen MA, Aeppli DP, OkenMM, Frizzera G. bcl-2 andother genomic alterations inthe prognosis of large-cell lymphoma. N Engl J Med1047;320:1047^54.
5. Offit K, Lo Coco F, Louie DC, et al. Rearrangementof the bcl-6 gene as a prognostic marker in diffuselarge-cell lymphoma. NEngl JMed1994;331:74^80.
6. Lo Coco F, Gaidano G, Louie DC, Offit K, ChagantiRS, Dalla-Favera R. p53 mutations are associatedwith histologic transformation of follicular lymphoma.Blood1993;82:2289^95.
7.Alizadeh AA, EisenMB, Davis RE, et al. Distinct typesof diffuse large B-cell lymphoma identified by geneexpression profiling. Nature 2000;403:503^11.
8. Rosenwald A,Wright G, ChanWC, et al. The use ofmolecular profiling to predict survival after chemother-apy for diffuse large-B-cell lymphoma. N Engl JMed2002;346:1937^47.
9. Shipp MA, Ross KN, Tamayo P, et al. Diffuse largeB-cell lymphomaoutcome predictionby gene-expres-sion profiling and supervised machine learning. NatMed 2002;8:68^74.
10. Folkman J. Angiogenesis in cancer, vascular, rheu-matoid, and other disease. Nat Med1995;1:27^31.
11. Bergers G, Benjamin LE. Tumorigenesis and theangiogenic switch. Nat Rev Cancer 2003;3:401^10.
12. Coussens LM,Werb Z. Inflammation and cancer.Nature 2002;420:860^7.
13. Bergers G, Javaherian K, Lo KM, Folkman J,Hanahan D. Effects of angiogenesis inhibitors onmul-tistage carcinogenesis in mice. Science 1999;284:808^12.
14. Ferrara N, Hillan KJ, Gerber HP, NovotnyW.Discov-
ery and development of bevacizumab, an anti-VEGFantibody for treating cancer. Nat Rev Drug Discov2004;3:391^400.
15. Hurwitz H, Fehrenbacher L, NovotnyW, et al. Beva-cizumab plus irinotecan, fluorouracil, and leucovorinfor metastatic colorectal cancer. N Engl JMed 2004;350:2335^42.
16. Johnson SH, Fehrenbacher L, Novotny WF, et al.Randomized phase II trial comparing bevacizumabplus carboplatin and paclitaxel with carboplatin andpaclitaxel alone in previously untreated locallyadvanced or metastatic non-small-cell lung cancer.J Clin Oncol 2004;22:2184^91.
17. Miller KD, Chap LI, Holmes FA, et al. Randomizedphase III trial of capecitabine compared with bevaci-zumab plus capecitabine in patients with previouslytreated metastatic breast cancer. J Clin Oncol 2005;23:792^9.
18. Doussis-Anagnostopoulou IA,Talks KL,Turley H,et al.Vascular endothelial growth factor (VEGF) isexpressed by neoplastic Hodgkin-Reed-Sternbergcells inHodgkin’s disease.JPathol 2002;197:677^83.
19. Foss HD, Araujo I, Demel G, Klotzbach H, HummelM, Stein H. Expression of vascular endothelial growthfactor in lymphomas and Castleman’s disease.JPathol1997;183:44^50.
20.Wang ES,Teruya-FeldsteinJ,WuY, Zhu Z, Hicklin DJ,MooreMA.Targeting autocrine andparacrineVEGF re-ceptor pathways inhibits human lymphomaxenograftsin vivo. Blood 2004;104:2893^902.
21. Lyden D, Hattori K, Dias S, et al. Impaired recruit-ment of bone-marrow-derived endothelial and hema-topoietic precursor cells blocks tumor angiogenesisand growth. Nat Med 2001;7:1194^201.
22. Heissig B, Hattori K, Dias S, et al. Recruitment ofstem and progenitor cells from the bonemarrownicherequires MMP-9 mediated release of kit-ligand. Cell2002;109:625^37.
23. Luttun A,TjwaM,Moons L, et al. Revascularizationof ischemic tissues by PlGF treatment, and inhibitionof tumor angiogenesis, arthritis, and atherosclerosisby anti-Flt1. Nat Med 2002;8:831^40.
24. Rafii S, Lyden D, Benezra R, Hattori K, Heissig B.Vascular and haematopoietic stem cells: novel targetsfor anti-angiogenesis therapy? Nat Rev Cancer 2002;2:826^35.
25. Cursiefen C, Chen L, Borges LP, et al. VEGF-A stimulates lymphangiogenesis and hemangio-genesis in inflammatory neovascularization viamacrophage recruitment. J Clin Invest 2004;113:1040^50.
26.GrunewaldM, Avraham I, DorY, et al.VEGF-inducedadult neovascularization: recruitment, retention, androle of accessory cells. Cell 2006;124:175^89.
27. Conejo-Garcia JR, Benencia F, Courreges MC,et al. Tumor-infiltrating dendritic cell precursorsrecruited by a h-defensin contribute to vasculogen-esis under the influence of VEGF-A. Nat Med 2004;10:950^8.
28. Maruyama K, Ii M, Cursiefen C, et al. Inflammation-induced lymphangiogenesis in the cornea arises fromCD11b-positive macrophages. J Clin Invest 2005;115:2363^72.
29. Yang L, DeBusk LM, Fukuda K, et al. Expansionof myeloid immune suppressor Gr+CD11b+ cells intumor-bearing host directly promotes tumor angio-genesis. Cancer Cell 2004;6:409^21.
30. Pollard JW. Tumour-educated macrophages pro-mote tumour progression and metastasis. Nat RevCancer 2004;4:71^8.
31. Farinha P,Masoudi H, Skinnider BF, et al. Analysis ofmultiple biomarkers shows that lymphoma-associatedmacrophage (LAM) content is an independent pre-dictor of survival in follicular lymphoma. Blood 2005;106:2169^74.
32. Ronnov-Jessen L, Petersen OW, Koteliansky VE,Bissell MJ. The origin of the myofibroblasts in breastcancer. Recapitulation of tumor environment in cultureunravels diversity and implicates converted fibroblastsand recruited smooth muscle cells. JClin Invest 1995;95:859^73.
33. Orimo A, Gupta PB, Sgroi DC, et al. Stromal fibro-blasts present in invasive human breast carcinomaspromote tumor growth and angiogenesis through
Cancer Research. on September 21, 2020. © 2006 American Association forclincancerres.aacrjournals.org Downloaded from

elevated SDF-1/CXCL12 secretion. Cell 2005;121:335^48.
34. Darland DC, Massingham LJ, Smith SR, Piek E,Saint-Geniez M, D’Amore PA. Pericyte production ofcell-associatedVEGF is differentiation-dependent andis associatedwith endothelial survival. Dev Biol 2003;264:275^88.
35. Chang CC, McClintock S, Cleveland RP, et al.Immunohistochemical expression patterns of germinalcenter and activation B-cell markers correlate withprognosis in diffuse large B-cell lymphoma. AmJSurgPathol 2004;28:464^70.
36. Hiratsuka S, Nakamura K, Iwai S, et al. MMP9induction by vascular endothelial growth factor recep-tor-1 is involved in lung-specific metastasis. CancerCell 2002;2:289^300.
37. Kaplan RN, Riba RD, Zacharoulis S, et al.VEGFR1-positive haematopoietic bone marrow progenitors
initiate the pre-metastatic niche. Nature 2005;438:820^7.
38. De PalmaM,Venneri MA, Roca C, Naldini L. Target-ing exogenous genes to tumor angiogenesis by trans-plantation of genetically modified hematopoietic stemcells. Nat Med 2003;9:789^95.
39. Monti S, Savage KJ, KutokJL, et al. Molecular pro-filing of diffuse large B-cell lymphoma identifies robustsubtypes including one characterized by host inflam-matory response. Blood1851;105:1851^61.
40.Dave SS,Wright G,Tan B, et al. Predictionof survivalin follicular lymphoma based on molecular features oftumor-infiltrating immune cells. N Engl J Med 2004;351:2159^69.
41. FolkmanJ. How is blood vessel growth regulated innormal and neoplastic tissue? GHA. Clowesmemori-al Award lecture. Cancer Res1986;46:467^73.
42.Benjamin LE, Hemo I, Keshet E. A plasticity window
for blood vessel remodeling is defined by pericytecoverage of the preformed endothelial network and isregulated by PDGF-B and VEGF. Development 1998;125:1591^8.
43. Bergers G, Song S, Meyer-Morse N, Bergsland E,Hanahan D. Benefits of targeting both pericytes andendothelial cells in the tumor vasculature with kinaseinhibitors. JClin Invest 2003;111:1287^95.
44. Stopeck AT, BellamyW, UngerJ, et al. Phase II trialof single agent bevacizumab (Avastin) in patients withrelapsed, aggressive non-Hodgkin’s lymphoma(NHL): Southwest Oncology Group Study S0108.Proc Am Soc Clin Oncol 2005;23:6592.
45. Ganjoo KN, An CS, RobertsonMJ, et al. Rituximab,bevacizumab and CHOP (RA-CHOP) in untreated dif-fuse large B-cell lymphoma: safety, biomarker andpharmacokinetic analysis. Leuk Lymphoma 2006;47:998^1005.
Hemangiogenesis in Non ^ Hodgkin’s Lymphoma
www.aacrjournals.org Clin Cancer Res 2006;12(19) October1, 20065631
Cancer Research. on September 21, 2020. © 2006 American Association forclincancerres.aacrjournals.org Downloaded from

2006;12:5622-5631. Clin Cancer Res Jia Ruan, Elizabeth Hyjek, Pouneh Kermani, et al.
Hodgkin's Lymphoma−Histologic Subtype of Non Magnitude of Stromal Hemangiogenesis Correlates with
Updated version
http://clincancerres.aacrjournals.org/content/12/19/5622
Access the most recent version of this article at:
Cited articles
http://clincancerres.aacrjournals.org/content/12/19/5622.full#ref-list-1
This article cites 44 articles, 8 of which you can access for free at:
Citing articles
http://clincancerres.aacrjournals.org/content/12/19/5622.full#related-urls
This article has been cited by 14 HighWire-hosted articles. Access the articles at:
E-mail alerts related to this article or journal.Sign up to receive free email-alerts
Subscriptions
Reprints and
To order reprints of this article or to subscribe to the journal, contact the AACR Publications
Permissions
Rightslink site. (CCC)Click on "Request Permissions" which will take you to the Copyright Clearance Center's
.http://clincancerres.aacrjournals.org/content/12/19/5622To request permission to re-use all or part of this article, use this link
Cancer Research. on September 21, 2020. © 2006 American Association forclincancerres.aacrjournals.org Downloaded from