Embed Size (px)
Citation preview

313ISSN 1479-6708Future Neurology (2014) 9(3), 313–322
part of
10.2217/FNL.14.23 © 2014 Future Medicine Ltd
MANAGEMENT PERSPECTIVE
Making clozapine safer: current perspectives on improving its tolerability
Bosky Nair1 & James Hunter MacCabe*,2
1National Psychosis Unit, Bethlem Royal Hospital, Monks Orchard Road, Beckenham, Kent, BR3 3BX, UK 2Institute of Psychiatry, King’s College London, National Psychosis Unit, Bethlem Royal Hospital, South London & Maudsley NHS
Foundation Trust, Monks Orchard Road, Beckenham, Kent, BR3 3BX, UK
*Author for correspondence: Tel.: +44 20 7848 0757; Fax: +44 20 7848 0287; [email protected]
ABSTRACT: Clozapine is the gold standard treatment for refractory schizophrenia and its benefits are supported by an evidence base. Yet, it remains largely underused in clinical practice. This is because of low acceptability from patients and reluctance in initiating, and delays in prescribing by clinicians. A major deterrent is often the common adverse reactions, which clinicians are apt to disregard, focusing instead on the severe but rare complications of clozapine, such as agranulocytosis. We will review recent evidence on increasing the prescription of clozapine, focusing particularly on improving the safety and tolerability of the drug, by effective management of its adverse effects. The adverse effects considered in our review include sedation, seizures, myoclonus, hypersalivation, nausea, constipation, hypotension, hypertension, tachycardia, myocarditis, cardiomyopathy, weight gain, diabetes, dyslipidemia, neutropenia, agranulocytosis, fever, nocturnal enuresis and obsessive–compulsive symptoms. We will also discuss strategies to enable successful clozapine rechallenge after severe cardiac and hematological adverse reactions, thus aiming to offer patients their best chance at recovery.
KEYWORDS • adverse drug reactions • clozapine • safety • schizophrenia • tolerability • treatment resistant
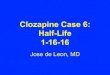
Clozapine is by far the best-supported treatment for patients with treatment-resistant schizophrenia [1,2]. A recent multiple-treatments meta-analysis comparing 15 antipsychotic drugs and placebo in the acute treatment of schizophrenia has shown that clozapine is way ahead of its competition in terms of efficacy (Figure 1) [3]. It has consistently shown a reduction in aggression, mortality rates and suicide [4–6]; however, it remains underprescribed. Current prescribing guidelines suggest offering clozapine to patients with schizophrenia whose illness has not responded adequately to treatment despite the sequential use of adequate doses of at least two different antipsychotic drugs, where at least one of the drugs was a nonclozapine second-generation antipsychotic [7]. Approximately 30% of patients with schizophrenia have treatment-refractory illness according to these definitions, yet only a third of those eligible receive clozapine [8,9]. The delays in prescribing and premature with-drawal over concerns of adverse effects mean that clozapine is prescribed on an average 4 years too late [10]. It is common for patients taking clozapine to discontinue in their first year of treatment with 42% discontinuing over 24 months [11].
A large proportion of patients (48%), discontinue clozapine based on patient preference [12]. In more than a third of those discontinuing, adverse effects are recorded in the case record as the reason for discontinuation [12]. In this article, we will discuss strategies aimed at reducing adverse effects of clozapine and increasing its acceptability, thus improving outcomes for this patient group.
For reprint orders, please contact: [email protected]

Future Neurology (2014) 9(3)314
Figure 1. Forest plot for efficacy of antipsychotics drugs compared with placebo. Treatments are ranked according to their surface under the cumulative ranking values. CrI: Credible interval; SMD: Standardized mean difference. Reproduced with permission from [3].
MAnAgEMEnT PERSPECTivE Nair & MacCabe
future science group
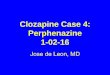
In their survey of 130 patients assessing change 6 months or more after clozapine treat-ment, Waserman and Criollo, showed that patients reported hypersalivation as the most common subjective experience of adverse effect [13]. Other common side effects were weight gain, constipation and thirst (Figure 2).
This is a surprise to most clinicians, per-haps because clinicians are more focused on the medically serious adverse effects, including neutropenia, cardiac effects and diabetes, and give insufficient attention to the common and debilitating adverse effects that affect patients’ quality of life, and hence their adherence to treatment.
Adverse reactions often occur when clozapine is initiated too hastily or titrated to a dose higher than necessary. Insufficient discussion of likely adverse effects can often make patients less pre-pared thus influence adherence to treatment.
The general principles in clozapine initiation and titration should include the following steps:
● Starting low, and going slow;
● Using the lowest effective dose;
● Asking about adverse effects;
● Offering reassurance about short-lived adverse effects;
● Treating adverse effects aggressively.
The guidelines for blood monitoring show national variation but the broad principles are similar in most developed countries. In the UK, current recommendations suggest moni-toring the white cell count weekly for the first 18 weeks, then fortnightly until 6 months, and monthly thereafter. If the white blood count falls below 3.5 × 109/l and/or the absolute neu-trophil count falls below 2.0 × 109/l, then the
Clozapine -0.88 (-1.03 to -0.73)
Overall change in symptoms SMD (95% Crl)
Amisulpride -0.66 (-0.78 to -0.53)
Olanzapine -0.59 (-0.65 to -0.53)
Risperidone -0.56 (-0.63 to -0.50)
Paliperidone -0.50 (-0.60 to -0.39)
Zotepine -0.49 (-0.66 to -0.31)
Haloperidol -0.45 (-0.51 to -0.39)
Quetiapine -0.44 (-0.52 to -0.35)
Aripiprazole -0.43 (-0.52 to -0.34)
Sertindole -0.39 (-0.52 to -0.26)
Ziprasidone -0.39 (-0.49 to -0.30)
Chlorpromazine -0.38 (-0.54 to -0.23)
Asenapine -0.38 (-0.51 to -0.25)
Lurasidone -0.33 (-0.45 to -0.21)
Iloperidone -0.33 (-0.43 to -0.22)
-1 -0.5
Favors active drug
0

315
Figure 2. Ratings in percentages by 130 patients on their subjective experience of clozapine treatment. Data taken from [13].
Making clozapine safer: current perspectives on improving its tolerability MAnAgEMEnT PERSPECTivE
future science group www.futuremedicine.com
frequency of monitoring is increased. Clozapine must be withdrawn if the white cell count falls below 3.0 × 109/l and/or the ANC falls below 1.5 × 109/l (Table 1).
Often the stringent blood monitoring regime associated with clozapine can deter patients from an effective trial of clozapine. In a survey of patient perceptions on clozapine, need for blood tests topped the list of reasons the patients did not like clozapine as a treatment option [15]. Improving patients’ understanding of the need for blood tests may ensure that an effective trial is achieved. This can be addressed by discussion with the patient about the reasons why clozapine is being recommended, the evidence that this may be of benefit to the particular patient, the purpose of blood tests and any concerns that patients may have relating to blood tests. Some clinicians may be hesitant to initiate clozapine for patients who they consider may not be able to tolerate blood tests or adhere to treatment [16]. However, the increased insight gained on clozapine often results in improvements in adherence.
Where a patient refuses clozapine due to fre-quent blood monitoring, there are three com-mon scenarios. For some patients, blood tests are just one of a number of concerns about clozapine, and since blood tests are an essential prerequisite of clozapine treatment, the discus-sion becomes focused around blood tests, when the patients’ main concerns may be about other aspects of clozapine. In such cases a discussion and exploration of the patients’ concerns about
clozapine can be very helpful. In the second sce-nario, the patient holds paranoid ideas about the purpose of the blood tests, and suspects that the blood may be used for malign purposes. In the third scenario, the patient may be ambivalent or even enthusiastic about taking clozapine, but has a fear of needles. In these cases it is helpful to discuss use of practical measures such as using lidocaine or prilocaine cream 60 min before ven-ipuncture. Smaller butterfly needles can be less daunting for some patients. Premedication with low-dose benzodiazepines, prior to venipuncture or behavioral approaches to address needle pho-bia, can also be tried. When all other measures fail, the use of restraint may be warranted, if the legal framework permits this. It is also impor-tant to note that restraint may be unhelpful in ensuring compliance to clozapine treatment and thus used only after careful consideration of risks and benefits. It is important to keep the frequency of blood tests to a minimum and obvi-ate unnecessary blood tests in order to maintain the therapeutic alliance with the patient.
Below we have listed the common adverse effects of clozapine and recommendations on their management.
CNS effects●● Sedation
Sedation is almost a universal adverse effect in the first 3 months of treatment with clozapine, but usually improves. Reduction of sedative effects can be achieved by slowing down titra-tion, asymmetric dose split with lower daytime
Energy
AppetiteBloatedness
Unusual movementsSalivation during the day
Dizziness
Abdominal painUrination
ThirstConstipation
WeightSalivation at night
0 10 20 30 40 50 60 70 80 90 100Ratings by 130 participants (%)

Future Neurology (2014) 9(3)316
MAnAgEMEnT PERSPECTivE Nair & MacCabe
future science group
dosing and avoiding concomitant use of other sedative or hypnotic medications. Aripiprazole at the dose of 5–15 mg daily can be used for its alerting effects [17].
●● Seizures & myoclonusThe risk of developing seizures is dependent on the plasma concentration of clozapine [18]. Anticonvulsant cover with sodium valproate or lamotrigine is required if the plasma level exceeds 0.5 mg/l or at a dose greater than 600 mg/day. If a seizure occurs, clozapine should be stopped for 24 h. When recommenced, the dose should be reduced by 25–50% and an anticonvulsant should be added or increased. The antiepileptics, carbamazepine and phenytoin are best avoided due to its propensity to reduce clozapine levels possibly resulting from pharmacokinetic drug interaction via the CYP450 system. Myoclonus, which is brief involuntary twitching of muscle or a group of muscles, can sometimes occur with clozapine. They may be a harbinger of future seizure activity requiring dose reduction or treat-ment with anticonvulsants. If sodium valproate is used as an anticonvulsant, it is essential to note that there is tentative evidence that patients on clozapine and concomitant sodium valproate are at increased risk of myocarditis [19].
Gastrointestinal●● Hypersalivation
Hypersalivation is noted to be worse at the start of treatment but may persist in some. It is distressing, socially embarrassing and can at times cause life-threatening complications such as aspiration pnuemonia. A Cochrane review by Syed et al. in 2008 showed limited evidence for antimuscarinics and some Chinese remedies [20]. Hyoscine hydrobromide up to 300 μg
three-times daily is commonly used in the UK but has so far been lacking in evidence from randomized controlled trials. It is worth noting that hyoscine hydrobromide is an anticholiner-gic agent and may cause cognitive impairement. Pirenzapine can be considered as an alternative, at a dose of 25–100 mg, on the basis of exten-sive clinical experience but no effect was dem-onstrated on a single randomized controlled trial [21,22]. Amisulpride and sulpiride, evidenced by one small randomized controlled trials each, and terazosin in combination with benztropine, are alternate agents [23–25].
●● NauseaNausea is commonly observed in the first 6 weeks of treatment. Hyoscine, which also acts as an antiemetic can be used to treat nausea, as well as hypersalivation. Prochlorperazine or metoclopramide should be used with caution if extrapyramidal side effects have occurred in the past.
●● ConstipationConstipation is a very common adverse effect and often persists, thus affecting adherence to medication. It can develop serious complications such as obstruction, necrosis, perforation, toxic megacolon and pulmonary aspiration, and can be potentially fatal [26]. It can sometimes lead to clozapine toxicity due to sequestration in the gut and later sudden release. Prompt treatment should be initiated with good level of hydration, high fibre diet, and exercise. Bulk forming or osmotic laxatives should be used, however they may be ineffective or even detrimental if adequate hydration is not maintained. Thus, it may be nec-essary to use osmotic laxatives in combination with a stimulant laxative such as senna.
Table 1. Clozapine monitoring routine and according to benign ethnic neutropenia criteria.
Classification Routine monitoring (×109/l) BEN parameters (×109/l) Comment
WBCs Neutrophils WBC Neutrophils
Green ≥3.5 ≥2.0 ≥3.0 ≥1.5 Continue clozapine treatment
Amber ≥3.0 and <3.5
≥1.5 and <2 ≥2.5 and ≤3.0
≥1.0 and ≤1.5 Exercise caution Increase monitoring to twice weekly
Red <3.0 <1.5 <2.5 <1.0 Stop clozapine treatment Increase monitoring to daily
BEN: Benign ethnic neutropenia; WBC: White blood cell. Reproduced with permission from [14].

317
Making clozapine safer: current perspectives on improving its tolerability MAnAgEMEnT PERSPECTivE
future science group www.futuremedicine.com
Cardiovascular effects●● Hypotension
Hypotension occurs in the first few weeks of treatment and is usually short-lived, lasting 4–6 weeks. In such cases, slowing titration and splitting daily dose of clozapine to reduce peak plasma concentration and peak trough variability can reduce the possibility of orthostatic hypoten-sion [27]. Patients can be advised to stand slowly from sitting or lying positions, and exert caution with physical activity, consumption of alcoholic beverages and heat exposure, which can worsen orthostatic hypotension. If nonpharmacological methods are ineffective, fludrocortisone can be added, although it carries the risk of congestive cardiac failure [28]. It is essential to note that hypotension is often associated with myocarditis.
●● HypertensionHypertension is observed during the first month of titration and has to be carefully monitored especially in those patients who have existing essential hypertension. Treatment involves use of antihypertensives, such as ACE inhibitors or β-blockers, the latter being preferred if there is coexisting tachycardia.
●● TachycardiaTachycardia is a very common and usually benign adverse reaction; however, it often causes alarm, since it can also be a precursor of more serious adverse effects, such as myocarditis and cardiomyopathy. The symptoms that should raise concern include shortness of breath, chest pain, lethargy and fever. In such instances, the patient should be transferred to an acute medi-cal setting, and troponin, C-reactive protein (CRP), ECG and echocardiogram should be performed. If patient is mildly tachycardic, CRP, troponin and ECG must be performed. A heart rate above 130 bpm or an increase of 20 bpm above the baseline requires daily C-reactive protein and troponin, as well as consultation with a cardiologist. If tachycardia persists, 24-h heart rate monitoring and echocardiography is warranted [29].
Tachycardia can be treated by dose reduction and slowing the uptitration. Patients should be encouraged to reduce smoking and caffeine intake, which can contribute to tachycardia. β-blockers, such as bisoprolol and atenolol or ivabradine, that cause selective and specific inhibition of cardiac pacemaker I
f current are
effective in treatment of tachycardia [30,31].
●● MyocarditisMyocarditis is an inflammatory disorder of the myocardium, which can occur in patients on clozapine, particularly during the first 2 months of treatment [32]. There is some variability in the incidence rates of fatal myocarditis obtained from various countries, with 0.8 in 10,000 in Canada and 1 in 67,000 in the USA, and much higher rates quoted in studies from Australia and New Zealand [33]. Patients may present with chest pain, palpitations, breathlessness and fatigue. On physical examination, fever, tachycardia, arrhythmia or features of acute heart failure may be observed. Investigations reveal elevated CRP and troponin levels. ECG may show diffuse T-wave inversion and saddle ST segments.
All patients can be monitored as per the following guidelines [29]:
● Baseline: troponin, CRP and echocardiogram;
● Weekly (day 7, 14, 21 and 28): CRP and troponin;
● Every second day for 28 days: pulse, blood pressure, temperature and respiratory rate.
Management strategies include the following steps:
● If suspected (tachycardia with heart rate ≥120 bpm or increased by >30 bpm, CRP 50–100 mg/l or slightly elevated troponin but without other symptoms or signs): clozapine can be continued while signs of illness can be carefully monitored;
● If troponin is two-times the upper limit of normal or CRP >100 mg/l: clozapine must be stopped immediately; urgent echocardiogram and referral to cardiologist is essential.
●● CardiomyopathyCardiomyopathy is a more chronic disease of myocardial contractile dysfunction and devel-ops usually after at least 8 weeks of treatment, although it can develop at any time [34]. There is huge variation in the presentation of patients developing cardiomyopathy ranging from sub-clinical symptoms to fulminant pulmonary edema and cardiogenic shock [35]. In such cases, clozapine should be immediately discontinued, followed by echocardiogram and urgent cardi-ology referral. Some patients with cardiotoxic-ity have benefited from continuing clozapine, while left ventricular dysfunction is managed with ACE inhibitors, diuretics, β-blockers or

Future Neurology (2014) 9(3)318
MAnAgEMEnT PERSPECTivE Nair & MacCabe
future science group
angiotensin antagonists within well-controlled supervised environments [36].
Metabolic effects●● Weight gain
There is strong correlation between clozapine use and weight gain from prospective studies and double-blind randomized controlled trials [37]. Weight gain is a common cause for patients discontinuing clozapine. In addition, there are significant health risks associated with weight gain, which makes it essential for clinicians to engage in a dialog with patients on dietary modification and exercise. There is evidence for the role of educational and psychosocial pro-grams for managing weight gain associated with antipsychotics [38,39]. Addition of aripipazole at a dose of 5–15 mg can have significant benefits with weight, BMI and fasting cholesterol levels [40]. Metformin has also been shown to reduce bodyweight and reverse metabolic abnormalities in patients on clozapine who have pre-existing metabolic syndrome [41]. Other measures include use of orlistat and topiramate, although the latter is associated with cognitive impairment. Gastric banding has been used in extreme cases [42].
●● DiabetesClozapine has dose-dependent effect in raising insulin levels. The increase is 36% over a period of 5 years but often is missed and patients may present with severe complications, such as diabetic ketoaci-dosis [43]. Diabetes should be considered during routine monitoring of patients on clozapine by measuring fasting blood glucose and Hb1Ac levels.
●● DyslipidemiaTriglyceride levels can double on treatment with clozapine [43]. It is therefore essential to routinely
monitor lipid profile every 3 months for a year, followed by annual tests. Treatment includes dietary and lifestyle modifications, use of statins, fibrates and fish oils [44,45].
The following table shows the recommended monitoring for metabolic effects of clozap-ine as described in The Maudsley Prescribing Guidelines (Table 2) [46].
Hematological effects●● Neutropenia
Nearly 3% of patients on clozapine develop neutro-penia [47]. There are no clear risk factors, although the following have been proposed over the years: those of a younger age group, African–Caribbean ancestry, low baseline white cell counts, history of clozapine-induced neutropenia, and recent ini-tiation on clozapine. Half of those patients who develop neutropenia do so in the first 18 weeks of treatment [47]. A third of the patients develop blood dyscrasia if rechallenged with clozapine, among whom nearly half develop agranulocytosis [48]. The second episode of neutropenia tends to occur earlier in the course of treatment, is more rapid and severe, with slower rate of recovery. The risk of neutropenia is not dose related.
●● AgranulocytosisAgranulocytosis results from dysfunctional mye-lopoiesis where the neutrophil count falls to less than 0.5 × 109/l. Clozapine-induced agranulocy-tosis can occur in 0.8% of patients, with 80% of cases occurring within first 18 weeks [47]. There is an increase in risk with increasing age and among people of Asian ethnic origin. Mortality rate from agranulocytosis is 5%, with overall risk of death from clozapine-induced agranulocytosis presently considered to be less than 3 among 10,000 patients on clozapine [49,50].
Table 2. Monitoring requirements for clozapine use.
Parameters to monitor
Baseline 1 month 3 months 6 months 12 months 4–6 monthly Annually
Weight, BMI and waist circumference
X X X X X – X
Fasting plasma glucose, HbA1c or oral glucose tolerance test
X X – X X X –
Fasting lipids X – X X X – XLiver function tests
X – – X – X
Data taken from [46].

319
Making clozapine safer: current perspectives on improving its tolerability MAnAgEMEnT PERSPECTivE
future science group www.futuremedicine.com
●● RechallengeThose patients who develop neutropenia on clo-zapine and are being considered for a rechallenge will require specialist input from hematologists, as needed. It is necessary to review their timeline of neutropenia, looking closely at the rate and timing, and association with other medications. Clozapine-induced neutropenia usually occurs early within the first 18 weeks of treatment, is sud-den, shows slow recovery between 7 and 21 days and the white blood cell count returns to normal levels when off clozapine. Rechallenge must not be attempted in patients who develop agranulocytosis as 80% of them will have further episodes [51].
●● Benign ethnic neutropeniaIt is necessary to consider whether patients may have benign ethnic neutropenia (BEN), which is common among people of African and Middle Eastern origin. By definition, BEN is ‘the occur-rence of neutropenia, defined by normative data in white populations, in individuals of other ethnic groups who are otherwise healthy and who do not have repeated or severe infections’ [52]. Clozapine discontinuation among individuals with BEN, is inadvertently higher due to a low baseline white cell count [14,47]. Thus, clozapine monitoring parameters have been amended for use in patients diagnosed with BEN (Table 1) [14].
In those patients, where clozapine rechallenge after neutropenia is being considered, discontinu-ation of other drugs known to suppress the bone marrow, such as valproate, should be undertaken, if possible. Lithium, at plasma levels greater than 0.6 mmol/l, has been found to increase neutro-phil count and is therefore used in conjunction with clozapine [53–55]. Although it does not protect against agranulocytosis, lithium may speed the recovery of white cell count in patients after they develop agranulocytosis [54].
Granulocyte colony stimulating factor, which increases granulocyte maturation in the bone marrow, has been used as cotherapy with clo-zapine [56]. It does not appear to protect against agranulocytosis. Caution has to be maintained regarding its use due to uncertainty about its safety and efficacy in the long run. It must be used only if neutropenia is judged not to be clozapine-induced.
Other effects●● Fever
Fever is common in first the 3 weeks of initia-tion, but can occur at any time during treatment.
Patients who develop fever should have their full blood count checked urgently to exclude agranulocytosis. It is essential to exclude myo-carditis and pericarditis by performing prompt echocardiogram, troponin levels and creatine kinase levels. Neuroleptic malignant syndrome should also be considered. Clozapine titration should be slowed down in case of fever, and sus-pended if temperature rises to above 38.5° with use of supportive measures such as antipyretic medications [57].
●● Nocturnal enuresisThis is a side effect that often persists, much to the dismay of patients and clinicians [58]. Measures to prevent episodes include reduc-ing evening doses and restricting fluid intake nearing bedtime. Desmopressin, can be used at a dose of 120 μg sublingual administration to reduce production of urine, although it should be avoided in hypertension [59]. Other drugs used include oxybutynin at a dose of 2.5–5 mg up to three-times daily or solifenacin 5–10 mg once daily [60].
●● Obsessive–compulsive symptomsObsessive–compulsive symptoms can develop as a late complication of clozapine therapy, which is hypothesized to be secondary to its antiseroton-ergic effect. Treatment is along the lines of treat-ment for obsessive–compulsive symptoms and include cognitive behavioral therapy [61], and the use of pharmacological agents such as selective serotonin re-uptake inhibitors, clomipramine, sulpiride, amisulpiride and aripiprazole [62,63].
●● Blurring of visionIn the event of blurring of vision, coprescrip-tion of anticholinergics should be avoided. It is essential to check plasma levels of clozapine and exclude hyperglycemia or impaired glucose tolerance.
ConclusionIn conclusion, clozapine has a unique position among all first- and second-generation antipsy-chotics in the treatment of refractory schizophre-nia. However, it remains underused, partly due to the reduced acceptability among the patient group due to the more common side effects and stringent blood monitoring guidelines. Also, some clinicians remain reluctant to prescribe it, often leading to unnecessary delays. Clinician factors studied have shown this reluctance stems

Future Neurology (2014) 9(3)320
MAnAgEMEnT PERSPECTivE Nair & MacCabe
future science group
from fear of serious adverse reactions, lim-ited experience and knowledge, as well as less active marketing and promotion of this generic drug [64,65]. A multidisciplinary approach that includes presence of pharmacists at the point of prescribing can encourage clozapine prescribing among clinicians [16].
The more serious and life-threatening con-cerns such as neutropenia, agranulocytosis, myocarditis and metabolic side effects can be prevented by early detection and prompt treat-ment. It is essential to work in collaboration with the patient and their families as much as possible, hearing their concerns and addressing them, maintaining clear communication about the treatment plan, anticipated adverse reactions and how to go about managing them. Another strategy that can facilitate such clinician–patient dialog, particularly with ambivalent individu-als, is motivational interviewing. The long-term benefits of clozapine and evidence substantiat-ing them can be introduced early on during discussions around treatment.
Future perspectiveAn exciting collaborative research currently being undertaken at the Institute of Psychiatry involves development of pharmacogenomic bio-markers to produce clinical decision-making tools for the treatment of schizophrenia, known as the CRESTAR collaboration. Its primary aim is to develop clinical prediction tools that will help clinicians to determine the patients who are
likely to require clozapine, and those who are at risk of side effects. This would enable provi-sion of more tailored treatment, which is safer, commenced sooner and requires less monitor-ing, since blood monitoring would be focused on those patients who were truly at risk. The study would focus on developing algorithms to predict treatment resistance and propensity to the adverse effects of clozapine.
There is also a growing speculation on the role of glutamatergic drugs in the treatment of schizophrenia, particularly in those failing to respond to conventional treatment. These agents that are hypothesized to reduce nega-tive and cognitive symptoms of schizophrenia could prove valuable in augmentation strate-gies; although evidence from further research is required to substantiate this.
AcknowledgementsThe authors would like to thank E Whiskey and S Gee for their valuable insights and contributions to this article.
Financial & competing interests disclosureThe authors have no relevant affiliations or financial involvement with any organization or entity with a finan-cial interest in or financial conflict with the subject matter or materials discussed in the manuscript. This includes employment, consultancies, honoraria, stock ownership or options, expert testimony, grants or patents received or pending, or royalties.
No writing assistance was utilized in the production of this manuscript.
EXECUTivE SUMMARY ● Clozapine is the only evidence-based treatment for treatment-resistant schizophrenia.
● It shows superiority in terms of its efficacy, reduction of aggression, mortality rates and suicide.
● Clozapine remains underprescribed mainly due to its much feared adverse effects.
● It is important for clinicians to engage patients in an open discussion about the adverse effects, as well as the benefits of treatment with clozapine.
● Prompt and effective management of adverse reactions can go a long way in enabling successful trial of clozapine.
References1 Essali A, Al-Haj HN, Li C, Rathbone J.
Clozapine versus typical neuroleptic medication for schizophrenia. Cochrane Database Syst. Rev. 1, CD000059 (2009).
2 Asenjo LC, Komossa K, Rummel-Kluge C et al. Clozapine versus other atypical antipsychotics for schizophrenia. Cochrane Database Syst. Rev. 11, CD006633 (2010).
3 Leucht S, Cipriani A, Spineli L et al. Comparative efficacy and tolerability of 15 antipsychotic drugs in schizophrenia: a multiple-treatments meta-analysis. Lancet 382(9896), 951–962 (2014).
4 Krakowski MI, Czobor P, Citrome L, Bark N, Cooper TB. Atypical antipsychotic agents in the treatment of violent patients with schizophrenia and schizoaffective disorder. Arch. Gen. Psychiatry 63(6), 622–629 (2006).
5 Tiihonen J, Lonnqvist J, Wahlbeck K et al. 11-year follow-up of mortality in patients with schizophrenia: a population-based cohort study (FIN11 study). Lancet 374(9690), 620–627 (2009).
6 Meltzer HY, Alphs L, Green AI et al. Clozapine treatment for suicidality in schizophrenia: International Suicide Prevention Trial (InterSePT). Arch. Gen. Psychiatry 60(1), 82–91 (2003).

321future science group www.futuremedicine.com
Making clozapine safer: current perspectives on improving its tolerability MAnAgEMEnT PERSPECTivE
7 National Collaborating Centre for Mental Health. Schizophrenia: Core Interventions in the Treatment and Management of Schizophrenia in Adults in Primary and Secondary Care. British Psychological Society, Leicester, UK (2009).
8 Meltzer HY. Treatment-resistant schizophrenia – the role of clozapine. Curr. Med. Res. Opin. 14(1), 1–20 (1997).
9 Downs J, Zinkler M. Clozapine: national review of postcode prescribing. Psychiatrist 31, 384–387 (2007).
10 Howes OD, Vergunst F, Gee S, McGuire P, Kapur S, Taylor D. Adherence to treatment guidelines in clinical practice: study of antipsychotic treatment prior to clozapine initiation. Br. J. Psychiatry 201(6), 481–485 (2012).
11 Ciapparelli A, Dell’Osso L, Pini S, Chiavacci MC, Fenzi M, Cassano GB. Clozapine for treatment-refractory schizophrenia, schizoaffective disorder, and psychotic bipolar disorder: a 24-month naturalistic study. J. Clin. Psychiatry 61(5), 329–334 (2000).
12 Taylor DM, Douglas-Hall P, Olofinjana B, Whiskey E, Thomas A. Reasons for discontinuing clozapine: matched, case-control comparison with risperidone long-acting injection. Br. J. Psychiatry 194(2), 165–167 (2009).
13 Waserman J, Criollo M. Subjective experiences of clozapine treatment by patients with chronic schizophrenia. Psychiatr. Serv. 51(5), 666–668 (2000).
14 Whiskey E, Olofinjana O, Taylor D. The importance of the recognition of benign ethnic neutropenia in black patients during treatment with clozapine: case reports and database study. J. Psychopharmacol. 25(6), 842–845 (2011).
15 Taylor D, Shapland L, Laverick G, Bond J, Munro J. Clozapine- a survey of patient perceptions. Psychiatrist 24, 450–452 (2000).
16 Gee S, Vergunst F, Howes O, Taylor D. Practitioner attitudes to clozapine initiation. Acta. Psychiatr. Scand. doi:10.1111/acps.12193 (2013) (Epub ahead of print).
17 Rocha FL, Hara C. Benefits of combining aripiprazole to clozapine: three case reports. Prog. Neuropsychopharmacol. Biol. Psychiatry 30(6), 1167–1169 (2006).
18 Pisani F, Oteri G, Costa C, Di RG, Di PR. Effects of psychotropic drugs on seizure threshold. Drug Saf. 25(2), 91–110 (2002).
19 Ronaldson KJ, Fitzgerald PB, Taylor AJ, Topliss DJ, Wolfe R, McNeil JJ. Rapid clozapine dose titration and concomitant sodium valproate increase the risk of
myocarditis with clozapine: a case–control study. Schizophr. Res. 141(2–3), 173–178 (2012).
20 Syed R, Au K, Cahill C et al. Pharmacological interventions for clozapine-induced hypersalivation. Cochrane Database Syst. Rev. 3, CD005579 (2008).
21 Schneider B, Weigmann H, Hiemke C, Weber B, Fritze J. Reduction of clozapine-induced hypersalivation by pirenzepine is safe. Pharmacopsychiatry 37(2), 43–45 (2004).
22 Bai YM, Lin CC, Chen JY, Liu WC. Therapeutic effect of pirenzepine for clozapine-induced hypersalivation: a randomized, double-blind, placebo-controlled, cross-over study. J. Clin. Psychopharmacol. 21(6), 608–611 (2001).
23 Kreinin A, Novitski D, Weizman A. Amisulpiride treatment of clozapine-induced hypersalivation in schizophrenia patients: a randomised, double-blind, placebo-controlled cross-over study. Int. Clin. Psychopharmacol. 21(2), 99–103 (2006).
24 Wang J, Omori IM, Fenton M, Soares B. Sulpiride augmentation for schizophrenia. Cochrane Database Syst. Rev. 1, CD008125 (2010).
25 Reinstein M, Sirotovskaya L, Chasanov M, Jones L, Mohan S. Comparative efficacy and tolerability of benztropine and terazosin in the treatment of hypersalivation secondary to clozapine. Clin. Drug Invest. 17(2), 97–106 (1999).
26 Palmer SE, McLean RM, Ellis PM, Harrison-Woolrych M. Life-threatening clozapine-induced gastrointestinal hypomotility: an analysis of 102 cases. J. Clin. Psychiatry 69(5), 759–768 (2008).
27 Gugger JJ. Antipsychotic pharmacotherapy and orthostatic hypotension: identification and management. CNS Drugs 25(8), 659–671 (2011).
28 Testani M Jr. Clozapine-induced orthostatic hypotension treated with fludrocortisone. J. Clin. Psychiatry 55(11), 497–498 (1994).
29 Ronaldson KJ, Fitzgerald PB, Taylor AJ, Topliss DJ, McNeil JJ. A new monitoring protocol for clozapine-induced myocarditis based on an analysis of 75 cases and 94 controls. Aust. NZ J. Psychiatry 45(6), 458–465 (2011).
30 Sulfi S, Timmis AD. Ivabradine – the first selective sinus node I(f ) channel inhibitor in the treatment of stable angina. Int. J. Clin. Pract. 60(2), 222–228 (2006).
31 Lally J, Brook J, Dixon T et al. Ivabradine, a novel treatment for clozapine induced sinus
tachycardia: a case series. Ther. Adv. Psychopharmacol. doi:10.1177/2045125313512325 (2013) (Epub ahead of print).
32 La GL, Graham D, Trontell A. Myocarditis and cardiomyopathy associated with clozapine use in the United States. N. Engl. J. Med. 345(3), 224–225 (2001).
33 Warner B, Alphs L, Schaedelin J, Koestler T. Clozapine and sudden death. Lancet 355(9206), 842 (2000).
34 Kilian JG, Kerr K, Lawrence C, Celermajer DS. Myocarditis and cardiomyopathy associated with clozapine. Lancet 354(9193), 1841–1845 (1999).
35 Leo RJ, Kreeger JL, Kim KY. Cardiomyopathy associated with clozapine. Ann. Pharmacother. 30(6), 603–605 (1996).
36 Layland JJ, Liew D, Prior DL. Clozapine-induced cardiotoxicity: a clinical update. Med. J. Aust. 190(4), 190–192 (2009).
37 Covell NH, Weissman EM, Essock SM. Weight gain with clozapine compared with first generation antipsychotic medications. Schizophr. Bull. 30(2), 229–240 (2004).
38 Menza M, Vreeland B, Minsky S, Gara M, Radler DR, Sakowitz M. Managing atypical antipsychotic-associated weight gain: 12-month data on a multimodal weight control program. J. Clin. Psychiatry 65(4), 471–477 (2004).
39 Vreeland B, Minsky S, Menza M, Rigassio RD, Roemheld-Hamm B, Stern R. A program for managing weight gain associated with atypical antipsychotics. Psychiatr. Serv. 54(8), 1155–1157 (2003).
40 Fleischhacker WW, Heikkinen ME, Olie JP et al. Effects of adjunctive treatment with aripiprazole on body weight and clinical efficacy in schizophrenia patients treated with clozapine: a randomized, double-blind, placebo-controlled trial. Int. J. Neuropsychopharmacol. 13(8), 1115–1125 (2010).
41 Chen CH, Huang MC, Kao CF et al. Effects of adjunctive metformin on metabolic traits in nondiabetic clozapine-treated patients with schizophrenia and the effect of metformin discontinuation on body weight: a 24-week, randomized, double-blind, placebo-controlled study. J. Clin. Psychiatry 74(5), e424–e430 (2013).
42 Hamoui N, Kingsbury S, Anthone GJ, Crookes PF. Surgical treatment of morbid obesity in schizophrenic patients. Obes. Surg. 14(3), 349–352 (2004).
43 Henderson DC, Cagliero E, Gray C et al. Clozapine, diabetes mellitus, weight gain,

Future Neurology (2014) 9(3)322
MAnAgEMEnT PERSPECTivE Nair & MacCabe
future science group
and lipid abnormalities: a five-year naturalistic study. Am. J. Psychiatry 157(6), 975–981 (2000).
44 Ojala K, Repo-Tiihonen E, Tiihonen J, Niskanen L. Statins are effective in treating dyslipidemia among psychiatric patients using second-generation antipsychotic agents. J. Psychopharmacol. 22(1), 33–38 (2008).
45 Caniato RN, Alvarenga ME, Garcia-Alcaraz MA. Effect of omega-3 fatty acids on the lipid profile of patients taking clozapine. Aust. NZ J. Psychiatry 40(8), 691–697 (2006).
46 Taylor D, Paton C, Kapur S. The Maudsley Prescribing Guidelines in Psychiatry (11th Edition). Wiley-Blackwell, West Sussex, UK, 95 (2012).
47 Munro J, O’Sullivan D, Andrews C, Arana A, Mortimer A, Kerwin R. Active monitoring of 12,760 clozapine recipients in the UK and Ireland. Beyond pharmacovigilance. Br. J. Psychiatry 175, 576–580 (1999).
48 Dunk LR, Annan LJ, Andrews CD. Rechallenge with clozapine following leucopenia or neutropenia during previous therapy. Br. J. Psychiatry 188, 255–263 (2006).
49 Andres E, Zimmer J, Affenberger S, Federici L, Alt M, Maloisel F. Idiosyncratic drug-induced agranulocytosis: update of an old disorder. Eur. J. Intern. Med. 17(8), 529–535 (2006).
50 Cohen D, Bogers JP, van Dijk D, Bakker B, Schulte PF. Beyond white cell monitoring:
screening in the initial phase of clozapine therapy. J. Clin. Psychiatry 73(10), 1307–1312 (2012).
51 Manu P, Sarpal D, Muir O, Kane JM, Correll CU. When can patients with potentially life-threatening adverse effects be rechallenged with clozapine? A systematic review of the published literature. Schizophr. Res. 134(2–3), 180–186 (2012).
52 Haddy TB, Rana SR, Castro O. Benign ethnic neutropenia: what is a normal absolute neutrophil count? J. Lab. Clin. Med. 133, 15–22 (1999).
53 Adityanjee. Modification of clozapine-induced leukopenia and neutropenia with lithium carbonate. Am. J. Psychiatry 152(4), 648–649 (1995).
54 Blier P, Slater S, Measham T, Koch M, Wiviott G. Lithium and clozapine-induced neutropenia/agranulocytosis. Int. Clin. Psychopharmacol. 13(3), 137–140 (1998).
55 Silverstone PH. Prevention of clozapine-induced neutropenia by pretreatment with lithium. J. Clin. Psychopharmacol. 18(1), 86–88 (1998).
56 Whiskey E, Taylor D. Restarting clozapine after neutropenia: evaluating the possibilities and practicalities. CNS Drugs 21(1), 25–35 (2007).
57 Pui-yin CJ, Shiu-yin CC, Chung KF, Lai-wah DE, Wai-nang TO, Chan WF. The incidence and characteristics of clozapine-induced fever in a local psychiatric unit in
Hong Kong. Can. J. Psychiatry 53(12), 857–862 (2008).
58 Jeong SH, Kim JH, Ahn YMet al. A 2-year prospective follow-up study of lower urinary tract symptoms in patients treated with clozapine. J. Clin. Psychopharmacol. 28(6), 618–624 (2008).
59 Steingard S. Use of desmopressin to treat clozapine-induced nocturnal enuresis. J. Clin. Psychiatry 55(7), 315–316 (1994).
60 Lurie SN, Hosmer C. Oxybutynin and intranasal desmopressin for clozapine-induced urinary incontinence. J. Clin. Psychiatry 58(9), 404 (1997).
61 McCabe JH, Travis M. Clozapine induced obsessive compulsive symptoms. Prog. Neuropsychopharmacol. Biol. Psychiatry 28(7), 1209 (2004).
62 Englisch S, Zink M. Treatment-resistant schizophrenia: evidence-based strategies. Mens. Sana Monogr. 10(1), 20–32 (2012).
63 Englisch S, Esslinger C, Inta D et al. Clozapine-induced obsessive–compulsive syndromes improve in combination with aripiprazole. Clin. Neuropharmacol. 32(4), 227–229 (2009).
64 Nielsen J, Dahm M, Lublin H, Taylor D. Psychiatrists’ attitude towards and knowledge of clozapine treatment. J Psychopharmacol. 24(7), 965–971 (2010).
65 Mistry H, Osborn D. Underuse of clozapine in treatment-resistant schizophrenia. Adv. Psychiatr. Treat. 17, 250–255 (2011).