Embed Size (px)
Citation preview
PATHOLOGY
Rec
Fac
De
Bas
Tur
Management of Bisphosphonate-RelatedOsteonecrosis of the JawWith a Platelet-Rich
Fibrin Membrane: Technical Report
eived
ulty of
*Fellow
yProfesAddres
partme
kent U
kiye; e
Sıdıka Sinem Soydan, DDS, PhD,* and Sina Uckan, DDS, PhDy
Bisphosphonate-related osteonecrosis of the jaw (BRONJ) is a challenging complication resulting from the
long-term application of bisphosphonates. In most cases, BRONJ occurs after a surgical procedure involv-
ing the jawbone. Currently, the management of BRONJ remains controversial, and there is no definitive
treatment other than palliative methods. Platelet-rich fibrin (PRF) represents a relatively new biotechnol-
ogy for the stimulation and acceleration of tissue healing and bone regeneration. This technical note
describes the total closure of moderate bone exposure in persistent BRONJ in 2 weeks with a double-layerPRF membrane. PRF may stimulate gingival healing and act as a barrier membrane between the alveolar
bone and the oral cavity. PRF may offer a fast, easy, and effective alternative method for the closure of
bone exposure in BRONJ.
� 2013 American Association of Oral and Maxillofacial Surgeons
J Oral Maxillofac Surg -:1-5, 2013
Bisphosphonate-related osteonecrosis of the jaw
(BRONJ) is characterized by exposed necrotic bone,
which can be accompanied by pain, swelling, pares-
thesia, suppuration, soft tissue ulceration, and intra-and extraoral sinus tracts.1,2 The incidence of BRONJ
is higher with bisphosphonates (BPs) administered
monthly through a parenteral route than with oral
BPs taken weekly. Most BRONJ cases occur after
surgical procedures of oral tissues. However, 30% of
cases occur spontaneously.3 Although the reported
frequency of BRONJ is low, it causes complications
in dental and oral and maxillofacial surgical treatmentsof patients receiving BPs. Themost effective treatment
for BRONJ is still controversial and a challenging issue
for oral and maxillofacial surgeons.
Although antiresorptive therapies other than BPs
and receptor activator of nuclear factor-kB ligand in-
hibitor therapies are claimed to cause osteonecrosis
of the jaws, BPs are responsible for most of the con-
cern. Themost accepted pathologic etiology of BRONJis oversuppression of bone turnover and inhibition of
angiogenesis owing to systematic usage of BPs.2,4,5
from the Department of Oral and Maxillofacial Surgery,
Dentistry, Baskent University, Ankara, Turkey.
.
sor.
s correspondence and reprint requests to Dr Soydan:
nt of Oral and Maxillofacial Surgery, Faculty of Dentistry,
niversity, 11. Sokak no 26 Bahcelievler, Cankaya, Ankara,
-mail: [email protected]
1
Despite BPs having a specific effect on osteoclasts
and a great affinity to bone, the loss of oral mucosa
in almost every BRONJ case raises the question of
whether they affect oral soft tissue.Several studies have examined whether BPs have an
adverse effect on oral epithelial and mucosal tissues.6-10
The results of these studies have been consistent,
showing that nitrogen-containing BPs decrease oral
epithelial cell migration, promote apoptosis, disturb
cell viability, and impede oral mucosa wound healing.
Platelet-rich fibrin (PRF) is a second-generation
platelet concentrate (natural autologous fibrin matrix)that was first described by Choukroun et al11 in 2000.
It regulates inflammation and stimulates chemotactic
factors involved in the immune response.12 PRF con-
tains a substantial quantity of fibrins, platelets, and
leukocytes. It secretes 3 proinflammatory cytokines
(interleukin-1b, interleukin-6, and tumor necrosis fac-
tor-a), an anti-inflammatory cytokine (interleukin-4),
and a key promoter of angiogenesis (vascular endothe-lial growth factor).13 PRF also accelerates angiogene-
sis, the multiplication of fibroblasts and osteoblasts,
Received June 24 2013
Accepted July 23 2013
� 2013 American Association of Oral and Maxillofacial Surgeons
0278-2391/13/00938-5$36.00/0
http://dx.doi.org/10.1016/j.joms.2013.07.027
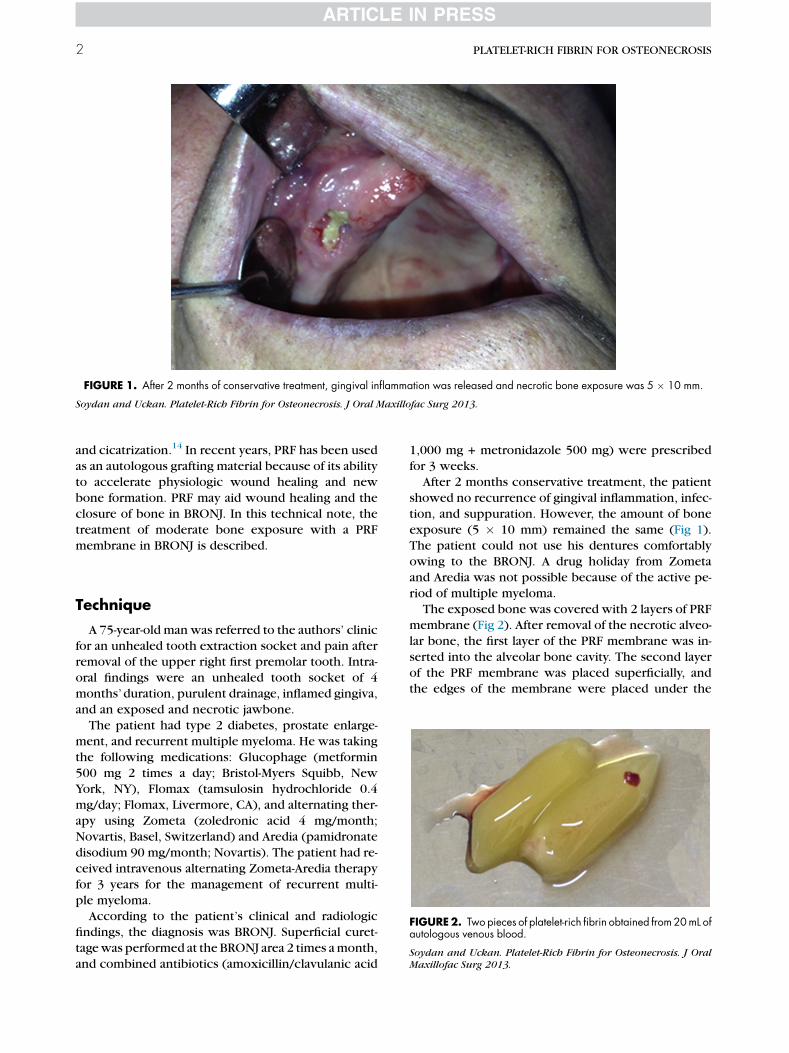
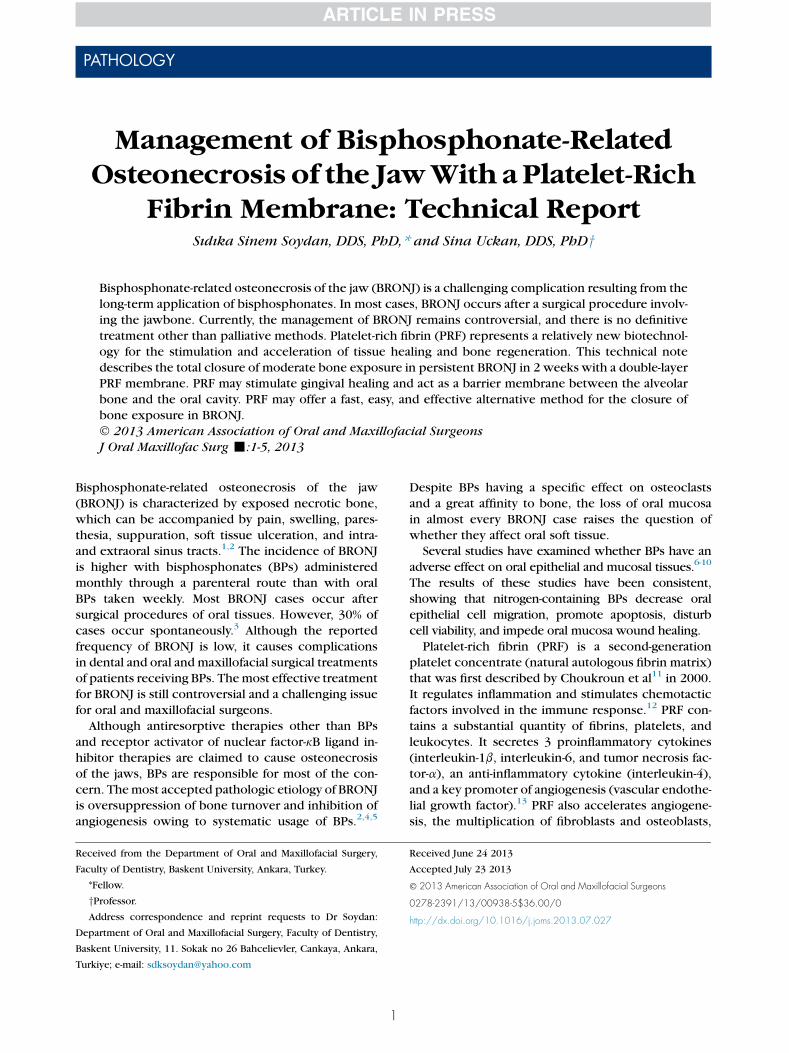
FIGURE 1. After 2 months of conservative treatment, gingival inflammation was released and necrotic bone exposure was 5 � 10 mm.
Soydan and Uckan. Platelet-Rich Fibrin for Osteonecrosis. J Oral Maxillofac Surg 2013.
2 PLATELET-RICH FIBRIN FOR OSTEONECROSIS
and cicatrization.14 In recent years, PRF has been used
as an autologous grafting material because of its ability
to accelerate physiologic wound healing and new
bone formation. PRF may aid wound healing and the
closure of bone in BRONJ. In this technical note, the
treatment of moderate bone exposure with a PRF
membrane in BRONJ is described.
FIGURE2. Two pieces of platelet-rich fibrin obtained from20mL ofautologous venous blood.
Soydan and Uckan. Platelet-Rich Fibrin for Osteonecrosis. J OralMaxillofac Surg 2013.
Technique
A 75-year-old man was referred to the authors’ clinic
for an unhealed tooth extraction socket and pain afterremoval of the upper right first premolar tooth. Intra-
oral findings were an unhealed tooth socket of 4
months’duration, purulent drainage, inflamed gingiva,
and an exposed and necrotic jawbone.
The patient had type 2 diabetes, prostate enlarge-
ment, and recurrent multiple myeloma. He was taking
the following medications: Glucophage (metformin
500 mg 2 times a day; Bristol-Myers Squibb, NewYork, NY), Flomax (tamsulosin hydrochloride 0.4
mg/day; Flomax, Livermore, CA), and alternating ther-
apy using Zometa (zoledronic acid 4 mg/month;
Novartis, Basel, Switzerland) and Aredia (pamidronate
disodium 90 mg/month; Novartis). The patient had re-
ceived intravenous alternating Zometa-Aredia therapy
for 3 years for the management of recurrent multi-
ple myeloma.According to the patient’s clinical and radiologic
findings, the diagnosis was BRONJ. Superficial curet-
tagewas performed at the BRONJ area 2 times amonth,
and combined antibiotics (amoxicillin/clavulanic acid
1,000 mg + metronidazole 500 mg) were prescribed
for 3 weeks.
After 2 months conservative treatment, the patient
showed no recurrence of gingival inflammation, infec-
tion, and suppuration. However, the amount of bone
exposure (5 � 10 mm) remained the same (Fig 1).
The patient could not use his dentures comfortablyowing to the BRONJ. A drug holiday from Zometa
and Aredia was not possible because of the active pe-
riod of multiple myeloma.
The exposed bone was covered with 2 layers of PRF
membrane (Fig 2). After removal of the necrotic alveo-
lar bone, the first layer of the PRF membrane was in-
serted into the alveolar bone cavity. The second layer
of the PRF membrane was placed superficially, andthe edges of the membrane were placed under the
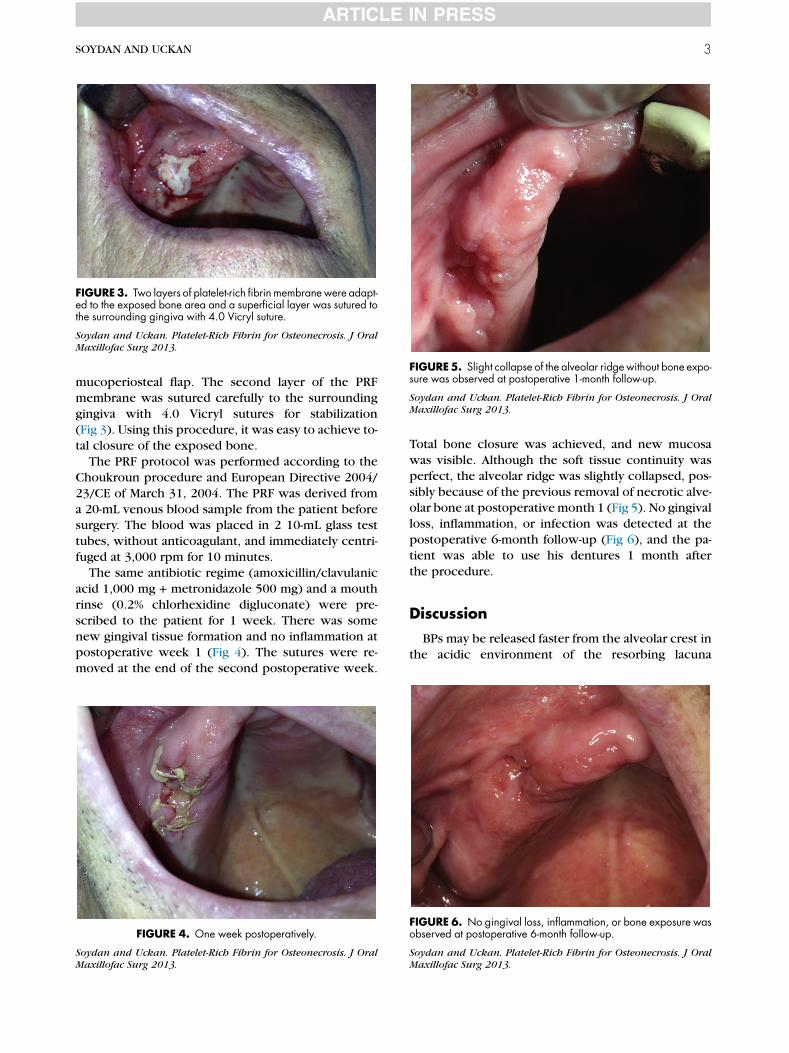
FIGURE5. Slight collapse of the alveolar ridge without bone expo-sure was observed at postoperative 1-month follow-up.
Soydan and Uckan. Platelet-Rich Fibrin for Osteonecrosis. J OralMaxillofac Surg 2013.
FIGURE3. Two layers of platelet-rich fibrin membrane were adapt-ed to the exposed bone area and a superficial layer was sutured tothe surrounding gingiva with 4.0 Vicryl suture.
Soydan and Uckan. Platelet-Rich Fibrin for Osteonecrosis. J OralMaxillofac Surg 2013.
SOYDAN AND UCKAN 3
mucoperiosteal flap. The second layer of the PRFmembrane was sutured carefully to the surrounding
gingiva with 4.0 Vicryl sutures for stabilization
(Fig 3). Using this procedure, it was easy to achieve to-
tal closure of the exposed bone.
The PRF protocol was performed according to the
Choukroun procedure and European Directive 2004/
23/CE of March 31, 2004. The PRF was derived from
a 20-mL venous blood sample from the patient beforesurgery. The blood was placed in 2 10-mL glass test
tubes, without anticoagulant, and immediately centri-
fuged at 3,000 rpm for 10 minutes.
The same antibiotic regime (amoxicillin/clavulanic
acid 1,000 mg + metronidazole 500 mg) and a mouth
rinse (0.2% chlorhexidine digluconate) were pre-
scribed to the patient for 1 week. There was some
new gingival tissue formation and no inflammation atpostoperative week 1 (Fig 4). The sutures were re-
moved at the end of the second postoperative week.
FIGURE 4. One week postoperatively.
Soydan and Uckan. Platelet-Rich Fibrin for Osteonecrosis. J OralMaxillofac Surg 2013.
Total bone closure was achieved, and new mucosa
was visible. Although the soft tissue continuity was
perfect, the alveolar ridge was slightly collapsed, pos-
sibly because of the previous removal of necrotic alve-olar bone at postoperativemonth 1 (Fig 5). No gingival
loss, inflammation, or infection was detected at the
postoperative 6-month follow-up (Fig 6), and the pa-
tient was able to use his dentures 1 month after
the procedure.
Discussion
BPs may be released faster from the alveolar crest in
the acidic environment of the resorbing lacuna
FIGURE 6. No gingival loss, inflammation, or bone exposure wasobserved at postoperative 6-month follow-up.
Soydan and Uckan. Platelet-Rich Fibrin for Osteonecrosis. J OralMaxillofac Surg 2013.

4 PLATELET-RICH FIBRIN FOR OSTEONECROSIS
produced by osteoclasts, resulting in locally high con-
centrations of BPs. The high concentration of BPs after
invasive dental surgical procedures could affect cells
other than osteoclasts in the microenvironment,
such as osteoblasts, endothelium cells, fibroblasts,
and keratinocytes.15
Although BP levels within tooth extraction sites
have not been quantified, Landesberg et al7 foundthat their proliferation in the oral epithelium was in-
hibited at pamidronate concentrations above 0.1
mmol/L in vitro. Sheper et al9 reported that direct con-
tact of clinically relevant concentrations of zoledro-
nate with epithelial and fibroblast cells induced
apoptosis, potentially resulting in BRONJ.
Epithelialization is an essential step in the manage-
ment of BRONJ because alveolar bone exposure inBRONJ exposes the bone to the unique infectious mi-
croenvironment of the oral cavity. A biofilm forms on
the exposed bone surface, and actinomyces facilitate
the adherence of other microflora, which results in
a heterogeneous population of bacteria primed for
the development of persistent infection.16 Infection
contributes to the pathophysiology of BRONJ by en-
hancing osteoclast-independent bone resorption.17
The elimination of dental plaque,which contains a sub-
stantial quantity of oral bacteria, with superficial curet-
tage, combined with antibiotic therapy, ameliorates
BRONJ-related symptoms and aids bone healing.18
In the presented case, a protocol comprising 2
months conservative treatment was applied for the
management of suppuration, infection, and gingival
ulceration.Although the conservative treatment resolved
the patient’s complaints, additional treatment was
needed to manage the prolonged bone exposure,
which showed no improvement at the 2-month
follow-up. There was insufficient surrounding gingi-
val tissue for tension-free closure of the exposed
area. In addition, it is known that coercive closure
of the bone results in increased bone exposure inBRONJ cases. Therefore, the bone was closed with
2 layers of PRF membrane.
Someprevious studies have reported that a combina-
tion of necrotic bone curettage and platelet-rich
plasma (PRP) seems to be promising for the treatment
of refractory BRONJ.19,20 PRP can enhance wound
healing and bone maturation. However, there is no
current consensus on whether it promotes softtissue healing in BRONJ cases.
PRP is used as an adjunct in a gel formulation, which
is formed by mixing (derived from the centrifugation
of autologous whole blood) bovine thrombin concen-
trate and calcium chloride. PRF does not require het-
erogeneous agents, and it can be used as a graft
material or barrier membrane. Therefore, the produc-
ing and application procedures with PRF are not as
complicated as those with PRP. PRF also contains
more growth factors (7 times higher) than PRP.21
Pripatnanont et al22 found that PRF was composed
of densely thick fibrin networks, with activated plate-
lets meshed among the fibrins. These dense fibrins
provide a natural matrix scaffold for the storage and at-
tachment of tissue cells and the stimulation of angio-
genesis. In addition to the matrix scaffold, plateletsprovide and sustain the release of growth factors in
the wound area.14 Many growth factors, such as
platelet-derived growth factor and transforming
growth factor-b, are released by PRF.23 A recent study
has reported the slow release of key growth factors by
PRF, with the growth factors released for at least 1
week and up to 28 days.24 Therefore, PRF could stim-
ulate the release of growth factors for a significant timeduring wound healing.
With PRF, fibrin membranes enriched with plate-
lets and growth factors can be obtained from
anticoagulant-free blood.12 The PRF membrane has
a similar network to fibrin and leads to more efficient
cell migration and proliferation and thus cicatrization.
Recent studies have described the ability of PRF to in-
crease cell proliferation in rat osteoblasts, human os-teoblasts, human periodontal ligament fibroblasts,
and human pulp fibroblasts by upregulating osteopro-
tegerin and alkaline phosphatase.25-28 PRF also has
been reported to stimulate the proliferation of
gingival fibroblasts and to accelerate soft tissue
healing. However, neither PRF nor PRF membranes
have been used in the treatment of BRONJ.
PRF membranes are an easy, cheap, and rapid alter-native treatment approach for the closure of bone ex-
posure in BRONJ. PRF promotes gingival healing and
acts as a barrier membrane between the alveolar
bone and the oral cavity. More comprehensive studies
are needed to understand the physiologic and histo-
logic efficiency of PRF membranes with regard to
soft tissue healing.
References
1. Marx RE: Pamidronate (Aredia) and zoledronate (Zometa) in-duced avascular necrosis of the jaws: A growing epidemic. JOral Maxillofac Surg 61:1115, 2003
2. Ruggiero SL, Mehrotra B, Rosenberg TJ, et al: Osteonecrosis ofthe jaws associated with the use of bisphosphonates: A reviewof 63 cases. J Oral Maxillofac Surg 62:527, 2004
3. Ruggiero SL, Dodson TB, Assael LA, et al: American Associationof Oral and Maxillofacial Surgeons position paper onbisphosphonate-related osteonecrosis of the jaws—2009 Up-date. J Oral Maxillofac Surg 67:2, 2009
4. Marx RE, Fortin M, Broum V: Bisphosphonate-induced exposedbone (osteonecrosis/osteopetrosis) of the jaws: Risk factors, rec-ognition, prevention and treatment. J Oral Maxillofacial Surg 63:1567, 2005
5. Migliorati CA: Bisphosphonates and oral cavity avascular bonenecrosis. J Clin 21:4253, 2003
6. Reid IR: Osteonecrosis of the jaw: Who gets it, and why? Bone44:4, 2009
SOYDAN AND UCKAN 5
7. Landesberg R, Cozin M, Cremers S, et al: Inhibition of oral muco-sal cell wound healing by bisphosphonates. J Oral MaxillofacSurg 66:839, 2008
8. Kim RH, Lee RS, Williams D, et al: Bisphosphonates induce se-nescence in normal human oral keratinocytes. J Dent Res 90:810, 2011
9. Sheper MA, Badros A, Chaisuparat R, et al: Effect of zoledronicacid on oral fibroblasts and epithelial cells: A potential mecha-nism of bisphosphonate-associated osteonecrosis. Br J Haematol144:667, 2009
10. Kobayashi Y, Hiraga T, Ueda A, et al: Zoledronic acid delayswound healing of the tooth extraction socket, inhibits oral epi-thelial cell migration, and promotes proliferation and adhesionto hydroxyapatite of oral bacteria, without causing osteonecro-sis of the jaw, in mice. J Bone Miner Metab 28:165, 2010
11. Choukroun J, Adda F, Schoeffer C, et al: PRF: An opportunity inperio-implantology. Implantodontie 42:55, 2000
12. Dhoan DM, Choukroun J, Diss A, et al: Platelet-rich fibrin (PRF):A second-generation platelet concentrate. Part II: Platelet-related biologic features. Oral Surg Oral MedOral Pathol Oral Ra-diol Endod 101:45, 2006
13. Choukroun J, Diss A, Simonpieri A, et al: Platelet-rich fibrin(PRF): A second-generation platelet concentrate. Part V: Histo-logic evaluation of PRF effect on bone allograft maturation in si-nus lift. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 101:299, 2006
14. Dhoan DM, Choukroun J, Diss A, et al: Platelet-rich fibrin (PRF):A second-generation platelet concentrate. Part III: Leucocyte ac-tivation: A new feature for platelet concentrate? Oral Surg OralMed Oral Pathol Oral Radiol Endod 101:51, 2006
15. Walter C, Klein MO, Pabst A, et al: Influence of bisphosphonateson endothelial cells, fibroblasts, and osteogenic cells. Clin OralInvestig 14:35, 2010
16. Sedghizadeh PP, Kumar SK, Gorur A, et al: Identification of mi-crobial biofilms in osteonecrosis of the jaws secondary tobisphosphonate therapy. J Oral Maxillofac Surg 66:767, 2008
17. Hansen T, Kunkel M,Weber A, et al: Osteonecrosis of the jaws inpatients treated with bisphosphonates—Histomorphologicanalysis in comparison with infected osteoradionecrosis. JOral Pathol Med 35:155, 2006
18. Dimopoulos MA, Kastritis E, Bamia C, et al: Reduction of osteo-necrosis of the jaw (ONJ) after implementation of preventive
measures in patients with multiple myeloma treated with zole-dronic acid. Ann Oncol 20:117, 2009
19. Curi MM, Cossolin GS, Koga DH, et al: Bisphosphonate-re-lated osteonecrosis of the jaws—An initial case series reportof treatment combining partial bone resection and autolo-gous platelet-rich plasma. J Oral Maxillofac Surg 69:2465,2011
20. Lee CY, David T, Nishime M: Use of platelet- rich plasma inthe management of oral bisphosphonate-associated osteone-crosis of the jaw: A report of 2 cases. J Oral Implantol 33:371, 2007
21. Dohan DM, Choukroun J, Diss A, et al: Platelet-rich fibrin (PRF):A second-generation platelet concentrate. Part I: Technologicalconcepts and evolution. Oral Surg Oral Med Oral Pathol Oral Ra-diol Endod 101:e37, 2006
22. Pripatnanont P, Nuntanaranont T, Vongvatcharanon S, et al: Theprimacy of platelet-rich fibrin on bone regeneration of variousgrafts in rabbit’s calvarial defects. J Craniomaxillofac Surg,2013 [Epub ahead of print]
23. Dohan Ehrenfest DM, de Peppo GM, Doglioli P, et al: Slow re-lease of growth factors and thrombospondin-1 in Choukroun’splatelet-rich fibrin (PRF): A gold standard to achieve for all surgi-cal platelet concentrates technologies. Growth Factors 27:63,2009
24. He L, Lin Y, Hu X, et al: A comparative study of platelet-rich fibrin(PRF) and platelet-rich plasma (PRP) on the effect of prolifera-tion and differentiation of rat osteoblasts in vitro. Oral SurgOral Med Oral Pathol Oral Radiol Endod 108:707, 2009
25. Simon BJ, Gupta P, Tajbakhsh S: Quantitative evaluation of ex-traction socket healing following the use of autologous plateletrich fibrin matrix in humans. Int J Periodontics Restorative Dent31:284, 2011
26. Chang YC, Zhao JH: Effects of platelet-rich fibrin on human peri-odontal ligament fibroblasts and application for periodontal in-fra bony defects. Aust Dent J 56:365, 2011
27. Chang IC, Tsai CH, Chang YC: Platelet-rich fibrin modulates theexpression of extracellular signal-regulated protein kinase andosteoprotegerin in human osteoblasts. J Biomed Mater Res A95:327, 2010
28. Huang FM, Yang SF, Zhao JH, et al: Platelet-rich fibrin increasesproliferation and differentiation of human dental pulp cells. J En-dod 36:1628, 2010