Embed Size (px)
Citation preview

MALAYSIA AUGUST 2014
Pharmacists may be better stroke case managers than nurses
spotlightManaging acute sports injuries
Feature Community pharmacies ‘first port of call’ for coughs, colds
NeWsPharmaceutical industry turns to edutainment

PT IMPACT Rottapharm Agiolax.pdf 1 3/26/13 10:38 AM

AUGUST 2014 3
Pharmacists may be better stroke case managers than nursesElvira Manzano
Patients recovering from a minor stroke are
more likely to attain optimal blood pressure
and lipid control if they are actively managed by
pharmacists, a randomized controlled trial has
shown.
Researchers compared pharmacist- vs nurse-
led care in 279 adults (mean age, 68 years) who
had minor ischemic stroke or transient ischemic
attack between 2009 and 2012 and whose blood
pressure or lipid levels were above the Canadian
guideline targets.
“Both pharmacist- and nurse-led care resulted
in significant improvements in blood pressure
and LDL cholesterol control at 6 months. Howev-
er, even greater improvements were seen in pa-
tients whose care was managed by a pharmacist
care manager who was empowered to initiate
and titrate medications,” said principal investiga-
tor Professor Finlay A. McAlister, of the University
of Alberta in Edmonton, Canada.
More patients in the pharmacist-led group met
the guideline-recommended targets for systolic
blood pressure (≤140 mmHg) and LDL choles-
terol (≤2.0 mmol/L) compared with patients in the
nurse-led group (43.4 vs 30.9 percent; p=0.03).
Clinical events occurred infrequently during the
study, with no significant differences in cardiovas-
cular events and deaths between groups. [CMAJ
2014; doi:10.1503/cmaj.140053]
At baseline, more than 75 percent of patients
were taking antiplatelet agents, antihypertensive
medications, or statins, but none met the guide-
line targets for systolic BP and LDL cholesterol.
The average systolic BP was 134 mmHg and the
average LDL cholesterol was 3.23 mmol/L. About
two-thirds had a moderate-to-high risk stroke risk
based on the ABCD score.
Patients were randomized to active prescribing
by pharmacists or nurse-led screening and feed-
back to primary care physicians (control group),
in addition to usual care. At 6 months, gains were
greater in the pharmacist-led group vs the con-
trol group (OR 2.31, 95% CI, 1.29-420, p=0.005).
The benefits of pharmacist-led care were largely
driven by the higher proportion of patients who

AUGUST 2014 4
met their LDL cholesterol targets (51.1 vs 33.8
percent for nurse-led care; p=0.003). The 12.5
percent difference in the percentage of patients
who achieved blood pressure and lipid control
exceeded the pre-specified 10 percent threshold
necessary for a meaningful endpoint.
Patients in the pharmacist-led group had more
medication changes over the study period (192
by pharmacist case managers, 71 by their attend-
ing physicians, 26 by patients) compared with
those in the nurse-led group (85 by physicians,
26 by patients).
“Case management by non-physician health-
care providers can improve risk factor manage-
ment for at-risk patients. It is more effective if the
case manager can actively modify medications,”
said McAlister. However, he cautioned that the
study does not support calls for pharmacists to
prescribe medication without the supervision of
a primary care doctor or a specialist within the
team.
“We believe both approaches hold great
promise not only for patients with stroke or tran-
sient ischemic attack but also for patients at high
risk of vascular disease,” the researchers said.
Optimization of blood pressure and lipid con-
trol reduces the risk of heart attack, secondary
stroke, and death in these patients.

AUGUST 2014 NEWS 5
Pharmaceutical industry turns to edutainmentMalvindErjit Kaur dhillon
Medicine need not be boring nor dull, as a
medical edutainment company demon-
strates.
EP Plus Group Sdn Bhd, formed in 1997,
aims to be at the helm of brand marketing for the
pharmaceutical industry by introducing fresh
and inventive ideas to promote products.
EP Plus Group’s head of marketing Jennifer
Yong said: “We want to share medical knowl-
edge in a fun and exciting manner. We try to
take different approaches, so when doctors at-
tend our medical talks or round-table discus-
sions, they are in a stimulating environment. We
prioritize starting and ending on time, as well as
making sure there are a lot of take-home mes-
sages. We are constantly pushing the boundar-
ies and innovating as we want to challenge the
status quo.”
The group’s resolve to be different was dem-
onstrated at the recent 23rd Malaysian Congress
of Obstetrics and Gynaecology, where EP Plus
launched a new concept in women’s health-
care, with an emphasis on a healthy vagina and
prevention of antimicrobial resistance.
The launch, which took place at the EP Plus
booth, showcased splashes of creativity as the
booth was designed along the concept of a
bathroom, combining the products Multi-Gyn®
and Monurol®.
Revolving around evoking the five senses, the
booth featured a rain shower on the inside and
half-covered curtains on the outside. This was
to draw curious visitors into the booth. Agent M,
a vagina-shaped mascot, also made an appear-
ance in the booth, giving away tickets to visitors
for an opportunity to be photographed with it in
the photography booth.
“The launch also aimed to create a higher
noise level to draw the attention of the crowd.
Internally, we want to tell people this is the way
we are going to move forward. This is the first
time we’ve done a conceptual booth and we will
constantly be coming up with different concepts
and ideas in line with the brand strategy,” Ms
Yong said.
The group works towards enriching lives by
introducing innovative European pharmaceu-
tical products to the Southeast Asian market.
These products are unique as some of them
are the first in their class. One such example is
the Multi-Gyn range of products, especially Ac-
tiGel®. This natural product helps prevent and
treat bacterial vaginosis via biologically active
2QR complex and the use of aloe vera extract to
restore and keep the flora of the vagina healthy.
EP Plus takes pride in being a medical
edutainment specialist, with aspirations to be
the most desired, innovative and leading medi-
cal edutainment brand by 2020. It is one step
closer towards this goal by standing out from
the crowd through its approach of sharing med-
ical knowledge in a refreshing way

AUGUST 2014 NEWS 6
Advocating personal hygiene through a multichannel campaign
L to R: Dr Chin Wai Seong, Siti Nordiana, Yamusiah, Ashlee Ng, Datuk Harjeet Singh, Chong Yen Nee, Norhayati and Christabel Wong pledging their commitment at the cam-paign launch.
dr joslyn ngu
Personal hygiene has always been an im-
portant point for Lifebuoy, prompting the
launch of the innovative Salam Sesuci Lifebuoy
– Spread Peace, Not Germs campaign recently.
The Salam Sesuci Lifebuoy campaign aims
to promote active hand washing and bath-
ing with soap. With the proper shield against
germs, Malaysians can stay protected regard-
less of place and time. “Most of us know that
personal hygiene is an important element in
staying protected. We understand that during
this fasting month the emphasis is on self-re-
flection and purification via the mind and body,
hence personal hygiene is especially important
during this time,” said Ashlee Ng, a personal
care director at Unilever Malaysia.
The campaign’s priority is to educate par-
ents, especially mothers, regarding microor-
ganisms that are too small to be viewed with the
naked eye but are present everywhere and can
be spread through personal contact. Mothers
play the main role in inculcating proper hygiene
habits amongst their children and have strong
emotional stakes in their children’s health, said
Ms Ng.
“We are pleased that the Salam Sesuci Life-
buoy campaign understands the prominence of
personal hygiene especially during Ramadan
and directs its focal point at mothers as they
are the first line of defense in ensuring the best
health for their children and family,” said Datuk
Harjeet Singh Hardev Singh, deputy secretary
general (strategic) of the Ministry of Women,
Family and Community Development. “This ini-
tiative is in sync with the ministry’s efforts in in-
tegrating women and community as part of the
mainstream national development process and
improving Malaysia’s overall social well-being.”
Besides advocating the healthy routine of
personal hygiene, the campaign also supports
the practice of giving. The campaign encour-
ages mothers and their families to pledge their
commitment to hand-washing in a dedicated
Facebook page. Once the number of pledges
reaches the 80,000 mark, RM80,000 will be do-
nated to two underprivileged homes, namely
Rumah Taqwa and Rumah Putera Harapan.
“We are taking small steps by targeting 80,000

AUGUST 2014 NEWS 7
pledges. As a brand, we have always worked
towards leaving a positive impact on society
through the solutions we offer,” explained Ms
Ng.
Other than the Facebook pledging activ-
ity, the campaign also encompasses a se-
ries of webisodes that emphasizes on es-
sential values and beneficial health and
hygiene pointers during Ramadan, explained
through stories and testimonials of fami-
lies from different backgrounds. In addition,
educational resources such as infographics
will be used to increase understanding and
awareness.
“We want people to continue embracing this
healthy practice even after Ramadan and Hari
Raya. Using just one medium is not enough,”
explained Ms Ng. “That is why we trust that
speaking to the local community, through local
identifications and in local voices is important to
get the message across effectively.”
For more information on the campaign and
to pledge, visit www.facebook.com/Lifebuoy
Malaysia

AUGUST 2014 NEWS 8
Challenging type 2 diabetics towards better disease managementPanK jit sin
A new nutrition program, the Glucerna® Chal-
lenge Me program, is part of Abbott’s ef-
forts to educate and improve the quality of life
of people with type 2 diabetes (T2D) through
proper nutrition and provision of useful tools.
Running for 12 weeks, the Challenge Me pro-
gram allows participants to create a simple plan
that incorporates a healthy meal plan, special-
ized nutrition and exercise.
Malaysia has been plagued by increasingly
high rates of diabetes in recent years, with the
National Health and Morbidity Survey 2011 esti-
mating the prevalence of diabetes to affect one-
in-five for adults aged 18 years and above by
2020.
Proper diabetes management is important
because people with the condition are two to
four times more likely to suffer a heart attack or
stroke compared to healthy individuals. They
are also at additional risk of other health compli-
cations such as kidney failure, blindness, lower-
limb amputation and death.
These factors make proper management
especially important to people with T2D. Here,
maintaining healthy blood sugar levels is the first
step to proper diabetes management. Addition-
ally, weight management and physical activity
are important factors to take into consideration
as they contribute to additional health-related
complications in people with diabetes.
Medical director of Abbott Nutrition Malaysia
Dr Shaalani Ramachandran said: “The effective
management of diabetes is becoming increas-
ingly important because of the prevalence of this
disease. Whilst everyone should be vigilant in
monitoring their nutritional intake and all-round
health, research and experience have shown
that diabetics often struggle with this. That’s
why we developed the Glucerna Challenge Me
– to provide people with diabetes with an easy-
to-use resource that helps them take charge of
managing their condition and feel confident they
can lead a healthier lifestyle.”
More information regarding the program can
be obtained at www.glucernachallengeme.com.
my or by calling 1-800-88-6233.
Patients with diabetes should be advised to follow a regular exercise plan that suits them
C
M
Y
CM
MY
CY
CMY
K
NovaRice Med Ad-Pharmacy Today(2014)FA(OL).pdf 1 2/27/14 6:12 PM

AUGUST 2014 NEWS 10
Consensus on menopause hormone therapydr joslyn ngu
Hormone replacement therapy (HRT) can
be a confusing topic. In view of this,
healthcare practitioners have to be careful in
getting the right information and ensuring that
their sources can be trusted.
Examples of reliable sources are interna-
tional organizations such as the International
Menopause Society and North American Meno-
pause Society, said Dr Peter Roos, department
of gynecology, University of Cape Town, South
Africa. Local sources i.e. South African Meno-
pause Society (SAMS) and Malaysia Meno-
pause Society (MMS) are also important, as
disease management is different in every part
of the world. Dr Roos was speaking at the 23rd
Congress of the Obstetrical & Gynecological
Society of Malaysia held in Kuala Lumpur, re-
cently.
In 1997, the first consensus meeting on
menopause in the East Asian region was held
in Geneva, Switzerland. Among the consen-
sus statements formed was that every woman
should be educated on the risks and benefits of
using HRT in menopause, and given the free-
dom to choose if they wish to use HRT or not
to, Dr Roos said.
Another consensus was on the existence
of convincing data that showed HRT relieved
vasomotor symptoms, and reduced the risk of
coronary artery disease (CAD), osteoporosis
and Alzheimer’s disease (AD). Although long-
term use of HRT increases the risk of bleeding
and breast cancer, its benefits still outweigh the
risks, Dr Roos said. The 1997 consensus also
mentioned that women may continue to use
HRT indefinitely with surveillance and under-
standing of the risks. For women with meno-
pause, HRT may improve their quality of life.
In 2013, numerous organizations collabo-
rated to produce the global consensus state-
ments of menopause hormone therapy (MHT).
The statements were very similar to those writ-
ten in 1997, Dr Roos said. One of the 2013 con-
sensus statements said that for women aged
below 60 and less than 10 years after meno-
pause, MHT is the most effective treatment for
vasomotor symptoms, and also an effective
preventive method for osteoporosis in at-risk
women. The consensus also recommended
the use of systemic MHT in premature ovarian
insufficiency prior to natural menopause. (Cli-
macteric 2013;16:203-4)
The 2013 consensus also acknowledged
that the risk of ischemic stroke and venous
thromboembolism (VTE) increased with oral
MHT. However, absolute risk of ischemic stroke
and VTE with oral MHT is rare for women aged
below 60, and some studies demonstrated
the reduction of this risk through the usage of
transdermal instead of oral MHT.
In women older than 50, the association be-
tween MHT and breast cancer is a complicated

AUGUST 2014 NEWS 11
issue, Dr Roos said. It is commonly linked with
the introduction of progesterone. Nevertheless,
the resulting risk is small and decreases after
discontinuation. Even so, the 2013 consensus
does not recommend custom-compounded bi-
oidentical hormone therapy and the usage of
MHT in breast cancer survivors.
Menopause is an important event that has
a strong medical and social impact on wom-
en’s lives. There are significant associations
between menopause and aging with increased
risks of cardiovascular disease (CVD), osteo-
porosis, lower genitourinary problems, AD
and vascular dementia. As the age of onset of
menopause remains between 50 and 60 years
while the average women’s lifespan increases,
menopause will become an increasingly bigger
issue, Dr Roos said.

N u v a F l e x B _ P T _ A u g 1 4 - 1 2 0 1 4 - 0 7 - 0 9 T 1 5 : 1 0 : 1 6 + 0 8 : 0 0

AUGUST 2014 FEATURE 13
Community pharmacies ‘first port of call’ for coughs, colds
When it comes to battling coughs and
colds, some of the best advice pharma-
cists can give comes from listening to the cus-
tomer and hearing about their symptoms.
New Zealand’s Unichem Miramar Pharmacy
owner and pharmacist Ann Privett said listen-
ing to what the customer has to say helps in
finding the right product for the right symptom.
“Everyone has a symptom they would like to be
treated the most.”
People often need guidance when it comes
to cough and cold remedies, as each cold is dif-
ferent and presents a different set of symptoms,
she said.
Asking what remedies they have tried be-
fore for particular symptoms can be helpful,
because the biggest trap is recommending
something that has not worked for them in the
past, Ms Privett said. “There’s nothing worse
than blowing your credibility by recommending
something they have already tried and which
has failed.”
When it comes to coughs and colds, Ms
Privett is a firm believer in “old-fashioned” rem-
edies, such as the “mysterious power” of chest
rubs like Vicks® and some natural health prod-
ucts. “It’s treating the whole person rather than
just the cough or cold.”
Natural health remedies have been steadily
growing in popularity since Ms Privett began
work as a pharmacist in the 1970s, but she
suggests taking a cautious route when recom-
mending alternative treatments. “Some people
don’t believe in it, you have to suss it out before
you recommend it,” she said.
If a customer seems open to a recommenda-
tion, ask them if they would like to find out more
about a natural remedy for their symptoms.
Ms Privett most often recommends anything
with at least zinc and vitamin C in it, as well as
products with echinacea and olive leaf extract.
But natural health products are recommended
as an extra line of defence alongside conven-
tional treatments, she said.
“You’ve got to be caring, understanding, give
hints and tips and lots of TLC. All we’re doing
is giving symptom relief, because no one can
cure it.”
Stand out from supermarkets
With many cough and cold remedies available
in lower strength formulas from supermarkets,
it is important for pharmacies to distinguish
Pharmacists can help distinguish between serious and non-threatening symptoms

AUGUST 2014 FEATURE 14
themselves as the medicine specialists, New
Zealand’s Green Cross Health professional ser-
vices manager Alison Van Wyk said.
A strong focus on care and advice is what
helps pharmacies stand out from supermar-
kets, as pharmacists can ask a range of ques-
tions about the customer’s current medicines
and their lifestyle, and then present the best
possible solution for their ailment. Finding out
what medicines the customer might already be
taking for their cold is key to preventing any
double-ups on dosages. “You can’t get that in a
supermarket,” Mrs Van Wyk said.
Pharmacist Martin Harris at Massey Amcal
Pharmacy, New Zealand, believes pharmacy is
the “main player” when it comes to taking care
of coughs and colds. “There’s not a lot you can
do in conventional medicine apart from relieve a
few symptoms, it’s all viral and there’s not a lot
your GP can do,” Mr Harris said.
People come “far and wide” for his Get Well
Fast pack of vitamins and natural health rem-
edies, including a herbal cough and cold tonic,
which he made with the help of some medical
herbalists. As owner of the Nutrition Medicine
Clinic, Mr Harris is an advocate for taking care of
the natural health of a person, and their family,
to help reduce the severity of illnesses in winter.
In combination with the knowledge a phar-
macist offers when it comes to coughs and
colds, there are many medicines which can only
be purchased from a pharmacist, especially
high-strength products.
“It’s not just about the products, it’s about
the helpful hints,” Mrs Van Wyk said. This rep-
utation as the medicines specialist is seeing
more and more people coming into pharmacies
especially to speak to the pharmacist, and that
is a “very strong message”, she said.
Be wary of serious symptoms
Distinguishing between symptoms of a cold or
more serious symptoms of influenza or strep
throat is important. Strep throat if left untreated
can lead to rheumatic fever.
Colds generally do not present with high fe-
ver, joint pains, or body chills, and symptoms
usually take a few days to develop compared
with flu symptoms, which can develop with-
in three to four hours, according to the PTNZ
Healthcare Handbook 2013.
Mrs Van Wyk said encouraging health litera-
cy is vital and this includes engaging in conver-
sations with customers about their illness and
symptoms, especially how long they may have
had certain symptoms for.
Keeping an eye out for customers who are
complaining of a particularly sore throat is im-
portant, and pharmacists should make sure
customers are aware of the risks of strep throat
and rheumatic fever.
New Zealand Self Medication Industry execu-
tive director Tim Roper said pharmacists are gen-
erally seen as the “first port of call” for customers
on their journey to full health. “The key is that the
pharmacist uses his or her skill to treat the self-
limiting condition and look for red flags that could
require a GP referral,” Mr Roper said. –PTNZ

FA_Circarol_Pharmacy Today_Aug 2014.pdf 1 6/12/2014 10:00:37 AM

saras raMiya
Sports injuries are any form of injuries related
to any sports activity or exercise and can
be acute or chronic. Acute injuries may occur
immediately after contact or non-contact sports,
exercise or physical activity and must be man-
aged promptly, consultant sports physician Dr
Mohd Nahar Azmi Mohamed says.
Chronic injuries are injuries that develops
slowly and is persistent and long-lasting, or
constantly recurring for months or even years
when patients do not receive the appropriate
treatment or have not been treated at all. Chron-
ic injuries may start with mild symptoms and
low-grade pain, and are often ignored or simply
overlooked, Dr Nahar told Pharmacy Today.
Discussing acute injuries further, he said pa-
tients will usually have the five cardinal signs
of inflammation, which are swelling, redness,
warmth, pain and loss of function or deformity
after they sustain injuries. The signs may or
may not appear immediately but subsequently
patients will suffer from, and complain of, the
symptoms which also depends on the severity
of injuries.
“For example, a football player sprains his
ankle after being tackled or running on uneven
surface and sustains injuries. He will have imme-
diate pain and swelling. The swelling area may
feel warm and look red or bruised depending on
the degree of injuries. Because of the swelling
he cannot move and starts to limp.”
As head of the sports medicine department
in University Malaya Medical Centre (UMMC),
Dr Nahar related that about 30-35% of patients
presenting at UMMC’s sports medicine clinic
have sports injuries. However, this figure is an
estimation and does not represent the percent-
age of the incidence of sports injuries in Malay-
sia. “We need to have a database to determine
the percentage of sports-related injuries in our
country,” he said.
Furthermore, he said the level of awareness
of sports injuries among the public and even
among pharmacists and general practitioners
is still low in general. Most of the patients will
not even seek medical attention immediately af-
ter sustaining injuries. They just rest or go for
a massage and hope that they will recover. Of
course, they do not experience pain when they
rest so they mistakenly think that they have re-
covered from their injuries. Even when some
of them seek treatment or advice from a phar-
macist or general practitioner, they are usually
prescribed painkiller and heat rub ointment and
asked to rest for a few days or months and told
that they can resume playing games after that.
By the time the resting period is over and they
resume playing games, they still feel pain, are
weak or even have stiffness. Finally, they de-
cide to stop playing games. “From our experi-
AUGUST 2014 SPOTLIGHT 16
Managing acute sports injuries
Dr Mohd Nahar Azmi Mohamed
AUGUST 2014 SPOTLIGHT 17
ence, some patients have complained that the
injured area is worsening and the swelling has
increased after they applied heat rub oitment or
went for a massage.”
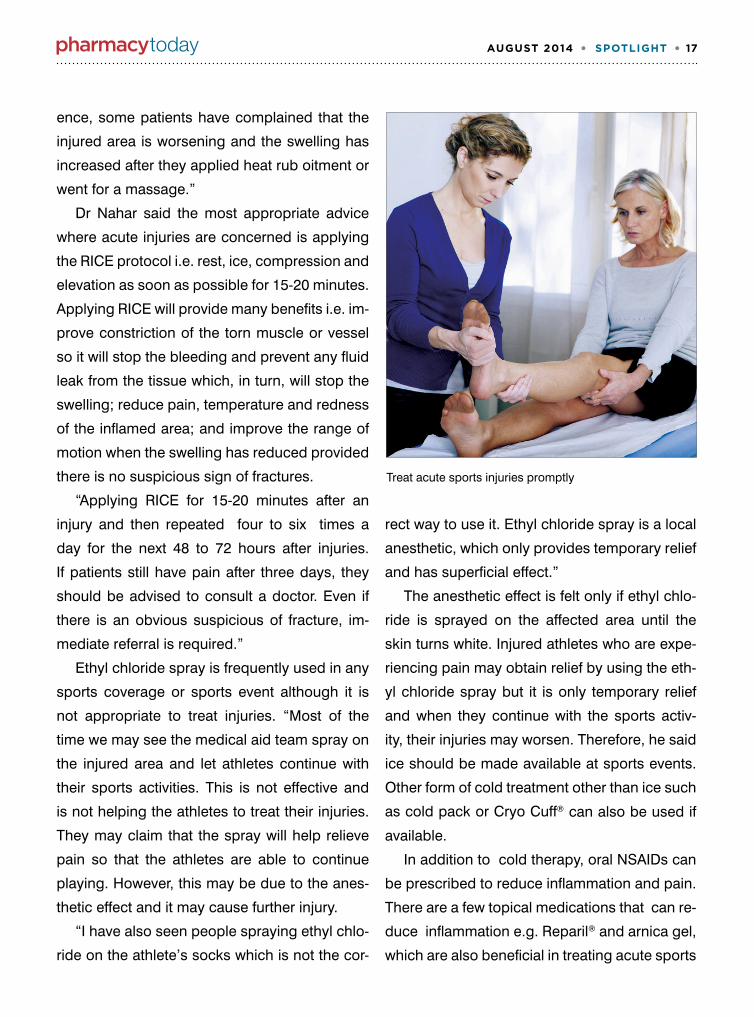
Dr Nahar said the most appropriate advice
where acute injuries are concerned is applying
the RICE protocol i.e. rest, ice, compression and
elevation as soon as possible for 15-20 minutes.
Applying RICE will provide many benefits i.e. im-
prove constriction of the torn muscle or vessel
so it will stop the bleeding and prevent any fluid
leak from the tissue which, in turn, will stop the
swelling; reduce pain, temperature and redness
of the inflamed area; and improve the range of
motion when the swelling has reduced provided
there is no suspicious sign of fractures.
“Applying RICE for 15-20 minutes after an
injury and then repeated four to six times a
day for the next 48 to 72 hours after injuries.
If patients still have pain after three days, they
should be advised to consult a doctor. Even if
there is an obvious suspicious of fracture, im-
mediate referral is required.”
Ethyl chloride spray is frequently used in any
sports coverage or sports event although it is
not appropriate to treat injuries. “Most of the
time we may see the medical aid team spray on
the injured area and let athletes continue with
their sports activities. This is not effective and
is not helping the athletes to treat their injuries.
They may claim that the spray will help relieve
pain so that the athletes are able to continue
playing. However, this may be due to the anes-
thetic effect and it may cause further injury.
“I have also seen people spraying ethyl chlo-
ride on the athlete’s socks which is not the cor-
rect way to use it. Ethyl chloride spray is a local
anesthetic, which only provides temporary relief
and has superficial effect.”
The anesthetic effect is felt only if ethyl chlo-
ride is sprayed on the affected area until the
skin turns white. Injured athletes who are expe-
riencing pain may obtain relief by using the eth-
yl chloride spray but it is only temporary relief
and when they continue with the sports activ-
ity, their injuries may worsen. Therefore, he said
ice should be made available at sports events.
Other form of cold treatment other than ice such
as cold pack or Cryo Cuff® can also be used if
available.
In addition to cold therapy, oral NSAIDs can
be prescribed to reduce inflammation and pain.
There are a few topical medications that can re-
duce inflammation e.g. Reparil® and arnica gel,
which are also beneficial in treating acute sports
Treat acute sports injuries promptly

AUGUST 2014 SPOTLIGHT 18
injuries. Doctors can also prescribe reparil tab-
let and papain to reduce inflammation. Dr Nahar
said Reparil gel with or without Reparil tablet
and NSAIDs are commonly prescribed to pa-
tients with injuries at UMMC’s sports medicine
clinic.
Topical NSAIDs such as ketoprofen gel or
diclofenac gel can be used as part of sports in-
juries management.
Physiotherapy is included as part of the treat-
ment. Initially, physiotherapy can manage the
pain and the recovery and healing process.
When the symptoms are reduced, patients have
to undergo a rehabilitation program before they
can resume sports activities.
Pharmacists should refer patients to a doctor
when initial treatment does not improve the pain
and swelling after three days. Patients should
also be referred immediately when they present
with any deformity in their limbs or any part of
their body. They should preferably be referred
to a sports physician, orthopedic surgeon or a
general practitioner who has experience treat-
ing sports injuries if patients do not improve.
In his take home message, Dr Nahar pointed
out that sports injuries are becoming more com-
mon lately because everyone is becoming more
physically active and health conscious. There-
fore, it is best for pharmacists to be aware of
and prescribe appropriate treatment and refer
patients who are not improving and those with
any deformity.
With regard to raising the level of awareness
of sports injuries among the public, Dr Nahar
said: “We would like to organize a forum to raise
the awareness of the public so they know what
to do when they sustain injuries. At the moment,
I think most of us are focusing on athletes and
students who are involved in competition sports.
We do need to give full awareness to the public
as well to educate them and make them under-
stand the steps they need to take when injured
during sports or physical activity.”
KEY POINTS■ The five cardinal signs of inflammation
in acute injuries are swelling, redness, warmth, pain and loss of function.
■ Apply ice for 15-20 minutes after an in-jury. 4-6 times per day for the next 48-72 hours.
■ In addition to ice, prescribing an oral and or topical NSAIDs to reduce pain and inflammation e.g. diclofenac sodi-um or any COX-2 inhibitor, Reparil, ar-nica or papain.
■ Avoid heat rub and massage during the acute stage of injury.
■ Refer patients when they are not im-proving with treatment or if they present with any deformity.


AUGUST 2014 SPOTLIGHT 20
Menopause, a new phase in lifesaras raMiya
Hot flushes, mood swings and heavy pe-
riods are some of the symptoms that
women have to endure when they reach the
perimenopause stage. Pharmacists have an im-
portant role in helping women who are under-
going perimenopause.
For starters, pharmacists can have conversa-
tions with their customers who walk in with com-
plaints of night sweats, memory problems and
a host of other signs and symptoms, and gently
tell them that they could be going through peri-
menopause and advise them on remedies that
can help them along the way.
Consultant obstetrician and gynecologist
Dr Wong Kim Lei defines perimenopause as
the years covering pre-menopause and meno-
pause. Perimenopausal symptoms may first
appear from the age of 40 onwards, about five
to 10 years before menopause, and become
worse when women attain menopause. Meno-
pause is reached when a woman has not had
menses for 12 consecutive months. This is fol-
lowed by the post-menopausal years.
According to clinical psychologist Hariyati
Shahrima Abdul Majid (PhD), perimenopause
brings about changes not only in physical
health but also psychological health. “In our so-
ciety, when we talk about psychological health
people often fear or are ashamed to talk about it
because it is considered a taboo in our society.”
N u v a _ P T C a me o _ J u l 1 4 - 1 2 0 1 4 - 0 7 - 0 2 T 1 6 : 5 7 : 2 5 + 0 8 : 0 0
However Ms Hariyati emphasized that it is
important to create awareness so people re-
alize that they should not be ashamed to talk
about perimenopause and the psychological
problems involved.
Signs like mood swings, memory problems
and not sleeping well can result in women feel-
ing stressed. People have to recognize that
these signs point to the development of peri-
menopause, a normal process that takes place
over time.
“When women experience symptoms of per-
imenopause, their bodies are undergoing fluc-
tuating levels of hormones. There are different
hormones that control our wellbeing,” said Dr
Wong.
For women, the most important hormone
is estrogen. During perimenopause, the num-
ber of eggs in the ovaries is close to depletion,
causing hormone levels to fluctuate. The fluctu-
ation in hormone levels is caused by the lack of
eggs to provide a constant level of hormones,
and leads to signs and symptoms like mood
swings and changes in the body, metabolic
rate, hair and skin. “These changes are scary to

AUGUST 2014 SPOTLIGHT 21
women but if they prepare themselves well and
know that these things can happen then they
are more comfortable with the changes,” said
Dr Wong.
There are ways to chart the changes in hor-
mone levels i.e. by measuring the levels. Blood
tests can detect levels of estrogen, progester-
one, follicle stimulating hormone and luteiniz-
ing hormone. Generally, during puberty, some
eggs will mature while some don’t and this
causes fluctuation in hormone levels. In women
aged 20-40, hormone levels are constant, eggs
mature at the same time and menstrual cycles
are regular. From the age of 40 onwards, the
number of eggs reduce and eventually deplete
– ovulation may or may not happen – causing
fluctuation in hormone levels, said Dr Wong.
The most common complaint by women
aged 40 and above is hair loss. Apart from
perimenopause, other factors like imbalance of
growth hormone, stress and chemicals used on
the hair i.e. hair dye or other chemicals used to
style the hair, may be causing hair loss. How-
ever, the most important factor to the reced-
ing hairline is estrogen depletion. About 80%
of women lose half their hair when they reach
menopause. Another sign that indicates peri-
menopause is graying of hair, said Dr Wong.
In general, the fluctuation of hormones
causes a lot of discomfort in women. They ex-
perience sudden episodes of hot flushes, which
make them irritable. They can’t sleep at night
due to night sweat and are tired in the morn-
ing. These symptoms, in addition to aches and
pains make them feel moody, irritable and tem-
peramental, said Dr Wong.
She added that lifestyle is very important.
Women need to understand what they are going
through and obtain support from their husband
and children. Exercise and adequate nutrition,
including proper diet and nutritional supplemen-
tation e.g. Nuvafemme®, is very important. Seek
help from a gynecologist to determine whether
the problems are due to perimenopause or oth-
er pathological problems, she said.
Changes in estrogen levels affect a part of
the brain called hypothalamus, which secretes
neurotransmitters such as norepinephrine, se-
rotonin, dopamine and acetylcholine as well as
catecholamine and cortisols, said Ms Hariyati.
The direct relationship between the changes in
estrogen and these neurotransmitters actually
has an impact on mood and wellbeing. “As a re-
sult, you may actually feel a decrease in positive
emotions. It is not necessarily something that
you desire or something that you actually create
but it comes with the differences of the changes
in the neurotransmitter.”
“Reduced estrogen levels are also associ-

AUGUST 2014 SPOTLIGHT 22
ated with increase in stress hormones called
catecholamines or cortisol which can also re-
sult in changes in your emotions so you’re more
likely to be stressed or angry,” said Ms Hariyati.
Changes in estrogen levels are also associated
with changes in another neurotransmitter called
acetylcholine, which processes and stores in-
formation.
Ms Hariyati advised that women should
take measures to ensure that these changes
do not impact their quality of life and wellbeing
because in their 40s, many women are at the
height of their career.
Women can use the Perimenopause Crys-
tal Quiz, which is a simple self-assessment
that is supposed to shed light on symptoms
experienced by women aged 40-56, said Datin
Swanee Teh, Nuvanta NuvaceuticalsTM business
unit manager and a pharmacist.
Regarding treatment for perimenopause
signs and symptoms, Datin Swanee said, “We
need to take the cue from Japanese women
who have a high intake of soy. They hardly have
symptoms of menopause or perimenopause.”
Researchers have discovered that the phy-
toestrogen genistein found in soy mimics the
properties of estrogen produced by a woman’s
body naturally. When estrogen levels are low,
genistein helps fill in the gap. When levels are
high, genistein will compete with estrogen in the
body thereby regulating hormonal fluctuations,
said Datin Swanee.
Genistein benefits mood, memory, bone and
heart without any adverse effects on breast or
uterine tissues. Research has also highlighted
genistein’s metabolic-regulating benefits, es-
pecially on fat cells. Genistein is a fat regulator,
which reduces belly fat and inhibits fat accu-
mulation to complement the woman’s effort in
achieving a healthy weight, she added.
Datin Swanee pointed out that a genistein
supplement should be one that is derived from
100% organic soy and is non-genetically modi-
fied. Drinking soymilk is insufficient and not ad-
visable, as it would take at least two gallons of
soymilk to derive the amount of genistein from
one tablet and 80% of soy products in the mar-
ket are genetically modified, she added.
Dr Wong, Ms Hariyati and Datin Swanee
were speaking at a workshop, which was orga-
nized by the Nuvaceuticals division of Nuvanta
Sdn Bhd recently, to raise awareness on
perimenopause.
Left to right: Dr Wong, Datin Swanee and Ms Hariyati with two women who are going through menopause
B i o O i l _ J P O G _ M a r 1 4 - 1 2 0 1 4 - 0 1 - 1 5 T 1 6 : 4 8 : 3 1 + 0 8 : 0 0

AUGUST 2014 PHARMACY PRACTICE 24
Managing COPD in primary care
By Professor Neil Barnes
london Chest hospital, london, uK
By Dr. Ong Kian Chung
President, singapore CoPd association Mt Elizabeth Medical Centre, singapore
Introduction
Chronic obstructive pulmonary disease
(COPD) is a chronic disease involving air-
ways inflammation that affects about 5 percent
of the older population.
While cigarette smoking is the biggest risk
factor, long-term exposure to indoor air pollu-
tion caused by burning of biomass fuels, oc-
cupational dust and chemicals, and underde-
veloped lungs are among other contributing
factors.
Until recently, it was thought that only 15 to
20 percent of cigarette smokers would even-
tually develop COPD at some stage in their
lives. It is now known that about half of smok-
ers will develop this debilitating disease. By
2020, COPD will be the third leading cause of
death worldwide (after ischemic heart disease
and stroke) and the sixth leading cause of dis-
ability.
In many countries, COPD exacerbations are
now either the most common or second most
common reason for hospitalization with an iden-
tifiable medical condition. The situation is likely
to get worse due to an aging population. That
puts general practice in an even more important
position to diagnose the patients before their
lung function deteriorates irreversibly.
COPD is characterized by increased CD8+
T-cells and macrophages in biopsies, and in-
creased neutrophils in sputum.
Diagnosis
Diagnosis of COPD is a two-step process. The
first is making a clinical diagnosis. A GP should
suspect COPD if a smoker or ex-smoker com-
plains of dyspnea, cough, frequent chest infec-
tions and chronic sputum production. But first,
rule out other diseases including asthma, tu-
berculosis, congestive heart failure, obliterative
bronchiolitis and diffuse panbronchiolitis using
differential diagnosis.
The second part of the diagnosis is equally
as important, but happens rather patchily. It con-
sists of the need to confirm clinical diagnosis by
performing spirometry lung function test (LFT).
It is a fairly simple procedure and doesn’t cost
much. Still, many GPs don’t use it. That’s akin to
managing someone with hypertension without
measuring their blood pressure.
In spirometry, more than 80 percent of the
values of forced expiratory volume in one sec-
ond (FEV1), as predicted on the basis of an indi-
vidual patient’s age, sex and ethnicity, will clas-
sify them as having mild COPD, whereas 30 to
50 percent of predicted FEV1 indicates severe

AUGUST 2014 PHARMACY PRACTICE 25
disease. A FEV1 of less than 30 percent of the
predicted value suggests very severe COPD.
While confirming the COPD diagnosis, the lev-
el of lung function also tells you something about
their likelihood of problems in the future. The
worse their lung function, the more likely they are
to run into other health problems in the future.
Practice guidelines
The revised Global initiative for chronic Obstruc-
tive Lung Disease (GOLD) guidelines define two
separate aims in COPD management: symptom
reduction and risk reduction.
The COPD Assessment Test (CAT) is an
eight-point unidimensional measure of health
status impairment. The score ranges from 0 to
40. A score of more than 10 indicates a ‘more
symptomatic’ patient who should be placed into
B or D groups of the assessment chart. The 0-4
point modified British Medical Research Council
(mMRC) dyspnea scale also helps understand
the level of breathlessness (see Figure).
The assessment of risk can either be done
using the FEV1/FVC (forced vital capacity) ratio
with spirometry, using 1-4 GOLD classification
of airflow limitation or it can be based on the
number of exacerbations the patient has had
during the past year. Post-bronchodilator FEV1/
FVC of <0.70 confirms persistent airflow limi-
tation. Patients with a history of two or more
exacerbations per year or very severe airflow
limitation belong to the high risk groups C or D.
Treatment
Treatment strategy for COPD is similar to isch-
emic heart disease as it uses a range of different
4
(C) (D) 2 or more
3
2
(A) (B) Less than 2
1
mMRC 0-1CAT<10
mMRC >2CAT=10
Ris
k(G
old
Cla
ssifi
catio
n of
Airfl
ow L
imita
tion)
Risk
(Exacerbation history)
Symptoms(mMRC or CAT score)
drug and non-drug therapies such as smoking
cessation, lifestyle changes, flu vaccination to
help prevent chest infections, pulmonary reha-
bilitation and drug therapy. The latter includes
short- and long-acting β2-agonists (SABA/
LABA) and muscarinic antagonists (SAMA/
LAMA), inhaled corticosteroids (ICS), phospho-
diesterase-4 (PDE-4) inhibitors and long-acting
anticholinergics such as tiotropium that are
commonly recommended in varying combina-
tions, depending on the disease severity.
Patients with COPD are at high risk of devel-
oping other comorbidities such as cardiovas-
cular disease, osteoporosis, depression and
anxiety, skeletal muscle dysfunction, metabolic
syndrome and lung cancer that can have a sig-
nificant impact on their prognosis. Depending
on their clinical condition, the GOLD guidelines
recommend that an appropriate fluid balance
with special attention to administration of diuret-
ics, anticoagulants, and treatment of comorbidi-
ties and nutritional deficiencies should be con-
sidered.
COPD exacerbations deteriorate quality of
life, reduce lung function that becomes irrevers-
ible in many patients, lead to avoidable hospital-
izations and death. Although frequent exacerba-

AUGUST 2014 PHARMACY PRACTICE 26
tions amount to two or more breathing attacks in
a year, each patient needs to be judged individu-
ally. If someone ends up in a hospital just once
with a really bad exacerbation, that should be
taken as a red flag from the risk reduction point
of view.
Emphasis on risk reduction is, in fact, the
most important change over the previous GOLD
guidelines. Just as in the management of isch-
emic heart disease you want to stop your pa-
tients having angina and chest pain, but also
want to stop them from having a myocardial in-
farct. That concept is familiar to most GPs be-
cause it is how they approach the treatment of
other chronic diseases.
Compliance
Compliance with drug or non-drug therapies
can be a challenge. A good doctor-patient re-
lationship can, however, help improve compli-
ance. If patients feel that the doctor has listened
to them and that the treatment addresses their
needs, they are more likely to stick to the drug
and non-drug treatment regimen. A simple drug
regimen also helps. If patients are required to
take multiple medications at different times of
the day, they have more chances to slip up.
One of the problems with COPD patients is
that they begin to exercise less because they
easily get short of breath. And because they ex-
ercise less, they end up developing other health
problems. That’s why it is important to recom-
mend physical activity at an early stage of COPD.
The more they keep themselves active, the better
it will be not just for their COPD symptoms, but
also for other associated chronic diseases.
The aims of COPD management
Reduce symptoms:
Relieve symptoms, improve exercise
tolerance, improve health status
Reduce risk:
Prevent disease progression, prevent and
treat exacerbations, reduce mortality
To answer the quiz for your CPD points, please go to www.mims-cpd.com.my



P u b l i s h E r
Ben Yeo
C o n t r i b u t i n g E d i t o r s
Saras Ramiya, Pank Jit Sin, Malvinderjit Kaur Dhillon, Dr Joslyn Ngu (Malaysia)
P H A R M A C Y P R A C T I C E E D I T O R
Prof Dr P.T. Thomas
g E n E r a l M a n a g E r
Kimberly Lai
d i v i s i o n M a n a g E r
Meera Jassal
b u s i n E s s M a n a g E r s
Grace Yeoh, Sumitra Pakry, Tiffany Collar
d E s i g n E r
Ken Koh
P r o d u C t i o n
Jasmine Chay
C i r C u l a t i o n E x E C u t i v E
Saratha Nadarajah
a C C o u n t i n g M a n a g E r
Christine Goh
P u b l i s h E d b y
MIMS (Hong Kong) Limited 27th Floor, OTB Building 160 Gloucester Road, Wanchai, Hong Kong Tel: (852) 2559-5888 Fax: (852) 2559-6910 Email: [email protected]
Pharmacy Today is published 11 times a year by MIMS Medica. Pharmacy Today is a controlled circulation publication to pharmacists in Malaysia. It is also available on subscription to members of allied professions. The price per annum is US$48 (surface mail) and US$60 (overseas airmail); back issues at US$5 per copy. Editorial matter published herein has been prepared by professional editorial staff. Articles ending with PTNZ have been adapted from Pharmacy Today New Zealand. Views expressed are not necessarily those of MIMS Medica. Although great effort has been made in compiling and checking the information given in this publication to ensure that it is accurate, the authors, the publisher and their servants or agents shall not be responsible or in any way liable for the continued currency of the information or for any errors, omissions or inaccuracies in this publication whether arising from negligence or otherwise howsoever, or for any consequences arising therefrom. The inclusion or exclusion of any product does not mean that the publisher advocates or rejects its use either generally or in any particular field or fields. The information contained within should not be relied upon solely for final treatment decisions.
© 2014 MIMS Medica. All rights reserved. No part of this publication may be reproduced in any language, stored in or introduced into a retrieval system, or transmitted, in any form or by any means (electronic, mechanical, photocopying, recording or otherwise), without the written consent of the copyright owner. Permission to reprint must be obtained from the publisher. Advertisements are subject to editorial acceptance and have no influence on editorial content or presentation. MIMS Medica does not guarantee, directly or indirectly, the quality or efficacy of any product or service described in the advertisements or other material which is commercial in nature. Printed in Malaysia by KHL Printing Co Sdn Bhd. Lot 10 & 12, Jalan Modal 23/2, Seksyen 23, Kawasan MIEL, Fasa 8, 40000 Shah Alam, Selangor Darul Ehsan.
PP17931/12/2013(033147) ISSN 1170-1927
Ed itor ial adv isory board
Dato’ Eisah A. Rahman Pharmaceutical Services Division, Ministry of Health
Datuk Nancy Ho President,Malaysian Pharmaceutical Society
Yip Sook Ying Secretary, Malaysian Pharmaceutical Society
Assoc Prof Dr Mohamad Haniki Nik Mohamed Malaysian Academy of Pharmacy
Prof Dr P.T. Thomas Dean, School of Pharmacy, Taylor’s University





























