Embed Size (px)
Citation preview
Management of Common Findings in Abdominal Imaging Reports Anthony E. Hanbidge
� This program has not received financial support
� This program has not received in-kind support
� Potential for conflict(s) of interest: � Anthony Hanbidge has no potential for
conflict(s) of interest
Disclosure of Commercial Support
Faculty/Presenter Disclosure � Faculty: Anthony Hanbidge
� Relationships with commercial interests: � None
1) Describe radiologist’s role in patient assessment
2) Recognize the importance of context in image interpretation
3) Discuss the management of common abdominal imaging findings
Learning Objectives
Patient Management

For discussion: � Incidental gallbladder polyp � Asymptomatic simple ovarian cyst � Asymptomatic cystic pancreatic
mass � Incidental cystic renal mass � Incidental solid renal mass
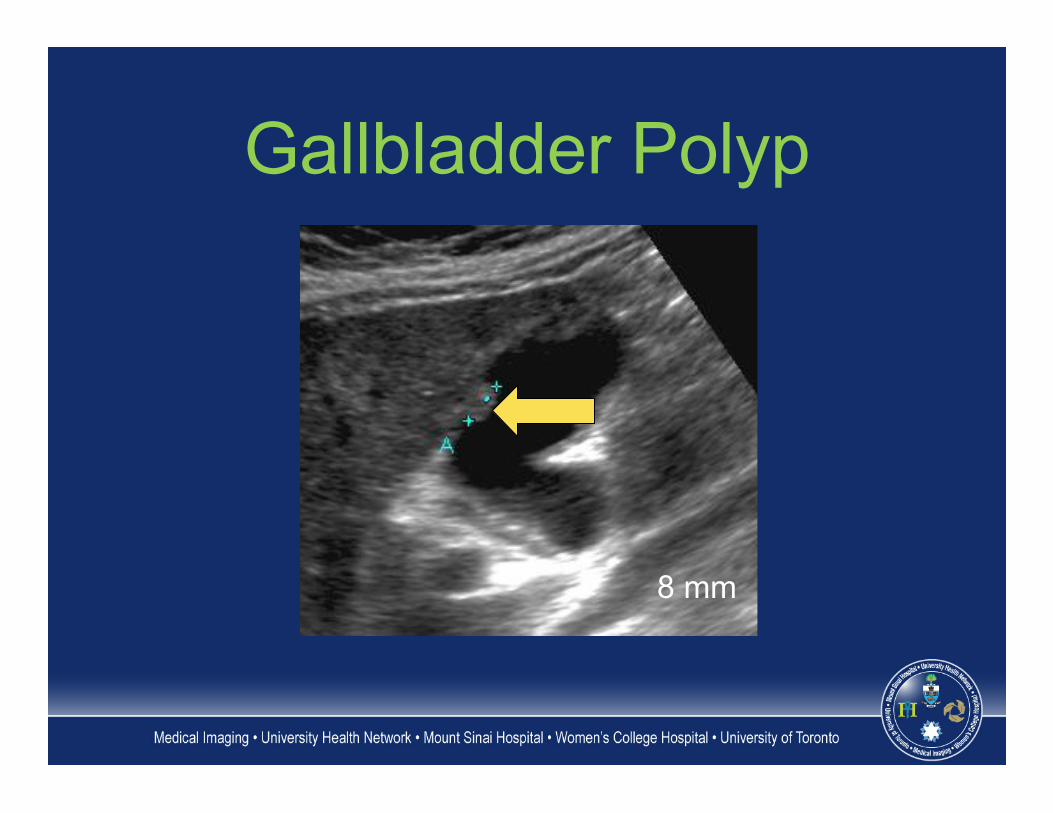
Gallbladder Polyp
8 mm
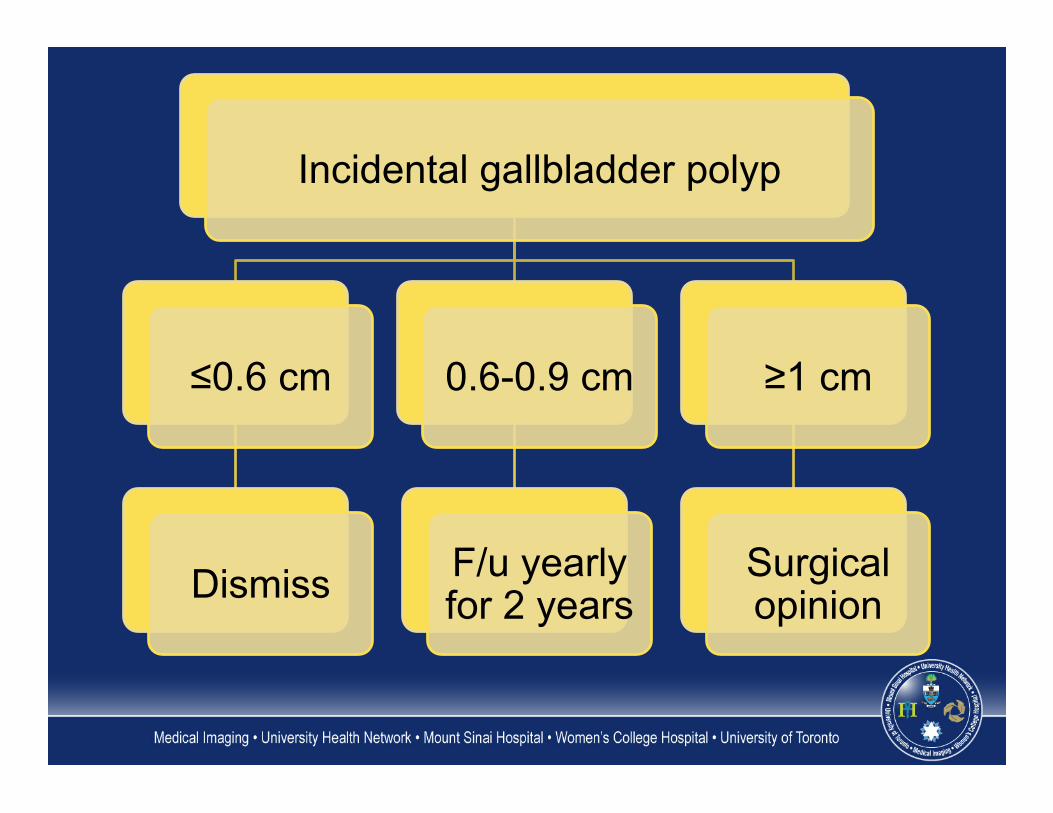
Incidental gallbladder polyp
≤0.6 cm
Dismiss
0.6-0.9 cm
F/u yearly for 2 years
≥1 cm
Surgical opinion
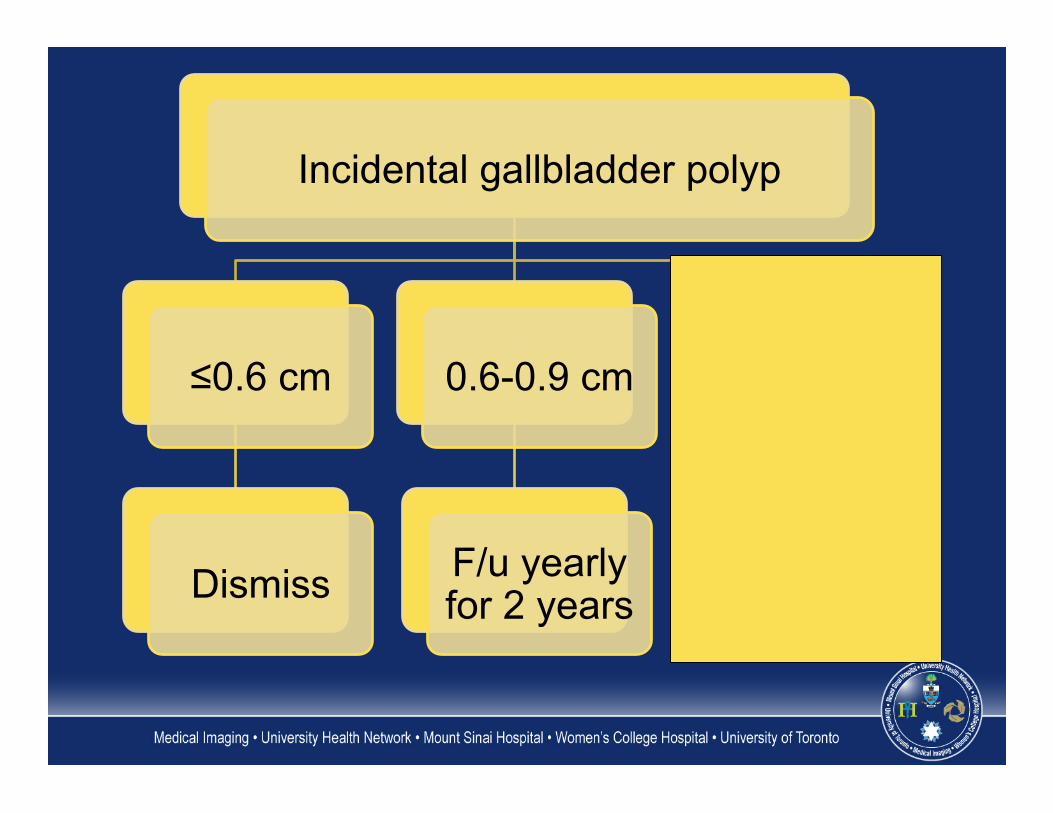
Incidental gallbladder polyp
≤0.6 cm
Dismiss
0.6-0.9 cm
F/u yearly for 2 years
≥1 cm
Surgical opinion
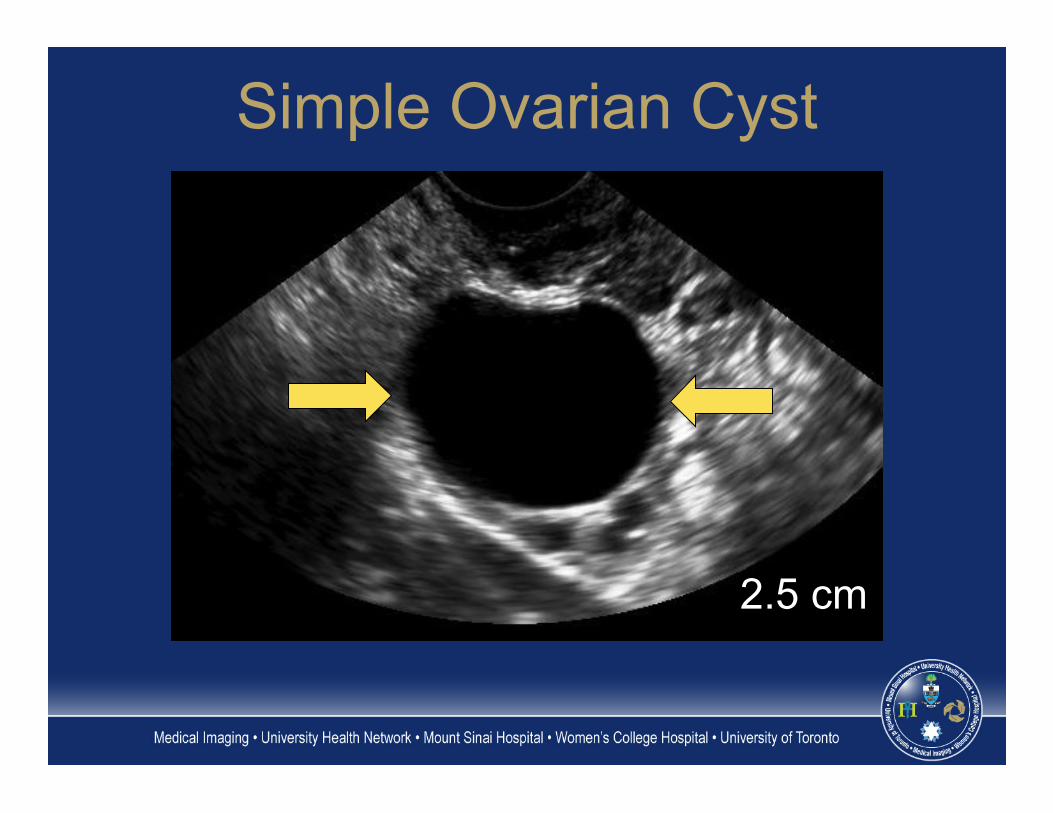
Simple Ovarian Cyst
2.5 cm
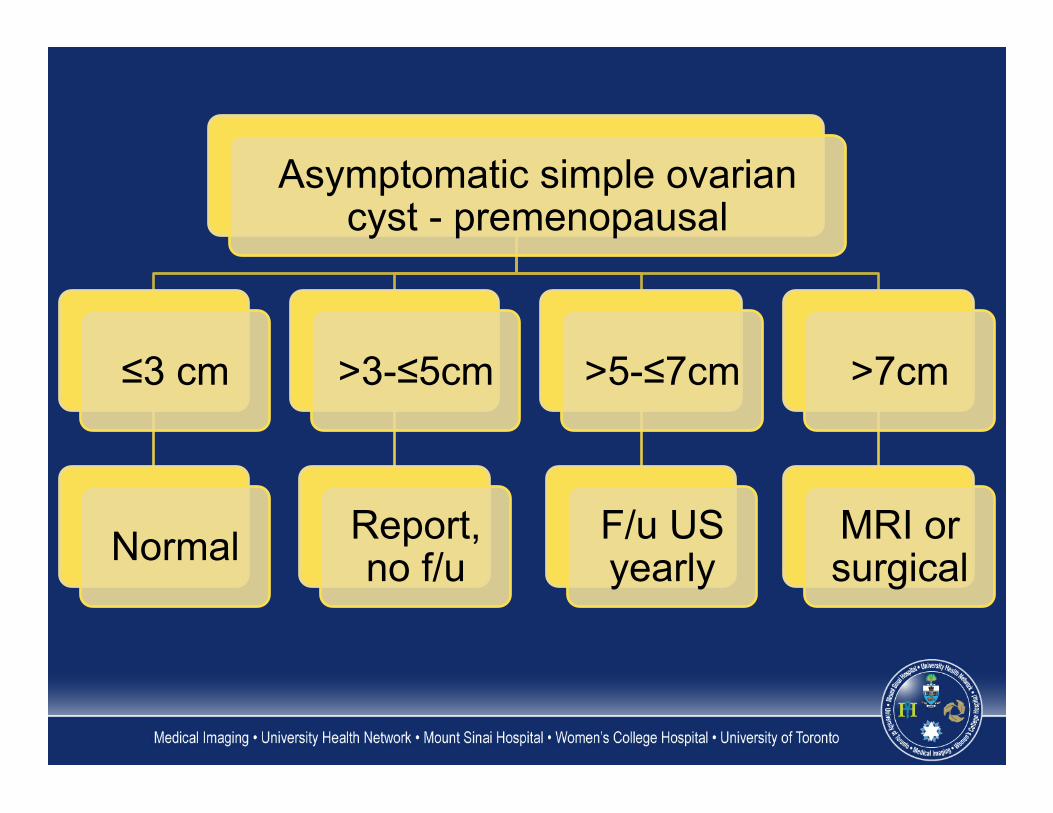
Asymptomatic simple ovarian cyst - premenopausal
≤3 cm
Normal
>3-≤5cm
Report, no f/u
>5-≤7cm
F/u US yearly
>7cm
MRI or surgical
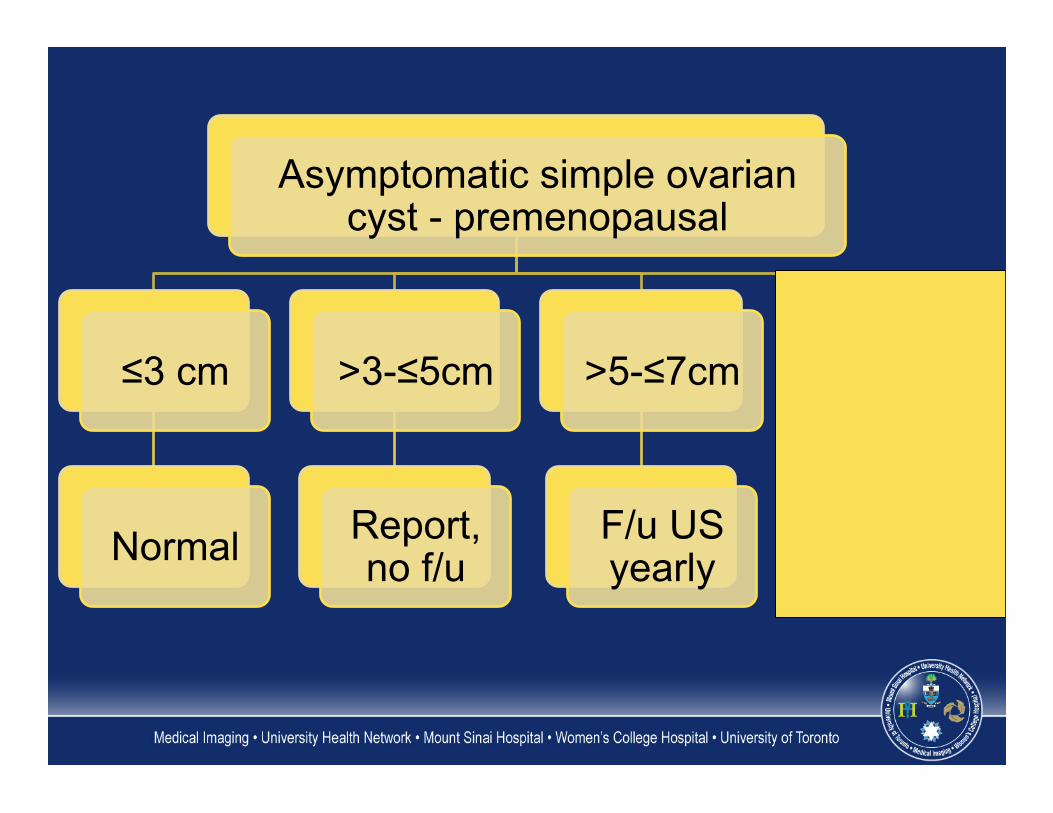
Asymptomatic simple ovarian cyst - premenopausal
≤3 cm
Normal
>3-≤5cm
Report, no f/u
>5-≤7cm
F/u US yearly
>7cm
MRI or surgical
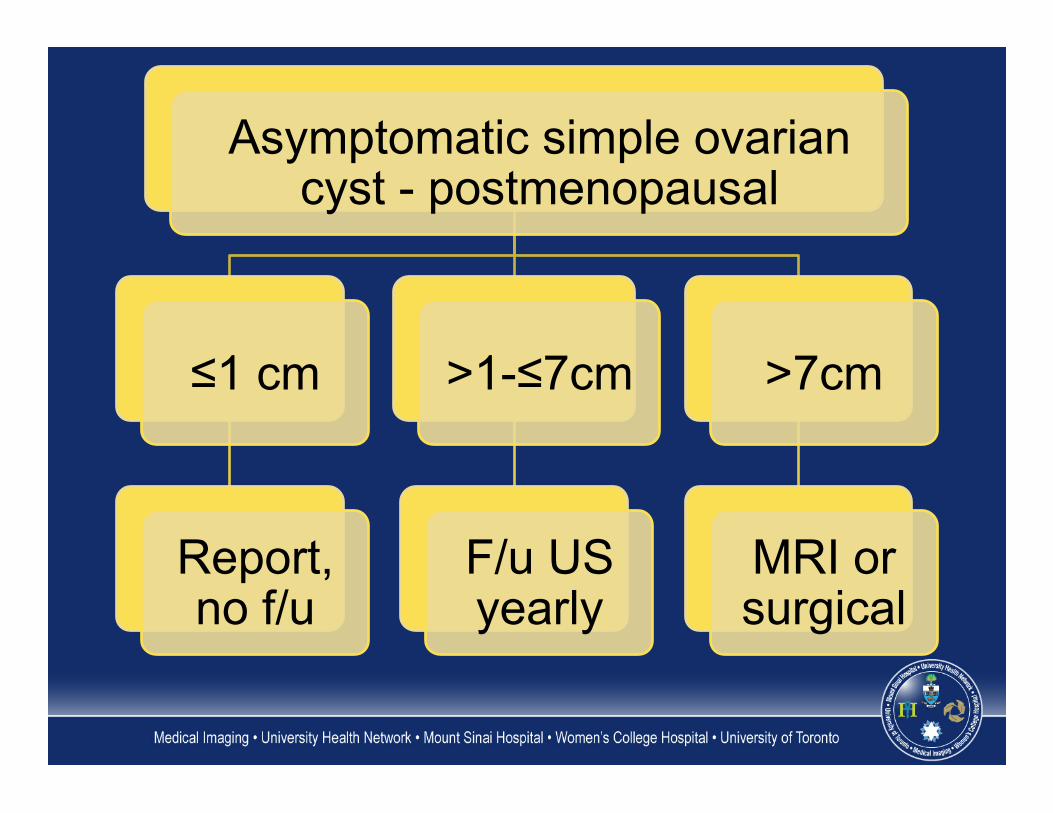
Asymptomatic simple ovarian cyst - postmenopausal
≤1 cm
Report, no f/u
>1-≤7cm
F/u US yearly
>7cm
MRI or surgical
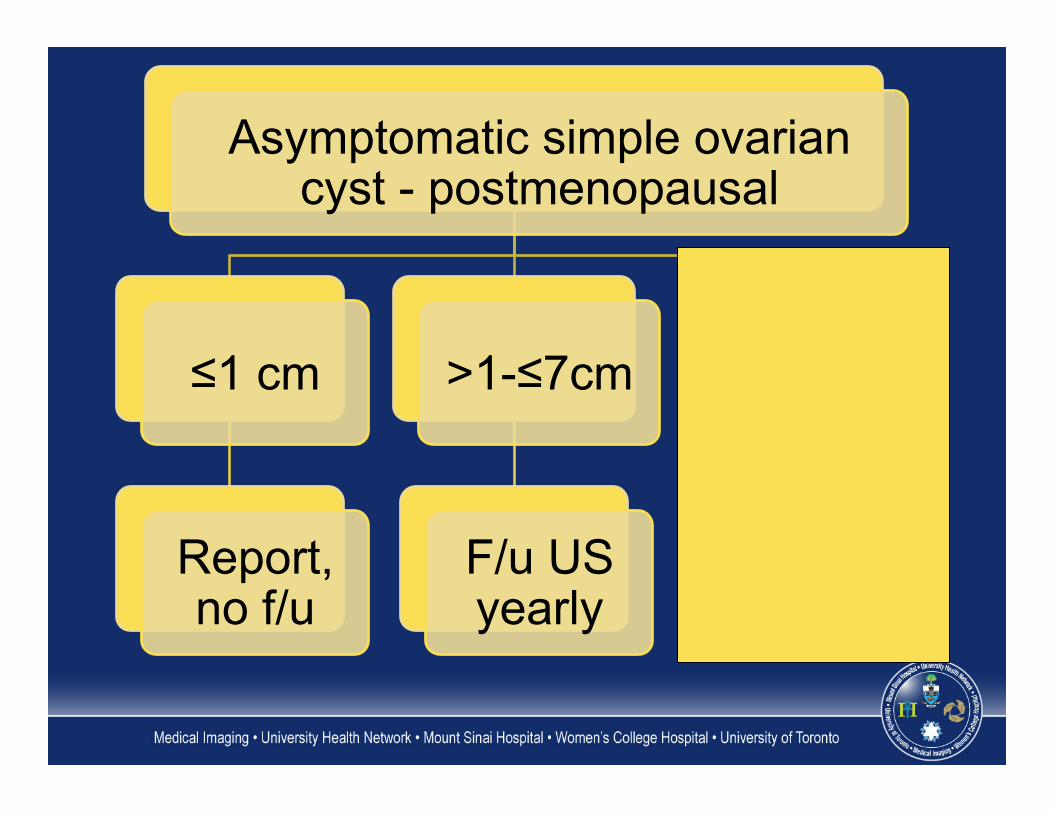
Asymptomatic simple ovarian cyst - postmenopausal
≤1 cm
Report, no f/u
>1-≤7cm
F/u US yearly
>7cm
MRI or surgical
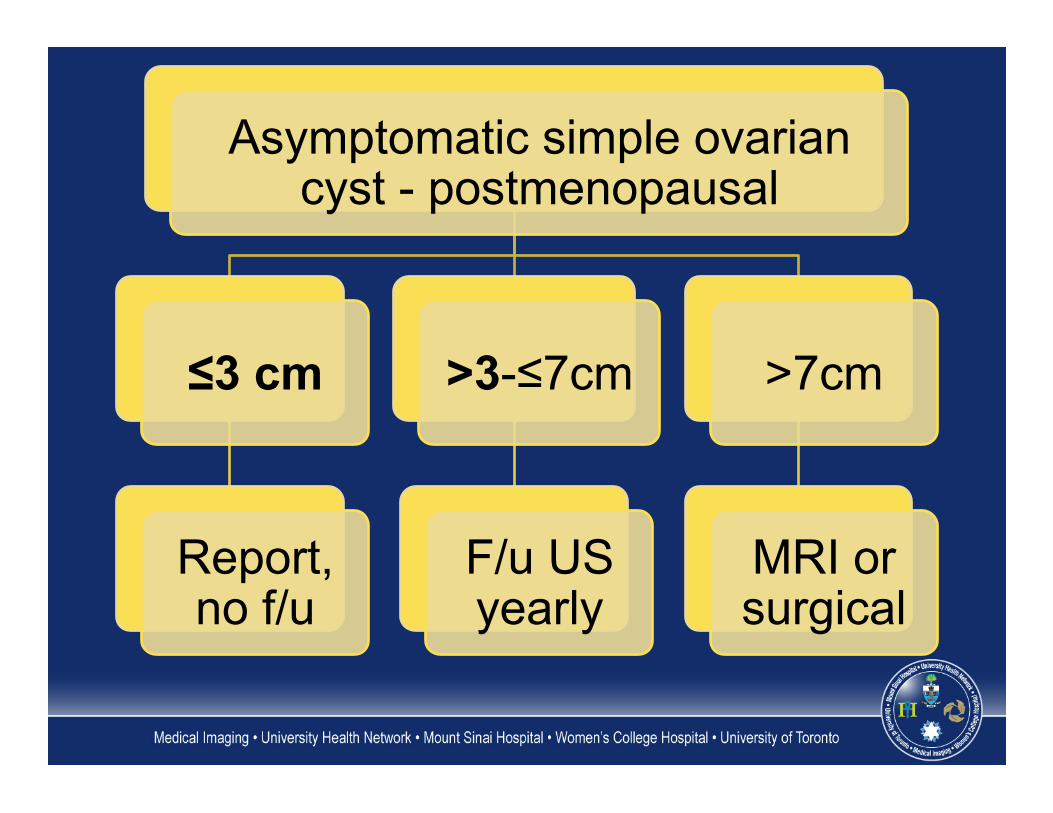
Asymptomatic simple ovarian cyst - postmenopausal
≤3 cm
Report, no f/u
>3-≤7cm
F/u US yearly
>7cm
MRI or surgical
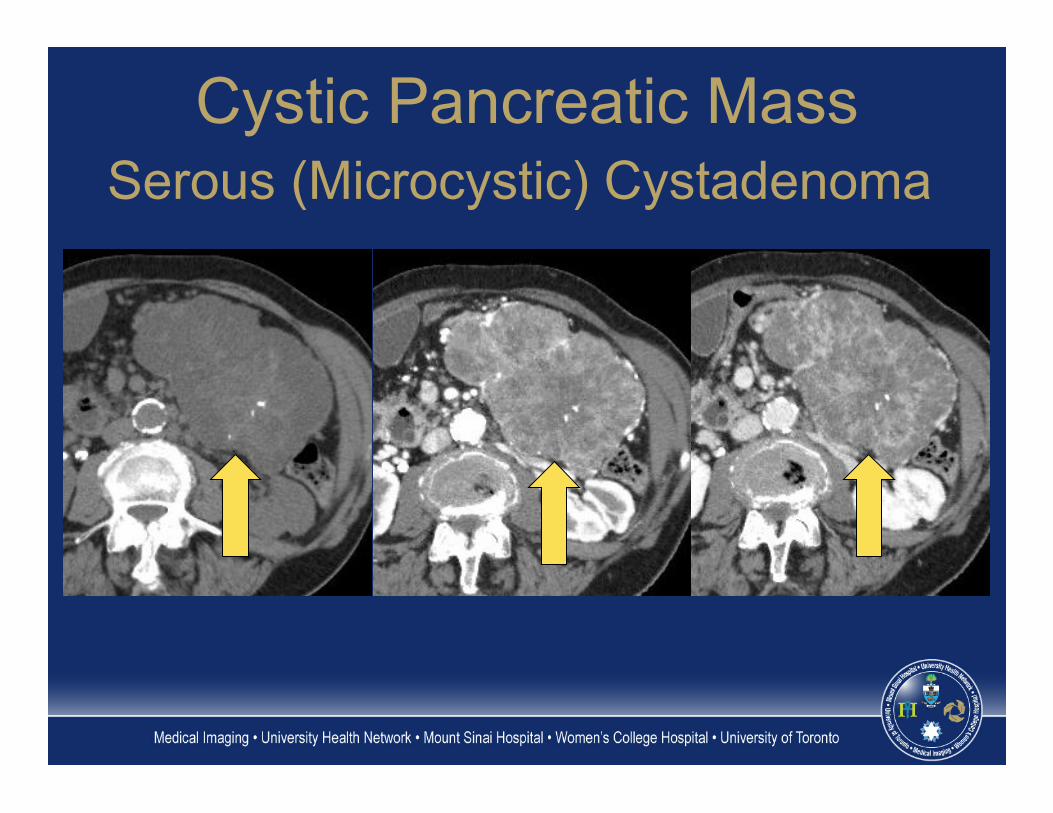
Cystic Pancreatic Mass Serous (Microcystic) Cystadenoma
Asymptomatic cystic pancreatic mass
<2 cm
Single f/u 1 yr *
Stable
Benign, no further f/u
Growth
2–3 cm
Imaging characterization
(MRI/MRCP)
Uncharacterized cystic mass
F/u yearly
BD-IPMN
F/u every 6 months for 2 years*
Serous cystadenoma
F/u every 2 years
>3cm
Serous cystadenoma
Consider resection when ≥4
cm
Uncharacterized cystic mass
Cyst aspiration
Resect, co-morbidities/risk
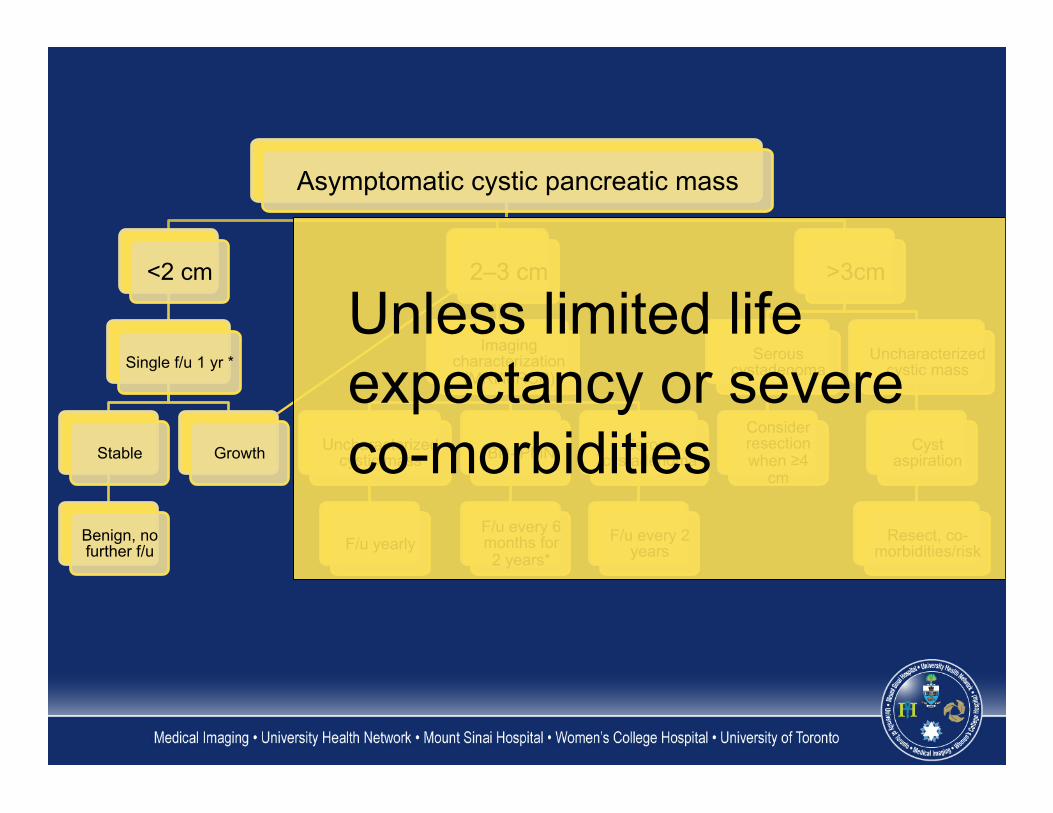
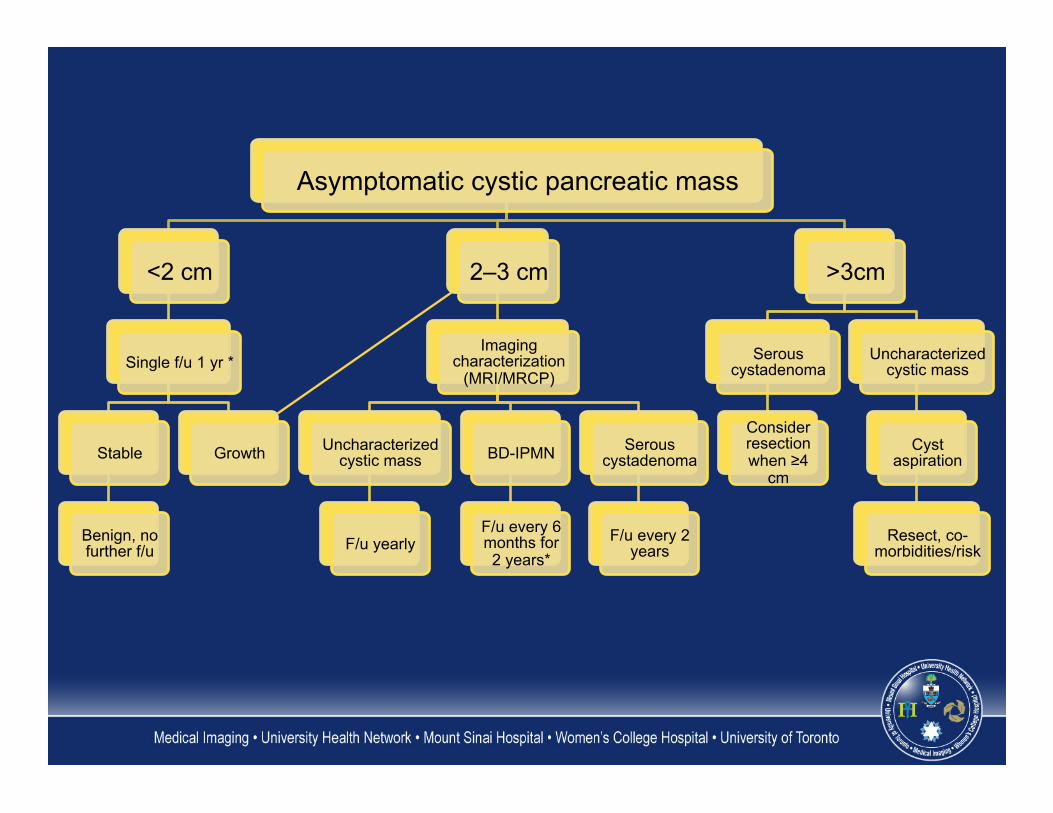
Asymptomatic cystic pancreatic mass
<2 cm
Single f/u 1 yr *
Stable
Benign, no further f/u
Growth
2–3 cm
Imaging characterization
(MRI/MRCP)
Uncharacterized cystic mass
F/u yearly
BD-IPMN
F/u every 6 months for 2 years*
Serous cystadenoma
F/u every 2 years
>3cm
Serous cystadenoma
Consider resection when ≥4
cm
Uncharacterized cystic mass
Cyst aspiration
Resect, co-morbidities/risk
Unless limited life expectancy or severe co-morbidities
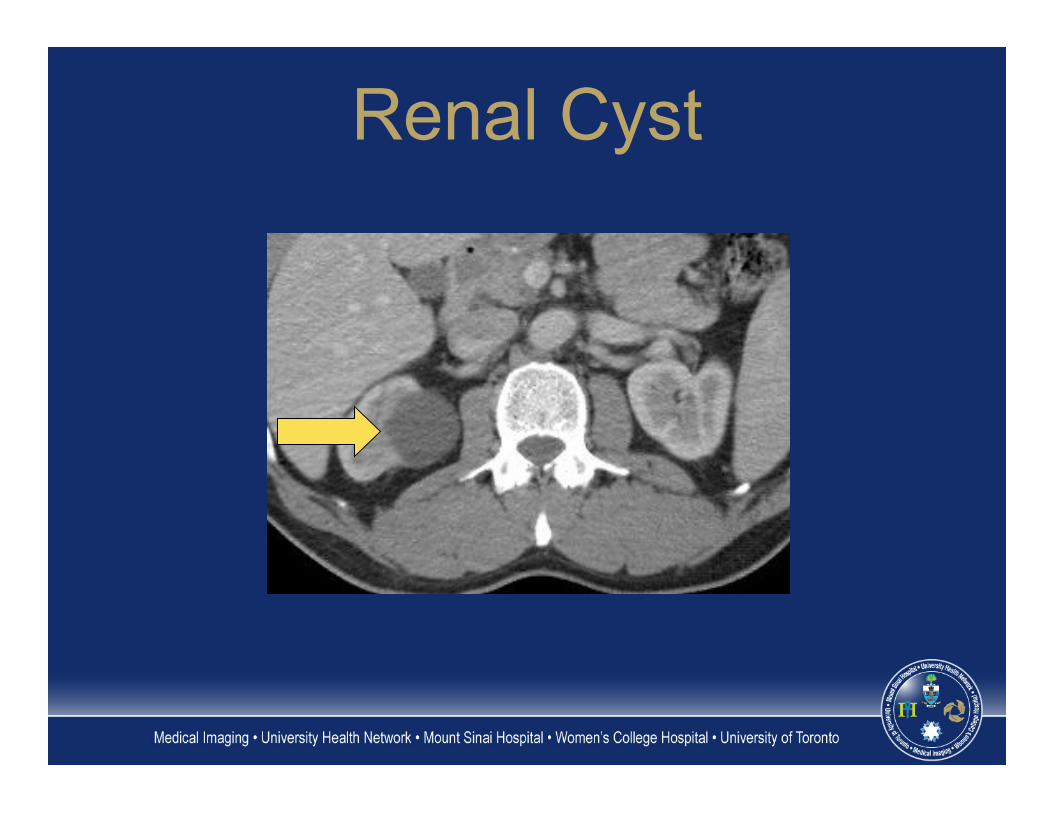
Renal Cyst
I - simple cyst II - minimally complex, few hairline
septa, fine Ca++ or short segment thickened Ca++ in wall or septa, homogeneously high attenuation masses <3 cm that do not enhance
Bosniak classification
IIF - multiple hairline septa, smooth thickening of wall or septa, thick nodular calcification, no enhancing soft tissue components, intrarenal, non-enhancing high attenuation masses (>3 cm)
Bosniak classification
III - Thickened irregular or smooth walls or septa with measurable enhancement
IV – Criteria of III but also containing enhancing soft tissue components adjacent to or separate from the walls or septa
Bosniak classification
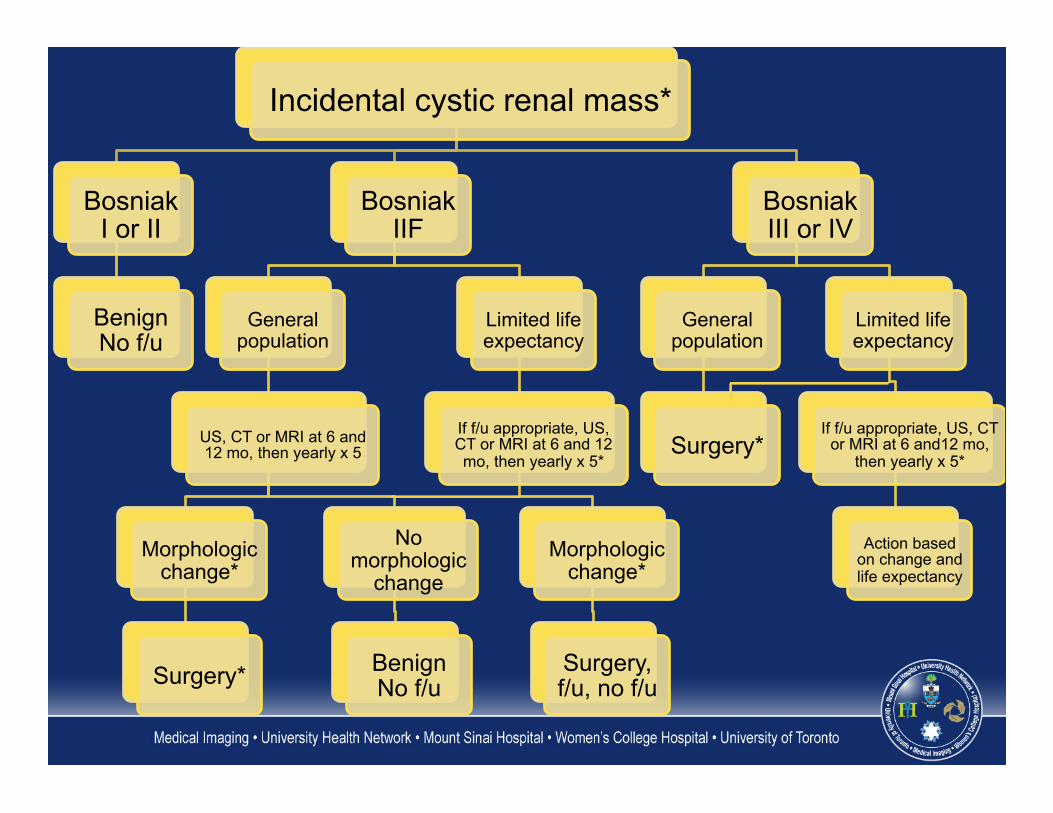
Incidental cystic renal mass*
Bosniak I or II
Benign No f/u
Bosniak IIF
General population
US, CT or MRI at 6 and 12 mo, then yearly x 5
Morphologic change*
Surgery*
No morphologic
change
Benign No f/u
Limited life expectancy
If f/u appropriate, US, CT or MRI at 6 and 12 mo, then yearly x 5*
Morphologic change*
Surgery, f/u, no f/u
Bosniak III or IV
General population
Surgery*
Limited life expectancy
If f/u appropriate, US, CT or MRI at 6 and12 mo,
then yearly x 5*
Action based on change and life expectancy
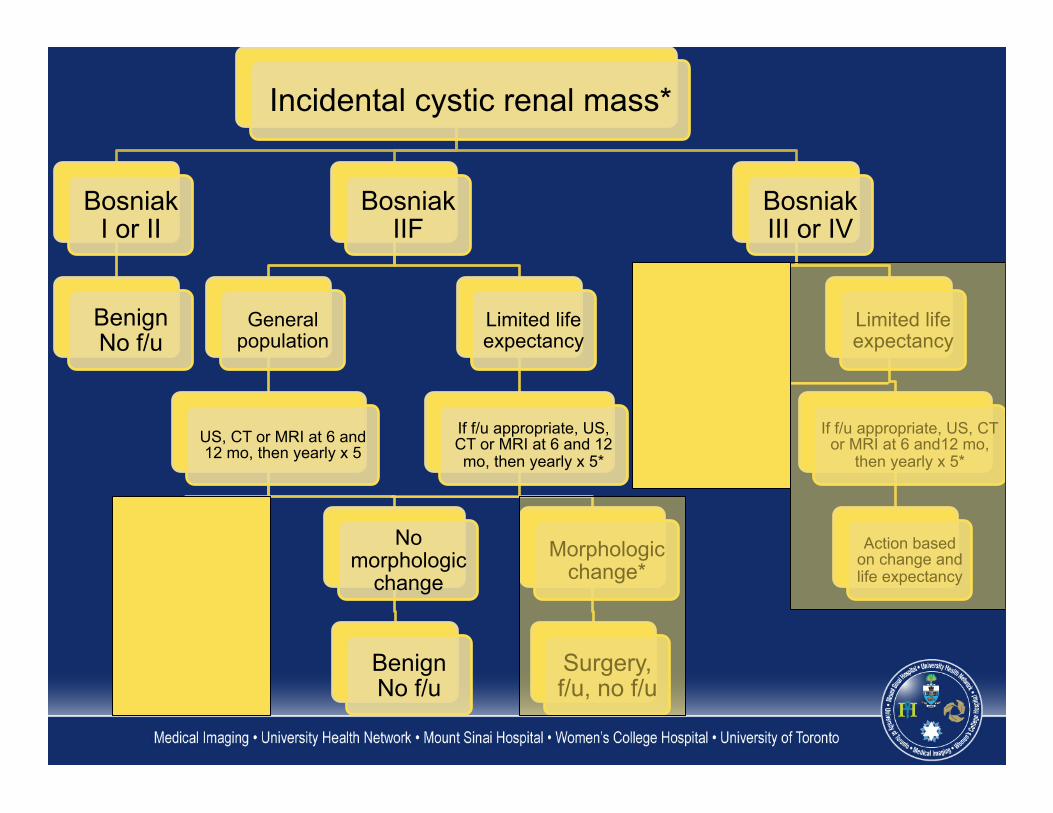
Incidental cystic renal mass*
Bosniak I or II
Benign No f/u
Bosniak IIF
General population
US, CT or MRI at 6 and 12 mo, then yearly x 5
Morphologic change*
Surgery*
No morphologic
change
Benign No f/u
Limited life expectancy
If f/u appropriate, US, CT or MRI at 6 and 12 mo, then yearly x 5*
Morphologic change*
Surgery, f/u, no f/u
Bosniak III or IV
General population
Surgery*
Limited life expectancy
If f/u appropriate, US, CT or MRI at 6 and12 mo,
then yearly x 5*
Action based on change and life expectancy
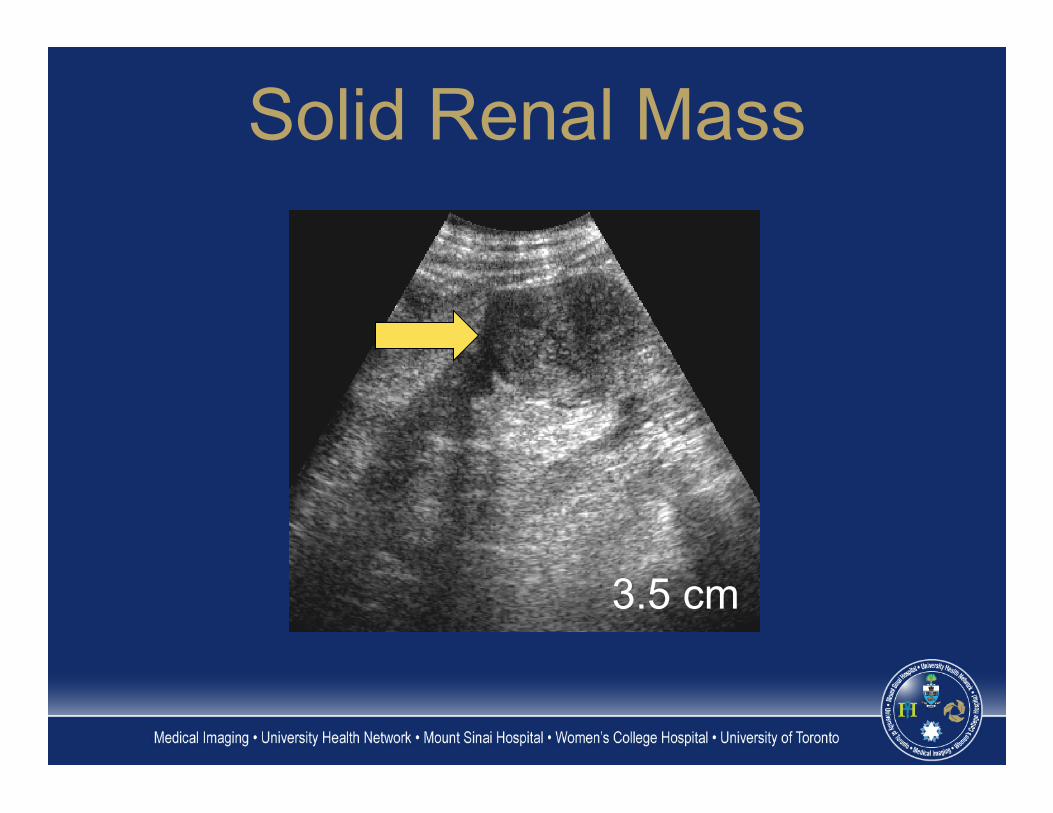
3.5 cm
Solid Renal Mass
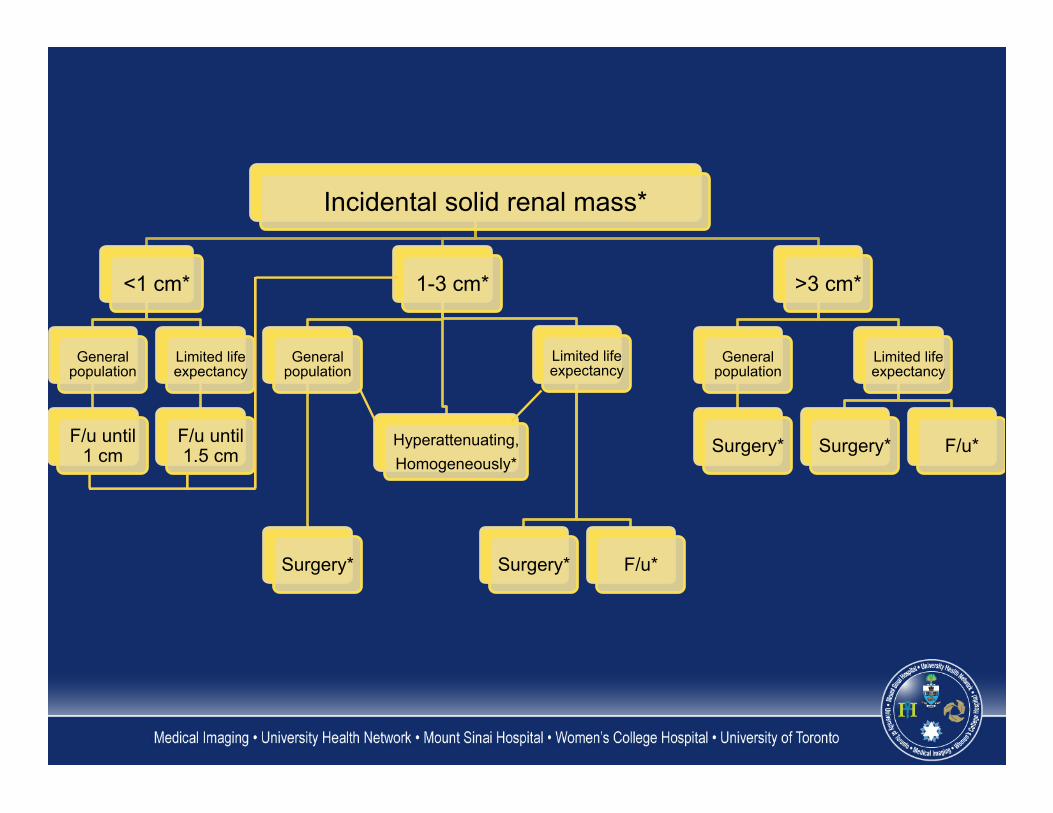
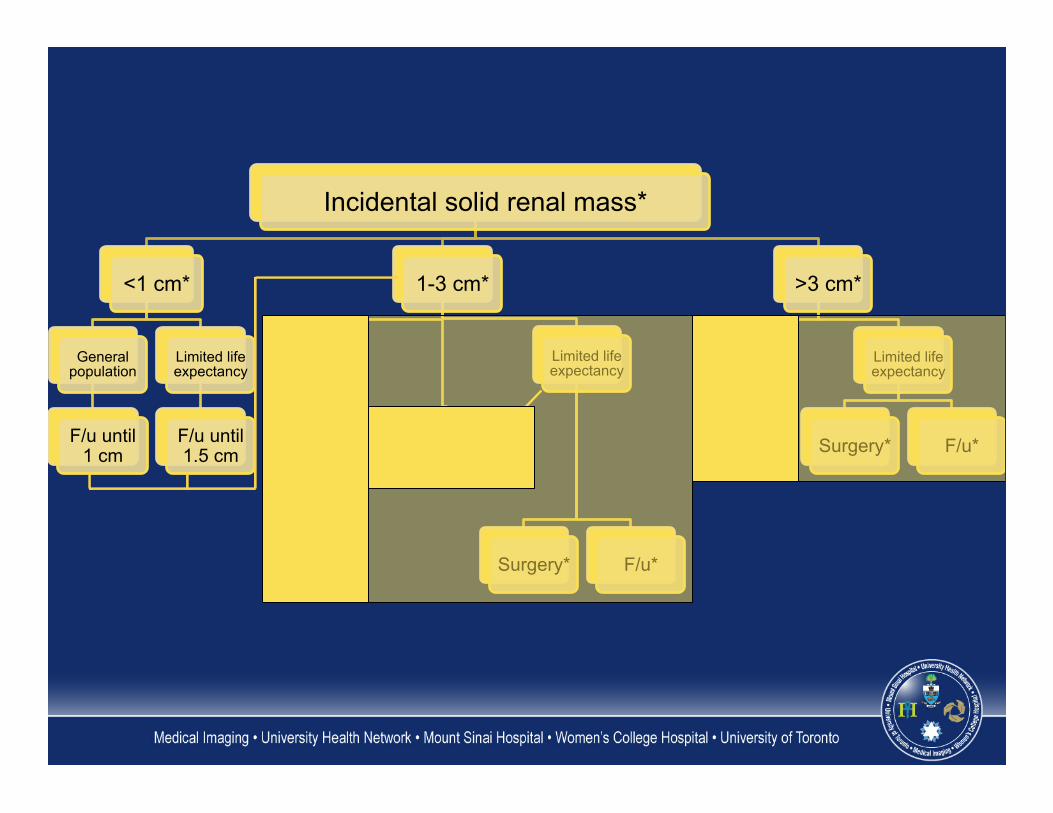
Incidental solid renal mass*
<1 cm*
General population
F/u until 1 cm
Limited life expectancy
F/u until 1.5 cm
1-3 cm*
General population
Surgery*
Hyperattenuating, Homogeneously*
Limited life expectancy
Surgery* F/u*
>3 cm*
General population
Surgery*
Limited life expectancy
Surgery* F/u*
Incidental solid renal mass*
<1 cm*
General population
F/u until 1 cm
Limited life expectancy
F/u until 1.5 cm
1-3 cm*
General population
Surgery*
Hyperattenuating, Homogeneously*
Limited life expectancy
Surgery* F/u*
>3 cm*
General population
Surgery*
Limited life expectancy
Surgery* F/u*
Summary � Imaging 1 piece of puzzle � History, physical, labs � Communication is key in directing appropriate care
References Berland ll et al. Managing incidental findings on abdominal CT: white paper of the ACR incidental findings committee. J Am Coll Radiol. 2010 Oct;7(10):754-73. doi: 10.1016/j.jacr.2010.06.013. Levine D et al. Management of asymptomatic ovarian and other adnexal cysts imaged at US: Society of Radiologists in Ultrasound Consensus Conference Statement. Radiology. 2010 Sep;256(3):943-54. doi: 10.1148/radiol.10100213. Epub 2010 May 26. Review. Corwin MT et al. Incidentally detected gallbladder polyps: is follow-up necessary?--Long-term clinical and US analysis of 346 patients. Radiology 2011;258:277-282. doi: 10.1148/radiol.10100273. Epub 2010 Aug 9.
PubMed
Managing incidental findings
and
ACR
Follow-up imaging � Consider decreasing interval if
younger � Consider omitting if limited life
expectancy � US vs. MRI
Follow-up imaging � If no growth after 2 years, follow
yearly � If growth or suspicious features
develop, consider resection
Solid renal mass � Follow guidelines only if infections
and fat containing angiomyolipomas have been excluded
Differential diagnosis � Renal cell cancer � Oncocytoma � Fat poor angiomyolipoma � Benign entities more likely in small
renal masses than large ones
Differential diagnosis � Renal cell cancer more probable
If hyperattenuating and homogeneously enhancing � Consider MRI and biopsy to
diagnose fat poor angiomyolipoma
Surgery � Open or laparoscopic nephrectomy
or partial nephrectomy (all provide tissue diagnosis)
� Open, laparoscopic or percutaneous RFA (biopsy first for tissue diagnosis)
Surgery � Open or laparoscopic nephrectomy
or partial nephrectomy (all provide tissue diagnosis)
� Open, laparoscopic or percutaneous RFA (biopsy first for tissue diagnosis)
� Biopsy first to confirm RCC
Differential diagnosis � Probable diagnosis renal cell
cancer � Fat poor angiomyolipoma,
oncocytoma and other benign neoplasms may be found at surgery
Follow-up � Observation may be considered for
a solid renal mass of any size in a patient with limited life expectancy or co-morbidities that increase the risk of treatment
Incidental cystic renal mass � Follow guidelines only if non-
neoplastic causes of mass excluded (e.g. infection)
Morphologic change � Change refers to change in feature
characteristics, such as number of septations or thickness
� Growth should be noted but by itself does not indicate malignancy
? No follow-up � Cystic masses 1.5 cm or smaller
that are not clearly simple cysts or that cannot be characterized completely may not require further evaluation in this group
Surgery � Open or laparoscopic nephrectomy
or partial nephrectomy (all provide tissue diagnosis)
� Open, laparoscopic or percutaneous RFA (biopsy first for tissue diagnosis)
Percutaneous biopsy � Percutaneous biopsy of Bosniak III
masses can be considered but may not be diagnostic




![Abdominal CT Findings of Cholecystogastric Fistula · the fistula [9]. Cholangitis; peritonitis; cholecystitis intestinal obstruction gastrointestinal hemorrhage and malignancy are](https://img.pdfslide.net/doc/110x75/5f7a5d1adfd91a379605cde5/abdominal-ct-findings-of-cholecystogastric-fistula-the-fistula-9-cholangitis.jpg)
























