Embed Size (px)
Citation preview
Main textbooks
Paul Coulthard, Keith Horner, Philip Sloan, et al. Master Dentistry. Volume 1,2, Oral and Maxillofacial Surgery, Radiology, Pathology, and Oral Medicine.
Churchill Livingstone 2003
Updated knowledge from library and Website.
Dental Caries
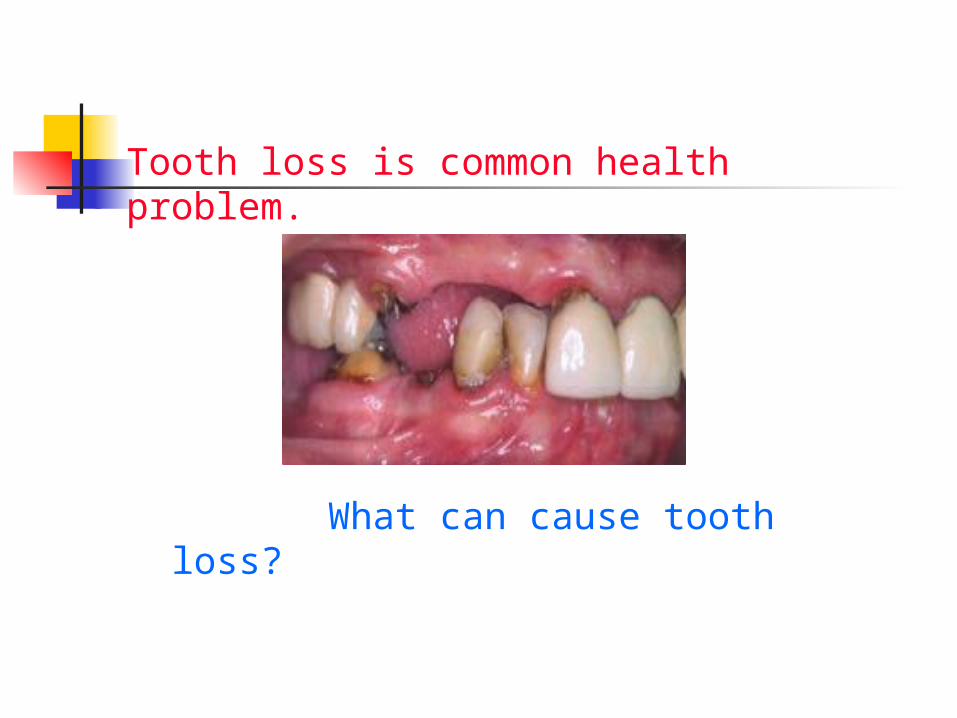
Tooth loss is common health problem.
What can cause tooth loss?
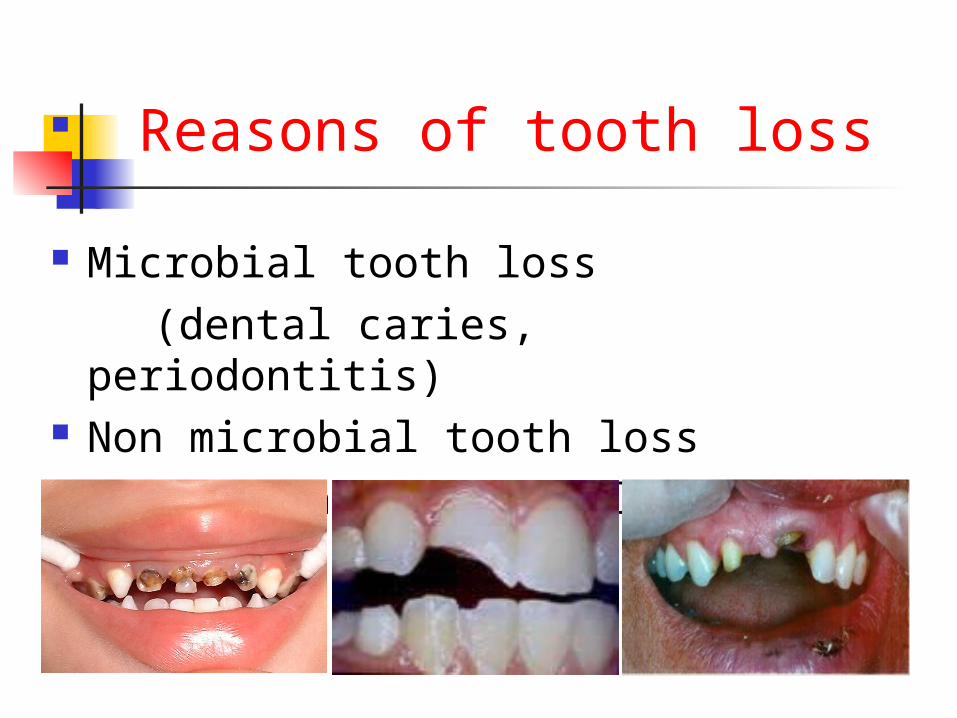
Reasons of tooth loss
Microbial tooth loss (dental caries, periodontitis) Non microbial tooth loss (trauma, congenital loss)
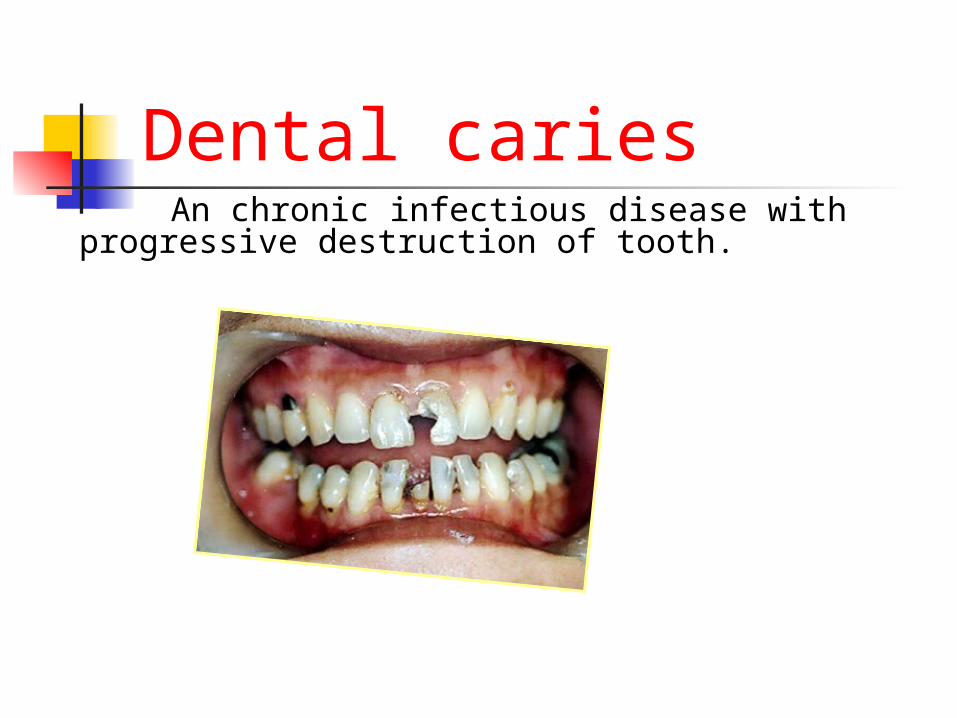
Dental caries An chronic infectious disease with progressive
destruction of tooth.
Prevalence and incidence
http://www.wrongdiagnosis.com/d/dental_caries/stats-country.htm(2004)
Almost everyone is affected by dental caries.
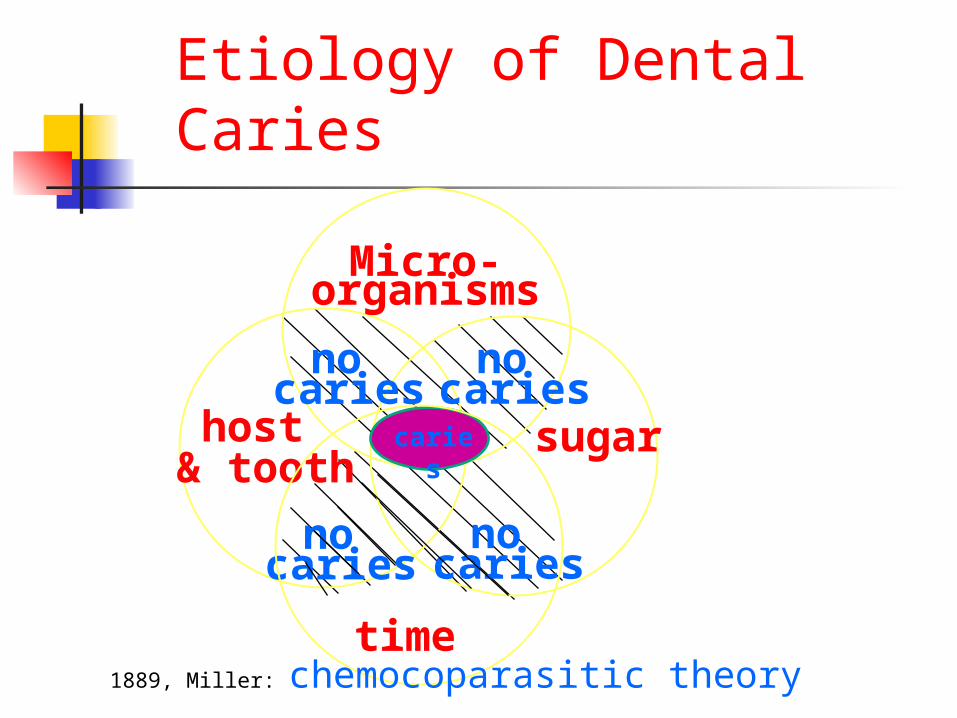
Etiology of Dental Caries
Micro-organisms
host & tooth
sugar
time
no caries
no caries
no caries
no caries
caries
1889, Miller: chemocoparasitic theory
MAJOR FACTORS 3 necessary requirements:
1) Microorganisms—bacteria, plaque
2) sugar --- carbohydrates
3) host & tooth---saliva, tooth
( and) 4) time.
Role of bacteria There are many kinds of bacteria in
normal oral cavity.
Mainly the bacteria causing caries are Streptococcus Mutans (MS).
Microorganisms:
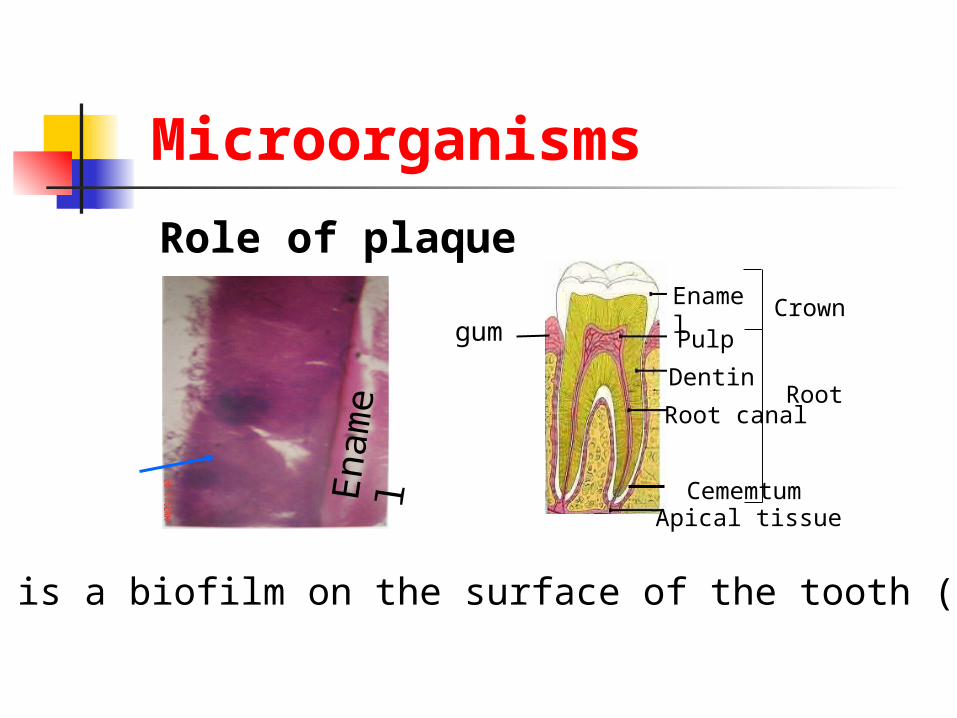
Role of plaque
Plaque is a biofilm on the surface of the tooth (enamel).
Enam
el
EnamelPulp
Root canal
Cememtum Apical tissue
Dentin
Crown
Root
gum
Microorganisms

Role of Tooth
• Quality
• Position
• Structure
• arrangement
host & tooth

Role of saliva:
It plays role in remineralization on the teeth.
Saliva has the buffering action and cleansing effect.
host & tooth
Role of carbohydrates:
the most important cause; refined carbohydrates are directly
proportional with dental caries.
Sugar:
MINOR FACTORS:
Enamel composition Morphology of the tooth Habit of brushing teeth Immunity
Clinical classification of caries
According to three basic factors : severity and rate of progression
anatomical site(involving site) age patterns at which lesions
predominate
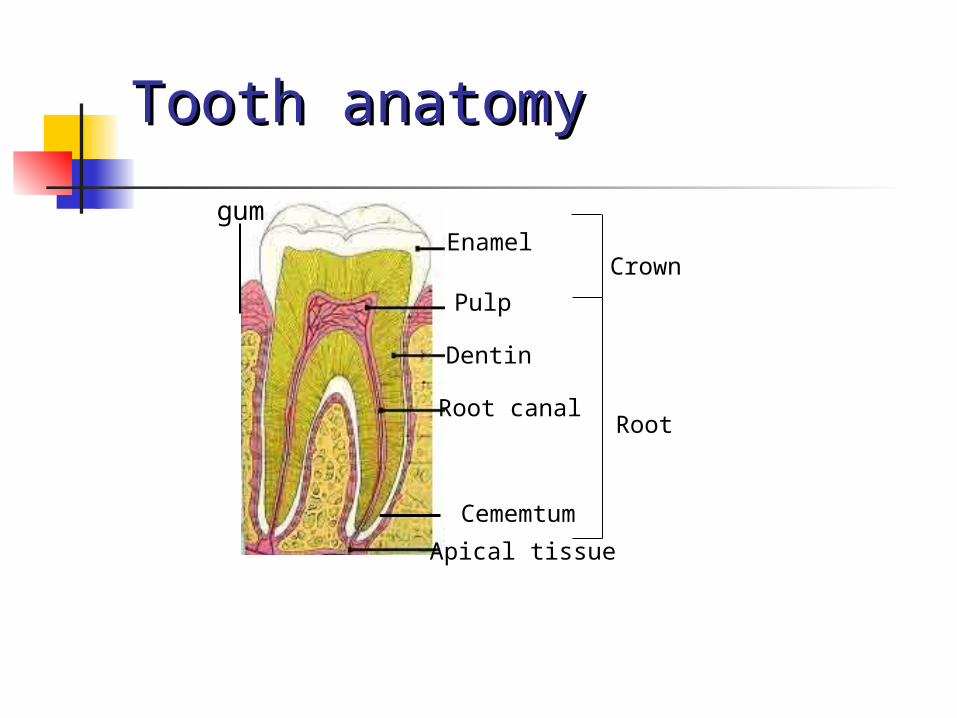
Tooth anatomyTooth anatomy
Root
Enamel
Pulp
Root canal
Cememtum
Apical tissue
Dentin
Crown
gum
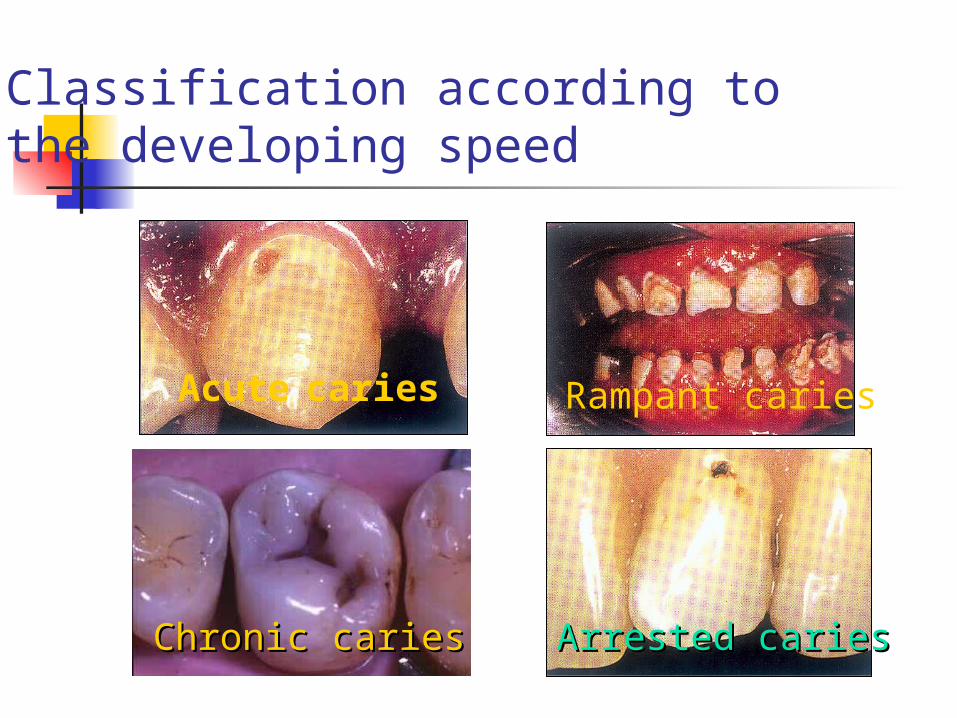
Acute caries
Chronic cariesChronic caries Arrested cariesArrested caries
Rampant caries
Classification according to the developing speed
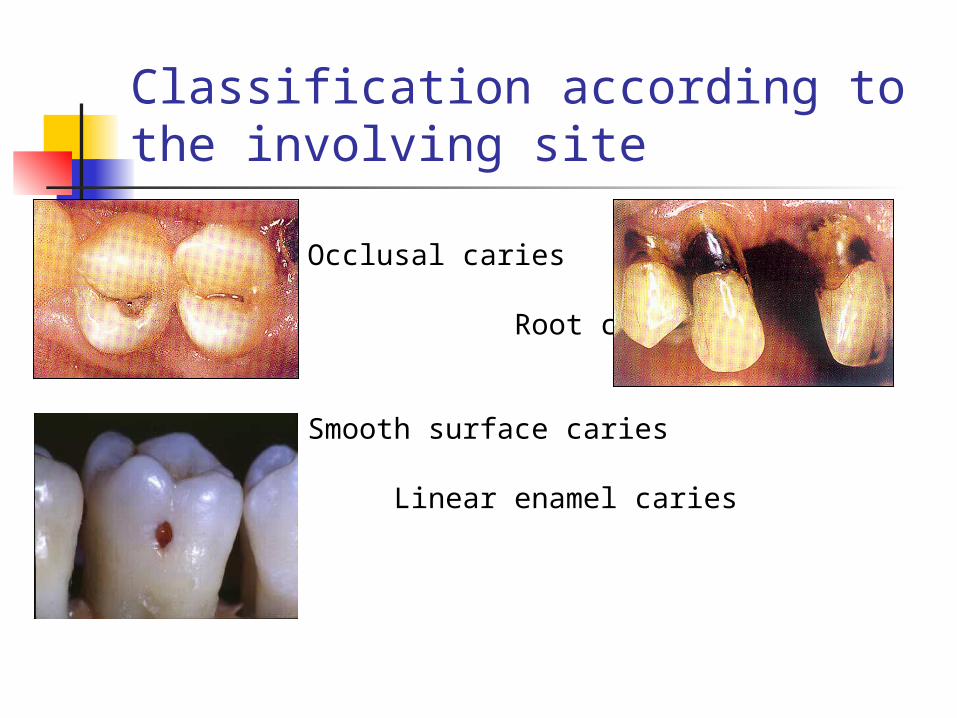
Classification according to the involving site
Occlusal caries
Root caries
Smooth surface caries
Linear enamel caries
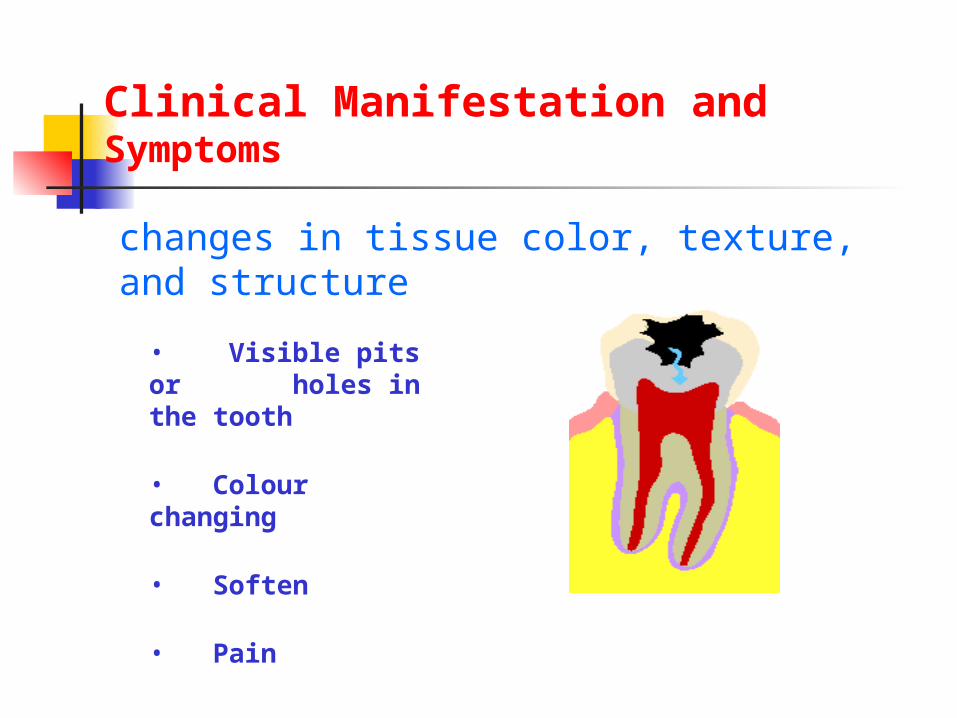
Clinical Manifestation and Symptoms
• Visible pits or holes in the tooth
• Colour changing
• Soften
• Pain
changes in tissue color, texture, and structure
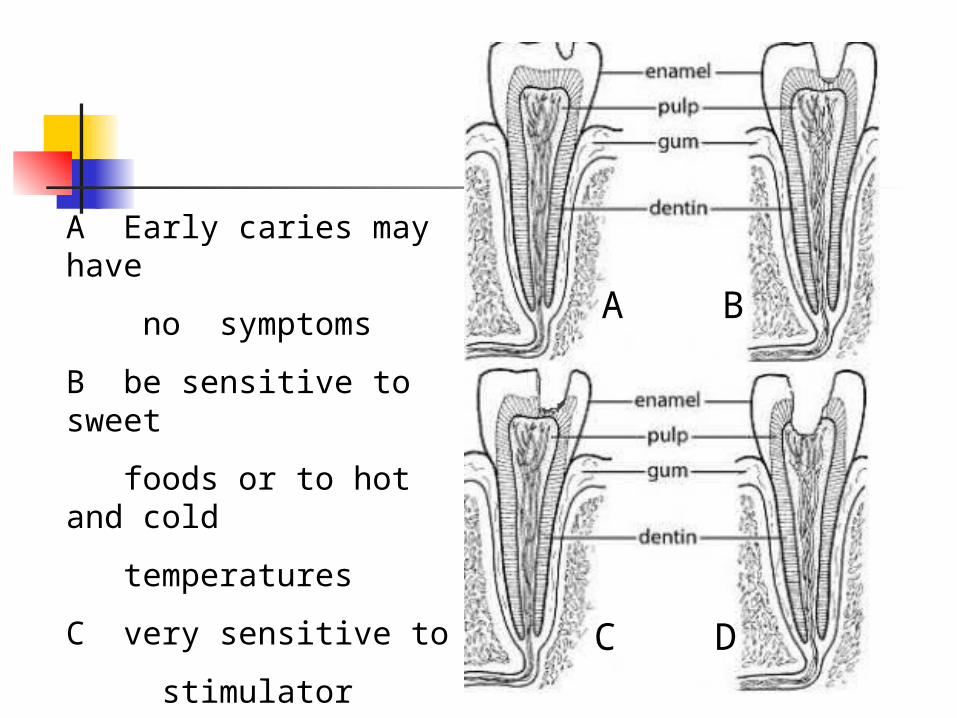
A B
C D
A Early caries may have
no symptoms
B be sensitive to sweet
foods or to hot and cold
temperatures
C very sensitive to
stimulator
D the acute pain
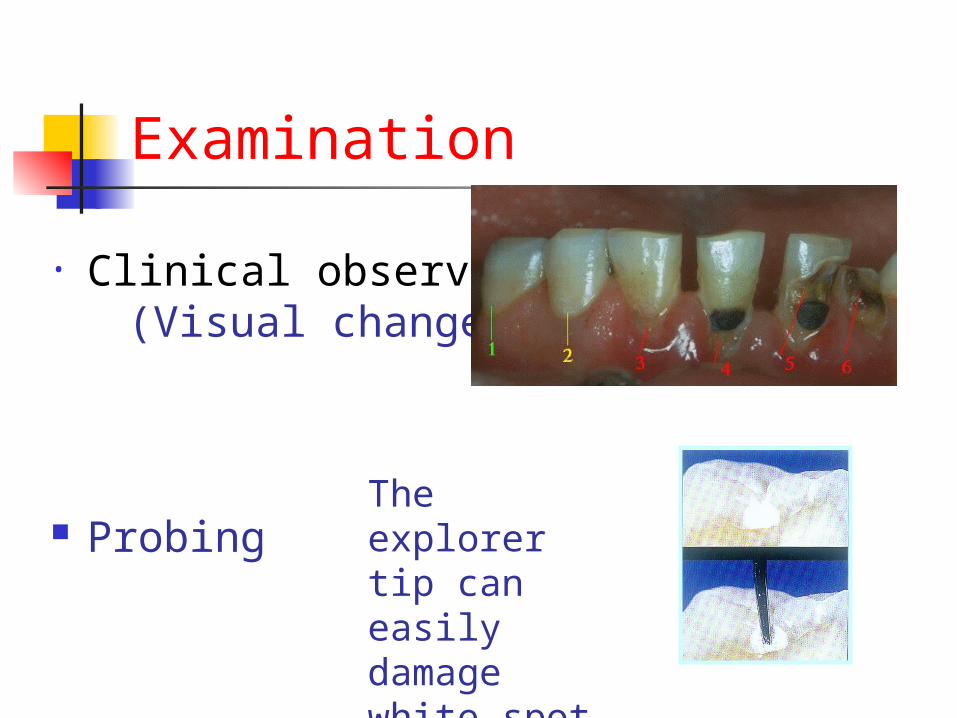
Examination
• Clinical observations (Visual change)
ProbingThe explorer tip can easily damage white spot lesions
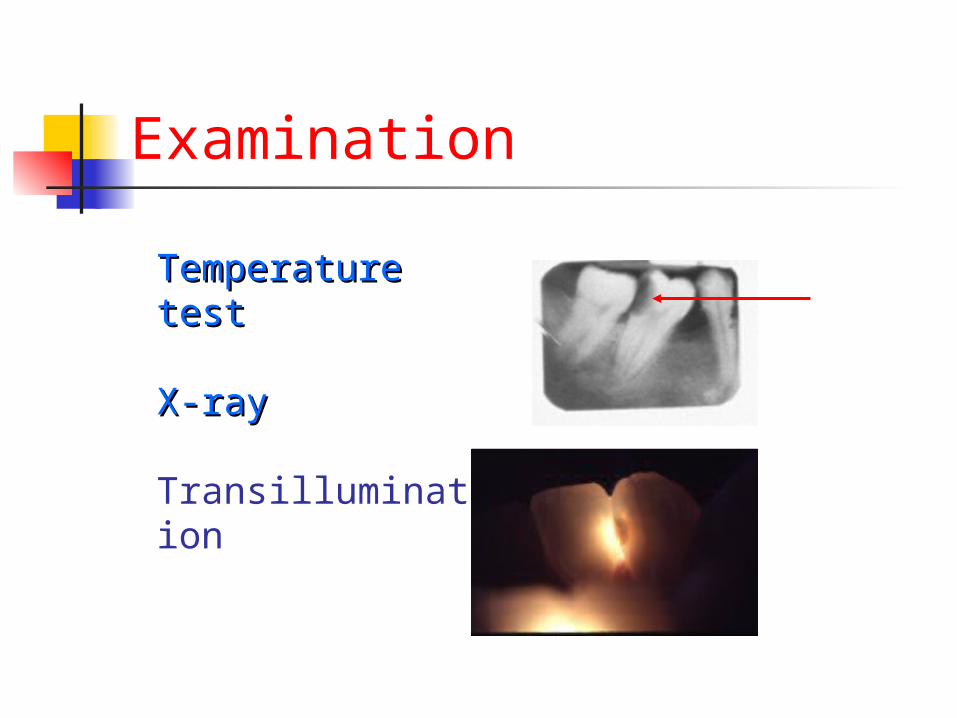
Examination
Temperature Temperature testtest
X-rayX-ray
Transillumination

DiagnosisDiagnosis
Clinical signs visual – color, texture, shape, location, cavitation, Clinical symptoms
Diagnostic test--examination
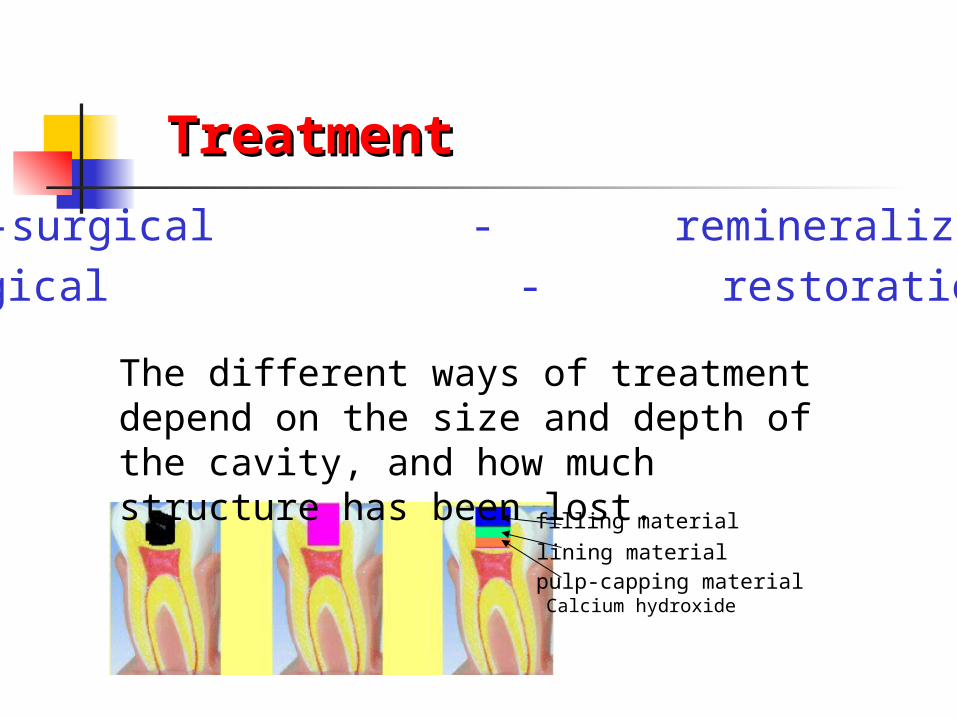
TreatmentTreatment
Non-surgical - remineralization
Surgical - restoration
The different ways of treatment depend on the size and depth of the cavity, and how much structure has been lost.
Calcium hydroxide pulp-capping material lining material filling material
Prevention is the most important for dental caries.

Problem for review
What is the etiology of dental caries?
Be familiar with the definitions of dental caries and classification.
Simply describe clinical manifestation and symptoms of dental caries.
Endodontics
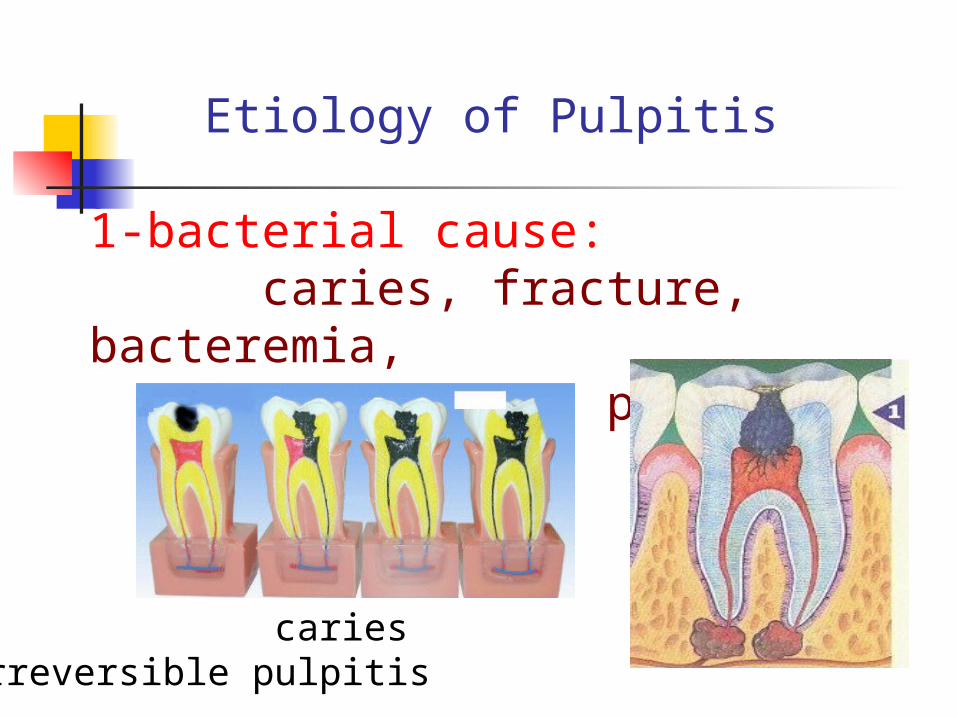
Etiology of Pulpitis
1-bacterial cause: caries, fracture, bacteremia, periodontal pocket
caries irreversible pulpitis
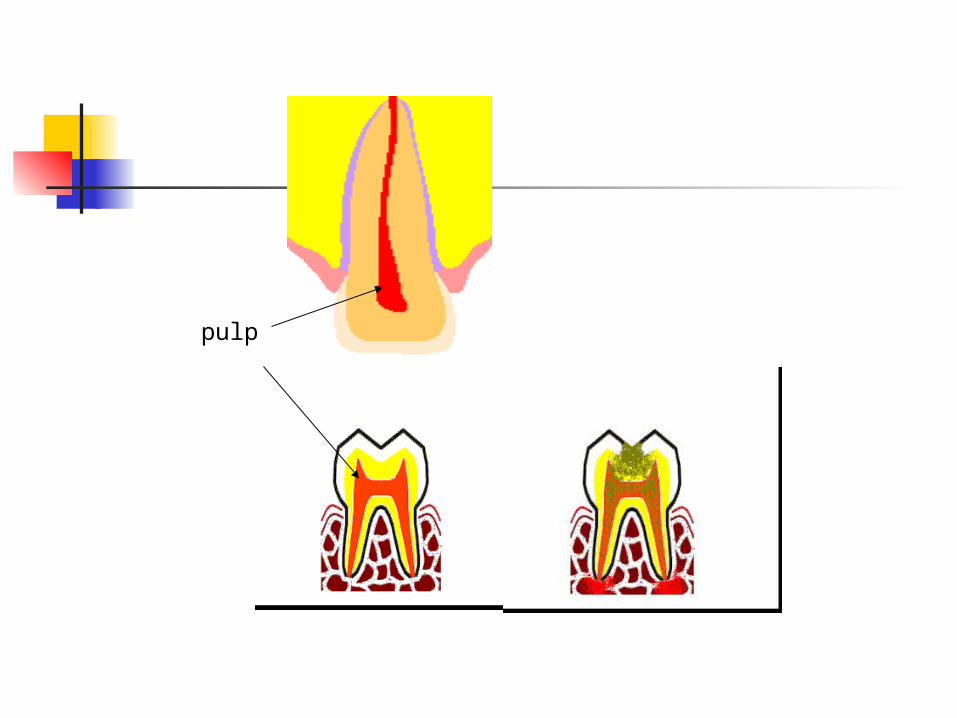
pulp
2-physical cause: sever thermal change (cavity preparation), large metallic restoration
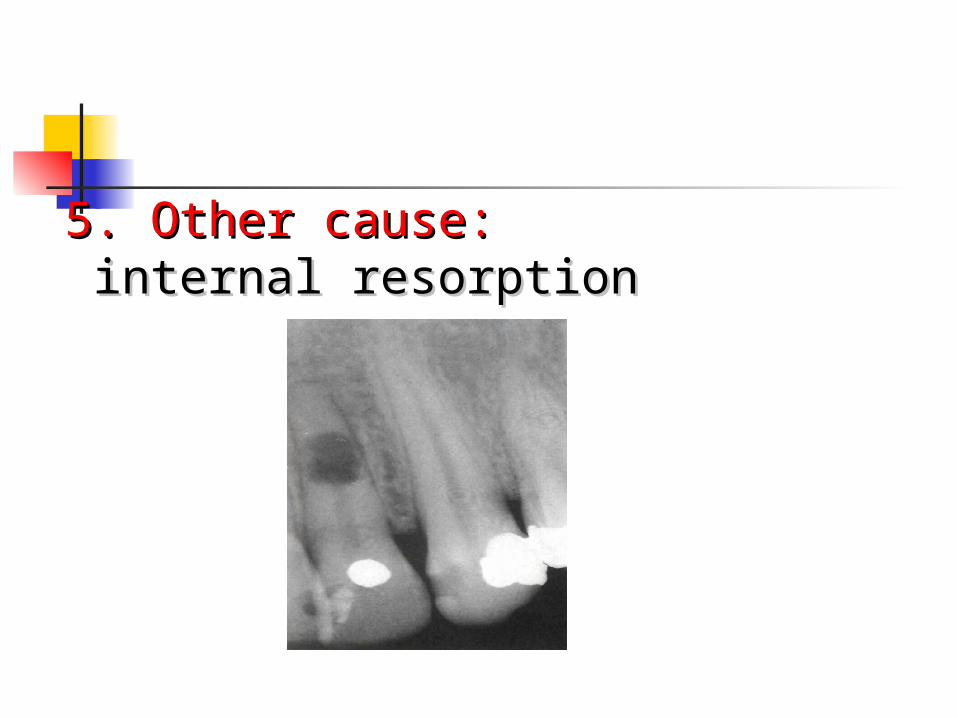
5. Other cause:5. Other cause: internal resorptioninternal resorption
Possible Pulpal Diagnoses
Normal Reversible pulpitis Irreversible pulpitis—acute, chronic, polyp Necrosis Previous endodontic treatment
Reversible pulpitis
Clinically
1. sharp pain & respond to sudden changes in temperature
2. pain disappear as the stimuli removed last less than 20 sec3. easily localized & unaffected by body
position
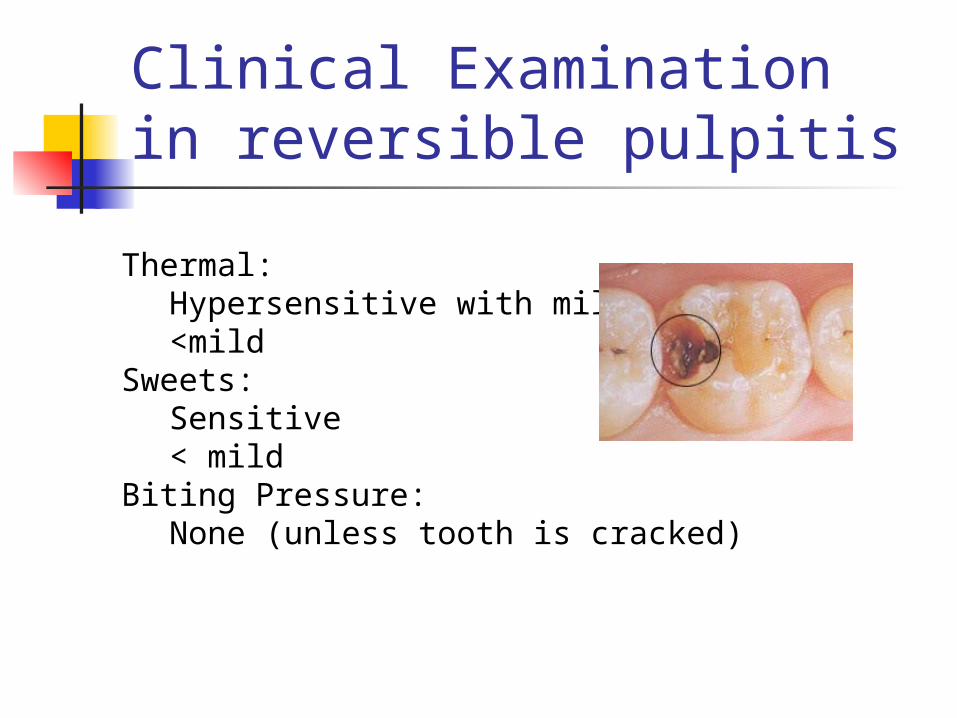
Clinical Examination in reversible pulpitis
Thermal:Hypersensitive with mild pain<mild
Sweets:Sensitive< mild
Biting Pressure:None (unless tooth is cracked)
Treatment of Reversible Pulpitis Remove irritant if present If no pulp exposure: direct restore If pulp exposure:
Carious: initiate RCT Mechanical: >1 mm: initiate RCT <1 mm crown planned: initiate RCT <1 mm: direct cap or RCT
If recent operative or trauma – postpone additional treatment and monitor.
Irreversible Pulpitis
Reversible pulpitis are left untreated.
Symptoms of Irreversible Pulpitis
Thermal: Hypersensitive-moderate to severe
Sweets: Moderately to severely sensitive
Biting Pressure: Usually sensitive in later stages
(periapical symptom)
spontaneous pain: Moderate to severe

DiagnosisIrreversible Pulpitis
Hypersensitive to hot or cold that is prolonged.
A history of spontaneous pain.
Vital or partially vital pulp.
may occur as a sequel of focal reversible pulpitis or occur due to acute exacerbation of chronic pulpitis.
clinically1- big cavity or margin of a restoration 2- sleep pain 3- spontaneous pain 4- pain lasts 5- difficult to localized
Acute pulpitis:
a result of acute pulpitis, or develops as chronic one.Clinically1-spontaneous dull, itching pain2-increased pain threshold (need strong stimuli) due to degeneration of the nerve fibers3- the pain lasts for about 2 h.
Chronic pulpitis
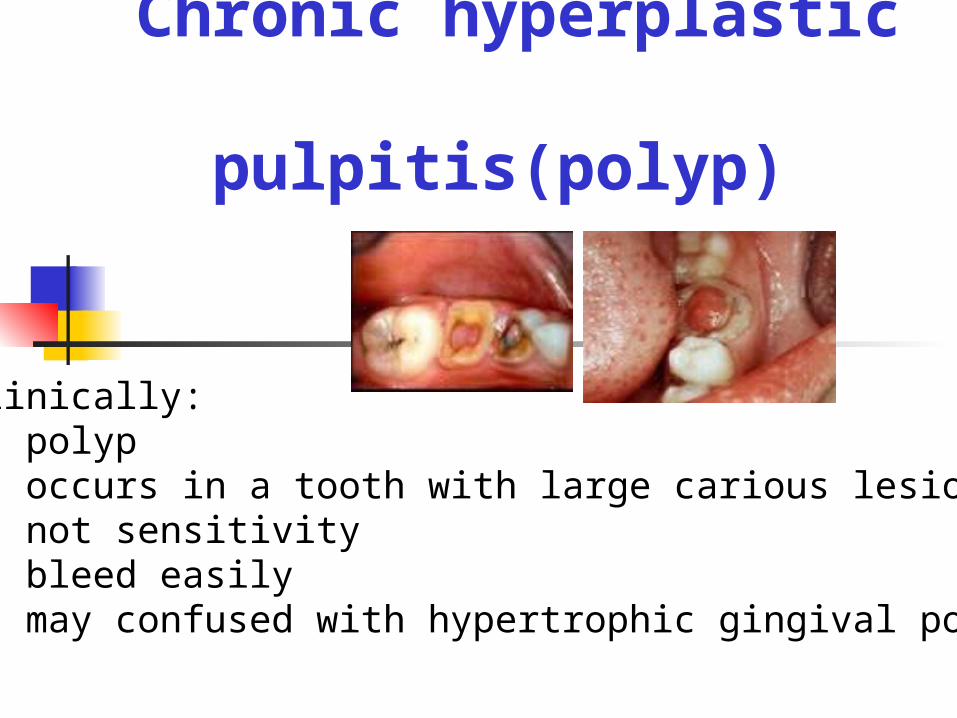
Chronic hyperplastic pulpitis(polyp)
Clinically:1- polyp2- occurs in a tooth with large carious lesion3- not sensitivity4- bleed easily5- may confused with hypertrophic gingival polyp

Treatment of Irreversible Pulpitis
Root canal treatment or extraction
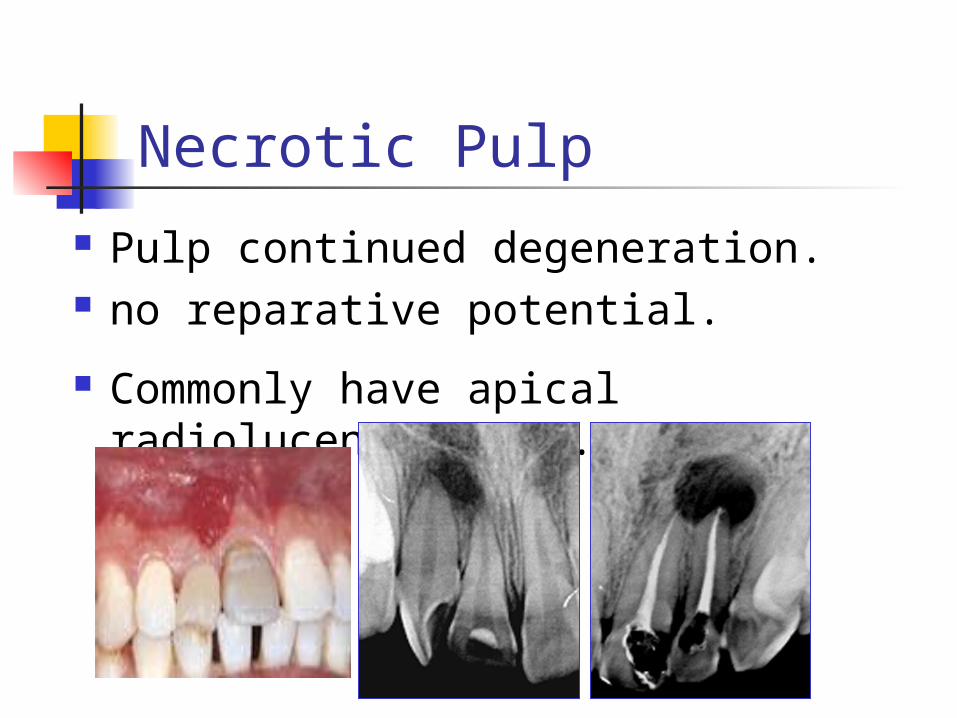
Necrotic Pulp Pulp continued degeneration. no reparative potential.
Commonly have apical radiolucent lesion.
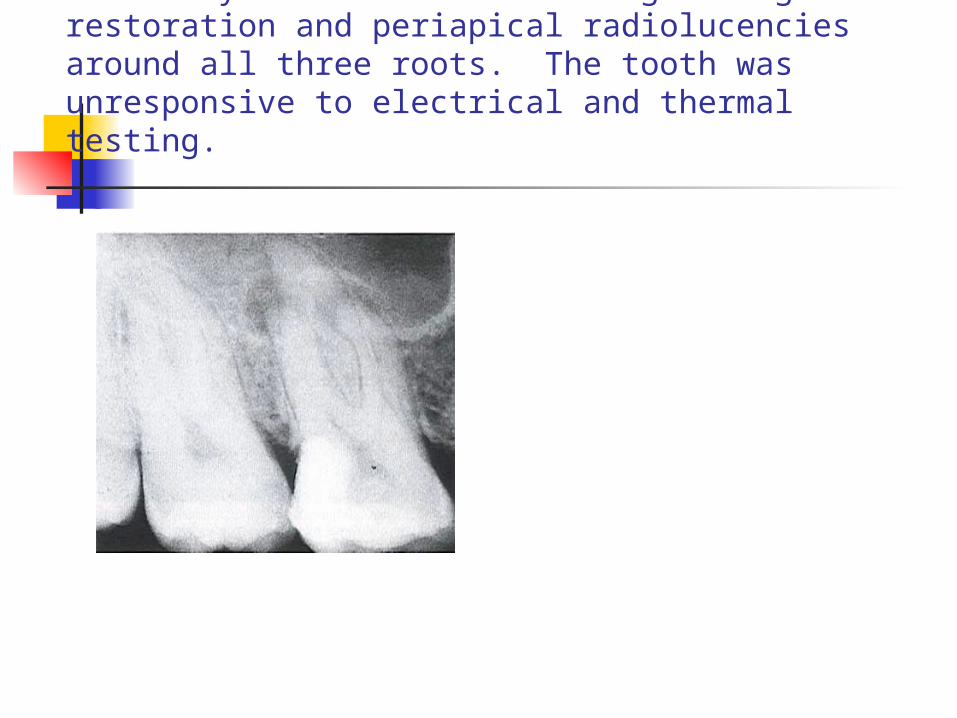
Maxillary first molar with large amalgam restoration and periapical radiolucencies around all three roots. The tooth was unresponsive to electrical and thermal testing.
Symptoms of Necrotic Pulp Thermal:
No response
Sweets: No response
Biting Pressure: Usually moderate to severe pain (not
symptom of necrotic pulp, but rather periapical inflammation)
Moderate to severe spontaneous pain
Diagnosis of Necrotic Pulp
Distinguishing features: No response to cold. No response to EPT.
Caveats Decreased sensitivity Periapical radiolucency is strong but not
conclusive evidence that pulp is necrotic.
Necrotic Pulp(additional considerations)
Antibiotic coverage Pain Management
Occlusal Reduction
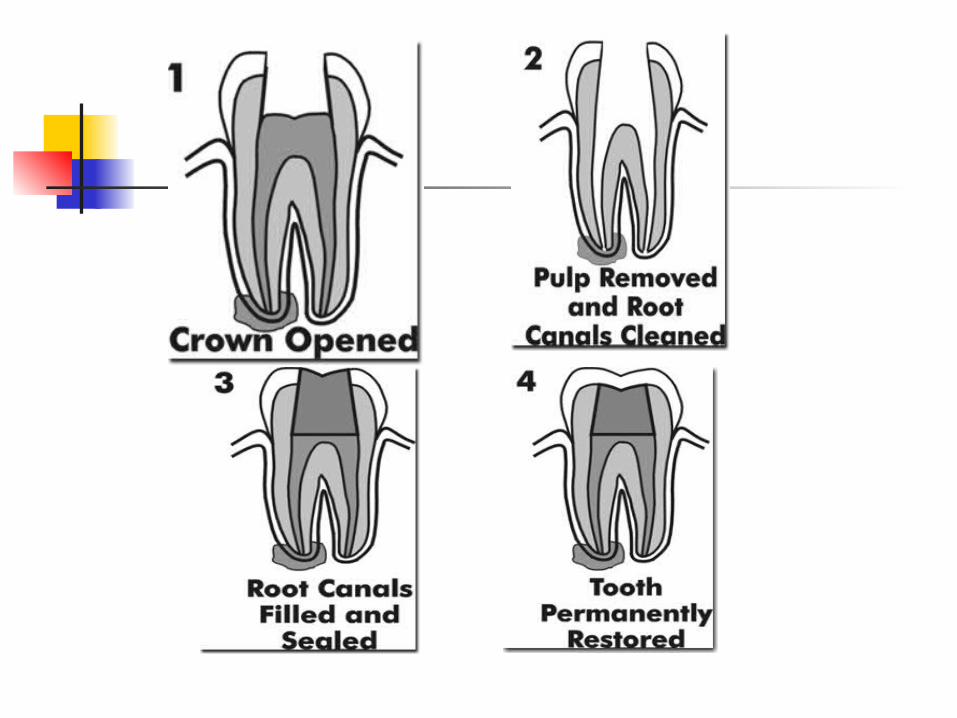
Root Canal Treatment
The procedure involves removing inflamed or damaged tissue from inside a tooth and cleaning, filling and sealing the remaining space, to prevent re-infection.
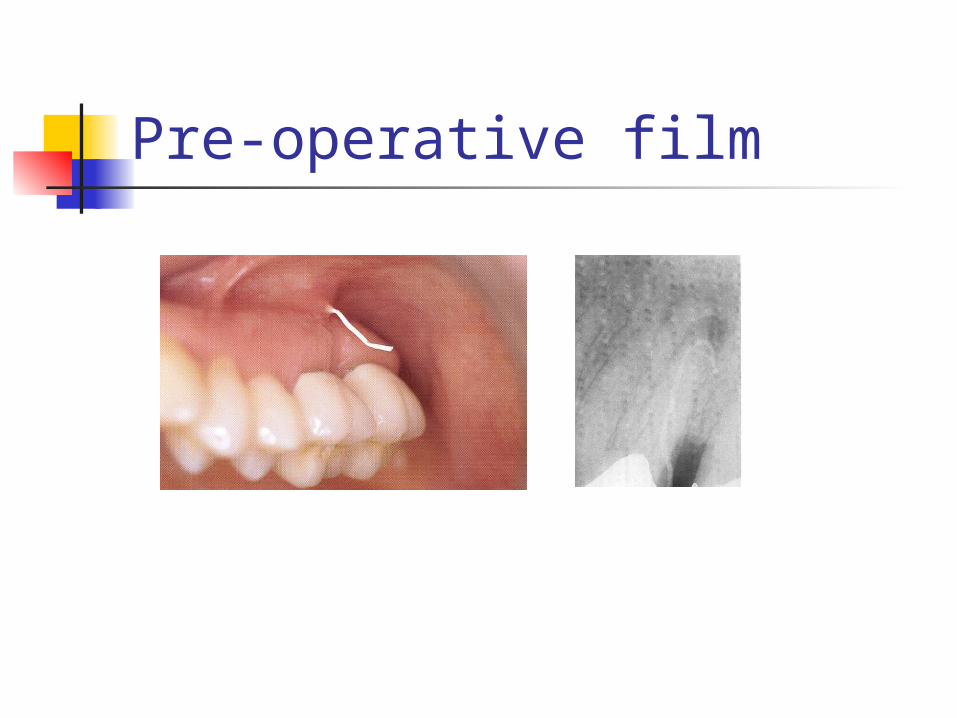
Pre-operative film
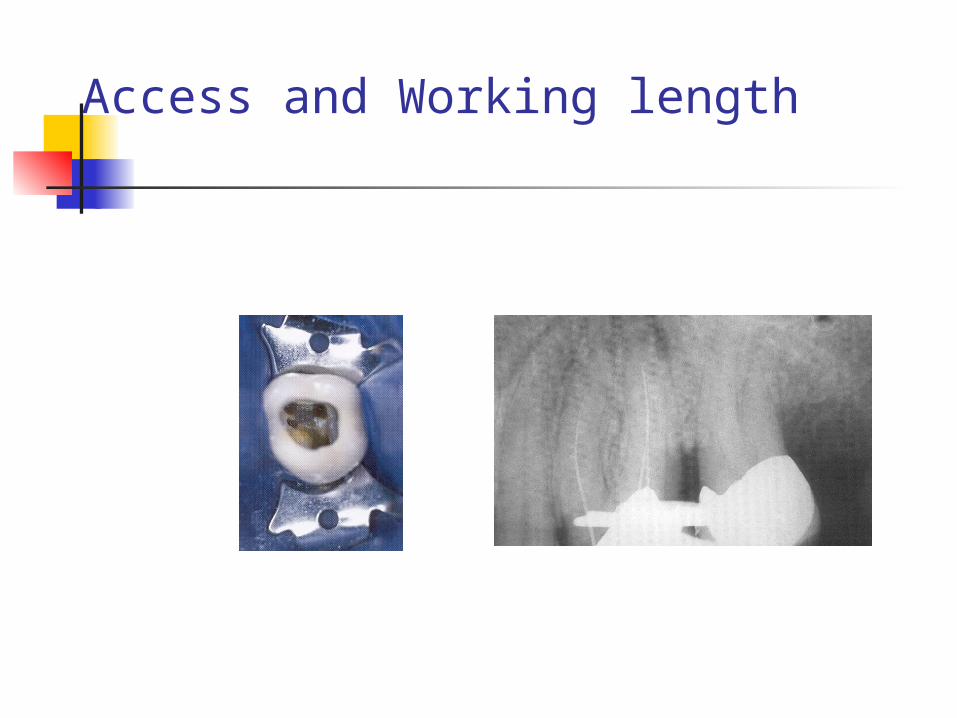
Access and Working length
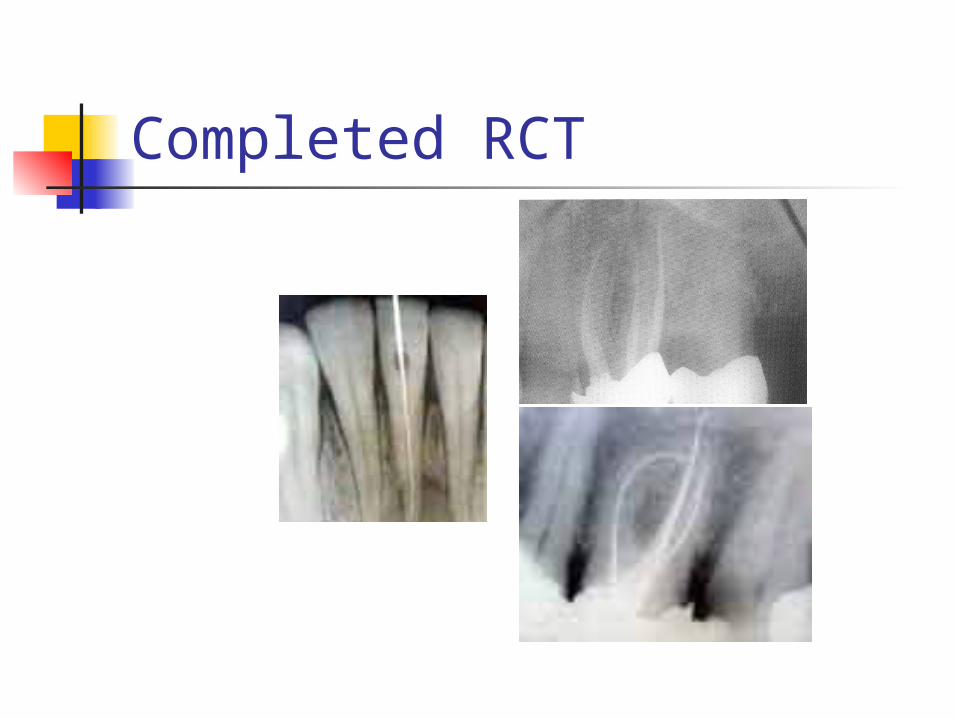
Completed RCT

case
Points you must know:
What is root canal treatment? Simply describe the clinical
manifestation of pulpitis.
The oral manifestation of HIV Infection
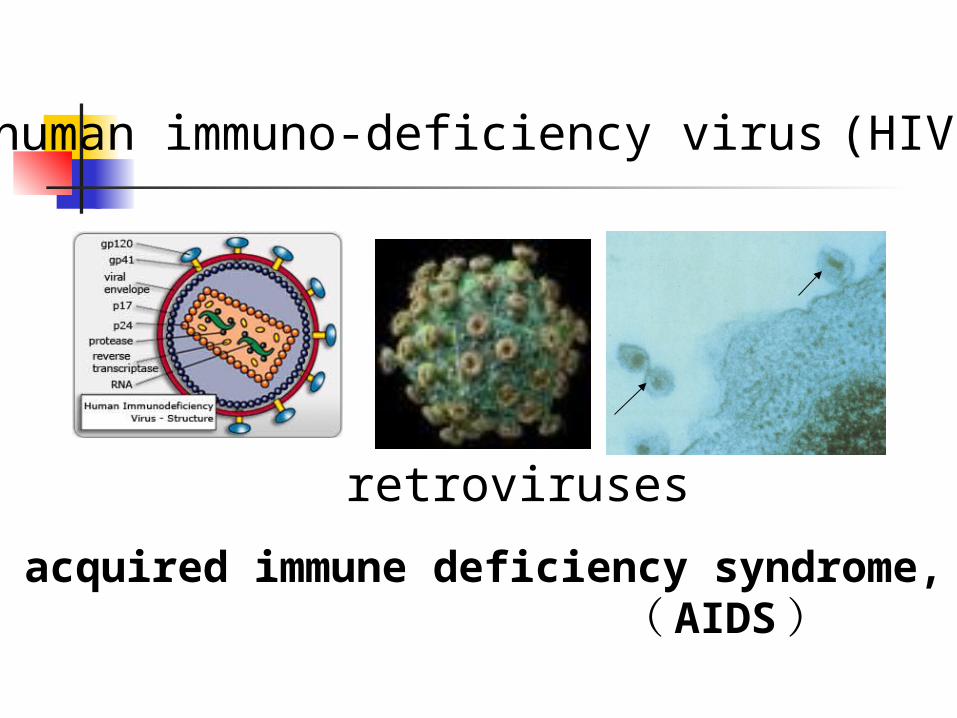
human immuno-deficiency virus (HIV)
retroviruses
acquired immune deficiency syndrome, ( AIDS)
Oral manifestations are often the first clinical feature of HIV infection.
The first AIDS case, worldwide : 1981, AIDS China : 1985, AIDS, Beijing,Argentina Shanghai : 1987, AIDS Hangzhou: 1985, AIDS--hemophila 2009, 1272/236 (HIV/AIDS)
Epidemiology
Oral Manifestations observed in HIV
Fungal Neoplastic Viral Bacterial Other
Fungal Manifestations ----candidiasis
Can manifest in 4 different ways Pseudomembraneous
candidiasis Erythematous candidiasis Hyperplastic candidiasis Angular chilitis
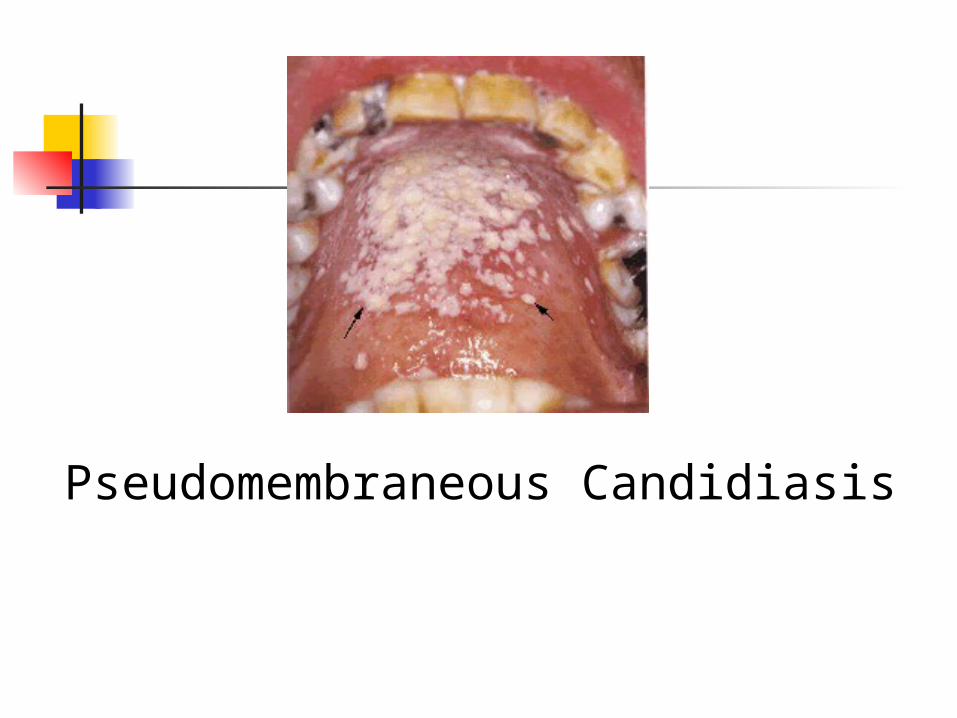
Pseudomembraneous Candidiasis

Erythematous Candidiasis
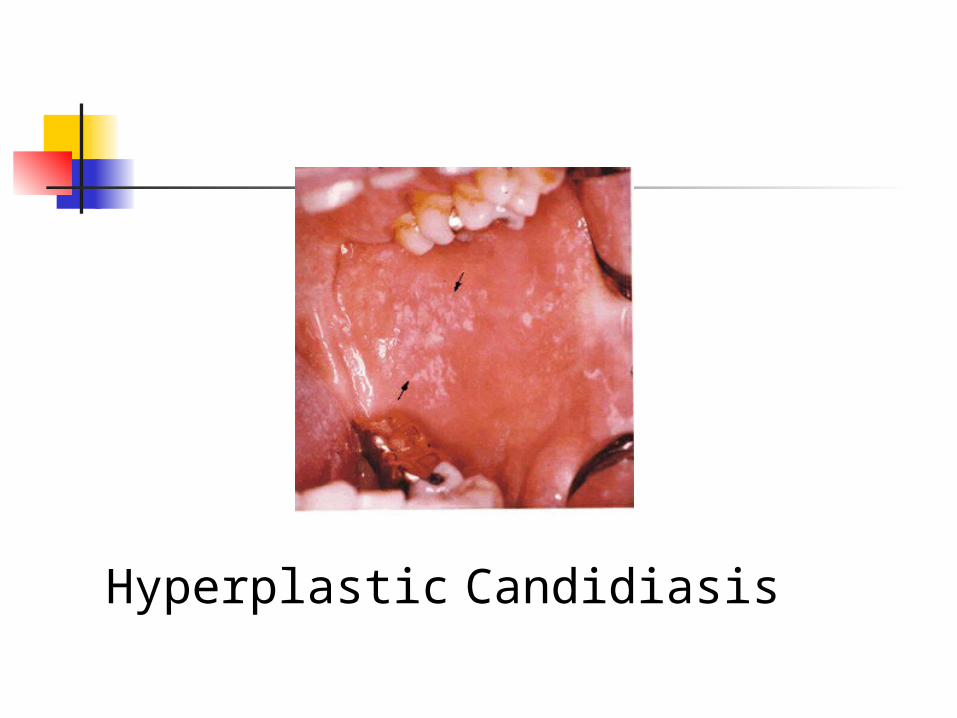
Hyperplastic Candidiasis

Angular chilitis
Neoplastic Oral Manifestations
There are two types of neoplasms associated with oral manifestations in HIV individuals Kaposi’s Sarcoma (KS) Non-Hodgkin’s Lymphoma
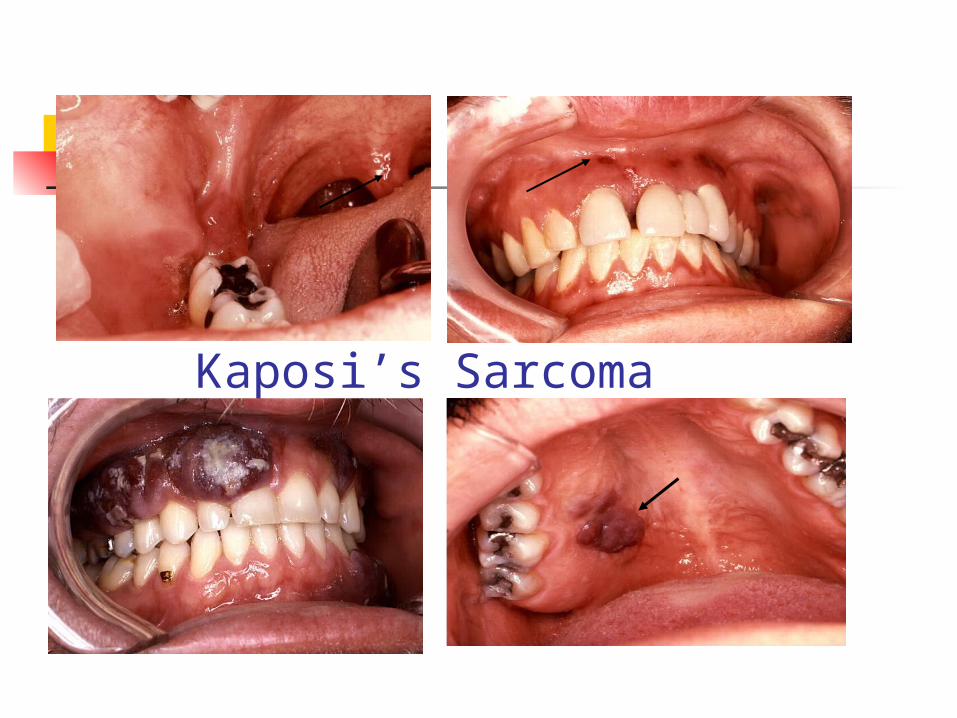
Kaposi’s Sarcoma
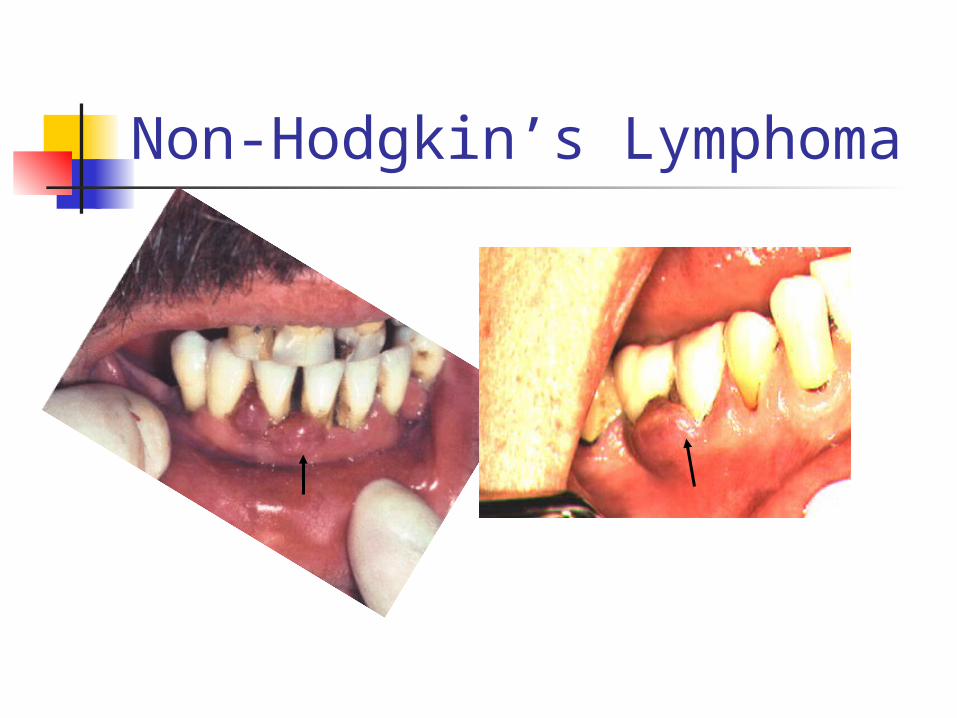
Non-Hodgkin’s Lymphoma
Viral Manifestations
Herpes Simplex Virus (HSV) lesions Herpes Zoster Hairy leukoplakia Cytomegalovirus (CMV) ulcers Human Papillomavirus (HPV)
lesions
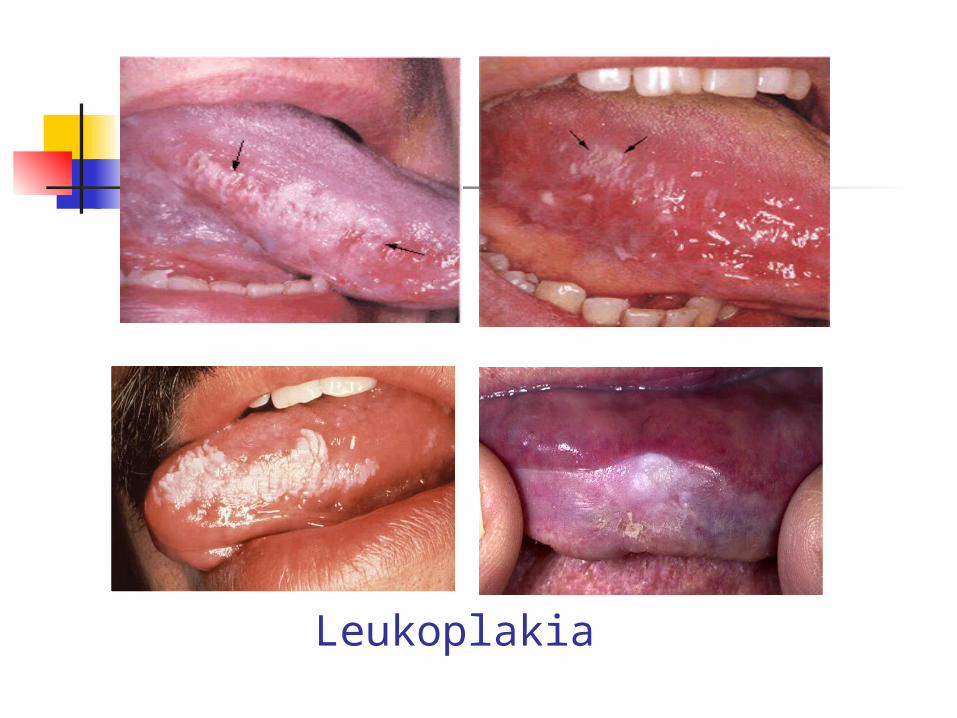
Leukoplakia
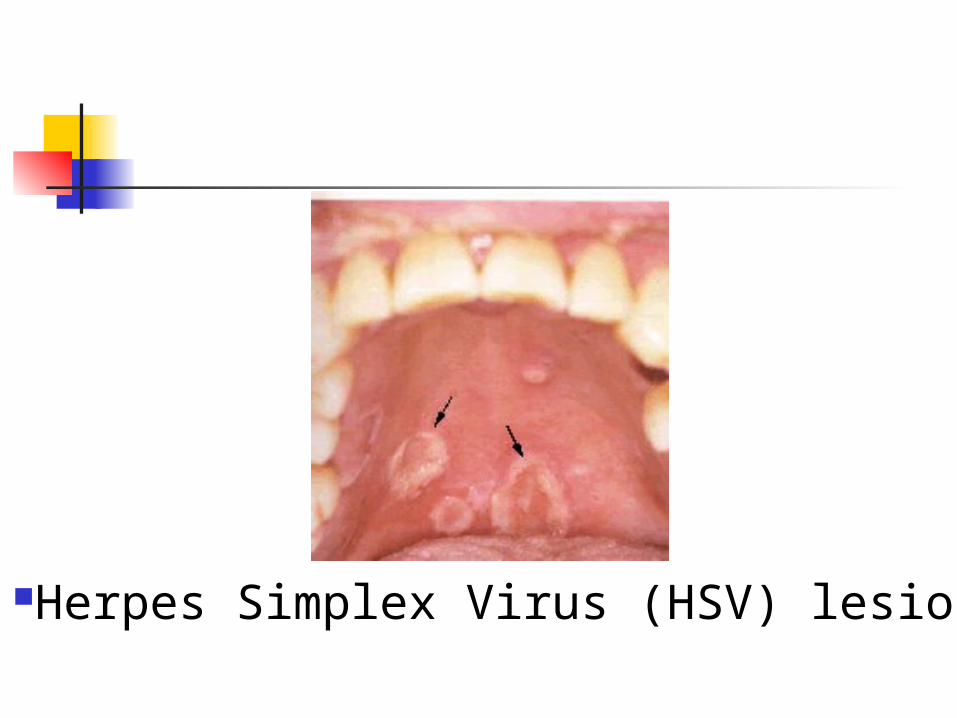
Herpes Simplex Virus (HSV) lesions
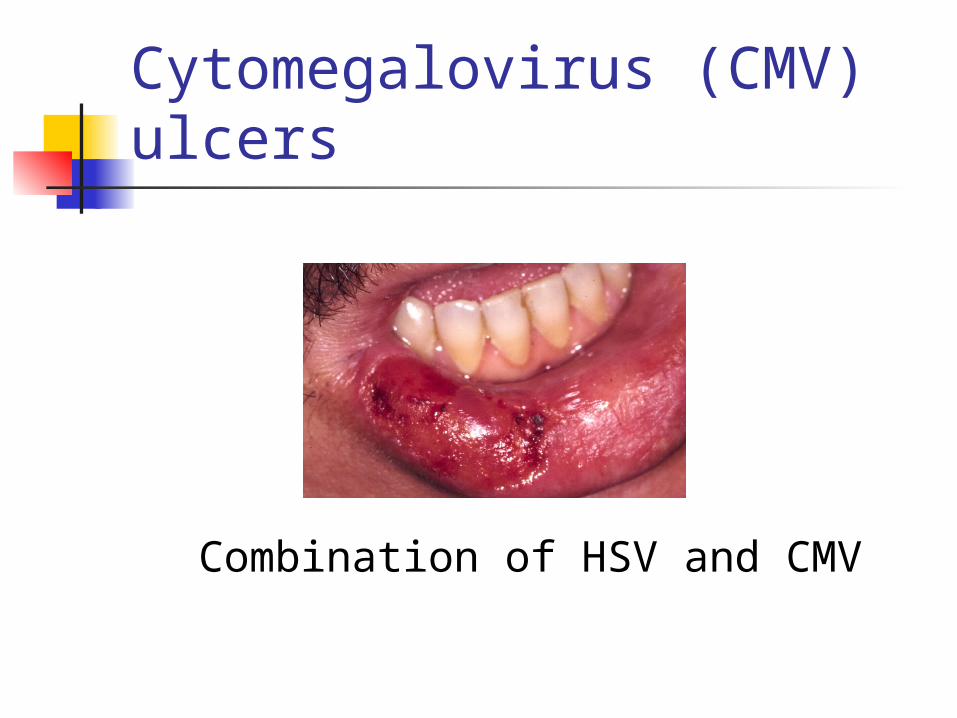
Cytomegalovirus (CMV) ulcers
Combination of HSV and CMV
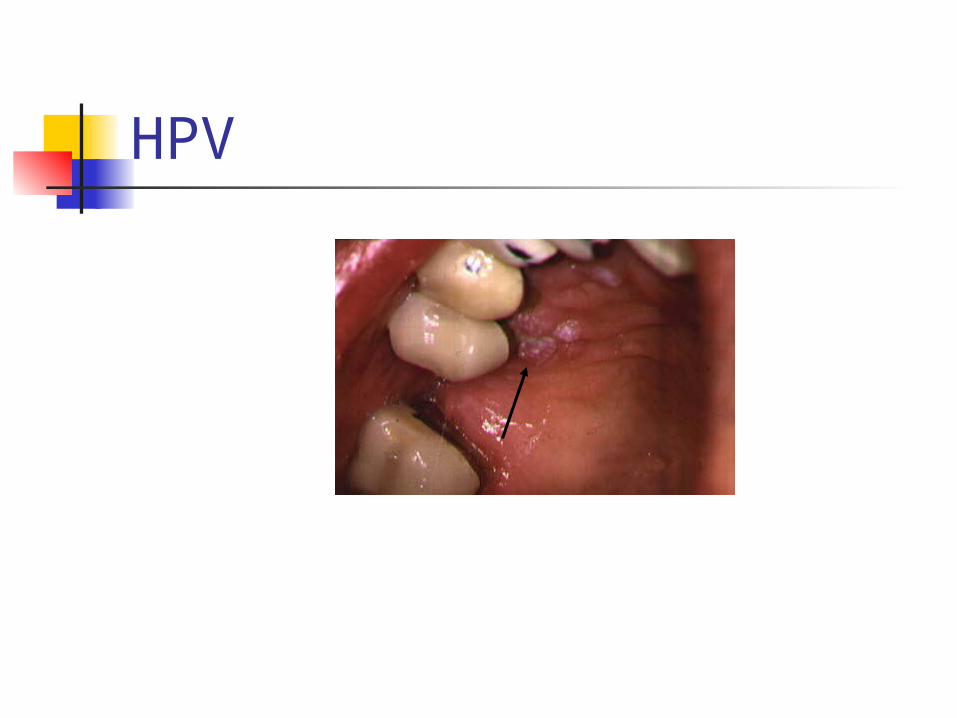
HPV
Bacterial Manifestations
Linear Gingival Erythema Necrotizing Ulcerative PeriodontitisTuberculosis

Linear Gingival Erythema(red-band gingivitis)
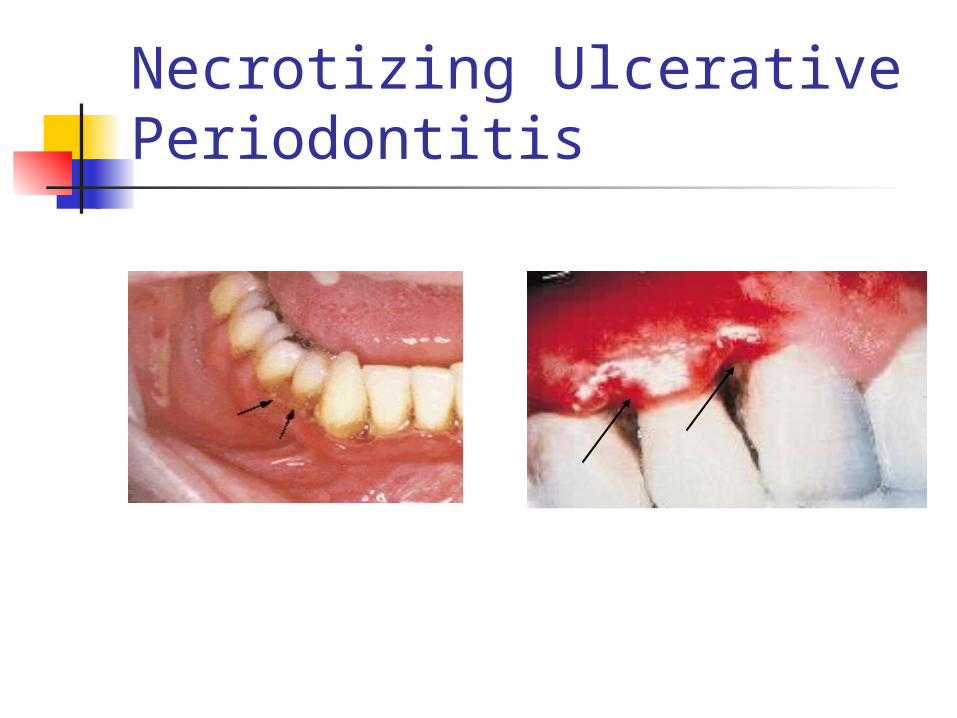
Necrotizing Ulcerative Periodontitis
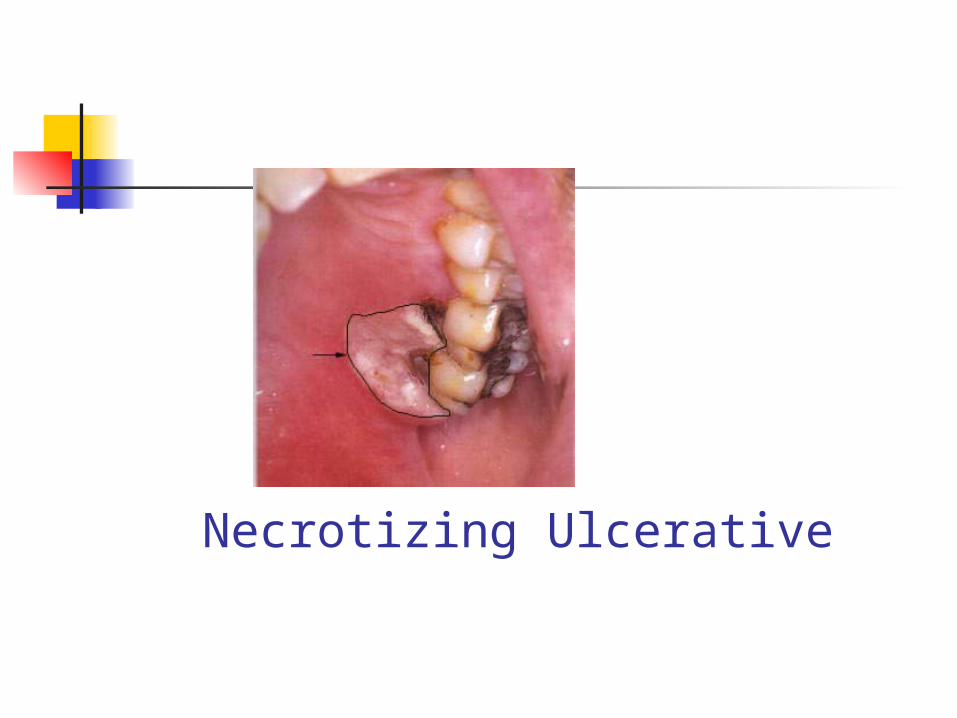
Necrotizing Ulcerative
Tuberculosis
Oral lesions in people with tuberculosis are seen rarely.
They have been reported as ulcers on the tongue secondary to
pulmonary tuberculosis.
Other Oral Manifestations
Aphthous Ulcerations (canker sores) Minor Major
Salivary Gland Disease Xerostomia
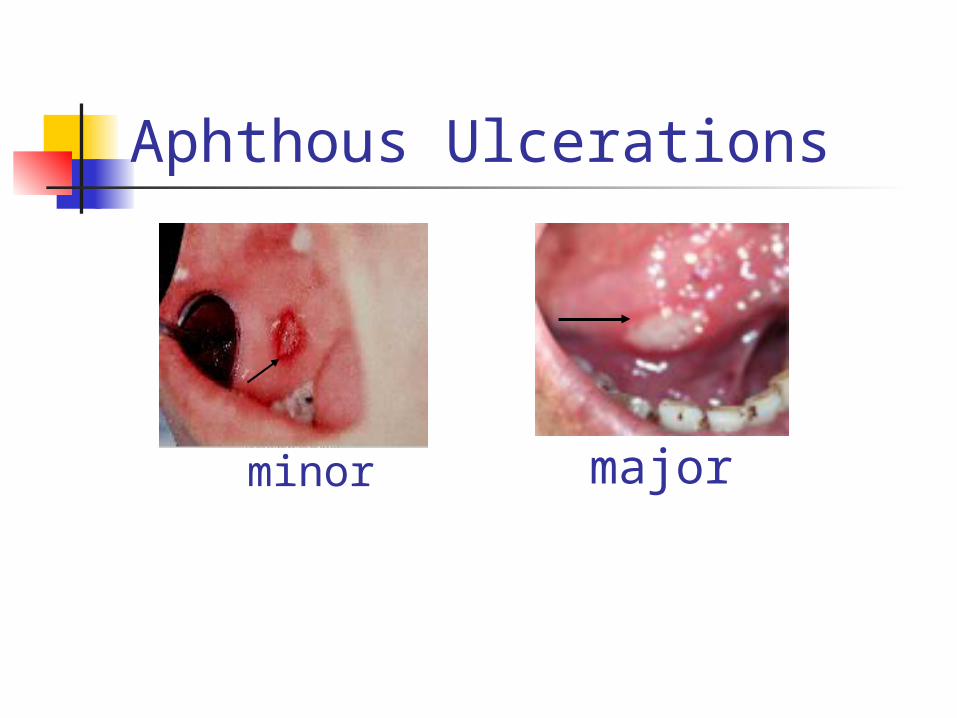
Aphthous Ulcerations
minor major
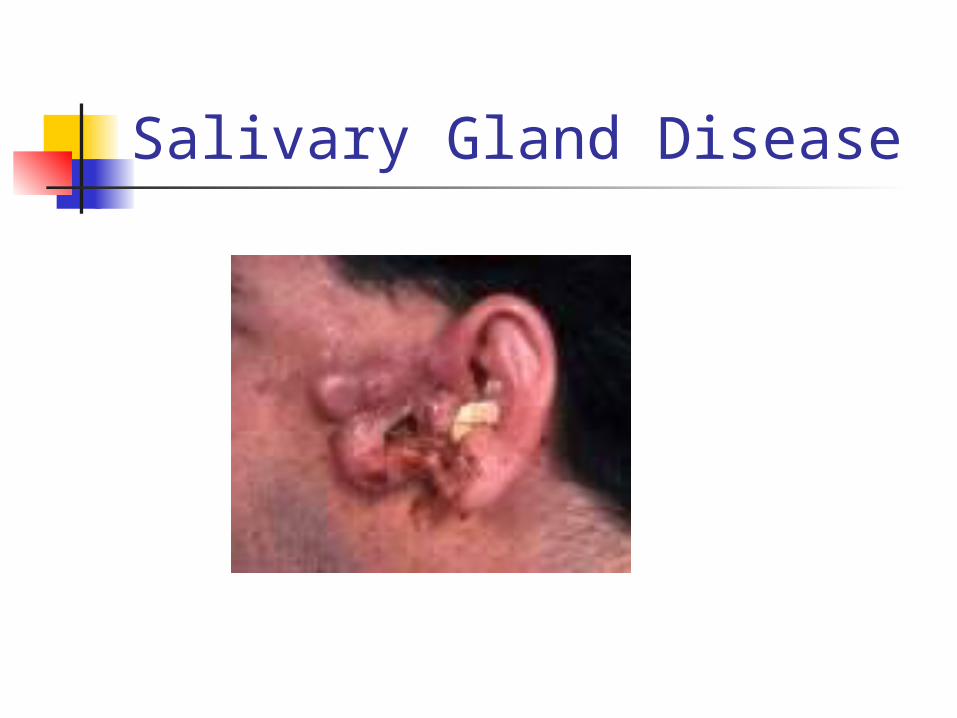
Salivary Gland Disease
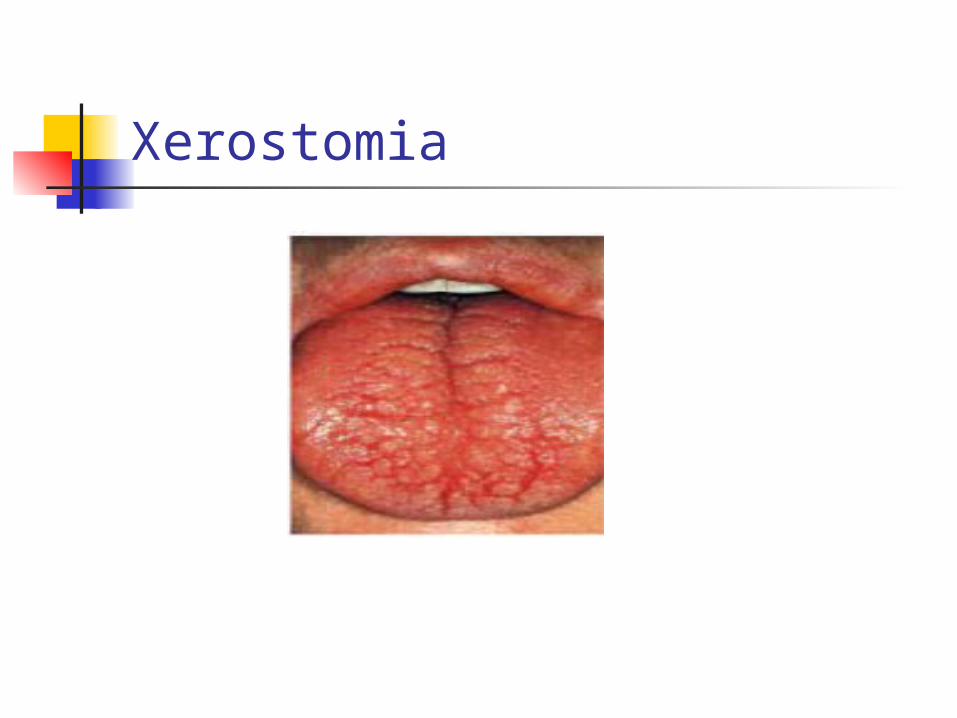
Xerostomia
Conclusions
Lesions or other manifestations in the mouth may be the initial indicator of a persons HIV status or it may indicate a further decrease or worsening of an infected individuals immune system.
You must know: What is the main oral
manifestation of HIV infection? List the four categories of oral
manifestations that may present in HIV
Be familiar with fungal oral manifestation that may present in HIV infected individuals




























