Embed Size (px)
Citation preview

Malrotation and Volvulus in Adults
Boyoung Song, MD SUNY Downstate
Department of Surgery
www.downstatesurgery.org

Case Presentation
HPI: Pt is a 19 yo male who presented with RLQ abdominal pain x 1 day. Denies n/v, fever, changes in appetite or bowel habits. No similar previous episodes.
PMHx/PSHx: None Meds: None NKDA SocHx/FHx: denies
www.downstatesurgery.org

Case Presentation
PE: 99 122/78 63 100% Alert and oriented, NAD S1S2 RRR Clear chest Soft abdomen, nondistended. RLQ tenderness
without rebound or guarding
www.downstatesurgery.org

Case Presentation
Laboratory Work
www.downstatesurgery.org

CT scan
www.downstatesurgery.org

www.downstatesurgery.org

www.downstatesurgery.org

www.downstatesurgery.org

www.downstatesurgery.org

www.downstatesurgery.org

www.downstatesurgery.org

www.downstatesurgery.org

www.downstatesurgery.org

www.downstatesurgery.org

www.downstatesurgery.org

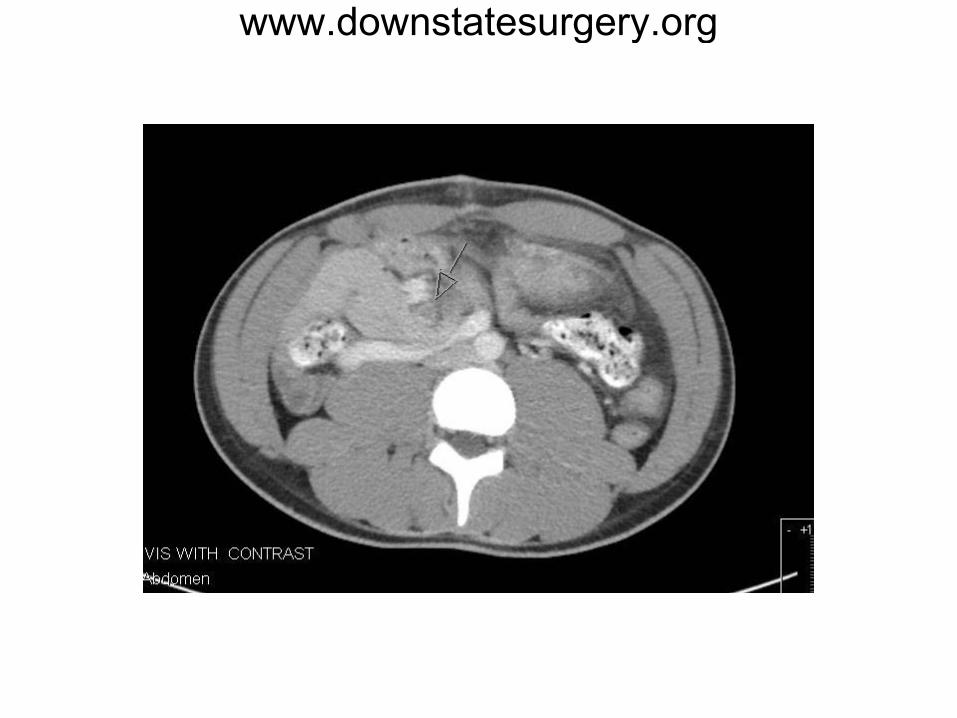
CT Scan
• Reversal of SMA and SMV • Colon on the left side, small bowel on the
right • Tubular fluid filled structure in anterior
abdomen just left to the midline with 2 appendicolith (~1.3cm)
DX: Appendicitisi with malrotation
www.downstatesurgery.org
Case Presentation
OR: - Exploratory laparotomy, appendectomy via midline epigastric incision Path: Mainly periappendicitis with fecolith. POD#1: + flatus, tolerated diet, D/C home
www.downstatesurgery.org

Case Presentation
POD #5: Pt presented to ED with persistent nausea and bilious vomiting x 3 days. Constipation since surgery. No fever, pain. PE: 98.6 127/83 98 98% + normal BS, well healed incision, soft nondistended nontender abd
www.downstatesurgery.org

Case Presentation
Laboratory Work
www.downstatesurgery.org

www.downstatesurgery.org

www.downstatesurgery.org

www.downstatesurgery.org

www.downstatesurgery.org
www.downstatesurgery.org

www.downstatesurgery.org

Case Presentation
CT scan: GI malrotation with stomach and proximal small bowel dilated – VOLVULUS NGT inserted with return of bilious content Resuscitated
www.downstatesurgery.org
Case Presentation
OR for Exploratory laparotomy, Ladd’s procedure via RUQ transverse incision 1.Entire small bowel eviscerated – dusky distended SB and congested mesentary 2.Root of the mesentary inspected – untwisted 180 degrees 3.Appendectomy site inspected 4.Adhesion bands lysed along the duodenum medially and laterally 5.Normal pink color of the small bowel noted 6.SB returned to the right side and colon to left side with mesentary opened down the midline
www.downstatesurgery.org

Case Presentation
POD #1-2: NPO, NGT, awaiting bowel function POD #3: + flatus, NGT discontinued POD #4: +BM and flatus, started diet POD #5: tolerated regular diet, discharged home
www.downstatesurgery.org

Questions?
www.downstatesurgery.org
Malrotation and Volvulus
Malrotation: abnormalities of intestinal position and attachment.
- nonrotation; incomplete rotation, reverse rotation
Volvulus: Twisting of bowel around the axis of the superior mesentary artery
www.downstatesurgery.org

Epidemiology Incidence: 1 out of 500 live births; also found in
0.2 – 1% of autopsies - many cases discovered during laparotomy or work up
for other entities
Symptomatic malrotation: 75-90% of cases occur <1 year of age, 50-64% <1 month, 25-40% within one week of life
Volvulus: 68-71% occur as neonates; 2:1 male to female ratio during 1st wk of life but equalizes after one year
www.downstatesurgery.org

Embryology
Stage I - 6th – 10th week of gestation - GI tract lengthens, leaves the abdominal cavity and herniates into umbilical cord - 90 degree counterclock rotation and return of bowel into abdominal cavity
Disruption in Stage I – Omphalocele
www.downstatesurgery.org
Embryology
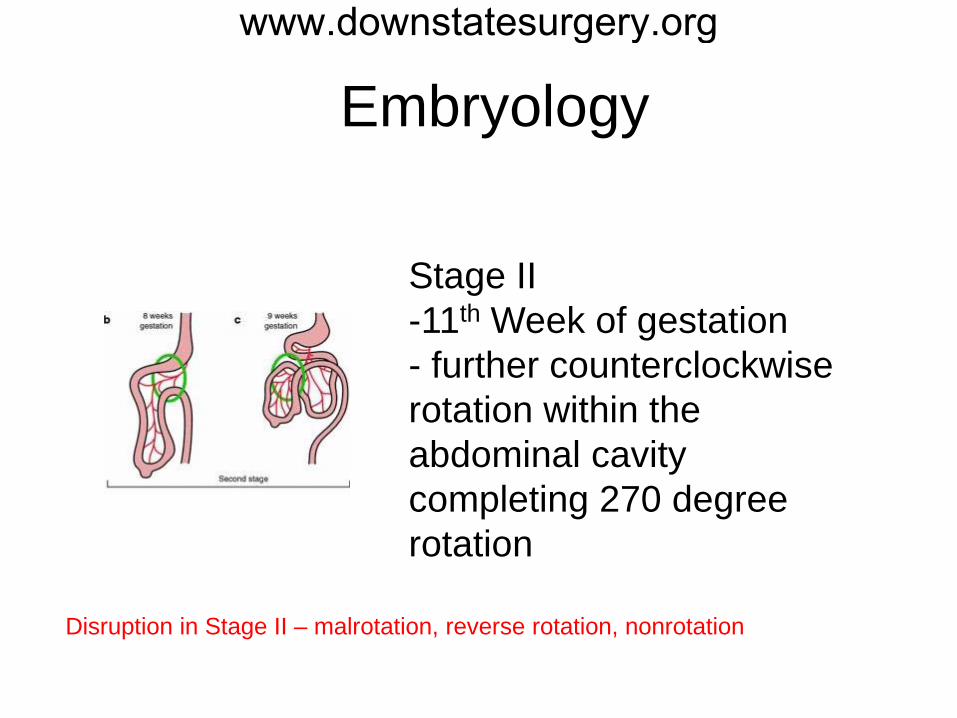
Stage II -11th Week of gestation - further counterclockwise rotation within the abdominal cavity completing 270 degree rotation
Disruption in Stage II – malrotation, reverse rotation, nonrotation
www.downstatesurgery.org
Embryology
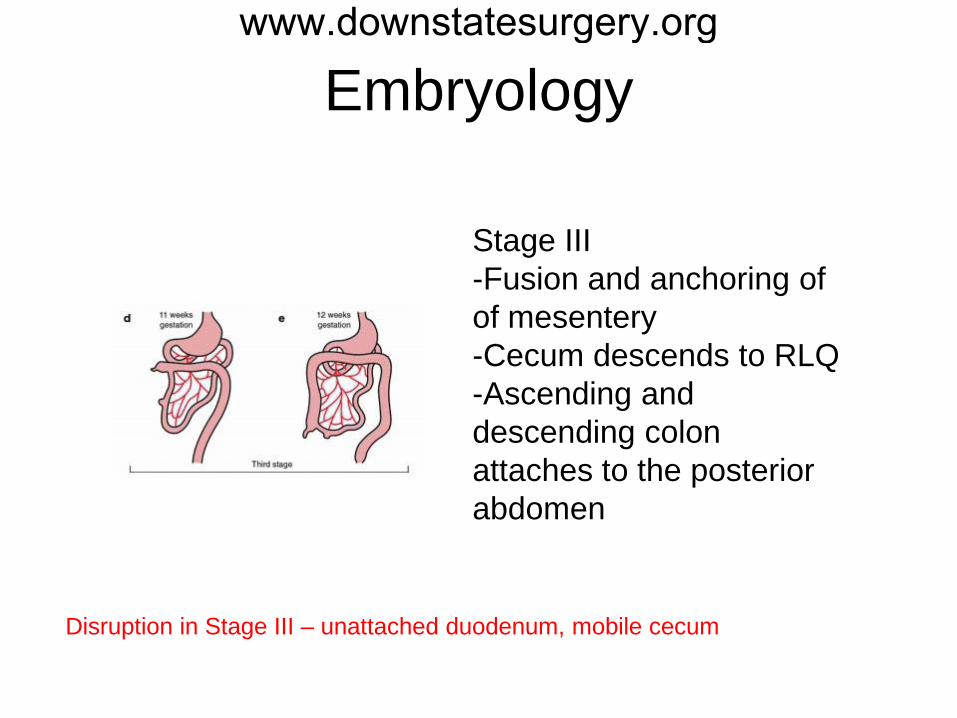
Stage III -Fusion and anchoring of of mesentery -Cecum descends to RLQ -Ascending and descending colon attaches to the posterior abdomen
Disruption in Stage III – unattached duodenum, mobile cecum
www.downstatesurgery.org
Symptoms and Signs
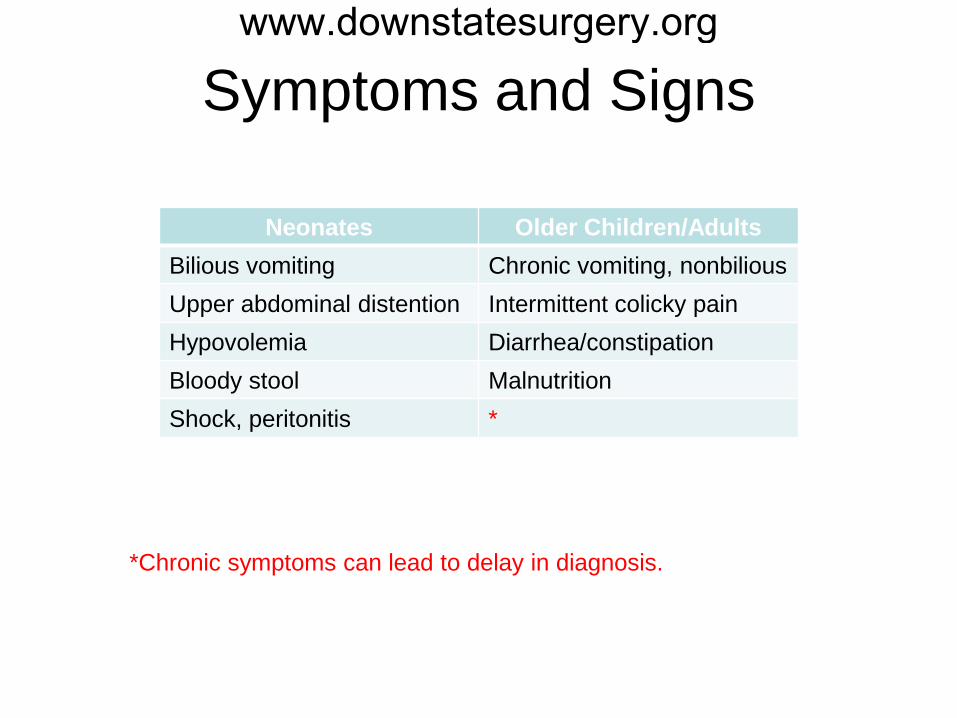
Neonates Older Children/Adults Bilious vomiting Chronic vomiting, nonbilious Upper abdominal distention Intermittent colicky pain Hypovolemia Diarrhea/constipation Bloody stool Malnutrition Shock, peritonitis *
*Chronic symptoms can lead to delay in diagnosis.
www.downstatesurgery.org

Diagnostic Tests
• Plain radiograph may or may not be helpful
• Upper GI series can delineate the course of duodenum and locate Ligament of Treitz in its abnormal position – Bird beak sign – Corkscrew sign – Abnormal duodenum shape with jejunum not
crossing midline
www.downstatesurgery.org
• Ultrasound is not very useful in setting of malrotation. However it can reveal abnormalities of mesenteric vasculature
• CT scans can demonstration presence of SBO, transition points, relationship of SMA and SMV, location of small bowel and colon, “WHIRLING SIGN”
Diagnostic Tests www.downstatesurgery.org

Imaging Tests
Birdbeak sign Corkscrew
WHIRL SIGN
www.downstatesurgery.org

Treatment
• Symptomatic patient regardless of age found to have malrotation must undergo Ladd’s procedure – Division of Ladd’s bands – Detorsioning of midgut volvulus – Appendectomy – Widening of the mesentery base
www.downstatesurgery.org

Treatment
• Asymptomatic, incidentally found malrotation is recommended to be corrected surgically. – Before advent of parenteral nutrition, mortality
of volvulus was 23-33%. – Currently, it ranges from 3% to 9%. – Risk of mortality increases 25x with presence
of necrotic bowel.
www.downstatesurgery.org
• There are no predictors for developing volvulus with ischemia and surgery remains to be the only solution as corrective measure.
• Although rare now, with advanced imaging, vague chronic symptoms in adults can lead to devastating ischemic bowel and death.
• Benefits and risks should be weighed individually.
Treatment www.downstatesurgery.org
Conclusions
• Understanding of embryology and anatomy is important in identifying malrotation.
• Symptomatic intestinal malrotation and volvulus is rare condition in adult population.
• High index of suspicion should be followed with prompt work-up and treatment.
• The goal is to prevent any non-reversible ischemic injury to the bowel.
www.downstatesurgery.org

References • Dassinger M, Smith S. Coran: Pediatric Surgery 7th Edition • Bernstein S, Russ P: Midgut Volvulus: A Rare Cause of Acute Abdomen
in an Adult Patient. Amer J of Radiology 1998, 171:639-641 • Powell D, Otherson B, et al: Malrotation of the Intestines in Children:
The Effect of Age on Presentation and Therapy. J of Pediatric Surg 1989, 24: 777-780
• Emanuwa O, Ayantunde A: Midgut Malrotation First Presenting as Acute Bowel Obstruction in Adulthood. World J of Emer Surg 2011, 6:22
• Gamblin T, Stephens E, et al: Adult Malrotation: A Case Report and Review of the Literature. Current Surgery 2003, 60:517-520
• Pickhardt P, Bhalla S: Intestinal Malrotation in Adolescents and Adults. Amer J of Radiology 2002, 179:1429-1435
• Parish A, Cuffari C: Intestinal Malrotation. www.eMedicine.com
www.downstatesurgery.org

QUESTIONS? www.downstatesurgery.org





![Sci Forschen Journal of Surgery: Open Access · 2019. 7. 17. · a barium enema and stated an incidence of intestinal malrotation of 0.19% [5]. ... Colon anomaly with no clear presence](https://img.pdfslide.net/doc/110x75/6128feca1e0aec1ea225c0ed/sci-forschen-journal-of-surgery-open-access-2019-7-17-a-barium-enema-and-stated.jpg)










![International Journal of Surgery Case Reports · are three abnormalities that can be found in a horseshoe kidney: ectopia, malrotation and vascular changes [14]. Graves defined three](https://img.pdfslide.net/doc/110x75/6099326dc9156b0a10725ec3/international-journal-of-surgery-case-reports-are-three-abnormalities-that-can-be.jpg)




![Disorders of intestinal rotation and fixation (‘‘malrotation’’)deepblue.lib.umich.edu/bitstream/handle/2027.42/46708/... · 2020. 2. 13. · consequences [4]. ‘‘Malrotation’’](https://img.pdfslide.net/doc/110x75/60afb5330f88520c4e13c968/disorders-of-intestinal-rotation-and-ixation-aamalrotationaa-2020-2.jpg)






