-
Management of Acute Myocarditis Ri
-
Outline of PresentationMedical TreatmentConventional
TreatmentImmuno-suppressantsImmuno-modulating therapyMechanical
Circulatory SupportPercutaneous cardiopulmonary supportVentricular
assist deviceHeart Transplantation
-
Medical Treatment A Clinical Trial of Immunosuppressive Therapy
for Myocarditis. NEJM 1995;333(5): 269~275 Etiology, Evaluation and
Management of Acute Myocarditis Cardiol. in Review 2001;9(2): 88~95
Antiinflammatory Therapy in Myocarditis Curr. Opin.Cardiol
2003;18:189~193
-
Conventional Treatment
-
Immuno-suppressantsStudy MethodsEnrollmentOnset of HF in 2yrs
without CAD or other significant causeLVEF < 45%Biopsy proved
lymphocytic myocarditisTherapyStepped regimen of conventional drugs
for HFPrednisone + azathioprine for 24 wksPrednisone + cyclosporin
for 24 wksEnd PointsPrimary: LV performance (LVEF, PCWP, LV
diameter)Secondary: survival
-
Distinct Form of Myocarditis
-
Immuno-suppressantsResultsImmunosuppressants did not have
benefit on the LV function or improve survivalIndependent
predictors of improvement in LV functionBetter base-line LV
ejection fractionLess intensive conventional therapy at
base-lineShorter duration of disease
-
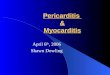
Immuno-suppressantsDiscussionDilemma: is myocarditis due to
immunity ?Stronger immune response associated with less severe
initial diseaseHigher cardiac IgG Ab better LVEFHigher level of NK
cells less intensive carePathogenesis of acute myocarditis
-
Pathogenesis of Acute Myocarditis
Circulation 1999; 99:1091~1100
-
Conclusion to immunosuppressants Prominent immunologic response
may be a benefit rather than a principal cause of
myocarditisRoutine use of immunosuppressants is not recommended for
patient with stable clinical courseHowever, aggressive
immunosuppressants for fulminant myocarditis and/or deterioration
clinical course is still controversial.Timing ?What can we do more
?
-
Immuno-modulating TherapyIVIGNo improvement in LV performance
Circulation 2001; 103:2254~2259Immuo-adsorption + sequential
IVIGDeplete a variety of circulating Ig and immune complexIg
substitutionSignificant improvement in LV function J Am Coll
Cardiol 2000; 35:1590~1598
-
Mechanical Circulatory Support Circulatory Support for Fulminant
Myocarditis: Consideration for implantation, weaning and
explantation Eur J Cardiothorac Surg.; 2003(24): 399~403 Fulminant
Myocarditis in Adults and children: bi-ventricular assist device
for recovery Eur J Cardiothorac Surg.; 2004(26): 1169~1173
-
Indication in Fulminant CasesLife saving approach in patients of
fulminant myocarditisConcerned questions:Timing of
implantationIntractable cardiogenic shockBefore multi-organ
failureDevice selectionPercutaneous cardiopulmonary support
(PCPS)Ventricular assist device (VAD)
-
ECMOAdvantagesEasy to implant and explant, lower costThe support
duration to recovery was shorterECMO vs. BiVAD: 5.5 3 ds vs. 10.2
6.1 dsTroponin level as a good indicator for recoveryCan be
switched to VAD at any timeDisadvantagesInadequate unloading of the
LV
-
Conclusion to MCSPatients surviving the acute phase crisis of
acute myocarditis have a favorable long-term survival rate and
LVEF, whether or not mechanical support is used.However, the
selection of MCS is still individualized.
-
Heart Transplantation
-
Timing and OutcomeTransplantation should be avoided in acute
phaseViral myocarditis: potential recovery by conventional
therapyAutoimmune: high incidence of recurrence Transplantation in
chronic stage (DCM)No significant difference in outcome compared
with other causes of HF