Embed Size (px)
Citation preview
Malaria drug-sensitivity testing:new assays, new perspectivesHarald Noedl1, Chansuda Wongsrichanalai2 and Walther H. Wernsdorfer1
1Dept of Specific Prophylaxis and Tropical Medicine, Institute of Pathophysiology, University of Vienna, Kinderspitalgasse 15,
A-1095 Vienna, Austria2Dept of Immunology and Medicine, Armed Forces Research Institute of Medical Sciences (USAMC-AFRIMS), 315/6 Rajvethi Road,
10400 Bangkok, Thailand
Over the past five decades, the drug resistance of
Plasmodium falciparum has become an issue of utmost
concern. At the same time, in vitro assays for assessing
antimalarial drug sensitivity have become indispens-
able tools for the surveillance of drug resistance and the
planning of therapeutic guidelines. Several new in vitro
assays have been introduced, designed to be easier to
handle than previous tests and allow a faster identifi-
cation of drug-resistant parasites, as well as for simple
evaluation of new drugs. This review examines the vari-
ous new approaches to the in vitro assessment of
malaria drug sensitivity and their limitations.
The efficacy of antimalarial drugs depends primarily ontheir ability to kill malaria parasites by interrupting theiressential life functions, leading to inhibition of multi-plication and allowing the immune system to removedamaged parasites completely from the circulation. Thisefficacy varies according to the susceptibility of eachparasite clone within a natural, often genetically hetero-geneous, population of malaria parasites, and is generallyreferred to as drug sensitivity. With spreading resistanceof Plasmodium falciparum to available treatments in thepast five decades, drug sensitivity has become an issue ofutmost importance for the development of therapeuticguidelines and policies.
Drug resistance has emerged as one of the greatestchallenges facing malaria control today. It has beenimplicated in enhanced mortality from malaria in hyper-and holoendemic areas [1] and in the development of newand expanding foci of falciparum malaria, but above all ithas been identified as a factor in the economic constraintsof malaria control [2]. At a time when malaria parasiteshave developed strategies to evade almost any availableantimalarial treatment, surveillance and prevention ofdrug resistance have become more important thanever before.
Drug resistance
One of the most important factors limiting success in thetreatment of malaria, whether for preventive or forcurative purposes, is the varying response of individualparasites to the drugs used. Parasite populations mayadapt to the introduced chemical environment and thereby
enter the state of drug resistance. They are capable ofpassing on their genetic information to future generationsof drug-resistant malaria parasites. Drug resistance inmalaria has therefore also been defined as the ‘ability of aparasite strain to survive and/or multiply despite theadministration and absorption of a drug given in dosesequal to or higher than those usually recommended, butwithin the limits of tolerance of the subject’ [3]. Anotherreason for failing to clear the parasite from the patient’sbody may be that not enough of the drug, or its activemetabolite, reaches the parasite, an event that is calleddrug failure. Unlike drug resistance, drug failure is aprocess not directly related to the parasite and is almostsolely dependent on the host organism and the propertiesof the drug.
As long as chemotherapy remains a key factor in thefight against malaria, the need for a sound knowledge ofthe efficacy of antimalarial drugs cannot be overempha-sized. Emerging and spreading resistance to an increasingnumber of antimalarial drugs has been a major concernespecially in Asia, but recently also in Africa and SouthAmerica [4]. The limited armory of safe, effective andaffordable antimalarial drugs calls for utmost prudence intheir use [5].
Assessing the drug sensitivity of malaria parasites
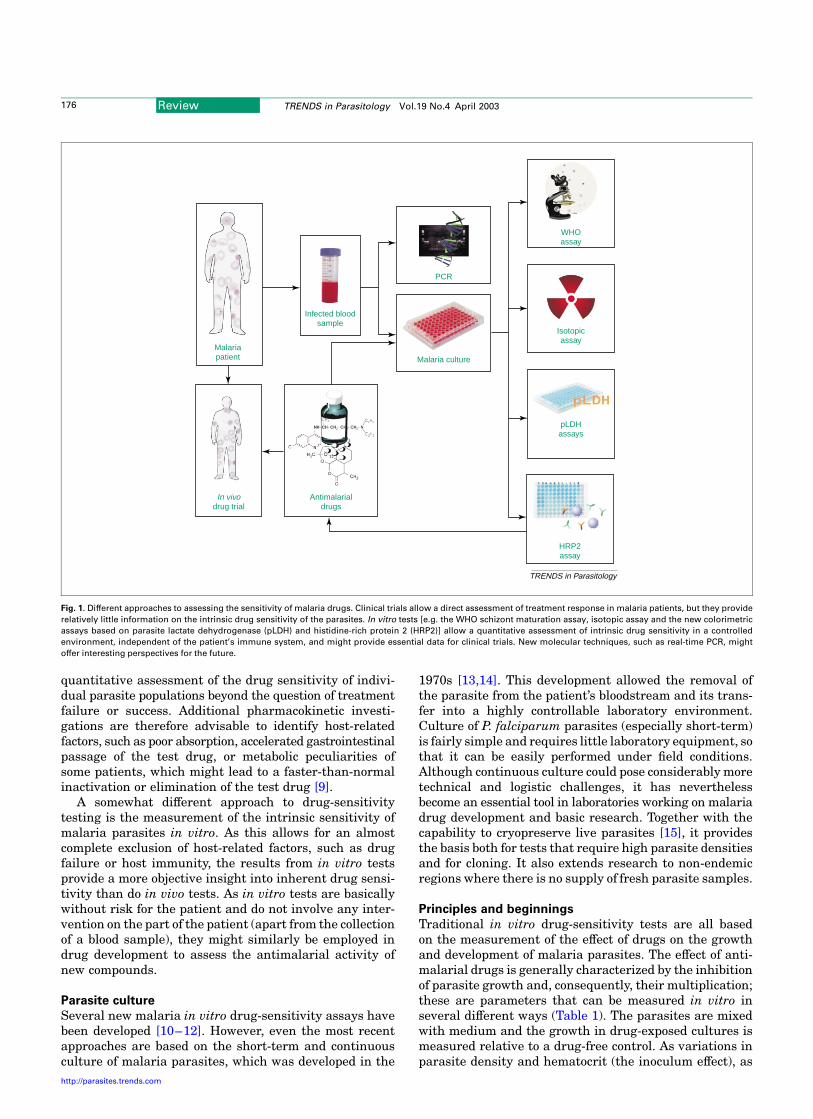
There are several different approaches to the assessmentof P. falciparum susceptibility to antimalarial drugs [6](Fig. 1). The most traditional approach is the assessmentof therapeutic (in vivo) response, which was originallydefined by the WHO in terms of parasite clearance[sensitive (S) and three degrees of resistance (RI, RII,RIII)] [3]. As re-infection is difficult to exclude in areaswith intense malaria transmission, the WHO introduced amodified protocol based on clinical outcome (adequateclinical response, early treatment failure and late treat-ment failure) for areas with intense transmission, whereparasitemia in the absence of clinical signs or symptoms iscommon [7]. The genetic diversity of parasites has beenexploited to develop molecular protocols whereby truerecrudescences could be distinguished from re-infections[8], but these methods add to the cost of in vivo drug-sensitivity studies. All in vivo tests have to be carriedout with set, standard therapeutic doses of drugs withinthe limits of general tolerability. They do not permit aCorresponding author: Harald Noedl ([email protected]).
Review TRENDS in Parasitology Vol.19 No.4 April 2003 175
http://parasites.trends.com 1471-4922/03/$ - see front matter q 2003 Elsevier Science Ltd. All rights reserved. doi:10.1016/S1471-4922(03)00028-X
quantitative assessment of the drug sensitivity of indivi-dual parasite populations beyond the question of treatmentfailure or success. Additional pharmacokinetic investi-gations are therefore advisable to identify host-relatedfactors, such as poor absorption, accelerated gastrointestinalpassage of the test drug, or metabolic peculiarities ofsome patients, which might lead to a faster-than-normalinactivation or elimination of the test drug [9].
A somewhat different approach to drug-sensitivitytesting is the measurement of the intrinsic sensitivity ofmalaria parasites in vitro. As this allows for an almostcomplete exclusion of host-related factors, such as drugfailure or host immunity, the results from in vitro testsprovide a more objective insight into inherent drug sensi-tivity than do in vivo tests. As in vitro tests are basicallywithout risk for the patient and do not involve any inter-vention on the part of the patient (apart from the collectionof a blood sample), they might similarly be employed indrug development to assess the antimalarial activity ofnew compounds.
Parasite culture
Several new malaria in vitro drug-sensitivity assays havebeen developed [10–12]. However, even the most recentapproaches are based on the short-term and continuousculture of malaria parasites, which was developed in the
1970s [13,14]. This development allowed the removal ofthe parasite from the patient’s bloodstream and its trans-fer into a highly controllable laboratory environment.Culture of P. falciparum parasites (especially short-term)is fairly simple and requires little laboratory equipment, sothat it can be easily performed under field conditions.Although continuous culture could pose considerably moretechnical and logistic challenges, it has neverthelessbecome an essential tool in laboratories working on malariadrug development and basic research. Together with thecapability to cryopreserve live parasites [15], it providesthe basis both for tests that require high parasite densitiesand for cloning. It also extends research to non-endemicregions where there is no supply of fresh parasite samples.
Principles and beginnings
Traditional in vitro drug-sensitivity tests are all basedon the measurement of the effect of drugs on the growthand development of malaria parasites. The effect of anti-malarial drugs is generally characterized by the inhibitionof parasite growth and, consequently, their multiplication;these are parameters that can be measured in vitro inseveral different ways (Table 1). The parasites are mixedwith medium and the growth in drug-exposed cultures ismeasured relative to a drug-free control. As variations inparasite density and hematocrit (the inoculum effect), as
Fig. 1. Different approaches to assessing the sensitivity of malaria drugs. Clinical trials allow a direct assessment of treatment response in malaria patients, but they provide
relatively little information on the intrinsic drug sensitivity of the parasites. In vitro tests [e.g. the WHO schizont maturation assay, isotopic assay and the new colorimetric
assays based on parasite lactate dehydrogenase (pLDH) and histidine-rich protein 2 (HRP2)] allow a quantitative assessment of intrinsic drug sensitivity in a controlled
environment, independent of the patient’s immune system, and might provide essential data for clinical trials. New molecular techniques, such as real-time PCR, might
offer interesting perspectives for the future.
TRENDS in Parasitology
HRP2assay
pLDHassays
Isotopicassay
WHOassay
In vivodrug trial
Antimalarialdrugs
Malaria culture
PCR
Infected bloodsample
Malariapatient
Review TRENDS in Parasitology Vol.19 No.4 April 2003176
http://parasites.trends.com

well as the stage-dependent action of antimalarial drugs,may have a significant impact on the outcome of these tests[16,17], it is important to control the culture for parasitedensity, hematocrit and developmental stage of the para-sites whenever possible. When performed with serial dilu-tions of drugs, these tests will generally result in sigmoiddose–response curves. Although the principles are thesame in all of these tests, they differ considerably in thetechnique used to assess parasite growth.
In 1968, Rieckmann et al. [18] described an in vitrodrug-sensitivity test for P. falciparum capable of measur-ing the ability of the parasite to develop from early ringstage to mature schizonts when challenged by increasingconcentrations of chloroquine. This ‘macrotechnique’ wascapable of distinguishing between chloroquine-sensitiveand -resistant parasite isolates by using morphologicalchanges to monitor the effect of antimalarials on parasitematuration. Ten years later, the assay was further deve-loped to produce a microculture procedure for measuringthe inhibition of schizont maturation in a 24-hour test, the‘microtest’, which remains one of the most common tech-niques for the assessment of drug sensitivity in vitro [19].
Schizont maturation
The first test to use schizont maturation as a measureof parasite growth was the macrotest, which has severallimitations, owing primarily to the suboptimal culture con-ditions used in this assay. The microtest, which followedthe macrotest, overcomes many of these disadvantages byadapting several elements from the continuous culture,which was first available in 1976 [13,14]. Schizont matu-ration assays are relatively simple to perform [20]. Theyrequire little technical equipment, can be used even forsamples with low parasite densities, and usually requireonly 24 h of incubation. Schizonts are counted against thetotal number of parasites on thick films prepared from thecellular layer of the cultured samples. However, as this is alabor-intensive procedure, schizont maturation assays aregenerally not very popular with microscopists and theotherwise undisputed economy of the assay vanishes whentechnicians have to be paid by Western standards. Inaddition, schizont maturation tests require highly trainedpersonnel to limit individual variability in counting andassessing the developmental stages of the parasites.
Using schizont maturation as the endpoint of parasitegrowth elegantly avoids the problem of backgroundgrowth that is associated with most other techniques by
excluding all previous stages. However, this might alsoresult in a loss of data. Parasites that grow from ring tolate-trophozoite stage, yet do not reach the schizont stagewithin 24 h, contribute the same weight as parasites thatdo not show any development at all. Drugs that lead to aminor but consistent slowdown of parasite growth, suchas certain antibiotics, might theoretically give the sameresults as drugs that completely inhibit parasite growth.Furthermore, drugs that exert their action primarilyduring later stages of parasite development, such asthe combination of sulfadoxine and pyrimethamine,might be difficult to measure in assays that are limitedto 24 h of incubation.
Measuring parasitemia
Analogous to schizont maturation assays, the parasitegrowth may also be measured by assessing the increase inthe percentage of infected red blood cells in the culture.Soon after the introduction of continuous in vitro cultiva-tion of P. falciparum [10], several drug-sensitivity assayswere developed based on the measurement of the increasein parasitemia during a culture period of 48–96 h [21–23].As these methods involve longer incubation times, they areapplicable to most blood schizontocidal antimalarials,irrespective of the speed and stage specificity of theiraction. However, reading of the test results remains par-ticularly labor intensive and, owing to the natural limita-tions of microscopy, is prone to variability of interpretation.Methods have therefore been developed that allow anautomatic reading of drug-sensitivity tests in a flow cyto-meter [24,25], but these tests require highly sophisticatedlaboratory equipment. A different approach is the assess-ment of parasite growth using DNA stains, which allowsfor a relatively simple reading of the results [26].
Isotopic assays
Desjardins et al. [27] developed an in vitro drug-sensitivityassay based on the incorporation of tritium-labeled hypo-xanthine. As an alternative to using radiolabeled hypo-xanthine, Elabbadi et al. proposed ethanolamine [28],which has the major advantage that the culture mediumcan be supplemented with hypoxanthine, resulting inimproved parasite growth. Several other precursors(e.g. palmitate, serine, choline, inositol and isoleucine)have also been suggested for use in isotopic assays.
These assays allow a fairly high degree of automatiz-ation and are therefore considerably faster to perform than
Table 1. Comparison of the most common assays for the measurement of the drug sensitivity of Plasmodium falciparum parasites
in vitroa
WHO microtest Isotopic assays pLDH enzymatic assay pLDH DELI assay HRP2 assay
Sensitivityb High Moderate Low High High
Culture time 24 h 42 h (up to 72 h) 48 h 48 h 48–72 h
Assessment of growth
inhibition
Microscopy (schizont
maturation)
Incorporation of radio-
labeled precursors
Enzymatic activity of pLDH pLDH ELISA HRP2 ELISA
Demands on equipment Low (microscope) High (scintillation counter) Moderate (plate reader) Moderate (ELISA plate
reader)
Moderate (ELISA plate
reader)
Amount of labour
involvedb
High Low Low Moderate Low
Year first published; Ref. 1978 [19] 1979 [27] 1993 [10] 2001 [11] 2002 [12]
aAbbreviations: DELI, double-site enzyme-linked LDH immunodetection; HRP2, histidine-rich protein 2; pLDH, parasite lactate dehydrogenase.bThe values (high, moderate and low) given indicate relative levels between the different assays.
Review TRENDS in Parasitology Vol.19 No.4 April 2003 177
http://parasites.trends.com

are tests based on the morphological assessment of para-site growth. Automatic reading of the test results con-siderably reduces the influence of the variability caused byhuman factors. The assays are well suited for screening ofantimalarial candidate compounds. Furthermore, theypermit longer and variable incubation times, allowingthe testing of a large variety of drugs. The fact that themeasurement of the metabolic activity is limited to thesecond half of the culture period ensures a low and stablebackground.
However, this technique also has its limitations, theforemost being its use of isotopic material. Since the late1970s, the regulations regarding the handling of radio-active material have become considerably more restrictive,essentially aiming at limiting the application to domainswhere there is no alternative to their use. In many otherfields, isotopic assays have therefore been replaced byother tests. Another limitation is the high purchase costof the equipment, such as liquid scintillation countersand harvesting machines. In addition, the relatively highparasite densities of approximately 0.5% required for thistest limits its application to the use of culture-adaptedparasite strains or field samples with adequately highparasitemia.
Parasite lactate dehydrogenase
Parasite lactate dehydrogenase (pLDH) is a terminalenzyme in the Embden–Meyerhof pathway (glycolysis) ofthe malaria parasite [29]. Its production and accumulationcan be used both in vivo and in vitro as indices of parasiteviability. pLDH was one of the first plasmodial enzymesshown to be electrophoretically, immunologically and kine-tically distinct from that of the host [30]. It was usedprimarily as an indicator for the presence of malariaparasites [31]. The levels of pLDH correspond to the para-site density upon initial diagnosis [29] and show a rapiddecrease with the initiation of treatment and the resultinglower parasite densities [32]. pLDH plays an importantrole in the anerobic carbohydrate metabolism of humanmalaria parasites. As malaria parasites principally relyon anerobic glycolysis, they require the regeneration ofnicotinamide adenine dinucleotide (NAD) for the continuousflux of glucose through this pathway [33].
On the basis of the knowledge that pLDH activity isdistinguishable from host LDH activity using the 3-acetylpyridine adenine dinucleotide analog of NAD (APAD),Makler et al. developed a drug-sensitivity assay thatdetermines inhibition profiles by measuring the enzymaticactivity of pLDH [10]. Pyruvate is formed from L-lactase inthe presence of LDH and APAD coenzyme. This reactionresults in the formation of reduced APAD, which in turnreduces blue tetrazolium, forming a blue formazan productthat can be measured by spectrophotometry. However, theassay requires initial parasite densities of 1–2% and, insubsequent tests with fresh parasite isolates, was found tobe too insensitive for field application [34].
The limitations associated with this test led to thedevelopment of a new pLDH-based assay that measurespLDH levels in a double-site enzyme-linked LDH immuno-detection (DELI) assay that was made possible by thedevelopment of monoclonal antibodies (mAbs) specific for
pLDH, making this test considerably more sensitive [11,35].The DELI assay is equally applicable to the detection ofparasites for diagnostic purposes as to drug-sensitivitytesting. Studies from the same group suggest that, unlikeits predecessor, the assay is also field applicable and theresults are comparable with those obtained by isotopicassay [36,37]. However, limited supplies of mAbs haveconstrained the further validation and application ofthe DELI assay.
Histidine-rich protein II
The most recent addition to the list of in vitro drug-sensitivity tests for P. falciparum is based on the measure-ment of a histidine- and alanine-rich protein produced byP. falciparum in the course of its growth and multipli-cation: histidine-rich protein 2 (HRP2) [12]. Similar to theDELI test, this assay is based on methods originallydeveloped for the diagnosis of falciparum malaria [38]. It is,10 times more sensitive than the isotopic assay andrequires little technical equipment. HRP2 levels are closelyassociated with parasite density and development [39,40].The HRP2 assay uses a longer culture time than mostother assays (72 h instead of 48 h), which also allows thetesting of slow-acting drugs without changes in the proto-col. Parasite growth and development is assessed bymeasuring the production of HRP2 in a simple, commer-cially available, double-site sandwich, ELISA test kit (oressentially any ELISA that is specific to HRP2). Thestability and persistence of HRP2, which can be a majorproblem in predicting clinical treatment outcome usingmalaria rapid-diagnostic tests (dipsticks) [41], turnsinto an advantage when using HRP2 for in vitro drug-sensitivity assays, as it provides a highly stable back-ground. The background can be excluded by subtracting acontrol value taken after 24 h from all results, therebylimiting the measurement of parasite growth to the laterpart of the culture. The data suggest that the resultsobtained with the HRP2 assay are comparable with thoseobtained by the WHO microtest and the isotopic assays.The assay works well with clones and laboratory strainsof falciparum parasites, and is currently being testedwith field isolates.
Advantages such as the relative ease of imple-mentation, the possibility of replacing isotopic tests, andthe reduced requirements for laboratory equipment andtraining of personnel might make this new generation ofELISA-based drug-sensitivity tests a promising alterna-tive for the future and could contribute to a revivedinterest in utilizing in vitro assays as a tool for anti-malarial resistance surveillance. However, the amount ofdata published so far is too limited to determine whetherthese tests will have the potential to replace traditionalassays completely. As ELISA-based tests are easy andrapid to perform, even with large numbers of samples, theyare also well suited for the screening of candidate drugs.Several other applications for these tests are also conceiv-able, such as bioassays or their use in vaccine development.
Plasmodium vivax
As yet, drug resistance in P. vivax has not gained the sameattention as that of P. falciparum and, until little more
Review TRENDS in Parasitology Vol.19 No.4 April 2003178
http://parasites.trends.com

than 10 years ago, it was generally understood thatchloroquine could be trusted to produce a clinical, para-sitological cure of an acute attack of vivax malaria.However, high levels of chloroquine resistance havesince been documented in western Oceania and Indonesia[42–44]. Because of its ability to produce relapse fromhypnozoites, drug sensitivity of P. vivax is considerablymore difficult to assess by in vivo tests as compared withP. falciparum [6]. Unfortunately, attempts to establishP. vivax in continuous culture have essentially failed so far.Nevertheless, short-term culture of P. vivax was reportedmany years ago [45,46] and is relatively simple to perform.By adapting methods used for drug-sensitivity testing ofP. falciparum, several assays have been developed, basedmostly on morphological assessment of schizont matu-ration [47,48]. However, the presence of different asexualforms of P. vivax in natural parasite populations has longbeen recognized as a problem requiring particular atten-tion in the evaluation of such tests. This approach recentlyled to a morphological P. vivax drug-sensitivity test using amore elaborate evaluation system that allows for morpho-logical growth assessment without requiring fully syn-chronized samples [49,50]. The measurement of theenzymatic activity of genus-specific pLDH as a measureof growth, although feasible in theory, turned out to requireparasite densities that were too high to be applicable toP. vivax [34]. ELISA-based drug-sensitivity assays, similarto those for P. falciparum, could therefore provideinteresting alternatives for P. vivax drug-sensitivitytesting in the future.
Molecular techniques
Following the availability of molecular techniques, severalmarkers have been investigated for their association withantimalarial drug resistance. The recent introduction ofreal-time polymerase chain reaction (PCR) into malariaresearch could offer interesting perspectives for the future[51,52]. The association between pyrimethamine resist-ance and point mutations on the dihydrofolate reductase(dhfr) gene, as well as sulfadoxine resistance and pointmutations on the dihydropteroate synthetase (dhps) gene,are the most well documented [4,54]. A recent study sug-gests that the presence of a single dhfr mutation (Arg59)with a single dhps mutation (Glu540) might be a usefulpredictor of high-degree sulfadoxine–pyrimethamine (SP)resistance [55]. Molecular surveillance of SP resistanceis of significant importance for East Africa, where it isspreading. Substitution of threonine for lysine at position76 (T76) on the chloroquine resistance transporter ( pfcrt)gene is known to be a key determinant of chloroquineresistance. Although its presence is not a useful predictorof chloroquine resistance in vivo, especially amongsemi-immune individuals, its absence is highly predictiveof chloroquine sensitivity. Molecular surveillance ofchloroquine-resistant P. falciparum by collecting blooddots on filter paper has been initiated in Africa [56,57]. Inaddition, genetic data might provide valuable informationfor the identification of new drug or vaccine targets.
Available evidence suggests the roles of the multidrug-resistance gene 1 (pfmdr1) on the resistance of P. falciparumto several blood schizonticides including chloroquine,
mefloquine, quinine and artemisinin. The presence ofAsn86, Tyr184, Ser1034 and Asn1042 (wild-type) orAsn86, Phe184, Ser1034 and Asn1042 was found to beassociated with increased resistance to mefloquine inSoutheast Asia (A.L. Pickard, unpublished). Thesemarkers might play an important role in trackingmefloquine resistance in the region.
The precise relationships between particular poly-morphisms and specific drugs have yet to be elucidated[53]. Currently, several obstacles remain, such as markedregional differences or contradicting reports of the signi-ficance of individual markers. If these difficulties can beovercome, molecular techniques could become an extremelyvaluable tool for the detection of drug resistance andcould also help uncover the geographical origins of drugresistance [2,58].
Applications and limitations
Can in vitro tests provide guidelines for changes in publichealth policies? As the results of in vitro tests are essen-tially quantitative, they allow a simple comparison of dataoriginating from different geographical regions or fromdifferent points in time. Once established, regular in vitromonitoring is easier to accomplish than in vivo tests and,consequently, allows an earlier detection of changes in drugsusceptibility. Therefore, they are particularly well suited toprovide guidelines for public health policies. Furthermore,they are indispensable tools in the basic research, drugdevelopment and epidemiology of drug resistance.
Can in vitro tests replace clinical trials? Clinical trialscan provide a plethora of parameters that are essential forthe application of antimalarial drugs and that cannot beassessed by in vitro tests. The results obtained from in vitrodrug-sensitivity tests do not necessarily reflect the clinicaloutcome of malaria therapy as this is not merely depen-dent on the intrinsic drug sensitivity of the pathogen, butis also dependent on several host-related factors such asthe immune status of the patient. Although the immunestatus of individuals might at first sight seem to be anobstacle to determining the specific drug response ofparasite populations, it is also an essential factor in settingtreatment guidelines for communities in malaria-endemicregions. However, it is also important that in vivo testscover non-immune patients, such as children or migrantsfrom non-endemic regions, which are considerably moreaffected by antimalarial drug resistance, an aim that couldbe difficult to achieve. Ideally in vivo and in vitro testscomplement one another: they are not alternatives andtherefore in vitro tests cannot replace clinical trials.
The ordeal of choice
The abundance of available drug-sensitivity assays obviouslyleaves the researcher with the difficulty of choice. Both theWHO microtest and the isotopic assays have proven theirreliability in their respective discipline after more thantwo decades of use: the WHO assay in the field, the isotopicassay in well-equipped research laboratories. However,both assays are associated with serious drawbacks: theWHO assay with the subjectivity of the results and theamount of labor involved; the isotopic assay with the lackof sensitivity and with the fact that it involves the
Review TRENDS in Parasitology Vol.19 No.4 April 2003 179
http://parasites.trends.com

handling of radioactive material. The new colorimetricassays (DELI and HRP2 assays) overcome many of thesedisadvantages and might currently be the methods ofchoice. They are sensitive, relatively simple and quick toperform, do not require highly specialized equipment, andhave the potential to replace traditional assays. However,they are still a long way from the ‘drug resistance dipstick’.As more information on the genetic background of resist-ance becomes available, and as new and improved tools(such as real-time PCR) are developed, molecular tech-niques might become an extremely valuable tool for thesurveillance and early detection of antimalarial drugresistance in the future.
Conclusions
The rapid progression of antimalarial drug resistance inrecent years has made surveillance of drug sensitivity allthe more important. High priority should be given to newassays that facilitate and accelerate the accurate assess-ment of the drug response, strategies limiting the spreadof antimalarial drug resistance, and the development ofnovel antimalarial compounds and vaccines. The relativeease with which some of the new in vitro drug-sensitivityassays can be used, together with their ready availability,could lead to a renewed interest in this essential researchfield. Given the limited resources for malaria controlmeasures and drug development, the considerate useof available resources is essential. The newest generationof drug-sensitivity assays might provide one step inthis direction.
References
1 Trape, J.F. et al. (2002) Combating malaria in Africa. Trends Parasitol.18, 224–230
2 Bloland, P. (2001) Drug Resistance in Malaria. WHO/CDS/DRS.4.Geneva, WHO
3 World Health Organization (1973) Chemotherapy of Malaria andResistance to Antimalarials. Report of a WHO scientific group. WHOTechnical Report Series, No. 529. Geneva, WHO
4 Sibley, C.H. et al. (2001) Pyrimethamine-sulfadoxine resistance inPlasmodium falciparum: what next? Trends Parasitol. 17, 582–588
5 Winstanley, P.A. (2000) Chemotherapy for falciparum malaria: thearmoury, the problems and the prospects. Parasitol. Today 16,146–153
6 White, N.J. (2002) The assessment of antimalarial drug efficacy.Trends Parasitol. 18, 458–464
7 World Health Organization (1996) Assessment of Therapeutic Efficacyof Antimalarial Drugs for Uncomplicated Falciparum Malaria inAreas With Intense Transmission. WHO/MAL/96.1077. Geneva, WHO
8 Snounou, G. and Beck, H.P. (1998) The use of PCR genotyping in theassessment of recrudescence or reinfection after antimalarial drugtreatment. Parasitol. Today 14, 462–467
9 Wernsdorfer, W.H. and Payne, D. (1988) Drug sensitivity tests inmalaria parasites. In Malaria. Principles and Practice of Malariology(Wernsdorfer, W.H. and McGregor, I., eds), pp. 1765–1800, ChurchillLivingstone
10 Makler, M.T. et al. (1993) Parasite lactate dehydrogenase as an assayfor Plasmodium falciparum drug sensitivity. Am. J. Trop. Med. Hyg.48, 739–741
11 Druilhe, P. et al. (2001) A colorimetric in vitro drug sensitivity assay forPlasmodium falciparum based on highly sensitive double-site pLDHantigen capture ELISA. Am. J. Trop. Med. Hyg. 64, 233–241
12 Noedl, H. et al. (2002) Histidine rich protein II, a novel approach toantimalarial drug susceptibility testing. Antimicrob. Agents Che-mother. 46, 1658–1664
13 Trager, W. and Jensen, J.B. (1976) Human malaria parasites incontinuous culture. Science 193, 673–675
14 Haynes, J.D. et al. (1976) Culture of human malaria parasitesPlasmodium falciparum. Nature 263, 767–769
15 Diggs, C. et al. (1975) Protein synthesis in vitro by cryopreservedPlasmodium falciparum. Am. J. Trop. Med. Hyg. 24, 760–763
16 Duraisingh, M.T. et al. (1999) Inoculum effect leads to overestimationof in vitro resistance for artemisinin derivatives and standardantimalarials: a Gambian field study. Parasitology 119, 435–440
17 Zhang, Y. et al. (1986) Stage-dependent inhibition of chloroquine onPlasmodium falciparum in vitro. J. Parasitol. 72, 830–836
18 Rieckmann, K.H. et al. (1968) Effects of chloroquine, quinine, andcycloguanil upon the maturation of asexual erythrocytic forms of twostrains of Plasmodium falciparum in vitro. Am. J. Trop. Med. Hyg. 17,661–671
19 Rieckmann, K.H. et al. (1978) Drug sensitivity of Plasmodiumfalciparum. An in vitro micro technique. Lancet i, 22–23
20 World Health Organization (1990) In vitro Micro-Test (Mark II) for theAssessment of the Response of Plasmodium falciparum to Chloroquine,Mefloquine, Quinine, Sulfadoxine/Pyrimethamine and Amodiaquine.WHO/MAP/87.2, Rev.1. Geneva, WHO
21 Richards, W.H. and Maples, B.K. (1979) Studies on Plasmodiumfalciparum in continuous cultivation. I. The effect of chloroquine andpyrimethamine on parasite growth and viability. Ann. Trop. Med.Parasitol. 73, 99–108
22 Nguyen-Dinh, P. and Trager, W. (1980) Plasmodium falciparumin vitro: determination of chloroquine sensitivity of three new strainsby a modified 48-hour test. Am. J. Trop. Med. Hyg. 29, 339–342
23 Nguyen-Dinh, P. and Payne, D. (1980) Pyrimethamine sensitivity inPlasmodium falciparum: determination in vitro by a modified 48-hourtest. Bull. WHO 58, 909–912
24 van Vianen, P.H. et al. (1990) Automated flow cytometric analysis ofdrug susceptibility of malaria parasites. Am. J. Trop. Med. Hyg. 43,602–607
25 Saito-Ito, A. et al. (2001) A rapid, simple and sensitive flow cytometricsystem for detection of Plasmodium falciparum. Parasitol Int. 50,249–257
26 Smeijsters, L.J. et al. (1996) Simple, fast, and accurate fluorometricmethod to determine drug susceptibility of Plasmodium falciparumin 24-well suspension cultures. Antimicrob. Agents Chemother. 40,835–838
27 Desjardins, R.E. et al. (1979) Quantitative assessment of anti-malarialactivity in vitro by a semi-automated microdilution technique.Antimicrob. Agents Chemother. 16, 710–718
28 Elabbadi, N. et al. (1992) Use of radioactive ethanolamine incorpor-ation into phospholipids to assess in vitro antimalarial activity bythe semiautomated microdilution technique. Antimicrob. AgentsChemother. 36, 50–55
29 Makler, M.T. and Hinrichs, D.J. (1993) Measurement of the lactatedehydrogenase activity of Plasmodium falciparum as an assessment ofparasitemia. Am. J. Trop. Med. Hyg. 48, 205–210
30 Sherman, I.W. (1961) Heterogeneity of lactic dehydrogenase in avianmalaria (Plasmodium lophurae). J. Exp. Med. 114, 1049–1062
31 Piper, R. et al. (1999) Immunocapture diagnostic assays for malariausing Plasmodium lactate dehydrogenase (pLDH). Am. J. Trop. Med.Hyg. 60, 109–118
32 Oduola, A.M. et al. (1997) Plasmodium falciparum: evaluation oflactate dehydrogenase in monitoring therapeutic responses to stan-dard antimalarial drugs in Nigeria. Exp. Parasitol. 87, 283–289
33 Sherman, I.W. (1998) Carbohydrate metabolism in asexual stages. InMalaria. Parasite Biology, Pathogenesis, and Protection (Sherman,I.W., ed.), pp. 135–144, ASM Press
34 Basco, L.K. et al. (1995) Plasmodium falciparum and Plasmodiumvivax: lactate dehydrogenase activity and its application for in vitrodrug susceptibility assay. Exp. Parasitol. 80, 260–271
35 Piper, R. et al. (1999) Immunocapture diagnostic assays for malariausing Plasmodium lactate dehydrogenase (pLDH). Am. J. Trop. Med.Hyg. 60, 109–118
36 Moreno, A. et al. (2001) Evaluation under field conditions of thecolourimetric DELI-microtest for the assessment of Plasmodiumfalciparum drug resistance. Trans. R. Soc. Trop. Med. Hyg. 95,100–103
37 Moreno, A. et al. (2001) Use of the DELI-microtest to determine thedrug sensitivity of Plasmodium falciparum in Burkina Faso. Ann.Trop. Med. Parasitol. 95, 309–312
Review TRENDS in Parasitology Vol.19 No.4 April 2003180
http://parasites.trends.com

38 Wongsrichanalai, C. (2001) Rapid diagnostic techniques for malariacontrol. Trends Parasitol. 17, 307–309
39 Desakorn, V. et al. (1997) Semi-quantitative measurement of Plasmo-dium falciparum antigen PfHRP2 in blood and plasma. Trans. R. Soc.Trop. Med. Hyg. 91, 479–483
40 Howard, R.J. et al. (1986) Secretion of a malarial histidine-rich protein(Pf HRP II) from Plasmodium falciparum-infected erythrocytes. J. CellBiol. 103, 1269–1277
41 Mayxay, H. et al. (2001) Persistence of Plasmodium falciparum HRP-2in successfully treated acute falciparum malaria. Trans. R. Soc. Trop.Med. Hyg. 95, 179–182
42 Fryauff, D.J. et al. (1998) Chloroquine-resistant Plasmodium vivaxin transmigration settlements of West Kalimantan, Indonesia.Am. J. Trop. Med. Hyg. 59, 513–518
43 Rieckmann, K.H. et al. (1989) Plasmodium vivax resistance tochloroquine? Lancet ii, 1183–1184
44 Baird, J.K. et al. (1996) Survey of resistance to chloroquine byPlasmodium vivax in Indonesia. Trans. R. Soc. Trop. Med. Hyg. 90,409–411
45 Bass, C.C. and Johns, F.M. (1912) The cultivation of materialplasmodia (Plasmodium vivax and Plasmodium falciparum) in vitro.J. Exp. Med. 16, 567–579
46 Chotivanich, K. et al. (2001) Ex-vivo short-term culture and develop-mental assessment of Plasmodium vivax. Trans. R. Soc. Trop. Med.Hyg. 95, 677–680
47 Brockelman, C.R. et al. (1989) Development of in vitro microtest for theassessment of Plasmodium vivax sensitivity to chloroquine. SoutheastAsian J. Trop. Med. Public Health 20, 41–47
48 Russel, B.M. et al. Simple in vitro assay for determining the sensitivityof P. vivax isolates from fresh human blood to antimalarials in areaswhere P. vivax is endemic. Antimicrob. Agents Chemother. (in press)
49 Tasanor, O. et al. (2002) An in vitro system for assessing the sensitivityof Plasmodium vivax to chloroquine. Acta Trop. 83, 49–61
50 Congpuong, K. et al. (2002) Sensitivity of Plasmodium vivax tochloroquine in Sa Kaeo Province, Thailand. Acta Trop. 83, 117–121
51 Lee, M.A. (2002) Real-time fluorescence-based PCR for detection ofmalaria parasites. J. Clin. Microbiol. 40, 4343–4345
52 Hermsen, C.C. (2001) Detection of Plasmodium falciparum malariaparasites in vivo by real-time quantitative PCR. Mol. Biochem.Parasitol. 118, 247–251
53 Nzila, A.M. et al. (2000) Towards an understanding of the mechanismof pyrimethamine-sulfadoxine resistance in Plasmodium falciparum:genotyping of dihydrofolate reductase and dihydropteroate synthase ofKenyan parasites. Antimicrob. Agents Chemother. 44, 991–996
54 Wongsrichanalai, C. et al. (2002) Epidemiology of drug-resistantmalaria. Lancet Infect Dis. 2, 209–218
55 Kublin, J.G. et al. (2002) Molecular markers for failure of sulfadoxine-pyrimethamine and chlorproguanil-dapsone treatment of Plasmo-dium falciparum malaria. J. Infect. Dis. 185, 380–388
56 Djimde, A. et al. (2001) A molecular marker for chloroquine-resistantfalciparum malaria. N. Engl. J. Med. 344, 257–263
57 Djimde, A. et al. (2001) Application of a molecular marker forsurveillance of chloroquine-resistant falciparum malaria. Lancet358, 890–891
58 Wellems, T.E. and Plowe, C.V. (2001) Chloroquine-resistant malaria.J. Infect. Dis. 184, 770–776
Books on parasitology
Malaria and Rome: A History of Malaria in Ancient Italyby Robert Sallares, Oxford University Press; 2002.
US$ 75.00 (hbk) (250 pages) ISBN 0199248508
A comprehensive book on the history of malaria in Roman Italy.
Adaptive Dynamics of Infectious Diseases: In Pursuit of Virulence
ManagementEdited by Ulf Dieckmann, Johan A. J. Metz, Maurice W. Sabelis and
Karl Sigmund,
Cambridge University Press, 2002.
US$ 80.00 (hbk) (532 pages) ISBN 0521781655
This book examines the concepts and techniques behind mathematical evolutionary
modelling and disease management.
Review TRENDS in Parasitology Vol.19 No.4 April 2003 181
http://parasites.trends.com