Embed Size (px)
Citation preview

Full Terms & Conditions of access and use can be found athttp://www.tandfonline.com/action/journalInformation?journalCode=ierz20
Download by: [Professor Andrej Trampuz] Date: 03 January 2017, At: 12:39
Expert Review of Anti-infective Therapy
ISSN: 1478-7210 (Print) 1744-8336 (Online) Journal homepage: http://www.tandfonline.com/loi/ierz20
Management of infections associated withneurosurgical implanted devices
Anna Conen, Christoph A. Fux, Peter Vajkoczy & Andrej Trampuz
To cite this article: Anna Conen, Christoph A. Fux, Peter Vajkoczy & Andrej Trampuz (2016):Management of infections associated with neurosurgical implanted devices, Expert Review ofAnti-infective Therapy, DOI: 10.1080/14787210.2017.1267563
To link to this article: http://dx.doi.org/10.1080/14787210.2017.1267563
Accepted author version posted online: 02Dec 2016.Published online: 13 Dec 2016.
Submit your article to this journal
Article views: 26
View related articles
View Crossmark data

REVIEW
Management of infections associated with neurosurgical implanted devicesAnna Conena, Christoph A. Fuxa, Peter Vajkoczyb and Andrej Trampuzc
aClinic of Infectious Diseases and Hospital Hygiene, Department of Internal Medicine, Kantonsspital Aarau, Aarau, Switzerland; bDepartment ofNeurosurgery, Charité - Universitätsmedizin Berlin, Berlin, Germany; cCenter for Musculoskeletal Surgery, Charité - Universitätsmedizin Berlin,Berlin, Germany
ABSTRACTIntroduction: Neurosurgical devices are increasingly used. With it, neurosurgical device-related infec-tions gain relevance. As biofilms are involved in implant-associated infections the diagnosis andtreatment is challenging and requires specific anti-biofilm concepts and management algorithms.Areas covered: The literature concerning the management of neurosurgical device-associated infec-tions is scarce and heterogeneous treatment concepts are discussed, but no standardized diagnosticand treatment procedures exist. Therefore, we emphasize extrapolating management strategies pre-dominantly from orthopedic device-associated infections, where the concept is better established andclinically validated. This review covers infections associated with craniotomy fixation devices, cranio-plasties, external ventricular and lumbar drainages, internal shunts and neurostimulators.Expert commentary: Sonication of the removed implants significantly improves microbiological diag-nosis. A combined surgical and antimicrobial management is crucial for successful treatment: appro-priate surgical intervention is combined with prolonged anti-biofilm therapy of usually 12 weeks. Inselected patients, new treatment algorithms enable cure of neurosurgical device-associated infectionswithout implant removal or with a one-stage implant exchange, considerably improving the quality ofpatient lives.
ARTICLE HISTORYReceived 24 August 2016Accepted 29 November 2016
KEYWORDSBiofilm; cranioplasty;craniotomy; device;infection; ventriculardrainage; management;neurosurgical;neurostimulator; shunt
1. Introduction
The use of implants to treat age-related disease conditionsgains increasing interest in the context of the demographicalevolution, not only in orthopedic patients with prosthetic jointreplacement but also in neurology and neurosurgery [1]. Inthe United States, an estimated 450,000 neurosurgicalimplants are inserted annually, about 3–15% of which becomeinfected [1]. Numbers of implanted and infected neurosurgicaldevices will increase; therefore, the need for an effective diag-nostic and treatment management in neurosurgical implant-associated infections is emphasized [2,3]. The most commonlyused neurosurgical implants are fixation devices for craniot-omy or cranioplasty, synthetic cranioplasties, internal shuntsystems, external ventricular and lumbar drainages, andneurostimulators.
With older age, not only cerebrovascular diseases increase,but also neoplasms with consecutive brain metastases.Decompressive craniectomies and craniotomies for diagnosticand therapeutic purposes are performed. Thereafter, theremoved piece of skull is replaced and fixed with titaniumfixation devices. Alternatively, a titanium or synthetic cranio-plasty is used instead. In case of a chronic hydrocephalus, apermanent drainage of cerebrospinal fluid (CSF) may benecessary. This can be achieved by an internalized shuntsystem, draining the CSF into the right atrium (ventriculoatrial[VA] shunts) or – more commonly – into the peritoneal space
(ventriculoperitoneal [VP] shunts). In case of an acute rise ofintracranial pressure which compromises CSF circulation, forexample, after intracerebral bleeding, intercurrent percuta-neous CSF drainage can be achieved by an external ventriculardrainage (EVD) or external lumbar drainage (ELD). Deep brainstimulators are one of the newest treatment modalities in themanagement of Parkinson’s disease and other movement dis-orders, whereas spinal cord stimulators are increasingly usedto treat chronic refractory pain syndromes mostly due todegenerative spine diseases.
As biofilms are involved in implant-associated infections, thediagnosis and treatment is difficult. With newer diagnosticmethods such as sonication, the diagnostic yield can beimproved [4]. For antimicrobial treatment, drug combinationswith anti-biofilm agents have to be administered [5–8]. Inaddition, in device-associated infections involving the centralnervous system (CNS), the individual CSF penetration levels ofantimicrobial agents have to be considered. Implant-associatedinfections are associated with high morbidity, mortality, andhealth-care costs. Usually, they require additional surgical inter-ventions, which are not trivial facing the fact that CNS isinvolved. In orthopedic patients, revision surgery of an infectedprosthetic joint is three times more expensive than primaryimplantation [1,9,10]. For neurosurgical implants, excess costscan only be estimated but probably will be even higher.
The literature concerning the management of neurosurgi-cal device-associated infections is scarce and heterogeneous
CONTACT Anna Conen [email protected] Clinic of Infectious Diseases and Hospital Hygiene, Kantonsspital Aarau, Tellstrasse 25, CH-5001 Aarau,Switzerland
EXPERT REVIEW OF ANTI-INFECTIVE THERAPY, 2016http://dx.doi.org/10.1080/14787210.2017.1267563
© 2016 Informa UK Limited, trading as Taylor & Francis Group

treatment concepts are discussed which often include a com-plete device removal. This can be very bothersome for thepatient compromising quality of life. As no standardized diag-nostic and treatment procedure exists, many concepts need tobe extrapolated from other implant-associated infections.
The aim of this review is to resume the pathophysiologicalaspects of implant-associated infections and to discuss thecurrent diagnostic and treatment challenges. The manage-ment strategy will mainly be extrapolated from orthopedicdevice-associated infections, where the concept is well estab-lished and clinically validated. This review will cover the mostcommonly used neurosurgical implants, including craniotomyfixation devices, cranioplasties, internal shunt systems,external ventricular and lumbar drainages, andneurostimulators.
2. Concept of biofilm and pathogenesis of infectionof neurosurgical implants
Implants are highly susceptible to bacterial colonization. Asfew as 100 bacteria in contact with a device are enough tocause infection during or shortly after surgery [11,12]. Within afew minutes, bacteria adhere to the implant surface, multiplyand embed themselves in a matrix consisting of extracellularpolymeric substances (EPS). This three-dimensional commu-nity of bacteria attached to a surface and embedded in EPSis called biofilm [13]. The biofilm protects microorganismsfrom the host immune system and renders them tolerant toantimicrobial treatments, because microorganisms are in astationary growth phase with a slow replication rate [13].Many antibiotics, including betalactams or vancomycin, exclu-sively kill replicating bacteria. Therefore, they have no activityagainst biofilms in vivo despite being fully active in vitro. Inaddition, the granulocyte function is disturbed in the peri-implant region, called frustrated phagocytosis [11].
The vast majority of neurosurgical implants becomesinfected by exogenous colonization with bacteria of the skinor mucosal flora. The colonization occurs in the preoperativestage trough skin defects or open wounds, intraoperativelythrough contamination of the implant, or postoperatively dur-ing wound healing, particularly in case of a persistent wounddrainage [11,12,14]. Rarely, and almost exclusively VA shunts,neurosurgical implants become infected through hematogen-ous seeding from a distant site of infection. Due to the endo-vascular placement of VA shunts, hematogenous infection anytime after implantation during bacteremia is possible. This is incontrast to prosthetic joints, which are hematogenouslyinfected in about 30% of cases [15].
3. Risk factors for neurosurgical implant-associatedinfections
There are many perioperative risk factors known to be asso-ciated with neurosurgical device-associated infections, whichare principally the same as for other surgical site infections.The predominant risk factors for post-craniotomy infectionsare the presence of EVD with an odds ratio (OR) of 7.2 (95%confidence interval [CI] 2.9–18.1), the administration of pre-operative chemotherapy with an OR of 5.2 (95% CI 2.3–11.6),
and the presence of a postoperative CSF leakage with an ORof 3.5 (95% CI 1.4–8.5) [16–18]. Other risk factors are not onlycontaminated wound classes, including contamination class2 with an OR of 3.2 (95% CI 1.2–8.1) and contamination class3 with an OR of 8.0 (95% CI 2.6–24.5), morbid obesity (OR 3.1,95% CI 1.4–6.8), and emergency operations (OR 3.0, 95% CI1.1–8.1), but also chronic steroid use, prior hospitalization forlonger than 1 day and prolonged duration of surgery [16–19].For shunts, risk factors for infection are previous shunt infec-tion (relative risk (RR) 3.8, 95% CI 2.4–6.1), postoperative CSFleakage (hazard ratio 19.2, 95% CI 7.0–52.9), the use of aneuroendoscope (RR 1.6, 95% CI 1.0–2.5), but also advancedage, shunt revision for dysfunction, longer duration of shuntsurgery, and the experience of the neurosurgeon [20–22]. ForEVD, risk factors for infection are intraventricular and subar-achnoid hemorrhage, cranial fracture with CSF leakage, dura-tion of catheterization, and EVD irrigation [23–25]. For ELD,the following risk factors for infection have recently beendescribed: duration of catheterization longer than 4 days(OR 6.1, 95% CI 1.8–20.4), drainage site leakage (OR 13.6,95% CI 4.1–45.7), and length of hospitalization [for the dura-tion of 16–20 days, OR 3.5 (95% CI 1.5–8.1) and for theduration ≥21 days, OR 5.8 (95% CI 2.1–16.2)] [26].
4. Classification of neurosurgical implant-associatedinfections
The classification of neurosurgical device-associated infectionsis extrapolated from other implant-associated infections[14,15,27]. The classification is essential for the determinationof the management strategy, as discussed in the Section 6.
Early or acute infections occur within 4 weeks after deviceimplantation (Table 1). Clinical presentation usually is acutewith fever and local signs of inflammation, including localwarmth, erythema, swelling, tenderness, and wound drainage.In early device-associated infections, an ‘immature’ biofilm ispresent and therefore eradication of infection with implantretention is successful if rigorous surgical debridement is fol-lowed by a 12-week anti-biofilm therapy. Delayed and lateinfections occur after 4 weeks of device implantation (delayedwithin 1 year and late after 1 year of implantation). The clinicalpresentation is low grade with persistent wound drainage orfistula. A ‘mature’ biofilm is present and eradication of infec-tion with implant retention is very unlikely. Therefore, implantremoval or exchange in a one-stage or two-stage procedure isnecessary, followed again by a 12-week anti-biofilm therapy ifan implant is in place. The concept of ‘immature’ and ‘mature’biofilm is based on in vitro observations [6], experimental invivo models [6–8,28], and clinical studies [5,29,30] but has alsorecently been reviewed by Bjarnsholt et al. [31].
EVD and ELD are exceptions to this classification, since theyare temporary implants, which are in place for only a few daysto weeks. In case of infection, they usually can be exchangedor even removed without replacement. Because of their tem-porary placement, no anti-biofilm therapy is needed andshould be discarded, as resistant strains may emerge andcompromise treatment of potential later infections of perma-nent implants, including shunt systems.
2 A. CONEN ET AL.

5. Sonication in the diagnosis of neurosurgicalimplant-associated infections
To optimize diagnosis in biofilm-associated infections, sonica-tion of removed implant components and prolonged incuba-tion of cultures is recommended [4]. By sonication,microorganisms are released from the implant surface andcan qualitatively and quantitatively be detected from thedetached biofilm in the sonication fluid. Compared to tissuecultures, sensitivity of sonication fluid is significantly higherwith 80–90% compared to 60%. In particular, sensitivity ishigher in case of antimicrobial pretreatment (75% with sonica-tion vs. 45% without sonication) [4]. The specificity is high with99%, which allows distinction of contamination and infection,especially if skin flora is cultured.
Sonication was initially evaluated in prosthetic joints, butseems to be useful for other implants as well, including osteo-syntheses, cranioplasties, and catheter tips of EVD and shuntsystems [32–34]. The sensitivity for detecting osteosynthesis-associated infections was 90.4% for sonication fluid and 56.8%for peri-implant tissue cultures (p < 0.05), for polymicrobialinfections, it was 20.8% and 8.0%, respectively (p < 0.001) [32].In a case report, successful sonication and pathogen identifica-tion in a low-grade cranioplasty-associated infection weredemonstrated, detecting coagulase-negative staphylococciand Prevotella spp. Both pathogens were missed in tissue cul-tures [33]. Sonication of EVD (14 patients) and VP shunts (13patients) was performed in 27 patients [34]. Sonication of EVDtips was significantly more likely to detect bacterial growth (9 of14 cases, 64%) than cultures of aspirated ventricular CSF (2 of14 cases, 14%; p < 0.05). This is explained by the fact thatmicroorganisms grow on the implant surface as biofilm andare not detectable as planktonic bacteria in the CSF. In fivepatients with a positive sonication culture of the EVD tip but anegative CSF culture, results were interpreted as contamination:one patient became afebrile after EVD removal, two developedmeningitis a few days after EVD removal, and two remainedasymptomatic. In the VP shunt group, there was no significantdifference between positive culture results of CSF and sonica-tion fluid of VP shunts, possibly due to low patient numbers:bacterial growth was detected in 62% (8 of 13 cases) of soni-cated VP shunts and 45% (5 of 11 cases, CSF not cultured in 2cases) of the corresponding intraoperative CSF samples.
It is important to note that in case of EVD removal forsonication, the cutaneous exit site should be disinfectedand air-dried before the catheter is pulled out. The ventri-cular catheter tip then is aseptically cut and placed in asterile tube. Otherwise, skin flora of the EVD catheter exitsite will be cultured, which has no diagnostic importance.
6. General treatment concept of neurosurgicalimplant-associated infections
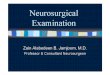
In this section, the general treatment concepts of implant-asso-ciated infections are discussed (Figure 1). The specific treatmentconcepts for the individual neurosurgical implants aredescribed in the Section 7. These recommendations are validfor permanent implants only, that is, fixation devices for cra-niotomy, cranioplasty, internal shunt systems, and neurostimu-lators. EVD and ELD are intercurrent implants and usuallycompletely removed in case of infection. Therefore, treatmentis shorter and without anti-biofilm antibiotics.
Successful treatment requires an interdisciplinary man-agement and includes a combination of appropriate surgeryand anti-biofilm therapy, which should include bactericidalantimicrobial drugs [15,27]. Surgery is necessary to removenecrotic tissue and to reduce bacterial load, that is, tomechanically clean the implant in acute infections orexchange the implant if symptom duration is longer thanthe proposed 4 weeks. The postoperative soft tissue cover-age of the implant is a prerequisite for success; otherwise,the implant is at risk for consecutive superinfection withselected microorganisms of the skin flora.
The implant management strategy depends on two factors,namely the antimicrobial susceptibility pattern of the causingpathogen (susceptibility vs. non-susceptibility to anti-biofilmtreatment) and the symptom duration (acute infections withsymptom duration of less than 4 weeks vs. delayed or lateinfections with longer symptom duration). Without anti-bio-film therapy and in case of a long symptom duration, which isassociated with a ‘mature’ biofilm, eradication of infectionwithout implant removal or exchange, respectively, is unlikely.
Anti-biofilm therapy includes rifampin combinations againststaphylococci and Propionibacterium spp. as well as fluoroquino-lones against gram-negative bacilli (Tables 2 and 3). Antimicrobialtreatment combinations with bactericidal activity generally are
Table 1. Classification of neurosurgical device-associated infections: extrapolation from other implant-associated infections.
Early infection Delayed and late infection
When ≤4 weeks after implantation Delayed: >4 weeks after implantationLate: >12 months after implantation
Clinical presentation AcuteFever, local signs of infection (including local warmth,erythema, swelling, tenderness, and wound drainage)
Low-gradePersistent wound drainage, fistula
Biofilm ‘Immature’ ‘Mature’Surgical treatment Debridement and implant retention possible Removal or exchange of the implant necessary
(one- or two-stage exchange)Antimicrobial treatment Anti-biofilm treatment for 12 weeks
● Usually 2 weeks intravenous treatment● Then, 10 weeks oral treatment
Anti-biofilm treatment for 12 weeks
● Usually 2 weeks intravenous treatment● Then, 10 weeks oral treatment
Adapted from Zimmerli et al. [15], Kleber et al. [27], and Conen et al. [14].
EXPERT REVIEW OF ANTI-INFECTIVE THERAPY 3

preferred. If the infected compartment includes the CNS, sufficientCSF penetration of the antimicrobial agents is a prerequisite forsuccess [35]. In addition, higher drug doses are recommended forCNS infections. Rifampin acts bactericidal also in the stationarygrowth phase of staphylococci and has a good CSF penetration(achieving 56% of plasma levels in CSF). Because of a rapid emer-gence of resistance in case of monotherapy, rifampin must alwaysbe combined with another antimicrobial agent with a good CSFpenetration, for example, cotrimoxazole (i.e. trimethoprim/sulfa-methoxazole; CSF penetration 40–50% of plasma levels), levoflox-acin (30–50% of plasma levels), moxifloxacin (>50% of plasmalevels) or doxycycline (26% of plasma levels). Treatment failuredue to acquired rifampin resistance has been observed in shuntinfections with coagulase-negative staphylococci treated withintravenous vancomycin and rifampin. This can be explained byinsufficient CSF penetration of vancomycin resulting in rifampinmonotherapy in the CSF [14]. In addition, rifampin should not beused in case of persistent wound drainage because of the risk ofconsecutive superinfection with selected rifampin-resistant micro-organisms of the skin flora [36]. For gram-negative bacilli, cipro-floxacin is the only anti-biofilm therapy and has a CSF penetrationof about 26% of plasma levels [5,35,37,38].
If the microorganism is known and susceptible to anti-biofilmtherapy, then surgery includes implant debridement and retentionin early infections (i.e. symptom duration up to 4 weeks), or a one-or two-stage implant exchange with a short (i.e. 2 weeks) implant-free interval at any time of infection. In all these cases, surgery isfollowed by a 12-week anti-biofilm therapy. The implant-free
interval may be prolonged in case of severe soft tissue damagethat does not allow adequate postoperative wound closure.
If the microorganism is not susceptible to anti-biofilm ther-apy, cure is possible only with implant removal and reinsertionusually after 6 weeks of postoperative antibiotic treatment,when the infection is eradicated. In shunt-associated infections,the implant-free interval can be shorted from 6 to 1 week (incase of coagulase-negative staphylococci or Propionibacteriumacnes), 2 weeks (Staphylococcus aureus, Streptococcus spp.,Enterococcus spp., and culture-negative infections), or 3 weeks(gram-negative bacilli), because CSF infections (i.e. meningitis)without implant are usually cleared after a shorter treatmentduration. Alternatively, if implant removal is not possible, long-term antimicrobial suppression therapy can be discussed.Agents for long-term antimicrobial suppression therapy arecotrimoxazole and doxycycline in case CNS is involved, andadditionally clindamycin, if CNS is not involved. The followingmicroorganisms are considered difficult to treat, as no anti-biofilm treatment is available: rifampin-resistant staphylococci,quinolone-resistant gram-negative bacilli, Enterococcus spp.,and Candida spp.
7. Specific infections
7.1. Post-craniotomy and cranioplasty-associatedinfections
Craniotomy refers to the surgical removal of a section of theskull, the so-called bone flap, to access the intracranial
Microorganism known,
susceptible to anti-biofilm antibiotics
Microorganism known, NOT
susceptible to anti-biofilm antibiotics
Two-stage exchange of implant with long interval (6-8 weeks without implant)- 6 weeks antibiotic therapy
Implant retention and long-term antibiotic suppression
therapy
Early infection #: Implant debridement and retention
- 12 weeks anti-biofilm therapy*
One-stage exchange of implant- 12 weeks anti-biofilm therapy*
Two-stage exchange of implant (short interval, 2 weeks without implant)- 12 weeks anti-biofilm therapy*
Surgery- Debridement- Implant retention or exchange- Soft tissue coverage
Anti-biofilm treatment- Rifampin combinations against staphylococci- Fluoroquinolones against gram-negative bacilli
Figure 1. Treatment algorithm according to the susceptibility pattern of the causing microorganism: Implemented from other implant-associated infections §.Adapted from Zimmerli et al. [15].§ Excluded are external ventricular and lumbar drainage-associated infections, which have a different management strategy due to their temporary placement# Early infection, i.e. within four weeks of implantation* Usually 2 weeks intravenous and 10 weeks oral treatment
4 A. CONEN ET AL.

compartment. It is used to perform brain and skull-base tumorsurgery, to drain brain abscesses or to exclude intracerebralvascular malformations from the circulation (e.g. aneurysms).After the surgical intervention, the bone flap is replaced to itsoriginal position and fixed with titanium plates, screws, orclamps, which represent the implant. The post-craniotomy
infection rate lies between 0.5% and 7%. Infections usuallymanifest early at median of 1.5 months (range, 4 days - 5years) after craniotomy. The most common causing pathogensare not only S. aureus and coagulase-negative staphylococcibut also gram-negative bacilli [40,41]. In 50 patients includedin a study by Dashti et al., the predominant symptoms were
Table 2. Antimicrobial treatment of neurosurgical device-associated infections according to the causing microorganism, CNS not involved.a
Microorganism Intravenous treatment, daily dose (2 weeks) Oral treatment, daily dose (10 weeks)
Staphylococcus aureus or coagulase-negative staphylococci, methicillinsusceptible
Flucloxacillin 4 × 2 g IVORCefazolin 3 × 2 g IVb
ORVancomycin 2 × 15 mg/kg body weight IVb,e
PLUS in all regimensRifampin 2 × 450 mg POc
Levofloxacin 2 × 500 mg POORCotrimoxazole 3 × 960 mgd POORDoxycycline 2 × 100 mg POORFusidic acid 3 × 500 mg POPLUS in all regimensRifampin 2 × 450 mg POc
S. aureus or coagulase-negativestaphylococci, methicillin resistant
Vancomycin 2 × 15 mg/kg body weight IVe
ORDaptomycin 1 × 8 mg/kg body weight IVPLUS in all regimensRifampin 2 × 450 mg POc
Levofloxacin 2 × 500 mg POORCotrimoxazole 3 × 960 mgd POORDoxycycline 2 × 100 mg POORFusidic acid 3 × 500 mg POPLUS in all regimensRifampin 2 × 450 mg POc
Streptococcus species Penicillin 4 × 5 Mio U IVORCeftriaxone 1 × 2 g IVf
Amoxicillin 3 × 750–1000 mg PO
Enterococcus speciesg, penicillinsusceptible
Amoxicillin 4 × 2 g IV PLUS Gentamicin 1 × 3 mg/kg body weight IVh
ORAmoxicillin 4 × 2 g IV PLUS Ceftriaxone 2 × 2 g IVPLUS consider for both regimensFosfomycin 3 × 5 g IV
Amoxicillin 3 × 1000 mg PO
Enterococcus speciesg, penicillinresistant
Vancomycin 2 × 15 mg/kg body weight IVe
ORDaptomycin 1 × 10 mg/kg body weight IVPLUS consider for both regimensFosfomycin 3 × 5 g IVPLUS consider for both regimensGentamicin 1 × 3 mg/kg body weight IVh
Linezolid 2 × 600 mg PO
Propionibacterium acnes Penicillin 4 × 5 Mio U IVORCeftriaxone 1 × 2 g IVf
PLUS in all regimensRifampin 2 × 450 mg POc
Levofloxacin 2 × 500 mg PO PLUSRifampin 2 × 450 mg POc
Enterobacteriaceae Amoxicillin/Clavulanate 3 × 2.2 g IVORCeftriaxone 1 × 2 g IVf
Ciprofloxacin 2 × 750 mg PO
Non-fermenters (e.g. Pseudomonasaeruginosa), quinolone-susceptible
Cefepime 3 × 2 g IVi
ORCeftazidime 3 × 2 g IVi
ORPiperacillin/Tazobactam 3 × 4.5 g IVi
ORMeropenem 3 × 2 g IVi
Ciprofloxacin 2 × 750 mg PO
Culture-negative infection Amoxicillin/Clavulanate 3 × 2.2 g IVPLUSRifampin 2 × 450 mg POc
Levofloxacin 2 × 500 mg PO PLUSRifampin 2 × 450 mg POc
Adapted from Zimmerli et al. [15] and Kleber et al. [27].CNS: Central nervous system; IV: intravenous; PO: oral.aIncluding post-craniotomy and cranioplasty-associated infections, neurostimulator-associated infections without brain lead infection.bIn case of a non-type I allergic reaction to penicillin use intravenous cefazolin, in case of a type I allergic reaction to penicillin use intravenous vancomycin.cStart rifampin as soon as all drainages are removed and wounds are dry.dOne cotrimoxazole double strength tablet (960 mg) contains 160 mg trimethoprim and 800 mg sulfamethoxazole.eGoal: Vancomycin trough level 15–20 mg/l, measure at least twice weekly; start rifampin only if trough level is in the therapeutic range.fIn case of a non-type I allergic reaction to penicillin use intravenous ceftriaxone.gEnterococcus species usually are difficult to treat, especially if fosfomycin cannot be used; therefore, a long-term antimicrobial suppression treatment has to bediscussed with an infectious diseases specialist.
hMeasure aminoglycoside trough levels and creatinine to monitor for toxicity at least twice weekly.iCombination therapy with an aminoglycoside should be considered particularly if multiresistant Pseudomonas spp. is present, for example, tobramycin 3–5 mg/kgbody weight once daily or gentamicin 3 mg/kg body weight once daily. Measure aminoglycoside trough levels and creatinine to monitor for toxicity at least twiceweekly.
EXPERT REVIEW OF ANTI-INFECTIVE THERAPY 5

change of mental state (36%), purulent wound drainage (34%),fever (22%), and headache (20%), less common were localswelling (14%), and seizures (4%) [40].
In craniectomy, the bone flap is removed and not imme-diately replaced. This intervention is performed for decom-pression surgery after trauma, intracerebral hemorrhage,malignant cerebral infarction, or in case of an infectedbone flap. Cranioplasty is the reinsertion of the cryopre-served autologous bone flap using titanium plates, screws,or clamps for fixation, or the implantation of a syntheticimplant made of polyether ether ketone, poly methyl metha-crylate, or titanium. The cranioplasty-associated infection
rate lies between 1% and 26% and the main involved patho-gens are S. aureus, coagulase-negative staphylococci, andgram-negative bacilli [42,43]. With the use of autologousbone flaps, an additional risk is the bone flap resorption,an aseptic bone necrosis occurring in 2–32% with a higherincidence in younger patients and in patients with multipleskull fragments [44–46]. The average time interval betweencraniectomy and cranioplasty is 7.3 months (range,1–40 months), a time, during which the patient lives witha disfiguring deformity, no brain protection and a possiblyaltered CSF dynamic leading to hydrocephalus [42]. In areview by Yadla et al., there was neither an association of
Table 3. Antimicrobial treatment of neurosurgical device-associated infections according to the causing microorganism, CNS involved.a
Microorganism Intravenous treatment, daily dose (2 weeks) Oral treatment, daily dose (10 weeks)
Staphylococcus aureus or coagulase-negative staphylococci, methicillinsusceptible
Flucloxacillin 6 × 2 g IVORMeropenem 3 × 2 g IVb
ORVancomycin 2 × 15 mg/kg body weight IVb,c
PLUS in all regimensRifampin 2 × 600 mg POd
Cotrimoxazole 2 × 1920 mge POORLevofloxacin 2 × 500 mg POORDoxycycline 2 × 100 mg POPLUS in all regimensRifampin 2 × 600 mg POd
S. aureus or coagulase-negativestaphylococci, methicillin resistant
Vancomycin 2 × 15 mg/kg body weight IVc
PLUSRifampin 2 × 600 mg POd
Cotrimoxazole 2 × 1920 mge POORLevofloxacin 2 × 500 mg POORDoxycyclin 2 × 100 mg POPLUS in all regimensRifampin 2 × 600 mg POd
Streptococcus species Penicillin 4 × 5 Mio U IVORCeftriaxone 2 × 2 g IVf
Prolonged IV treatment recommended (outpatienttherapy with ceftriaxone 1 × 2 g IV possible)
Enterococcus speciesg, penicillinsusceptible
Amoxicillin 6 × 2 g IV PLUSFosfomycin 3 × 5-8 g IV PLUSConsider gentamicin 1 × 3 mg/kg body weight IVh
Prolonged IV treatment recommended (consider inselected patients Linezolid 2 × 600 mg PO)
Enterococcus speciesg, penicillinresistant
Vancomycin 2 × 15 mg/kg body weight IVc PLUSFosfomycin 3 × 5-8 g IV PLUSConsider gentamicin 1 × 3 mg/kg body weight IVh
Prolonged IV treatment recommended (consider inselected patients Linezolid 2 × 600 mg PO)
Propionibacterium acnes Penicillin 4 × 5 Mio U IVORCeftriaxone 2 × 2 g IVf
PLUS in all regimensRifampin 2 × 600 mg POd
Levofloxacin 2 × 500 mg PO PLUSRifampin 2 × 600 mg POd
Enterobacteriaceae Ceftriaxone 2 × 2 g IV Prolonged IV treatment recommended, thenciprofloxacin 2 × 750 mg PO
Non-fermenters (e.g. Pseudomonasaeruginosa), quinolone-susceptible
Cefepime 3 × 2 g IVi
ORCeftazidime 3 × 2 g IVi
ORMeropenem 3 × 2 g IVi
Prolonged IV treatment recommended, thenciprofloxacin 2 × 750 mg PO
Culture-negative infection Ceftriaxone 2 × 2 g IV PLUS Vancomycin 2 × 15 mg/kg body weight IVc PLUS
Rifampin 2 × 600 mg POd
Levofloxacin 2 × 500 mg PO PLUSRifampin 2 × 600 mg POd
Adapted from Zimmerli et al. [15] and Kleber et al. [27].CNS: Central nervous system; IV: intravenous; PO: oral.aExcluding external ventricular and lumbar drainages as temporary implants, including ventriculoperitoneal and ventriculoatrial shunt-associated infections,neurostimulator-associated infections with brain lead infection. In case of a secondary infective endocarditis in ventriculoatrial shunt infections, consult also theendocarditis guidelines [39].
bIn case of a type I or a non-type I allergic reaction to penicillin use intravenous vancomycin or intravenous meropenem, meropenem has better CSF penetrationthan vancomycin and is therefore preferred over vancomycin.
cGoal: vancomycin trough level 15–20 mg/l, measure at least twice weekly.dStart rifampin as soon as all drainages are removed and wounds are dry; start rifampin with caution in vancomycin therapy and only if vancomycin trough levels aredocumented in the therapeutic range (trough level 15–20 mg/l), earlier switch to the oral treatment combination with better CSF penetration recommended.
eOne cotrimoxazole double strength tablet (960 mg) contains 160 mg trimethoprim and 800 mg sulfamethoxazole.fIn case of a non-type I allergic reaction to penicillin use intravenous ceftriaxone.gEnterococcus species usually are difficult to treat, especially if fosfomycin cannot be used; therefore, a long-term antimicrobial suppression treatment has to bediscussed with an infectious diseases specialist.
hMeasure aminoglycoside trough levels and creatinine to monitor for toxicity at least twice weekly.iCombination therapy with an aminoglycoside should be considered particularly if multiresistant Pseudomonas spp. is present, for example, tobramycin 3–5 mg/kgbody weight once daily or gentamicin 3 mg/kg body weight once daily. Measure aminoglycoside trough levels and creatinine to monitor for toxicity at least twiceweekly.
6 A. CONEN ET AL.

cranioplasty material (autologous vs. allogeneic) nor of thetime point of cranioplasty (early within 3 months vs. latemore than 3 months after craniectomy) with infection [47].Limitations of this review are the inclusion of predominantlyretrospective studies with the inherent risk of recall andobserver bias, the lack of uniform definitions of infectionand complication, and the variability of follow-up time. Butrecently, an association between infection and a time inter-val of more than 2 weeks until cranioplasty was described inan observational cohort of 754 cranioplasties [41]. Therefore,not only for cosmetic reasons and brain protection, but alsobecause of a potentially lower infection risk, timely cranio-plasty should be considered.
In both, post-craniotomy and cranioplasty-associatedinfections, the distinction between superficial and deepwound infections is not possible because the superficialand deep compartments are in contiguity after surgery.Therefore, all infections should be considered as deep andbone flap-/cranioplasty-associated. Surgical revision withdebridement of necrotic tissue and evacuation of pus isnecessary, as is debridement or exchange of the implant,depending on the duration of infection and the susceptibilitypattern of the microorganism (Figure 1). The current clinicalpractice in post-craniotomy and cranioplasty-associatedinfections is the removal of the bone flap or implant anddelayed cranioplasty after weeks to months, once the infec-tion is cleared. Newer concepts inspired by the orthopedicliterature include debridement and retention of the infectedbone flap or cranioplasty in acute infections or immediate(one-stage) cranioplasty at any time of infection if soft tissuesare preserved. Alternatively, a two-stage exchange of theimplant with only a short (i.e. 2 weeks) implant-free intervalis possible. Both strategies include a 12-week anti-biofilmtherapy postoperatively (Table 2). These newer conceptsmay lead to better cosmetic results and brain protection.
7.2. VP and VA shunt-associated infections
Neurosurgical shunt systems are permanent implants used in thepresence of chronic communicating hydrocephalus as a result ofintracerebral hemorrhage or infection, in case of an obstructivehydrocephalus secondary to tumors or congenital malforma-tions, or in case of a normal pressure hydrocephalus in elderlypeople [2,14,48,49]. Normal pressure hydrocephalus increaseswith age with a pooled prevalence of 1.3% in subjects olderthan 65 years of age [2]. Two different shunt systems are usedfor CSF drainage either into the peritoneal cavity – the VP shunt –or into the right atrium – the VA shunt. The infection rate is aboutthe same for both systems (5–15% for VP and 2.5–12% for VAshunts), but VA shunts require significantly more revisions due todysfunction (49.7% in VA vs. 33.8% in VP shunts, p < 0.001)[50,51]. In addition, complications in VA shunts are more severeand include myocardial injury, cardiac arrhythmias, distal discon-nection, and intra-atrial migration, intra-cardiac thrombi withsubsequent pulmonary embolism or endocarditis with consecu-tive septic embolism. Difficult revisions may explain the highermortality in VA shunts reported in older studies [51–53].Nowadays, VP shunts are generally preferred because of the
lower complication rate. However, in patients with previousabdominal surgery, a history of peritonitis, morbid obesity, andprevious VP shunt failure, VA shunts are chosen. In thesepatients, not only the perioperative complication risk in abdom-inal surgery is increased, but also CSF resorption is impairedbecause of peritoneal fibrosis and adhesions due to previoussurgery and infections, which leads to dysfunction of the abdom-inal shunt part.
In a retrospective analysis including 78 adult patients withneurosurgical shunt systems, shunt infection was mainlyacquired intraoperatively through shunt contamination (72%)or early postoperatively (27%) through skin wounds (proximaland distal shunt part) and perforated gut (distal shunt part inVP shunts) [14]. For VA shunts, hematogenous seeding from adistant site of infection is possible, as found in one patient. Thepredominant microorganisms involved in shunt infections arecoagulase-negative staphylococci (37%), S. aureus (18%), P.acnes (9%), and polymicrobial infections (15%) includinggram-negative bacilli [14]. In early infections, mainly microor-ganisms of the skin flora are found, that is, coagulase-negativestaphylococci, S. aureus, and P. acnes, whereas in delayed andlate infections, mainly polymicrobial infections due to wounddehiscence and gut perforation of the distal VP shunt part.
Shunt infections can present with few or no clinical signsand symptoms [14]. Chronic low-grade shunt infection oftenresults in shunt dysfunction manifesting as hydrocephalus(e.g. headache, vomiting, and seizures). Of 78 patients, only78% had fever, 64% neurological signs or symptoms, and 49%local signs of infection. Nevertheless, symptom durationbefore infection diagnosis was usually short with a medianof 5 days (range, 0–21 days). The clinical presentation dependson which shunt part is infected. Proximal shunt infectionsmanifest with signs of ventriculitis, meningitis, or shunt dys-function. Distal shunt infections in VP shunts manifest withsigns of peritonitis, pseudoappendicitis, or intraabdominalpseudocysts detected by sonography or computed tomogra-phy scan. In VA shunt infections fever, signs of right sidedendocarditis and shunt nephritis are typically present[14,48,49,54]. Chronic VA shunt infections by coagulase-nega-tive staphylococci or P. acnes may persist for weeks or monthsbefore endocarditis and immune complex-mediated shuntnephritis occur. These severe late complications of a chroniclow-grade VA shunt infection were recently presented in acase report [54]. A 26-year-old woman with congenital hydro-cephalus and a VA shunt in place since 14 years complained offever and myalgia. Blood and CSF investigations as well asechocardiography were without pathologies at the initial visit;the patient was then lost to follow-up. Four years later, shepresented with end-stage renal disease requiring hemodialy-sis. A kidney biopsy revealed immune complex-mediated glo-merulonephritis and echocardiography right-sidedendocarditis. P. acnes was cultured in CSF collected from theshunt system. The shunt was explanted, a third ventriculocis-ternostomy performed and the patient treated with 4 weeks ofintravenous penicillin and at a later stage a kidney transplant.
The diagnostic yield of different CSF collection sites wasstudied in a retrospective analysis, comparing CSF from ventri-cular, lumbar, or shunt valve puncture [14]. Overall, CSF leuko-cyte count was elevated in only 80%. Leukocyte counts were
EXPERT REVIEW OF ANTI-INFECTIVE THERAPY 7

significantly higher in lumbar and shunt valve puncture withmedian 573 and 484 cells/µl compared to ventricular CSF withmedian 8.5 cells/µl (p < 0.001 and p = 0.016, respectively). Thispossibly reflects differences in inflammation and CSF flow inpatients with hydrocephalus. Alternatively, it could be explainedby the fact that lumbar and shunt valve punctures were per-formed in patients with more advanced shunt infections. CSFcultures were positive in 66% overall, with the highest positivityrate in CSF from shunt valve puncture (91%), compared toventricular (70%) and lumbar (45%) CSF, respectively. The highmicrobial density close to the biofilms at the site of infectionmight explain these results, which was also supported by arelatively high positivity rate of shunt tip cultures with 78%(when the study was performed, no sonication was available; itcan be expected that with sonication, the shunt tip positivity ratewould have been even higher). However, differences in the rateof antimicrobial pretreatment might play a role as well. Bloodcultures are particularly important in VA shunt infections withpositivity rates of at least 83%, explained by the endovascularposition of the implant, whereas in VP shunt infections, thediagnostic yield is low with a positivity rate of only 11% [14].
No standardized treatment algorithm for shunt infectionsexists. The only randomized trial of 50 patients was publishedin 1981, comparing cure rates of 3 different treatment strate-gies: shunt removal, one-stage shunt exchange, and shuntretention [55]. Patients were treated with 2 weeks of intraven-tricular combined with 3 weeks of systemic antimicrobial ther-apy. No anti-biofilm therapy with rifampin was used. Curerates were 95% with shunt removal, 88% with one-stageshunt exchange, and only 36% if no revision surgery wasperformed. The predominant pathogens involved in thisstudy were coagulase-negative staphylococci in 62%.
In a retrospective observational study of 78 patients, 81%were treated with a combined surgical and antimicrobial ther-apy and 19% with an antibiotic treatment only [14]. The over-all cure rate was 96%, being 98% in the combined and 87% inthe conservative treatment group. The combination treatmentgroup included shunt removal without replacement (47%) anda one- (10%) or two-stage shunt exchange with or without anintercurrent EVD (23%). Overall, only two patients had aninfection relapse, one in the combined and one in the anti-microbial alone treatment group. Both relapses were causedby coagulase-negative staphylococci with newly acquiredrifampin resistance. Both patients initially received a vancomy-cin and rifampin treatment combination. It was speculatedthat insufficient CSF vancomycin levels due to the low CSFpenetration rate of vancomycin resulted in a functional rifam-pin monotherapy in CSF with the emergence of resistance. Inaddition, insufficient vancomycin trough levels could havecontributed to the failure; however, these were not measuredin this retrospective study. Based on these results, it is recom-mended to treat such patients if possible with the combina-tion of cotrimoxazole and rifampin, because of a much betterCSF penetration of cotrimoxazole compared to vancomycin;alternatively, an initial high-dose single vancomycin treatmentfor a few days may reduce the bacterial load before switchingto the oral combination. Overall, these data show that bothretention and immediate shunt replacement are efficient. In
Table 3, treatment recommendations are summarized. In con-trast to post-craniotomy and cranioplasty-associated infec-tions, CSF penetration of the antimicrobial treatment is aprerequisite for success in shunt-associated infections.Furthermore, in VA shunt infections, longer intravenous treat-ment durations may be mandatory in case of a secondaryinfective endocarditis [39].
An algorithm for the management of shunt infections isproposed in Figure 2. If a shunt infection is suspected, CSFshould preferably be collected from shunt valve puncture.In case of pathological CSF results (i.e. CSF leukocyte count>5 × 106 cells/µl, with predominantly granulocytes, CSFlactate levels >1.9 mmol/l, and total protein levels>0.45 g/l as well as a decreased glucose CSF/blood ratio<0.5), empiric treatment should cover the predominantpathogens with intravenous vancomycin (2 × 15 mg/kgbody weight daily) plus an intravenous cephalosporin(ceftriaxone 2 × 2 g or cefepime 3 × 2 g or ceftazidime3 × 2 g daily according to local surveillance data). If there isacute infection, absence of ventriculitis, abscess, shunt dys-function, skin erosion, or gut perforation and if the micro-organism is known to be susceptible to anti-biofilm therapy,the implant can be retained or immediately exchanged.Thereafter, the patient should be treated for 12 weekswith a CSF-penetrating anti-biofilm therapy. In all othercases, the shunt should be explanted and reinserted oncethe infection is cleared – in case of coagulase-negativestaphylococci or P. acnes usually after 5–7 days, in case ofS. aureus, Streptococcus spp., Enterococcus spp., and culture-negative infections after 14 days, and in case of gram-nega-tive bacilli after 21 days. Eventually an intercurrent EVD/ELDneeds to be inserted. If CSF culture is still positive at thetime of shunt reimplantation, a 12-week anti-biofilm therapyis recommended with the new implant in situ. If CSF cultureis negative at the time of shunt reimplantation, a 4-weekanti-biofilm therapy should strongly be discussed, in parti-cular if an intercurrent EVD/ELD was in place, making per-sistent infection on the EVD/ELD more likely. With thisstrategy, any remaining viable microorganism should beeradicated.
7.3. External ventricular and lumbar drainages
In contrast to the other neurosurgical implants mentioned inthis review, which are permanent, EVD and ELD are temporaryimplants. They are used to treat acute hydrocephalus, forexample, after intracranial or subarachnoid bleeding, acutemeningitis, or head trauma. In Table 4, the differencesbetween internalized shunts and EVD/ELD, respectively, arecontrasted. The fact that 44% of patients with an externalCSF drainage require a permanent shunt at a later timepoint represents a challenge in case of an ongoing EVD- orELD-associated infection [56].
The overall infection risk of external CSF drainages liesbetween 10% and 15% [23,24,26,57,58]. EVD and ELD indwel-ling times have been found to be associated with the infectionrisk: the latter is increasing over the first 10 days with a peakafter 7–11 days, and markedly lower thereafter. This is contra-
8 A. CONEN ET AL.

intuitive, as one would expect the infection risk to be linear asshown for central venous catheters [23,24,26,59]. Changes inrisk profiles over time may explain part of the results, which arenot free from confounding, especially in the continuously smal-ler patient population at risk. In a study of 48 patients with an
EVD, the median indwelling time was 7 days (range, 1–39 days)and the infection occurred at median of 6 days (range,1–17 days) [56]. Interestingly, 23% of patients with an EVD-associated infection only presented within 10 days after EVDremoval, what implies that one must be aware of EVD-
Table 4. Comparison of infections associated with ventriculoperitoneal and ventriculoatrial shunts and external ventricular and lumbar drainages, respectively.
Ventriculoperitoneal and ventriculoatrial shunt External ventricular and lumbar drainage
Indication Chronic, persistent hydrocephalus Acute hydrocephalus: CSF drainage or intracranialpressure monitoring
Infection risk 5–15% 10–15% (increases with duration of catheterization)Risk factors for infection Serial revisions
Postoperative CSF leakagePrevious infectionProlonged duration of surgeryAbdominal infectionsa
Infections with secondary bacteremiab
Catheter irrigationDuration of catheterizationIntracranial hemorrhageCranial fracture with CSF leakage
Infection acquisition IntraoperativeContiguous (skin wound, perforated gut a, etc.)Hematogenousb
Contiguous
At the end Shunt dysfunction, hydrocephalus Up to 44% require an internal shunt
CSF: Cerebrospinal fluid.aVentriculoperitoneal shunts.bVentriculoatrial shunts.
Shunt-associated infection
Empirical antimicrobial therapy in case of pathological CSFresults *
Vancomycin IV PLUSCeftriaxone orcefepime/ceftazidime IV(according to localsurveillance data)
No ventriculitis / meningitis / abscessNo dysfunctionNo erosion (intact skin and gut)
AND
Early infectionAND
Microorganisms known to besusceptible to anti-biofilm antibioticsShunt retention or
immediate reinsertion
possible
Remove shunt, treat infection, insert intercurrent EVD/ELD if necessary
12 weeks anti-biofilm
treatment(usually 2 weeks IV then 10weeks oral treatment)
Diagnostic:
CSF sample (valve puncture)Blood cultures #
Reinsert shunt once infection is cleared, usually after 7-21 days(dependent on: microorganism §, extent of infection, CSF results)
Adapt antimicrobial treatmentto culture results
NoYes
CSF culture -
at reinsertion:
4 weeks anti-biofilm treatment
CSF culture +
at reinsertion:
12 weeks anti-biofilm treatment
−−−
−
−
−−
−−
Figure 2. Proposed management algorithm for shunt-associated infections. Adapted from Conen et al. [14].Abbreviations: CSF: Cerebrospinal fluid; EVD: external ventricular drainage; ELD: external lumbar drainage; IV: intravenous* Pathological CSF results: CSF leukocyte count >5x106 cells/µl, with predominantly granulocytes, CSF lactate >1.9 mmol/l, CSF total protein >0.45 g/l, glucose CSF/blood ratio <0.5# Blood cultures especially in ventriculo-atrial shunt infections recommended§ For low-virulent microorganisms, including coagulase-negative staphylococci and P. acnes, re-implantation after 5–7 days; for S. aureus, Streptococcus spp.,Enterococcus spp. and culture-negative infections 14 days; for Enterobacteriaceae and P. aeruginosa 21 days
EXPERT REVIEW OF ANTI-INFECTIVE THERAPY 9

associated meningitis also in patients in whom EVD has beenremoved. This has also been shown by Jost et al. in the sonica-tion study of EVD catheter tips [34]. In five patients with positiveEVD sonication cultures, the respective CSF culture results werenegative or interpreted as contamination. Two of these fivepatients developed overt meningitis a few days after EVDremoval. We strongly believe that sonication improves earlyrecognition of EVD-related infections. Patients whose removedEVD tips are densely colonized may be considered at high riskfor developing meningitis and merit close clinical follow-up.
Low-virulentmicroorganisms causemost of the infections asso-ciated with external CSF drainages. Culture results are positive inabout 77%. Coagulase-negative staphylococci are the predomi-nant microorganisms found in 63%, P. acnes in 15% and polymi-crobial infections in 21% [56]. Nearly all EVD-associated infectionsare acquired through external contamination because of repetitivemanipulations on the system (e.g. regular CSF collection for diag-nostic purposes) and/or via EVD colonization with skin and envir-onmental flora. Microorganisms contiguously spread along thedrainage tube to the internal EVD system and the CSF.
In the context of a suspected EVD- or ELD-associated infec-tion, the interpretation of clinical signs and symptoms and CSFresults is difficult. The primary medical condition leading tothe EVD/ELD placement itself, for example, intracerebralbleeding or infection, may cause identical pathological clinical(fever and alterations in Glasgow Coma Scale) and CSF find-ings. Nevertheless, patients with an external CSF drainage-associated infection usually present with signs of ventriculitisand meningitis (headache, neck stiffness, increase in CSF
leukocyte count, and lactate level, which has been found tobe a valuable test to identify patients with bacterial meningitisafter neurosurgery) or exit site infection [56,60]. In a retro-spective study of 48 patients, clinical signs and symptoms aswell as CSF results at the time of EVD placement and at thetime of EVD infection were compared [56]. In case of an EVD-associated infection, fever (79% vs. 15% at EVD insertion,p < 0.001), headache, vomiting, and neck stiffness (31% vs.6% at EVD insertion, p = 0.003) were the predominant signsand symptoms [56]. Furthermore, there was a significantlyhigher CSF leukocyte count at the time of infection diagnosiscompared to EVD insertion (175 compared to 46 cells/µl,p = 0.021). Some authors suggest the calculation of the cellindex, which is the ratio between leukocyte and erythrocytecounts in CSF compared to blood [61]. This index is based onthe hypothesis that intraventricular hemorrhage dilutes theCSF with blood. On the other hand, additional leukocytesinvade the CSF to clear the blood. Therefore, leukocyte levelin the CSF is variable and it is not possible to define anabsolute cutoff indicative of infection. However, a continuousincrease of the cell index is highly indicative of infection. Thismanagement would imply daily CSF sampling with again ahigher risk to provoke an iatrogenic EVD-associated infection.
An algorithm for suspected EVD- and ELD-associated infectionsis proposed in Figure 3 and antimicrobial management strategiesare presented in Table 5. Optimal CSF penetration of the antimi-crobial drugs is critical, as is the fact that for intercurrent implants,no rifampin as anti-biofilm therapy must be used. In a febrilepatient with an EVD/ELD in place, CSF analysis is recommended,
>300x106 cells/µl, CSF/bloodglucose ratio <0.5, CSF lactate >2.1 mmol/l
Febrile patient with EVD/ELD
CSF purulent?CSF gram stain: gram-positivebacteria (mostly staphylococci)
Consider contamination
and colonization
If infection suspected: Increased cell index* and EVD/ELD in situ > 3 days
Immediately start antimicrobial treatment
- Vancomycin IV PLUS- Ceftriaxone or cefepime/ceftazidime IV
(according to local surveillance data)
Adapt treatment to culture results; treatment duration 7-21 days (dependent on: microorganism §,extent of infection, CSF results)
EVD/ELD replacement mainly if- S. aureus, gram-negative and Candida
infections- Inadequate response to treatment
Consider intraventricular antibiotics in
persistent infections despite appropriate intravenous treatment
No Yes
NoYes
Figure 3. Proposed management algorithm for suspected external ventricular- and lumbar drainage-associated infections. Adapted from Beer et al. [57].Abbreviations: CSF: Cerebrospinal fluid; EVD: external ventricular drainage; ELD: external lumbar drainage; IV: intravenous* Cell index: Ratio of leukocyte/erythrocyte ratio in CSF and leukocyte/erythrocyte ratio in blood§ For coagulase-negative staphylococci and P. acnes 5–7 days; for S. aureus, Streptococcus spp., Enterococcus spp. and culture-negative infections 14 days; forEnterobacteriaceae and P. aeruginosa 21 days.
10 A. CONEN ET AL.

as is the exclusion of other nosocomial infections (e.g. centralvenous catheter infection, urinary tract infection, pneumonia,and Clostridium difficile colitis). Particular attention is warranted ifCSF is not purulent but gram stain shows gram-positive bacteria,which makes contamination or EVD/ELD colonization with predo-minantly coagulase-negative staphylococci rather likely than trueinfection. In case of purulent CSF (i.e. CSF leukocyte count >300cells/µl or increasing cell index, lactate >2.1 mmol/l and adecreased glucose CSF/blood ratio <0.5), empiric treatmentshould cover the main pathogens using intravenous vancomycin(2 × 15 mg/kg body weight daily) plus an intravenouscephalosporin (ceftriaxone 2 × 2 g or cefepime 3 × 2 g or ceftazi-dime 3 × 2 g daily according to local surveillance data).Intraventricular therapy can be used if the patient does notrespond to systemic therapy or if highly resistant microorganismsare present [62]. Replacement of the EVD/ELD should be consid-ered in infections with S. aureus, gram-negative bacilli, or Candidaspp. or in case of an inadequate response to therapy. Treatmentduration is usually 7 days in case of coagulase-negative staphylo-cocci and P. acnes, 14 days in case of S. aureus, Streptococcus spp.,Enterococcus spp., and culture-negative infections, and 21 days incase of gram-negative bacilli.
Daily CSF sampling and prophylactic EVD/ELD exchangeare not recommended, as every EVD/ELD manipulationincreases the risk for infection [59,63,64]. As EVD/ELD are
intercurrent implants, rifampin-containing treatment regi-mens are strongly discouraged. Rifampin is the only anti-biofilm therapy to curatively treat permanent implant-asso-ciated infections with staphylococci or Propionibacteriumspp. Every systemic antimicrobial therapy changes theskin microbiome. With rifampin therapy, rifampin-resistantmicroorganisms emerge on the skin increasing the risk of arifampin-resistant infection of the possibly ensuing perma-nent shunt, which then would not be curatively treatable[36]. For the same reason, we strongly discourage from theuse of rifampin-coated EVD/ELD [65]. With the use ofrifampin-coated EVD/ELD, pathogens are exposed to rifam-pin monotherapy in CSF and rifampin-resistant microor-ganisms (mainly coagulase-negative staphylococci)emerge.
7.4. Neurostimulator-associated infections (deep brainand spinal cord stimulators)
Neurostimulators include spinal cord stimulators to treatchronic refractory pain, and deep brain stimulators to treatmovement disorders, especially Parkinson’s disease and dysto-nia, but refractory pain as well. Parkinson’s disease is one ofthe most common neurological disorders with about 4.1 mil-lion patients worldwide. Studies estimate that until 2030, the
Table 5. Antimicrobial treatment in external ventricular- and lumbar drainage-associated infections according to the causing microorgan-ism, CNS involved.
Microorganism Intravenous treatment, daily dosea
Staphylococcus aureus or coagulase-negativestaphylococci, methicillin susceptible
Flucloxacillin 6 × 2 g IVORMeropenem 3 × 2 g IVb
ORVancomycin 2 × 15 mg/kg body weight IVb,c
S. aureus or coagulase-negative staphylococci,methicillin resistant
Vancomycin 2 × 15 mg/kg body weight IVc
Streptococcus species Penicillin 4 × 5 Mio U IVORCeftriaxone 2 × 2 g IVd
Enterococcus species, penicillin susceptible Amoxicillin 6 × 2 g IVPLUSConsider gentamicin 1 × 3 mg/kg body weight IVe
Enterococcus species, penicillin resistant Vancomycin 2 × 15 mg/kg body weight IVc
PLUSConsider gentamicin 1 × 3 mg/kg body weight IVe
Propionibacterium acnes Penicillin 4 × 5 Mio U IVORCeftriaxone 2 × 2 g IVd
Enterobacteriaceae Ceftriaxone 2 × 2 g IVNon-fermenters (e.g. Pseudomonas aeruginosa) Cefepime 3 × 2 g IVf
ORCeftazidime 3 × 2 g IVf
ORMeropenem 3 × 2 g IVf
Culture-negative infection Ceftriaxone 2 × 2 g IVPLUSVancomycin 2 × 15 mg/kg body weight IVc
IV: Intravenous; CNS: central nervous system.aTreatment duration dependent on the microorganism: coagulase-negative staphylococci and P. acnes 5–7 days; S. aureus, Streptococcusspp., Enterococcus spp., and culture-negative infections 14 days; Enterobacteriaceae and P. aeruginosa 21 days.
bIn case of a type I or non-type I allergic reaction to penicillin use intravenous vancomycin or intravenous meropenem, meropenem hasbetter CSF penetration than vancomycin and is therefore preferred over vancomycin.
cGoal: vancomycin trough level 15–20 mg/l, measure at least twice weekly.dIn case of a non-type I allergic reaction to penicillin use intravenous ceftriaxone.eMeasure aminoglycoside trough levels and creatinine to monitor for toxicity at least twice weekly.fCombination therapy with an aminoglycoside should be considered particularly if multiresistant Pseudomonas spp. is present, for example,tobramycin 3–5 mg/kg body weight once daily or gentamicin 3 mg/kg body weight once daily. Measure aminoglycoside trough levelsand creatinine to monitor for toxicity at least twice weekly.
EXPERT REVIEW OF ANTI-INFECTIVE THERAPY 11

number of patients suffering from Parkinson’s disease willhave doubled and the use of deep brain stimulators probablywith it [3]. Both stimulators consist of an impulse generator,which is implanted subcutaneously in the abdominal wall forspinal cord stimulators and in the chest wall for deep brainstimulators. The generator is connected via wires to the leadsthat are placed in the spinal epidural space for spinal cordstimulators and in the brain for deep brain stimulators.
The majority of infections occur early within 1 month afterimplantation. For spinal cord stimulators, the infection rate isabout 5% (range, 2.5–14%) with 38% manifesting as earlyimplant-associated infections [10,66–68]. For deep brain sti-mulators, the infection rate is about 5.6% (range, 0–15%) with52% manifesting as early infections [69–71]. The wide rangesin infection rates result from a lack of a standardized definitionof infection and different follow-up times in the studies. Forboth implants, the most common causing pathogens are S.aureus, coagulase-negative staphylococci, and P. acnes. Inspinal cord stimulator-associated infections, alsoPseudomonas aeruginosa has been described in a significantproportion.
More than 50% of neurostimulator-associated infectionspresent with a pocket infection at the impulse generatorimplantation site, manifesting with local signs of inflammation,including local warmth, erythema, swelling, tenderness, andwound drainage. Less common are wire or wire extenderinfections and lead infections with consecutive spinal epiduralor brain abscesses [66,69].
Most studies recommend device removal, antimicrobialtreatment, and reimplantation once the infection is cured,usually 3 months later. However, removal of the leads, mainlyin deep brain stimulators with lead placement in the brain, isassociated with high morbidity. Therefore, the following man-agement strategies are suggested, depending on the site ofinfection (epidural or brain abscess vs. pocket infection vs.lead extender or wire infection), the susceptibility pattern ofthe causing microorganism (susceptibility vs. non-susceptibil-ity to anti-biofilm therapy), and the duration of infection (earlyinfection within 4 weeks of implantation vs. delayed/late
infections) (Table 6). Implant debridement and retention inacute infections or immediate or early reimplantation (i.e.within 2 weeks) at any stage of infection is possible if themicroorganism is susceptible to anti-biofilm therapy and nobrain or epidural abscess is present. In every scenario, theaffected portion of the device needs surgical debridementand consecutive soft tissue coverage. In case of an epiduralor brain abscess, abscess evacuation and complete deviceremoval are needed. The following infection sites and man-agement strategies can be discriminated preconditioned thatno difficult to treat microorganisms are detected and an acuteinfection is present: in case of a pocket infection, the genera-tor and the implantation site (due to the soft tissue condition)should be changed; wires and leads can be retained. If extra-cranial wires are infected, the wires and wire connectorsshould be changed; generator and leads can be retained. Incase the device was removed, immediate or delayed reimplan-tation after 2–6 weeks is possible. In every scenario, surgicaltreatment is followed by a 12-week anti-biofilm therapy,except if a long implant-free interval (i.e. 6 weeks) is chosen,where no anti-biofilm treatment is necessary. In selectedpatients, a long-term antimicrobial suppression therapy canbe discussed, if a difficult to treat microorganism was detectedor a chronic infection is present and the device cannot beremoved.
8. Conclusions
Neurosurgical device-associated infections gain relevance withthe aging population and newer treatment options such asneurostimulators for pain and movement disorders. In analogyto every implant-associated infection, infected neurosurgicaldevices should be treated as biofilm infections.Microbiological diagnosis is significantly improved by sonica-tion of the removed implants and prolonged incubation ofcultures. An interdisciplinary management is of high impor-tance, including surgical intervention and usually a 12-weekanti-biofilm therapy. Different CSF penetration levels andhigher drug doses should be respected in case CNS is
Table 6. Recommendations for the management of neurostimulator-associated infections according to the site of infection.
Clinical situation Management of the neurostimulator Antimicrobial therapya
Pocket infection(no difficult to treat microorganisms detected)
Change generator (and implantation sitebecause of soft tissue condition)Keep wires and leads
12 weeks anti-biofilm treatment
Extracranial wire infection(no difficult to treat microorganisms detected)
Change wires, lead extenders, or connectorsitesKeep generator and leads
12 weeks anti-biofilm treatment
Neurostimulator removed(no difficult to treat microorganisms detected)
Immediate reimplantation (one-stageexchange)
Delayed reimplantation (two-stage exchange)• Short implant-free interval (2 weeks)• Long implant-free interval (≥6 weeks)
12 weeks anti-biofilm treatment
12 weeks anti-biofilm treatment6 weeks antimicrobial therapy, no anti-biofilm therapy needed
Pocket infection, extracranial wire infection(difficult to treat microorganismsb detected)
Remove implant, reinsert after a longimplant-free interval (≥6 weeks)
If no removal: debridement and soft tissuecoverage before initiation of suppressiontherapy
6 weeks antimicrobial therapy, no anti-biofilm therapy needed
Long-term antimicrobial suppression therapyc
aFor microorganism-specific treatments without central nervous system involvement, see Table 2 and with central nervous system involvement Table 3, respectively.bRifampin-resistant staphylococci, quinolone-resistant gram-negative bacilli, Enterococcus spp., Candida spp.cAgents for long-term antimicrobial suppression therapy are cotrimoxazole and doxycycline in case central nervous system is involved, and additionally clindamycin,if central nervous system is not involved.
12 A. CONEN ET AL.

involved. The adherence to treatment algorithms is necessaryto achieve high treatment success. Moreover, it is important tonote that there are efficient strategies to cure infections with-out implant removal or with a one-stage implant exchange.
9. Expert commentary
Neurosurgical device-associated infections are increasing, butvalidated diagnostic and treatment concepts are lacking. Mostrecommendations are therefore extrapolated from otherdevice-associated infections. From this experience, we learnedthat combined surgical and antimicrobial management is cru-cial for successful treatment outcome.
The microbiological diagnosis is significantly improved bysonication of the removed implants and prolonged cultureincubation. Regarding surgical treatment, cure withoutimplant removal or with a one-stage implant exchange arenew options, which considerably improve the quality ofpatient lives. Furthermore, in these less invasive surgical con-cepts, the antimicrobial treatment needs to be optimized andeffective against microbial biofilms.
There are some critical points to be respected in the treat-ment of neurosurgical device-associated infections. First, thereare differences in CSF penetration between antimicrobialdrugs – some do, others do not reach therapeutic drug levels.For that reason, some drug combinations foreseen in ortho-pedic device-associated infections cannot be used for CNSinfections. Also, higher drug doses are recommended toachieve therapeutic drug levels in CSF. Second, removal ofthe implant is often difficult or impossible in neurosurgicalimplants, as brain tissue may be involved and forced removalmay result in severe complications such as intracerebral bleed-ing. Therefore, the management of neurosurgical device infec-tions is even more challenging.
10. Five-year view
Future clinical studies should cover diagnostic aspects, mainlythe routine implementation of sonication in neurosurgicaldevice-associated infections to optimize microbiological diag-nosis or alternative biomarkers such as neutrophil degranula-tion products to discriminate between infection andinflammation. Modern molecular tests, such as multiplex poly-merase chain reaction, may improve the sensitivity for detec-tion of infection, especially in patients receiving previousantibiotics. Rapid identification of the causative pathogen andits susceptibility can further improve the treatment outcome.
Furthermore, the proposed treatment algorithms should bevalidated in larger clinical studies involving sufficient patientnumbers, as it has been demonstrated for orthopedic devices.Different antimicrobial treatment combinations should becompared in their efficiency to clear CNS infections with anindwelling device or eradicate biofilms from implant surface.
Finally, prophylaxis should be addressed. Newly designedneurosurgical implants with antimicrobial properties mayimprove treatment outcome of device-associated infections.These implants include anti-biofilm coatings (with antimicrobials,anti-adhesive properties), systems for local drug-delivery (such asresorbable hydrogels, or non-resorbable biomaterials
impregnated with antibiotics), or other innovative approachessuch as bacteriophage therapy, lytic enzymes, or targeting bio-film matrix or quorum-sensing. With improved infection preven-tion and treatment options, it is expected that more complexsurgeries and implants can be used, which may open new ideasand treatment options in the field of neurosurgical implants.
Key issues
● Neurosurgical implants are increasingly used, which is par-alleled by an increase in neurosurgical device-associatedinfections.
● The most commonly used neurosurgical implants are craniot-omy fixation devices, cranioplasties, internal shunt systems,external ventricular and lumbar drainages and neurostimula-tors (i.e. spinal cord and deep brain stimulators).
● Every implant-associated infection is a biofilm infection andneeds careful diagnostic and treatment management toachieve cure.
● No standardized diagnostic and treatment procedure exists;therefore, many concepts are extrapolated from experiencewith other implant-associated infections.
● Microbiological diagnostic is optimized by sonication of theremoved implants and prolonged incubation of cultures,which allows cultivating microorganisms directly from thedetached biofilm.
● Interdisciplinary management is of high importance, includingsurgical intervention and usually a 12-week anti-biofilmtherapy.
● Different CSF penetration levels and higher drug dosesshould be respected in the treatment of neurosurgicaldevice-associated infections.
● The adherence to treatment algorithms is necessary toachieve high treatment success.
● There are efficient strategies to cure infections withoutimplant removal or with a one-stage implant exchange.
Funding
This paper was not funded.
Declaration of interest
The authors have no relevant affiliations or financial involvement with anyorganization or entity with a financial interest in or financial conflict withthe subject matter or materials discussed in the manuscript. This includesemployment, consultancies, honoraria, stock ownership or options, experttestimony, grants or patents received or pending, or royalties.
References
Papers of special note have been highlighted as either of interest (•) or ofconsiderable interest (••) to readers.
1. Darouiche RO. Treatment of infections associated with surgicalimplants. N Engl J Med. 2004;350:1422–1429.
2. Martin-Laez R, Caballero-Arzapalo H, Lopez-Menendez LA, et al.Epidemiology of idiopathic normal pressure hydrocephalus: a systema-tic review of the literature. World Neurosurg. 2015;84:2002–2009.
3. Baker MG, Graham L. The journey: Parkinson’s disease. BMJ.2004;329:611–614.
EXPERT REVIEW OF ANTI-INFECTIVE THERAPY 13

4. Trampuz A, Piper KE, Jacobson MJ, et al. Sonication of removed hipand knee prostheses for diagnosis of infection. N Engl J Med.2007;357:654–663.
•• This article describes the method of sonication for optimizingthe diagnosis of biofilm-associated infections.
5. Zimmerli W, Widmer AF, Blatter M, et al. Role of rifampin fortreatment of orthopedic implant-related staphylococcal infections:a randomized controlled trial. Foreign-Body Infection (FBI) studygroup. JAMA. 1998;279:1537–1541.
6. Furustrand Tafin U, Corvec S, Betrisey B, et al. Role of rifampinagainst Propionibacterium acnes biofilm in vitro and in an experi-mental foreign-body infection model. Antimicrob AgentsChemother. 2012;56:1885–1891.
7. Furustrand Tafin U, Majic I, Zalila Belkhodja C, et al. Gentamicinimproves the activities of daptomycin and vancomycin againstEnterococcus faecalis in vitro and in an experimental foreign-body infection model. Antimicrob Agents Chemother.2011;55:4821–4827.
8. Oliva A, Furustrand Tafin U, Maiolo EM, et al. Activities of fosfomy-cin and rifampin on planktonic and adherent Enterococcus faecalisstrains in an experimental foreign-body infection model.Antimicrob Agents Chemother. 2014;58:1284–1293.
9. Kurtz SM, Lau E, Watson H, et al. Economic burden of peripros-thetic joint infection in the United States. J Arthroplasty.2012;27:61–5 e1.
10. Kumar K, Wilson JR, Taylor RS, et al. Complications of spinal cordstimulation, suggestions to improve outcome, and financial impact.J Neurosurg Spine. 2006;5:191–203.
11. Zimmerli W, Waldvogel FA, Vaudaux P, et al. Pathogenesis offoreign body infection: description and characteristics of an animalmodel. J Infect Dis. 1982;146:487–497.
12. James RC, Macleod CJ. Induction of staphylococcal infections inmice with small inocula introduced on sutures. Br J Exp Pathol.1961;42:266–277.
13. Costerton JW, Stewart PS, Greenberg EP. Bacterial biofilms: a com-mon cause of persistent infections. Science. 1999;284:1318–1322.
14. Conen A, Walti LN, Merlo A, et al. Characteristics and treatmentoutcome of cerebrospinal fluid shunt-associated infections inadults: a retrospective analysis over an 11-year period. Clin InfectDis. 2008;47:73–82.
•• This article includes the largest adult patient population withshunt-associated infections and describes clinical, diagnostic,and treatment aspects.
15. Zimmerli W, Trampuz A, Ochsner PE. Prosthetic-joint infections. NEngl J Med. 2004;351:1645–1654.
•• This article comprehensively describes surgical and antimicro-bial treatment strategies in implant-associated infections.
16. Sneh-Arbib O, Shiferstein A, Dagan N, et al. Surgical site infectionsfollowing craniotomy focusing on possible post-operative acquisi-tion of infection: prospective cohort study. Eur J Clin MicrobiolInfect Dis. 2013;32:1511–1516.
17. Lieber BA, Appelboom G, Taylor BE, et al. Preoperative chemother-apy and corticosteroids: independent predictors of cranial surgical-site infections. J Neurosurg. 2016;125:187–195.
18. Chiang HY, Kamath AS, Pottinger JM, et al. Risk factors and out-comes associated with surgical site infections after craniotomy orcraniectomy. J Neurosurg. 2014;120:509–521.
19. Mangran AJ, Horan TC, Pearson ML, et al. Guideline for preventionof surgical site infection, 1999. Infect Control Hosp Epidemiol.1999;20:250–278.
20. McGirt MJ, Zaas A, Fuchs HE, et al. Risk factors for pediatric ven-triculoperitoneal shunt infection and predictors of infectiouspathogens. Clin Infect Dis. 2003;36:858–862.
21. Borgbjerg BM, Gjerris F, Albeck MJ, et al. Risk of infection aftercerebrospinal fluid shunt: an analysis of 884 first-time shunts. ActaNeurochir (Wien). 1995;136:1–7.
22. Kulkarni AV, Drake JM, Lamberti-Pasculli M. Cerebrospinal fluidshunt infection: a prospective study of risk factors. J Neurosurg.2001;94:195–201.
23. Lozier AP, Sciacca RR, Romagnoli MF, et al. Ventriculostomy-relatedinfections: a critical review of the literature. Neurosurgery.2002;51:170–181; discussion 81-2.
24. Arabi Y, Memish ZA, Balkhy HH, et al. Ventriculostomy-associatedinfections: incidence and risk factors. Am J Infect Control.2005;33:137–143.
25. Lyke KE, Obasanjo OO, Williams MA, et al. Ventriculitis complicatinguse of intraventricular catheters in adult neurosurgical patients.Clin Infect Dis. 2001;33:2028–2033.
26. Liang H, Zhang L, Gao A, et al. Risk factors for infections related tolumbar drainage in spontaneous subarachnoid hemorrhage.Neurocrit Care. 2016;25:243–249.
27. Kleber C, Schaser KD, Trampuz A. [Complication management ofinfected osteosynthesis: therapy algorithm for peri-implant infec-tions]. Chirurg. 2015;86:925–934. German.
28. John AK, Baldoni D, Haschke M, et al. Efficacy of daptomycin inimplant-associated infection due to methicillin-resistantStaphylococcus aureus: importance of combination with rifampin.Antimicrob Agents Chemother. 2009;53:2719–2724.
29. Giulieri SG, Graber P, Ochsner PE, et al. Management of infectionassociated with total hip arthroplasty according to a treatmentalgorithm. Infection. 2004;32:222–228.
30. Tschudin-Sutter S, Frei R, Dangel M, et al. Validation of a treatmentalgorithm for orthopaedic implant-related infections with device-retention-results from a prospective observational cohort study.Clin Microbiol Infect. 2016;22:457 e1–9.
• This article validates the treatment algorithm of implant deb-ridement and retention in acute infections if anti-biofilm ther-apy is available.
31. Bjarnsholt T, Ciofu O, Molin S, et al. Applying insights from biofilmbiology to drug development - can a new approach be developed?Nat Rev Drug Discov. 2013;12:791–808.
32. Yano MH, Klautau GB, Da Silva CB, et al. Improved diagnosis ofinfection associated with osteosynthesis by use of sonication offracture fixation implants. J Clin Microbiol. 2014;52:4176–4182.
33. Thomaidis PC, Pantazatou A, Kamariotis S, et al. Sonication assistedmicrobiological diagnosis of implant-related infection caused byPrevotella disiens and Staphylococcus epidermidis in a patient withcranioplasty. BMC Res Notes. 2015;8:307.
34. Jost GF, Wasner M, Taub E, et al. Sonication of catheter tips forimproved detection of microorganisms on external ventricular drainsand ventriculo-peritoneal shunts. J Clin Neurosci. 2014;21:578–582.
35. Nau R, Sorgel F, Eiffert H. Penetration of drugs through the blood-cerebrospinal fluid/blood-brain barrier for treatment of centralnervous system infections. Clin Microbiol Rev. 2010;23:858–883.
36. Achermann Y, Eigenmann K, Ledergerber B, et al. Factors asso-ciated with rifampin resistance in staphylococcal periprostheticjoint infections (PJI): a matched case-control study. Infection.2013;41:431–437.
37. Widmer AF, Frei R, Rajacic Z, et al. Correlation between in vivo andin vitro efficacy of antimicrobial agents against foreign body infec-tions. J Infect Dis. 1990;162:96–102.
38. Chambers H, Eliopoulos G, Gilbert D, et al. editors. Sanford guide toantimicrobial therapy. Sperryville, USA: Antimicrobial Therapy.2016.
39. Habib G, Lancellotti P, Antunes MJ, et al. 2015 ESC guidelines forthe management of infective endocarditis: the task force for themanagement of Infective endocarditis of the European Society ofCardiology (ESC). Endorsed by: European Association for Cardio-Thoracic Surgery (EACTS), the European Association of NuclearMedicine (EANM). Eur Heart J. 2015;36:3075–3128.
40. Dashti SR, Baharvahdat H, Spetzler RF, et al. Operative intracranialinfection following craniotomy. Neurosurg Focus. 2008;24:E10.
• This manuscript describes clinical and microbiological charac-teristics of craniotomy-associated infections.
41. Morton RP, Abecassis IJ, Hanson JF, et al. Predictors of infectionafter 754 cranioplasty operations and the value of intraoperativecultures for cryopreserved bone flaps. J Neurosurg. 2016;125(3):766–770.
14 A. CONEN ET AL.

42. Riordan MA, Simpson VM, Hall WA. Analysis of factors contributingto infections after cranioplasty: a single-institution retrospectivechart review. World Neurosurg. 2016;87:207–213.
43. Sundseth J, Sundseth A, Berg-Johnsen J, et al. Cranioplasty withautologous cryopreserved bone after decompressive craniectomy:complications and risk factors for developing surgical site infection.Acta Neurochir (Wien). 2014;156:805–811; discussion 11.
44. Iwama T, Yamada J, Imai S, et al. The use of frozen autogenousbone flaps in delayed cranioplasty revisited. Neurosurgery.2003;52:591-6; discussion 5-6.
45. Moreira-Gonzalez A, Jackson IT, Miyawaki T, et al. Clinical outcomein cranioplasty: critical review in long-term follow-up. J CraniofacSurg. 2003;14:144–153.
46. Schwarz F, Dunisch P, Walter J, et al. Cranioplasty after decom-pressive craniectomy: is there a rationale for an initial artificialbone-substitute implant? A single-center experience after 631 pro-cedures. J Neurosurg. 2016;124:710–715.
47. Yadla S, Campbell PG, Chitale R, et al. Effect of early surgery, material,and method of flap preservation on cranioplasty infections: a sys-tematic review. Neurosurgery. 2011;68:1124–1129; discussion 30.
48. Sacar S, Turgut H, Toprak S, et al. A retrospective study of centralnervous system shunt infections diagnosed in a university hospitalduring a 4-year period. BMC Infect Dis. 2006;6:43.
49. von der Brelie C, Simon A, Groner A, et al. Evaluation of an institu-tional guideline for the treatment of cerebrospinal fluid shunt-associated infections. Acta Neurochir (Wien). 2012;154:1691–1697.
50. Korinek AM, Fulla-Oller L, Boch AL, et al. Morbidity of ventricularcerebrospinal fluid shunt surgery in adults: an 8-year study.Neurosurgery. 2011;68:985–994; discussion 94-5.
51. Borgbjerg BM, Gjerris F, Albeck MJ, et al. A comparison betweenventriculo-peritoneal and ventriculo-atrial cerebrospinal fluidshunts in relation to rate of revision and durability. ActaNeurochir (Wien). 1998;140:459–464; discussion 65.
52. Lam CH, Villemure JG. Comparison between ventriculoatrial andventriculoperitoneal shunting in the adult population. Br JNeurosurg. 1997;11:43–48.
53. Olsen L, Frykberg T. Complications in the treatment of hydroce-phalus in children. A comparison of ventriculoatrial and ventricu-loperitoneal shunts in a 20-year material. Acta Paediatr Scand.1983;72:385–390.
54. Burstrom G, Andresen M, Bartek J Jr., et al. Subacute bacterial endo-carditis and subsequent shunt nephritis from ventriculoatrial shunt-ing 14 years after shunt implantation. BMJ Case Rep. 2014;2014.
55. James HE, Walsh JW, Wilson HD, et al. The management of cere-brospinal fluid shunt infections: a clinical experience. ActaNeurochir (Wien). 1981;59:157–166.
56. Walti LN, Conen A, Coward J, et al. Characteristics of infectionsassociated with external ventricular drains of cerebrospinal fluid. JInfect. 2013;66:424–431.
•• This article describes clinical and diagnostic findings of exter-nal ventricular drainage-associated infections compared to thetime of drainage insertion.
57. Beer R, Lackner P, Pfausler B, et al. Nosocomial ventriculitis andmeningitis in neurocritical care patients. J Neurol. 2008;255:1617–1624.
• This review comprehensively describes risk factors and clinicalcharacteristics of ventricular drainage-associated infectionsand includes a management algorithm.
58. Ramanan M, Lipman J, Shorr A, et al. A meta-analysis of ventricu-lostomy-associated cerebrospinal fluid infections. BMC Infect Dis.2015;15:3.
59. Holloway KL, Barnes T, Choi S, et al. Ventriculostomy infections: theeffect of monitoring duration and catheter exchange in 584patients. J Neurosurg. 1996;85:419–424.
60. Leib SL, Boscacci R, Gratzl O, et al. Predictive value of cerebrospinalfluid (CSF) lactate level versus CSF/blood glucose ratio for thediagnosis of bacterial meningitis following neurosurgery. ClinInfect Dis. 1999;29:69–74.
61. Pfausler B, Beer R, Engelhardt K, et al. Cell index–a new parameterfor the early diagnosis of ventriculostomy (external ventriculardrainage)-related ventriculitis in patients with intraventricularhemorrhage? Acta Neurochir (Wien). 2004;146:477–481.
62. Tunkel AR, Hartman BJ, Kaplan SL, et al. Practice guidelines for themanagement of bacterial meningitis. Clin Infect Dis. 2004;39:1267–1284.
63. Schade RP, Schinkel J, Roelandse FW, et al. Lack of value of routineanalysis of cerebrospinal fluid for prediction and diagnosis ofexternal drainage-related bacterial meningitis. J Neurosurg.2006;104:101–108.
64. Hader WJ, Steinbok P. The value of routine cultures of the cere-brospinal fluid in patients with external ventricular drains.Neurosurgery. 2000;46:1149–1153; discussion 53-5.
65. Klimo P Jr., Thompson CJ, Baird LC, et al. Pediatric hydrocephalus:systematic literature review and evidence-based guidelines. Part 7:antibiotic-impregnated shunt systems versus conventional shuntsin children: a systematic review and meta-analysis. J NeurosurgPediatr. 2014;14(Suppl 1):53–59.
66. Follett KA, Boortz-Marx RL, Drake JM, et al. Prevention and manage-ment of intrathecal drug delivery and spinal cord stimulation sys-tem infections. Anesthesiology. 2004;100:1582–1594.
67. Shamji MF, Westwick HJ, Heary RF. Complications related to the useof spinal cord stimulation for managing persistent postoperativeneuropathic pain after lumbar spinal surgery. Neurosurg Focus.2015;39:E15.
68. Cameron T. Safety and efficacy of spinal cord stimulation for thetreatment of chronic pain: a 20-year literature review. J Neurosurg.2004;100:254–267.
69. Bjerknes S, Skogseid IM, Saehle T, et al. Surgical site infections afterdeep brain stimulation surgery: frequency, characteristics and man-agement in a 10-year period. PLoS One. 2014;9:e105288.
• This review describes clinical and microbiological characteris-tics and treatment outcome of deep brain stimulator-asso-ciated infections.
70. Sillay KA, Larson PS, Starr PA. Deep brain stimulator hardware-related infections: incidence and management in a large series.Neurosurgery. 2008;62:360–366; discussion 6-7.
71. Bhatia R, Dalton A, Richards M, et al. The incidence of deep brainstimulator hardware infection: the effect of change in antibioticprophylaxis regimen and review of the literature. Br J Neurosurg.2011;25:625–631.
EXPERT REVIEW OF ANTI-INFECTIVE THERAPY 15