Embed Size (px)
DESCRIPTION
chemical accident prevention and preparedness, lesson learnt
Citation preview
Number 2Dec 2012JRC77996
MAHBulletinSECURITY TECHNOLOGY ASSESSMENT UNITInstitute for the Protection and Security of the Citizen
European Commission21027 Ispra (VA) Italy
http://ipsc.jrc.ec.europa.eu/ Cop
yrig
ht ©
Eur
opea
n U
nion
, 201
2
Summary
In preparing this bulletin, 47 acci-dents in eMARS involving contrac-tor safety issues were studied. Accidents were chosen on the basis that a contract worker was killed or injured or was involved in the accident.
In general, with some exceptions, most accidents took place in the general chemical or petrochemi-cal industries.
Please note:
The accident descriptions and lessons learned are reconstructed from accident reports submitted to the EU’s Major Accident Report-ing System
https://emars.jrc.ec.europa.eu
or
http://emars.jrc.it
as well as other open sources. EMARS consists of over 800 reports of chemical accidents contributed by EU Member States and OECD Countries.
Chemical Accident Prevention & PreparednessLessons Learned Bulletin No. 2
Major accidents involving contractors
operators and government regulators. In future the CAPP Lessons Learned Bulletin will be produced
The aim of the bulletin is to provide insights on lessons learned from accident reported in the European Major Accident Reporting System (eMARS) and other accident sources for both industry
on a semi-annual basis. Each issue of the Bulletin focuses on a particular theme.
Accident 1Petrochemical
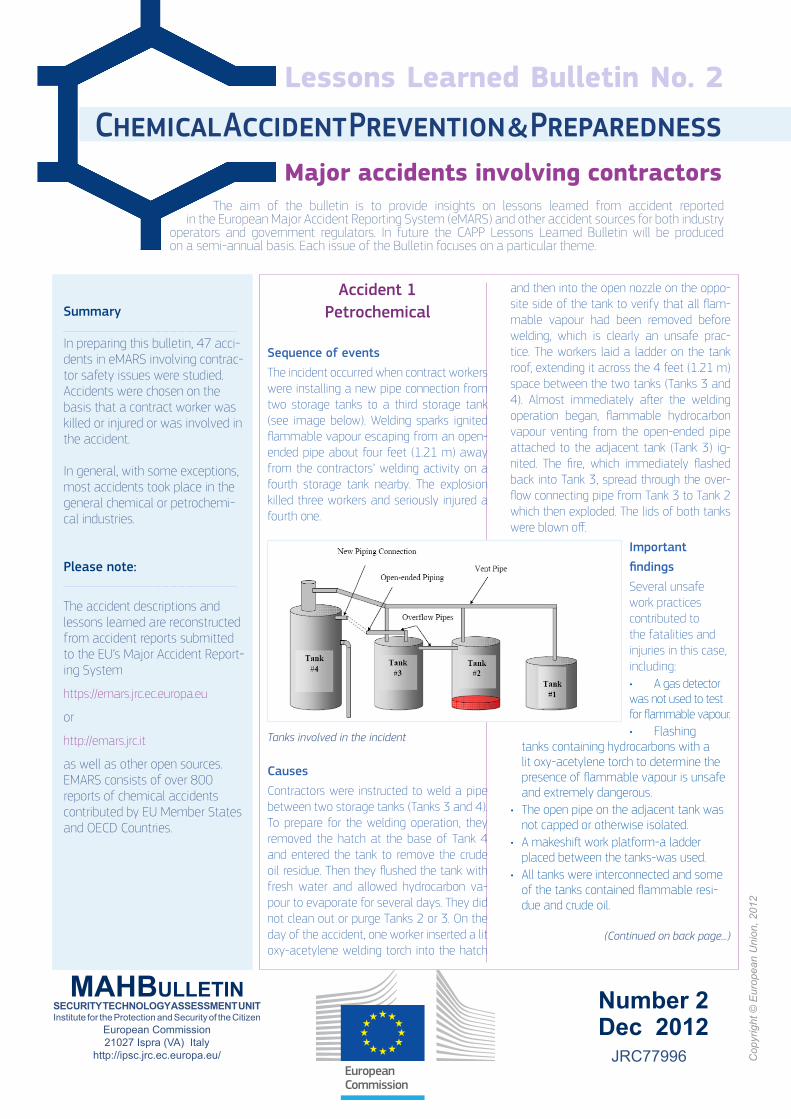
Sequence of events The incident occurred when contract workers were installing a new pipe connection from two storage tanks to a third storage tank (see image below). Welding sparks ignited flammable vapour escaping from an open-ended pipe about four feet (1.21 m) away from the contractors’ welding activity on a fourth storage tank nearby. The explosion killed three workers and seriously injured a fourth one.
Tanks involved in the incident
CausesContractors were instructed to weld a pipe between two storage tanks (Tanks 3 and 4). To prepare for the welding operation, they removed the hatch at the base of Tank 4 and entered the tank to remove the crude oil residue. Then they flushed the tank with fresh water and allowed hydrocarbon va-pour to evaporate for several days. They did not clean out or purge Tanks 2 or 3. On the day of the accident, one worker inserted a lit oxy-acetylene welding torch into the hatch
and then into the open nozzle on the oppo-site side of the tank to verify that all flam-mable vapour had been removed before welding, which is clearly an unsafe prac-tice. The workers laid a ladder on the tank roof, extending it across the 4 feet (1.21 m) space between the two tanks (Tanks 3 and 4). Almost immediately after the welding operation began, flammable hydrocarbon vapour venting from the open-ended pipe attached to the adjacent tank (Tank 3) ig-nited. The fire, which immediately flashed back into Tank 3, spread through the over-flow connecting pipe from Tank 3 to Tank 2 which then exploded. The lids of both tanks were blown off.
ImportantfindingsSeveral unsafe work practices contributed to the fatalities and injuries in this case, including:• A gas detector was not used to test for flammable vapour.• Flashing
tanks containing hydrocarbons with a lit oxy-acetylene torch to determine the presence of flammable vapour is unsafe and extremely dangerous.
• The open pipe on the adjacent tank was not capped or otherwise isolated.
• A makeshift work platform-a ladder placed between the tanks-was used.
• All tanks were interconnected and some of the tanks contained flammable resi-due and crude oil.
(Continued on back page...)
Accident 2 Coke production
Sequence of eventsDuring the welding of a pipeline of a tank containing potassium carbonate solution sat-urated with hydrogen sulphide an explosion occurred. The explosion broke off the tank’s lid which subsequently leaned over to the side. One worker was thrown by the force of the explosion out of the tank’s tray, fell to the ground and died. The second worker was also thrown off the tray but onto technical pipe-lines. He survived but was seriously injured. The accident occurred in the coal derivatives unit in the area of the potassium carbonate recovery installation and in the vicinity of coke gas condenser room. The employees in-volved in the accident worked for a company which performed contract renovation works.
Causes The major cause of the accident was an ex-plosion inside the tank which occurred when flammable gas (hydrogen sulphide) inside the tank was ignited by sparks (that entered the tank through the open probe). The spark-ing occurred as a result of welding activities above the tank..
Important findings• Neither the operator nor contractors ap-
peared to have taken appropriate safety precautions.
• Welding activities were performed without a formal written permission for works with the use of open fire on the operating facility.
• The tank contents were not sufficiently isolat-ed from the pipeline before the work began.
• Additionally, it appeared that safety mea-sures used for working on elevated surfaces were not appropriate.
Lessons Learned• Access to the work area should not be per-
mitted until hazards in the work area have been identified and controlled. Documenta-tion of building and construction works should be reviewed periodically for this purpose.
• Instructions for renovation works should inform contractors of what potential haz-ards could exist and the procedures in place to minimise them Moreover, the op-erator should make sure that contractors comply with the safety regulations and renovation procedures.
[EMARS Accident # 707. See also EMARS Ac-cidents # 775 and 600]
Accident 3 General chemicals manufacture
Sequence of eventsA fire occurred in and around the area of a factory which manufactured polyurethane resins and moulded them into car seat cush-ions. Contractors were working during shut down to remove redundant pipework in fac-tory area using oxy-acetylene torch. Sparks from hot work ignited combustible material in the area. At approximately 09.15 am the contractors noticed flames. Employees in the area sounded the fire alarm at 09.17 am. At approximately 09.20 am a gas cylinder ex-ploded and flames shot through the roof of the building. All personnel were evacuated to an area some 100 metres from the factory perimeter. No sprinkler system was installed in the establishment although combustible ma-terials were present, including a wooden roof. Fire spread to the process and manufacturing area resulting in the subsequent destruction of the entire factory. There were no on-site ca-sualties or off-site effects reported.
CausesSparks from a cutting operation ignited combustible material. Hot work was per-formed in an area from which combustible materials had not been excluded.
Important findings• An inadequate permit to work system al-
lowed hot work to be carried out in area from which combustible materials had not been excluded. It is unlikely that a thorough hazard analysis was conducted prior to the hot working taking place.
• The fire protection measures applied by the facility were not adequate for the produc-tion and handling of polyurethane foams. Standard fire protection norms for commer-cial buildings were not followed either, e.g., there was no sprinkler system installed.
Lessons Learned• Authorities should use all means to en-
force relevant fire protection norms in commercial establishments. There should be specific fire protection standards ap-plied to activities where dangerous sub-stances are involved.
• Hot work requires implementation of a robust permit to work system that is fully audited.
[EMARS Accident # 527. See also EMARS Accident # 400.]
TIPS
Do not work on a makeshift work platform!
Contractor safety includes look-ing at hazards in the area around where work is taking place, for example, dangerous substances that are nearby, or equipment and infrastructure that are not directly involved in the job.
If written instructions or sign-posting are provided, they should be clear and in a language un-derstood by the contractors.
The operator must pay atten-tion to the possibility that third party workers might change the system when it is clearly not al-lowed. Therefore a continuous presence of a supervisor or a spot check at designated inter-vals is recommended when of certain hazards are present, such as those associated with toxic releases.
A permit-to-work should include not only a list of the actions that are authorised but also those that are explicitly NOT autho-rised. This measure is particu-larly important for avoiding ad hoc changes that could increase accident risks during temporary shut down or maintenance work.
Chemical Accident Prevention & Preparedness
Major accidents involving contractors
Accident 4 Petrochemical
Sequence of eventsThe alkylation unit was going into shut down. Two contractors were fixing a copper tube to a T-piece of a drain. During the work they turned the T-piece over 90°. Due to this fact a valve on the T-piece was accidentally opened and an amount of hydrogen fluoride (HF) was released. One of the contractors was very seri-ously injured. His eyes, nose and mouth were burned and he inhaled HF fumes, which caused internal injuries to them. The second person only had small injuries around his mouth.
CausesBecause the alkylation unit was shut down, the biggest equip-ment was already emptied and the installation was cleaned with nitrogen. Then it was decided to drain the unit to remove all flu-ids left. The drain consisted of two valves and a blind flange. The blind flange was removed and replaced by a T-piece consisting of a manometer and a small valve. The T-piece was mounted in a horizontal way. A permit was written for two contractors to add a copper tube to the small valve on the T-piece. Because it was not easy to work with the T-piece mounted horizontally they decided to rotate the T-piece. While rotating the piece, the handle of the small valve touched a pipeline which opened the valve and 360ml HF was released.
Important findingsThe T-piece on the drain was a temporary piece only installed for the shutdown. There was no standard in the company to which temporary pieces had to comply. The T-piece used screw thread which made it possible to turn the T-piece. The accident showed that a standard for temporary pieces must be drawn up.In the company it was seen as normal that the manual valves in the line on which the T-piece was fitted had a small internal leak. So in the work permit protective clothing should have been specified for working on this line since they should have antici-pated that HF would build up between the fixed (leaking) valves and the quarter turn valve on the temporary T-piece. A quarter turn valve is easily manipulated accidently, certainly while doing mechanical work in the immediate vicinity.
Lessons LearnedThe operator should ensure that all contractors understand the hazards associated with a temporary workplace and the process in case of emergency in requiring them to follow a training prior to their work. Some types of equipment are designed or replaced in a way that reduces human error. These equipment should be installed when a process This is particularly important in the case of contractors who are less familiar with the way equip-ment works than employees of the site.
More information: http://www.hseni.gov.uk/improving_maintenance_-_a_guide_to_reducing_human_error.pdf
[EMARS Accident # 30. See also EMARS Accidents # 775 and 600.]
Accident 5 Petrochemical
Sequence of eventsA temporary employee, who had only been working in the com-pany since a short period of time, first of all closed the valve under supervision of his mentor. After a while the temporary em-ployee returned without his mentor. Since he had doubts if the valve was really closed he turned it a second time. At that time he thought he closed it, but in fact with this action he opened the valve again, activating the alarm. He then decided to turn the valve a third time. At this point the valve was then closed. What he did not know was that there was always a (minor) delay in the decrease of pressure in the pipeline because of which the alarm bells con-tinue to go off for a short time. Note that the pipeline was some hundred meters long and there was still some pressure on the pipe immediately after changes in the valves. In other words there was always a certain delay when closing the pipe due to which the pressure appeared high in a small part of the pipeline. One had to take this delay into account. He then asked for assis-tance of the mentor. (The mentor had not been present when the temporary employee had opened and closed the valve a couple of times.) They decided to turn the valve a fourth time thinking it would close it, but actually opened it again. Significantly, they also turned off the alarm at this time, without taking into account the fact that the alarm had only gone off because of the delay in the decrease in pressure in the pipe line. To sum up, the status of the valve when they left it was ‘open’ and the alarm bells did were not triggered since they had been turned off. As a result, 50 tonnes of butane escaped from the system causing material loss. No injuries occurred but ap-proximately 55 people were at risk from the release of a large amount of a flammable substance but no fire occurred.
CausesThe unclear markings on the valve caused confusion in regard to whether the valve was open or shut. The operators should also not have turned off the alarm.
Important findings The question is, why did this confusion about opening or clos-ing the valve occur? Two years prior to this accident a similar accident had happened. The correction that was applied after that accident was that a warning sign with the word ‘open’ was placed over the valve (in other words it covered the valve). How-ever, in a closed situation the warning sign showed the word ‘open’ and in an open situation the sign showed the word ‘open’ as well. The only difference was that in an open situation the word ‘open’ was read vertically and in a closed situation hori-zontally. Hence, the improvement/correction that was made due to the accident that had happened 2 years before caused even more confusion for someone that did not know the practical reason behind it. This ‘opening and closing’ should have been noticed in the control room, but did not result in any action since the alarm had been turned off.
(Continued on back page...)
Lessons Learned Bulletin No. 2
Who are contractors?
Contractors are usually those who are involved in the installation or maintenance of equipment and systems at a facility and not employees of the dangerous establish-ment. Their work usually associated with the regular/irregular maintenance, which is not part of the normal routine work.
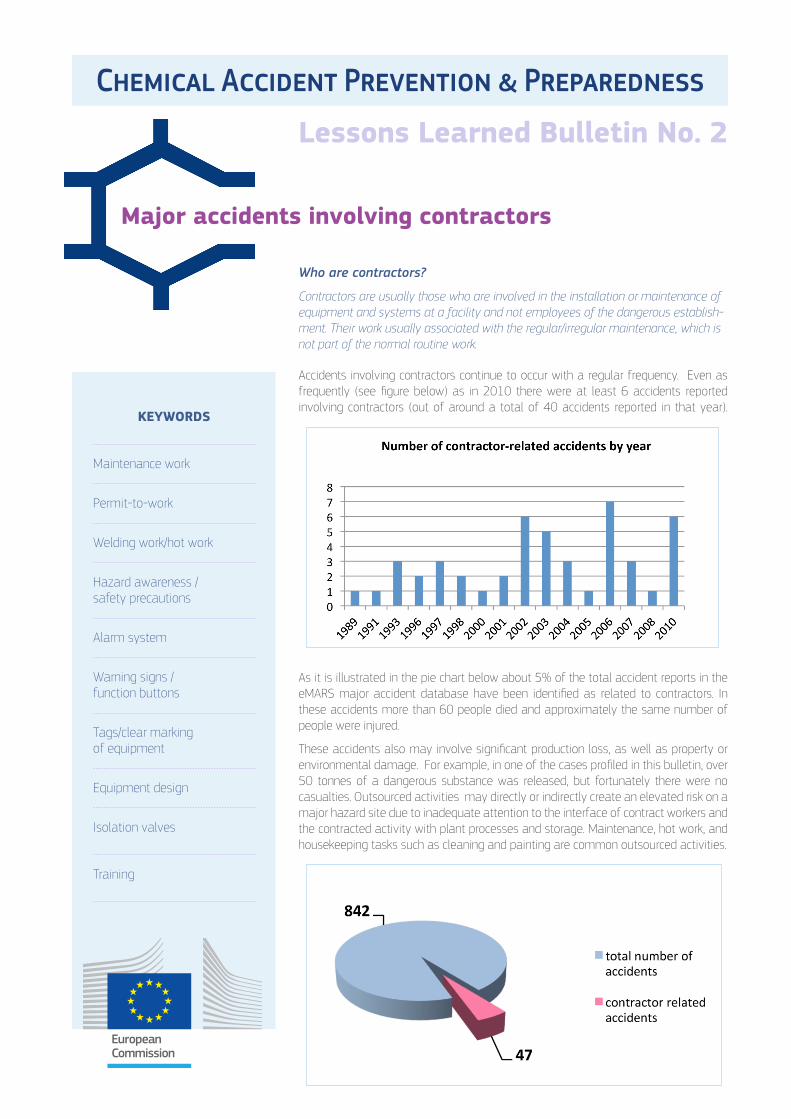
Accidents involving contractors continue to occur with a regular frequency. Even as frequently (see figure below) as in 2010 there were at least 6 accidents reported involving contractors (out of around a total of 40 accidents reported in that year).
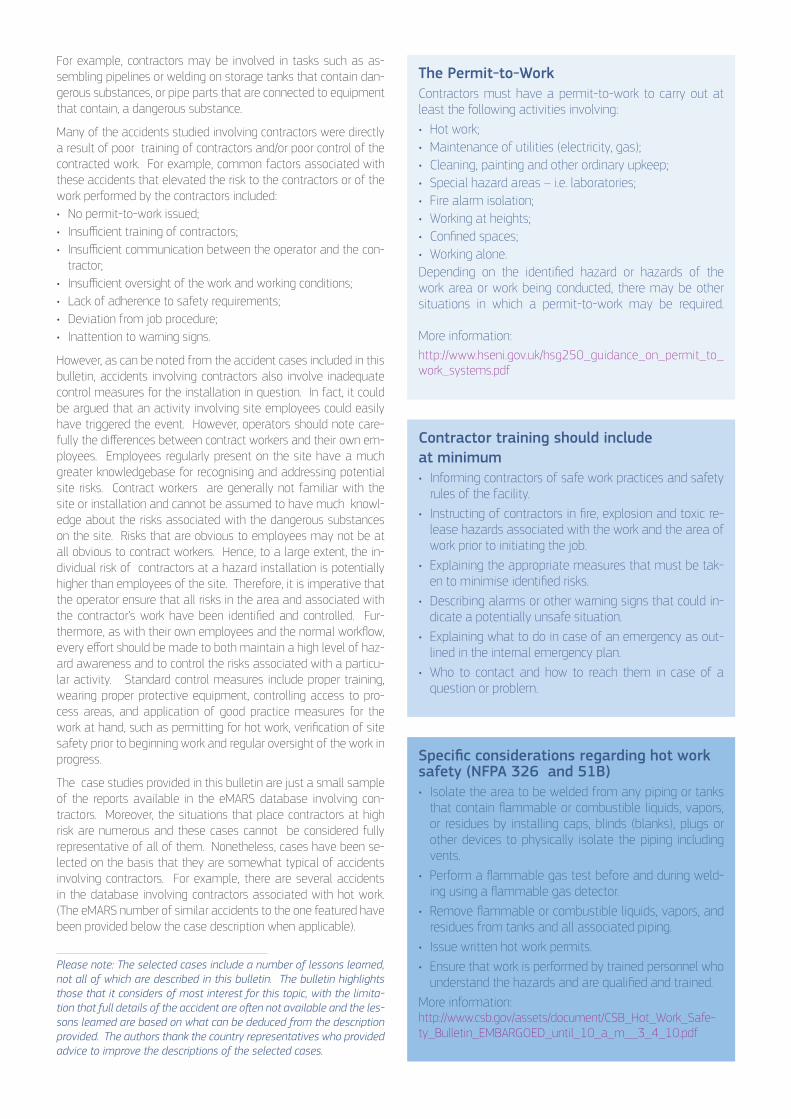
As it is illustrated in the pie chart below about 5% of the total accident reports in the eMARS major accident database have been identified as related to contractors. In these accidents more than 60 people died and approximately the same number of people were injured.
These accidents also may involve significant production loss, as well as property or environmental damage. For example, in one of the cases profiled in this bulletin, over 50 tonnes of a dangerous substance was released, but fortunately there were no casualties. Outsourced activities may directly or indirectly create an elevated risk on a major hazard site due to inadequate attention to the interface of contract workers and the contracted activity with plant processes and storage. Maintenance, hot work, and housekeeping tasks such as cleaning and painting are common outsourced activities.
Major accidents involving contractors
Chemical Accident Prevention & Preparedness
KEYWORDS
Maintenance work
Permit-to-work
Welding work/hot work
Hazard awareness /safety precautions
Alarm system
Warning signs /function buttons
Tags/clear marking of equipment
Equipment design
Isolation valves
Training
For example, contractors may be involved in tasks such as as-sembling pipelines or welding on storage tanks that contain dan-gerous substances, or pipe parts that are connected to equipment that contain, a dangerous substance.
Many of the accidents studied involving contractors were directly a result of poor training of contractors and/or poor control of the contracted work. For example, common factors associated with these accidents that elevated the risk to the contractors or of the work performed by the contractors included:• No permit-to-work issued;• Insufficient training of contractors;• Insufficient communication between the operator and the con-
tractor; • Insufficient oversight of the work and working conditions;• Lack of adherence to safety requirements;• Deviation from job procedure;• Inattention to warning signs.
However, as can be noted from the accident cases included in this bulletin, accidents involving contractors also involve inadequate control measures for the installation in question. In fact, it could be argued that an activity involving site employees could easily have triggered the event. However, operators should note care-fully the differences between contract workers and their own em-ployees. Employees regularly present on the site have a much greater knowledgebase for recognising and addressing potential site risks. Contract workers are generally not familiar with the site or installation and cannot be assumed to have much knowl-edge about the risks associated with the dangerous substances on the site. Risks that are obvious to employees may not be at all obvious to contract workers. Hence, to a large extent, the in-dividual risk of contractors at a hazard installation is potentially higher than employees of the site. Therefore, it is imperative that the operator ensure that all risks in the area and associated with the contractor’s work have been identified and controlled. Fur-thermore, as with their own employees and the normal workflow, every effort should be made to both maintain a high level of haz-ard awareness and to control the risks associated with a particu-lar activity. Standard control measures include proper training, wearing proper protective equipment, controlling access to pro-cess areas, and application of good practice measures for the work at hand, such as permitting for hot work, verification of site safety prior to beginning work and regular oversight of the work in progress.
The case studies provided in this bulletin are just a small sample of the reports available in the eMARS database involving con-tractors. Moreover, the situations that place contractors at high risk are numerous and these cases cannot be considered fully representative of all of them. Nonetheless, cases have been se-lected on the basis that they are somewhat typical of accidents involving contractors. For example, there are several accidents in the database involving contractors associated with hot work. (The eMARS number of similar accidents to the one featured have been provided below the case description when applicable).
Please note: The selected cases include a number of lessons learned, not all of which are described in this bulletin. The bulletin highlights those that it considers of most interest for this topic, with the limita-tion that full details of the accident are often not available and the les-sons learned are based on what can be deduced from the description provided. The authors thank the country representatives who provided advice to improve the descriptions of the selected cases.
The Permit-to-WorkContractors must have a permit-to-work to carry out at least the following activities involving:• Hot work;• Maintenance of utilities (electricity, gas);• Cleaning, painting and other ordinary upkeep; • Special hazard areas – i.e. laboratories;• Fire alarm isolation;• Working at heights;• Confined spaces;• Working alone.Depending on the identified hazard or hazards of the work area or work being conducted, there may be other situations in which a permit-to-work may be required. More information:http://www.hseni.gov.uk/hsg250_guidance_on_permit_to_work_systems.pdf
Specific considerations regarding hot work safety (NFPA 326 and 51B)• Isolate the area to be welded from any piping or tanks
that contain flammable or combustible liquids, vapors, or residues by installing caps, blinds (blanks), plugs or other devices to physically isolate the piping including vents.
• Perform a flammable gas test before and during weld-ing using a flammable gas detector.
• Remove flammable or combustible liquids, vapors, and residues from tanks and all associated piping.
• Issue written hot work permits. • Ensure that work is performed by trained personnel who
understand the hazards and are qualified and trained. More information: http://www.csb.gov/assets/document/CSB_Hot_Work_Safe-ty_Bulletin_EMBARGOED_until_10_a_m__3_4_10.pdf
Contractor training should includeat minimum• Informing contractors of safe work practices and safety
rules of the facility.• Instructing of contractors in fire, explosion and toxic re-
lease hazards associated with the work and the area of work prior to initiating the job.
• Explaining the appropriate measures that must be tak-en to minimise identified risks.
• Describing alarms or other warning signs that could in-dicate a potentially unsafe situation.
• Explaining what to do in case of an emergency as out-lined in the internal emergency plan.
• Who to contact and how to reach them in case of a question or problem.

ContACtFor more information on related to this bulletin on lessons learned from major industrial accidents, please contact
or [email protected] Technology Assessment Unit
European CommissionJoint Research Centre
Institute for the Protectionand Security of the Citizen
Via E. Fermi, 2749 21027 Ispra (VA) Italy
http://mahb.jrc.ec.europa.eu
If your organisation is not already re-ceiving the MAHBulletin, please con-tact [email protected]. Please include your name and email address of your organisation’s focal point for the bulletin.
Mottoof the semester
Learning without thought is labor lost; thought without learning is perilous (Confucius)
MAHBulletin
Accident 1Petrochemical
(Continued from cover page...)
Lessons Learned• When two or more oil tanks are linked to
each other, the connection pipes should be equipped with isolation valves to pre-vent the escape of flammable vapour.
• The company should develop and imple-ment written procedures and provide contractor training to ensure safe work practices during hot work, tank cleaning and work at elevated locations. These measures would have assisted workers in identifying and eliminating hazards prior to beginning the welding operation.
More information:http://www.csb.gov/assets/document/Par-tridge_Report1.pdf
[EMARS Accident # 686]
Accident 5Petrochemical
(Continued from internal pages...)
Lessons Learned• Safety equipment should be better de-
signed to minimize human errors either in normal plant operations or maintenance (e.g. warning signs, function buttons, valve safety signs etc.);
• If alarm systems are applied in an estab-lishment, these equipment supposed to function properly, and if their functionality has limitations, a backup system should be in place too.
• Alarms should be designed and installed in a way to be understood and that they could generate actions when it is nec-essary. Those alarms which are active, should not be delayed or turned off nei-ther manually nor automatically).
[EMARS Accident # 645. See also EMARS Accident # 400]
This publication was developed from in-formation provided by Seveso inspectors through surveys and a Mutual Joint Visit workshop on good enforcement practice for inspectors to promote effective industrial risk management in industrial parks and on dom-ino effect sites. Industrial parks and domino effect sites pose particular challenges for risk management to prevent industrial accidents because they create a situation in which there may be more than one operator responsible for measures necessary to prevent or miti-gate consequences of a potential accident. The Seveso Inspections Series is intended to be a set of publications reflecting conclusions and key points from technical exchanges, re-search and analyses on topics relevant to the effective implementation of the inspection requirements of the Seveso Directive.
Available soonSeveso Inspection Series Volume 5: Chemical hazards risk management in industrial parks and domino effect establishments
All MAHB publications can be found at http://ipsc.jrc.ec.europa.eu/index.php?id=503