Embed Size (px)
Citation preview

Ginical Practice
Management ofHigh-Risk Pregnancy:Report of a Combined Obstetrical andNeonatal Intensive Care Unit
SUMMARY..The methodology, equipment and personnel requiredto carry out an intensive-care program in the management of high-riskpregnancies have been outlined. The perinatal mortality rate has been de¬termined and its etiology has been analyzed.
There appear to be three conditions in which the degree of high riskis such as to warrant provision of the complete facilities of the service we
described, viz., (a) severe pre-eclampsia; (b) marked intrauterine growthretardation with placental insufficiency as determined from serial measure¬ments of uterine growth and estriol determinations; and (c) irreversiblelabour in premature pregnancies where a birth weight of 2200 g. or lessis anticipated. Numerous other conditions that we have monitored haveperhaps had their good outcome because of monitoring facilities. A lesssophisticated and more easily applied method of monitoring should beavailable within the context of routine labour and delivery rooms.
There is a pressing need to re-evaluate and change some of our
methods of educating our undergraduate, postgraduate and practisingphysicians and to provide continuing education in the realm of prenatalcare and recognition of high-risk pregnancy. Regionalization and centrali-zation of this type of intensive care for high-risk pregnancies are required.
Indispensable to the success of this type of project is the incorpora¬tion, without physical, emotional or intellectual barriers, of both a pedia¬tric and an obstetrical component within the intensive-care unit.
Any attempt to improve thequality of perinatal care must as¬
sess and implement advances indiagnosis and management of con¬
ditions hazardous to the ante-partum, intrapartum and neonatalorganism. Some of the newer tech¬niques used to assess fetal reserve
and placental function must bestandardized, and their risk assessedand balanced against the benefitsthat may accrue. The practicality ofapplication of these techniques and
S. B. EFFER,M.D., F.R.C.S.[C],*
London, Ont.
neonatal aspects of perinatal wast-age and morbidity.ANTEPARTUMMANAGEMENTAn already existing area of 14
antepartum beds was selected tocare for high-risk complications ofpregnancy. This area is adjacent tothe labour unit and to the Obstet¬rical and Neonatal Intensive CareUnit (O.N.I.C.U.).
Patients are freely admitted tothis ward by their private or staffattending physician or obstetrician.A team of house staff, consisting ofa junior rotating intern, a residentin a family practice course and anobstetrical resident, see each patientevery morning. They are assisted bya team of specially trained nurseswho are conversant with the specialprocedures used in assessing feto-placental status, as well as fetalcardiovascular and biochemicalmonitoring procedures.
In this group of high-risk preg¬nancies, investigations include sys¬tematic hematological and hormonal(estriols) values, uterine growthcurves, nutritional and electrolytebalance, placental transfer tests,fetal electrocardiography and am¬
niotic fluid studies.In addition, a scoring system, re¬
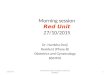
cently described,1 was used to pre¬dict perinatal mortality. Each pa¬tient has a "prognostic risk score"(PRS) assigned at the onset oflabour. This score includes pathol¬ogical factors, function tests, pa¬tient vital statisties, such as age,height, weight, ethnic origin andeconomic status, and a completephysical examination. After thecurrent statistical evaluation of thevalidity of this system of scoring(Fig. 1), it is hoped to developfurther systems able to predict, atearlier stages of gestation, pregnan¬cies needing further investigation.The resident team freely consults
with the Obstetrical Director of theO.N.I.C.U. and incorporates the ad¬vice given in their discussions withthe patient's attending doctor. This
This project was supported by the Ontario Hospital Services Commission Pilot Project andthe R. G. Ivey Foundation.?Assistant Professor, Department of Obstetrics and Gynecology, University of Western Ontario,St. Joseph's Hospital, London, Ontario. Present address: Associate Professor, Department ofObstetrics and Gynecology, McMaster University, Hamilton, Ontario.Reprint requests to: Dr. S. B. Effer, Department of Obstetrics and Gynecology, McMaster Uni¬versity Clinic, Hamilton General Hospital, Hamilton, Ontario.
the provision of the facilities to im¬plement them must be weighedagainst the cost on the one handand the possible improvement insurvival and health on the other.The ability to pre-select the popu¬lation which can benefit from thesemethods, and the willingness to al¬ter our concepts of medical care inorder that this service will be ac-cessible to this population are pre-requisites to any serious attempt toimprove the quality of perinatalcare.
The program which we will out¬line is aimed at looking separatelyat antepartum, intrapartum and
Canad. Med. Ass. J., Oct. 4, 1969, vol. 101.389 55

IO
9
A
A .
JMIN,
t
i:XX .. .. J : .* !. ! .
.?«:;.:.... . .:
: .
. .
.:: #. r«o.7i
. .
K> X> MOSOSTK
400 sootISK
FIG. 1..Multiple weighting factors are added and correction factors applied to produce a "prognostic risk score" which isplotted against one-minute Apgar score.
whole team then together arrives ata decision regarding the ideal me¬
thod and time of terminating thepregnancy.
INTRAPARTUM CAREAn area of 90 square metres ad¬
jacent to and within 50 metres ofthe labour, antepartum, prematureand neonatal intensive-care areas
was remodelled. This core area con¬
sists of three rooms: a labour anddelivery room equipped to monitorlabour, and for the delivery of thepatient vaginally or by cesarean
section; a contiguous neonatal adap¬tation and resuscitation room; andbetween the first two rooms, a
laboratory equipped with electronicpolygraphs and biochemical bloodmeasuring systems. All three areasintercommunicate by sound andclosed-circuit television to permitcontinuous surveillance by all mem¬bers of the intensive-care team. Thenewborn, immediately upon birth, isgiven to the neonatal resident and/or his consultant, who within 60seconds of birth has the newbornin a heated environment, beingmonitored and resuscitated. Time isnot wasted by the obstetrical staffin applying suction to a baby whocan more safely and effectively belooked after by the neonatalogist,
provided his unit is within 10seconds distance of, i.e. contiguouswith, the delivery room.
Delivery RoomThe labour and delivery room is
staffed by a nurse specially trainedto render expert supportive care tothe patient and to the team of phy¬sicians carrying out biophysical andbiochemical monitoring procedures.The nurse in this unit is drawn fromthe antepartum area, where eachshift has one nurse assigned to theO.N.I.C.U. for patients in labour.
LaboratoryThe technical staff required to
run the laboratory (serving the de¬livery area in which approximately10% of the hospital deliveries oc¬
cur) consists of two full-time elec¬tronic technicians and two bio¬chemistry technicians. It is possibleto manage with this reduced staff,instead of around-the-clock shiftcoverage, by allowing theO.N.I.C.U. Director freedom to ar-
range versatility of working condi¬tions, duties and employee selection.The ideal technical staff for thisarea, with interest in the programand expert technical ability, is dif¬ficult to find because of the unpre-dictability of patient scheduling, the
great differences between fetal andadult monitoring technologicalproblems, and the lack of pre-cedents in this type of work.
Neonatal RoomThe neonatalogists (Drs. N.
Jaco and M. Sutton) and theirteam of residents and intensive-carenurses take over the immediateresuscitative care and further moni¬toring procedures as dictated by theclinical condition (Apgar scores),the cardiovascular adaptation pat¬terns and the blood gas status ofthe newborn in the first half hourof life.
MATERIALS ANDMETHODSThis discussion will be confined
to intrapartum patients admitted tothe O.N.I.C.U. labour and deliveryarea. Patients were referred to theUnit by family physicians, privateobstetricians or resident house staff.The reasons for referral fell intothree major categories: (a) clini¬cally detected fetal distress in pa¬tients already in labour in the rou¬tine labour setting; (b) totalmanagement of labour, of spon¬taneous or induced origin, in pa¬tients to whom had been assignedthe label "high-risk pregnancy"; (c)
56 Canad. Med. Ass. J.. Oct. 4, 1969, vol. 101.390

TABLE I..SUMMARY OF INDICATIONS FOR ADMISSION TO O.N.I.C.U.
July /, 1967 to December 31, 1968
Maternal complications ofpregnancy*
Toxemia. 65Hypertension. 1Urinary tract infection. 0Excess weight gain. 0Diabetes mellitus. 3Prediabetes. 7Rhesus incompatibility. 10Rheumatic fever (valvular disease). 1Varicose veins. 0Epilepsy. 0Chronic chest disease. 0Anemia. 0
Gestational duration pathologyPrematurity. 7Postmaturity. 5Premature rupture of membranes. 8
Placental pathologyPlacenta praevia. 0Abruptio placentae. 10First-trimester bleeding. 1Third-trimester bleeding (uncPd). 5Placental insufficiency. 4Abnormal estriol excretions. 2
No. of cases. *Primary**Secondary
***Other
Fetal distress (clinically detected)*
Fetal bradycardia. 11Fetal tachycardia. 9Fetal heart irregularities. 9Meconium-stained liquor amnii . 3Occult cord prolapse. 0
Uterine factorsProlonged labour. 17Cephalopelvic disproportion. 5Uterine inertia. 1Uterine anomalies. 0Previous uterine surgery. 1Leiomyomata uteri. 0Incompetent cervix. 0Failed induction of labour. 0
History ofPoor obstetrical performance. 13Infertility. 4Elderly gravida. 5No prenatal care. 0Grandmultiparity. 1
Fetal factorsBreech presentations. 2Twin pregnancies. 1
6140
103911
32***
50040
2411110000
23118811
301
a history of perinatal loss(es), cre¬
ating either a high-risk or premium-baby situation.The reassurance afforded to the
attending staff by continuous ob¬servation of fetal status soon cre¬
ated such a demand that more cleardelineation of the service available,and the indications for it, was man-
datory. This information was dis¬seminated to the medical staff ofthe community and surroundingregion by three main methods: (a)a formal presentation by the authorat a quarterly staff meeting; (b)posting of bulletins in key areas ofthe hospital; (c) personal com¬
munications by (1) the O.N.I.C.U.staff with practising physicians and(2) the obstetrical resident, whomaintains a close surveillance onall patients in labour.Two hundred and eleven patients
were admitted and 215 babies were
delivered between July 1, 1967 andDecember 31, 1968. The indica¬tions for admission were coded as
primary, secondary and other(Table I).On admission to the O.N.I.C.U.
a standardized data form was com¬
pleted (Fig. 2). The managementof labour was standardized afterpresenting a protocol to the attend¬ing obstetrical staff for discussionand approval. The protocol covered
controlled analgesia and anesthesia,frequency of vaginal examinations,blood pressure recordings, labour¬ing position of patient, indicationsfor and timing of fetal scalp bloodsampling and other routine pro-
physician, private obstetrician or theUnit Director when specifically re¬ferred to his care. Owing to thenature of the pilot project no eco¬nomic structure has been estab¬lished, and no charges additional to
JJnit No._Age_E.D.C_ Gest'n
Date
PRE-PREGNANT WT._KG. PRESENT Wt._KG. HEIGHT_Uterine Measurements_/._/_: FHR-High_Low_Mean_DELIVERY Apgar-_1 min._5 min._Other/ Birth Time._
Sex_Wt._gm. Length_cm.PLACENTA Wt._gm. Volume_ml. Diams._cm.cervix on admission t0 o.n.i.c.u.
length_cm. Thickness_mm.consistency_position_dilatation_cm. membranes_station_cm. Above_Below_
CMS.
BPM.
SPS.
CORD
w-
Knots_ Around Neck_"YES ~"N0~ YES NO TIMES
Prolapse_Tightly_J_oosely_Other Complications_Done_Not Done_Positive_Negative..
FIG. 2..Data recording sheet.
cedures. The protocol was modi¬fied only to conform to specificmedically indicated situations. Bystandardizing the labour manage¬ment, certain statistical evaluationscan now be made regarding the ef¬ficacy of the management. The pa¬tient was delivered by her attending
those applied to other equivalentclinical situations were made to thepatient.PARAMETERS MONITORED1. Maternal heart rate (MHR)..
This was recorded on a beat-to-beatbasis with a threshold tachometer,
Canad. Med. Ass. J., Oct. 4, 1969, vol. 101.391 57

which used the R wave of thematernal ECG. It was recorded onone channel of an eight-channelGrass Model 7 Polygraph.
2. Maternal blood pressure..In¬direct brachial blood pressureswere recorded with the patient in alateral position at half-hourly inter-
on abdominally placed electrodeswas used or the signal from a Dop-tone pulse detector used to triggerour tachometer.
4. Fetal ECG..The fetal ECGwas sampled occasionally when ab¬normal heart rate patterns becameobvious.
?^ JBJ|||||1
laliftiiiilFIG. 3..Modified spring loaded scalp clip applicator with
silver, silver-chloride scalp electrode.
vals up to 6 cm. of cervical dila¬tation and every 10 minutes there¬after. Femoral artery catheterizationand Statham transducer recordingof blood pressure continuouslywere reserved for specific hyper¬tensive problems.
3. Fetal heart rate (FHR)..When the cervix was dilated 2 to3 cm. or more, favourable, and withadequate descent of the presentingpart, a scalp clip of silver, silver-chloride was applied, using a spe-cially modified long Kelly clamp(Fig. 3). The clip itself was de¬signed after the one described byHon.2 We found that we were ableto insert scalp clips earlier in labourby a blind sterile examining handtechnique, keeping the Kelly clamptips and scalp clip between two ex¬
amining fingers, than by the use ofa cone. The insertion of a cone ina posteriorly positioned cervix weoften found difficult, but this maywell be a matter of personal orien¬tation. The well-applied clip usu¬
ally provided a signal with an R-wave amplitude of 200 to 500 /*V.which, when suitably filtered, was
quite adequate to trigger a thres¬hold tachometer which could dif-ferentiate accurately down to a 0.2to 0.5 beat-per-minute variation. Inorder to achieve this we used aGrass EEG pre-amplifier. Whenclinical conditions did not permitthe artificial rupture of membranes,either cancellation of maternal ECG
5. Intrauterine pressures..Theuterine contractions were monitoredwith a Statham transducer attachedto a normal saline-filled disposableLevin tube inserted transcervicallyafter amniotomy. When the latterwas contraindicated, either a trans-abdominal amniocentesis was car¬
ried out and a p-90 catheter fedthrough a thin-walled 16-gaugeneedle, or a simple tokodynamo-meter was used to identify at leastthe frequency and timing of con¬
tractions.6. Uterine work..A polygraph
integrator was used in some of our
records to determine the area underthe curve of the intrauterine pres¬sure curves, and thus give more
ready assessment of efficacy of oxy-tocin when this agent was necessary.In addition to the above biophysi¬cal parameters, written notes were
inserted on one empty channel ofthe polygraph, accurately timing:drug administrations, vaginal ex¬
aminations and findings, patient po¬sition and any other manipulationsor variables, such as scalp bloodsampling.
7. Biochemical and hematologicalstudies on scalp blood were:
(a) pH; PcOjj?; Po2; 02 satura¬tion; base deficit; bicarbonate.
(b) Microhematocrit.(c) Micro blood sugar in pre-
or frank diabetics and in fetuseswith intrauterine growth retarda¬tion.
(d) Direct Coombs' test, serumbilirubin and hemoglobin in Rh-sensitized patients who had receivedintrauterine transfusions.
8. Cord artery and vein..Allthe above biochemistry was studied,and in addition, electrolytes, serum
proteins with electrophoresis, hemo¬globin electrophoresis, calcium andphosphorus were estimated.
9. Maternal blood samples..Awarmed finger-prick sample wasobtained in order that arterializedcapillary blood gases could be de¬termined. Feto-maternal gradientswere studied.
10. Amniotic fluid cytology, bio¬chemistry and spectrophotometrywere carried out.
DELIVERY
Vaginal delivery was selected un¬
less obstetrical indications for ce¬
sarean section became apparent.Fetal distress, characterized by latedecelerations of the FHR or bypersistent fetal tachycardia, unex¬
plained by maternal tachycardia or
pyrexia, was considered an indica¬tion for cesarean section if vaginaldelivery could not be anticipatedbefore a sum of amplitudes of de¬celerations of 600 beats was at¬tained.6 When these situations ex¬
isted, uterine contractility was in¬hibited, by stopping oxytocin wherethis was being used, and/or by theuse of high-dose isoxuprine hydro¬chloride, until preparations for ce¬sarean section were complete.
NEWBORN MANAGEMENT
By agreement with our neonatalcolleagues, the time of birth wasdefined as the time when the entirefetus was outside the maternal birthtract. Precise one-minute and five-minute Apgar scores were deter¬mined and their components noted.Resuscitation and monitoring of thenewborn heart rate was in progressusually before 60 seconds hadelapsed. Umbilical artery catheteri¬zation was limited to excessivelysmall newborns or to babies inwhom the fetal scalp blood or cordblood showed significant acidosis.All resuscitative and monitoringprocedures were carried out on a
table with an overhead radiantheater; this table was 15 metresfrom the delivery site, with no in-terposing deterring doors.
58 Canad. Med. Ass. J., Oct. 4, 1969, vol. 101.392

STAFF AND PERSONNELMedical PersonnelThe obstetrical team consisted of
one obstetrician director, who isoriented as a perinatal physiologist,one full-time resident, the juniorhouse staff and the attending privatephysician and/or obstetrician.
Nursing PersonnelThe antepartum ward for high-
risk pregnancies was found to re¬
quire a ratio of one nurse to fourpatients on each of the day andevening shifts, and one to six onthe night shift; in addition to theabove, one extra nurse on eachshift was available for O.N.I.C.U.patients in labour. These require¬ments, after pro-rating for time off,sickness and vacation time, placethe total staff requirements at ap¬proximately one nurse per 100 an¬nual deliveries.
Paramedical PersonnelElectronic ..The con¬
stantly available supervision of theequipment by a technician wasfound essential in view of the fre¬quent electronic adjustments andcalibrations required. It was foundthat one full-time technician wouldbe required to handle the load of100 patients per year monitoredin labour. This technical help alsomaintains the equipment and pro¬vides scalp lead manufacture aswell as on-line repairs.
Biochemistry..The carrying outof blood-gas and acid-base estima¬tions of scalp blood at a moment'snotice, the calculation of the valueson line, and the following of bloodgases in the newborn were found torequire two full-time technicians ina setting where 200 to 250 patientsare monitored annually.
Clerical..One full-time clerk isrequired to carry out the scoringprocedures and the computer cod¬ing of data being stored.Computation..Computer coding
and analysis were not used in thisproject, but would facilitate andstandardize findings when such fa¬cilities as ours are offered on an
expanded regionalized basis to out-iying communities.
RESULTSThe 211 patients who were
monitored have been classified ac¬
cording to the diagnostic criteria foradmission to the O.N.I.C.U. (TableI). The results of this study will beoutlined in the main with regard toperinatal mortality and degree ofinfant depression. Detailed correla¬tions of fetal cardiovascular activityand blood-gas studies will be thesubject of a further study.
There were eight perinatal deaths(rate: 37.2/1000 total births). Dur¬ing the same period of study theperinatal mortality in the remainderof the population delivered in our
delivery suite was 28.8/1000. Com¬parison of these two figures is notvalid for two main reasons: (a)No patient who has a stillborn in¬fant is admitted to the O.N.I.C.U.This automatically decreases theO.N.I.C.U. rate, and the factor bywhich it is reduced has been as¬certained by studying the percent¬age of stillbirths which occur beforethe onset of labour, in both themature and premature weightgroups. (b) The cases studied were
high-risk pregnancies exclusively,with an expected poor outcome.Prediction of risk by a scoring sys¬tem may enable one to assess, atleast to some degree, the efficacyof the management undertaken.
PROGNOSTIC MSK SCORESAn attempt was made to find
a quantitative expression of thedegree of risk of perinatal deathfaced by any one patient. Statisticalinformation used to develop thisscoring system was taken from twomain studies: "Supplement to theSecond Report of the PerinatalMortality Study in Ten UniversityTeaching Hospitals, Ontario, Can¬ada";3 and the first report of the1958 British Perinatal MortalitySurvey.4One hundred and fifty-five items
were listed, each with its respectiverisk factor. These factors includedstandard vital statisties, such as
weight, age and height, as well as
epidemiological data, includingplace of birth and place and dura¬tion of residence. Medical, surgicaland obstetrical past and presentcomplications are also included inthe scoring system.The procedure of scanning the
questionnaire and searching throughthe findings of a physical examina¬tion takes approximately 15 to 20minutes when performed by a
medically non-skilled but trained
coding clerk. Each of our 211 pa¬tients was coded with the dataavailable at the onset of labour. Asimilar procedure was applied to a
random group of 350 patients ad¬mitted to the standard labour anddelivery unit of our hospital duringtwo months of our study.Two correction factors were
found necessary to validate thescoring system as applied to our
study patients. One dealt with theexclusion of antepartum stillbirthsfrom our study. This correction fac¬tor was taken from the Britishstudy,4 in which the percentages ofantepartum and intrapartum deathswere ascertained both for premature(under 2500 g.) and mature groupsseparately. This correction factorwas applied after delivery in orderto take into account the birthweight of the infant. The secondcorrection factor was derived frommany factors we considered as hav¬ing an additive score, which ap¬parently did not produce additiverisk. We evaluated the raw scoringof our random non-study group,and found that the actual score ex¬
ceeded the perinatal mortality rate
by a factor of 4.3. Therefore, aftermaking the above first correction,we further divided the score ob¬tained by 4.3 and believe that thisshould represent the perinatal mor¬
tality of our patients as accuratelyas possible.
Using the above two correctionfactors, we would have expected a
total of 10 perinatal deaths in our
study (a rate of 47.8/1000 totalbirths). Our actual results showedeight perinatal deaths (37.2/1000births) (Table III). By this methodof assessment we would assume
that a 20% reduction has beenachieved. We are fully aware of thedifficulties in any comparative statis¬ties in this area, and have tried to
make as valid an approach as pos¬sible by the method described.A bar graph representation of a
frequency histogram of the distri¬bution of the prognostic risk scores
(PRS) showed that 89% of ran¬
dom patients going into labour hada PRS of 50 or less (Fig. 4). Ageneral estimate has frequently sug¬gested that 10% of all pregnancieshave some increased risk. From theabove two statements we wouldsuggest that, using our scoring sys¬tem, any score above 50 representshigh-risk pregnancies.
Canad. Med. Ass. J., Oct. 4, 1969, vol. 101.393 59

In our group of patients moni¬tored as high-risk pregnancies 46%had a score over 50, as opposed tothe 11% in random patients.
Further appraisal of our scoringsystem was made by correlating theprognostic risk score (PRS) withthe outcome in terms of perinatalmortality and infant depression(Fig. 1). There was a good correla¬tion between the one-minute Apgarand the PRS (r = 0.71, P<0.01).
utero is required. Our work in pro¬gress in this area suggests thatsimple measurement of the uterusfrom the superior border of thesymphysis to the fundus uteri, whileby no means free of error, has im¬proved random clinical guessing bya large factor (Fig. 4).Two of our perinatal deaths were
in patients referred from other cen¬tres. We merely point out that thisfactor must be considered when
ftANDOM PATIfNT*control»
SO-** IOO-149
MOONOSTIC
1SO-199 300-349 7SO ?
RISK SCOUt
317 HO 24
FIG. 4..Prognostic risk scores: comparison of frequencydistribution in high-risk group and random group of patients.
PERINATAL MORTALITY
Maturity and weight were crucialfactors in perinatal survival (TableII). There was only one perinataldeath of an infant over 1900 g.; thisinfant had congenital anomalies andweighed 2198 g. With the weight ofthe infant playing such an impor¬tant role in survival, it became in¬creasingly evident that a more ac¬
curate clinical or other method ofpredicting the size of the infant in
comparing statisties, as it will bethe main cause of a rising perinatalmortality rate in any project whichinvolves increasing regionalizationreferral, as we feel it should.One of these referrals from out of
town was a patient in whom pre¬mature labour complicated a hys-terotomy and fetal umbilical arterytransfusion. The fetus and motherremained well for 72 hours follow¬ing restoration of the former to theintrauterine environment. The baby
was born vaginally after failure tocontrol premature labour with ex¬
isting uterine inhibitors, and died ofmarked immaturity (744 g.) (TableII).
PREMATURITYOur high prematurity rate reflects
the high-risk nature of our studygroup. Thirty-eight infants under2500 g. were delivered (17.7%). Agraphic representation of the rela¬tionship of gestation and birthweight, with superimposition ofLubchenco's percentile line, isshown in Fig. 6.5A large number of our patients
were transferred from our ante¬partum area.patients in whom dif¬ferent complications of pregnancyall contributed to functional insuf¬ficiency of the placenta, resulting inintrauterine growth retardation. Ourresults clearly reflect this situationby the incidence of dysmaturity we
have shown. The careful selectionof time of delivery, with monitoringthroughout induction and activelabour, has contributed to a reduc¬tion in stillbirths in this group ofpatients; no perinatal deaths oc¬curred in this group, though labourwas often induced with a predictedsmall baby, on the basis of ab¬normal estriols, uterine growthcurves, uterine measurements andamniotic fluid studies.The immediate and on-site avail¬
ability of expert pediatric neonatalcare, always present before deliveryin high-risk pregnancies, in orderthat resuscitation may be preparedfor and staff and equipment ready,is the only explanation for theabsence of neonatal deaths in thesevery high-risk dysmature infants.
ETIOLOGICAL FACTORSToxemia of pregnancy was by
far the commonest pathologicalcondition qualifying for admissionto the O.N.I.C.U. The toxemias ofpregnancy were subdivided into thesevere (blood pressure over 160systolic or 110 diastolic) and mild.No perinatal deaths occurred in themild toxemias. Two perinatal deathswere associated with severe tox¬emia; both mothers had neglectedantepartum care. One patient wasreferred from out of town 11 daysbefore term with a very marked in¬trauterine growth retardation andsevere pre-eclampsia. The other
60 Canad. Med. Ass. J., Oct. 4, 1969, vol. 101.394

TABLE IL.PERINATAL DEATHS
AgeDaysgest.
N.B.wt.
Wt.gest.(%)
Apgarmin.1 5
Prognosticrisk score High-risk factors Main causes of death
26 254 1729 <10 121.8
Toxemia; abruptio; age;placental insufficiency;previous intrauterine deathSevere pre-eclampsia; placentalinsufficiency; previous intra¬uterine death; cord prolapseSevere Rh disease; failed intra¬uterine transfusion; abruptioplacentaeProlonged rupture of membranes(100 days); breech; previousintrauterine deathAbruptio; polyhydramnios;congenital renal anomalies;premature rupture of mem¬branesAbruptio; premature breech;no prenatal careSevere Rh sensitization; twoprevious intrauterine deaths;premature labour after extra¬uterine fetal transfusionAbruptio; placenta praevia;prematurity
Neonatal aspiration; severedysmaturity
Delayed toxemia management;abruptio; cord prolapse;dysmaturityAbruptio complicating failedintrauterine transfusion;prematurityPrematurity; breech
Neonatal pneumothorax;renal anomalies
Prematurity; subduralhematoma;neonatal pneumothoraxImmaturity
Neonatal cooling; respiratorydistress syndrome
perinatal death was in a case re¬ferred by the attending physicianimmediately at 295 days' gestation,on the occasion of the first prenatalvisit. Both these babies weighedunder 1800 g.
Twenty of our 71 cases of tox¬emia had severe pre-eclampsia.Rh sensitization accounted for a
larger proportion than one wouldhave expected because of the par¬ticular interest taken at this centreand by the author in this condition.In the present study eight patientshad severe Rh disease, with theamniotic fluid presenting indicationsfor either early induction or intra¬uterine transfusion. The latter pro-
S-f
. .
cedure was resorted to in five, andthere were three survivors.
I have found a useful place forcontinuous monitoring of the fetalheart rate during intrauterine trans¬fusion, by using a stainless-steelelectrode (36-gauge) insertedthrough the catheter used for in-fusing the packed cells into theperitoneal cavity. In several in¬stances a warning tachycardia hasdeveloped, and the transfusion hasbeen interrupted, only to be re-surried after the fetal heart resumeda normal rate.
Placental insufficiency, associatedwith known pathological changes or
idiopathic in nature, would appear
. . .
.. . . . . .
. .. . . ... .. . .
. * *w ... .. .
. .. .
.£.... .
. ..
r-0.71
NfWBORN WEIGHT (grams)FIG. 5..Height of uterine fundus measured from superior border of symphysis along
convex surface of abdomen, plotted against newborn weight.
to impose one of the greatestthreats to the fetus, especially whena severe degree is present in earlypregnancy. One of the most danger¬ous situations associated with thiscondition, we found, was the neces¬
sity to induce labour in the face ofunripe conditions. Oxytocin ad¬ministration was found to behazardous even in doses as low as
1.0 mU per min., and may wellhave been causal in the develop¬ment of abruptio placentae in some
circumstances, even when patternsof recorded uterine activity were
within normal limits. Recourse tocesarean section in these early anddysmature pregnancies had even
worse results.Clinically detected fetal distress
occasioned the transfer of 42 pa¬tients from a routine labour settingto our unit. In none of these didperinatal death occur.
Of 18 women on whom cesarean
sections were carried out for fetaldistress, only four had been ad¬mitted to our unit with this as an
indication for admission. Of the 42patients admitted to the O.N.I.C.U.with clinically detected fetaldistress, 36 gave birth to babies whowere born with Apgar ratings atone minute over 6, and all 42 in¬fants had five-minute Apgar scores
over 6. Thus it would appear thatclinically detected fetal distress cor¬
relates very poorly with infant out¬come from a perinatal morbidity or
mortality standpoint.Canad. Med. Ass. J., Oct. 4, 1969, vol, 101.395 61

*o-l
WEEKS OF AMINORRHEAFIG. 6..Weight-gestation correlation of high-risk pregnancies and their distribution into Lubchenco's percentiles.
Forty-five cesarean sections werecarried out in our O.N.I.C.U., arate of 21.1%. Forty per cent ofthese were performed because ofcephalopelvic disproportion. Manypatients with borderline pelvis were
admitted in order that a physiologi¬cal approach to stimulation oflabour could be safely carried out.With uterine pressures continuouslyrecorded, little danger of hyper-tonus, hypersystole, or abnormalfrequency or rhythm of uterine con-
tractions was present. When any ofthese developed, it was immediatelyrecognized and corrected.A comparison was made between
the results of the cesarean sectionscarried out for fetal distress andthose for CPD (Table IV). Fromour results it would appear thatneither the surgical procedure itselfnor the concomitant anesthetic
played a significant role in the de¬pression of the newborn.
Obstetrical history..It is of notethat three of our perinatal deaths(37.5%) occurred in patients whohad had previous perinatal losses.This high incidence is especiallynoteworthy because this indicationfor referral to our unit representsonly 10% of our admissions; fur¬ther, only 5% of patients in our
hospital with such a history arrivedin our unit for care.
DISCUSSIONIt became apparent during our
study that numerous patients whomight have benefited from referralto our unit were not admitted. Simi¬larly, many patients with lesser de¬grees of high risk were being re¬ferred who might well have been
cared for in a less sophisticated at¬mosphere.Our entire efforts cannot solve
the problem of the preventable peri¬natal losses; the mothers of someinfants of obviously viable size (wellover 2200 g.) may arrive in hospitalwith the baby dead in utero andwith a history of slight, and some¬times not so slight, toxemia or
TABLE IV..CESAREANSECTION
TABLE IIL.PREDICTED AND ACTUAL PERINATAL MORTALITYPROGNOSTIC RISK SCORE BASIS
* Rate per thousand live births.t Rate corrected for exclusion of antepartum stillbirths.
** Correction factor applied eliminating false additive risk (c.f. 4.3).
bleeding managed inadequately.This leads to a conclusion that amethod of improved education ofthe undergraduate, the postgradu¬ate and the practising physiciansshould be sought. In both outlyingcommunities and in universitycentred programs an exchange ofresidents in family-practice or spe-cialty-training programs with prac¬tising physicians and specialistsmight prove useful. Mutual benefitsmay accrue, on the one hand, from
62 Canad. Med. Ass. J., Oct. 4, 1969, vol. 101.396

a re-exposure to academic environ-ment with newer methods of in-vestigating and managing conditionswhich lead to perinatal loss andwhich are now preventable, and onthe other hand, by an awareness ofthe actual problems of practices inthe outlying areas.
Another ancillary approachwould be the expanded use ofscoring methods for assessing preg-nancies and providing, if necessary,an itinerant scoring service withcarefully delineated and classifiedindications that would warrant re-ferral of the mother to a regionalcentre for care.
The role of an antepartum wardfor the management and investiga-tion of complicated pregnancies hasbecome quite apparent. The numberof beds that would be required formanagement of pregnancies whichare in this way complicated wouldappear to be in the range of oneantepartum bed per 150 annual deli-veries. This ratio may be loweredto one bed per 100 annual de-liveries in a special referral area.
Intrapartum monitoring of thepatient in labour has made it pos-sible that many deliveries whichpreviously would have been effectedby a cesarean section are managedand watched conservatively, withthe delivery of perfectly healthybabies who have never been de-pressed. The commonest examplesof these are the bradycardias andfetal heart irregularities which,when seen on a beat-to-beat basis,are discovered to be either headcompression patterns or just normalvagally induced variations in thebasal heart rate patterns.
The second observation of im-portance is that in patients withtrue fetal distress this complicationis recognized immediately, and de-livery is effected when necessary bycesarean section at an earlier stage,
before more lasting and damaginghypoxia can ensue.
In our study, numerous examplesof marked newborn bradycardiaresponded immediately to accuratesuction and endotracheal aspiration.When this is done, an immediatereturn to normal heart rate andcolour clearly shows that adequatepediatric resuscitative care must beavailable, at least for every high-risk delivery if not for all routinedeliveries.The newborn area has also
demonstrated the need for awarmed environment to carry outthe resuscitation of the newbornand for it to be immediately avail-able from the standpoints of bothtime and space.
The obvious questions to beasked in the final evaluation of thistype of project are: have any babiesactually been saved, has the pen-natal mortality been reduced, andhas morbidity decreased? An at-tempt has been made to answerthese questions, in part, by the useof a predictive scoring system. Wehave been disappointed in any at-tempt to make comparisons regard-ing the state of depression of in-fants. This disappointment stemsmainly from the recognition thatApgar scores which appear in cli-nical records represent in factmerely a retrospective guess. Whilea five-minute Apgar score has beensaid to correlate better with theeventual neurological status and de-velopment it would appear fromsome of our graphs that a one-min-ute Apgar score may have thegreater significance when this scoreis actually assigned at one minuteand if every point is correctlyevaluated.
R.um.Cet article expose la mc.thodo-
logie, l'appareillage et le personnel
n.cessaires pour la r.alisation d'unprojet de soins intensifs applicableaux cas de grossesse . risque .lev..Nous avons .tudi. le taux demortalit. p.rinatale et analys. son
A notre avis, ii y a trois types decas de grossesse dont les risquessont assez .levc.s pour justifier lerecours au service complet que nousd.crivons. Ce sont: a) un stat s.vc.rede pr.-&lampsie, b) un net retarddans la croissance intra-ut.rine, ac-compagnc. d'une insuffisance pla-centaire qui peut s'.valuer par desmesures p.riodiques de la croissanceut.rine et le dosage de l'estriol, et c)le travail irr.versible des cas d'ac-couchement pr.matur. oji ons'attend t. la naissance d'un b.b.pesant au plus 2200 g. II est.videmment de nombreux autresstats que nous avons trait.s dansce centre et dont l'heureux d.noue-ment est peut-.tre di2 aux moyensd'action dont nous disposions. Ondevrait aussi songer c. installer unsyst.me de surveillance moms corn-plet et d'application plus facile dansle cadre des salles de travail etd'accouchement existantes.
Nous estimons qu'il est urgent dereviser et de changer certaines denos m.thodes d'enseignement auxfuturs me.decins, aux r.sidents etaux m.decins pratiquants et de leurfournir les moyens pour un perfec-tionnement continu dans le domainedes soins prc.natals et de la d&ou-verte des cas de grossesse c. risque.lev.. 11 faudrait . la fois centrali-ser et r.gionaliser ce type de d.-partement de soins intensifs.
Pour que pareil projet re.ussisse,il faudrait inclure dans le cadre dece d.partement de soins intensifs,les facteurs pe.diatrique et obst.-trical indispensables.
I wish to acknowledge the able as-sistance of the two residents who at-tended all the patients in the intensivecare unit, Drs. H. N. Ramaprakash andJ. K. Milne, as well as of all the tech-nical, nursing and secretarial staff, andalso the full support of the Chief of theDepartment of Obstetrics, Dr. J. H.Walters.
REFERENCES
1 EFFER, S. B.: High risk pregnancy. Paper presented at the annualmeeting of the Ontario Medical Association, Toronto, May 6-10,1968.
2. HON, E. H.: Amer. J. Obstet. Gynec., 86: 772, 19633. Ontario Perinatal Mortality Study Committee: Second report of the
perinatal mortality study in ten university teaching hospitals,Ontario, Canada; supplement, Department of Health, Toronto,1967.
4. BUTLER, N. R. AND BONHAM, D. G.: Perinatal mortality. The firstreport of the 1958 British Perinatal Mortality Survey under theauspices of the National Birthday Trust Fund, E. & S. Living-stone Ltd., Edinburgh, 1963.
5. LUBCHENCO, L. 0. et al.: Pediatrics, 32: 793, 1963.6. CALDEYRO-BARCIA, R. et al.: In: The child, edited by A. Dorfman,
The Year Book Publishers, Chicago, p. 8. in press.
Canad. Med. Ass. J., Oct. 4, 1969, vol. 101-397 63