Embed Size (px)
Citation preview
VOL. 7 SUPPL. 3 2007 REVIEWS IN GASTROENTEROLOGICAL DISORDERS S27
LOPERAMIDE IN THE TREATMENT OF IBS OR IBD
Management of Diarrhea in Clinical Practice: Strategies for PrimaryCare PhysiciansLawrence R. Schiller, MD
Digestive Health Associates of Texas, Baylor University Medical Center, Dallas, TX
The evaluation and management of diarrhea can be a challenging problem for primary care physicians. The differential diagnosis is large and the multi-plicity of diagnostic tests makes the evaluation complex. A strategy of takinga thorough history and performing simple objective tests can make the diag-nostic process easier. This strategy will often lead to a specific diagnosis thatcan be treated specifically. When a diagnosis is not proven, however, diarrheacan be managed symptomatically with antidiarrheals such as loperamide.Such an approach improves the quality of life of patients with diarrhea andmay mitigate associated symptoms, such as fecal incontinence.[Rev Gastroenterol Disord. 2007;7(suppl 3):S27-S38]
© 2007 MedReviews, LLC
Key words: Acute diarrhea • Chronic diarrhea • Rehydration • Irritable bowel syndrome •Symptomatic therapy • Loperamide
Diarrhea, defined as loose stools, occurs when the intestine does not com-plete absorption of electrolytes and water from luminal contents.1 This canoccur when a nonabsorbable, osmotically active substance is ingested
(“osmotic diarrhea”) or when electrolyte absorption is impaired (“secretory diar-rhea”). Most cases of acute and chronic diarrhea are due to the latter mechanism.Secretory diarrhea can be the result of bacterial toxins; reduced absorptive sur-face area due to disease or resection; luminal secretagogues, such as bile acids orlaxatives; circulating secretagogues, such as various hormones, drugs, and poi-sons; and medical problems that compromise regulation of intestinal function.
RIGDCME_12-12.qxd 12/12/07 10:09 PM Page S27

Managing Diarrhea in Clinical Practice continued
S28 VOL. 7 SUPPL. 3 2007 REVIEWS IN GASTROENTEROLOGICAL DISORDERS
Because diarrhea can be a symptomof so many different conditions, it isbest to organize the differential diag-nosis of diarrhea by duration intoacute diarrhea, lasting less than 4weeks and usually only a few days,and chronic diarrhea, lasting morethan 4 weeks.1-3 This distinguishes be-tween self-limited diarrhea predomi-nantly due to infectious causes andmore persistent problems that are dueto a variety of causes.
Before assessing the cause of diar-rhea or attempting empiric therapy, itis essential to evaluate the patient’sfluid and electrolyte status.3 Diarrheacan be life threatening if volume orelectrolyte depletion has occurred. Or-thostatic changes in pulse and bloodpressure should be measured. Patientswith longstanding or voluminous di-arrhea should have serum electrolyteconcentrations assayed. Intravenousor oral rehydration and electrolyte re-pletion take precedence over diagnosisin the management of these patients.
Acute DiarrheaOn average, each American has about1 bout of acute diarrhea per year.Acute diarrhea typically is self-limitedand management usually consists ofproviding adequate hydration eitherorally or intravenously while await-ing spontaneous resolution.4,5
The primary care physician mustdistinguish among 3 groups of pa-tients: a) patients who have mild diar-rhea that does not require specifictreatment or further evaluation andwho only need modest rehydrationand symptomatic management, b) pa-tients with specific epidemiologicalclues (eg, travelers’ diarrhea or diar-rhea in a daycare worker) suggestive ofconditions that should be treated withempiric antibiotics, and c) patients
with particularly severe acute diar-rhea who require an initial diagnosticevaluation focused on infectiouscauses.5 Examples of the latter groupof patients include those requiringhospitalization due to dehydration,patients with bloody diarrhea or se-vere abdominal pain, and patients inwhom diarrhea does not resolve in afew days.
The initial evaluation should in-clude a complete blood count, serum
electrolyte panel, serum creatinineand blood urea nitrogen assays,stool bacterial culture, stool ova and
parasite examination, and stool as-says for Giardia antigen, Crypto-sporidium antigen, and Clostridiumdifficile toxin titer (especially if thepatient was treated with antimicro-bials within 90 days or if the patientis a healthcare worker or resident inan institution with a high rate of C.difficile infection). If the diagnosis isstill obscure and the diarrhea contin-ues, biopsy of the rectum or colonshould be considered in order to dif-ferentiate self-limited colitis fromearly idiopathic inflammatory boweldisease.
Bacterial and viral infections ac-count for the vast majority of acutediarrheas (Table 1). Several of theseare of special importance.
Table 1Differential Diagnosis of Acute Diarrhea
Mechanism Examples
Infection BacteriaEscherichia coli (enterotoxigenic, enteroinvasive, enterohemorrhagic)
Campylobacter spp.Salmonella spp.Shigella spp.Clostridium difficileAeromonas spp.Pleisiomonas spp.
VirusesAdenovirusRotavirusNorovirus
Parasites/ProtozoaEntamoeba histolyticaGiardia lambliaCryptosporidiumMicrosporidiumCyclospora
Food poisoningFood allergiesMedicationInitial presentation of chronic diarrhea
Adapted with permission from Schiller LR and Sellin JH.1
On average, each American has about 1 bout of acute diarrhea per year.
RIGDCME_12-12.qxd 12/12/07 10:09 PM Page S28

Managing Diarrhea in Clinical Practice
VOL. 7 SUPPL. 3 2007 REVIEWS IN GASTROENTEROLOGICAL DISORDERS S29
Campylobacter jejuni remains acommon cause of acute community-acquired diarrhea. Tissue invasion oc-curs frequently and severe colitismimicking idiopathic ulcerative coli-tis can occur. Studies suggest an asso-ciation between C. jejuni infectionand Guillain-Barré syndrome. Ery-thromycin or a fluoroquinolone canshorten the duration of symptoms ifgiven early in the course of the infec-tion, but most cases recover withoutany antibiotic treatment.
Because of the morbidity and rela-tively high case fatality rate, acutediarrhea due to Escherichia coliO157:H7 has received much attention.This organism produces a hemor-rhagic segmental colitis and is associ-ated with hemolytic-uremic syn-drome. Infection has been associatedwith eating undercooked hamburgerand outbreaks are distressingly fre-quent. Stool electrolyte analysis sug-gests a secretory diarrhea, but franklybloody diarrhea or a strongly positivefecal occult blood test is typical. An-tibiotics should not be used to treatthis infection because they do not im-prove the course of the illness andmay predispose some patients to thedevelopment of hemolytic-uremicsyndrome.6
C. difficile–associated colitis is themost common cause of infectious di-arrhea in hospitalized patients. It usu-ally occurs following broad-spectrumantibiotic therapy and characteristi-cally produces pseudomembranouscolitis. Diagnosis in adults is con-firmed by finding C. difficile toxin instool samples. Symptomatic improve-ment with metronidazole is rapid, butrelapse of diarrhea occurs in morethan 20% of patients when antibiotictherapy is discontinued. Relapsesshould be treated with oral van-comycin.7 Leukocytosis with a “leftshift” can be dramatic and fecalleukocytes are easy to find in patientswith pseudomembranous colitis.
Travelers’ diarrhea is a commonclinical scenario. Although a numberof different organisms may be re-sponsible, empiric antibiotic therapycan be used in most patients toshorten the duration of the diarrhea.Although most travelers returningfrom locations in the western hemi-sphere have diarrhea due to organ-isms that respond to fluoroquinolonesor rifaximin, those returning fromSoutheast Asia may have invasive or-ganisms (eg, Shigella spp., Salmonellaspp., or Campylobacter spp.) that maybe treated with other antibioticstrategies. Addition of an antidiar-rheal drug such as loperamide mayspeed resolution of travelers’ diarrheatreated with antibiotics.8,9
Norovirus is a common cause ofoutbreaks of viral gastroenteritis.Upper tract symptoms of pain andvomiting are prominent early in thecourse of the illness, but diarrhea canbecome very severe. This infection isvery communicable and can affectthousands of patients in a short pe-riod of time. No specific treatment isneeded, but rehydration and sympto-matic therapy may be helpful.
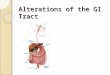
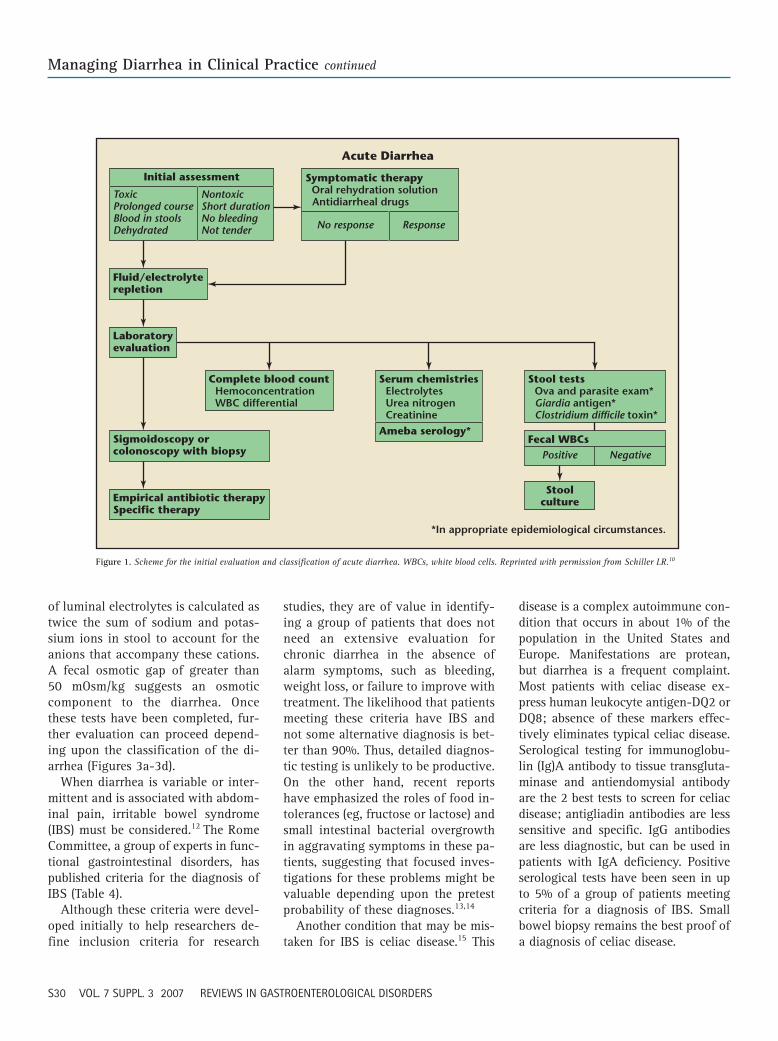
When an acute bout of diarrhealasts more than a week, the list oflikely infectious causes changes; mostbacterial and viral causes would haverun their course and protozoal etiolo-gies, such as giardiasis and cryp-tosporidiosis, are more likely. Giventhe proper epidemiological clues, em-piric treatment for these protozoamay be more cost effective than prov-ing the diagnosis with expensivetests. Most clinicians pursue a test-and-treat strategy, however. A schemefor the evaluation of acute diarrhea ispresented in Figure 1.10
Chronic DiarrheaChronic continuing diarrhea (ie, last-ing more than 4 weeks) is less likely tobe due to infection and has a broaderdifferential diagnosis (Table 2).1,3
Sometimes the history provides anobvious clue that precludes the needfor an extensive evaluation (eg,diarrhea starting soon after chole-cystectomy or other operations, orafter certain medications are started[Table 3]).11
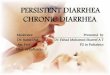
In others, the differential diagnosiscan be so broad that it must be mademore manageable by categorizing thediarrhea by stool characteristics suchas watery, inflammatory, or fatty(Figure 2).
Watery diarrhea is defined as veryliquid stools without evidence ofblood, pus, or fat. The implication ofwatery diarrhea is that either an os-motically active substance or unab-sorbed electrolytes are causing excesswater to be retained intraluminally.Inflammatory diarrhea is character-ized by stools with pus or blood, sug-gesting disruption of the mucosa byinfection or inflammation. Fatty diar-rhea (steatorrhea) suggests the pres-ence of a condition reducing fat ab-sorption in the small intestine.
Efforts to classify the type of diar-rhea involve examining stools for thepresence of occult blood (guaiac test-ing), white blood cells (Wright’s stainor fecal lactoferrin assay), and fat(Sudan stain).3 All of these tests canbe done on “spot” samples or on aquantitative stool collection. Quanti-tative collection for 48 or 72 hoursprovides a better idea of stool outputand fat excretion, but is not essentialfor classification purposes.
Watery diarrhea can be furthercharacterized as osmotic or secretoryby analysis of fecal sodium andpotassium concentrations and calcu-lation of the fecal osmotic gap: thedifference between total luminal os-molality (equal to plasma osmolality—approximately 290 mOsm/kg—becausethe colon cannot maintain an osmoticgradient against plasma) and theosmolality contributed by luminalelectrolytes. The osmotic contribution
RIGDCME_12-12.qxd 12/12/07 10:09 PM Page S29
Managing Diarrhea in Clinical Practice continued
S30 VOL. 7 SUPPL. 3 2007 REVIEWS IN GASTROENTEROLOGICAL DISORDERS
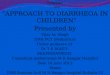
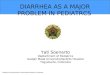
of luminal electrolytes is calculated astwice the sum of sodium and potas-sium ions in stool to account for theanions that accompany these cations.A fecal osmotic gap of greater than50 mOsm/kg suggests an osmoticcomponent to the diarrhea. Oncethese tests have been completed, fur-ther evaluation can proceed depend-ing upon the classification of the di-arrhea (Figures 3a-3d).
When diarrhea is variable or inter-mittent and is associated with abdom-inal pain, irritable bowel syndrome(IBS) must be considered.12 The RomeCommittee, a group of experts in func-tional gastrointestinal disorders, haspublished criteria for the diagnosis ofIBS (Table 4).
Although these criteria were devel-oped initially to help researchers de-fine inclusion criteria for research
studies, they are of value in identify-ing a group of patients that does notneed an extensive evaluation forchronic diarrhea in the absence ofalarm symptoms, such as bleeding,weight loss, or failure to improve withtreatment. The likelihood that patientsmeeting these criteria have IBS andnot some alternative diagnosis is bet-ter than 90%. Thus, detailed diagnos-tic testing is unlikely to be productive.On the other hand, recent reportshave emphasized the roles of food in-tolerances (eg, fructose or lactose) andsmall intestinal bacterial overgrowthin aggravating symptoms in these pa-tients, suggesting that focused inves-tigations for these problems might bevaluable depending upon the pretestprobability of these diagnoses.13,14
Another condition that may be mis-taken for IBS is celiac disease.15 This
disease is a complex autoimmune con-dition that occurs in about 1% of thepopulation in the United States andEurope. Manifestations are protean,but diarrhea is a frequent complaint.Most patients with celiac disease ex-press human leukocyte antigen-DQ2 orDQ8; absence of these markers effec-tively eliminates typical celiac disease.Serological testing for immunoglobu-lin (Ig)A antibody to tissue transgluta-minase and antiendomysial antibodyare the 2 best tests to screen for celiacdisease; antigliadin antibodies are lesssensitive and specific. IgG antibodiesare less diagnostic, but can be used inpatients with IgA deficiency. Positiveserological tests have been seen in upto 5% of a group of patients meetingcriteria for a diagnosis of IBS. Smallbowel biopsy remains the best proof ofa diagnosis of celiac disease.
Initial assessment
Fluid/electrolyterepletion
Laboratoryevaluation
Sigmoidoscopy orcolonoscopy with biopsy
Empirical antibiotic therapySpecific therapy
Complete blood count Hemoconcentration WBC differential
ToxicProlonged courseBlood in stoolsDehydrated
NontoxicShort durationNo bleedingNot tender
Symptomatic therapy Oral rehydration solution Antidiarrheal drugs
No response Response
Serum chemistries Electrolytes Urea nitrogen CreatinineAmeba serology*
Acute Diarrhea
Stoolculture
*In appropriate epidemiological circumstances.
Stool tests Ova and parasite exam* Giardia antigen* Clostridium difficile toxin*
Fecal WBCsPositive Negative
Figure 1. Scheme for the initial evaluation and classification of acute diarrhea. WBCs, white blood cells. Reprinted with permission from Schiller LR.10
RIGDCME_12-12.qxd 12/12/07 10:09 PM Page S30

Managing Diarrhea in Clinical Practice
VOL. 7 SUPPL. 3 2007 REVIEWS IN GASTROENTEROLOGICAL DISORDERS S31
TreatmentSpecific TreatmentsIf a specific cause for diarrhea is dis-covered, therapy aimed at that prob-lem can cure or mitigate the problem.Not every specific cause has a specific
treatment, however, and there remainsa very real need for symptomatic ther-apy with nonspecific antidiarrhealdrugs in many patients.1-4
Specific treatments are sometimesused empirically to establish a
diagnosis. Examples include thera-peutic trials of pancreatic enzymesfor pancreatic exocrine insufficiencyor bile acid–binding resins for bileacid–induced diarrhea. General rulesfor such therapeutic trials are: a) to
Table 2Major Causes of Chronic Diarrhea
Secretory Diarrhea Osmotic Diarrhea Inflammatory Diarrhea Fatty Diarrhea
Nonosmotic laxative abuse
Congenital electrolyte malabsorption
Bacterial toxins
Ileal bile acid malabsorption
Inflammatory bowel diseaseIleal Crohn’s diseaseLymphocytic colitisCollagenous colitisDiverticulitis
Vasculitis
Drugs and poisons
Disordered regulationPostvagotomyPostsympathectomyDiabetic neuropathyHyperthyroidismAddison’s diseaseIrritable bowel syndromeFunctional diarrhea
Neuroendocrine tumorsGastrinomaVIPomaSomatostatinomaMastocytosisCarcinoid syndromeMedullary carcinoma of the thyroid
NeoplasiaCarcinoma of colonLymphomaVillous adenoma
Epidemic secretory diarrhea(Brainerd)
Idiopathic secretory diarrhea(Sporadic)
Osmotic laxative abuseMg��, SO4
�2, PO4�3,
lactulose, polyethyl-ene glycol
Carbohydrate malabsorption
Inflammatory bowel diseaseUlcerative colitisCrohn’s diseaseDiverticulitisUlcerative jejunoileitis
InfectionsInvasive bacterial infection
Clostridium, Escherichiacoli, tuberculosis, others
Ulcerating viral infectionCytomegalovirus,Herpes simplex
Invasive parasitesAmebiasis
Ischemic colitis
Radiation enterocolitis
NeoplasiaCarcinoma of colonLymphoma
Malabsorption syndromesMucosal diseasesShort bowel syndromePostresection diarrheaSmall bowel bacterialovergrowth
Mesenteric ischemia
MaldigestionPancreatic insufficiencyReduced luminal bile acid
Data from Schiller LR and Sellin JH1 and Fine KD and Schiller LR.3
RIGDCME_12-12.qxd 12/12/07 10:09 PM Page S31

Managing Diarrhea in Clinical Practice continued
S32 VOL. 7 SUPPL. 3 2007 REVIEWS IN GASTROENTEROLOGICAL DISORDERS
Table 3Drugs Associated With Diarrhea
Category Drug Category Drug
Acetylcholinesterase Donepezilinhibitors Galantamine
TacrineAminosalicylate drugs Balsalazide
MesalamineOlsalazineSulfasalazine
Antacids and gastric acid Magnesium-containing antacidssecretion inhibitors Histamine-2 receptor antagonists
Proton pump inhibitorsAntibiotics and antiviralsAntidepressants Selective serotonin reuptake
inhibitorsAntiepileptics Lamotrigine
Tiagabine Valproic acid Zonisamide
Antiestrogens Anastrozole Letrozole Tamoxifen
Antihypertensives ACE inhibitorsAngiotensin II-receptor
antagonistsBeta-adrenergic receptor
antagonistsAnti-inflammatory and Colchicine
arthritis drugs Leflunomide Nonsteroidal anti-
inflammatory drugs Antineoplastic agents Alemtuzumab
BicalutamideCapecitabine Cis-platinumDoxorubicin Estramustine Imatinib Levamisole Paclitaxel Temozolomide Vinorelbine
Antiparkinson’s disease Entacapone drugs and drugs used in Glatiramer acetate neurological diseases Riluzole
Tolcapone
Antiplatelet drugs AnagrelideDipyridamoleTiclopidine
Asthma preparations AminophyllinInhaled steroids
Biologicals Erythropoietin analogsInterferonsOprelvekinVaccines
Chelation therapy Penicillamine Succimer
Cholesterol reducers Gemfibrozil HMG-CoA reductase
inhibitorsNiacin
Diabetes medications AcarboseMetforminOral hypoglycemicsRepaglinide Rosiglitazone
DigoxinDiuretics AmilorideImmunosuppressive drugs Cyclosporine
Mycophenolate mofetil SirolimusTacrolimus
LaxativesMegestrolModafinil Osteoporosis treatment BisphosphonatesPheochromocytoma therapy Metyrosine Phosphodiesterase inhibitors Cilostazol
Sildenafil PilocarpineProstaglandin analog MisoprostolProtease inhibitors Amprenavir
FosamprenavirIndinavirLopinavir/ritonavirRitonavirSaquinavirNelfinavir
QuinidineSevelamerThalidomideTretinoin
ACE, angiotensin-converting enzyme; HMG-CoA, 3-hydroxy-3-methylglutaryl coenzyme A. Adapted with permission from Schiller LR.11
RIGDCME_12-17.qxd 12/18/07 1:48 AM Page S32

Managing Diarrhea in Clinical Practice
VOL. 7 SUPPL. 3 2007 REVIEWS IN GASTROENTEROLOGICAL DISORDERS S33
History
Physicalexamination
Onset Congenital Abrupt Gradual
Pattern Continuous IntermittentDuration
Epidemiology Travel Food Water
Aggravatingfactors Diet Stress
Mitigatingfactors Diet OTC drugs Rx drugs
Previousevaluation
Iatrogenicdiarrhea Drugs Radiation Surgery
Factitiousdiarrhea Laxatives
General Fluid balance Nutrition
Skin Flushing Rashes Dermato- graphism
Abdomen Hepatomegaly Mass Ascites Tenderness
Anorectal Sphincter competence Fecal occult blood test
Thyroid Mass
Chest Wheezing
Extremities Edema
Heart Murmur
Systemic diseases Hyperthyroidism Diabetes mellitus Collagen-vascular diseases Tumor syndromes AIDS Ig deficiencies
Stoolcharacteristics Watery Bloody Fatty
Fecalincontinence
Initial Approach to Chronic Diarrhea: I
Abdominalpain Inflammatory bowel disease Irritable bowel syndrome IschemiaWeight loss Malabsorption Neoplasm
Routinelaboratorytests
Stoolanalysis
Categorize
Weight
OsmoticSecretory
Watery diarrhea Inflammatory diarrhea Fatty diarrhea
Laxativescreen
Electrolytes Osmotic gap
pH Carbohydrate malabsorption
Fecaloccultblood test Bleeding
Stool WBCs Inflammation
Fat output Sudan stain Quantitative
Complete blood count Anemia Leukocytosis
Chemistry screen Fluid/electrolyte status Nutritional status Serum protein/globulin
Initial Approach to Chronic Diarrhea: II
Figure 2. Scheme for the initial evaluation and classification of chronic diarrhea. AIDS, acquired immune deficiency syndrome; Ig, immunoglobulin; OTC, over the counter;Rx, prescription; WBCs, white blood cells. Reprinted with permission from Fine KD and Schiller LR.3
RIGDCME_12-12.qxd 12/12/07 10:09 PM Page S33

Managing Diarrhea in Clinical Practice continued
S34 VOL. 7 SUPPL. 3 2007 REVIEWS IN GASTROENTEROLOGICAL DISORDERS
use a high enough dose of the drug toproduce the desired effect, and b) tomeasure a clinically relevant endpoint(eg, fecal fat excretion or stool weight)to prove effectiveness. Trials with in-sufficient doses or without hard end-points are likely to be equivocal.3
Symptomatic TherapyNonspecific or symptomatic therapyis helpful in many patients with diar-rhea. Potential benefits include reduc-tion in stool frequency and more rest-ful sleep, increased productivity due toreduction of symptoms during the day,and reduced fluid losses, permitting
easier maintenance of hydration andelectrolyte balance. In patients withchronic diarrhea, reduction of food-stimulated bowel movements by an-tidiarrheal drugs may allow for betternutrition as food intake can increasewithout causing more diarrhea. Asso-ciated symptoms of fecal inconti-nence also may be improved by bettercontrol of diarrhea.
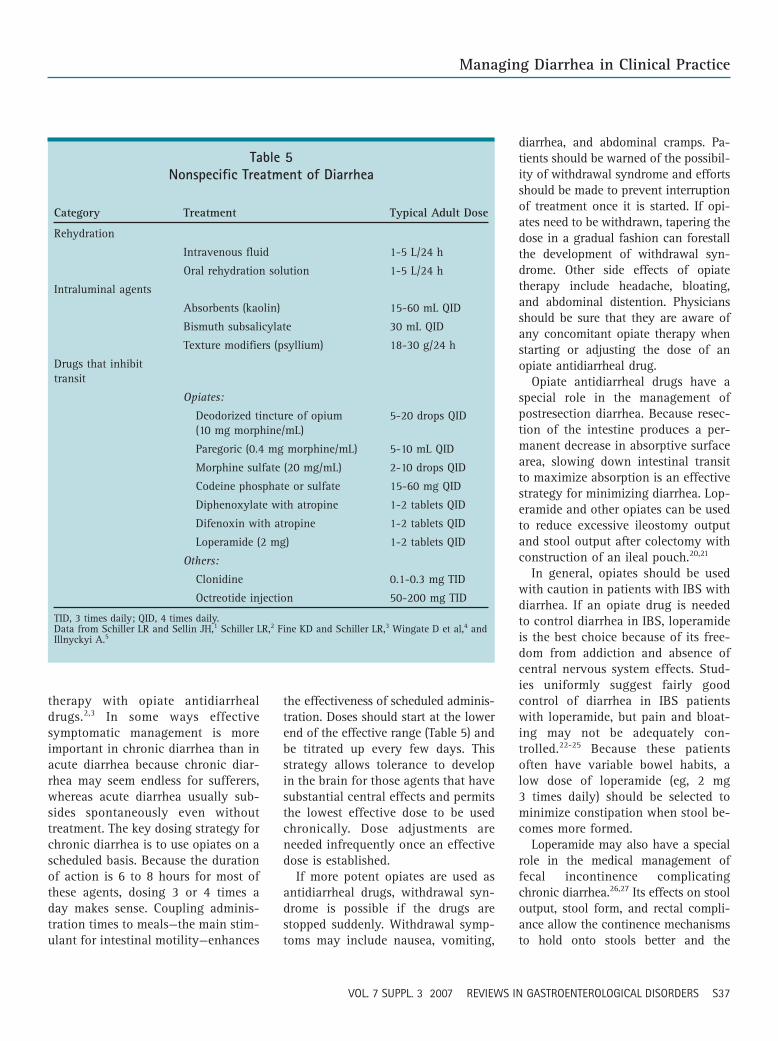
Several different categories ofnonspecific therapies can be used(Table 5).1-5
Rehydration is life saving whendiarrhea is severe. Daily losses of upto 500 g of stool usually do notrequire any special efforts at rehy-dration as long as oral intake ismaintained. However, patients withvomiting can become dehydratedwith fecal losses of this magnitude.Stool weights above 1000 g/24 h fre-quently compromise fluid balanceand may be associated with dehydra-tion and electrolyte imbalance. If thepatient is not vomiting, oral rehydra-tion solutions work well to maintainfluid balance, but they do not de-crease stool output. Diarrhea actuallymay become worse with rehydrationsolution, but urine output increasesif intake of the solution is adequate.
Secretorydiarrhea
Excludeinfection
Selectivetesting
Small-bowelradiographs
Sigmoidoscopyor colonoscopywith biopsy
Cholestyraminetrial for bile aciddiarrhea
CT scan ofabdomen
Small-bowelbiopsy andaspirate forquantitativeculture
Excludestructuraldisease
Bacterialpathogens “Standard” Aeromonas Plesiomonas
Other pathogens “Standard” ova � parasites Coccidia Microsporidia Giardia antigen Cryptosporidium antigen
Plasma peptides Gastrin Calcitonin VIP Somatostatin
Other tests TSH ACTH stimulation Serum protein electrophoresis Immunoglobulins
Urine 5-HIAA Metanephrines Histamine
Chronic Secretory Diarrhea
Osmoticdiarrhea
Stoolanalysis
Low pH Carbohydrate malabsorption
Dietary reviewBreath H2 test (lactose)Lactase assay
High mgoutput Inadvertent ingestion Laxative abuse
Chronic Osmotic Diarrhea
Figure 3a. Scheme for evaluation of secretory diarrhea. ACTH, corticotropin; CT, computed tomography; 5-HIAA,5-hydroxyindoleacetic acid; TSH, thyroid-stimulating hormone; VIP, vasoactive intestinal peptide. Reprinted withpermission from Fine KD and Schiller LR.3
Figure 3b. Scheme for evaluation of osmoticdiarrhea. H2, hydrogen. Reprinted with per-mission from Fine KD and Schiller LR.3
RIGDCME_12-12.qxd 12/12/07 10:09 PM Page S34
Managing Diarrhea in Clinical Practice
VOL. 7 SUPPL. 3 2007 REVIEWS IN GASTROENTEROLOGICAL DISORDERS S35
Inflammatorydiarrhea
Excludestructuraldisease
CT scan ofabdomen
Small-bowelbiopsy
Excludeinfection
Small-bowelradiographs
Sigmoidoscopy orcolonoscopy withbiopsy
Bacterialpathogens “Standard” Aeromonas Plesiomonas Tuberculosis
Other pathogens Parasites Viruses
Chronic Inflammatory Diarrhea
Fattydiarrhea
Excludestructuraldisease
CT scan ofabdomen
Excludepancreaticexocrineinsufficiency
Small-bowelradiographs
Secretintest
Empiric trialof pancreaticenzymes
Stoolchymotrypsinactivity
Small-bowelbiopsy andaspirate forquantitativeculture
Chronic Fatty Diarrhea
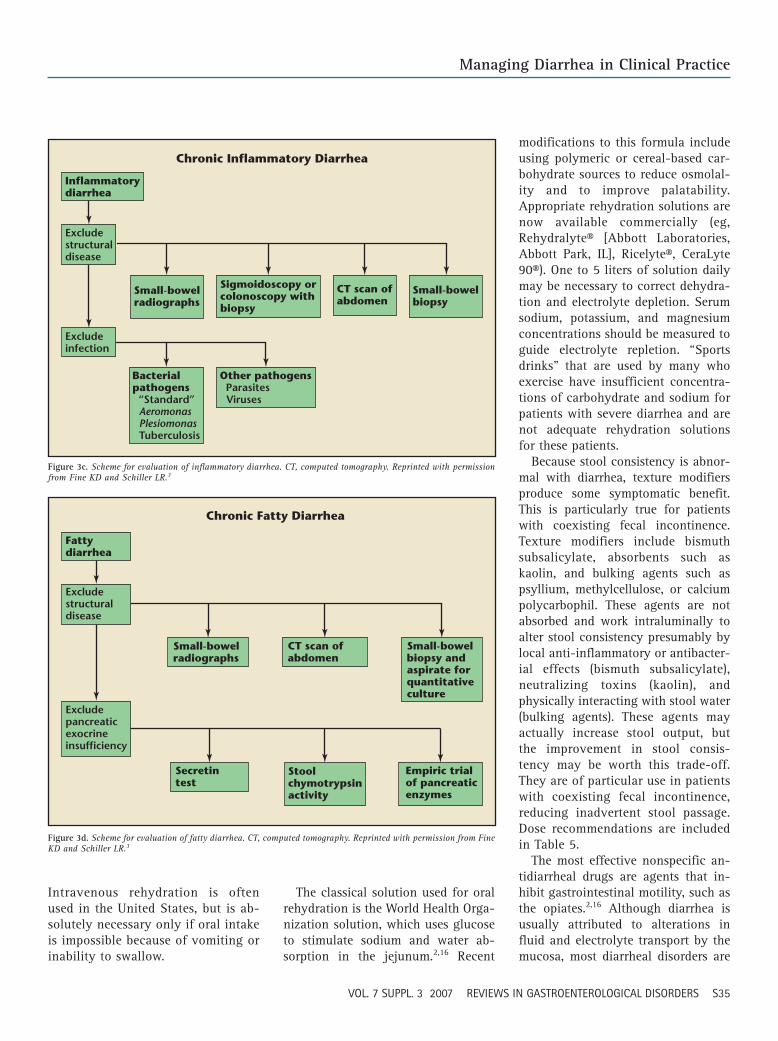
Figure 3d. Scheme for evaluation of fatty diarrhea. CT, computed tomography. Reprinted with permission from FineKD and Schiller LR.3
Figure 3c. Scheme for evaluation of inflammatory diarrhea. CT, computed tomography. Reprinted with permissionfrom Fine KD and Schiller LR.3
modifications to this formula includeusing polymeric or cereal-based car-bohydrate sources to reduce osmolal-ity and to improve palatability.Appropriate rehydration solutions arenow available commercially (eg,Rehydralyte® [Abbott Laboratories,Abbott Park, IL], Ricelyte®, CeraLyte90®). One to 5 liters of solution dailymay be necessary to correct dehydra-tion and electrolyte depletion. Serumsodium, potassium, and magnesiumconcentrations should be measured toguide electrolyte repletion. “Sportsdrinks” that are used by many whoexercise have insufficient concentra-tions of carbohydrate and sodium forpatients with severe diarrhea and arenot adequate rehydration solutionsfor these patients.
Because stool consistency is abnor-mal with diarrhea, texture modifiersproduce some symptomatic benefit.This is particularly true for patientswith coexisting fecal incontinence.Texture modifiers include bismuthsubsalicylate, absorbents such askaolin, and bulking agents such aspsyllium, methylcellulose, or calciumpolycarbophil. These agents are notabsorbed and work intraluminally toalter stool consistency presumably bylocal anti-inflammatory or antibacter-ial effects (bismuth subsalicylate),neutralizing toxins (kaolin), andphysically interacting with stool water(bulking agents). These agents mayactually increase stool output, butthe improvement in stool consis-tency may be worth this trade-off.They are of particular use in patientswith coexisting fecal incontinence,reducing inadvertent stool passage.Dose recommendations are includedin Table 5.
The most effective nonspecific an-tidiarrheal drugs are agents that in-hibit gastrointestinal motility, such asthe opiates.2,16 Although diarrhea isusually attributed to alterations influid and electrolyte transport by themucosa, most diarrheal disorders are
Intravenous rehydration is oftenused in the United States, but is ab-solutely necessary only if oral intakeis impossible because of vomiting orinability to swallow.
The classical solution used for oralrehydration is the World Health Orga-nization solution, which uses glucoseto stimulate sodium and water ab-sorption in the jejunum.2,16 Recent
RIGDCME_12-12.qxd 12/12/07 10:09 PM Page S35

Managing Diarrhea in Clinical Practice continued
S36 VOL. 7 SUPPL. 3 2007 REVIEWS IN GASTROENTEROLOGICAL DISORDERS
Table 4Rome Criteria for Irritable Bowel Syndrome
• Recurrent abdominal pain or discomfort (at least 3 days per month over the last 3 months) that is associated with 2 or more of the following:
✓ Relieved by defecation
✓ Onset associated with a change in stool frequency
✓ Onset associated with a change in stool form or appearance
• Supporting symptoms include:
✓ Altered stool frequency
✓ Altered stool form
✓ Altered stool passage (straining and/or urgency)
✓ Mucus in stools
✓ Abdominal bloating or subjective distention
• Bowel movement patterns:
✓ Diarrhea predominant
✓ Constipation predominant
✓ Mixed diarrhea and constipation
Adapted from Longstreth GF et al.12
associated with rapid transit throughthe small intestine and/or colon.Slowing the movement of fluid bo-luses through the intestine allowsmore time for absorption by the mu-cosa and, therefore, the total amountsof fluid and electrolytes absorbed in-crease even though the rates of ab-sorption may not change. Thisscheme depends on the ability of theintestine to absorb some fluid andelectrolytes; conditions like cholera inwhich absorption is not possible donot respond to therapy with opiates.
Opiates work by interacting withmu-opiate receptors located in themucosa, enteric nervous system, andcentral nervous system.2 The potencyof opiates used as antidiarrheal drugsvaries widely. Loperamide, diphe-noxylate, and difenoxin have moder-ate potency, whereas codeine, mor-phine, and opium have moresubstantial potency related to recep-tor occupancy, absorbability, and the
presence of central effects. Most pa-tients with diarrhea respond to themoderately potent agents, which aresubject to less stringent controlled-drug regulation. Loperamide is rela-tively poorly absorbed and does notcross the blood–brain barrier readily,making it unlikely to be abused; it isno longer a controlled substance inthe United States and even is avail-able over the counter. Diphenoxylateand difenoxin are still available byprescription only with a small amountof atropine added to discourageabuse. Codeine, morphine, and de-odorized tincture of opium are cate-gory II controlled substances and re-quire special prescription blanks insome states. Although these drugs canbe abused and their use must be mon-itored closely, most patients with se-vere diarrhea appreciate the relief thatthey afford and will not jeopardizetheir access to the drugs by abusingthem. The potent opiates should only
be used when less potent agents failfor patients with severe diarrhea.
When used for treating acute diar-rhea, opiates should be titrated up bygiving doses after each bowel move-ment until the diarrhea abates.2,4 Thisreduces the chance that too muchmedication will be given and increasesthe chance that an effective dose willbe given promptly. Maximum dosetargets are shown in Table 5. Becausemost cases of acute diarrhea resolvepromptly and spontaneously, this dos-ing scheme assures that the antidiar-rheal drug will be withdrawn as theunderlying condition improves.
Loperamide has been studied inadults and children greater than 2 yearsold with acute diarrhea.17-19 In gen-eral, it reduces the duration of loosestools in both groups and may helpwith some of the additional symptomsexperienced by these patients (eg,cramps and urgency). Adding lo-peramide to antibiotic therapy short-ens the course of travelers’ diarrhea.6,7
It has been relatively safe in con-trolled studies, although some side ef-fects were more frequent in the grouptreated with loperamide.8,17-19
Concerns that treating acute infec-tious diarrhea with an agent that im-pedes motility might delay clearanceof the pathogen from the gut largelyhave not been confirmed in con-trolled trials, but some individualcases where this may have occurredhave been reported. Opiate antidiar-rheal drugs are contraindicated inpseudomembranous colitis due to an-tibiotic use, bloody diarrhea or dysen-tery, diarrhea due to enteroinvasiveorganisms like Shigella spp., andacute ulcerative colitis that could becomplicated by megacolon. The mostfrequent adverse effect seen whenthese agents are used to treat acutediarrhea is “rebound” constipationonce the infection has cleared.
Chronic diarrhea of virtually anycause may also respond to nonspecific
RIGDCME_12-12.qxd 12/12/07 10:09 PM Page S36
Managing Diarrhea in Clinical Practice
VOL. 7 SUPPL. 3 2007 REVIEWS IN GASTROENTEROLOGICAL DISORDERS S37
therapy with opiate antidiarrhealdrugs.2,3 In some ways effectivesymptomatic management is moreimportant in chronic diarrhea than inacute diarrhea because chronic diar-rhea may seem endless for sufferers,whereas acute diarrhea usually sub-sides spontaneously even withouttreatment. The key dosing strategy forchronic diarrhea is to use opiates on ascheduled basis. Because the durationof action is 6 to 8 hours for most ofthese agents, dosing 3 or 4 times aday makes sense. Coupling adminis-tration times to meals—the main stim-ulant for intestinal motility—enhances
the effectiveness of scheduled adminis-tration. Doses should start at the lowerend of the effective range (Table 5) andbe titrated up every few days. Thisstrategy allows tolerance to developin the brain for those agents that havesubstantial central effects and permitsthe lowest effective dose to be usedchronically. Dose adjustments areneeded infrequently once an effectivedose is established.
If more potent opiates are used asantidiarrheal drugs, withdrawal syn-drome is possible if the drugs arestopped suddenly. Withdrawal symp-toms may include nausea, vomiting,
diarrhea, and abdominal cramps. Pa-tients should be warned of the possibil-ity of withdrawal syndrome and effortsshould be made to prevent interruptionof treatment once it is started. If opi-ates need to be withdrawn, tapering thedose in a gradual fashion can forestallthe development of withdrawal syn-drome. Other side effects of opiatetherapy include headache, bloating,and abdominal distention. Physiciansshould be sure that they are aware ofany concomitant opiate therapy whenstarting or adjusting the dose of anopiate antidiarrheal drug.
Opiate antidiarrheal drugs have aspecial role in the management ofpostresection diarrhea. Because resec-tion of the intestine produces a per-manent decrease in absorptive surfacearea, slowing down intestinal transitto maximize absorption is an effectivestrategy for minimizing diarrhea. Lop-eramide and other opiates can be usedto reduce excessive ileostomy outputand stool output after colectomy withconstruction of an ileal pouch.20,21
In general, opiates should be usedwith caution in patients with IBS withdiarrhea. If an opiate drug is neededto control diarrhea in IBS, loperamideis the best choice because of its free-dom from addiction and absence ofcentral nervous system effects. Stud-ies uniformly suggest fairly goodcontrol of diarrhea in IBS patientswith loperamide, but pain and bloat-ing may not be adequately con-trolled.22-25 Because these patientsoften have variable bowel habits, alow dose of loperamide (eg, 2 mg 3 times daily) should be selected tominimize constipation when stool be-comes more formed.
Loperamide may also have a specialrole in the medical management offecal incontinence complicatingchronic diarrhea.26,27 Its effects on stooloutput, stool form, and rectal compli-ance allow the continence mechanismsto hold onto stools better and the
Table 5Nonspecific Treatment of Diarrhea
Category Treatment Typical Adult Dose
Rehydration
Intravenous fluid 1-5 L/24 h
Oral rehydration solution 1-5 L/24 h
Intraluminal agents
Absorbents (kaolin) 15-60 mL QID
Bismuth subsalicylate 30 mL QID
Texture modifiers (psyllium) 18-30 g/24 h
Drugs that inhibit transit
Opiates:
Deodorized tincture of opium 5-20 drops QID(10 mg morphine/mL)
Paregoric (0.4 mg morphine/mL) 5-10 mL QID
Morphine sulfate (20 mg/mL) 2-10 drops QID
Codeine phosphate or sulfate 15-60 mg QID
Diphenoxylate with atropine 1-2 tablets QID
Difenoxin with atropine 1-2 tablets QID
Loperamide (2 mg) 1-2 tablets QID
Others:
Clonidine 0.1-0.3 mg TID
Octreotide injection 50-200 mg TID
TID, 3 times daily; QID, 4 times daily.Data from Schiller LR and Sellin JH,1 Schiller LR,2 Fine KD and Schiller LR,3 Wingate D et al,4 andIllnyckyi A.5
RIGDCME_12-12.qxd 12/12/07 10:09 PM Page S37

Managing Diarrhea in Clinical Practice continued
S38 VOL. 7 SUPPL. 3 2007 REVIEWS IN GASTROENTEROLOGICAL DISORDERS
rectum to behave as a better reservoirfor feces. Both effects may minimizeaccidental passage of stool.
Dr. Schiller has indicated that he has norelationships or activities to disclose thatcould be perceived as potential conflictsof interest.
References1. Schiller LR, Sellin JH. Diarrhea. In: Feldman M,
Friedman L, Brandt LJ, eds. Sleisenger & Ford-tran’s Gastrointestinal and Liver Disease, 8th ed.Philadelphia, PA: WB Saunders Co., 2006:159-186.
2. Schiller LR. Review article: anti-diarrhoeal phar-macology and therapeutics. Aliment PharmacolTher. 1995;9:87-106.
3. Fine KD, Schiller LR. AGA technical review onthe evaluation and management of chronic diar-rhea. Gastroenterology. 1999;116:1464-1486.
4. Wingate D, Phillips SF, Lewis SJ, et al. Guide-lines for adults on self-medication for the treat-ment of acute diarrhoea. Aliment PharmacolTher. 2001;15:773-782.
5. Ilnyckyi A. Clinical evaluation and managementof acute infectious diarrhea in adults. Gastroen-terol Clin North Am. 2001;30:599-609.
6. Panos GZ, Betsi GI, Falagas ME. Systematicreview: are antibiotics detrimental or beneficialfor the treatment of patients with Escherichiacoli O157:H7 infection? Aliment PharmacolTher. 2006;24:731-742.
7. McFarland LV, Elmer GW, Surawicz CM. Break-ing the cycle: treatment strategies for 163 cases
of recurrent Clostridium difficile disease. Am JGastroenterol. 2002;97:1769-1775.
8. Dupont HL, Jiang ZD, Belkind-Gerson J, et al.Treatment of travelers’ diarrhea: randomizedtrial comparing rifaximin, rifaximin plus lo-peramide, and loperamide alone. Clin Gastroen-terol Hepatol. 2007;5:451-456.
9. Ericsson CD, Dupont HL, Okhuysen PC, et al. Lop-eramide plus azithromycin more effectively treatstravelers’ diarrhea in Mexico than azithromycinalone. J Travel Med. 2007;14:312-319.
10. Schiller LR. Diarrhea. Med Clin North Am. 2000;84:1259-1274.
11. Schiller LR. Evaluation of chronic diarrhea. In:The Requisites in Gastroenterology. Edited byRustgi AK. Volume 2: Small and Large Intestine.Edited by Lichtenstein GR, Wu GD. St. Louis,MO: Mosby, 2004:31-51.
12. Longstreth GF, Thompson WG, Chey WD, et al.Functional bowel disorders. Gastroenterology.2006;130:1480-1491.
13. Shepherd SJ, Gibson PR. Fructose malabsorptionand symptoms of irritable bowel syndrome:guidelines for effective dietary management. JAm Diet Assoc. 2006;106:1631-1639.
14. Frissora CL, Cash BD. Review article: the role ofantibiotics vs. conventional pharmacotherapyin treating symptoms of irritable bowelsyndrome. Aliment Pharmacol Ther. 2007;25:1271-1281.
15. Alaedini A, Green PHR. Narrative review: celiacdisease: understanding a complex autoimmunedisorder. Ann Intern Med. 2005;142:289-298.
16. Schiller LR. Chronic diarrhea. Curr Treat OptionsGastroenterol. 2005;8:259-266.
17. Hanauer SB, Dupont HL, Cooper KM, LaudadioC. Randomized, double-blind, placebo-controlledclinical trial of loperamide plus simethicone ver-
sus loperamide alone and simethicone alone inthe treatment of acute diarrhea with gas-relatedabdominal discomfort. Curr Med Res Opin. 2007;23:1033-1043.
18. Kaplan MA, Prior MJ, McKonly KI, et al. A mul-ticenter randomized controlled trial of a liquidloperamide product versus placebo in the treat-ment of acute diarrhea in children. Clin Pediatr(Phila). 1999;38:579-591.
19. Li ST, Grossman DC, Cummings P. Loperamidetherapy for acute diarrhea in children: system-atic review and meta-analysis. PLoS Med. 2007;27:4:e98.
20. Dupont AW, Sellin JH. Ileostomy diarrhea. CurrTreat Options Gastroenterol. 2006;9:39-48.
21. Herbst F, Kamm MA, Nicholls RJ. Effects of lo-peramide on ileoanal pouch function. Br J Surg.1998;85:1428-1432.
22. Chang HY, Kelly EC, Lembo AJ. Current gut-directed therapies for irritable bowel syndrome.Curr Treat Options Gastroenterol. 2006;9:314-323.
23. Hadley SK, Garder SM. Treatment of irritablebowel syndrome. Am Fam Physician. 2005;72:2501-2506.
24. Lesbros-Pantoflickova D, Michetti P, Fried M, et al.Meta-analysis: the treatment of irritable bowelsyndrome. Aliment Pharmacol Ther. 2004;20:1253-1269.
25. Efskind PS, Bernklev T, Vatn MH. A double-blindplacebo-controlled trial with loperamide in irri-table bowel syndrome. Scand J Gastroenterol.1996;31:463-468.
26. Scarlett Y. Medical management of fecal incon-tinence. Gastroenterology. 2004;126(1 Suppl 1):S55-S63.
27. Cheetham M, Brazzelli M, Norton C, Glazener CM.Drug treatment for faecal incontinence in adults.Cochrane Database Syst Rev. 2003;3:CD002116.
Main Points• Diarrhea can be a symptom of many different conditions; therefore, it is best to organize the differential diagnosis of diarrhea by
duration into acute diarrhea, typically lasting a few days or less than 4 weeks, and chronic diarrhea, lasting more than 4 weeks.
• Bacterial and viral infections account for the vast majority of acute diarrheas. One of several common clinical scenarios is travelers’diarrhea. Although a number of different organisms may be responsible, empiric antibiotic therapy can be used in most patients toshorten the duration of the diarrhea, with the addition of an antidiarrheal drug such as loperamide to speed resolution.
• Chronic diarrhea is less likely to be due to infection than acute diarrhea and has a broader differential diagnosis. Often the historyprovides an obvious clue that precludes the need for an extensive evaluation; other times the differential diagnosis can be so broadthat it must be made more manageable by categorizing the diarrhea by stool characteristics such as watery, inflammatory, or fatty.
• If a specific cause for diarrhea is discovered, therapy aimed at that problem can cure or mitigate the problem. However, not everyspecific cause has a specific treatment and there remains a very real need for symptomatic therapy with nonspecific antidiarrhealdrugs in many patients.
• Several symptomatic therapies are helpful in the treatment of diarrhea: rehydration, use of intraluminal agents such as kaolin andbismuth subsalicylate, and treatment with agents that inhibit gastrointestinal motility, including opiates such as loperamide.
• Loperamide has been proven to reduce the duration of loose stools in adults and children greater than 2 years of age with acutediarrhea; it has been used to reduce excessive ileostomy output and stool output after colectomy with construction of an ilealpouch; and its effects on stool output, stool form, and rectal compliance may serve a role in the medical management of fecalincontinence complicating chronic diarrhea. Additionally, if an opiate drug is needed to control diarrhea in irritable bowel syn-drome, loperamide is the optimal choice because of its freedom from addiction and absence of central nervous system effects.
RIGDCME_12-12.qxd 12/12/07 10:09 PM Page S38