Embed Size (px)
Citation preview
2012THE COMMISSION FOR A
SOCIALLY SUSTAINABLE MALMÖInterim Report
06-03-2012

Preface
This Report is submitted to Malmö Municipal Executive Committee and aims to describe the way in which the Commission for a Socially Sustainable Malmö has interpreted its mission. The Final Report shall be submitted in December 2012. The following is a report of what has been accomplished so far and the progress of the work.
The Interim Report is based on the directive allocated to the Commission by the Municipal Executive Committee (KS 09/11/2010) and the project plan agreed for the mission (KS 01/03/2011).
According to the directive, the Commission shall produce a scientifically founded basis for strategies of reducing the health inequalities in Malmö. The key parts of this work are, firstly, to demonstrate that there is scientific evidence in support of the idea that social factors play a significant role in the development of public health. Secondly, that there are inequalities with regard to health in Malmö, which are dependent on social factors. Thirdly, the Final Report shall present strategies for what implementations should be possible to carry out in Malmö in the future, in order to reduce health inequalities.
As we are still in the midst of the working process, we will not be able to present any conclusions in this Interim Report. The concluding Summary highlights a number of areas that are of importance for the Municipal Executive Committee to consider already at this stage.
The work around the Commission has attracted a great level of engagement, not least from senior advisers, researchers and officials contributing with expertise and data as well as from other parties in Malmö, including organizations and cultural associations. This is evidence of a great desire to affect Malmö's development. We would like to thank everyone who has contributed, and is contributing, with data and who is participating in discussions, seminars etc. Not until the final report will we report the names of everybody who contributed in different ways.
The interim report was written by the undersigned as well as the Commission's Head Secretary, Anna Balkfors. All commissioners shall be included as co-authors of the final report.
The Commission's final report shall be seen as an introduction to a long-term process, the purpose of which is to consciously, and with the best imaginable knowledge base, reduce health inequalities in Malmö. A holistic view is required, encompassing economic, ecological and social sustainability.
Sven-Olof IsacssonProfessor Emeritus of Social Medicine, Lund University, Skåne
University Hospital, Malmö. Chairman of the Commission for a Socially Sustainable Malmö.
Summary
The Municipal Executive Committee in Malmö decided in 2010 to establish the Commission for a Socially Sustainable Malmö. The inspiration came from the extensive research that has been compiled by WHO under the management of Professor Michael Marmot in 2008. It demonstrated that the inequalities in health have increased in recent years. Not just in the poorer areas of the world, but also in welfare states, including Sweden. It was clearly evident that the causes of this development were of a social nature. Many countries initiated an analysis of this relationship within their own borders. Decisions about long-term measures have since been made; in Norway and Denmark among other countries.
These types of decisions have been delayed in Sweden despite an analysis by the Swedish National Institution of Public Health. Despite this delay, it was realized that something must be done in Malmö because of the increasing segregation and indications that health disparities were increasing. The decision to create a politically independent commission was made in May 2010. Malmö thereby became the first municipality in the country to appoint a local commission similar in nature to the ones appointed by WHO, which later resulted in national commissions in both England and Denmark, among other countries.
The term “inequality in health” is connected with differences which are remediable. The Swedish National Institution of Public Health applies the following definition of equality in health: “Equity in health is the absence of potentially remediable, systematic differences in one or more aspects of health across socially, economically, demographically, or geographically defined population groups or subgroups.1”
The directive from the Municipal Executive Committee specifies that the Commission shall produce scientific data as a base for how the socially-caused inequalities in health could possibly be reduced. Thorough work has been done to recruit commissioners who fulfil the requirements;
this is a prerequisite for being able to complete the task.
Three conditions are required in order to be able to produce a report that shall be perceived as well-founded and reliable by local politicians, decision-makers and the public.
Firstly, to demonstrate that there is scientific support for the significance of social factors for the global development of health.
Secondly, that inequalities in health caused by social factors also exist in Malmö.
3
Thirdly, that the final report shall propose strategies for implementations which ought to be practically possible to carry out in Malmö in the future, in order to reduce health inequalities.
With regard to the first condition, the evidence in the international literature is convincing. An account of the causal relationship will be given in this interim report.
With regard to the second condition, many researchers active in Malmö and Lund have produced, on behalf of the Commission, current and necessary knowledge about the health of Malmö's residents, connected to social determinants during the entire life span. This work is nearing completion.
The third condition builds upon defining how social determinants which contribute to creating inequalities in health are distributed among Malmö's population. Belonging to these factors are childhood conditions with respect to maternity care, child health care, pre-school, school, recreation, housing, economy etc. During the spring of 2012, the commissioners and other experts will complete the scientific
data within different areas and analyses of local conditions for strategies.
There are several motives for affecting the social determinants which are significant for health.
Ethical motives Social inequalities in health are a matter of life and death. If it is possible to affect the conditions for the population's health, the question is not whether society should be able to assist, but how.
Socioeconomic motives The inequalities in health cost the community large amounts of money, not least in lost production, and inhibit long-term, sustainable economic growth.
Sustainability motive Health is an extremely important precondition for creating a sustainable community. The development in health mirrors the development in society. Reduced social differences do not only promote the social aspect of sustainability with greater trust between people and in the community institutions, but also better conditions for ecological and economic sustainability.
The issues which the Commission has to process, encompass complex societal matters such as sustainability, segregation, homelessness, inequality, childhood conditions
1 Bremberg, Jämlikhet i hälsa: perspektiv, begrepp och mått, 2003
4
and the labour market. The challenge is to deepen analysis of the underlying causes and simultaneously try to be as concrete as possible.
On the whole, the work is going according to the project plan, with a certain amount of rescheduling. The reason for this is that it took time from the establishment of the directive (November 2010) to the finalization of the budget (March 2011) and the appointment of the commissioners. The allocated time and resources are limited in relation to the complexity and scope of the assignment.
Malmö's goal is to create a sustainable city in the long term: economically, ecologically and socially. The three parts are intimately related. Far-sightedness in planning and budgeting is required in order to succeed. An important ingredient in this work ought to be a good knowledge base incorporated into sensible decisions at all levels. We are hoping that the Commission's final report can contribute to making Malmö a sustainable, attractive and good city to live in for everybody.
Contents
Preface
Summary
1. Background – from political decision to Commission 6
1.1 From directive to Commission - working methods 7
1.2 Inequalities in health nothing new 10
1.3 Why reduce inequalities in health? 11
2. Social determinants of health – what relationships exist? 13
2.1 Social causes of health inequalities in Malmö 14
3. The health of Malmö's residents 15
3.1 Basic data about the health of Malmö’s residents 15
3.2 From pregnancy until the autumn of life 15
4. Knowledge base – discussion material 19
4.1 Childhood conditions – giving children a good start in life 19
4.2 Work and working environment 22
4.3 Reasonable living standard – income and health 23
4.4 Creating sustainable and healthy communities 24
4.5 Measuring inequality in health – measuring community development 26
4.6 What can we learn from history – Malmö and its surroundings 27
4.7 Implementation – organization and governance 28
5. The Commission's continuing work 30
References 33
Appendices
Appendix 1. Presentation of the commissioners, senior advisers and secretariat
Appendix 2. List of supporting reports/scientific research produced for the Commission
Appendix 3. The Commission's activities 2011

The Commission
6
1. Background– from political decision to Commission
On 5 May 2010 (ref. no. 363/10), the Municipal Executive Committee decided to appoint a politically independent Commission for a Socially Sustainable Malmö, with the task of deepening the analysis of the larger structural inequalities in health, which prevail in the city. Furthermore, the Municipal Executive Committee decided on a directive for the Commission on 09-11-2010, and to appoint Sven-Olof Isacsson, Professor Emeritus of Social Medicine at the Faculty of Medicine at Lund University as chairman. In connection with the directive being adopted, the Municipal Executive Committee commissioned the City Office to produce a project plan and budget for the Commission's work. The project plan and budget were decided by the Municipal Executive Committee on 01-03-2011.
The Commission's objective and work has gained attention elsewhere than in Malmö, and there may be reasons for repeating the motives here for the appointment of the Commission.
The Municipality's ambition is to work for a sustainable city from all aspects. There are presently great differences in the social and economic conditions for health among Malmö's residents, which affect the conditions for sustainable development. It is well-known that, for decades, the geographical differences in life expectancy have been large within the city. The differences in life expectancy are a result of differences in mortality for a large number of illnesses, which is in turn a result of differences in the factors which contribute to the incidence of the illnesses, e.g., smoking, alcohol abuse, excessive weight, poor dietary habits, lack of exercise, high blood pressure and a greater risk of incurring an accident.
It is perhaps not often considered that it is ultimately social factors (determinants) that contribute to these differences. Researchers usually speak of causes of the causes, where social factors explain the differences in many of the above-mentioned risks for being struck by illness and premature death. The differences in health geographically or between those who are socially prosperous and those who are not so well-off in Malmö have not decreased in recent years, but rather have increased. This is unethical and unacceptable given the presumption that this would be possible to prevent. The fact that it is possible to prevent a continued increase in health inequalities constitutes the basis of the Commission's work. The Commission's proposals shall be based on scientific data and realistic assessments of what is remediable and effective.
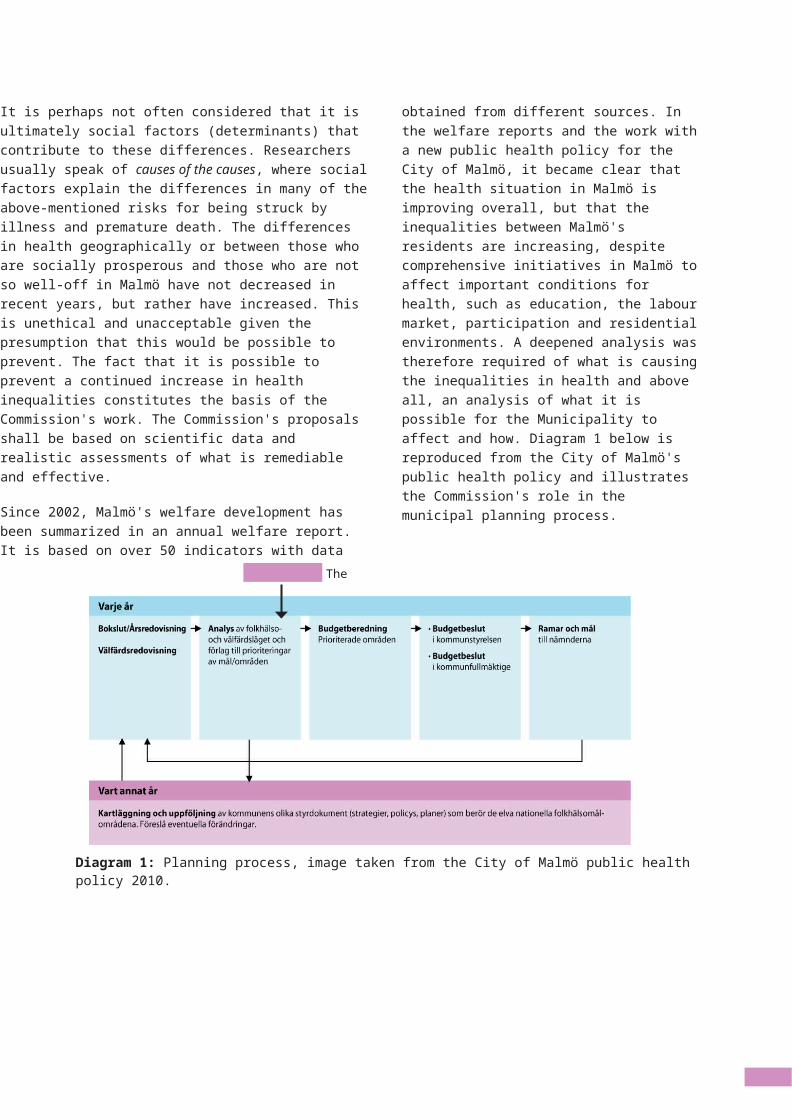
Since 2002, Malmö's welfare development has been summarized in an annual welfare report. It is based on over 50 indicators with data obtained from different sources. In the welfare reports and the work with a new public health policy for the City of Malmö, it became clear that the health situation in Malmö is improving overall, but that the inequalities between Malmö's residents are increasing, despite comprehensive initiatives in Malmö to affect important conditions for health, such as education, the labour market, participation and residential environments. A deepened analysis was therefore required of what is causing the inequalities in health and above all, an analysis of what it is possible for the Municipality to affect and how. Diagram 1 below is reproduced from the City of Malmö's public health policy and illustrates the Commission's role in the municipal planning process.
7
Diagram 1: Planning process, image taken from the City of Malmö public health policy 2010.
8
At the same time as the City of Malmö's public health policy was being produced in 2008, the World Health Organization (WHO) published the report Closing the gap in a generation. The Commission on Social Determinants of Health was responsible for the report, with Sir Michael Marmot as its chairman (which is why this commission is sometimes called the Marmot Commission). The report establishes that the global skewedness of health is ethically indefensible and that it depends essentially upon social determinants.
There are no necessary, biological reasons for the health-related inequalities in the world, countries and cities being so great. The Marmot Commission focuses primarily on the global health situation, but also describes the inequalities in health which exist within countries and cities. The differences and uneven distribution of health are not a natural phenomenon, but should instead be considered as a structural problem which can be changed and affected through political decisions. Comprehensive work for change is required to reduce the gap between those who have good social conditions for health and those that do not, involving new perspectives and working methods. The Marmot Commission presents over sixty proposals for measures and strategies for reducing the global inequality in health.
Work is now being performed around the word to implement the Marmot Review's conclusions. One example is a national analysis for the implementation of strategies for England - Fair Society, Healthy lives - a Strategic Review of Health Inequalities in England post-2010. Denmark produced a similar analysis in 2011, Ulighed I Sundhed - årsager og indsatser (Inequality in Health - Causes and Initiatives). There was discussion in Sweden about appointing a national parliamentary commission. Instead of a national commission, the Government assigned the Swedish National Institute of Public Health the task of drawing lessons from the Marmot Commission's work.
Backed with scientific support, with the knowledge that health inequalities in Malmö are increasing and with the ambition of working towards a sustainable city from all perspectives, the Municipal Executive Committee chose to appoint a local commission.
1.1. FROM DIRECTIVE TO COMMISSION - WORKING METHODSThe Commission was formed during the first part of 2011. In accordance with the directive, the Commission is comprised of a chairman, Sven-Olof Isacsson; a head secretary, Anna Balkfors as well as the required number of commissioners. The City Office shall be responsible for coordinating the work and assigning the requisite support from public officials.
9
The CommissionTo begin with, a thorough work was performed to recruit commissioners who could meet the expectations of the assignment. The primary task is to, on the basis of Malmö's challenges regarding social differences, injustices and inequalities, analyse the causes and relationships, and identify aspects possible to affect by whom and how? It is a matter of identifying the problem, challenges and analysis, and understanding what aspects are possible to affect and what is feasibly implementable. The Commission therefore contains both researchers and practitioners. However, not all areas are represented and, therefore, other experts are contributing to the Commission's work, including a number of senior advisers.
SecretariatIn order to meet expectations regarding transparency and dialogue as well as support for the Commission's internal communication, a communications officer was also recruited. The secretariat was supplemented with two persons in spring 2012. A presentation of commissioners, senior advisers and the secretariat is given in appendix 1.
ClientThe Public Health Council comprises the Municipal Executive Committee's preparatory organ for public health issues and has the task of preparing the proposals and strategies drafted by the Commission. The Commission's chairman has updated the Council on the Commission's ongoing work at every Public Health Council meeting. According to the Directive, the Public Health Council's chairman acts as an adjunct to the Commission in order to ensure
feedback to the Public Health Council and follows the Commission's work continuously. The members will be invited to contribute to the seminars/hearings that are planned for spring 2012.
BudgetThe Commission's budget of SEK 3 million has included the costs of remuneration to commissioners, the chairman, communications officer and certain clients, as well as for administration, seminars and meetings.
The work processA broad monitoring of global initiatives of this type was performed as part of the task of producing a project plan and forming the Commission. One of these involved establishing contact with the Marmot Commission.
Research overviews were processed and talks conducted with over seventy persons inside and outside the City of Malmö. Researchers, trade and industry actors, youths, persons from interested associations and City of Malmö personnel provided the data for the design of the work.
10
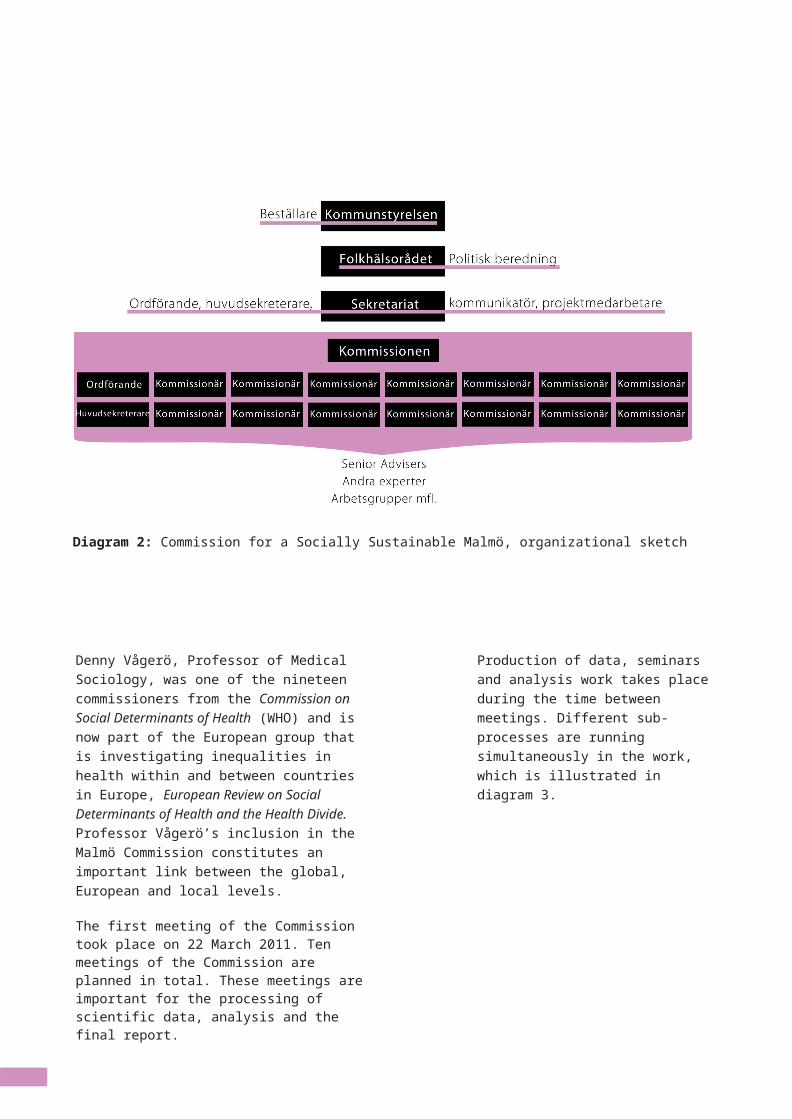
Diagram 2: Commission for a Socially Sustainable Malmö, organizational sketch
Denny Vågerö, Professor of Medical Sociology, was one of the nineteen commissioners from the Commission on Social Determinants of Health (WHO) and is now part of the European group that is investigating inequalities in health within and between countries in Europe, European Review on Social Determinants of Health and the Health Divide. Professor Vågerö’s inclusion in the Malmö Commission constitutes an important link between the global, European and local levels.
The first meeting of the Commission took place on 22 March 2011. Ten meetings of the Commission are planned in total. These meetings are important for the processing of scientific data, analysis and the final report.
Production of data, seminars and analysis work takes place during the time between meetings. Different sub-processes are running simultaneously in the work, which is illustrated in diagram 3.
The issues which the Commission has to process encompass complex societal matters such as sustainability, segregation, homelessness, inequality, childhood conditions and the labour market. The challenge is to deepen the analysis of the underlying causes and simultaneously try to be as concrete as possible.
On the whole, the work is going according to the project plan, with a certain amount of rescheduling. The reason for this is that it took time from the establishment of the directive (November 2010) to the finalization of the budget (March 2011) and the appointment of the commissioners. The allocated time and resources are limited in relation to the complexity and scope of the assignment.
11
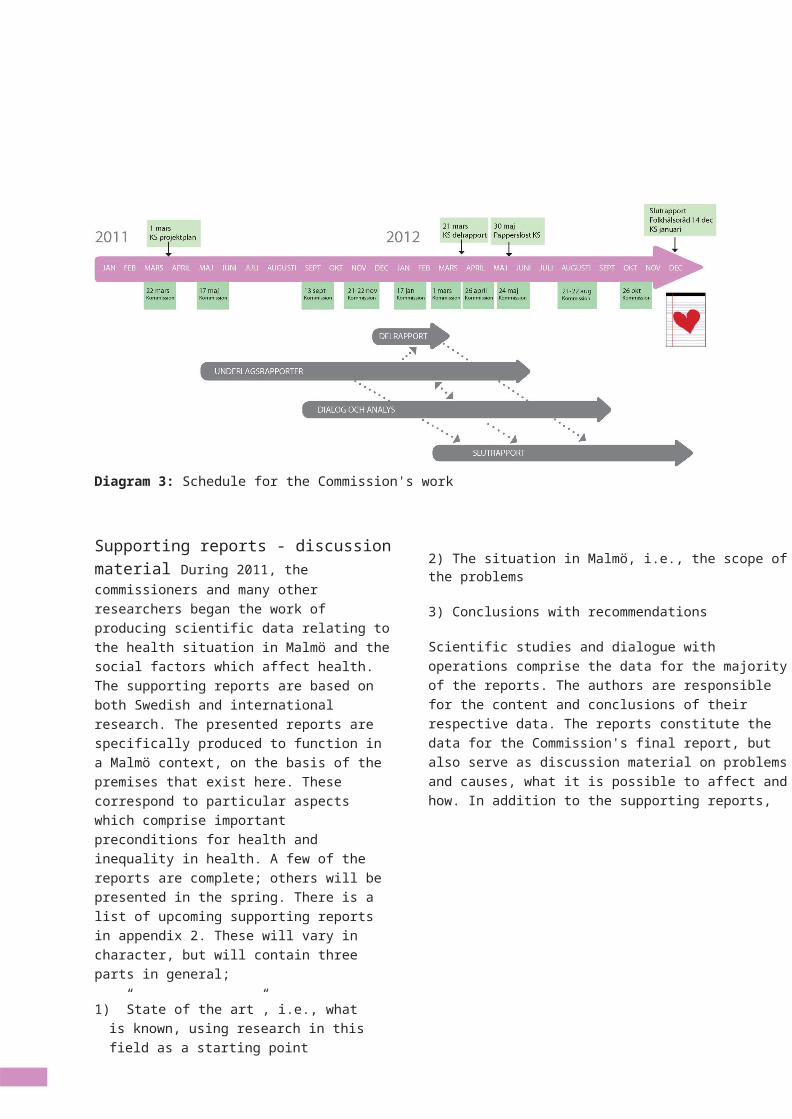
Diagram 3: Schedule for the Commission's work
Supporting reports - discussion material During 2011, the commissioners and many other researchers began the work of producing scientific data relating to the health situation in Malmö and the social factors which affect health. The supporting reports are based on both Swedish and international research. The presented reports are specifically produced to function in a Malmö context, on the basis of the premises that exist here. These correspond to particular aspects which comprise important preconditions for health and inequality in health. A few of the reports are complete; others will be presented in the spring. There is a list of upcoming supporting reports in appendix 2. These will vary in character, but will contain three parts in general;
1) ”State of the art”, i.e., what is known, using research in this field as a starting point
2) The situation in Malmö, i.e., the scope of the problems
3) Conclusions with recommendations
Scientific studies and dialogue with operations comprise the data for the majority of the reports. The authors are
responsible for the content and conclusions of their respective data. The reports constitute the data for the Commission's final report, but also serve as discussion material on problems and causes, what it is possible to affect and how. In addition to the supporting reports,
12
there are many other research overviews which will form the foundations for the work. It is only in the Commission's final report that the Commission's strategies, based on a holistic approach, are presented.
Working methods involvedIn the Directive for the Commission, there are not only expectations about what the Commission shall deliver, but also expectations on how the Commission shall work. It is an independent commission, whose work shall be transparent. The Commission shall actively invite organizations and Malmö's residents to share their experiences in order to contribute to the analysis and design of strategies. It is crucial that the Commission's work is made accessible, and that information is communicated both internally and externally (from the Directive).
Involvement and dialogue take place in different ways. Several commissioners collaborate with City of Malmö personnel and other operations on the development of knowledge base research. Many of the commissioners, in addition to contributing in this context within the City of Malmö, have also participated regionally, nationally and internationally on the basis of the Commission's issues.
As part of the analysis work, a number of seminars are planned during the year for the presentation and discussion of the research. A number of seminars will also be arranged which will be concerned with areas not covered by the supporting reports.

13
It is a relatively short time frame for such an extensive assignment. During the course of the process, the primary purpose of the external dialogue is to support and deepen the analysis work so that the final report shall be underpinned by as much scientific and experience-based knowledge as possible. This also places requirements on the strategic selection of participants in the dialogue.
Looking back ten years, a large number of scientific articles have been written about the health of Malmö's residents, determinants and conclusions drawn from them. The articles are based on questionnaires to Malmö's residents and on qualitative investigations. In addition, the City of Malmö and other actors are taking part in different dialogue forms which generate knowledge about Malmö's residents. We consider it our duty to utilize the existing knowledge obtained from dialogue and research.
The communication channels that were established included the website (malmo.se/kommission) where all material encompassing the Commission's work is available. It is also possible to contact the Commission through the website. Newsletters and social media (blogs, Facebook) are also used. Furthermore, the Commission has contributed in numerous contexts at the international, national and regional levels, and in Malmö, in order to obtain input to the work and communicate the issues. Since these issues have such a presence in the social debate, mass media have been interested and monitored the Commission's work. In appendix 3 there is a summarized compilation of the contexts that the Commission participated in.
Reference groupsRegion Skåne's Råd for jämlikhet i hälsa (Council for equity in health) started its work this year. The Commission has had continuous dialogue with the region and it is of great importance that this dialogue continues.
The Swedish Association of Local Authorities and Regions (SALAR) has taken the initiative to form the Samling for social hållbarhet - minska ojämlikhet i hälsa (Joint Action for Social Sustainability - reduce inequalities in Health) with 22 contributing municipalities and regions. The ambition is
to produce strategies proceeding from the municipal and regional arenas.
In addition, the Commission is establishing contact with other persons and reference groups, for example, associations linked to specific issues.
Final ReportThe Commission's recommendations will be presented in a written final report. It will include proposals for strategies, the expected effects of the strategies and proposals for how these can be monitored.
10 2 Bremberg, Jämlikhet i hälsa: perspektiv, begrepp och mått (Equity in health:
1.2. INEQUALITIES IN HEALTH NOTHING NEWThere are numerous definitions of inequalities in health. The Commission on Social Determinants of Health (CSDH) definition states, “Systematic inequalities in health which may be avoided with sensible action are simply unjust. It is these inequalities we are referring to with the term 'inequality', or 'unjustness' in health.”
The Swedish National Institution of Public Health applies the following definition of equity in health: “Equity in health is the absence of potentially remediable, systematic differences in one or more aspects of health across socially, economically, demographically, or geographically defined population groups or subgroups.2”
Inequalities in health are neither new nor unique to Malmö. In the middle of the 1800s, it was shown that shabby housing caused illness and death in many countries. Ludvig (Lubbe) Nordström's radio report about Lort-Sverige (Filthy Sweden) from 1938 produced indignation, but a literal sanitary awakening at the same time. After the Second World War, and accompanying a powerful economic growth, there was a rapid expansion of health care, firstly by hospitals and then by primary health care. England led the way with the establishment of the National Health Service.
But, the inequalities in health remained. Around 1970, the political interest in the inequalities in society intensified,
and various investigations were initiated in the Nordic countries, among them examinations of standard of living and living conditions. These also demonstrated inequalities in health, but the conclusions and initiatives were primarily the continued expansion of primary health care. Studies show that the social inequalities in mortality increased after 1970 in the Nordic countries.
The World Bank's Investing in health received global attention in 1993. The allocation of money for health improvement measures should not be seen as an expense, but as a necessary investment. A European study showed that if everybody had the same rates of mortality, sick leave and early retirement as the best educated 20% of the population do, overhead costs in the form of lost production and fees for medical care and transfers could be reduced by an amount corresponding to5.8% of GDP.
Improved global public health is connected to the pervasive political, social and economic changes that have taken place on all continents during the period after the Second World War. Reduced misery and poverty, increased economic resources, reduced size of families and a significantly improved level of education for both men and women constituted a few of the strongest driving forces. Increased access to medical care was also of importance, especially for the elderly, but it was social changes that were generally of greater importance for increased life expectancy than the expansion of medical care, both nationally and globally.
However, the benefits of these developments have not been distributed equally. The current inequalities in health between different regions, countries and populations in the world are enormous. “Social injustice is killing people on a grand scale”, wrote the Commission on Social Determinants of Health in its report to the World Health Organization in 2008. What forms the basis of such a dramatic assertion?
There is a 30 year difference in life expectancy if Japan or Norway is compared with South Africa or Tanzania. Similar differences exist within countries, sometimes of the same magnitude. The
cause lies in the different living conditions. The chances of a new-born child having a long and healthy life differ radically depending on where on the earth the child is born and the social environment in which the child grows up. From around the year 1990 we have seen a change in the trend of global health development. The development towards increased global equity, which continued uninterrupted after 1950, was halted in 1990. The differences between countries were thus larger in 2010 than in 1990.
11
10 2 Bremberg, Jämlikhet i hälsa: perspektiv, begrepp och mått (Equity in health:
1.3. WHY REDUCE INEQUALITIES IN HEALTH? Sustainable developmentThe three dimensions to sustainability - ecological, economic and social - are mutually dependent upon each other. No aspect is more important than another. It is not correct to talk about sustainable economic development if the ecological or social system is moving towards unsustainable development. In a strongly segregated society, with large social differences between different groups, the trust in other people and social institutions is reduced. The health and well-being of people is affected. Reduced social differences promote not only the social aspect of sustainability with greater trust and perceived justice, but also entail better conditions for economic and ecological sustainability, since these are closely associated. The development of health comprises an important indicator of the sustainability of all three dimensions of sustainable development.
Ethical motivesThere is also a strong ethical motive for reducing health inequalities in Malmö. A fundamental starting point in Swedish social and health policy is to proceed from the “humanistic view of people”. Having a humanistic approach entails all
people being accorded equal value; that everybody is provided with equivalent conditions for development. National legislation and municipal policies establish the creation of societal conditions for good health on equal terms as a fundamental goal.
In accordance with article 24.1 in the Children's Convention, each State that ratified the Convention shall recognize the right of all children to “...the enjoyment of the highest attainable standard of health and to facilities for the treatment of illness and rehabilitation of health. States Parties shall strive to ensure that no child is deprived of his or her right of access to such health care services.”3. Furthermore, States Parties to the Convention shall recognize “...the right of every child to a standard of living adequate for the child's physical, mental, spiritual, moral and social development.”4.
In accordance with the UN's declaration of human rights, every individual “...as a member of society, has the right to social security and is entitled to realization, through national effort and international co-operation and in accordance with the organization and resources of each State, of the economic, social and cultural rights indispensable for his dignity and the free development of his personality.”5. Health inequalities caused by social factors mean that all people are not provided with the same opportunities to develop and feel secure in their lives; the citizens to not have the same preconditions for reaching their
3 Convention on the Rights of the Child, article 244 Convention on the Rights of the Child, article 275 UN's Universal Declaration of Human Rights,
article 22
full potential. The fact that the health of citizens is determined by their socioeconomic situation constitutes an inhibiting factor to the individual's freedom.6
It is not possible to counter large inequalities in health using simply the national and municipal regulations applicable in Sweden and Malmö, but the international declarations and conventions that Sweden has ratified must also be incorporated.
Socioeconomic benefitsIt is not possible to put a definitive price tag on the costs of inequality in health - there is no unequivocal calculation. Every individual calculation is based upon a number of assumptions. That it concerns large amounts is not in doubt, similarly that there are socioeconomic benefits to be gained.
The costs of illness are high, in terms of both direct and indirect costs (productivity losses) and because well-being is unevenly distributed among the population. How resources should be allocated in order to reduce illness depends on the relationship of the costs to different measures. The Commission will therefore make health economics calculations for
specific measures. The purpose is to be able to give the client, the Municipal Executive Committee, an understanding of the effects that may be expected from investing in the proposed strategies.
Inequality also has a negative effect on the long-term economic growth in the community. According to research conducted by the International Monetary Fund (IMF), increased equality leads to increased efficiency and thereby a more long-term, sustainable growth.7
12 6 Ulighed i Sundhed – Årsager og Indsatser (Inequality in Health - Causes and Initiatives), Sundhedsstyrelsen (National Board of Health, Denmark), 2011
7 Equality and Efficiency Finance & Development, September 2011, Vol. 48, No. 3 Andrew G. Berg and Jonathan D. Ostry
13
2. Social determinants of healthWhat relationships exist?
What are the driving structural forces behind the inequality in health, and what is the Municipality able to affect? This question provides the focus for the Commission's work. Nowadays we have extensive knowledge about the factors which cause illness. It is often said as a joke that the risk of death is one hundred per cent. Nobody gets away. But, why do some individuals become sick already when they are young, with potential death as a result? There are decisive social factors included in the often complicated causal chain which determine the length of our lives. Examples of such factors are the social environment of the pregnant mother and growing child, school, school environment and importance of good education, meaningful work, good working environment, a safe physical environment and a secure and meaningful old age. There are also differences which result from being a man or a woman.
Research about the population's health is dominated by studies of life span, mortality and morbidity. It can easily become a “description of gloom” with focus on the pathogens which cause and perpetuate sickness. But, there are researchers who focus on health and the possibilities of living healthily for many years. One of them was Aaron Antonovsky, who introduced the term “salutogenesis”. The salutogenic perspective focuses on factors which cause and perpetuate health, and is the opposite of a pathogenic approach. An important term which belongs to the salutogenic research is the “sense of coherence”.
Even though Antonovsky and other researchers contributed to another point of view, the pathogenic “sickness perspective” still dominates within public health research. This also applies to the data about health in Malmö which has been produced.
It can often be simple to demonstrate the relationship between cause and effect without the need for a clear connection with the social environment to exist. Everyday examples include many infectious diseases, where it can be demonstrated
through simple tests that a certain bacteria or virus is causing the disease. The cause is known, and then treatment which is known to be effective may be initiated. However, the relationship is often considerably more complex, and the causes only partly known.
Myocardial infarction (heart attack) is the most common cause of death in Sweden, and a good example of how difficult it can be to establish the causes, which makes taking effective measures complicated. The most significant cause of heart attacks is arteriosclerosis of the coronary artery. It can begin in childhood

14
and then accelerate at different speeds in different individuals. A complicated interaction takes place between the individual's genetic makeup and a number of “risk factors”. The most well-known are blood pressure, blood fats, smoking of tobacco, exercise, excessive weight and diet. A foetus can be affected by various factors which increase the risk of suffering a heart attack later in life. The risk factors can accelerate the process of arteriosclerosis from birth throughout the rest of life. It progresses at different speeds among various individuals. Certain individuals have few or no risk factors, and may live for many years without suffering a heart attack. Others have several or many risk factors, and can become ill while still young. We know that it is possible to affect a large number of these risk factors, and thereby reduce the risks (do not smoke, do not gain weight, exercise regularly, receive treatment for high blood pressure and blood fats if having a better diet is not sufficient to reduce these levels). The earlier in life that this occurs, the smaller the risk is of suffering a heart attack. We know that there are often several risk factors which work together, and also strengthen each other, but all the risk factors are not yet known despite research in the field being intensive. We also know that arteriosclerosis increases with age, for which we still have no cure. In addition, the risks are greater for men than for women.
The majority of people are quite conscious of the significance of these risk factors for becoming ill, in this example, of suffering a heart attack. But, both heart attacks and many other diseases (cancer, musculoskeletal diseases, mental ill-health, respiratory diseases, illnesses related to abuse, some accidents) are more common among those exposed to adverse factors in
their social environment. There is strong scientific support for the theory that many of the known risk factors for different diseases are more common among individuals who are socially vulnerable. This social vulnerability is established already at birth.
Research about inequalities in health demonstrates that a direct relationship exists between holding a higher position in the social hierarchy and having better health. This is called the social gradient. The more influence, money, prestigious work, better housing etc. that a person has - the better the health of that person will be. This applies to both self-perceived health and a longer life. The statistics in the City of Malmö's report on well-being demonstrates this. Those who have a lower level of education, lack monetary support, live in cramped conditions and are not socially active have worse self-perceived health, but also higher rates of illness and mortality. The Commission will expand on this on the basis of a deepened analysis of the Malmö data.
15
An accumulation of risk factors affects health. This accumulation is clear in the area of housing and socially exposed environments. Low income, unemployment, low education and low confidence in society are prevalent in certain areas. Accidents, smoking, excessive weight and their implications for diabetes and cardiovascular diseases are more common in socially exposed groups.
It is clear that if social vulnerability could be reduced, many cases of illness, accidents and death could be avoided. The Commission will perform additional work with the issues that surround the segregation of housing, both as a reason for and effect of poor health.
2.1. SOCIAL CAUSES OF HEALTH INEQUALITIES IN MALMÖThe basis for the Municipal Executive Committee's decision to appoint a commission for a Socially Sustainable Malmö was the conviction that social factors exist which explain the inequalities in health that have been demonstrated in the city in recent years. However, even though it has been possible to demonstrate geographical differences in life expectancy of up to eight years between the sectors which previously comprised the Municipality, a deeper analysis of the social causes has been lacking, as well as how these could be influenced.
The extensive research that provided the basis for, among others, the WHO report 'Closing the Gap in a generation', the English: 'Fair Society, Healthy Lives' and the Danish report: 'Ulighed i Sundhed - årsager og indsatser', demonstrates convincingly that a number of social factors explain the inequalities in health:
• Children's early development - cognitive, emotional, social• School - incomplete education• Segregation and social surroundings• Income - poverty• Prolonged unemployment• Social vulnerability• Physical environment• Working environment• Lifestyle• Early reduced functional ability• The role of health and medical care• The excluding labour
16
market
17
3. The health of Malmö's residents3.1. BASIC DATA ABOUT THE HEALTH OF MALMÖ'S RESIDENTSWe consider it necessary to provide as reliable and current an image as possible of how the inequalities appear and their development over time in connection with social factors. This constitutes the foundation required for the recommendations which are contained in the final report. The annual report on well-being accounts for the results of approximately 50 indicators presented at a city district administration level, and to some extent between the sexes, foreign background and a comparison between Malmö and Sweden as a whole.
With the assistance of researchers, we have attempted to obtain as good an image as possible of the health inequalities in Malmö from a social perspective over the course of an entire life. It will be made available via information in the supporting reports, which the Commission will publish. Using these as the starting point, the Commission is working on a deepened analysis and recommendations.
3.2. FROM PREGNANCY TO THE AUTUMN OF LIFEThe life expectancy trendLife expectancy among women in Malmö during the period 2006-2010 was 82.7 years, which is six months less than the national average. The corresponding life expectancy for men in Malmö was 77.9 years, which is 1.2 years less than the national average. Between city districts during the same period, the difference for women is 4.3 years and for men it is 6.4. That the differences between city districts are not larger is probably a result of the city districts being more heterogeneous, in terms of population, than the 18 sectors where the differences amounted to eight years (Public Health Report for Malmö 1991).
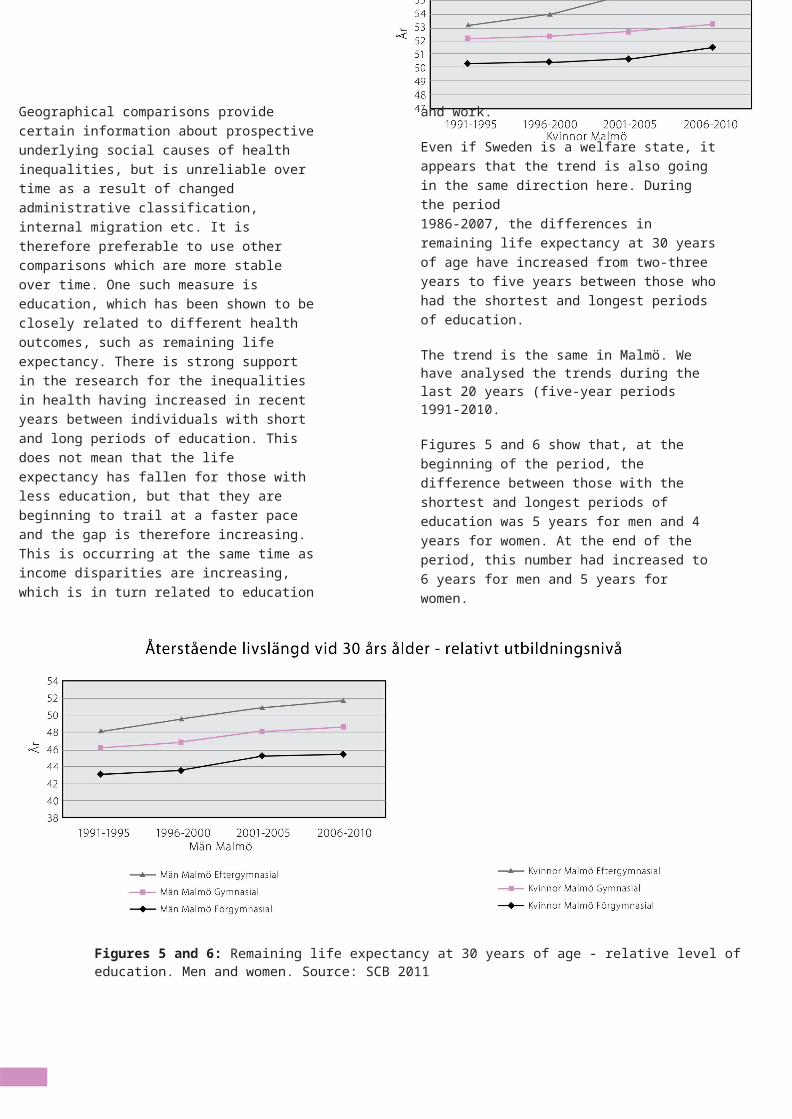
Geographical comparisons provide certain information about prospective underlying social causes of health inequalities, but is unreliable over time as a result of changed administrative classification, internal migration etc. It is therefore preferable to use other comparisons which are more stable over time. One such measure is education, which has been shown to be closely related to different health outcomes, such as remaining life expectancy. There is strong support in the research for the inequalities in health having increased in recent years between individuals with short and long periods of education. This does not mean that the life expectancy has fallen for those with less education, but that they are beginning to trail at a faster pace and the gap is therefore increasing. This is occurring at the same time as income disparities are increasing, which is in turn related to education and work.
Even if Sweden is a welfare state, it appears that the trend is also going in the same direction here. During the period1986-2007, the differences in remaining life expectancy at 30 years of age have increased from two-three years to five years between those who had the shortest and longest periods of education.
The trend is the same in Malmö. We have analysed the trends during the last 20 years (five-year periods 1991-2010.
Figures 5 and 6 show that, at the beginning of the period, the difference between those with the shortest and longest periods of education was 5 years for men and 4 years for women. At the end of the period, this number had increased to 6 years for men and 5 years for women.
18
Figures 5 and 6: Remaining life expectancy at 30 years of age - relative level of education. Men and women. Source: SCB 2011
19
Pregnant women in MalmöA report encompassing all pregnancies from 01-01-2000 until 31-12-2010 has been compiled by senior physician Johan Molin, Women's Health Clinic, SUS, Malmö. Reported here is tobacco usage, excessive weight and obesity, diabetes, mental ill-health and teenage pregnancy relating to city districts, education or country of origin.
On the basis of knowledge about how maternal health care works, possibilities should exist during the pregnancy for the mother to take advantage of the opportunities to create greater chances for a good life for the expected child (psychosocial and social initiatives). Unique possibilities may exist here to be involved at an early stage.
Children 0 - 5 yearsIn November 2010, the Kunskapcentrum (Centre of knowledge) for child health care in Region Skåne. The activities support child health care in the region with competence development for personnel as well as development of the content of child health care. Data is compiled about children's health and health care as part of the work.
The Director of Kunskapscentrum is child health care senior physician Marie Köhler, who is one of the commissioners. Marie Köhler is compiling extensive documentation about the health of Malmö's children, based on over ten sub-studies. When the compilation is complete, an analysis shall be made with suggestions about how health could be improved and how health risks and inequalities should be able to be reduced.
The extensive and unique knowledge about the health of the children and their families' living situations which the Commission is collecting will likely provide support for strategies concerning what is required for the children to receive an optimal chance for good health and quality of life during the rest of their lives.
The health of school pupils and school health care in Malmö Malmö, like many other municipalities in the country, lacks systematically collected knowledge about the health of school
pupils. The new school laws which became applicable on 1 July 2011 entail the introduction of combined pupil health (medicinal, psychological, psychosocial and special needs competencies).
The delineation of responsibilities has been clarified within school health care during 2011. One of the tasks was to initiate the work of collecting general background data about the pupils' health for the directors of the activities (Directors of Children and Youth in their respective city districts). This data can then constitute the basis for future interventions and as a reference for developmental work related to particularly exposed

20
groups of pupils. Coordinating school physician for primary and secondary schools, Stefan Kling, has been given the task of producing such a report on behalf of the Commission.
Part of this involves a repeated survey of classes 6, 9 and secondary school class 2, relating to lifestyle etc. These surveys are now being processed by the Commission in order to gain some understanding of how the pupils' habits relating to smoking, drugs, alcohol, enjoyment etc., have changed over time, as well as the differences between the sexes, schools and city districts.
It should be possible to create a system to follow the development of health among all children in Malmö, from pregnancy, through the first years within child health care and school health care. This issue should have a high priority if all children shall receive an optimal chance to a healthy and good life. The structure exists, but the cooperation or working methods require examination.
Malmö’s adult populationSince the year 2000, a public health survey is conducted in Region Skåne every four years. It is aimed at randomly selected people within the age group of 18 - 80 years. Three surveys have been conducted up until this point, and have been accounted for in the reports. The fourth will be conducted in 2012. Comparisons can be made over time.
Upon request from the Commission, researchers have specially processed the responses from all Malmö's residents who took part in the surveys in 2000, 2004 and 2008.
The questionnaire included questions concerning profession, education, lifestyle, physical and psychosocial working environment, social network, social support and faith, physical and mental health as well as contact with health care and dental care.
A majority of studies and reports demonstrates clear differences in the morbidity, mortality, self-perceived health and different health risks between different socioeconomic groups. This applies regardless of whether relative or absolute differences are measured, and includes studies based on both differences in educational level, income or employment/profession. There is currently a strong connection in Malmö between poor health and housing environment, income, education and whether the person was born in Sweden or another country.
Malmö's residents 60 - 90 years old.The project "Good Aging in Skåne" (GAS) is part of the Swedish National Study on Aging and Care
(SNAC). Professor Sölve Elmståhl is responsible for Skåne’s part of the project. He and his colleagues were assigned the task by the Commission of processing the results from
21
all participants from Malmö 2001 - 2004. All participants underwent a doctor's examination, psychological tests, and different functional tests and were interviewed about lifestyle and health.
Increasing age is of extremely great importance for functional ability and satisfaction with life. But, a lifestyle which is good for one's health, and environments which support individual activities, participation in associations with good accessibility increase the opportunities to strengthen the individual's physical, mental and social reserve capacity.
The significance of the environment on social differences in healthMaria Albin and Kristina Jakobsson, Professors at the Division for Occupational and Environmental Medicine at Lund University and pol. mag. Anders Djurfeldt was given the task by the Commission of producing information about the importance of the public environment (the residence, environment surrounding the residence, pre-school environment, school environment) as well as the working environment (working life term, form of employment, access to corporate health care, work, unemployment, physically demanding work, work accidents) for health in Malmö.
A pervading pattern based on a large number of studies is that individuals in Malmö with low education, who are born in a foreign country, are unemployed, who live with financial stress, are more exposed to negative factors in both the environment surrounding the home, in school/pre-school and at work.
Socioeconomic differences in health between men and womenSusanna Toivanen and Marit Gisselmann, researchers at CHESS Stockholm University/Karolinska Institutet, are writing a report for the Commission about socioeconomic differences in health among women and men. Women report more poor health than men at the same time as they have a longer life expectancy. In the coming report, the differences in health and life expectancy between women and men are illuminated, on the basis of theories about sex and gender, and the authors contribute to analyses based on Malmö data.
Health care consumption in MalmöGeneral Practitioner and researcher, Anders Beckman has studied the consumption of care in Region Skåne, and in Malmö in particular, for many years. On behalf of the Commission he analysed the relationship between consumption of care (doctor's visits as outpatient, visits to nurses, physiotherapists, psychologists as well as inpatient care) and the socioeconomic circumstances of children as well as adult men and women of all ages in Malmö.
Proceeding from the legislative requirement for equal care, it is important to have a picture of the situation in Malmö that is as correct as possible. The preliminary analysis that was made indicates that none of the alarming differences in the consumption of care resulted from socioeconomic causes. Further analyses are planned, which are of interest for both the City of Malmö and Region Skåne.
Studies, dissertations and scientific articlesResearch in the field of health care is extensive in Malmö. Since Malmö Public Hospital became the University Hospital in
22
1948, the research conducted at the Malmö section at the Faculty of Medicine at Lund University has been extensive. Nearly 10,000 scientific articles have already been published in international scientific journals since the year 2000. A significant number of these are studies of parts of Malmö's population or of patients residing in Malmö.
23
An examination of these publications provides additional and interesting information about the social skewedness of mortality, morbidity and preventative initiatives among Malmö's population.
Even though many of these studies are based on geographical comparisons within the city, an account of the socioeconomic profiles for sectors or city districts have been produced for many of them. Since many of these studies were based on well-defined illnesses, if they are classified with adequate scientific method they comprise an additional important contribution with regard to describing social differences in health in Malmö.
In summationIn 1991, the Department of Social Medicine and the Institution for Clinical Institution for Clinical Community Medicine produced the first public health report for Malmö. It summarized over twenty data sources which described health in Malmö from different perspectives. The report was produced on the initiative of the Community Environmental Health Council which had the overall responsibility for public health matters in the Municipality at the time.
Malmö was divided into 18 sectors at the time. During the period 1984 -1989, the life expectancy for men in Malmö was 73 years and for women it was 80. A significant increase has taken place since then, which was reported earlier. But, the differences between the sectors were large, as much as eight years for both men and women.
We can now establish on probable grounds that even if everyone in Malmö seems to have become healthier, the differences between those who live under the worst social conditions and those who live under better conditions have not decreased in recent years. If anything, the opposite has occurred. Malmö must learn from its history and ensure that the trend turns in the right direction in coming years. The unique information base that a large number of researchers has produced about the health of Malmö's residents on behalf of the Commission is considered invaluable for the Commission's continued work.
From pregnancy until the autumn of life
The Commission's continuing work:
During the spring, a number of supporting reports with a deepened analysis of health in Malmö will be presented. All researchers met on 6 February for a joint analysis and presentation of the supporting information. Follow-up and a deepened analysis are planned during the spring.
• Mödrahälsovård (Maternity health care), Johan Molin• Malmös barns hälsa (The health of Malmö's children), Marie Köhler• Sjukvårdskonsumtion i Malmö (Health care consumption in Malmö), Anders Beckman• Medicinsk elevhälsa Skolhälsovården (Medical health of pupils School Health Care), Stefan Kling• Livsvillkor,levnadsvanor och hälsa i Malmö (Living conditions, lifestyle and health in Malmö, Maria Fridh, Mattias Grahn, Martin Lindström, Birgit Modén and Maria Rosvall• Hur mår de äldre i Malmö? (How are the elderly in Malmö feeling?, Sölve Elmstål and Henrik Ekström• Mammografi (Mammography), Sophia Zackrisson• Socioekonomiska skillnader i hälsa bland män och kvinnor (Socioeconomic differences in health among men and women), Marit Gisselman, Petra Lindfors and Susanna Toivanen, CHESS Stockholm University/Karolinska Institutet• Miljöns betydelse för sociala skillnader i hälsa (The importance of the environment for social differences in health), Maria Albin, Anders Djurfeldt and Kristina Jakobsson
19
4. Knowledge base- discussion material
The commissioners and many other researchers are producing scientific data relating to the social factors which affect health. During spring, these knowledge bases will be presented. These correspond to particular aspects which comprise important preconditions for health and inequality in health. The reports constitute the data for the Commission's final report, but also serve as discussion material about problems and causes, what aspects are possible to affect and how.
A number of reports are complete and others will be presented during the spring. Their purpose is to provide scientific, factual data as a basis for the recommendations. We are also working to identify the preconditions for being able to implement the strategies.The knowledge base is presented below on the basis of the following areas:
• Childhood conditions - giving children a good start in life• Work and working environment - adult life• Reasonable living standard - income and health• Sustainable and healthy communities• How do we measure inequality in
health? How do we measure community development?
• What we can learn from history - Malmö and its surroundings• Implementation - organization and governance
4.1. CHILDHOOD CONDITIONS - GIVING CHILDREN A GOOD START IN LIFE The Marmot Commission concludes that an early start is necessary, which is also the starting point for the Malmö Commission. Malmö is characterized by a young population. Half of its residents are under 35 years old and 62,500 people are under 18 years old. The strategies from the Malmö Commission will encompass childhood conditions in several ways.
Children's health
Marie Köhler is compiling a report about children's health in Malmö. The report has a clear children's rights perspective, and for several parts she has received assistance from over ten researchers. The report encompasses the situation in Malmö and includes a treatment of the Children's Convention, the measuring of children's health, child health care, parental support, children that are in trouble, children and homelessness, asylum-seeking children, child safety, the importance of play and health, children of parents in
20
detention, social environment/residential environment and access to care, and children of parents with mental ill-health.
EconomyThe annual report Barnfattigdomen i Sverige (Poverty among children in Sweden) from 2010 illustrates that Malmö, according to Save the Children's definition, is the municipality with by far the highest proportion of relative poverty among children (Malmö 31 per cent, Stockholm 14 per cent, Göteborg 17 per cent). The term “child poverty” is controversial, but regardless of this, the situation is that every third child in Malmö is growing up in families with parents who cannot support themselves. An extensive scientific knowledge base exists which illustrates that poverty during childhood has negative effects, not just for health, but for the level of education, the need for financial support and the risk of becoming unemployed as an adult.Tapio Salonen, Professor of Social Work and commissioner, and Anna Angelin, Associate Professor of Social Work, are processing scientific studies about the causes of child poverty, its consequences and distribution at a national level and locally in Malmö. This work will result in two supporting reports which will, among other things, present prognoses and recommendations for halving child poverty in Malmö by 2020.
Education and healthThe relationship between education and health is clear. Health affects the level of education and the level of education affects health. A person’s level of education (highest completed education) affects that person's position in the labour market and thus the economic, physical and psychosocial conditions as well.
The general level of education in Sweden has risen, which is important for the development of public health. The differences in life expectancy between the different levels of education have increased simultaneously, which is illustrated in diagrams 5 and 6.The level of education in Malmö is lower than the national average. The eligibility rate (eligibility to apply for upper secondary schools) has fallen in the last two years by four percentage points, from 80 per cent to 76 per cent. The Swedish average in 2011 was 88 per cent. There are large differences between city districts and between schools. At one school in Malmö, 27 per cent of the pupils were eligible to apply for upper secondary schools, and at another school it was 100 per cent.
The Commission is working to identify and analyse factors of importance for the performance of pupils at school, such as school segregation, newly arrived pupils, freedom of choice, educational

21
working models applied, cooperation between school and home, etc. Evidence relating to effective measures will be investigated. In addition, empirical Malmö material will be compiled, which includes statistical data of the situation in Malmö and evaluations of educational initiatives. Contact is made with activities in the City of Malmö to the extent that is required. The ambition is to recommend initiatives which can increase the level of education among children and youths in Malmö.
The importance of pre-school for development, learning and healthPre-school can, and should be such a favourable environment for the child that it provides the opportunity to utilize abilities and skills, not only in pre-school, but also later in school. Sven Persson, commissioner and Professor of Pedagogy is writing a report together with commissioner Kerstin Larsson, Förskolans betydelse för barns lärande, utveckling och hälsa (The importance of pre-school for children's learning, development and health), concerning measures which can contribute to providing children with the best possible prerequisites.
The report focuses on the pre-school's quality and on what is required in order for the pre-school to be able to reduce social inequalities. Children from vulnerable socioeconomic conditions and children at risk benefit most from attending pre-schools of a high quality. On the basis of the existing knowledge and the situation in Malmö, proposals are made which can improve the pre-school's quality, through dialogue with pre-school representatives in Malmö.
Primary and secondary schoolThere are large differences in educational levels between city districts and schools in Malmö. The explanations for this and the aspects that are possible to affect are presented by commissioner Nihad Bunar, Professor of Child and Youth Studies, in a report for the Commission, Skolan och staden, forskningsperspektiv på integration och skolrelaterade klyftor i den moderna staden (The school and the city, research perspectives concerning integration and school-related disparities in the modern city).
The report presents, analyses and discusses part of the Swedish and international research concerning important factors for pupils' performance at school, as well as the mechanisms, processes and relationships in and throughout the education system that create and maintain social and health disparities between children and youths. Malmö is one of Sweden's most multicultural municipalities. Nearly half of all children between the ages of 7 and 15 years have a foreign background, of which 32 per cent are born in Sweden with both parents born in a foreign country, and 17 per cent were themselves born in a foreign country, which
22
affects the local education policy. The report takes its point of departure in the sociology of education’s reasoning about social disparities and injustices, as well as in a few main external factors which affect the pupils' school results. External factors include the time of entry in the Swedish school, background factors (class, gender, ethnicity) as well as the effects of residential segregation and freedom of school choice.
On the basis of research, the situation in Malmö and the political instruments available, a number of concrete measures are proposed.
Nihad Bunar will present an additional report in the spring, called Utbildningsreformer i urbana skolsystem– lärdomar från internationella och svenska erfarenheter (Educational reforms in urban school systems – lessons from international and Swedish experiences). Grounded in a Malmö perspective, the report will identify, discuss and analyse a number of the educational reforms that have been implemented in cities and regions with more extensive social inequalities.
Upper secondary schoolMargareta Cederberg is an Associate Professor of Pedagogy at Malmö University. She is writing a research overview for the Commission about pupils in upper secondary schools and their health. Particular focus is placed on pupils that did not complete a national secondary school programme within three years, the “drop-outs”. Submitting proposals for initiatives based on the research results is also part of the assignment.
The importance of after-school centresAfter-school centres are a municipal operation. In 2010, 78 per cent of 6 – 9-year-olds, and 29 per cent of 10 – 12-year-olds were registered with an after-school centre in Malmö. Research relating to the importance of after-school centres in children's development and health is limited. Research activities relating to after-school centres are being set up at Jönköping University. Responsible for these are Ann Ludvigsson, Associate Professor of Pedagogy and Carin Falkner, Associate Professor of Education. These two researchers are preparing a report for the Commission concerning the importance of after-school centres for children's health, learning and development. The supporting report will describe the after-school centre's function in the education system and what has happened in the last ten years, and then draw conclusions from this information. The situation in Malmö will be described, among other things, on the basis of the Swedish Schools Inspectorate's report and data on percentages of children, personnel
etc. Furthermore, the report will identify what has been done in Malmö and what has been evaluated, and provide recommendations in a summary.
23
Giving children a good start in life
The Commission's continuing work:
Children's health• Underlagsrapport om barns hälsa (Supporting report on children's health), Marie Köhler• Reports about Maternity health care, Child health care, School health care• Consideration is given to other research overviews in the area
Economy• Barnfattigdomens utveckling i Malmö (The development of child poverty in Malmö), Tapio Salonen• Barnfattigdom - en kunskapsöversikt (Child poverty - an overview of our knowledge), Anna Angelin
Pre-school, school, social environment• Förskolans betydelse för barns utveckling, lärande och hälsa (The pre-school's importance in the
development, learning and health of children), Sven Persson and Kerstin Larsson• Skolan och staden, forskningsperspektiv på integration och skolrelaterade klyftor i den moderna staden
(The school and the city, research perspectives concerning integration and school-related disparities in the modern city), Nihad Bunar
• Utbildningsreformer i urbana skolsystem – lärdomar från internationella och svenska erfarenheter (Educational reforms in the urban school system – lessons from international and Swedish experiences) (preliminary title), Nihad Bunar
• Gymnasiet och drop-outs (Upper secondary school and drop-outs), Margareta Cederberg• Fritidshemmens betydelse för barns hälsa, lärande och utveckling (The importance of after-school
centres for the health, learning and development of children), Ann Ludvigsson and Carin Falkner
Other• The Commission is monitoring the development of the Municipality's policy and ambitions for increasing participation among children and youths.• Childhood conditions encompass all other areas, such as physical planning, culture and recreation.• Analysis work will be done using the research and seminars as the starting point.• Upcoming seminars/hearings which encompass the Commission's issues and the children's learning,
health and development.

24
4.2. WORK AND WORKING ENVIRONMENT - ADULT LIFE Work and a good working environment promotes health. Unemployment contributes to poor health in a corresponding manner. For an individual, employment means better financial conditions and an everyday life that contributes to participation and meaningfulness. For the community, a high employment rate means a larger tax base which can in turn be used to finance welfare services. In 2009, 61 per cent of Malmö's residents of working age were employed, which represents a fall of three per cent in comparison to the previous year. The figures were still at a lower level than for the rest of the country, where the employment rate in 2009 was 75 per cent.
The Commission is processing the issue from the aspect of inequality in health. The Marmot Review and following reports encompass numerous strategies of the conditions for a fair labour market. It is concerned with strategies for improving access to good jobs and reducing long-term unemployment through the social gradient, i.e., in all groups, but particularly those with the worst economic and social conditions.
Professor Urban Janlert has contributed to the Commission with a knowledge overview about unemployment and health. Research shows the connection between unemployment and increased mortality: both the total number of mortalities and mortality through suicide and cardiovascular diseases. Unemployment is also related to increased mental ill-health and, to some extent, even increased somatic ill-health and abuse of alcohol and drugs.
The report describes the national unemployment trend in recent years, and demonstrates the effects on health as well as the variation between men and women. It also illustrates the relationship between the consumption of medical care and sick leave and early retirement, and describes the effects of unemployment in low and high business cycles. A central aspect for Malmö is the consequences of high youth unemployment, which is also emphasized. In addition to describing the effects of
unemployment, Janlert also explains the function of work which, according to the research, fills other important health-promoting functions than simply being a source of income.
Working environment and healthThe Municipality has a limited period in which to consider measures concerning the working environment in general, but there is still room for manoeuvre. This is highlighted by Maria Albin, Kristina Jakobsson and Anders Djurfeldt in a supporting report to the Commission that will be completed in the spring.
25
The report illuminates the significance of the working environment for social differences in health (see also page 17). Particular emphasis is placed on aspects such as the form of employment, length of working life, work accidents and access to corporate health care. The report gives a number of recommendations on the basis of the Municipality's room for manoeuvre. These are concerned with, for example, the municipality's role in its capacity as a large employer, and Malmö Municipality as a large actor in regard to procurements.
Growth and welfareThe Commission also examines the term “work” from the perspective of the relationship between growth and welfare. Mikael Stigendal has written the report Malmö - de två kunskapsstäderna (Malmö - the two knowledge cities) which was based on an attempt to understand the relationship between growth and welfare, linked to strategies for inequality in health. One aspect that is emphasized in the report is the view of work from ongoing international research.
The Commission will also emphasize Malmö in several reports, from regional and global perspectives. Stigendal's report covers Malmö as a regional growth motor, changes in the labour market based on Malmö's historical development, the growth of large cities and globalization as well as which lessons can be learnt. The report, which is available on the Commission's website, culminates in a number of issues which the Commission proceeds with in its continuing work.
The relationship between growth and welfare is related to issues regarding sustainable community development, and is therefore discussed in many contexts and in much data by the Commission.

26
Work and working environment - adult life
The Commission's continuing work:
• Arbetslöshet och hälsa (Unemployment and health), Urban Janlert• Malmö, de två kunskapsstäderna (Malmö, the two knowledge cities), Mikael Stigendal• Miljöns betydelse för sociala skillnader i hälsa (The importance of the environment for social
differences in health), Maria Albin, Anders Djurfeldt and Kristina Jakobsson• Continued analysis of the relationship between education and youth unemployment and work,
as well as Malmö and its surroundings; the future form of the labour market and the role of trade and industry
• Research and activities seminar about the importance of culture and recreational time for health/equality in health is planned.
• Issues concerning the relationship between inequality and structural discrimination will be investigated.
4.3. REASONABLE STANDARD OF LIVING - INCOME AND HEALTHFinances are significant for the possibilities of individuals and families to control and consciously manage their living conditions, and the private economic situation is important for their health. The Marmot Reports give strategies for a “reasonable standard of living”. From a political perspective, factors such as income and education are interesting since they imply that the level of health and its distribution can be affected by measures that are aimed at these factors. The Commission emphasizes this from different perspectives. There is a lot of literature in the area which commissioner Ulf Gerdtham, among others, has contributed to. Relevant research will be taken into account.
Tapio Salonen is writing a report for the Commission about the development, significance and role of income and residential segregation in Malmö. The report focuses on the income trend among Malmö's households over the last two decades, and its significance for the population's health and welfare conditions. New data is presented in it, which demonstrates a clear increase in the income inequality in Malmö between 1990 and 2008. There is a pronounced difference between the entire country and Malmö. The reasons for these differences will be discussed in the report.
Income inequality is connected to the city's physical space; income inequality has had an impact spatially in the city in that residential segregation has increased. The relatively large proportion of adults in the
population that are neither employed nor studying is highlighted, as well as the causes and consequences of this unemployment.
27
The report will also present different choices of measures at the local level in order to reduce or compensate for the consequences of an increased difference in economic living conditions. Addressing the underlying causes lies, to a large extent, outside of the Municipality's room for manoeuvre. The implications at both the national and local levels are reported.
Reasonable standard of living - The application of income support in Malmö's city districtsThe City of Malmö is one of the municipalities in Sweden with the highest proportion of the population requiring financial support. Identified during the course of the work was the need for an illumination of how the City of Malmö manages issues regarding reasonable living standards in relation to financial support. Torbjörn Hjort, Associate Professor of Social Work is contributing a knowledge base on this subject. The report describes how Government decisions concerning support policy are implemented in Malmö. It discusses both the local interpretations of State policy, implementations in municipal policy work and guidelines, as well as differences in completed financial support assessments.
Reasonable living standard - income and health
The Commission's continuing work:
• Utvecklingen av inkomstojämlikhet och bostadssegregation i Malmö (The development of income inequality and residential segregation in Malmö), Tapio Salonen• Skälig levnadsnivå - om handläggning och bedömning av socialbidragsärenden (Reasonable living standards - on the administration and assessment of income support matters), Torbjörn Hjort• Other research overviews about income and health will be taken into consideration.
4.4. CREATING SUSTAINABLE AND HEALTHY COMMUNITIES
The name Commission for a SOCIALLY SUSTAINABLE Malmö comes with an undertaking. The Commission was appointed in light of the city's need to strengthen those factors which are often presented as preconditions for social sustainability. The declaration; Rio Political Declaration on Social Determinants of Health 8, which was adopted by WHO's member states in 2011, provides evidence about how to clearly connect strategies for reducing inequality in health with the preconditions for sustainable development. There is extensive research about sustainability from various perspectives. The Commission is investigating the relationship between inequality in health and sustainability, partly for a general understanding and partly as a starting point for the processing of strategies for reducing inequality in health. The ambition is for the strategies proposed by the Commission to contribute to sustainable development, from all perspectives.
Sustainable developmentCommissioner Per-Olof Östergren, Professor of Global Health and Social Medicine, is writing a report called Hur hänger en socialt hållbar utveckling och hälsans jämlikhet ihop? (How are sustainable social development and inequality in health related?) The report describes how equality appears to be a key factor in the accomplishment of sustainable development. There is strong conviction in the research that unequally allocated resources in society have a great impact on health and its social distribution. Countries with equally allocated resources seem to have healthier populations than countries with great inequalities, even if the countries have the same average income.
This indicates the great importance of creating a more equal society, which will in turn increase the possibilities for social sustainability and for sustainable development as a whole. Discussions about health and equality often proceed from the social aspect, that is, the equality issue is localized in the social subsystem of sustainable development.
24
29
However, inequality is determined to a considerable extent by the factors in the economic system (e.g., labour market processes, systems for salary increases/distribution and financial distribution policy). The report demonstrates that it is not possible to disconnect the three dimensions of sustainability from each other.
Democracy and participation is one of three prioritized areas for the Commission and is defined in the directive as one of the most fundamental preconditions for health. Lack of influence and opportunities to influence one's own living situation has a strong connection to health. If individuals or groups perceive that they cannot influence their own living conditions and community development, powerlessness is the result. There are aspects of issues concerning democracy and participation in several of the Commission's knowledge bases.
The Commission is following ongoing development work led by Katarina Pelin, commissioner and Environmental Director for the City of Malmö. The work encompasses understanding of the room for
manoeuvre on sustainable city development, based on the well-being of the people. This is developmental work in the interaction between research and praxis. It is likely that the work will culminate primarily in discussion material; Välbefinnande och hållbar utveckling (Well-being and sustainable development).
Social capitalSocial capital is a definition used to identify our social network, our social support, our opportunities for participating in community life, and the degree of social belonging in our social surroundings. Maria Emmelin, Professor of Global Health at Lund University, is working on a report for the Commission; Kan socialt kapital ”byggas in” i våra bostadsområden och därmed förbättra invånarnas upplevda och mentala hälsa? (Can social capital be “built into” our residential areas and thereby improve the residents' perceived and mental health?). An overview of the term “social capital” is presented in the report,
8 Rio Political Declaration on Social Determinants of Health, Rio de Janeiro, Brazil, 21 October 2011
25
both as an individual and a collective resource at the geographic area level. The scientific data for how social capital might possibly affect perceived and mental health is introduced, as well as an examination of studies which specifically highlight how these relationships are linked to the residential environment. This data is used as the basis for a discussion of possible ways to “build in” social capital to the residential areas in Malmö with the aim of improving and increasing equality in health.
Segregation, city planning and healthMalmö's widespread residential segregation is clearly mirrored in health outcomes. Segregation means the spatial separation of groups within the population. Segregation can occur on the basis of socioeconomic factors, religion and ethnic background etc. and arises when social differences coincide with spatial separation. Differences in income and employment rates, among other things, become translated into residential segregation. The research demonstrates that tools exist which can be used to reduce segregation, partly through the reduction of social differences and partly through the reduction of spatial separation. The Commission is now investigating the potential of these tools on the basis of scientific support.
The possibilities of physical planning The overview plan is mentioned in the Commission's directive as an important landing strip for the Commission's
proposals. Work with researchers in the Commission (and in the rest of the world) is taking place which, together with city planners within the Municipality, is identifying the room for action available for social sustainability through physical planning. It contains a description of how segregation is distributed at present, what the consequences are and the opportunities for improvement that exist. One example of the room for manoeuvre is the Municipality's
26
position as an institutional actor, in city planning and on the housing market. Supplementary construction of different types of buildings and tenures, an even distribution of goods, services and attractive landmarks which act as magnets can all function as contributory factors to a more integrated city. Public transport, which promotes contact with the supply of goods and services, can contribute to reduced segregation in the same way. It is a matter of reducing the barrier effects that are created by traditional planning models, and providing good conditions for the establishment and localization of workplaces for activities with growth opportunities. Childhood conditions are also taken into consideration in the ongoing work.
Environment and healthMaria Albin, Anders Djurfeldt and Kristina Jakobsson are writing a report about Miljöns betydelse för sociala skillnader i hälsa (The importance of the environment for social differences in health). Presented in this report is Malmö data, consequences, analysis, possible strategies regarding environmental factors such as overcrowding and well-being related to social factors. Factors related to surroundings such as air and noise pollution, and lack of greenery and vegetation, can be affected by municipal city planning.
The future sustainable MalmöThe Marmot Review, Closing the gap in a generation, took the perspective of one generation for the strategies that were proposed. Within the framework for the Commission's objective of formulating goals and strategies, there is a continual forward-looking work with the formulation of the future sustainable Malmö. This involves identifying the capacity and structures for sustainability that exist in Malmö, with particular focus on social sustainability.
27
Creating sustainable and healthy communities
The Commission's continuing work:
• Continuing analysis based on literature and research about the mechanisms behind segregation, how it affects health and which parts are possible to affect.
• Malmö, de två kunskapsstäderna (Malmö, the two knowledge cities), Mikael Stigendal• Miljöns betydelse för sociala skillnader i hälsa – discussion material (The importance of the environment for social differences in health), Maria Albin, Anders Djurfeldt and Kristina Jakobsson• Kommissionens strategier och stadsplaneringen – discussion material (The Commission's
strategies and city planning), Bertil Johansson and Marianne Dock, Stadsbyggnadskontoret• Hur hänger en socialt hållbar utveckling och hälsans jämlikhet ihop? (How are sustainable social development and inequality in health related?), Per-Olof Östergren• Kan socialt kapital ”byggas in” i våra bostadsområden och därmed förbättra invånarnas
upplevda och mentala hälsa? (Can social capital be “built into” our residential areas and thereby improve the residents' perceived and mental health?) Maria Emmelin
• Välbefinnande och hållbar utveckling – discussion material (Well-being and sustainable development), Sharif Shawky/Katarina Pelin• A working group within the Commission has been established for continued analysis of the
potential of city planning to reduce inequality in health.
4.5. MEASURING INEQUALITY IN HEALTH - MEASURING COMMUNITY DEVELOPMENT
One condition for the formulating of goals and strategies is to measure and understand the problems. There are several perspectives on the Commission's objective regarding data, analysis and follow-up, which are specified in the directive. We have dealt with these issues in different ways.
Firstly, valid measurements and accessible data are required in order to describe the situation in Malmö. The majority of knowledge bases or discussion material includes data pertaining to the situation in Malmö. We are now working to compile and analyse these different descriptions, which means not only that the scope of the problem becomes clearer, but also its possibilities. We are investigating the significance of Malmö's demographic development on, among other things, immigration and emigration to and from the city.
Considerable data is available, for example, through the welfare report. We needed to compile data from difference sources within the City of Malmö and/or order data from
SCB and others. The Malmö Commission has, together with commissioners and City of Malmö personnel,
28
arranged two workshops about the indicators used to measure the development in Malmö. The starting point has been to identify valid measures.
Ulf Gerdtham and Gustav Kjellson have produced a report which is now available; “Mätning och analys av ojämlikhet i hälsa – om konsten att mäta något utan att veta vad och hur” (Measurement and analysis of inequality in health - about the art of measuring something without knowing what and how). Discussed here are proposals for measurements with their basis in the health economics literature to measure and analyse the socioeconomic, or income-related, inequality in health. The report provides insight about the importance of clearly defining inequality in health and demonstrates the complexity involved in measuring good and poor health. The report constitutes data for the Commission’s continued work relating to measurement.
As the Commission's objective concerns social sustainability, the conditions for measuring and following sustainable development are investigated. Per-Olof Östergren deals with this in the knowledge base; How are sustainable social development and inequality in health related? Michael Stigendal also does this in his supporting report Malmö - the two knowledge cities.
29
Measuring inequality in health, measuring community development
The Commission's continuing work:
• Mätning och analys av ojämlikhet i hälsa - om konsten att mäta något utan att veta vad och hur (Measurement and analysis of inequality in health - about the art of measuring something without knowing what and how), Ulf-G Gerdtham and Gustav Kjellsson
• One working group within the Commission, including Ulf Gerdtham, Per-Olof Östergren and Denny Vågerö, is processing proposals about how the City of Malmö can monitor the distribution of health in an adequate manner.
• Malmö, the two knowledge cities, Mikael Stigendal• How are sustainable social development and inequality in health related? Per-Olof Östergren• Social sustainability; globally, locally; seminar with the Commission, Globala Malmö and Malmö
University on 13 April• The future sustainable Malmö – seminar with The Delegation for Sustainable Cities, in Malmö 4-5 June
4.6. WHAT CAN WE LEARN FROM HISTORY - MALMÖ AND ITS SURROUNDINGSIn the final report, we will also describe Malmö from a historical perspective. The transformation of that Malmö: from an industrial city to more of a ‘knowledge city’ is of particular interest. Mikael Stigendal discusses this in Malmö - the two knowledge cities.
Malmö is treated from a regional, national and global perspective in several knowledge bases. The Municipality’s room for manoeuvre in terms of strategies must be taken into consideration in this analysis, as well as an understanding of the relationship between health and structural factors.
One contribution to this understanding is provided by Hans Abrahamsson, Visiting Professor in Global Political Studies, Malmö University. With its point of departure in the ongoing globalization, migration and urbanization processes, his report discusses the role that cities and their cross-boundary networking collaboration can play in globally sustainable community development. Many medium-sized cities find themselves in a state of tension between contributing to global community governance on the one hand, and turning into a battlefield for social conflicts on the other. The report focuses its attention on several factors which could affect the direction of movement in such a state of tension, from a peace and development perspective.
What can we learn from history - Malmö and its surroundings
The Commission's continuing work:
• Malmö, the two knowledge cities, Mikael Stigendal• Städer som noder för global samhällsstyrning eller som slagfält för sociala konflikter
(Cities as nodes for global community governance or battlefields for social conflicts), Hans Abrahamsson
• There has been a lot written about Malmö, both historical and current descriptions. The Commission will take these into account to the extent that it is possible.
30
4.7. IMPLEMENTATION - ORGANIZATION AND GOVERNANCE
The Commission's objective is to produce scientifically-based strategies for factors that are possible to affect and, taking the Municipality's room for manoeuvre as its starting point, presenting them in a final report. And what happens next? It is up to the client, the Municipal Executive Committee, to decide how and to what extent the strategies shall be implemented. What are the preconditions for implementation? What room for manoeuvre does the Municipality have? Which forces are working for and against the accomplishment of the changes?
Within the framework of the Commission's work, we are attempting to ensure that the strategies are scientifically-based, that they are feasible, and that calculations have been made of the expected effects of the strategies.
The following ongoing processes are contributing to this:• Illumination of the lessons we can learn
from previous initiatives in Malmö such as Välfärd för alla [Welfare for All], Metropolitan Policy etc.
• Examine lessons to be learned from countries and cities where the "Marmot Review” is now being implemented.
• Produce a knowledge overview of research concerning implementation and policy.
• Produce supporting report/discussion material about the room for manoeuvre, on the basis of the Municipality's financial governance system, for example, resource allocation.
• Examine the Municipality's room for manoeuvre in relation to the conditions at other levels or in other arenas.
• Health economic calculations of strategies/measures which can hopefully make it easier for the client to evaluate the expected effects of the strategies.
Implementation researchKarl Löfgren is Associate Professor of Public Administration, Governance and Management at Roskilde University. He is
writing a report about the research field of implementation, which accounts for what we know from research about the success factors for implementation of the type that the Commission is working on. The report will provide empirical examples from the City of Malmö wherever possible.
31
Health economic calculations of the Commission's strategiesIn order to propose measures, not only is knowledge about the health effects required, but also knowledge about the costs and consequences of alternative measures and strategies. In addition to such knowledge, principles are required in order to make assessments as to whether the costs of a certain measure/strategy correspond reasonably to the benefits that they produce. Health economic evaluations are concerned with weighing the costs of a particular measure against its effects, and comprise one of several important sources of information prior to decisions about prioritization. The calculations shall have, as much as possible, a community perspective and take into consideration both the costs and the extra quality-adjusted life years (QALYs) or life years gained. There is no room within the framework of the Commission's budget to perform health economic calculations of strategies. The City of Malmö has therefore, through the Commission, applied for project funds from The Delegation for Sustainable Cities, and been awarded funds in order to make the calculations.
Other aspects of organization and governance We will consider available evaluations which are documented from earlier initiatives in the City of Malmö regarding structural factors, such as Welfare for All and Metropolitan Policy.
Malmö-based research relating to organization and governance will be taken into account.
Swedish economist Ingvar Nilsson is writing a knowledge base for the Commission; Den ojämlika välfärden i Malmö ur ett socioekonomiskt perspektiv (The unequal welfare in Malmö from a socioeconomic perspective). The report builds upon calculations of the costs of alienation on a fundamental level, and the structural mechanisms behind them. The report illuminates the structural problems caused by governance and a monitoring system that do not always reward far-sighted behaviour, as well as by deficient access to social investment capital. In order to overcome the structural problems, an altered public organization structure is proposed, which promotes more efficient resource management. It is argued that it would require new governance, budget and monitoring systems which permit far-sightedness and a social investment approach. One of the things that the report proposes are structures for social investment funds and the requisite conditions for this.
32
Implementation – organization and governance
The Commission's continuing work:
• Den ojämlika välfärden i Malmö ur ett socioekonomiskt perspektiv (The unequal welfare in Malmö from a socioeconomic perspective), Ingvar Nilsson
• Implementering – en forskningsöversikt (Implementation – a research overview), Karl Löfgren• Implementeringsmodell för policy avseende jämlikhet i hälsa
(Implementation model for policy in regard to equality in health), Per-Olof Östergren• Other research will be taken into consideration with regard to effects of cooperation and preventative work.• WHO/Europe shall present its final report in September. It is likely that there will be aspects which are
useful for the City of Malmö.• The purpose of the planned seminars/hearings/dialogues arranged by the Commission is
to better understand the preconditions in order to be able to implement the proposals.• The Commission will perform health economic assessments of new proposals for strategies/
measures supported by the project funds awarded by The Delegation for Sustainable Cities.
33
5. The Commission's continuing work
The final report shall be completed in December 2012. The work leading up to that point will be extremely intense. The proposals for measures in the final report shall be based on scientific grounds, but shall also be practically possible to implement in Malmö.
The foundations of the final report will be constituted of the scientific data from the commissioners and other experts, together with other research and the external dialogue. There will be about 30 sources to this data in total, which will be printed in the Commission's report series when they are finished. The process leading up to printing is extensive. Critical examination of working material takes place through dialogue with authors, other experts, the secretariat and in seminars. The data shall serve as a reliable source for all interested parties. A few of them have already been printed while the remainder shall be finished during the spring.
Seminars and other activities shall be organized for the remaining time in order to highlight special issues. This is done partly to explore important issues in the data more deeply, and partly to provide supplementary knowledge that was not covered in the data. Some of these activities are aimed at different target groups within the Municipality. We hope that the organization, the City of Malmö, will take the opportunity to participate in seminars and dialogue concerning the content of the reports.
Work is being done simultaneously on the final report. The analysis is being carried out through the knowledge base and the seminars/hearings that were arranged, other research, in contact with senior advisers, persons concerned with the issues and within the Commission, of course. The strategies will be evaluated on the basis of different aspects, which are exemplified by the image below.
All of the commissioners shall be included as co-authors of the final report. The reaching of a consensus on a number of proposed measures will require extensive discussion in smaller and larger groups, and with the entire Commission. An important part here is the dialogue between the research community and the practitioners in the Commission. Even if the researchers agree about what is possible, it might be unrealistic, for various reasons, to actually implement a particular measure.
Malmö's goal is to create a sustainable city in the long term: economically, ecologically and socially. The three parts are intimately related. Far-sightedness in planning and budgeting is required in order to succeed. An important ingredient in this work ought to be a good knowledge base incorporated into sensible decisions at all levels. We are hoping that the Commission's final report can contribute to making Malmö a sustainable, attractive and good city to live in for everybody.

34
Diagram 7: Sketches of aspects which will be considered in the evaluation of different strategies.
35
References
Only a limited number of sources are presented in this interim report.
Bremberg S. in Hogstedt, C. (ed.), Välfärd, jämlikhet & folkhälsa – vetenskapligt underlag för begrepp, mått och indikatorer (Welfare, equality & public health – scientific data for concepts, measurement and indicators). The Swedish NationalInstitution of Public Health, 2003
Fair Society, Healthy Lives – The Marmot Review, Swedish translation of the indicators, 2010
Finance & Development (IMF), September 2011, Vol. 48, No. 3, Equality and Efficiency, Andrew G. Berg and Jonathan D. Ostry
Public Health Report for Malmö, 1991
UN Universal Declaration of Human Rights, 1948
UN Convention on the Rights of the Child, 1989
Rio Political Declaration on Social Determinants of Health. World Conference on Social Determinants of Health, Rio de Janeiro,Brazil, 21 October 2011
Save the Children. Barns hälsa i Sverige (Children's health in Sweden), 2004
Sundhedsstyrelsen (National Board of Health, Denmark), Ulighed i Sundhed – Årsager og Indsatser (Inequality in Health - Causes and Initiatives), 2011
Strategic Review of Health Inequalities in England, Fair Society, Healthy Lives – The Marmot Review, 2010
WHO & Commission on Social Determinants of Health, Closing the gap in a generation, 2008

The Commission for a Socially Sustainable Malmö is an independent commission appointed by the City of Malmö to produce goals and strategies to reduce inequalities in health.
Read more at www.malmo.se/kommission and www.malmokommissionen.se