Embed Size (px)
Citation preview

8/30/2017
1
Management of AKIER, Hospital and office
MICHELLE SHIELDS, RN, MSN, CRNPPCNP 2017
< 15 Stage 5
15–29 Stage 4
30–59 Stage 3
60–89 Stage 2
> 90 Stage 1
The Prevalence of CKD in the General Population
5.9M
5.3M
0.3M
0.4M
7.6M
Levey et al. Ann Intern Med. 2003;139:137-147.
< 15 Stage 5
15–29 Stage 4
30–59 Stage 3
60–89 Stage 2
> 90 Stage 1
26 Million CKD Patients
5.9M
5.3M
0.3M
0.4M
7.6M
Coresh et al: JAMA Nov 7, 07; 298(17):2038-2047.
X
CKD Incidence
1 in 9 Adults
3 times that of cancer
600 times that of AIDS

8/30/2017
2
< 15 Stage 5
15–29 Stage 4
30–59 Stage 3
60–89 Stage 2
> 90 Stage 1
26 Million CKD PatientsX
CKD Incidence
15% of Adults
96% of stage 1-2 are not aware
48% of CKD stage 4 are not aware
X30
Centers for Disease Control and Prevention. Chronic Kidney Disease Surveillance System—United States.2017 website. http://www.cdc.gov/ckd
Kidney Failure Is a Rapidly Growing Problem
0
100
200
300
400
500
600
700
1984 1986 1988 1990 1992 1994 1996 1998 2000 2002 2004 2006 2008 2010
Num
ber
of P
atients
(in th
ousands)
372,407
661,330
172,667
98,953
Incidence
Prevalence
Adapted from: US Renal Data System 2000 Annual Data Report.
Year
Centers for Disease Control and Prevention. Chronic Kidney Disease Surveillance System—United States. 2017website. http://www.cdc.gov/ckd

8/30/2017
3
Centers for Disease Control and Prevention. Chronic Kidney Disease Surveillance System—United States. 2017website. http://www.cdc.gov/ckd
Centers for Disease Control and Prevention. Chronic Kidney Disease Surveillance System—United States. 2017website. http://www.cdc.gov/ckd
Centers for Disease Control and Prevention. Chronic Kidney Disease Surveillance System—United States. 2017website. http://www.cdc.gov/ckd

8/30/2017
4
Centers for Disease Control and Prevention. Chronic Kidney Disease Surveillance System—United States.website. http://www.cdc.gov/ckd
Cardiovascular Disease (CVD) MortalityGeneral Population versus ESRD Patients
Foley RN, Parfrey PS, Sarnak MJ. Am J Kidney Dis. 1998;32(suppl):S112-S119.
GP=General PopulationESRD=End-Stage Renal Disease
Annual CVD mortality (%)
Age (years)
0.001
0.01
0.1
1
10
100
25-34 35-44 45-54 55-64 65-74 75-84 >85
GP maleGP femaleGP blackGP white
Dialysis maleDialysis femaleDialysis blackDialysis white
Expected Remaining Lifetimes (Years)
0
5
10
15
20
25
30
35
Age
Years
50-54
General population End-stage renal disease
60-64
20.4
4.4
28.6
6.0
US Renal Data System (USRDS) 2006 Annual Data Report: Atlas of End-Stage Renal Disease in the United States, National Institutes of Health, National Institute of Diabetes and Digestive and Kidney Diseases, Bethesda, MD, 2006.

8/30/2017
5
Medicare costs are 2.7 times greater for CKD patients than for non-CKD patients
$6,060
$16,476
$62,676
$0
$10,000
$20,000
$30,000
$40,000
$50,000
$60,000
$70,000
Non-CKD CKD Dialysis
Hunsicker LG. J Am Soc Nephrol . 2004;15:1363-1374
Based on data from USRDS 2002; costs based on diagnostic codes obtained from billing data; patients> 67 years of age
An
nu
al M
edic
are
Co
st P
er P
atie
nt
($)
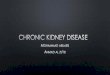
2016 Annual Data Report, Vol 2, ESRD, Ch 1 14
Data Source: Reference Table D1. Abbreviation: ESRD, end‐stage renal disease.
.
Figure 1.2 Trends in the annual number of ESRD incident cases (in thousands) by modality, in the U.S. population, 1996‐2014
Ishani A et al. J Am Soc Nephrol 2009
N= 233.803
Acute kidney injury increases risk of ESRD among elderly

8/30/2017
6
Acute Kidney Injury (AKI)
AKA: Acute renal failure, renal insufficiency Definition: Abrupt reversible decline in glomerular filtration rate (GFR) Demonstrated by increased metabolic waste products, ie blood
urea nitrogen (BUN) and creatinine
Definition of AKI
a sudden, sustained, and usuallyreversible decrease in the glomerularfiltration rate (GFR) occurring over aperiod of hours to days.
> 30 definitions used in published studies
KDIGO Classification of AKI
Stage Serum creatinine Urine output
1 1.5-1.9× baselineOR>0.3 mg/dL
<0.5 ml/kg/hr for 6-12 hrs
2 2-2.9× baseline<0.5 ml/kg/hr > 12 hrs
3 3 times baselineORincrease in Cr to ≥4.0 mg/dLOR Initiation of RRT
<0.3 ml/kg/hr > 24 hrsORAnuria > 12 hrs
KDIGO( Kidney Disease: Improving Global Outcomes)Clinical Practice Guideline for AKI. Kidney Int 2012

8/30/2017
7
Initial Evaluation of AKI
Evaluate for reversible causes: hypotension, volume depletion, obstruction
Evaluate for complications of AKI: hyperkalemia, acidosis, volume overload, hypocalcemia, hyperphosphatemia, anemia
Determine differential diagnosis of AKI: Prerenal, intrinsic damage, post renal etiology.
The kidney functions properly in patients with prerenal azotemia. True volume depletion can be treated with normal saline. Decreased effective arterial blood volume can be present in
CHF, Cirrhosis or nephrotic syndrome. Treatment should focus on the underlying disease.
Prerenal azotemia is the most common cause of acute kidney injury in the outpatient setting Look for patients with decreased PO, diarrhea, vomiting,
tachycardia, orthostasis…. Order: UA, Uosm, Una, Ucr, BMP, Uurea (if on diuretics)
Prerenal Azotemia
ATN - Acute Tubular Necrosis Usually occurs after an ischemic event or exposure to
nephrotoxic agents. Look for muddy brown casts and FeNa>2%
AIN - Acute Interstitial Nephritis Classic presentation is fever, rash, eosinophilia and Cr
bump 7-10 days after drug exposure. Urine may show leukocytes, leukocyte casts and
erythrocytes, cultures will be negative.
CIN - Contrast Induced Nephropathy Increased Cr of 0.5mg/dl or 25% 48hrs after contrast
administration.
Others – Glomerular Disease, Pigmented Nephropathy, Thrombotic Microangiopathy
Intrinsic Kidney Diseases

8/30/2017
8
Obstruction anywhere in the urinary tract Bladder outlet obstruction can be seen with bladder scan and
relieved with catheterization
Ureteral obstruction and hydronephrosis may be seen on ultrasound and noncontrast CT
Order: Order: UA, Uosm, Una, Ucr, BMP, Uurea (if on diuretics)
Patients often have a history of pelvic tumors, irradiation, congential abnormalities, kidney stones, genitourinary, procedures or surgeries, and prostatic enlargement.
Post renal Disease
Hou SH, Bushinsky DA, Wish JB. Am J Med 1983; 74: 243-8.Nash K, Hafeez A, Hou S. Am J Kidney Dis. 2002; 39: 930-6.
Kaufman J, Dhakal M, Patel B, Et al. Am J Kidney Dis 1991; 17: 191-8.
Etiology of AKI
0
10
20
30
40
50
60
70
80
Prerenal Intrarenal Obstruct Idiopath
Outpatient
Inpatient
ATN is the cause in more than 90%.
Sepsis is the leading cause of ATN

8/30/2017
9
Management of AKIImmediate Therapy
Volume status: Volume depletion:
Any patient with clinical history of volume loss, ie vomiting, hypotension, tachycardia or oliguria should be trialed on IVF.
Initial therapy crystalloid. Target fluid replacement to MAP, urine output or improved cardiac output if
invasive monitor is used. Bolus then maintenance fluid if tolerated. Closely monitor for signs of volume
overload.
Volume overload: From excessive correction of volume depletion or primary LV dysfunction, ie
Cardiorenal syndrome. Diuretics initial therapy, loop preferred as greater naturetic effect than thiazides.
Initial dose 40-80smg IV furosemide, if not responsive double the dose, add metolazone. If ineffective, acute dialytic therapy.
Management of AKIImmediate Therapy
Hyperkalemia Common and potentially life-threatening complication of AKI Stablize, translocate, Increase excretion If not responsive to medical therapy, dialyze
Acidosis: Both excretion of acid and regeneration of bicarbonate is impaired with decreased GFR. Other factors may increase acidosis including sepsis, trauma and multi organ failure with elevated lactic acidosis. Mild: oral bicarbonate replacement, Moderate: IVF with bicarbonate, Severe/refractory: dialysis.
Hypocalcemia: due to hyperphosphatemia, reduced 25D, elevated PTH. Calcium is protein bound, correct for hypoalbuminemia. If asymptomatic, initiate phosphate binders, vitamin D therapy. If symptomatic, IV calcium.
Management of AKI:
Nutrition: adjust TPN/protein intake Medication dosing: adjustment for eGFR to avoid under or over
dosing, timing for dialytic therapy, reassess dosing for renal recovery or dialysis modality)
Procedural considerations (prefer non-contrast CT, appropriate to delay contrast exposure, prophylaxis)

8/30/2017
10
Nephrotoxic Drug Exposure
Minimizing nephrotoxin Avoid Aminoglycosides, Amphotericin,
Bactrim, Vancomycin, NSAIDs, IV contrast, Fleet’s enemas
Renal dose medications – especially antibiotics and monitor level
Cautious use (metformin, long acting oral hypoglycemic agents, insulin, gemfibrozil and statins, neurotin, colchicine/allopurinol, morphine/codeine, lmwh)
Management of AKIIndications for dialysis
Fluid overload refractory to diuretics Hyperkalemia Metabolic acidosis; pH < 7.1 refractory to IV bicarbonate Signs of uremia such as pericarditis, neuropathy, or bleeding
disorders due to qualitative platelet dysfunction.
Case Study #1Evaluation of AKI in the ER.
89 y.o. female with history of DM, HTN, CHF recently with malaise, fever/chills, body aches, nausea and vomiting. Presents to ER for evaluation.
Home medications, ASA 81mg qd, lisinopril 10mg qd, spironolactone 25mg qd, HCTZ 25mg qd, lantus 24u qhs, Vit D 1000iu qd, naprosynprn body aches.
Physical exam: BP lying 102/64, HR 68, sitting 100/64, HR 72, standing 82/58, HR 110. Normocephalic, no JVD, lungs clear, cardiac exam with RRR, ii/vi murmur, abdomen softly distended, + 2 edema

8/30/2017
11
Case study #1
Labs: Sodium 148, K 5.4, Chloride 112, Co2 21, BUN 45, creatinine 1.2 UA benign. CXR no acute process A&P? D/Dx: 1. Viral illness 2. AKI?
Creatinine 1.2
Age/race/sex 32 AA male 54 AA female 68 w male 89 w femaleCreatinine 1.2 1.2 1.2 1.2GFR 90 ml/min 60 ml/min 64 ml/min 45 ml/min
Date 8/1/17 2/1/17 8/4/16 2/4/16Creatinine 1.2 mg/dL 0.7 mg/dL 0.8 mg/dL 0.7 mg/dLGFR 45 ml/min 83ml/min 71 ml/min 83ml/min

8/30/2017
12
Case Study #1Evaluation of AKI in the ER.
89 y.o. female with history of DM, HTN, CHF recently with malaise, fever/chills, body aches, nausea and vomiting. Presents to ER for evaluation.
Home medications, ASA 81mg qd, lisinopril 10mg qd, spironolactone 25mg qd, HCTZ 25mg qd, lantus 24u qhs, Vit D 1000iu qd, naprosynprn body aches.
Physical exam: BP lying 102/64, HR 68, sitting 100/64, HR 72, standing 82/58, HR 110. Normocephalic, no JVD, lungs clear, cardiac exam with RRR, ii/vi murmur, abdomen softly distended, + 2 edema
Differential Diagnosis
Prerenal: Dehydrated on diuretics, hypotensive, tachycardic, lisinopril
Intrinsic: Naprosyn, hypotension could lead to ATN Post renal: No clear urinary symptoms/abnormalities on exam
Treatment Plan
NSS at 125ml/hr Stop lisinopril, HCTZ, spironolactone, Naprosyn. If BP stabilizes, Discharge home with follow up/labs in 2-3 days with
PCP. Teach patient, sick day rule of holding lisinopril/HCTZ and
spironolactone if not taking in adequate fluids.

8/30/2017
13
Case Study #2 ER evaluation of AKI
69 yo AA male presents to the emergency room with dysuria. Noted hesitancy starting 3-6 months ago, difficulty initiating his urine stream, now decreased urine output over the last few days and flank pain.
Medications: ASA, levocetirizine, multivitamin PE: no acute findings other than left CVA tenderness and slightly
fullness over palpation of the bladder. Labs: BUN 26, creatinine 1.4, GFR 64 ml/min.
Differential diagnosis
Prerenal: normotensive Intrinsic: no new medications/UA bland Post renal: s/sx of bladder tenderness, CVA tenderness
On levocetirizine which causes urine retention
Case Study #2
Unable to obtain Renal imaging Admit for observation
Need renal imaging
Evaluate urine C&S, Initiate antibiotics if needed
Insert foley catheter, observe for improvement in renal function and possibility of post-obstructive diuresis.

8/30/2017
14
Case Study #3 Hospital Evaluation of AKI
41 yo obese female with history of DM type 2 for 10 years, HTN, one previous episode of AKI 2 years ago during hospitalization for pneumonia presents with worsening shortness of breath. She had seen PCP 5 days ago with complaints of cough, productive of yellow secretions, fevers, started on trimethoprim sulfa DS bid. Initial BP 72/58, HR 118, RR 32, SpO2 81% on room air
Initial Therpy? NSS wide, ABG, CXR
CXR
ABG: pH 7.18, Co2 68, O2 68, HCO3 18 Intubate Vitals: BP 82/68, HR 110, RR 12/12. start norepinephrine gtt Change IV include bicarbonate:
Sterile water with 3 amps sodium bicarbonate
¼ NSS with 2 amps of sodium bicarbonate
½ NSS with 1 amp of sodium bicarbonate
Labs

8/30/2017
15
Laboratory Evaluation
CBC/diff, CMP, lactic acid, UA, Urine and blood cultures Results:
Sodium: 154 Potassium: 5.4 Chloride: 113 Co2: 18 BUN: 112 Creatinine: 5.2 BUN/creat ratio =21 (> 20 prerenal) Lactic Acid 4.8 CPK 18,324
Evaluation of AKI
Prerenal: hypotensive, hypovolemic, sepsis Intrinsic: Rhabdomylosis, interstitial nephritis
UA: wbc 100, -leukocytes, -nitrate, WBC casts, Culture negative
Post renal: Obstruction Renal ultrasound with PVR:
R kidney 9.8cm, L kidney 8.9cm, increased cortical echogenicity, no bladder wall thickening, PVR 33cc.
-5 liters positive fluid balance/24 hours. CXR with pulmonary edema-IV furosemide initiated,
40mg IV, oliguric:80mg IV, oliguric,IV gtt at 10mg/hr initiated, nonoliguric,
CXR remains with pulmonary edema, by day 4, unable to wean from vent, initiate dialysis.
Day Day 1 Day 2 Day 3 Day 4BUN 112 106 102 108Creatinine 5.4 5.1 6.4 7.2Urine Output 468cc/24 hr 696cc/24 hr 1876 cc/24 hr 1272cc/24 hr

8/30/2017
16
-5 liters positive fluid balance/24 hours. CXR with pulmonary edema-IV furosemide initiated, 40mg IV, oliguric, 80mg IV, oliguric, IV gtt at 10mg/hr initiated, nonoliguric, CXR remains with pulmonary edema, by day 4, unable to wean from vent,
initiate dialysis.
Day Day 1 Day 2 Day 3 Day 4BUN 112 106 102 108Creatinine 5.4 5.1 6.4 7.2Urine Output 468cc/24 hr 696cc/24 hr 1876 cc/24 hr 1272cc/24 hr
Case #4, Evaluation of AKI in the Hospital
A 72 year old male with DM, HTN, hx of CAD with LAD stent placed in 2011, presents to the ER with left sided chest pain
Creatinine 2.2 (GFR 29 ml/min) baseline Creat 1.5 (GFR 39 ml/min) Plan for cardiac cath
Contrast induced nephropathy CIN - Contrast Induced Nephropathy
At risk: Existing CKD
289 patients with eGFR 30-59%, post exposure 4.2% developed AKI (Nijssen, 2017)
124 patients with creatinine >3, eGFR <30, 31% developed AKI (Rihal, 2002) type and amount of contrast; less if <125ml of low osmolar contrast Diabetic nephropathy; 250 pts with DN/creat >1.5, 33% AKI (Rudnick,
1995) Reduced renal perfusion: heart failure, hypotension, ACE, NSAID
Increased Cr of 0.5mg/dl or 25% 48hrs after contrast administration. Most patients are nonoliguic Urine studies benign vs muddy/granular casts associated with ATN Creatinine starts to decline 3-7days

8/30/2017
17
Prevention of CIN hold NSAIDs, metformin and diuretics for 24-48hrs. No evidence of holding
ACE beneficial Acetylcysteine — 1200 mg orally twice daily the day before and the day of
the procedure. Fluid administration — For all at-risk patients undergoing procedures involving
intra-arterial contrast administration, if there are no contraindications to volume expansion, we administer intravenous isotonic saline prior to and continued for several hours after contrast administration. No benefit to bicarbonate containing fluids over NSS.
●Outpatients ─ 3 mL/kg over one hour preprocedure and 1 to 1.5 mL/kg/hour during and for four to six hours postprocedure, with administration of at least 6 mL/kg postprocedure.
●Inpatients ─ 1 mL/kg/hour for 6 to 12 hours preprocedure, intraprocedure, and for 6 to 12 hours postprocedure.
Uptodate, 2017; AKI
Evaluation of AKI in the office
Acute, Subacute or Chronic Kidney Disease (CKD)? AKI develops in hours to days after insult. KDIGO stages 1-3 as
outlined earlier. Subacute defines a presentation that develops more slowly than
AKI, but results in elevated creatinine in less than three months. CKD is defined as an elevation in creatinine over more than three
months. NKF stages 1-5D as evidenced by reduced GFR/presence of kidney damage, ie albuminuria, abnormal findings on renal imaging present for more than three months.

8/30/2017
18
Evaluation of AKI in the office
Evaluation begins with careful history and physical exam Evaluation of lab results including duration of elevated creatinine,
assessment of GFR Careful examination of the urine with qualitative analysis (UA) and
microscopic exam Radiographic imaging Serologic testing and tissue diagnosis with kidney biopsy if indicated.
Evaluation of AKI in the office
If lab values not available for comparison Recent onset of symptoms or signs, ie sudden onset of anasarca or
discolored urine
Marked oliguria (urine output < 500cc/24 hr) or anuria (urine output < 100cc/24 hr)
Daily progressive increase in creatinine if serial labs drawn
Imaging showing small kidneys and increased echogenicity of renal parenchyma more likely CKD, normal sized kidneys with normal echogenicity less likely CKD but does NOT exclude.
Radiographic evidence of renal osteodystrophy.
Hou SH, Bushinsky DA, Wish JB. Am J Med 1983; 74: 243-8.Nash K, Hafeez A, Hou S. Am J Kidney Dis. 2002; 39: 930-6.
Kaufman J, Dhakal M, Patel B, Et al. Am J Kidney Dis 1991; 17: 191-8.

8/30/2017
19
Evalutation of Etiology: Office
Prerenal: Causes:
Overdiuresis, decreased oral intake, diarrhea, unreplensished insensible losses
decompensated heart failure/cardiorenal syndrome,
decompensated liver failure/hepatorenal syndrome,
NSAID causing afferent arteriole vasoconstriction, efferent vasoconstriction by renin-angiotensin system blockade, ACE-I, ARB
Evaluation of Etiology: office
Intrinsic: Renovascular: Atheroembolic disease, renal infarction, renal artery
aneurysm microangiopathy (hemolytic anemia/thrombocytopenic purpura TTP/hemolytic uremic syndrome HUS) scleroderma, malignant hypertension
Glomerular disease: Nephritic variable proteinuria, dysmorphic RBC, RBC casts
Nephrotic >3gm, active/inactive urine sediment
Interstitial: drug induced interstitial nephritis (WBC casts), cast nephropothy (multiple myloma) tumor lysis syndrome, acute urate nephropathy
Evaluation of etiology: office
Postrenal: Without history of CKD, reduced GFR suggests bilateral obstruction or
unilateral with known solitary kidney.
Stone, prostate or metastic obstruction most likely causes

8/30/2017
20
Clinical manifestations
Signs/symptoms related to reduced kidney function: edema, hypertension, decreased urine output. Weakness, fatigue, decreased appetite, dysguesia, mental status changes, seizures.
Symptoms often mild, severe symptoms as CKD progresses. Systemic symptoms such as fever, arthralgias and/or pulmonary
lesions suggestive of systemic disease such as vasculitis Livedo reticularis and splinter hemorrhages suggest atheroembolic
disease. Unilateral flank pain suggest obstruction, renal infarction or infection.
Initial evaluationMild injury: (<0.5 mg/dL above baseline creatinine)
Evaluate volume status, discontinue diuretics
repeat in 1-2 weeks, add UA, microalbumin/protein to creatinine ratio
evaluate for offending agents/etiology. Ie, NSAIDS, ACE-I, ARB, diuretics, PPI, hypotension, obstruction.
Initial Evaluation:Moderate injury (>0.5mg/dL)
Obtain UA, microscopy, renal US with PVR, microalbumin/creatinine ratio
Evaluate for Glomeruleronephritis, interstitial nephritis, ATN If no clear etiology, elevated creatinine, anemia, hypercalcemia,
SPEP, UPEP with immunofixation r/o myeloma Continued elevation of creatinine, no clear etiology, nephrology
evaluation, consider renal biopsy

8/30/2017
21
Case Study #5 68 yo male who presents to office with right knee pain after
completing yard work at home. Not worse in mornings, Increased pain with ambulation/stairs.
No clear effusion, edema or muscle abnormality on exam. Prescribed naproxyn 500mg twice daily. He returns with fatigue and weakness 2 weeks later. Labs:
Sodium 143 Co2 21
Potassium 5.6 BUN 31
Chloride 110 Creatinine 1.9
Labs: present, last office visit
Date 8/25/17 3/1/17BUN 31 23Creatinine 1.9 0.9GFR 32 ml/min 54 ml/mi
Medications: ASA, lisinopril, metoprolol, metformin, omeprazole, HCTZ
PE: Wt up 3 pounds, BP 110/70, HR 54Normocephalic, dry mucous membranes, no JVD, lungs clear to auscultation, S1, S2 reg, abdomen soft, trace edema.

8/30/2017
22
Differential Diagnosis
Prerenal: volume depleted with low BP on diuretic decreased cardiac output with bradycardia Naprosyn High risk for AKI given Diabetes, NSAIDS, ACE-I, diuretic
Intrinsic: NSAIDS Post renal: No s/sx urinary tract obstruction
Discontinue Naprosyn, HCTZ, ACE-I Repeat labs 2 weeks, consider restarting ACE-I. If no improvement, consider d/c omeprazole
Case study #6
87 year old presents to office for q 6 month appointment. Usual state of health, no change in medications, no illness, no
hospitalizations Medications: Lantus, glipizide, omeprazole, Lasix 20 qod, ASA 81,
metoprolol, levothyroxine Labs:
Sodium 148 Co2 18 Phos 5.2 Potassium 3.8 BUN 87 Ca 10.8
Chloride 108 Creatinine 2.6 GFR 16ml/min UA: sp grav 1.020, clear, no WBC, no Blood, no RBC, no Leuk, no nitrite, no bacteria, no
protein
cbc: wbc 4.5, rbc 2.1, hgb 8.4, hct 25
AKI evaluation
Prerenal: On diuretics
BUN/Creatinine ratio > 20
Intrinsic: On omeprazole, no new medications, UA bland
Post renal: Renal ultrasound without hydro, increased cortical echogenicity. R kidney 9.2cm, L kidney 10.3, no calculi

8/30/2017
23
Date 8/23/17 8/3/17 7/21/17 3/1/17 3/1/16BUN 48 56 87 23 25Creat 2.4 2.0 2.6 1.3 0.9GFR 17 22 16 37 57
Treatment Plan
Hold omeprazole, consider H2 Blocker Continue diuretics SPEP/UPEP with immunofixation Urine microscopy Refer to Nephrology
When to refer to Nephrology?
eGFR < 60 ml/min/1.73 m Multiple Risk Factors Heavy or Increasing proteinuria Uncontrolled hypertension Rapid progression or Acute Renal Failure
Target decline in GFR < 4 ml/min/1.73 m per year1

8/30/2017
24
Goals of Management in CKD Early identification and management of co-
morbid conditions. Early recognition of kidney disease Early referral to nephrology Early management of complications of CKD Empower patients through education to make
informed decisions in regards to their disease process, ability to impact disease progression and dialysis modality choice
Patient Education in CKD Education begins in primary care Continues through referral to Nephrology CKD Stage 1-3: CKD, risk factor reduction, co-
morbid disease management, CKD progression CKD Stage 4-5: Complications of CKD,
Signs/symptom management, Transplant, Dialysis Options Education, Fistula First/Vein preservation
RD, RN, NP, PA-C, MD and all staff empower patient to make a difference in the progression of their CKD.


![Simple Algorithm of Arterial Blood Gas Analysis to Ensure ... · a. acidosis→ hyperkalemia b. alkalosis→ hypokalemia Base excess & base deficit [9,10] In human physiology base](https://img.pdfslide.net/doc/110x75/5e68d1f9a3c8150f0033b9c4/simple-algorithm-of-arterial-blood-gas-analysis-to-ensure-a-acidosisa-hyperkalemia.jpg)