Embed Size (px)
Citation preview
General Information
Name ____________________________________________ Age _____ Today’s Date ___________________
Date of Birth ________________________ Email _________________________________________________
Address __________________________________ City ___________________ State ____ Zip _________
Phone (Home) _____________________ (Cell) ______________________ (Work) _____________________
Genetic Background: oAfrican American oHispanic oMediterranean oAsian oNative American oCaucasian oNorthern European
oOther _________________________________________________________________
When, where and from whom did you last receive medical or health care? ________________________________
___________________________________________________________________________________________
Emergency Contact: _____________________________________ Relationship ________________________
Phone (Home) _____________________ (Cell) ______________________ (Work) _____________________
How did you hear about our practice?
oClinic website oIFM website oReferral from doctor oReferral from friend/family memberoSocial media oOther ___________________________________________________________________
Current Health Concerns
Please rank current and ongoing health concerns in order of priority
Male Intake Questionnaire
Describe Problem Severity
Prior Treatment/Approach Success
Example: Post Nasal Drip X Elimination Diet X
1.
2.
3.
4.
5.
7.
8.
9.
9.
10.
Mild
Exce
llent
Mod
era
te
Goo
d
Seve
re
Fair
© 2015 The Institute for Functional MedicineVersion 2
IFM n Male Intake Questionnaire 2© 2015 The Institute for Functional Medicine
Allergies
Name of Medication/Supplement/Food: Reaction:
1.
2.
3.
4.
5.
Activity Type # of Times Per Week Time/Duration (Minutes)
Cardio/Aerobic
Strength/Resistance
Flexibility/Stretching
Balance
Sports/Leisure (e.g., golf)
Other:
Lifestyle Review
Sleep
How many hours of sleep do you get each night on average? ___________________________________________
Do you have problems falling asleep? oYes oNo Staying asleep? oYes oNoDo you have problems with insomnia? oYes oNo Do you snore? oYes oNoDo you feel rested upon awakening? oYes oNoDo you use sleeping aids? oYes oNo
If yes, explain: ______________________________________________________________________________
Exercise
Current Exercise Program:
Do you feel motivated to exercise? oYes oA little oNo
Are there any problems that limit exercise? oYes oNoIf yes, explain: ______________________________________________________________________________
Do you feel unusually fatigued or sore after exercise? oYes oNoIf yes, explain: ______________________________________________________________________________
IFM n Male Intake Questionnaire 3© 2015 The Institute for Functional Medicine
Nutrition
Do you currently follow any of the following special diets or nutritional programs? (Check all that apply)
oVegetarian oVegan oAllergy oElimination oLow Fat oLow Carb oHigh ProteinoBlood Type oLow sodium oNo Dairy oNo Wheat oGluten FreeoOther: _________________________________________________________________________________
Do you have sensitivities to certain foods? oYes oNoIf yes, list food and symptoms: _________________________________________________________________
Do you have an aversion to certain foods? oYes oNoIf yes, explain: ______________________________________________________________________________
Do you adversely react to: (Check all that apply)
oMonosodium glutamate (MSG) oArtificial sweeteners oGarlic/onion oCheese oCitrus foodsoChocolate oAlcohol oRed wine oSulfite–containing foods (wine, dried fruit, salad bars)oPreservatives oFood colorings oOther food substances: ____________________________________
Are there any foods that you crave or binge on? oYes oNo If yes, what foods?___________________________________________________________________________
Do you eat 3 meals a day? oYes oNo If no, how many _______________________________________
Does skipping a meal greatly affect you? oYes oNo
How many meals do you eat out per week? o0–1 o1–3 o3–5 o>5 meals per week
Check the factors that apply to your current lifestyle and eating habits:
oFast eateroEat too muchoLate-night eatingoDislike healthy foodsoTime constraintsoTravel frequentlyoEat more than 50% of meals away from homeoHealthy foods not readily availableoPoor snack choicesoSignificant other or family members don’t like
healthy foods
oSignificant other or family members have special dietary needs
oLove to eatoEat because I have tooHave negative relationship to foodoStruggle with eating issuesoEmotional eater (eat when sad, lonely, bored, etc.)oEat too much under stressoEat too little under stressoDon’t care to cookoConfused about nutrition advice
IFM n Male Intake Questionnaire 4© 2015 The Institute for Functional Medicine
Diet
Please record what you eat in a typical day:
Breakfast ___________________________________________________________________________________
Lunch _____________________________________________________________________________________
Dinner _____________________________________________________________________________________
Snacks _____________________________________________________________________________________
Fluids ______________________________________________________________________________________
How many servings do you eat in a typical week of these foods:
Fruits (not juice) _____ Vegetables (not including white potatoes) _____Legumes (beans, peas, etc) _____ Red meat _____ Fish _____Dairy/Alternatives _____ Nuts & Seeds _____ Fats & Oils _____Cans of soda (regular or diet) _____ Sweets (candy, cookies, cake, ice cream, etc.) _____
Do you drink caffeinated beverages? oYes oNo If yes, check amounts:
Coffee (cups per day) o1 o2-4 o>4 Tea (cups per day) o1 o2-4 o>4Caffeinated sodas—regular or diet (cans per day) o1 o2-4 o>4
Do you have adverse reactions to caffeine? oYes oNoIf yes, explain: ______________________________________________________________________________
When you drink caffeine do you feel: oIrritable or wired oAches or pains
Smoking
Do you smoke currently? oYes oNo Packs per day: ______ Number of years _____What type? oCigarettes oSmokeless oPipe oCigar oE-CigHave you attempted to quit? oYes oNo
If yes, using what methods: ____________________________________________________________________
If you smoked previously: Packs per day: _____ Number of years _____Are you regularly exposed to second-hand smoke? oYes oNo
Alcohol
How many alcoholic beverages do you drink in a week? (1 drink = 5 ounces wine, 12 ounces beer, 1.5 ounces spirits)o1–3 o4–6 o7–10 o>10 oNone
Previous alcohol intake? oYes (oMild oModerate oHigh) oNone
Have you ever had a problem with alcohol? oYes oNoIf yes, when? _______________________________________________________________________________Explain the problem: ________________________________________________________________________
Have you ever thought about getting help to control or stop your drinking? oYes oNo
Other Substances
Are you currently using any recreational drugs? oYes oNoIf yes, type: ________________________________________________________________________________
Have you ever used IV or inhaled recreational drugs? oYes oNo
IFM n Male Intake Questionnaire 5© 2015 The Institute for Functional Medicine
N/A Poorly Fine Very Well
Overall o 1 2 3 4 5 6 7 8 9 10
At school o 1 2 3 4 5 6 7 8 9 10
In your job o 1 2 3 4 5 6 7 8 9 10
In your social life o 1 2 3 4 5 6 7 8 9 10
With close friends o 1 2 3 4 5 6 7 8 9 10
With sex o 1 2 3 4 5 6 7 8 9 10
With your attitude o 1 2 3 4 5 6 7 8 9 10
With your boyfriend/girlfriend o 1 2 3 4 5 6 7 8 9 10
With your children o 1 2 3 4 5 6 7 8 9 10
With your parents o 1 2 3 4 5 6 7 8 9 10
With your spouse o 1 2 3 4 5 6 7 8 9 10
Stress
Do you feel you have an excessive amount of stress in your life? oYes oNo
Do you feel you can easily handle the stress in your life? oYes oNo
How much stress do each of the following cause on a daily basis (Rate on scale of 1-10, 10 being highest)Work ____ Family ____ Social ____ Finances ____ Health ____ Other ____
Do you use relaxation techniques? oYes oNoIf yes, how often? ___________________________________________________________________________
Which techniques do you use? (Check all that apply)
oMeditation oBreathing oTai Chi oYoga oPrayer oOther: ___________________________
Have you ever sought counseling? oYes oNo
Are you currently in therapy? oYes oNoIf yes, describe: _____________________________________________________________________________
Have you ever been abused, a victim of crime, or experienced a significant trauma? oYes oNo
What are your hobbies or leisure activities? _________________________________________________________
Relationships
Marital status: oSingle oMarried oDivorced oGay/Lesbian oLong-Term Partner oWidow/er
With whom do you live? (Include children, parents, relatives, friends, pets) ________________________________
___________________________________________________________________________________________
Current occupation: __________________________________________________________________________
Previous occupations:__________________________________________________________________________
Do you have resources for emotional support? oYes ooNo (Check all that apply)
oSpouse/Partner oFamily oFriends oReligious/Spiritual oPets oOther: _______________
Do you have a religious or spiritual practice? oYes oNo
If yes, what kind? ___________________________________________________________________________
How well have things been going for you? (Mark on scale of 1–10, or N/A if not applicable)
IFM n Male Intake Questionnaire 6© 2015 The Institute for Functional Medicine
History
Patient’s Birth/Childhood History:
You were born: oTerm oPremature oDon’t know
Were there any pregnancy or birth complications? oYes oNoIf yes, explain: ______________________________________________________________________________
You were: oBreast-fed/How long? _______ oBottle-fed/Type of formula: ___________ oDon’t know
Age of introduction of: Solid food: ______ Wheat _______ Dairy _______
As a child, were there any foods that were avoided because they gave you symptoms? oYes oNoIf yes, what foods and what symptoms? (Example: milk—gas and diarrhea) _________________________________________________________________________________________
_________________________________________________________________________________________
Did you eat a lot of sugar or candy as a child? oYes oNo
Dental History:
Check if you have any of the following, and provide number if applicable:
oSilver mercury fillings ____ oGold fillings ____ oRoot canals ____ oImplants ____oCaps/Crowns ____ oTooth pain ____ oBleeding gums ____ oGingivitis _____oProblems with chewing ____ oOther dental concerns (explain): _____
Have you had any mercury fillings removed? oYes oNo If yes, when: ____________________________
How many fillings did you have as a kid? ______________
Do you brush regularly? oYes oNo Do you floss regularly? oYes oNo
Environmental/Detoxification History
Do any of these significantly affect you?
oCigarette smoke oPerfume/colognes oAuto exhaust fumes oOther: ______________________
In your work or home environment are you regularly exposed to: (Check all that apply)
oMold oWater leaks oRenovations oChemicals oElectromagnetic radiationoDamp environments oCarpets or rugs oOld paint oStagnant or stuffy air oSmokersoPesticides oHerbicides oHarsh chemicals (solvents, glues, gas, acids, etc) oCleaning chemicalsoHeavy metals (lead, mercury, etc.) oPaints oAirplane travel oOther ________________________
Have you had a significant exposure to any harmful chemicals? oYes oNoIf yes: Chemical name, length of exposure, date: ____________________________________________________
Do you have any pets or farm animals? oYes oNoIf yes, do they live: oInside oOutside oBoth inside and outside
Men’s History
(Check box if applicable)
oTesticular mass oTesticular pain oProstate enlargement oProstate infection oChange in sex drive oImpotence oPremature ejaculation oDifficulty obtaining an erectionoDifficulty maintaining an erection oLoss of control of urine oUrinary urgency/hesitancy/change in streamoVasectomy oNocturia (urination at night) # of times per night _______________oSexually transmitted diseases (describe) ________________________________________________________

IFM n Male Intake Questionnaire 7© 2015 The Institute for Functional Medicine
Men’s History (cont.)
Screening/Procedures: (If applicable, provide date)
Last PSA test: _____________________ PSA Level: o0–2 o2–4 o4–10 o>10
Other tests/procedures (list type and dates) _________________________________________________________
___________________________________________________________________________________________
Family History:
Check family members that have/had any of the following
Age (if still alive)
Age at death (if deceased)
Cancer o o o o o o o o o o o o o
Heart disease o o o o o o o o o o o o o
Hypertension o o o o o o o o o o o o o
Obesity o o o o o o o o o o o o o
Diabetes o o o o o o o o o o o o o
Stroke o o o o o o o o o o o o o
Autoimmune disease o o o o o o o o o o o o o
Arthritis o o o o o o o o o o o o o
Kidney disease o o o o o o o o o o o o o
Thyroid problems o o o o o o o o o o o o o
Seizures/epilepsy o o o o o o o o o o o o o
Psychiatric disorders o o o o o o o o o o o o o
Anxiety o o o o o o o o o o o o o
Depression o o o o o o o o o o o o o
Asthma o o o o o o o o o o o o o
Allergies o o o o o o o o o o o o o
Eczema o o o o o o o o o o o o o
ADHD o o o o o o o o o o o o o
Autism o o o o o o o o o o o o o
Irritable Bowel Syndrome o o o o o o o o o o o o o
Dementia o o o o o o o o o o o o o
Substance abuse o o o o o o o o o o o o o
Genetic disorders o o o o o o o o o o o o o
Other: o o o o o o o o o o o o o
Mot
her
Fath
er
Brot
her
(s)
Sist
er (
s)
Chi
ld
Chi
ld
Chi
ld
Chi
ld
Ma
tern
al
Gra
ndm
othe
r
Ma
tern
al
Gra
ndfa
ther
Pate
rna
l G
rand
mot
her
Pate
rna
l G
rand
fath
er
Oth
er
IFM n Male Intake Questionnaire 8© 2015 The Institute for Functional Medicine
Gastrointestinal Yes Past
Irritable bowel syndrome o oGERD (reflux) o oCrohn’s disease/ulcerative colitis o oPeptic ulcer disease o oCeliac disease o oGallstones o oOther: o o
Respiratory
Bronchitis o oAsthma o oEmphysema o oPneumonia o oSinusitis o oSleep apnea o oOther: o o
Urinary/Genital
Kidney stones o oGout o oInterstitial cystitis o oFrequent yeast infections o oFrequent urinary tract infections o oSexual dysfunction o oSexually transmitted diseases o oOther: o o
Endocrine/MetabolicDiabetes o oHypothyroidism (low thyroid) o oHyperthyroidism (overactive thyroid) o oInfertility o oMetabolic syndrome/insulin resistance o oEating disorder o oHypoglycemia o oOther: o o
Inflammatory/Immune
Rheumatoid arthritis o oChronic fatigue syndrome o oFood allergies o oEnvironmental allergies o oMultiple chemical sensitivities o oAutoimmune disease o oImmune deficiency o oMononucleosis o oHepatitis o oOther: o o
Musculoskeletal Yes Past
Fibromyalgia o oOsteoarthritis o oChronic pain o oOther: o o
Skin
Eczema o oPsoriasis o oAcne o oSkin cancer o oOther: o o
Cardiovascular
Angina o oHeart attack o oHeart failure o oHypertension (high blood pressure) o oStroke o oHigh blood fats (cholesterol, triglycerides) o oRheumatic fever o oArrythmia (irregular heart rate) o oMurmur o oMitral valve prolapse o oOther: o o
Neurologic/EmotionalEpilepsy/Seizures o oADD/ADHD o oHeadaches o oMigraines o oDepression o oAnxiety o oAutism o oMultiple sclerosis o oParkinson’s disease o oDementia o oOther: o o
Cancer
Lung o oBreast o oColon o oProstate o oSkin o oOther: o o
Medical History: Illnesses/Conditions
Check YES = a condition you currently have, Check PAST = a condition you’ve had in the past.
IFM n Male Intake Questionnaire 9© 2015 The Institute for Functional Medicine
Diagnostic Studies Date Comments
Bone density
CT scan
Colonoscopy
Cardiac stress test
EKG
MRI
Upper endoscopy
Upper GI series
Chest X-ray
Other X-rays
Barium enema
Other:
Injuries
Broken bone(s)
Back injury
Neck injury
Head injury
Other:
Surgeries
Appendectomy
Dental
Gallbladder
Hernia
Tonsillectomy
Joint replacement
Heart surgery
Other:
Hospitalizations Date Reason
Medical History (cont.)
IFM n Male Intake Questionnaire 10© 2015 The Institute for Functional Medicine
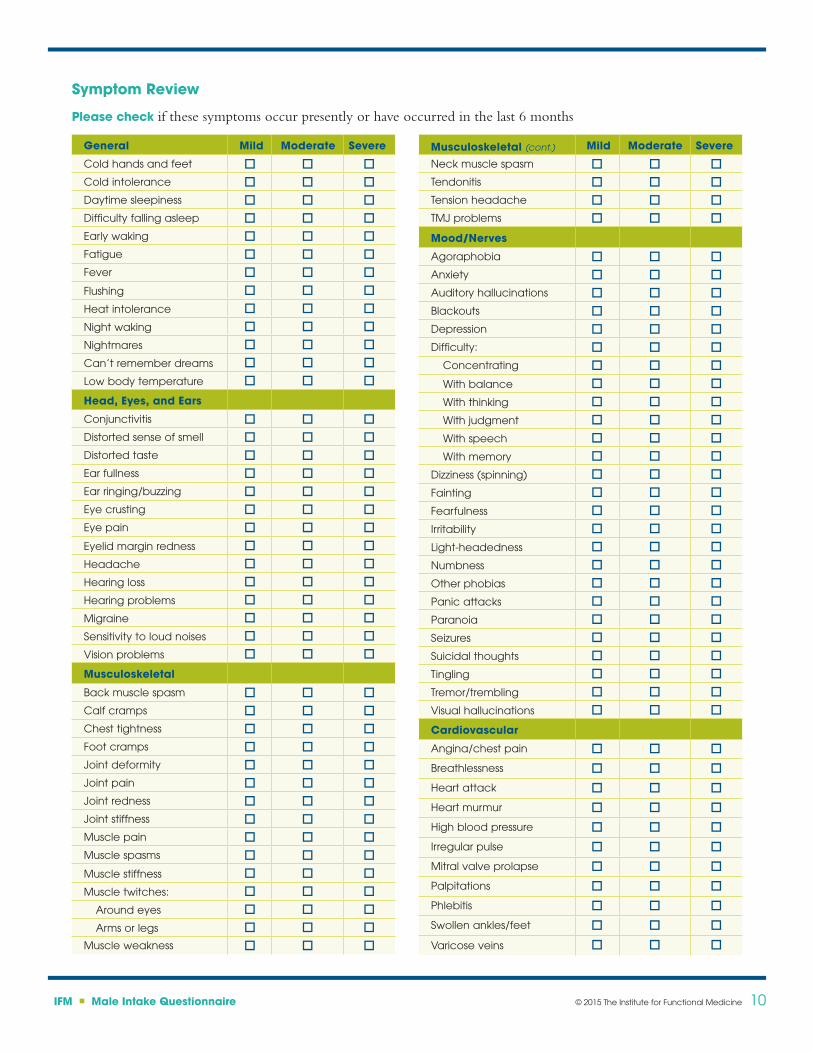
Symptom Review
Please check if these symptoms occur presently or have occurred in the last 6 months
General Mild Moderate Severe
Cold hands and feet o o oCold intolerance o o oDaytime sleepiness o o oDifficulty falling asleep o o oEarly waking o o oFatigue o o oFever o o oFlushing o o oHeat intolerance o o oNight waking o o oNightmares o o oCan’t remember dreams o o oLow body temperature o o o
Head, Eyes, and Ears
Conjunctivitis o o oDistorted sense of smell o o oDistorted taste o o oEar fullness o o oEar ringing/buzzing o o oEye crusting o o oEye pain o o oEyelid margin redness o o oHeadache o o oHearing loss o o oHearing problems o o oMigraine o o oSensitivity to loud noises o o oVision problems o o o
Musculoskeletal
Back muscle spasm o o oCalf cramps o o oChest tightness o o oFoot cramps o o oJoint deformity o o oJoint pain o o oJoint redness o o oJoint stiffness o o oMuscle pain o o oMuscle spasms o o oMuscle stiffness o o oMuscle twitches: o o o
Around eyes o o oArms or legs o o o
Muscle weakness o o o
Musculoskeletal (cont.) Mild Moderate Severe
Neck muscle spasm o o oTendonitis o o oTension headache o o oTMJ problems o o o
Mood/Nerves
Agoraphobia o o oAnxiety o o oAuditory hallucinations o o oBlackouts o o oDepression o o oDifficulty: o o o
Concentrating o o oWith balance o o oWith thinking o o oWith judgment o o oWith speech o o oWith memory o o o
Dizziness (spinning) o o oFainting o o oFearfulness o o oIrritability o o oLight-headedness o o oNumbness o o oOther phobias o o oPanic attacks o o oParanoia o o oSeizures o o oSuicidal thoughts o o oTingling o o oTremor/trembling o o oVisual hallucinations o o o
Cardiovascular
Angina/chest pain o o o
Breathlessness o o o
Heart attack o o o
Heart murmur o o o
High blood pressure o o o
Irregular pulse o o o
Mitral valve prolapse o o o
Palpitations o o o
Phlebitis o o o
Swollen ankles/feet o o o
Varicose veins o o o
IFM n Male Intake Questionnaire 11© 2015 The Institute for Functional Medicine
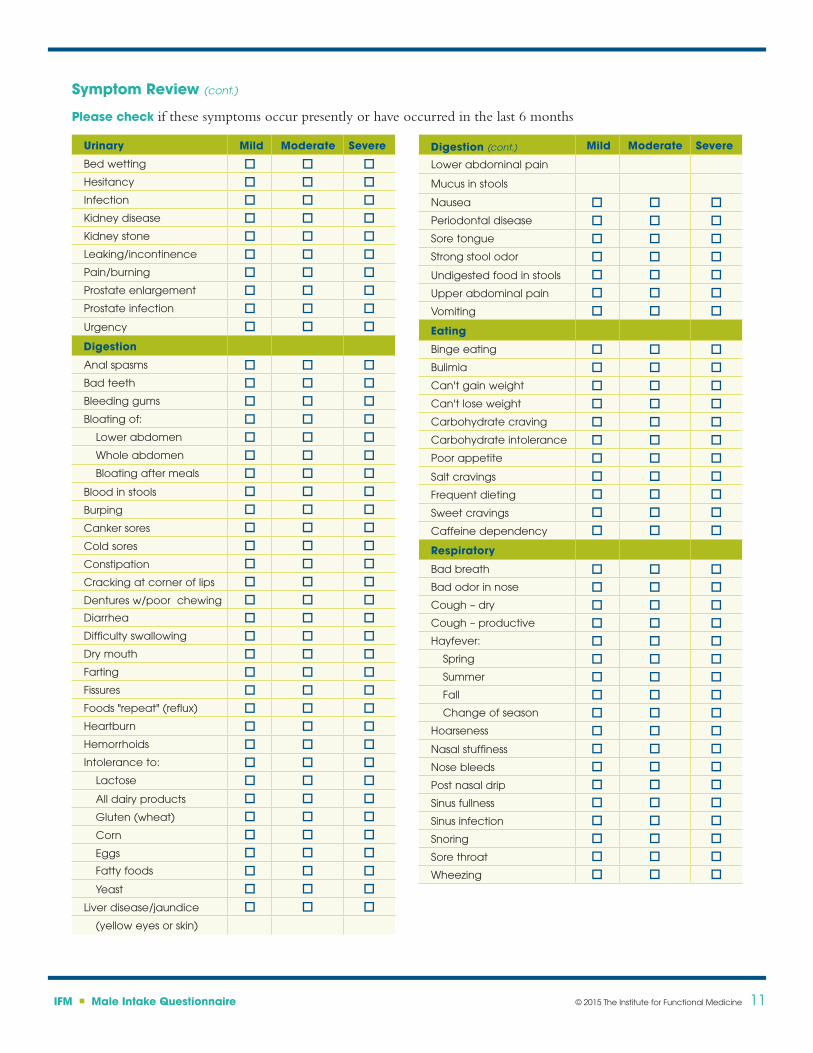
Symptom Review (cont.)
Please check if these symptoms occur presently or have occurred in the last 6 months
Urinary Mild Moderate Severe
Bed wetting o o oHesitancy o o oInfection o o oKidney disease o o oKidney stone o o oLeaking/incontinence o o oPain/burning o o oProstate enlargement o o oProstate infection o o oUrgency o o o
Digestion
Anal spasms o o oBad teeth o o oBleeding gums o o oBloating of: o o o
Lower abdomen o o oWhole abdomen o o oBloating after meals o o o
Blood in stools o o oBurping o o oCanker sores o o oCold sores o o oConstipation o o oCracking at corner of lips o o oDentures w/poor chewing o o oDiarrhea o o oDifficulty swallowing o o oDry mouth o o oFarting o o oFissures o o oFoods "repeat" (reflux) o o oHeartburn o o oHemorrhoids o o oIntolerance to: o o o
Lactose o o oAll dairy products o o oGluten (wheat) o o oCorn o o oEggs o o oFatty foods o o oYeast o o o
Liver disease/jaundice o o o(yellow eyes or skin)
Digestion (cont.) Mild Moderate Severe
Lower abdominal pain
Mucus in stools
Nausea o o oPeriodontal disease o o oSore tongue o o oStrong stool odor o o oUndigested food in stools o o oUpper abdominal pain o o oVomiting o o o
Eating
Binge eating o o oBulimia o o oCan't gain weight o o oCan't lose weight o o oCarbohydrate craving o o oCarbohydrate intolerance o o oPoor appetite o o oSalt cravings o o oFrequent dieting o o oSweet cravings o o oCaffeine dependency o o o
Respiratory
Bad breath o o oBad odor in nose o o oCough – dry o o oCough – productive o o oHayfever: o o o
Spring o o oSummer o o oFall o o oChange of season o o o
Hoarseness o o oNasal stuffiness o o oNose bleeds o o oPost nasal drip o o oSinus fullness o o oSinus infection o o oSnoring o o oSore throat o o oWheezing o o o
IFM n Male Intake Questionnaire 12© 2015 The Institute for Functional Medicine
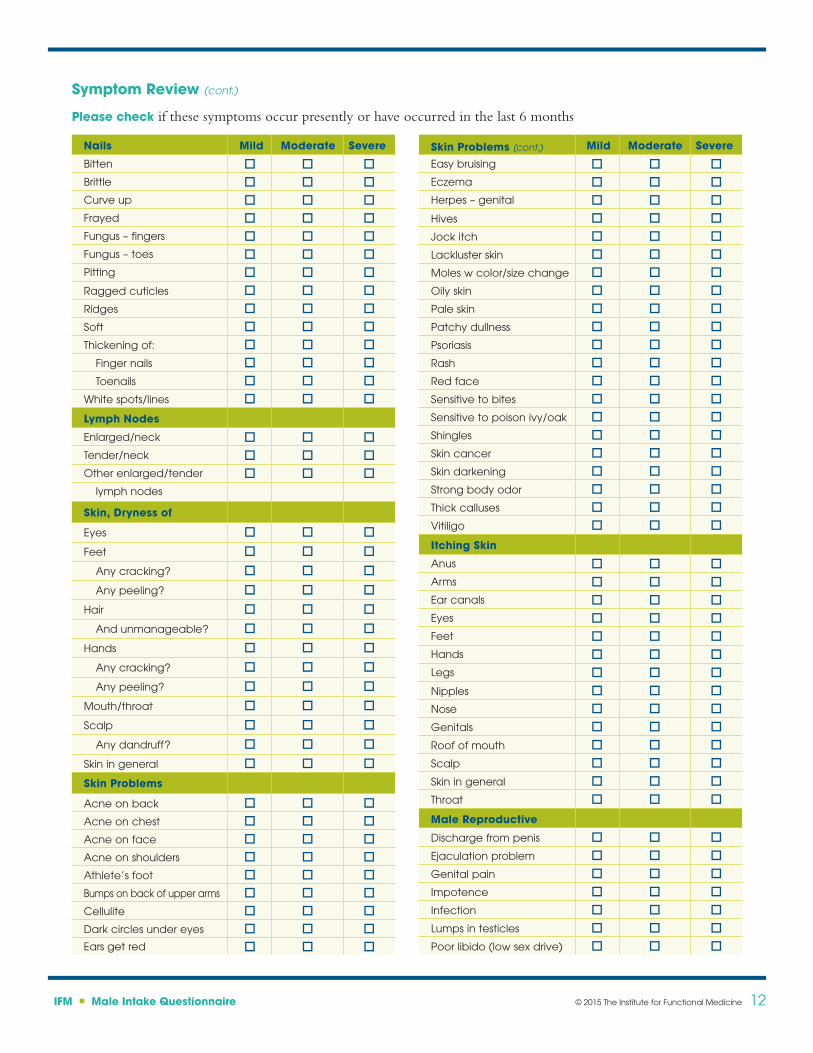
Symptom Review (cont.)
Please check if these symptoms occur presently or have occurred in the last 6 months
Nails Mild Moderate Severe
Bitten o o oBrittle o o oCurve up o o oFrayed o o oFungus – fingers o o oFungus – toes o o oPitting o o oRagged cuticles o o oRidges o o oSoft o o oThickening of: o o o
Finger nails o o oToenails o o o
White spots/lines o o o
Lymph Nodes
Enlarged/neck o o oTender/neck o o oOther enlarged/tender o o o
lymph nodes
Skin, Dryness of
Eyes o o o
Feet o o o
Any cracking? o o o
Any peeling? o o o
Hair o o o
And unmanageable? o o o
Hands o o o
Any cracking? o o o
Any peeling? o o o
Mouth/throat o o o
Scalp o o o
Any dandruff? o o o
Skin in general o o o
Skin Problems
Acne on back o o oAcne on chest o o oAcne on face o o oAcne on shoulders o o oAthlete’s foot o o oBumps on back of upper arms o o oCellulite o o oDark circles under eyes o o oEars get red o o o
Skin Problems (cont.) Mild Moderate Severe
Easy bruising o o oEczema o o oHerpes – genital o o oHives o o oJock itch o o oLackluster skin o o oMoles w color/size change o o oOily skin o o oPale skin o o oPatchy dullness o o oPsoriasis o o oRash o o oRed face o o oSensitive to bites o o oSensitive to poison ivy/oak o o oShingles o o oSkin cancer o o oSkin darkening o o oStrong body odor o o oThick calluses o o oVitiligo o o o
Itching Skin
Anus o o oArms o o oEar canals o o oEyes o o oFeet o o oHands o o oLegs o o oNipples o o oNose o o oGenitals o o oRoof of mouth o o oScalp o o oSkin in general o o oThroat o o o
Male Reproductive
Discharge from penis o o oEjaculation problem o o oGenital pain o o oImpotence o o oInfection o o oLumps in testicles o o oPoor libido (low sex drive) o o o
IFM n Male Intake Questionnaire 13© 2015 The Institute for Functional Medicine
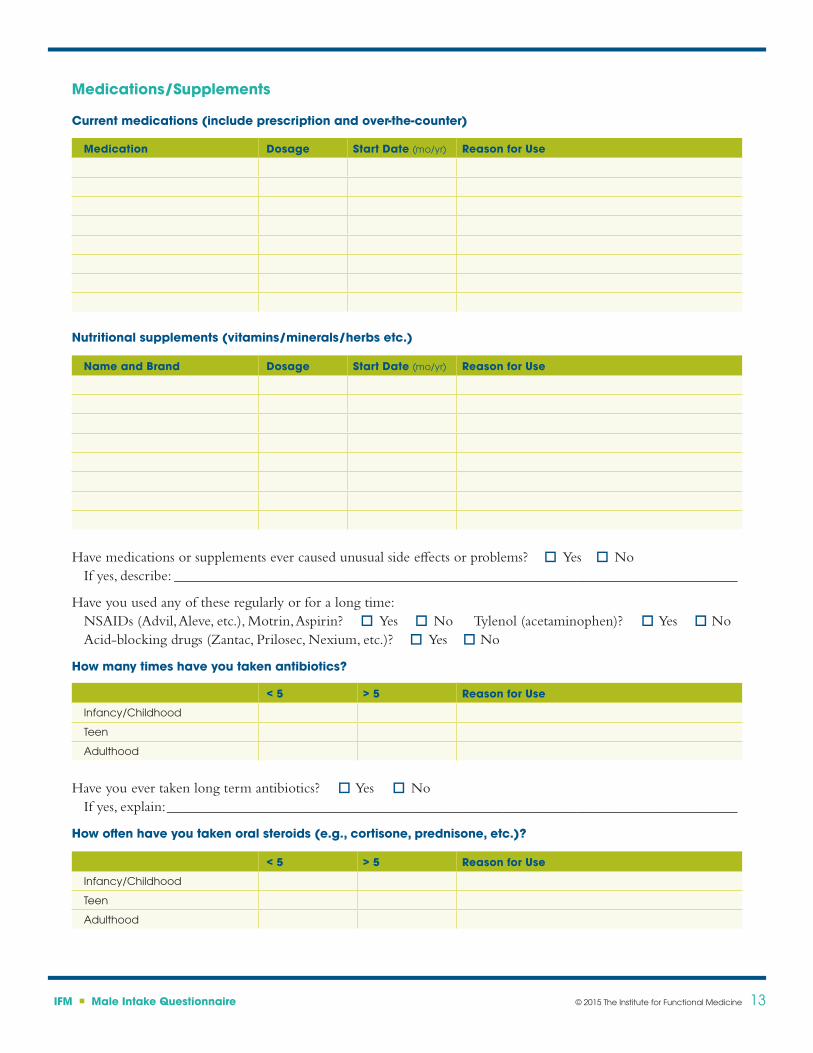
Medications/Supplements
Current medications (include prescription and over-the-counter)
Medication Dosage Start Date (mo/yr) Reason for Use
Nutritional supplements (vitamins/minerals/herbs etc.)
Name and Brand Dosage Start Date (mo/yr) Reason for Use
Have medications or supplements ever caused unusual side effects or problems? oYes oNoIf yes, describe: _____________________________________________________________________________
Have you used any of these regularly or for a long time:NSAIDs (Advil, Aleve, etc.), Motrin, Aspirin? oYes oNo Tylenol (acetaminophen)? oYes oNoAcid-blocking drugs (Zantac, Prilosec, Nexium, etc.)? oYes oNo
How many times have you taken antibiotics?
< 5 > 5 Reason for Use
Infancy/Childhood
Teen
Adulthood
< 5 > 5 Reason for Use
Infancy/Childhood
Teen
Adulthood
Have you ever taken long term antibiotics? oYes oNoIf yes, explain: ______________________________________________________________________________
How often have you taken oral steroids (e.g., cortisone, prednisone, etc.)?
IFM n Male Intake Questionnaire 14© 2015 The Institute for Functional Medicine
Readiness Assessment and Health Goals
Readiness Assessment
Rate on a scale of 5 (very willing) to 1 (not willing):
In order to improve your health, how willing are you to:Significantly modify your diet o 5 o4 o3 o2 o 1Take several nutritional supplements each day o5 o 4 o3 o2 o 1Keep a record of everything you eat each day o 5 o 4 o3 o2 o1Modify your lifestyle (e.g., work demands, sleep habits) o 5 o 4 o3 o2 o1Practice a relaxation technique o 5 o 4 o3 o2 o 1Engage in regular exercise o5 o4 o3 o2 o 1
Rate on a scale of 5 (very confident) to 1 (not confident at all):
How confident are you of your ability to organize and follow through on the above health-related activities? o 5 o 4 o3 o2 o 1
If you are not confident of your ability, what aspects of yourself or your life lead you to question your capacity to follow through? _____________________________________
_________________________________________________________________________________________
Rate on a scale of 5 (very supportive) to 1 (very unsupportive):
At the present time, how supportive do you think the people in your household will be to your implementing the above changes? o5 o4 o3 o2 o1
Rate on a scale of 5 (very frequent contact) to 1 (very infrequent contact):
How much ongoing support (e.g., telephone consults, email correspondence) from our professional staff would be helpful to you as you implement your personal health program? o5 o4 o3 o2 o1
Comments ________________________________________________________________________________
_________________________________________________________________________________________
IFM n Male Intake Questionnaire 15© 2015 The Institute for Functional Medicine
Health Goals
What do you hope to achieve in your visit with us? __________________________________________________
___________________________________________________________________________________________
___________________________________________________________________________________________
When was the last time you felt well? _____________________________________________________________
___________________________________________________________________________________________
___________________________________________________________________________________________
Did something trigger your change in health? ______________________________________________________
___________________________________________________________________________________________
___________________________________________________________________________________________
What makes you feel better? ____________________________________________________________________
___________________________________________________________________________________________
___________________________________________________________________________________________
What makes you feel worse? ____________________________________________________________________
___________________________________________________________________________________________
___________________________________________________________________________________________
How does your condition affect you? _____________________________________________________________
___________________________________________________________________________________________
___________________________________________________________________________________________
What do you think is happening and why? _________________________________________________________
___________________________________________________________________________________________
___________________________________________________________________________________________
What do you feel needs to happen for you to get better? ______________________________________________
___________________________________________________________________________________________
___________________________________________________________________________________________
Medical Symptoms Questionnaire (MSQ)
Patient Name _______________________________________________________________ Date ___________________
Rate each of the following symptoms based upon your typical health profile for the past 14 days.
Point Scale 0 – Never or almost never have the symptom1 – Occasionally have it, effect is not severe 2 – Occasionally have it, effect is severe
__________ Headaches __________ Faintness __________ Dizziness __________ Insomnia Total _________
__________ Watery or itchy eyes __________ Swollen, reddened or sticky eyelids __________ Bags or dark circles under eyes __________ Blurred or tunnel vision Total _________ (Does not include near or far-sightedness)
__________ Itchy ears __________ Earaches, ear infections __________ Drainage from ear __________ Ringing in ears, hearing loss Total _________
__________ Stuffy nose __________ Sinus problems __________ Hay fever __________ Sneezing attacks __________ Excessive mucus formation Total _________
__________ Chronic coughing __________ Gagging, frequent need to clear throat __________ Sore throat, hoarseness, loss of voice __________ Swollen or discolored tongue, gums, lips __________ Canker sores Total _________
__________ Acne __________ Hives, rashes, dry skin __________ Hair loss __________ Flushing, hot flashes __________ Excessive sweating Total _________
__________ Irregular or skipped heartbeat __________ Rapid or pounding heartbeat __________ Chest pain Total _________
3 – Frequently have it, effect is not severe 4 – Frequently have it, effect is severe
EYES
EARS
NOSE
MOUTH/THROAT
SKIN
HEART
HEAD
Version 2
MEDICAL SYMPTOMS QUESTIONNAIRE (MSQ)
__________ Chest congestion __________ Asthma, bronchitis __________ Shortness of breath __________ Difficulty breathing Total _________
__________ Nausea, vomiting __________ Diarrhea __________ Constipation __________ Bloated feeling__________ Belching, passing gas __________ Heartburn __________ Intestinal/stomach pain Total _________
__________ Pain or aches in joints __________ Arthritis __________ Stiffness or limitation of movement __________ Pain or aches in muscles __________ Feeling of weakness or tiredness Total _________
__________ Binge eating/drinking __________ Craving certain foods __________ Excessive weight __________ Compulsive eating __________ Water retention __________ Underweight Total _________
__________ Fatigue, sluggishness __________ Apathy, lethargy __________ Hyperactivity __________ Restlessness Total _________
__________ Poor memory __________ Confusion, poor comprehension __________ Poor concentration __________ Poor physical coordination __________ Difficulty in making decisions __________ Stuttering or stammering __________ Slurred speech __________ Learning disabilities Total _________
__________ Mood swings __________ Anxiety, fear, nervousness __________ Anger, irritability, aggressiveness __________ Depression Total _________
__________ Frequent illness __________ Frequent or urgent urination __________ Genital itch or discharge Total _________
Grand Total _________
DIGESTIVE TRACT
JOINTS/MUSCLE
WEIGHT
ENERGY/ACTIVITY
MIND
EMOTIONS
OTHER
LUNGS
Taking an Exposure History
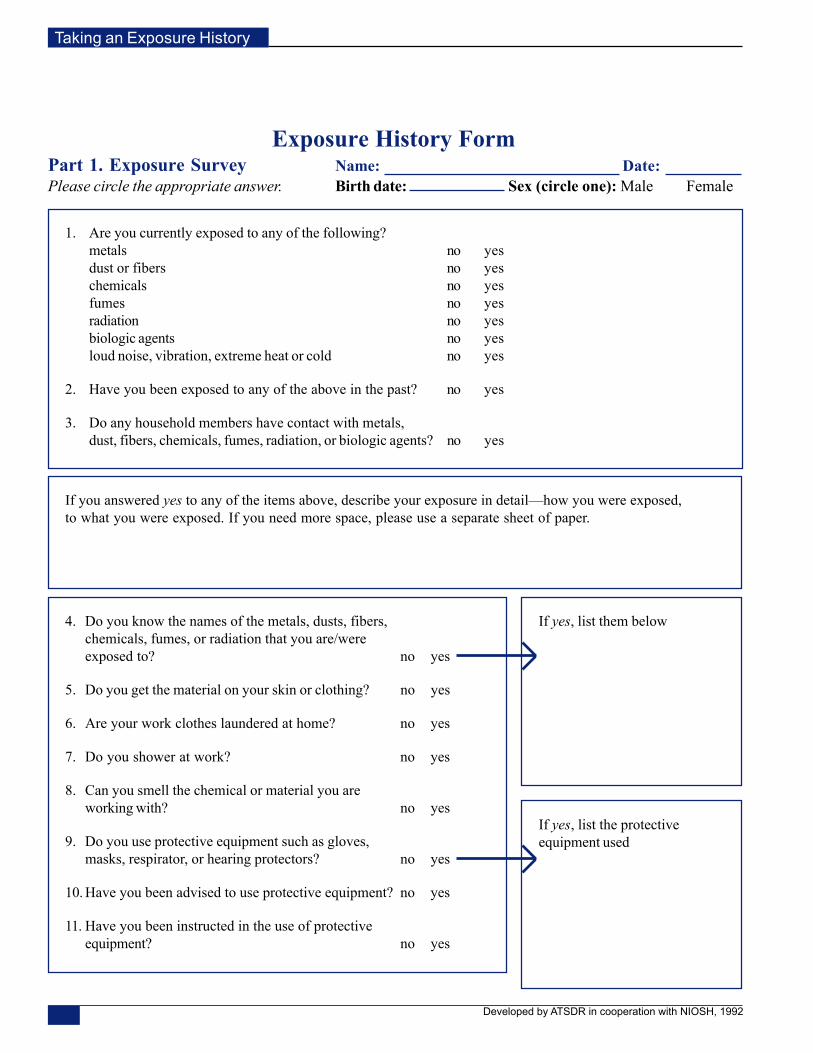
Exposure History FormPart 1. Exposure Survey Name: Date:Please circle the appropriate answer. Birth date: Sex (circle one): Male Female
1. Are you currently exposed to any of the following?metals no yesdust or fibers no yeschemicals no yesfumes no yesradiation no yesbiologic agents no yesloud noise, vibration, extreme heat or cold no yes
2. Have you been exposed to any of the above in the past? no yes
3. Do any household members have contact with metals,dust, fibers, chemicals, fumes, radiation, or biologic agents? no yes
If you answered yes to any of the items above, describe your exposure in detail—how you were exposed,to what you were exposed. If you need more space, please use a separate sheet of paper.
4. Do you know the names of the metals, dusts, fibers,chemicals, fumes, or radiation that you are/wereexposed to? no yes
5. Do you get the material on your skin or clothing? no yes
6. Are your work clothes laundered at home? no yes
7. Do you shower at work? no yes
8. Can you smell the chemical or material you areworking with? no yes
9. Do you use protective equipment such as gloves,masks, respirator, or hearing protectors? no yes
10. Have you been advised to use protective equipment? no yes
11. Have you been instructed in the use of protectiveequipment? no yes
If yes, list them below
If yes, list the protectiveequipment used
Developed by ATSDR in cooperation with NIOSH, 1992
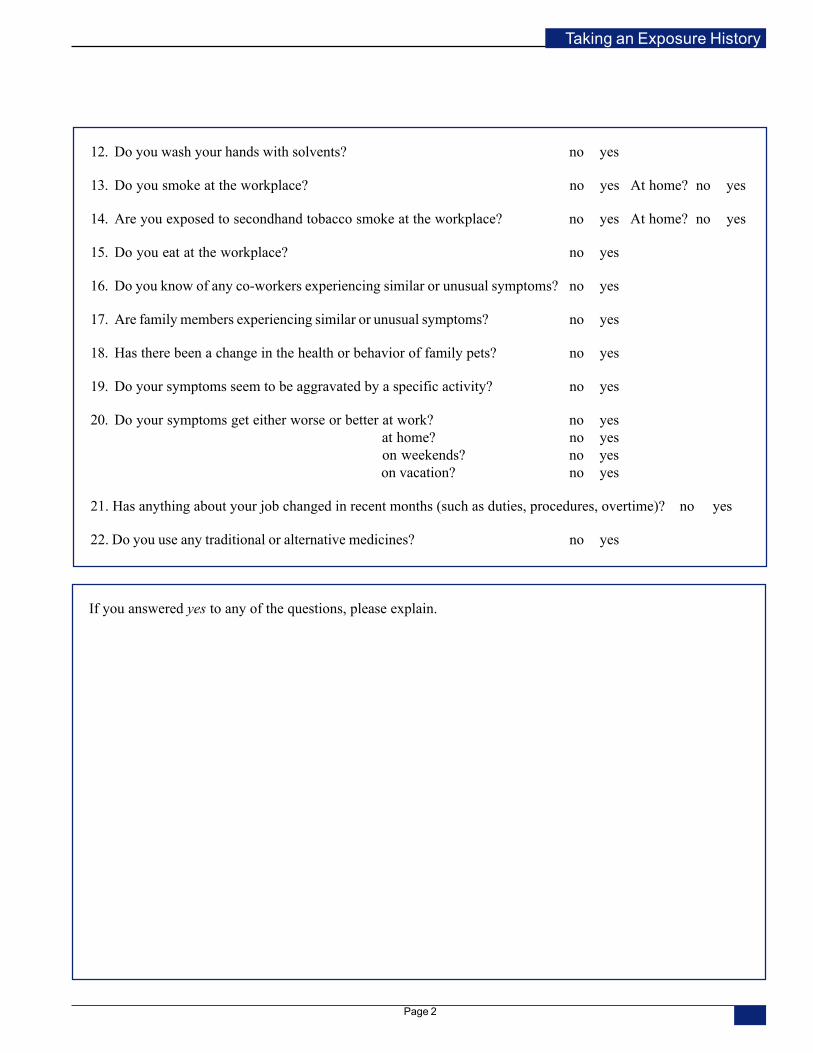
Taking an Exposure History
12. Do you wash your hands with solvents? no yes
13. Do you smoke at the workplace? no yes At home? no yes
14. Are you exposed to secondhand tobacco smoke at the workplace? no yes At home? no yes
15. Do you eat at the workplace? no yes
16. Do you know of any co-workers experiencing similar or unusual symptoms? no yes
17. Are family members experiencing similar or unusual symptoms? no yes
18. Has there been a change in the health or behavior of family pets? no yes
19. Do your symptoms seem to be aggravated by a specific activity? no yes
20. Do your symptoms get either worse or better at work? no yes at home? no yes on weekends? no yes on vacation? no yes
21. Has anything about your job changed in recent months (such as duties, procedures, overtime)? no yes
22. Do you use any traditional or alternative medicines? no yes
If you answered yes to any of the questions, please explain.
Page 2
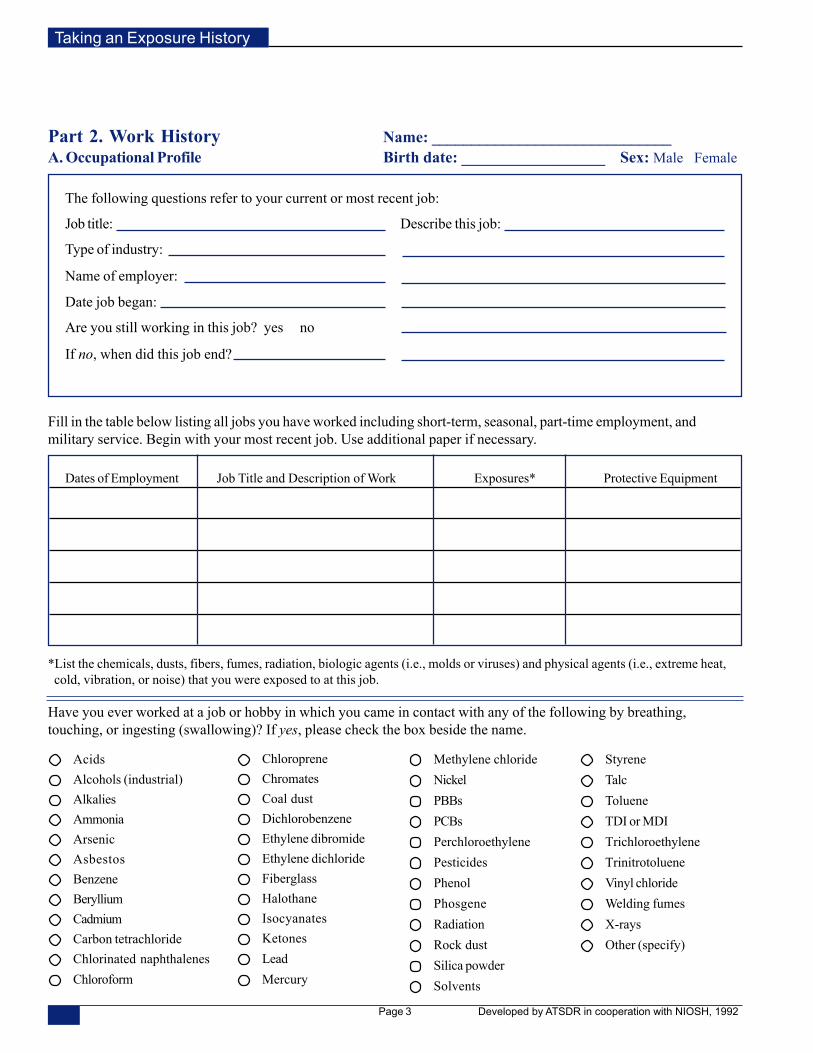
Taking an Exposure History
The following questions refer to your current or most recent job:
Job title: Describe this job:
Type of industry:
Name of employer:
Date job began:
Are you still working in this job? yes no
If no, when did this job end?
Part 2. Work History Name: ______________________________A. Occupational Profile Birth date: __________________ Sex: Male Female
Fill in the table below listing all jobs you have worked including short-term, seasonal, part-time employment, andmilitary service. Begin with your most recent job. Use additional paper if necessary.
*List the chemicals, dusts, fibers, fumes, radiation, biologic agents (i.e., molds or viruses) and physical agents (i.e., extreme heat, cold, vibration, or noise) that you were exposed to at this job.
Have you ever worked at a job or hobby in which you came in contact with any of the following by breathing,touching, or ingesting (swallowing)? If yes, please check the box beside the name.
Developed by ATSDR in cooperation with NIOSH, 1992
Dates of Employment Job Title and Description of Work Exposures* Protective Equipment
AcidsAlcohols (industrial)AlkaliesAmmoniaArsenicAsbestosBenzeneBerylliumCadmiumCarbon tetrachlorideChlorinated naphthalenesChloroform
ChloropreneChromatesCoal dustDichlorobenzeneEthylene dibromideEthylene dichlorideFiberglassHalothaneIsocyanatesKetonesLeadMercury
Methylene chlorideNickelPBBsPCBsPerchloroethylenePesticidesPhenolPhosgeneRadiationRock dustSilica powderSolvents
StyreneTalcTolueneTDI or MDITrichloroethyleneTrinitrotolueneVinyl chlorideWelding fumesX-raysOther (specify)
Page 3
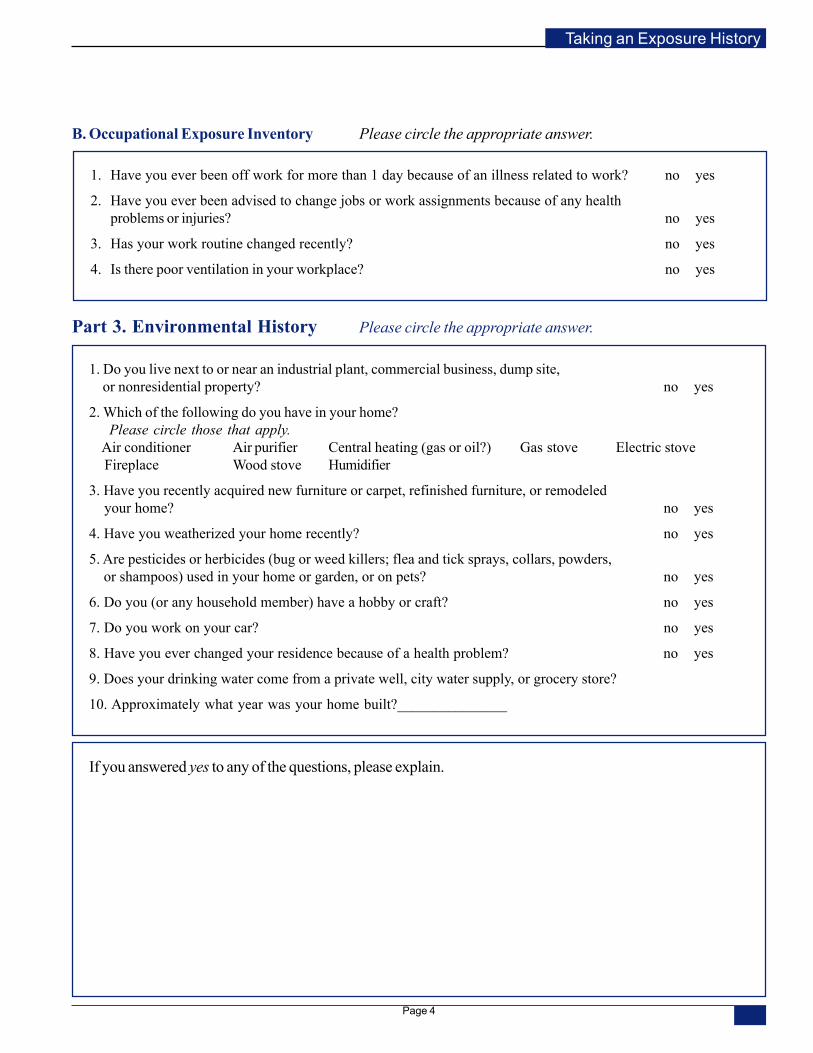
Taking an Exposure History
B. Occupational Exposure Inventory Please circle the appropriate answer.
Part 3. Environmental History Please circle the appropriate answer.
1. Have you ever been off work for more than 1 day because of an illness related to work? no yes
2. Have you ever been advised to change jobs or work assignments because of any healthproblems or injuries? no yes
3. Has your work routine changed recently? no yes
4. Is there poor ventilation in your workplace? no yes
1. Do you live next to or near an industrial plant, commercial business, dump site, or nonresidential property? no yes
2. Which of the following do you have in your home? Please circle those that apply. Air conditioner Air purifier Central heating (gas or oil?) Gas stove Electric stove Fireplace Wood stove Humidifier
3. Have you recently acquired new furniture or carpet, refinished furniture, or remodeled your home? no yes
4. Have you weatherized your home recently? no yes
5. Are pesticides or herbicides (bug or weed killers; flea and tick sprays, collars, powders, or shampoos) used in your home or garden, or on pets? no yes
6. Do you (or any household member) have a hobby or craft? no yes
7. Do you work on your car? no yes
8. Have you ever changed your residence because of a health problem? no yes
9. Does your drinking water come from a private well, city water supply, or grocery store?
10. Approximately what year was your home built?_______________
If you answered yes to any of the questions, please explain.
Page 4
This document was created by the Institute for Functional Medicine. This document may be copied or printed for your own use but cannot be resold or repurposed for commercial use.
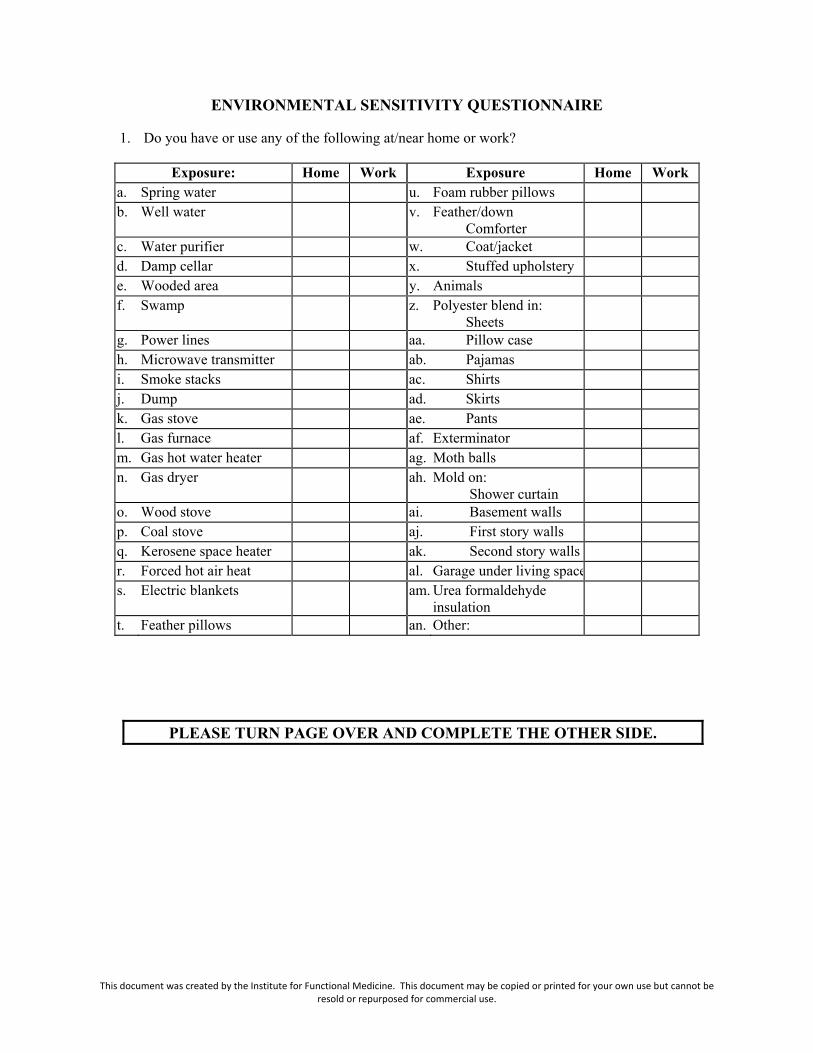
ENVIRONMENTAL SENSITIVITY QUESTIONNAIRE
1. Do you have or use any of the following at/near home or work?
Exposure: Home Work Exposure Home Work a. Spring water u. Foam rubber pillows b. Well water v. Feather/down
Comforter
c. Water purifier w. Coat/jacket d. Damp cellar x. Stuffed upholstery e. Wooded area y. Animals f. Swamp z. Polyester blend in:
Sheets
g. Power lines aa. Pillow case h. Microwave transmitter ab. Pajamas i. Smoke stacks ac. Shirts j. Dump ad. Skirts k. Gas stove ae. Pants l. Gas furnace af. Exterminator m. Gas hot water heater ag. Moth balls n. Gas dryer ah. Mold on:
Shower curtain
o. Wood stove ai. Basement walls p. Coal stove aj. First story walls q. Kerosene space heater ak. Second story walls r. Forced hot air heat al. Garage under living space s. Electric blankets am. Urea formaldehyde
insulation
t. Feather pillows an. Other:
PLEASE TURN PAGE OVER AND COMPLETE THE OTHER SIDE.
This document was created by the Institute for Functional Medicine. This document may be copied or printed for your own use but cannot be resold or repurposed for commercial use.
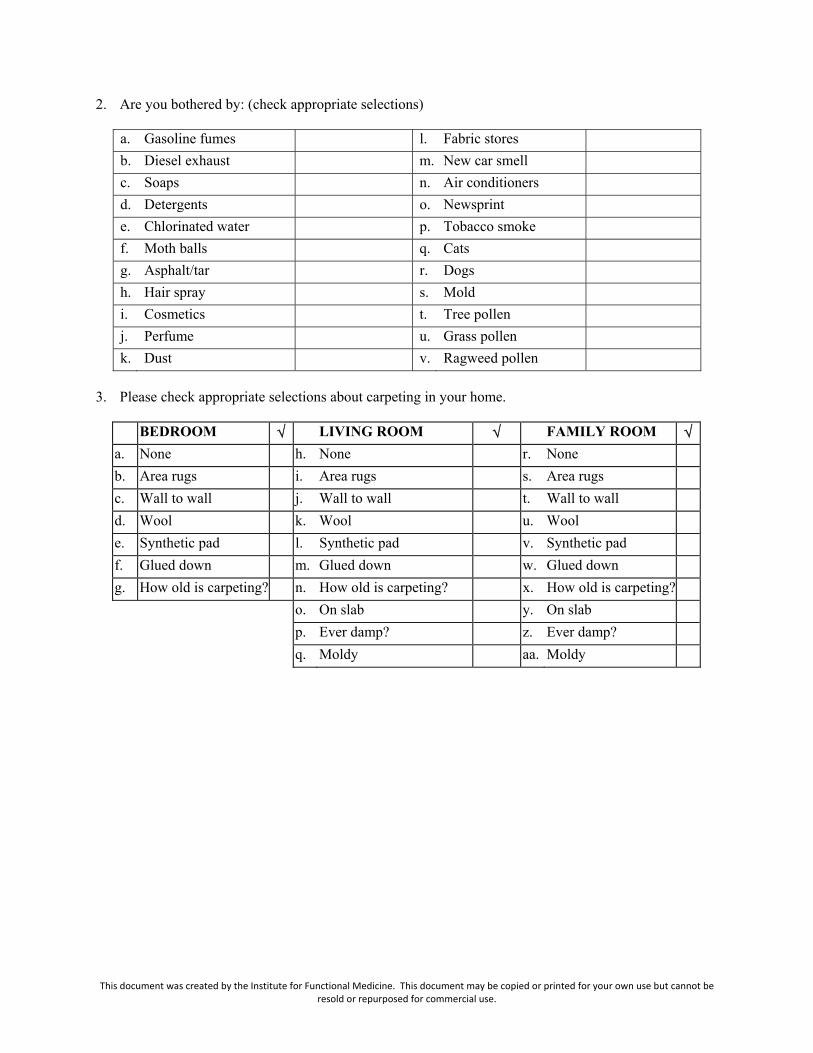
2. Are you bothered by: (check appropriate selections)
a. Gasoline fumes l. Fabric stores b. Diesel exhaust m. New car smell c. Soaps n. Air conditioners d. Detergents o. Newsprint e. Chlorinated water p. Tobacco smoke f. Moth balls q. Cats g. Asphalt/tar r. Dogs h. Hair spray s. Mold i. Cosmetics t. Tree pollen j. Perfume u. Grass pollen k. Dust v. Ragweed pollen
3. Please check appropriate selections about carpeting in your home.
BEDROOM � LIVING ROOM � FAMILY ROOM � a. None h. None r. None b. Area rugs i. Area rugs s. Area rugs c. Wall to wall j. Wall to wall t. Wall to wall d. Wool k. Wool u. Wool e. Synthetic pad l. Synthetic pad v. Synthetic pad f. Glued down m. Glued down w. Glued down g. How old is carpeting? n. How old is carpeting? x. How old is carpeting? o. On slab y. On slab p. Ever damp? z. Ever damp? q. Moldy aa. Moldy
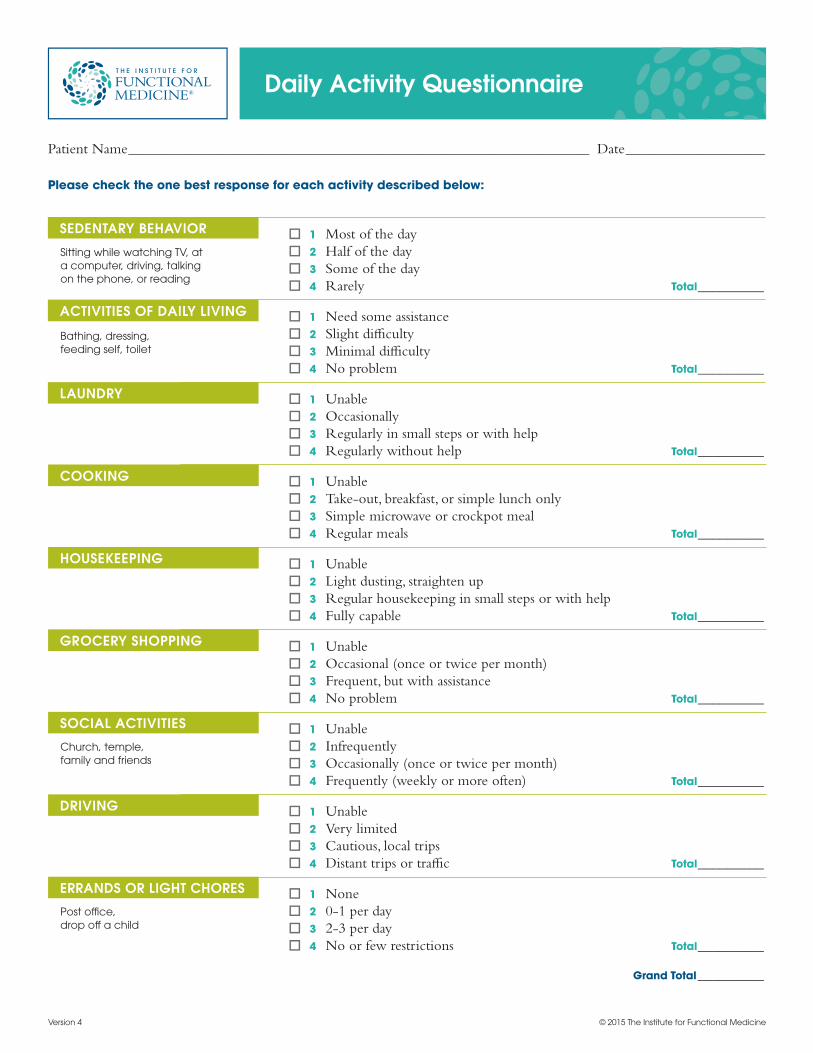
Daily Activity Questionnaire
Patient Name _______________________________________________________________ Date ___________________
Please check the one best response for each activity described below:
o 1 Most of the day o 2 Half of the day o 3 Some of the day o 4 Rarely Total _________
o 1 Need some assistance o 2 Slight difficulty o 3 Minimal difficulty o 4 No problem Total _________
o 1 Unable o 2 Occasionally o 3 Regularly in small steps or with help o 4 Regularly without help Total _________
o 1 Unable o 2 Take-out, breakfast, or simple lunch only o 3 Simple microwave or crockpot meal o 4 Regular meals Total _________
o 1 Unable o 2 Light dusting, straighten up o 3 Regular housekeeping in small steps or with help o 4 Fully capable Total _________
o 1 Unable o 2 Occasional (once or twice per month) o 3 Frequent, but with assistance o 4 No problem Total _________
o 1 Unable o 2 Infrequently o 3 Occasionally (once or twice per month) o 4 Frequently (weekly or more often) Total _________
o 1 Unable o 2 Very limited o 3 Cautious, local trips o 4 Distant trips or traffic Total _________
o 1 None o 2 0-1 per day o 3 2-3 per day o 4 No or few restrictions Total _________
Grand Total _________
ACTIVITIES OF DAILY LIVING
SEDENTARY BEHAVIOR
LAUNDRY
COOKING
HOUSEKEEPING
GROCERY SHOPPING
SOCIAL ACTIVITIES
DRIVING
ERRANDS OR LIGHT CHORES
© 2015 The Institute for Functional MedicineVersion 4
Bathing, dressing, feeding self, toilet
Sitting while watching TV, at a computer, driving, talking on the phone, or reading
Church, temple, family and friends
Post office, drop off a child
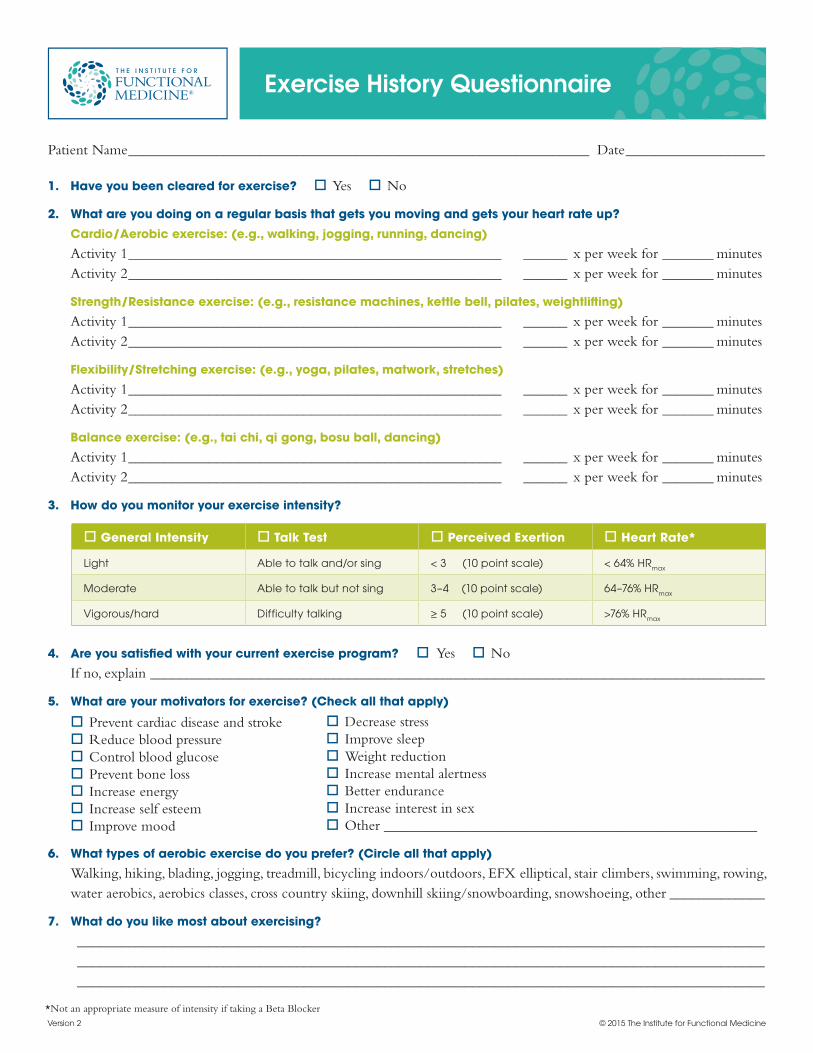
Patient Name _______________________________________________________________ Date ___________________
1. Have you been cleared for exercise? oYes oNo
2. What are you doing on a regular basis that gets you moving and gets your heart rate up? Cardio/Aerobic exercise: (e.g., walking, jogging, running, dancing) Activity 1 ___________________________________________________ ______ x per week for _______ minutes Activity 2 ___________________________________________________ ______ x per week for _______ minutes
Strength/Resistance exercise: (e.g., resistance machines, kettle bell, pilates, weightlifting) Activity 1 ___________________________________________________ ______ x per week for _______ minutes Activity 2 ___________________________________________________ ______ x per week for _______ minutes
Flexibility/Stretching exercise: (e.g., yoga, pilates, matwork, stretches) Activity 1 ___________________________________________________ ______ x per week for _______ minutes Activity 2 ___________________________________________________ ______ x per week for _______ minutes
Balance exercise: (e.g., tai chi, qi gong, bosu ball, dancing) Activity 1 ___________________________________________________ ______ x per week for _______ minutes Activity 2 ___________________________________________________ ______ x per week for _______ minutes
3. How do you monitor your exercise intensity?
Exercise History Questionnaire
© 2015 The Institute for Functional MedicineVersion 2
o General Intensity o Talk Test o Perceived Exertion o Heart Rate*
Light Able to talk and/or sing < 3 (10 point scale) < 64% HRmax
Moderate Able to talk but not sing 3–4 (10 point scale) 64–76% HRmax
Vigorous/hard Difficulty talking ≥ 5 (10 point scale) >76% HRmax
4. Are you satisfied with your current exercise program? oYes oNo If no, explain ____________________________________________________________________________________
5. What are your motivators for exercise? (Check all that apply)
oPrevent cardiac disease and strokeoReduce blood pressureoControl blood glucoseoPrevent bone lossoIncrease energyoIncrease self esteemoImprove mood
*Not an appropriate measure of intensity if taking a Beta Blocker
oDecrease stressoImprove sleepoWeight reductionoIncrease mental alertnessoBetter enduranceoIncrease interest in sexoOther ___________________________________________________
6. What types of aerobic exercise do you prefer? (Circle all that apply)Walking, hiking, blading, jogging, treadmill, bicycling indoors/outdoors, EFX elliptical, stair climbers, swimming, rowing, water aerobics, aerobics classes, cross country skiing, downhill skiing/snowboarding, snowshoeing, other _____________
7. What do you like most about exercising? ______________________________________________________________________________________________ ______________________________________________________________________________________________ ______________________________________________________________________________________________
8. Do you have an exercise partner? oYes oNo9. Do you enjoy group exercise or classes? oYes oNo10. Are you a member of a gym or fitness center? oYes oNo11. Are there any obstacles you have to engaging in movement and physical activity? oYes oNo
a. If yes, what are they? ______________________________________________________________________________________________ ______________________________________________________________________________________________ ______________________________________________________________________________________________
b. If yes, do you have control over the circumstances surrounding your obstacles? How can you overcome them? ______________________________________________________________________________________________ ______________________________________________________________________________________________ ______________________________________________________________________________________________
c. Are any of your obstacles out of your control? If yes, which ones? ______________________________________________________________________________________________ ______________________________________________________________________________________________ ______________________________________________________________________________________________
d. What are some possible solutions around these obstacles? What has worked before? ______________________________________________________________________________________________ ______________________________________________________________________________________________ ______________________________________________________________________________________________
12. What is the best time of day for you to exercise? ______________________________________________________13. When do you have the most energy and time? _______________________________________________________14. Are you ready to take action to make your exercise program work for you and your goals? oYes oNo15. Do you have any goals related to you strength, tone, body composition, or fitness level? oYes oNo
If yes, explain: ___________________________________________________________________________________16. Do you experience any pain or breathing problems while exercising? oYes oNo
If yes, explain: ___________________________________________________________________________________17. Do you have any joint or musculoskeletal problems that might flare up during exercise? oYes oNo
If yes, explain: ___________________________________________________________________________________18. Have you had any injuries while exercising? oYes oNo
If yes, explain: ___________________________________________________________________________________19. Have you experienced a loss of muscle tissue or a decline in strength over the last few years? oYes oNo 20. Have you fallen in the past few months? oYes oNo 21. Do you notice any balance problems? oYes oNo
If yes, explain: ___________________________________________________________________________________22. Do you have any of the following exercise contraindications? (Check all that apply)oAcute systemic infection (i.e., fever, body aches, swollen lymph nodes, etc.)oArrhythmiasoRecent heart attackoSevere congestive heart failureoUncontrolled angina/chest painoOther _______________________________________________________________________________________
EXERCISE HISTORY QUESTIONNAIRE
© 2015 The Institute for Functional Medicine
How Healthy Is Your Diet?
Circle your answers after careful thought, then add up your points (numbers in parentheses).
1. How many fruits do you normally eat each day (1/2 cup fresh or dried fruit, 1 medium piece, 1 cup unsweetened juice)? A. 0 (-2) B. 1 (0) C. 2 to 3 (+2) D. 4 or more (+3) (score) _____
2. How many vegetable servings do you normally eat each day (1 cup leafy greens, 1/2 cup any other veggie, raw or cooked)? A. 0 (-4) B. 1 (0) C. 2 (+1) D. 3 (+2) E. 4 or more (+3) (score) _____
3. How many different varieties of vegetables do you eat in a normal month? A. 2 or less (-4) B. 3 to 4 (0) C. 5 to 6 (+1) D. 7 to 8 (+3) E. 9 or more (+4) (score) _____
4. How many times do you eat dried beans or peas (legumes, lentils, chickpeas, kidney beans, green peas, etc.) in a normal week? A. 0 (-2) B. 1 to 2 (0) C. 3 to 4 (+1) D. 5 to 6 (+2) E. 7 or more (+3) (score) _____
5. How many times do you eat red meat in a normal week? A. 6 or more (-4) B. 4 to 5 (-3) C. 1 to 3 (-1) D. Less than once a week (+2) E. 0 (+3) (score) _____
6. How many times do you eat in a fast food restaurant in a normal week? A. 6 or more (-5) B. 4 to 5 (-4) C. 1 to 3 (-3) D. Less than once a week (-2) E. 0 (0) (score) _____
7. In a typical day, what do you drink most often? A. Soda (regular or diet) (-4) B. Caffeinated coffee or tea (-1) C. Decaffeinated coffee or tea (0) D. Milk or fruit juice (0) E. Herbal tea or water (+3) (score) _____
8. How many 12 oz. cans of soda do you drink in a normal day? A. 6 or more (-5) B. 4 to 5 (-4) C. 2 to 3 (-3) D. 1 (-2) E. Less than 1 (-1) F. 0 (0) (score) _____
9. How often do you eat fish in a typical week? A. Never (-2) B. Once (+1) C. Twice (+2) D. 3 to 5 times (+3) (score) _____
10. In a typical week, how often do you eat whole grains (100% whole grain bread, whole oats, brown rice, quinoa, whole rye crackers)? A. Never (-3) B. 1 to 2 times a week (-1) C. 3 to 4 times a week (0) D. 5 to 6 times a week (+1) E. 1 or more times a day (+3) (score) _____
11. How often do you eat sweets such as cookies, cakes, or ice cream? A. 1 or more times a day (-3) B. Every other day (-2) C. Twice a week (-1) D. Once a week (0) E. 2 to 3 times a month (+1) F. Rarely (+3) (score) _____
Your Total Score__________________
Scoring: 22–28 – Great eating habits 17–21 – Pretty good eating habits 10–16 – Needs some improvement 9 or less – Needs much improvement; try to change one habit at a time
© 2015 The Institute for Functional Medicine
Patient Name _______________________________________________________________ Date ___________________
Sleep is important for musculoskeletal healing and for healthy immune function, mood, cognitive and brain function,
and for many physiological functions.
Please answer the following questions as accurately and fully as possible. For Yes / No questions, please check the correct
answer and provide an explanation if one is requested. The information will help to determine whether you are getting the
sleep you need and to identify possible strategies to help you sleep better.
Sleep Problems:
1 Do you have a sleep problem that has been diagnosed? oYes oNo If yes, what? ___________________________________________________________________________________
2 Do you feel that you have a sleep problem? oYes oNo If yes, how would you describe it? _________________________________________________________________
Sleepiness Questions:
3 Do you feel well rested in the morning? oYes oNo Please explain _________________________________________________________________________________
4 Are there times during the day or evening that you feel sleepy? oYes oNo If yes, what times are these? _______________________________________________________________________
5 What do you do to wake up when you feel sleepy? ____________________________________________________
6 Have you ever had an accident at work, at home or on your job because you were sleepy? oYes oNo If yes, please explain ____________________________________________________________________________
7 Do you take naps? oYes oNo If yes, for how many minutes and at what time of day? _________________________________________________
8 Do you feel well rested after a nap? oYes oNo
Insomnia Questions:
9 Can you usually fall asleep within 20 minutes of lying in bed? oYes oNo
10 How long does it usually take you to fall asleep? ______________________________________________________
11 Do you ever feel so wired at night that it is difficult to fall asleep? oYes oNo
12 Have you had a saliva cortisol test? oYes oNo If yes, what was your night time level? ______________________________________________________________
Sleep Questionnaire
Version 2
© 2015 The Institute for Functional Medicine
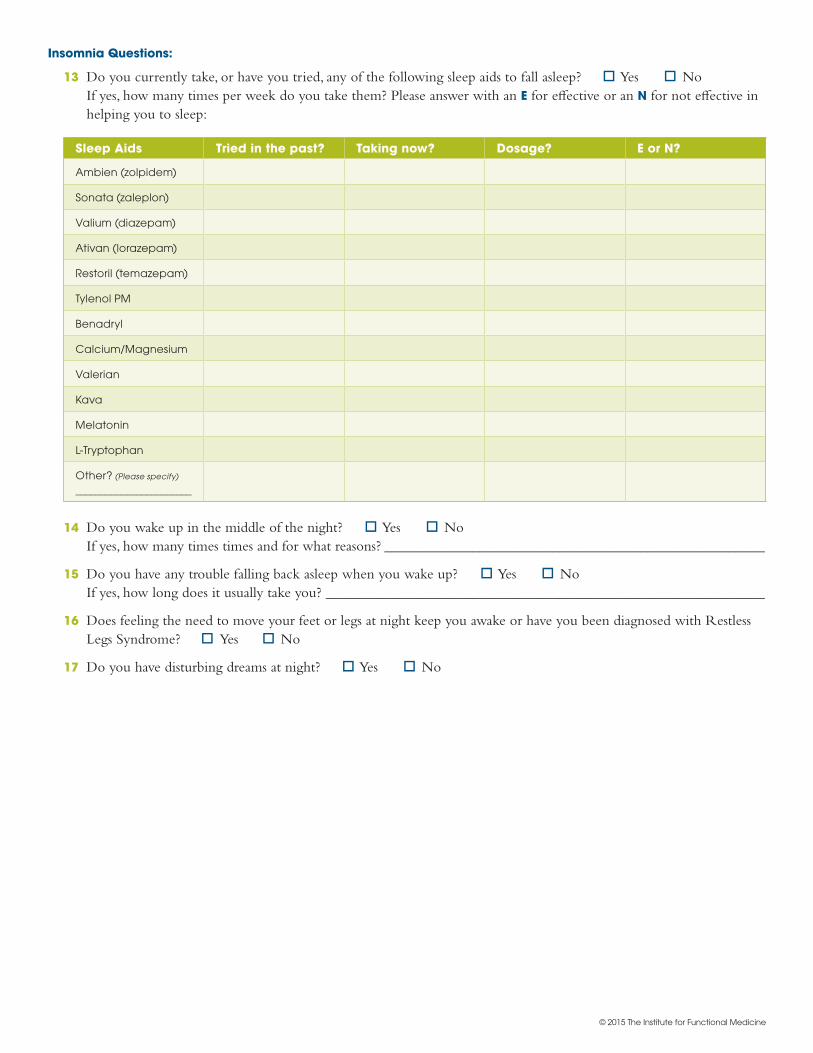
Insomnia Questions:
13 Do you currently take, or have you tried, any of the following sleep aids to fall asleep? oYes oNo If yes, how many times per week do you take them? Please answer with an E for effective or an N for not effective in helping you to sleep:
Sleep Aids Tried in the past? Taking now? Dosage? E or N?
Ambien (zolpidem)
Sonata (zaleplon)
Valium (diazepam)
Ativan (lorazepam)
Restoril (temazepam)
Tylenol PM
Benadryl
Calcium/Magnesium
Valerian
Kava
Melatonin
L-Tryptophan
Other? (Please specify)
_______________________
14 Do you wake up in the middle of the night? oYes oNo If yes, how many times times and for what reasons? ____________________________________________________
15 Do you have any trouble falling back asleep when you wake up? oYes oNo If yes, how long does it usually take you? ____________________________________________________________
16 Does feeling the need to move your feet or legs at night keep you awake or have you been diagnosed with Restless Legs Syndrome? oYes oNo
17 Do you have disturbing dreams at night? oYes oNo
© 2015 The Institute for Functional Medicine
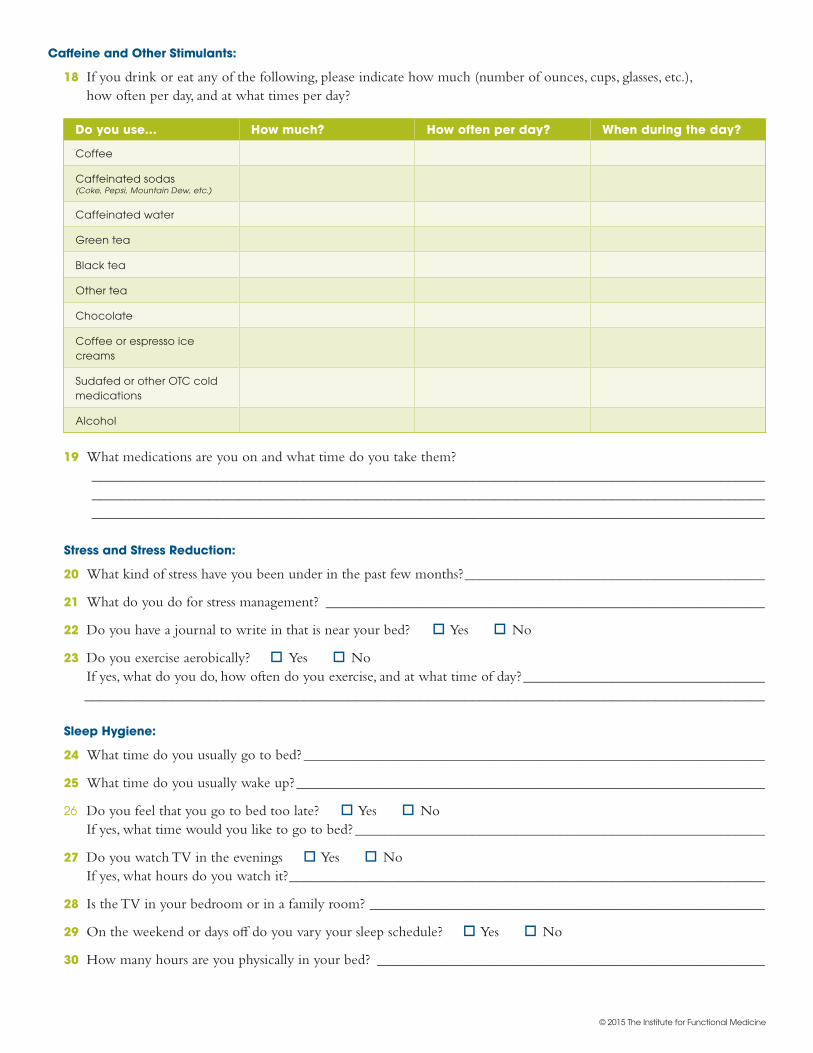
Caffeine and Other Stimulants:
18 If you drink or eat any of the following, please indicate how much (number of ounces, cups, glasses, etc.), how often per day, and at what times per day?
Stress and Stress Reduction:
20 What kind of stress have you been under in the past few months? _________________________________________
21 What do you do for stress management? ____________________________________________________________
22 Do you have a journal to write in that is near your bed? oYes oNo
23 Do you exercise aerobically? oYes oNo If yes, what do you do, how often do you exercise, and at what time of day? _________________________________ _____________________________________________________________________________________________
Sleep Hygiene:
24 What time do you usually go to bed? _______________________________________________________________
25 What time do you usually wake up? ________________________________________________________________
26 Do you feel that you go to bed too late? oYes oNo If yes, what time would you like to go to bed? ________________________________________________________
27 Do you watch TV in the evenings oYes oNo If yes, what hours do you watch it? _________________________________________________________________
28 Is the TV in your bedroom or in a family room? ______________________________________________________
29 On the weekend or days off do you vary your sleep schedule? oYes oNo
30 How many hours are you physically in your bed? _____________________________________________________
Do you use… How much? How often per day? When during the day?
Coffee
Caffeinated sodas (Coke, Pepsi, Mountain Dew, etc.)
Caffeinated water
Green tea
Black tea
Other tea
Chocolate
Coffee or espresso ice creams
Sudafed or other OTC cold medications
Alcohol
19 What medications are you on and what time do you take them? ____________________________________________________________________________________________ ____________________________________________________________________________________________ ____________________________________________________________________________________________
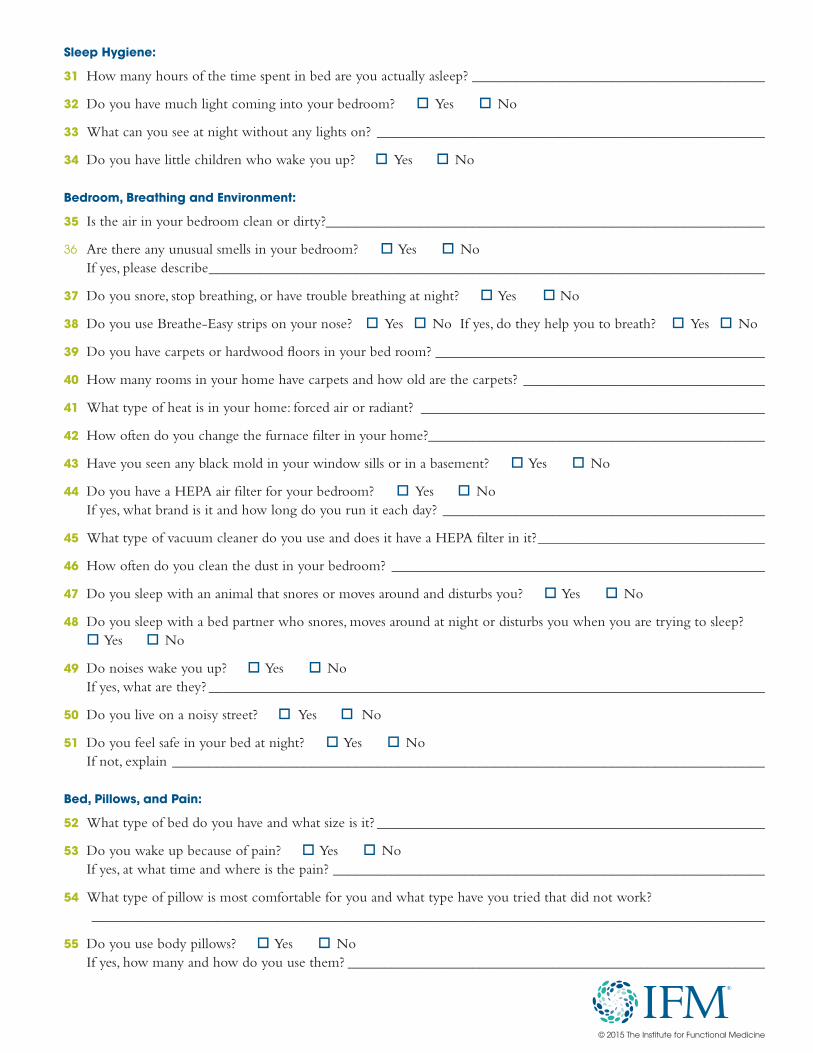
Sleep Hygiene:
31 How many hours of the time spent in bed are you actually asleep? ________________________________________
32 Do you have much light coming into your bedroom? oYes oNo
33 What can you see at night without any lights on? _____________________________________________________
34 Do you have little children who wake you up? oYes oNo
Bedroom, Breathing and Environment:
35 Is the air in your bedroom clean or dirty?____________________________________________________________
36 Are there any unusual smells in your bedroom? oYes oNo If yes, please describe ____________________________________________________________________________
37 Do you snore, stop breathing, or have trouble breathing at night? oYes oNo
38 Do you use Breathe-Easy strips on your nose? oYes oNo If yes, do they help you to breath? oYes oNo
39 Do you have carpets or hardwood floors in your bed room? _____________________________________________
40 How many rooms in your home have carpets and how old are the carpets? _________________________________
41 What type of heat is in your home: forced air or radiant? _______________________________________________
42 How often do you change the furnace filter in your home?______________________________________________
43 Have you seen any black mold in your window sills or in a basement? oYes oNo
44 Do you have a HEPA air filter for your bedroom? oYes oNo If yes, what brand is it and how long do you run it each day? ____________________________________________
45 What type of vacuum cleaner do you use and does it have a HEPA filter in it? _______________________________
46 How often do you clean the dust in your bedroom? ___________________________________________________
47 Do you sleep with an animal that snores or moves around and disturbs you? oYes oNo
48 Do you sleep with a bed partner who snores, moves around at night or disturbs you when you are trying to sleep? oYes oNo
49 Do noises wake you up? oYes oNo If yes, what are they? ____________________________________________________________________________
50 Do you live on a noisy street? oYes oNo
51 Do you feel safe in your bed at night? oYes oNo If not, explain _________________________________________________________________________________
Bed, Pillows, and Pain:
52 What type of bed do you have and what size is it? _____________________________________________________
53 Do you wake up because of pain? oYes oNo If yes, at what time and where is the pain? ___________________________________________________________
54 What type of pillow is most comfortable for you and what type have you tried that did not work? ____________________________________________________________________________________________
55 Do you use body pillows? oYes oNo If yes, how many and how do you use them? _________________________________________________________
© 2015 The Institute for Functional Medicine
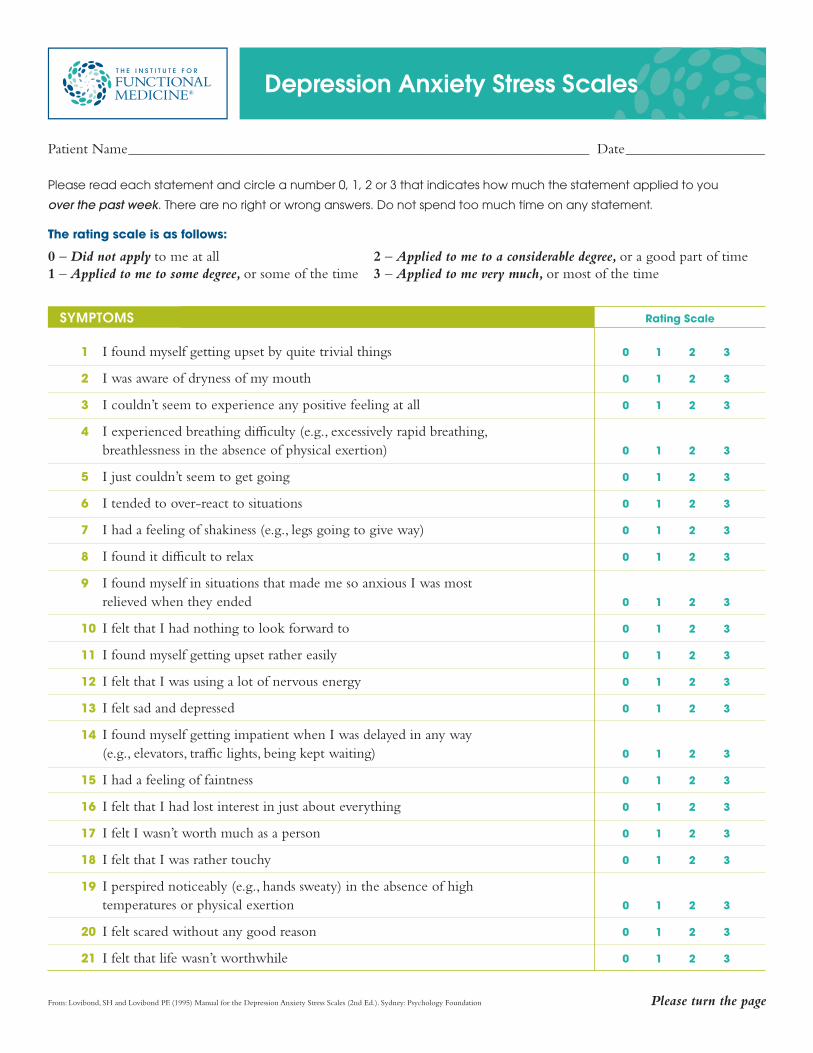
Depression Anxiety Stress Scales
SYMPTOMS
1 I found myself getting upset by quite trivial things 0 1 2 3
2 I was aware of dryness of my mouth 0 1 2 3
3 I couldn’t seem to experience any positive feeling at all 0 1 2 3
4 I experienced breathing difficulty (e.g., excessively rapid breathing, breathlessness in the absence of physical exertion) 0 1 2 3
5 I just couldn’t seem to get going 0 1 2 3
6 I tended to over-react to situations 0 1 2 3
7 I had a feeling of shakiness (e.g., legs going to give way) 0 1 2 3
8 I found it difficult to relax 0 1 2 3
9 I found myself in situations that made me so anxious I was most relieved when they ended 0 1 2 3
10 I felt that I had nothing to look forward to 0 1 2 3
11 I found myself getting upset rather easily 0 1 2 3
12 I felt that I was using a lot of nervous energy 0 1 2 3
13 I felt sad and depressed 0 1 2 3
14 I found myself getting impatient when I was delayed in any way (e.g., elevators, traffic lights, being kept waiting) 0 1 2 3
15 I had a feeling of faintness 0 1 2 3
16 I felt that I had lost interest in just about everything 0 1 2 3
17 I felt I wasn’t worth much as a person 0 1 2 3
18 I felt that I was rather touchy 0 1 2 3
19 I perspired noticeably (e.g., hands sweaty) in the absence of high temperatures or physical exertion 0 1 2 3
20 I felt scared without any good reason 0 1 2 3
21 I felt that life wasn’t worthwhile 0 1 2 3
Rating Scale
From: Lovibond, SH and Lovibond PF. (1995) Manual for the Depression Anxiety Stress Scales (2nd Ed.). Sydney: Psychology Foundation
Patient Name _______________________________________________________________ Date ___________________
Please read each statement and circle a number 0, 1, 2 or 3 that indicates how much the statement applied to you
over the past week. There are no right or wrong answers. Do not spend too much time on any statement.
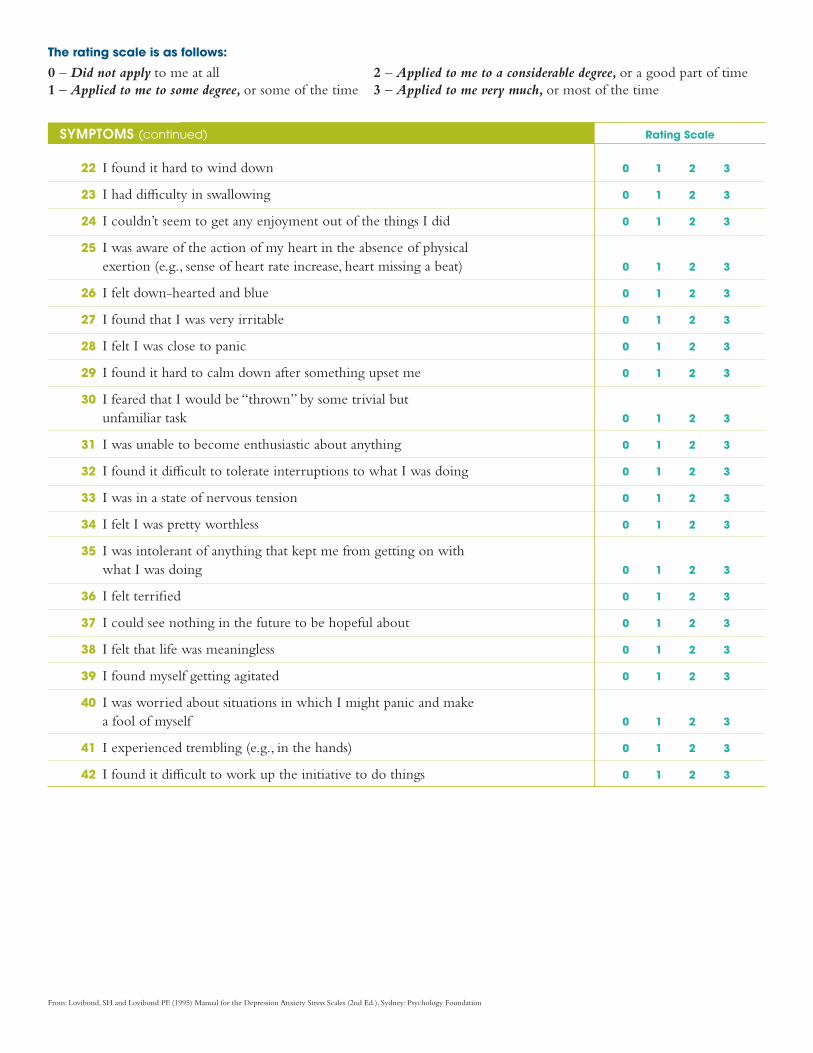
The rating scale is as follows:
0 – Did not apply to me at all1 – Applied to me to some degree, or some of the time
2 – Applied to me to a considerable degree, or a good part of time3 – Applied to me very much, or most of the time
Please turn the page
From: Lovibond, SH and Lovibond PF. (1995) Manual for the Depression Anxiety Stress Scales (2nd Ed.). Sydney: Psychology Foundation
SYMPTOMS (continued)
22 I found it hard to wind down 0 1 2 3
23 I had difficulty in swallowing 0 1 2 3
24 I couldn’t seem to get any enjoyment out of the things I did 0 1 2 3
25 I was aware of the action of my heart in the absence of physical exertion (e.g., sense of heart rate increase, heart missing a beat) 0 1 2 3
26 I felt down-hearted and blue 0 1 2 3
27 I found that I was very irritable 0 1 2 3
28 I felt I was close to panic 0 1 2 3
29 I found it hard to calm down after something upset me 0 1 2 3
30 I feared that I would be “thrown” by some trivial but unfamiliar task 0 1 2 3
31 I was unable to become enthusiastic about anything 0 1 2 3
32 I found it difficult to tolerate interruptions to what I was doing 0 1 2 3
33 I was in a state of nervous tension 0 1 2 3
34 I felt I was pretty worthless 0 1 2 3
35 I was intolerant of anything that kept me from getting on with what I was doing 0 1 2 3
36 I felt terrified 0 1 2 3
37 I could see nothing in the future to be hopeful about 0 1 2 3
38 I felt that life was meaningless 0 1 2 3
39 I found myself getting agitated 0 1 2 3
40 I was worried about situations in which I might panic and make a fool of myself 0 1 2 3
41 I experienced trembling (e.g., in the hands) 0 1 2 3
42 I found it difficult to work up the initiative to do things 0 1 2 3
Rating Scale
The rating scale is as follows:
0 – Did not apply to me at all1 – Applied to me to some degree, or some of the time
2 – Applied to me to a considerable degree, or a good part of time3 – Applied to me very much, or most of the time
General Office Policies Please review carefully. Sign and date.
• Patient Responsibility: You are encouraged to ask questions on any health-related topic and to take an active role in your health-care.
• Confidentiality: Information revealed during office visits is confidential. Your record and the information contained within it will not be disclosed to others unless you direct us to do so in writing. Exceptions to this confidentiality include disclosure of the intent to harm yourself or others and subpoena from specific government agencies (as outlined in the HIPAA Privacy Rule).
• Treatment Plan: Each treatment plan and/or procedure possesses both risks and benefits. You are encouraged to ask questions if you would like additional information. Although your plan will be thoroughly researched and customized to your individual personal goals and health status, no guarantees can be assured regarding the outcomes of treatment plan(s) or procedure(s).
• Office Visits: Effective April 1st, 2018: office visits are billed at $250.00 per hour. The first office visit is $500.00 and is typically 2 hours long. This length may vary. If a longer visit is necessary, you will notified of this prior to your appointment. Subsequent follow-up visits are a minimum of 30 minutes. There is no refund for services provided. You may be eligible for out-of-network insurance reimbursement or tax deduction for medical services.
• Insurance: We do not accept any insurance. All fees are settled directly between patient and provider. At the patient’s request, we will provide you with the necessary forms and diagnostic codes needed for you to submit an out-of-network claim to your insurance. Please note that we are are not Medicare providers and are opted out of the Medicare program. Our services can not be submitted to Medicare for reimbursement.
• Payment: We accept cash, money orders and most major credit cards. Checks are not accepted.
• Cancellation policy: When an appointment is scheduled, time is reserved especially for you and no one else. Since our appointments are much longer than standard office visits, cancellations are significant interruptions to the Clinic. Thus, a minimum of 3 days’ notice is required for cancellations of new patient visits and 1 day notice for existing patients. There will be a 100% office visit charge for “no-shows” or late cancellations.

• Specialty Laboratory Testing: Our clinic frequently uses specialty testing. These are usually an out-of-pocket expense. Occasionally, there is some insurance coverage. We will guide you through identifying the costs associated with your testing.
• Treatment Plan Questions: We encourage patients to call or e-mail with questions regarding their treatment plan. If there is a need for longer discussion regarding new symptoms or new concerns, then we recommend you schedule an additional follow-up appointment. Questions that require longer than 5-minute responses fit this scenario. Additionally, if it has been longer than 8 weeks since your last appointment, schedule an appointment rather than email.
• Emergencies and after-hours care: The Clinic is not a primary care clinic - we offer consultative services only. You must have a primary care doctor with whom you can consult in the event of an emergency or urgent problem. If you notice an adverse effect from one of the components of your Clinic treatment plan, you should discontinue it then email or call the Clinic during normal business hours. If you have a serious health problem that requires immediate attention, you should call your other doctors(s), call 911, or have someone take you to the nearest hospital emergency room.
• Please email us at [email protected] for any questions regarding this policy.
I agree to all terms and conditions of these General Office Policies.
Signature: Date: ____________________________________________________________________
I agree to allow Armen E. Nikogosian, MD to use or to describe my anonymous medical history and laboratory data for educational purposes in lectures, blogs, case reports, and other publications that are communicated to other professionals, but may include members of the public. This medical history and laboratory data might include photographs and/or other images of parts of my body other than my face (nutrition/physical exam findings only). Armen E. Nikogosian, MD will never publish any information that uses my name or that identifies me as the source of any of the information, data, or images that it publishes. If you do not wish to participate, initial here:______





























