Embed Size (px)
Citation preview

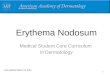
Making Progress with Chronic Venous Leg UlcersA Discussion on Aetiology, Disease Management, and the Role of MeDihoney® Antibacterial Dressings
8.11.07 15.11.07 2.2.08Completely Healed
Pho
to C
redi
ts:
Tave
rnel
li an
d R
eif

Chronic venous insufficiency (CVI) results when the veins in the legs lose the ability to pump venous blood effectively. A range of problems result from leakage of fluid into the interstitial space and the area is then prone to ulceration. Venous ulcers (VU) are chronic skin and subcutaneous ulcerations that occur on the lower leg around the malleolus. Once a venous ulcer develops, venous hypertension and the ulcer itself must be treated together for optimal healing outcomes.
The prevalence of venous ulcers is estimated to be between 0.06% and 2% 2-4 with 1% of the population aged 60 and older being affected at any given time5, 6. Approximately 60% to 70% of all leg ulcers originate from venous disease and occurrence is expected to rise as the population ages.
Annual treatment costs of venous ulcers are estimated to range between £1563624963.16 and £21889000007-9. Treatment costs for individual venous ulcerations have been reported to range between £599.13 to £845.54 per ulcer, with higher costs for the treatment of stalled ulcers (£6057)10. Expenses are not limited solely to the cost of ulcer care, but include other indirect costs associated with disability and lost days of work.
The usual treatment for venous ulcers includes compression therapy for oedema management and topical dressings to promote a moist wound healing environment. Clinicians have described venous ulcers as “hard to heal” and “frustrating”; and the presence or absence of healing has been described as an “emotional roller coaster”11. In general, if a venous wound has not healed by 30% within the first four weeks, it may be unlikely to heal by week 1212. Negative healing rates early in the treatment plan have been associated with non-healing at 24 weeks 13. For wounds that fail to show signs of progress toward healing, the presence of chronic infection should be considered14. Therefore it is imperative to identify hard to heal wounds, and change the treatment plan early in order to achieve the best possible outcome.
The purpose of this venous ulcer guide is to provide a brief overview of chronic venous insufficiency, venous ulceration and standard treatment, followed by the evidence supporting the use of MEDIHONEY® antibacterial active Leptospermum honey (ALH) dressings for stalled venous ulcers15-17.
ChroniC Venous insuffiCienCyWhen veins in the legs lose the ability to pump venous blood effectively, the condition is known as chronic venous insufficiency (CVI). One of the primary causes of CVI is venous hypertension, or high blood pressure in the veins, which damages the vein walls and valves. Other causes of valve damage or malfunction may be due to one of the following: congenital or acquired incompetence, inherent weakness, or thrombotic damage; when there is an outflow obstruction in the deep venous system; or when there is dysfunction of the calf-muscle pump. Venous incompetence may occur in the superficial and deep veins leading to retrograde (backward) blood flow resulting in a range of problems including varicose veins, oedema, and venous ulcers. (Figure 1)
risk faCtorsThe following risk factors for CVI have been identified: trauma, deep vein thrombosis, prolonged inactivity, family history of venous disease, obesity, and clotting disorders18.
CharaCteristiCsA patient may present with pitting oedema around the ankle and lower leg as the day progresses. Over time, red blood cells leak out of the capillaries into the tissue resulting in a brown discolouration, or haemosiderin staining, in the gaiter area of the leg. Atrophie blanche, or painful, white atrophic plaques, may be present around the ankle or foot. Over time the oedematous tissue of the lower extremity may develop stasis dermatitis (erythema and scale) with an accumulation of fibrin in the oedematous tissue resulting in non-pitting hardness (wood-like feel) of the skin in the lower one third of the leg. This results in an inverted champagne-bottle shape of the leg and there may be swelling above and below the area of constriction. (Figure 2)
the Link between CVi and VuThe exact link between CVI and VU is unknown despite years of clinical and laboratory research19. Several hypotheses for the mechanisms leading to ulceration have been suggested and include: (1) pericapillary fibrin cuffs and fibrinolytic abnormalities; (2) trapping of growth factors; and (3) trapping of white blood cells. Some have suggested the following events as leading to ulceration: an abnormal increase in diffusion of substances, such as plasma and erythrocytes, out of the capillaries into the extra vascular space20; fibrinogen passing into the interstitial fluid at a rate significantly faster than normal21 and development of fibrotic tissue as a consequence of fibrin deposition22 which may contribute to an inflammatory process in lipodermatosclerosis23. All of these factors may lead to venous ulcer formation.
Background
Pho
to C
redi
t: W
ebb
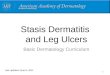
f igu r e 2
Chronic venous insufficiency results in an irregular shape of the leg, similar to an “inverted champagne bottle.”
Normal Venous FunctionValve prevents backwards blood flow
Venous InsufficiencyFaulty valve allows
backwards blood flow
F i g u r e 1

Venous uLCers CharaCteristiCsTypical characteristics of venous ulcers include: an ulcer located on or around the medial malleolus, or the gaitor aspect of the lower legs, above, or just below the ankle which may be shallow and moist with irregular borders. The base of the ulcer may be covered with fibrin like material, appear ruddy red, or yellow, and may have adherent or loose slough. There may be moderate or large amount of exudates and the skin surrounding the ulcer may appear macerated, crusty, and scaling. Haemosiderin (brown) skin staining may be apparent on the lower aspect of the leg. (Figure 3)
Once the skin barrier is breached, microorganisms from the host or the environment contaminate and colonise the ulcer. During the first four weeks the ulcer may be contaminated with normal skin flora, followed by Enterococci, Beta hemolytic streptococci, and Staph aureus. After the first 4 weeks, facultative anaerobic gram negative rods (for example, Proteus spp, Escherichia coli, and Klebsiella spp) colonise the wound14. Eventually, common obligate anaerobic flora (for example, Bacteroides and Peptostreptococcus ssp) populate the ulcer, contributing to a multi-microbial environment14.
Patients with venous ulcers commonly experience pain which is often misunderstood. Pain can be acute or chronic and may continue to exist long after the ulcer is healed. Patients have described their pain as throbbing, burning, sharp, sore, aching, stabbing, and itchy.24-26 When assessing pain, valid and reliable instruments should be used to measure the intensity and quality of pain as well as the impact of pain on quality of life26. Pain may result in gait changes that further result in calf muscle atrophy, and may affect the ability to sleep and function normally. It has also been associated with dissatisfaction with treatment.
Venous uLCer diagnosishistoryAssess the patient for a history of the following: phlebitis, lower leg swelling (oedema), tired or aching legs, trauma, maternal venous ulcer, vigorous exercise, hypercoagulation, multiple pregnancies.
PhysiCaL ex aMAssess for oedema, stasis dermatitis, haemosiderin staining of the gaitor area, lipodermatosclerosis, varicose veins, ulceration on the medial or lateral aspect of the lower leg. If an area of ulceration is present, perform a thorough wound assessment.
differentiaL diagnosis
The following diagnostic tests aid in a differential diagnosis: doppler studies, an ankle-brachial index (ABI) and colour duplex ultrasound testing which is a non-invasive way to accurately evaluate the venous anatomy and physiology.
Venous uLCer treatMentoedeMa ManageMentElevation of the lower extremities to decrease oedema is usually not sufficient to reduce the oedema. If the ABI is greater than 0.8 and the ulcer is determined to be venous in origin, compression therapy is the cornerstone of therapy27.
CoMPression ther aPyCompression therapy has been shown to improve venous ulcer healing rates, decrease recurrence and even prolong the interval between episodes of recurrence28-30. Compression therapy works in a variety of ways. It helps to reduce oedema, decrease venous hypertension, and protect the area from the environment31. Compression therapy decreases venous pressures and assists the calf pump muscle to improve blood flow, and relieve oedema. Some examples of effective interventions include multi-layer compression products such as bandages and stockings, limb elevation, intermittent pneumatic compression therapy devices and exercises.
toPiCaL Venous uLCer ther aPyA physiologically moist healing environment, in combination with sustained multi-layer elastic compression therapy should be provided. Dressings are selected based on the amount of exudates. If absorption is needed for excess wound fluid an absorptive dressing (i.e., Apinate, highly absorbent foam, or super absorbent polymer) can be applied.
MaintenanCe ther aPyOnce the VU has healed, the patient should be encouraged to wear lifelong graduated compression stockings to prevent recurrence.
Venous uLCer heaLingInitial healing rates within the first 4 weeks for venous ulcers can help predict the healing outcome at 12 to 24 weeks12. Healing rates of less than 0.055 cm per week have been associated with non-healing and healing rates greater than 0.1 cm per week have been associated with healing at 24 weeks13. If an ulcer fails to contract or epithelialize over a 2 to 4 week period, the treatment regime should be re-evaluated32 and the presence of chronic infection should be considered14. Studies have demonstrated that wounds that are not 30% smaller within 4 weeks are less likely to heal by week 12. Therefore, it is important to identify non-healing wounds and adjust the treatment plan early to improve outcomes.
Diagnosis and Management
Pho
to C
ourt
esy
of:C
haik
en
Pho
to C
ourt
esy
of:W
ebb
Venous ulcers can have several different characteristics; an ulcer located on or around the medial malleolus (left) and an ulcer(s) appears ruddy red, or yellow, and may have adherent or loose slough (right).
f igu r e 3

Once a wound has not demonstrated a 30% decrease in size by week four the treatment plan should be adjusted to improve healing outcomes. Failure of a wound to heal has been associated with the following factors: larger wound size, longer duration of the wound, a history of venous stripping or ligation, history of hip or knee replacement, an ABI of less than 0.80, more than 50% of the wound area covered in slough33, and chronic infection30. When a wound fails to heal in an orderly and timely fashion it is “stalled” or “stuck” in the inflammatory phase of healing.
A “stalled” wound is characterised by prolonged inflammation, impaired matrix remodeling, defective epithelization, high levels of matrix metalloproteinases (MMP2 and MMP9) which contribute to inflammation and tissue degradation, and chronic inflammation coupled with bacterial colonisation and excessive exudates which further impedes the healing process34.
Delayed healing can also occur due to critical colonisation or infection. Critical colonisation is described as the presence of replicating microorganisms on the surface; infected wounds are defined as those with microorganisms invading the deeper tissues eliciting an inflammatory process accompanied by vasodilation, increased temperature, increased pain, and increased permeability of vessels leading to oedema14. In addition, a link has been demonstrated between the presence of four or more groups of bacteria in leg ulcers and non-healing wounds35.
The overall goal for wound healing is to prepare the wound bed by removing all of the factors that delay healing36 including necrotic tissue, bacterial imbalance, and altered levels and composition of wound exudates.
Medihoney®
MEDIHONEY®, containing active Leptospermum honey (ALH), when added under compression, has been shown to improve healing rates above that of conventional advanced wound care dressings and compression therapy37-40. ALH dressings address the factors that cause delayed healing in chronic wounds, and have demonstrated healing though multiple mechanisms of action including: lowering the pH of the wound, improving O2 diffusion and reducing protease levels41; debriding devitalized tissue37, 40; lowering the bacterial load42-48; maintaining a moist wound healing environment; reducing oedema; and reducing wound re-injury during dressing removal49.
r ationaLe and signif iCanCe of Lowering the ph of ChroniC woundsThe failure of a chronic wound to heal has been correlated with alkaline pH levels. The surface pH of chronic wounds has
been reported to range from 7.15 to 8.950. A recent investigation demonstrated statistically significant decreases in wound pH and a reduction of wound size using ALH dressings 41. A series of 20 patients with chronic, non-healing wounds had their wound size and wound pH measured initially, and after a two-week time period. After application of ALH the mean pH decreased from 7.72 (SD 0.33) to 7.26 (SD 0.53) (< 0.001); each 0.1 decrease in pH was associated with an 8.1 % reduction in wound size (P < 0.012)41.
In addition, another effect of lowering the pH from alkaline toward acidic results in a shift to the right of the oxygen-haemoglobin dissociation curve, resulting in increased oxygen release. Lowering the pH by 0.6 units shifts the curve to the right, causing a release of almost 50% more oxygen and a pH shift from 7.8 to 6.9 has shown a fivefold increase in oxygen releases51.
r ationaLe and aCtion of debrideMentChronic wounds are noted for inflammation, an alkaline environment, oxidative stress, high levels of proteases and slough. Debridement removes these impediments and stimulates the healing process. ALH promotes debridement by autolysis and osmotic activity.
During autolysis the body breaks down tissue or cells. A moist environment aids the body’s own process of loosening and liquefying necrotic tissue.
Use of MEDIHONEY® dressings also creates an osmotic effect which occurs when the high sugar content of honey facilitates movement of fluid from an area of higher concentration to an area of lower concentration. Lymph fluid is drawn from the deeper tissue to the wound surface. The “osmotic effect” aids in cleansing, debridement, and oedema reduction. This constantly replenishes plasminogen at the surface of the wound. Plasminogen is then converted to plasmin which breaks the adhesion of necrotic tissue at the wound surface.
antibaCteriaL effeCts
Leptospermum honey’s antibacterial effect has been documented in-vivo42 and in-vitro54 for many organisms found in leg ulcers even those with antibiotic resistance55. Bacteria commonly associated with delayed leg ulcer healing, including Staphylococcus aureus, Methicillin resistant Staphylococcus aureus (multiresistant and non-multiresistant), Acinetobacter baumannii, Enterococci faecalis (Vancomycin susceptible and Vancomycin resistant), Enterococcus faecium (Vancomycin resistant), Escheriachia coli, Klebsiella pneumoniae, Entero bacter cloacae, and Pseudomonas aeruginosa, are susceptible to MEDIHONEY®56. In addition, researchers have been unable to induce resistance to honey under conditions that would otherwise induce antibiotic resistance57. Investigators have linked the antimicrobial efficacy of MEDIHONEY® to leg ulcer healing42, 43, 57-60.
The Role of MeDihoney®
Medihoney®
MEDIHONEY®, containing active Leptospermum honey (ie. Manuka), when added under compression, has been shown to improve healing rates above that of hydrogel and compression therapy14 (Figure 4). The dressings address the factors that cause delayed healing in chronic wounds, and the dressings have demonstrated healing though multiple mechanisms of action including:
Lowering the pH of the wound, improving O2 diffusion and reducing protease levels41
Fast and selective debridement37, 40
Antibacterial activity 42-48
f igu r e 4

inCLusion CriteriaThe following criteria were used to screen patients prior to including them in the study. Patients from vascular centers in the Ireland were eligible for entry into the study if they were adults with an ankle/brachial systolic blood pressure ratio of (ABI) ≥0.8; if they had a venous ulceration with an area of less than 100cm2 in size and if slough was present in more than 50% of the wound bed. The study was designed to investigate ALH’s ability to clear slough and promote wound healing. Prior to being enrolled in the study the mean ulcer duration was 39.5 weeks for the honey group and 29.9 weeks for the hydrogel group.
PriMary outCoMes
To determine the ability of ALH to deslough wounds after four weeks. To evaluate ALH’s impact on healing at 4 and at 12 weeks.
seCondary outCoMes To determine the decrease in wound size and rate of epithelialisation at week four.
To determine the decrease in MRSA.
treatMent ProtoCoL:Subjects were randomly assigned to a weekly treatment with either ALH (n=54) or hydrogel (n=54). The primary wound dressing was covered with hydrocellular foam and all subjects received sustained multi-layer compression bandages.
evidence Supporting the Use of MeDihoney®
a Large rCt Georgina Gethin, PhD, and Seamus Cowman, MSc, PhD, of the Faculty of Nursing and Midwifery, Royal College of Surgeons in Dublin, Ireland, recently completed a prospective large, multicenter randomized controlled trial of venous ulcer patients16.
A group of 108 patients with a history of non-healing venous ulcerations with greater than 50% slough in the base of the wound were enrolled in a multicenter trial to evaluate the desloughing efficacy and healing outcomes using either active Leptospermum honey (ALH) or hydrogel. Each of the patients had failed to respond to standard compression therapy and had greater than 50% slough covering the wound.
Pho
to C
ourt
esy
of:G
ethi
n
saMPLe Patient in aLh arM of study
figure 5
BEFORE AFTER
resuLtsOne hundred and eight patients with venous leg ulcers were enrolled. At the end of week four there was a 67% reduction in slough in the ALH group (p = 0.05) as compared to a 53% reduction in slough for those in the hydrogel group. The median wound size was smaller at four weeks in the ALH group (p = < 0.001) and the percentage of the VU covered in slough significantly declined in both groups from the baseline to week four (85% to 29% in the honey group; and from 78% to 43% for the hydrogel group).
When looking at the reduction in wound size all wounds decreased by 23% from a baseline of 4.7 cm2 to 3.65 cm2 by week 4. The ALH group demonstrated a 34% size reduction versus 13 % in the hydrogel group; this difference was statistically significant (z = -4.609; p < 0.001). Epithelialisation was noted earlier in the ALH group and this difference was statistically significant (x2 = 9.906; p = 0.042).
When looking at baseline wound cultures, 11 patients had ≥ 3 bacterial species at baseline and 15 had ≥ 3 bacterial species at week four. Staphylococcus aureus was the most common isolate, and MRSA was identified in 16 wounds (10 honey versus 6 hydrogel). After four weeks MRSA was eradicated in 70% (n = 7) of the ALH treated wounds versus 16% (n = 1) of the hydrogel treated wounds 60.
At the end of twelve weeks the percentage of patients healed was higher for ALH patients (44%) than for hydrogel patients (33%).
subjeCt withdr awaL
Subject withdrawals from the study were consistent with other VU studies. The main reasons for patient withdrawal included VU infections (hydrogel, 22%; ALH, 11%) and patient request (5.5% of hydrogel patients; no ALH patients).
ConCLusionsMEDIHONEY® aided in debridement of slough and increased healing of VUs compared to hydrogel.

inCLusion CriteriaAll subjects had confirmed venous incompetence and venous insufficiency with non-healing venous leg ulcers. The wounds had failed to heal (recalcitrant) despite compression therapy and an assortment of therapeutic modalities including topical silver dressings, non-adherent dressings, and topical antibiotic therapy.
treatMent ProtoCoLThe subjects were assigned to weekly treatment with MEDIHONEY® Apinate dressings. All patients received a multi-layer compression bandage.
PriMary outCoMes Wound closure
seCondary outCoMe Restoration of a more normal healing rate
resuLtsComplete wound closure was achieved within three to six weeks for all patients. The authors concluded that the results of this case series confirmed the beneficial effects of MEDIHONEY® on wound healing. An increased velocity of healing with the application of MEDIHONEY® and a 4-layer compression dressing was documented (See Table 1 below).
subjeCt withdr awaLThere were no subject withdrawals in this case series.
ConCLusionsAccelerated wound closure and healing were achieved in all eleven cases with stalled (recalcitrant) venous ulcers who had previously failed to heal with compression therapy and an assortment of therapeutic modalities including topical silver dressings, non-adherent dressings, and topical antibiotic therapy. The dressings demonstrated clinical effectiveness and ease of use.
evidence Supporting the Use of MeDihoney®
eLeVen Patient ConfirMatory Case seriesDr. Jason Hanft, DPM, FACFAS, Director of Podiatric Medical Education, Baptist Health South Florida, and colleagues completed a case series using MEDIHONEY® for eleven patients with recalcitrant venous leg wounds61, 62.
A group of eleven patients with non-healing chronic venous ulcerations were selected and enrolled in a six-week trial to evaluate the evidence of improved healing outcomes with active Leptospermum honey. All patients had delayed wound closure for as little as 4 months and for as long as 4 years. Of these, four exhibited bacterial burden. Each patient had failed to respond to an assortment of therapeutic modalities including four layer compression, topical silver dressings, non-adherent dressings, and topical antibiotic therapy.
1 9.7 4 months Klebsiella pneumoniae, 4 0.346 Enterobacter cloacae
2 6.9 4 years Methicillin- Resistant 4 0.246 Staphylococcus Aureus
3 6.9 4 months No growth 4 0.129
4 6.9 6 months No growth 3 0.168
5 6.9 6 months No growth 5 0.529
6 11.80 22 months Staphylococcus Aureus 5 0.421
7 11.80 8 months No growth 6 0.239
8 4.0 6 months Staphylococcus epidermiditis 4 0.143
9 5.4 19 months No growth 5 0.193
10 3.2 11 months No growth 6 0.114
11 6.2 8 months No growth 4 0.221
Pt # initial wound Prior duration bacterial burden week of wound healing size (cm2) of ulcer Prior to application 100% Closure Velocity per day (cm2)
tab le 1
BEFORE AFTER
Patient 1
Patient 5
BEFORE AFTER
Pho
to C
redi
ts:
Han
ftP
hoto
Cre
dits
: H
anft
f igu r e 6
f igu r e 7

evidence Supporting the Use of MeDihoney®
inCLusion CriteriaAll subjects had chronic venous insufficiency with non-healing venous leg ulcers. The wounds had failed to heal (recalcitrant) despite compression therapy with either Apinate or collagen dressings. Each of the patients had delayed wound closure, pain, inflammation, and periwound oedema.
treatMent ProtoCoLEach patient received weekly sharp debridement followed by application of MEDIHONEY® Apinate dressings. All patients received a multi-layer compression bandage.
PriMary outCoMes
Wound closure
seCondary outCoMes Pain management Inflammation Periwound oedema Serum glucose levels
resuLts
Five of eight patients healed within 6 weeks and the remaining three patients achieved at least 75% wound closure by the end of the 12-week study period (Figure 8). Of the eight patients, five were diabetic and reported no elevation in serum glucose levels during routine glucose monitoring. There was an immediate reduction in size, exudates, and odour, and all patients reported decreased pain. Inflammation and periwound oedema were quickly resolved.
subjeCt withdr awaLThere were no subject withdrawals in this case series.
ConCLusionsAccelerated wound closure and healing were achieved in all eight patients with stalled (recalcitrant) venous ulcers who had previously failed to heal with compression therapy and alginate or collagen dressings. Each of the patients reported elimination of pain and normal serum glucose levels. Effective management of slough, exudates, and inflammation were noted. The dressing demonstrated clinical effectiveness and ease of use.
evidence Supporting the Use of MeDihoney®
eight Patient ConfirMatory Case seriesDr. Matthew Regulski, DPM, FAPWCA, Director of the Wound Care Center of Ocean County, New Jersey, completed a case series using MEDIHONEY® for eight recalcitrant venous leg ulcers39.
A group of eight patients with non-healing or recurrent chronic venous leg ulcerations were selected and enrolled in a twelve-week trial to evaluate the evidence of improved healing outcomes with active Leptospermum honey. All patients had delayed wound closure, pain, inflammation, and periwound oedema. Each patient had failed to respond to an assortment of therapies including compression therapy, Apinate dressings, and collagen dressings.
f igu r e 8
Pho
to C
redi
ts:
Reg
ulsk
i
week 1 week 2 week 3
saMPLe Patient

goaL: Prepare the wound bed and promote moist wound healing.
aCtions: Educate the patient/caregiver about measures to improve or control symptoms associated with CVI and Venous Ulceration.
Encourage elevation of the legs and increased ambulation or exercises.
Improve mobility and the use of the calf pump muscle.
Evaluate patient for compression therapy.
Maintain skin integrity-moisturise and protect. If ulceration is present, assess for inflammation, swelling, and circulation.
If ulceration is present maintain moist environment for healing or VU pain management
If after 30 days no healing has occurred, reevaluate the plan of care and consider inclusion of MEDIHONEY®.
Medihoney® dressing aPPLiCation and reMoVaL If pain is normally present evaluate pain level and medicate according to the healthcare providers instructions
Wash hands thoroughly
Apply gloves
Assess the wound. Look for signs of healing. Also look for any signs of increased redness, pain, swelling, or heat within or around the wound*.
Cleanse the wound and skin around the wound with sterile saline, sterile water, or other safe wound cleanser.
Dry the skin around the wound by patting gently.
Protect the skin around the wound to avoid maceration. Apply a skin protectant barrier wipe or barrier ointment. (An initial increase in exudates is to be expected as a result of the highly osmotic effect of MEDIHONEY®).
Choose a MEDIHONEY® dressing that is appropriate for the amount of drainage (MEDIHONEY® Apinate dressing for moderate to heavy exudates; MEDIHONEY® Gel Sheet dressing for light to moderate exudates; MEDIHONEY® Wound Gel dressing for light to moderate exudates and wounds that are hard to dress or those that require a wound gel).
Apply the MEDIHONEY® dressing to fit the wound making sure the dressing is in contact with the wound base but not in contact with the periwound skin.
Apply an absorbent cover dressing.
Apply chosen compression therapy (i.e. elastic stockings or bandages, non-elastic bandages, multi-layer bandages, or pneumatic compression) to reduce ambulatory venous pressure and resulting leg oedema after measuring the ankle-brachial pressure index (Do not apply compression therapy to a limb with an ankle brachial index less than 0.8)63.
The frequency of the dressing change will depend on the patient condition and the amount of exudates. With proper management of wound exudates, the dressing has been left in place for up to seven days, as is the case with compression devices or under off-loading devices.
Dressing Change: Remove the dressing gently. If the dressing is difficult to remove, moisten with saline or water. Discard the old dressing in a disposal bag.
* The healthcare provider should be notified if the wound worsens. Report increased redness, pain, swelling,13 or heat on or around the wound.
Sample Guideline for Care:MeDihoney® in the Management of Stalled Venous Ulcers
Re f e Re n C e s
1. Tavernelli, K. and s. Reif, The challenges of chronic venous leg ulcers and how Leptospermum honey can help. 2008, The World Union of the Wound Healing societies. Poster.: Toronto, Canada.2. Goldman, M.P. and A. fronek, The Alexander House Group: consensus paper on venous leg ulcer. Journal Dermatological surgical Oncology, 1992. 18: p. 592-602.3. nelzen, O., D. Bergquist, and A. Lindhagen, Venous and non-venous leg ulcers: clinical history and appearance in a population study. British Journal of surgery, 1994. 81: p. 182-187.4. Phillips, T.J. and J.s. Dover, Leg ulcers. Journal American Academy Dermatology, 1991. 25: p. 965-987.5. Heit, J.A., et al., Trends in the incidence of venous stasis syndrome and venous ulcer: a 25-year population-based study. Journal of Vascular surgery, 2001. 33: p. 1022-1027.6. Cornwall, J.V., C.J. Dore, and J.D. Lewis, Leg ulcers: epidemiology and aetiology. British Journal of surgery, 1986. 73: p. 693-696.7. McGuckin, M. and M. Kerstein, Venous ulcers and family physicians. Advances in skin and Wound Care, 1998. 11: p. 693-696.8. simon, D.A. and C.n. McCollum, Approaches to venous leg ulcer within the community: compression, pinch skin grafts and simple venous surgery. Ostomy/Wound Management, 1996. 42: p. 34-40.9. Lazarus, G.s., et al., Definitions and guidelines for assessment of wounds and evaluation of healing. Archives of Dermatology, 1994. 130: p. 489-493.10. Kumar, R.n., et al., Direct healthcare costs of 4 common skin ulcers in new Mexico Medicaid fee-for-service patients. Advances in skin and Wound Care, 2004. 17(3): p. 143-149.11. Cullen, G.H. and T.J. Phillips, Treatment of venous ulceration. International Wound Journal, 2009. 6(5): p. 367-378.12. Tallman, P., et al., Initial rate of healing predicts complete healing of venous ulcers. Archives of Dermatology, 1997. 133(10): p. 1231-1234.13. sabolinski, M. and V. falanga, Heal rates at 4 weeks in venous ulcers treated with compression are predictive of complete healing by 24 weeks. 1999, Presented at American Academy of Dermatology 57th Annual Meeting: new Orleans, LA.14. Landis, s., et al., Infections in chronic wounds, in Chronic Wound Care: A Clinical source Book for Healthcare Professionals, D.L. Krasner, G.T. Rodeheaver, and R.G. sibbald, editors. 2007, HMP Communications: Malvern, PA.15. Bolton, L., evidence corner: Honey on sloughy venous ulcers. Wounds, 2008. 20(12): p. A13-A14.16. Gethin, G. and s. Cowman, Manuka honey vs. hydrogel-a prospective, open label, multicentre, randomised controlled trial to compare delsoughing efficacy and healing outcomes in venous ulcers. Journal of Clinical nursing, 2008. 18(3): p. 466-474.17. Robson, V., s. Dodd, and s. Thomas, standardized antibacterial honey (MeDIHOney®) with standard therapy in wound care: randomized controlled trial. Journal of Advanced nursing, 2009. 65(3): p. 565-575.18. Patterson, G.K., Vascular evaluation, in Wound Care, C. sussman and B.M. Bates-Jensen, editors. 2001, Aspen Publishers, Inc.: Gaithersburg, MD. p. 177-193.19. Donayre, C.e., Diagnosis and Management of Vascular Ulcers, in Wound Care, C. sussman and B.M. Bates-Jensen, editors. 2001, Aspen Publishers: Gaithersburg, MD.20. franzeck, U.K., et al., Transuctaneous oxygen tension and capillary morphologic characteristics and density in patients with chronic venous incompetence. Circulation, 1984. 70: p. 806-811.21. Wolfe, J.H., M. Morland, and n.L. Browse, The fibrinolytic activity of varicose veins. British Journal of surgery, 1979. 66: p. 185-187.22. neumann, H.A., et al., Transcutaneous oxygen tension in chronic venous insufficiency syndrome. Vasa, 1984. 13: p. 213-219.23. Lees, T.A. and D. Lambert, Patterns of venous reflux in limbs with skin changes associated with chronic venous insufficiency. British Journal of surgery, 1993. 80: p. 725-728.24. Charles, H., Venous leg ulcer pain and its characteristics. Journal of Tissue Viability, 2002. 12: p. 154-158.25. Closs, s.J., e.A. neison, and M. Briggs, Can venous and arterial leg ulcers be differentiated by the characteristics of the pain they produce? Journal of Clinical nursing, 2008. 17.26. nemeth, K.A., et al., Pain in pure and mixed aetiology venous leg ulcers: a three-phase point prevalence study. Journal of Wound Care, 2003. 12: p. 366-340.27. sibbald, R., et al., Bacteriology, inflammation, and healing: A study of nanocrystalline silver dressings in chronic venous leg ulcers. Advances in skin and Wound Care, 2007. 20(10): p. 549-558.28. Blair, s.D., et al., sustained compression and healing of chronic venous ulcers. British Medical Journal, 1988. 297(6657): p. 1159-1161.29. Mayberry, J.C., et al., fifteen-year results of ambulatory compression therapy for chronic venous ulcers. surgery, 1991. 109(5): p. 575-581.30. erickson, C.A., et al., Healing of venous ulcers in an ambulatory care program: the roles of chronic venous insufficiency and patient compliance. Journal of Vascular surgery, 1995. 22(5): p. 629-636.31. Kirsner, R.s., et al., Clinical and economic Outcomes with Graftskin for Hard-to-Heal Venous Leg Ulcers: A single-Center experience. Dermatologic surgery, 2002. 28(1): p. 81-82.32. Brem, H., R.s. Kirsner, and V. falanga, Protocol for the successful treatment of venous ulcers. The American Journal of surgery, 2004. 188(suppl): p. 1s-8s.33. Margolies, D.J., J.A. Berlin, and B.L. strom, Risk factors associated with the failure of a venous leg ulcer to heal. Archives of Dermatology, 1999. 135(8): p. 920-926.34. Chen, W.y.J. and A.A. Rogers, Recent insights into the causes of chronic leg ulceration in venous diseases and implications on other types of chronic wounds. Wound Repair and Regeneration, 2007. 15(4): p. 434-449.35. Trengrove, n.J., et al., Qualitative bacteriology and leg ulcer healing. Journal of Wound Care, 1996. 5(6): p. 277-280.36. enoch, s. and K. Harding, Wound bed preparation: The science behind the removal of barriers to healing. Wounds: A Compendium of Clinical Research and Practice, 2003. 15(7): p. 213-229.37. Gethin, G. and s. Cowman, Manuka honey vs. hydrogel-a prospective, open label, multicentre, randomised controlled trial to compare desloughing efficacy and healing outcomes in venous ulcers. Journal of Clinical nursing, 2008. 18(3): p. 466-474.38. smith, T., J.R. Hanft, and K. Legel, Topical Leptospermum honey in recalcitrant venous leg wounds: A preliminary case series. Advances in skin and Wound Care, 2009.39. Regulski, M., A novel wound care dressing for chronic leg ulcerations. Podiatry Management, 2008. november/December: p. 235-246.40. Robson, V., s. Dodd, and s. Thomas, standardized antibacterial honey (MeDIHOney®) with standard therapy in wound care: randomized clinical trial. Journal of Advanced nursing, 2009: p. 565-575.41. Gethin, G., s. Cowman, and R. Conroy, The impact of Manuka honey dressings on the surface pH of chronic wounds. International Wound Journal, 2008. 5(2): p. 185-194.42. Cooper, R.A., P.C. Molan, and K.G. Harding, Antibacterial activity of honey against strains of staphylococcus aureus from infected wounds. Journal of the Royal society of Medicine, 1999. 92(6): p. 283-285.43. Cooper, R.A., P.C. Molan, and K.G. Harding, The sensitivity to honey of Gram-positive cocci of clinical significance isolated from wounds. Journal of Applied Microbiology, 2002. 93: p. 857-863.44. Allen, K.L., P.C. Molan, and G.M. Reid, A survey of the antibacterial activity of some new Zealand honeys. The Journal of Pharmacy and Pharmacology., 1991. 43(12): p. 817-822.45. Molan, P.C., The antibacterial activity of honey: the nature of the antibacterial activity. Bee World, 1992. 73(1): p. 59-76.46. Willix, D.J., P.C. Molan, and C.G. Harfoot, A comparison of the sensitivity of wound-infecting species of bacteria to the antibacterial activity of manuka honey and other honey. Journal of Applied Bacteriology, 1992. 73(5): p. 388-394.47. Lawrence, J., The effect of honey on staphylococcus aureus. Journal of Wound Care, 1999. 8(10): p. 535.48. Cooper, R. and P. Molan, The use of honey as an antiseptic in managing Pseudomonas infection. Journal of Wound Care, 1999. 8(4): p. 161-164.49. Molan, P., Re-introducing honey in the management of wound and ulcers-theory and practice. Ostomy/Wound Management, 2002. 48(11): p. 28-40.50. Romanelli, M., et al., evaluation of surface pH of venous leg ulcers under Allevyn dressings. 1997, The Royal society of Medicine Press, London.: London.51. Leveen, H., et al., Chemical acidification of wounds. An adjuvant to healing and the unfavorable action of alkalinity and ammonia. Annals of surgery, 1973. 178: p. 745-750.52. Hayes, L.C., Active Leptospermum honey impregnated Apinate dressing facilitates healing in elderly patients with painful chronic wounds unable to tolerate silver containing dressings. 2008, June, Third Congress of Wound Healing societies. Poster.: Toronto, Canada.53. Milne, C.T., Comparison of honey-impregnated alginate dressings to non-impregnated Apinate dressings on wound healing. 2008, April, symposium on Advanced Wound Care. Poster: san Diego, CA.54. Blaser, G., et al., effect of medical honey on wounds colonised or infected with MRsA. Journal of Wound Care, 2007. 16(8): p. 325-328.55. Blair, s.e., et al., The unusual antibacterial activity of medical-grade Leptospermum honey: antibacterial spectrum, resistance and transcriptome analysis. european Journal of Clinical Microbiology & Infectious Diseases, 2009. 28(10): p. 1199-1208.56. George, n. and K. Cutting, Antibacterial honey (MeDIHOney®): in-vitro activity against clinical isolates of MRsA, VRe, and other multi-resistant g\Gram-negative organisms including Pseudomonas aeruginosa. Wounds, 2007. 19(9): p. 231-236.57. Blair, s.e., et al. (2009) The unusual antibacterial activity of medical-grade Leptospermum honey: antibacterial spectrum, resistance, and transcriptome analysis. european Journal of Clinical Microbiology and Infectious Disease 28, 1199-1208 DOI: 10.1007/s10096-009-0763-z.58. Cooper, R., Using honey to inhibit wound pathogens. nursing Times, 2008. 104(3): p. 46-49.59. Cooper, R.A., L. Jenkins, and R. Rowlands, The influence of catalase on the antibacterial activity of honey. 2008, April, symposium on Advanced Wound Care. Poster: san Diego, CA.60. Gethin, G. and s. Cowman, Bacteriological changes in sloughy venous leg ulcers treated with manuka honey or hydrogel: an RCT. Journal of Wound Care, 2008. 17(6): p. 241-247.61. Hanft, J., T. smith, and K. Legel, Topical Active Leptospermum Honey in Recalcitrant Venous Leg Wounds: A Preliminary Case series. April, 2009, The symposium on Advanced Wound Care and Wound Healing society: Dallas, Texas. Oral Abstract Presentation. 62. smith, T., K. Legel, and J.R. Hanft, Topical Leptospermum honey (MeDIHOney®) in recalcitrant venous leg wounds: a preliminary case series. Advances in skin and Wound Care, 2008. 22(2): p. 68-71.63. Wiersema-Bryant, L.A. and B.A. Kraemer, Management of Oedema, in Wound Care, C. sussman and B.M. Bates-Jensen, editors. 2001, Aspen Publishers, Inc.: Gaithersburg, MD. p. 237.