-
COUNTRY BRIEFING
Eliminating malaria in INDONESIA
APRIL 2012 1
Indonesia is seeking to eliminate malaria island by island as it
works toward national malaria elimination by 2030.
Overview Indonesia, a large archipelago, is the fourth most
popu-lous country in the world. Indonesia has a long history of
research and ingenuity in malaria control. The country has
experienced a 53 percent decrease in confirmed malaria cases
between 2005 and 2010, from 437,323 cases to 229,819 cases.1 Four
species of malaria parasites infect humans in Indonesia: Plasmodium
falciparum, P. vivax, P. malariae, and P. ovale; P. falciparum
accounts for 53 percent of infections.1 P. falciparum and P. vivax
mixed infections are very common, while P. malariae and P. ovale
infections are rare. The malaria disease burden and parasite
distribution in Indonesia is geographically asymmetrical, as most
cases are found in the eastern part of the nation. Drug-resistant
P. falciparum is a major issue in Indonesian Papua and other
eastern provinces; drug resistance is starting to become a
challenge in treating P. vivax as well.2 A fifth species, P.
knowlesi, has been discov-ered in Indonesian Borneo, yet no
large-scale surveys of this parasite have been conducted in
Indonesia to date.3, 4
Indonesia has at least 24 species of malaria vectors includ-ing
Anopheles balabacensis, Farauti Complex, An. koliensis, Punctulatus
Complex, Maculatus Group, and Sundaicus Complex.5, 6 A recently
decentralized health care system, along with a high diversity of
vectors, environments, and cultures, makes controlling malaria in
Indonesia especially challenging.
Indonesia is a country partner of the Asia Pacific Malaria
Elimination Network (APMEN), a diverse network com-posed of 12 Asia
Pacific countries, as well as leaders and experts from key
multilateral and academic agencies.7, 8 Although Indonesia faces
numerous challenges in eliminat-ing malaria, it has renewed its
malaria control strategy and elimination goals with the help of
foreign assistance and regional collaboration, and is currently
aiming for national elimination by 2030.6, 9
229,819
432
44
0.95
19
Reported cases of malaria(53% P. falciparum)
Deaths from malaria
% of population at risk(total population: 234 million)
Annual parasite incidence (cases/1,000 total
population/year)
% Slide positivity rate
At a Glance1*
*2010 statistics
Progress Toward EliminationMalaria in Indonesia was described by
Dutch settlers in the 1600s as a major health scourge, but was
likely present well before their arrival. In 1924, the central
malaria bureau was formed as a subdivision of the public health
service, and was the beginning of the Indonesian governments formal
cru-sade against malaria. For the next few decades, environmen-tal
modification techniques including new irrigation schemes, removing
algae from fishponds, and educating communities on local vector
control, basic diagnosis, and transmission were used to decrease
vector breeding habitats.14
Political turmoil during the Japanese invasion from 1942 to 1945
and the ensuing revolution for independence against the Dutch
colonialists from 1945 to 1949 undermined much of the countrys
malaria control measures during this time. After this period of
fighting, malaria control efforts such as indoor residual spraying
(IRS) with DDT were scaled up. This led to a significant reduction
in transmission and major economic benefits in highly endemic areas
as workers health and pro-ductivity increased.2 Mass chloroquine
treatment was success-fully used in western Papua, however, its
continual use was the cause of current resistance patterns seen in
this region.15
-
COUNTRY BRIEFING
APRIL 2012 2
Eliminating malaria in INDONESIA
In 1959, in accordance with the World Health Assemblys shift to
eradication, Indonesia shifted its malaria control program to an
elimination-focused program. The national malaria eradication
service (NMES) aimed to eliminate malaria in Indonesia by 1970.
Over 9,000 tons of DDT were used on the islands of Java and Bali
from 1959 to 1963. Insecticide resis-tance developed, and minimum
targets for elimination were never met.16 The feasibility of
elimination became less likely, and a combination of political and
financial constraints along with an attempted violent coup dtat in
1965 weakened and eventually discontinued the malaria program
activities.17
As the malaria program gradually shifted back to a control
strategy, the islands were stratified into two groups with
sepa-rate strategies. The islands of Java and Bali, where most of
the population is concentrated, had a case detection strategy
focused on active and passive case detection, mass fever sur-veys,
and migration surveillance. In contrast, the less populous outer
islands only used passive case detection and conducted malaria
surveys.2 From 1969 to 1999, the malaria burden was significantly
reduced on Java and Bali, but the disease burden on the outer
islands remained heavy due to the intrinsic chal-lenges of treating
a sparsely populated, vast geographical region with limited
transportation and infrastructure.
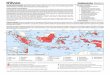
Malaria Transmission Limits
0 1,000 2,000 3,000 Kilometres 0 1,000 2,000 3,000
Kilometres
Plasmodium falciparum Plasmodium vivax
Water
P. vivax free
Unstable transmission (API
-
COUNTRY BRIEFING
APRIL 2012 3
The East Asian economic crisis of 1997 and subsequent fall of an
authoritarian regime led to several years of political and economic
instability exacerbated by a massive shift from a centralized to a
decentralized government system. Accord-ingly, the Indonesian
public health care system experienced major logistical and
financial setbacks. With limited resources available, implementing
and maintaining consistent and ac-curate malaria surveillance has
been a challenge.
The current malaria elimination program in Indonesia was
stimulated in 2000 by the start of the Roll Back Malaria
Initia-tive. The Indonesian Ministry of Health launched its
initiative Gebrak Malaria, or Crush Malaria, in April 2000, which
focused on malaria control in endemic areas. In April 2009, the
Indonesian Ministry of Health launched a formal set of elimination
targets, implementing a spatially progressive ap-proach to
elimination across all islands from west to east with the national
goal of elimination by 2030.6, 9
GOALS: 1. Eliminate malaria in low-transmission provinces (Java,
Bali, and Batam) by 20156
2. Eliminate malaria in intermediate- and variable-transmission
provinces (Kalimantan, Sulawesi, and Sumatra) by 20209
3. Achieve the pre-elimination stage in all remaining
malaria-endemic provinces by 20209
4. National malaria elimination by 20309
Reported Malaria Cases
Although confirmed cases have risen due to increased
availability of, and training in, laboratory confirmation, the
number of clinically diagnosed cases has actually decreased over
the last decade, which suggests an overall decrease in cases.
Source: World Health Organization, World Malaria Report 2011
0
50,000
100,000
150,000
200,000
250,000
300,000
350,000
400,000
450,000
500,000
1990 1992 1994 1996 1998 2000 2002 2004 2006 2008 2010
Num
ber of ca
ses
GNI per capita (US$) $2,500
Country income classification Lower middle
Total health expenditure per capita (US$) $55
Total expenditure on health as % of GDP 2.4
Private health expenditure as % total health expenditure
48
Eligibility for External Funding1012
Economic Indicators13
The Global Fund to Fight AIDS, Tuberculosis and Malaria
Yes
U.S. Governments Presidents Malaria Initiative No
World Bank International Development Association No
Eliminating malaria in INDONESIA
-
COUNTRY BRIEFING
APRIL 2012 4
Challenges to Eliminating MalariaMulti-island countryThe
Indonesian archipelago consists of over 17,000 islands spread out
over 1.9 million square kilometers.2 Although only 6,000 of these
islands are inhabited, the challenges associ-ated with malaria
control in the worlds fourth most populous nation are significant.
Ethnic and linguistic diversity, an ex-tremely mobile population, a
tropical climate, a lack of infra-structure, logistical challenges
to delivering health services, and frequent natural disasters
contribute to the challenge of eliminating malaria in
Indonesia.
Accurate surveillance and treatmentThe majority of malaria cases
are still diagnosed clinically in most Indonesian provinces outside
of the highly populated urban centers.18 Lack of equipment and
trained laboratory personnel have made it difficult to scale up
laboratory diag-nostics in remote areas. Drug resistance is also a
formidable
problem, and many first- and second-line drugs are becom-ing
ineffective in endemic areas.2, 19, 20
Information, education, and communicationNumerous gaps in
communication and education exist among the various provinces of
Indonesia. Although cam-paigns for education, mass
insecticide-treated net distribu-tion, and IRS have been conducted
with some success, many Indonesians living in endemic areas still
do not see malaria as a serious disease and have little knowledge
of its diagno-sis, treatment, and prevention.21, 22
ConclusionDespite numerous economic, political, and
environmental setbacks, Indonesia has made progress in malaria
control over the last few decades. Increased scale-up of
diagnostics, treatment, and education of citizens and health care
provid-ers should provide the catalyst Indonesia needs to move from
control to pre-elimination and ultimately achieve its national goal
of elimination by 2030.
Sources1. WHO. World Malaria Report 2011. Geneva: World Health
Organization; 2011.2. Elyazar I, Hay S, Baird JK. Malaria
Distribution, Prevalence, Drug Resistance and Control in Indonesia.
Advances in Parasitology. 2011; 74:
41175.3. Singh B, Kim Sung L, Matusop A, Radhakrishnan A,
Shamsul SS, Cox-Singh J, et al. A large focus of naturally acquired
Plasmodium
knowlesi infections in human beings. Lancet. 2004; 363(9414):
101724.4. White NJ. Plasmodium knowlesi: the fifth human malaria
parasite. Clin Infect Dis. 2008 ; 46(2): 1723.5. Sinka ME, Bangs
MJ, Manguin S, Chareonviriyaphap T, Patil AP, Temperley WH, et al.
The dominant Anopheles vectors of human malaria
in the Asia-Pacific region: occurrence data, distribution maps
and bionomic precis. Parasit Vectors. 2011; 4: 89.6. Kusriastuti R.
Intensified & Integrated Malaria Control: Towards Malaria
Elimination in Indonesia. ACT Malaria Executive Board and Part-
ners Meeting; 2010 March 1517th, 2010; Luang Prabang, Lao PDR;
2010.7. APMEN. Asia Pacific Malaria Elimination Network. [Available
from: www.apmen.org]8. Hsiang MS, Abeyasinghe R, Whittaker M,
Feachem RG. Malaria elimination in Asia-Pacific: an under-told
story. Lancet. 2010; 375(9726):
15867.9. Intensified Malaria Control Program in Kalimantan and
Sulawesi Islands: The Global Fund to Fight AIDS, Tuberculosis and
Malaria; 2008.10. World Bank: International Development Association
Eligibility. 2012 [Available from:
http://web.worldbank.org/WBSITE/EXTERNAL/EXT-
ABOUTUS/IDA/0,,contentMDK:20054572~menuPK:3414210~pagePK:51236175~piPK:437394~theSitePK:73154,00.html]11.
U.S. Governments Presidents Malaria Initiative (PMI). 2012 [cited;
Available from:
http://www.fightingmalaria.gov/countries/index.html]12. The Global
Fund to Fight AIDS Tuberculosis and Malaria. The Global Fund
Eligibility List. 2012 [Available from:
http://www.theglobalfund.
org/en/application/applying/ecfp/eligibility/]13. World Bank.
World Development Indicators Database. 2012 [Available from:
http://data.worldbank.org/]14. Keiser J, Singer BH, & Utzinger
J. Reducing the burden of malaria in different eco-epidemiological
settings with environmental manage-
ment: a systematic review. Lancet Infectious Diseases. 2005; 5:
695708.15. Van Dijk W. Mass chemoprophylaxis with chloroquine
additional to DDT indoor spraying. Doc Med Geogr Trop. 1958;
10(379384).16. Soerano M, et al. The development and trend
insecticide resistance in Anopheles aconitus Donitz and Anopheles
sundaicus Rodenwaldt.
Bull World Health Organ. 1965; 32: 1618.17. Takken W, Snellen
WB, Verhave JP, Knols BGJ, Atmosoedjono S, Swellengrebel NH, et al.
Environmental measures for malaria control in
Indonesiaan historical review on species sanitation: Wageningen
Agricultural University Papers; 1990.
Eliminating malaria in INDONESIA
-
COUNTRY BRIEFING
APRIL 2012 5
18. Sekartuti T, Sudomo E, Santoso TS, Utami BS. Intensifikasi
pemberantasan malaria di empat provinsi Indonesia timur: Survey
dasar untuk manajemen kasus, perilaku masyarakat, dan pengendalian
vector malaria: Badan Penelitian dan Pengembangan Kesehatan,
Departemen Kesehatan Indonesia; 2004.
19. Karyana M, Burdarm L, Yeung S, Kenangalem E, Wariker N,
Maristela R, et al. Malaria morbidity in Papua Indonesia, an area
with multidrug resistant Plasmodium vivax and Plasmodium
falciparum. Malar J. 2008; 7: 148.
20. Ratcliff A, Siswantoro H, Kenangalem E, Maristela R, Wuwung
RM, Laihad F, et al. Two fixed-dose artemisinin combinations for
drug-resis-tant falciparum and vivax malaria in Papua, Indonesia:
an open-label randomised comparison. Lancet. 2007 ; 369(9563):
75765.
21. Sanjana P, Barcus MJ, Bands MJ, Ompusunggu S, Elyazar I,
Marwoto H, et al. Survey of community knowledge, attitudes, and
practices during a malaria epidemic in Central Java, Indonesia. Am
J Trop Med Hyg. 2006; 75: 7839.
22. Pradono J, Kusumawardi N, Lubis N, Hapsari D, Sulistyawati
N, Christina C, et al. Survey Kesehatan Rumah Tangga 2004 Volume 3:
Badan Penelitian dan Pengembangan Kesehatan, Departemen Kesehatan
Indonesia; 2005.
Transmission Limits Maps SourcesGuerra, CA, Gikandi, PW, Tatem,
AJ, Noor, AM, Smith, DL, Hay, SI and Snow, RW. (2008). The limits
and intensity of Plasmodium falciparum
transmission: implications for malaria control and elimination
worldwide. Public Library of Science Medicine, 5(2): e38.
Guerra, CA, Howes, RE, Patil, AP, Gething, PW, Van Boeckel, TP,
Temperley, WH, Kabaria, CW, Tatem, AJ, Manh, BH, Elyazar, IRF,
Baird, JK, Snow, RW and Hay, SI. (2010). The international limits
and population at risk of Plasmodium vivax transmission in 2009.
Public Library of Science Neglected Tropical Diseases, 4(8):
e774.
Rita Kusriastuti (2009), Directorate of Vector-borne Diseases,
Ministry of Health, Jakarta, Republic of Indonesia. (Data years
20052008)
GloBAl HeAlTH GroUP ProjeCT TeAMeditor: Allison Phillips |
Managing editor: Chris Cotter | researcher and Content Developer:
Jessie de Jarnette | Graphic Designer: Kerstin Svendsen
The Malaria Atlas Project (MAP) provided the malaria
transmission maps. MAP is committed to disseminating information on
malaria risk, in partnership with malaria endemic countries, to
guide malaria control and elimination globally. Find MAP online at:
www.map.ox.ac.uk.
The Malaria Elimination Initiative at the Global Health Group of
the University of California, San Francisco
(www.globalhealthsciences.ucsf.edu/global-health-group) convenes
the Malaria Elimination Group (www.malariaeliminationgroup.org),
and supports countries actively pursuing elimination at the endemic
margins of the disease. Funding for the Malaria Elimination
Initiative is provided by the Bill & Melinda Gates Foundation
and Exxon Mobil Corporation.
About This BriefingThis country briefing was produced through a
collaboration of the Global Health Group, in partnership with the
National Malaria Control Program in Indonesia. Malaria transmission
risk maps were provided by the Malaria Atlas Project (MAP). Funding
was provided through a grant to the Global Health Group from the
Exxon Mobil Corporation.
APMENAdditional support was provided by the Asia Pacific Malaria
EliminationNetwork (APMEN). Find APMEN online at:
www.apmen.org.
Eliminating malaria in INDONESIA