Embed Size (px)
Citation preview

MANAGEMENT OF MANAGEMENT OF LABORLABOR
Dr Samar SarsamDr Samar Sarsam

• Admission assessment• *History: History of previous births. The
initial assessment of labor should include a review of the patient's prenatal care, including confirmation of the estimated date of delivery. Focused history taking should be conducted to include information, such as the frequency and time of onset of contractions, the status of the amniotic membranes (whether spontaneous rupture of the membranes has occurred, and if so, whether the amniotic fluid is clear or meconium stained), the fetal' movements, and the presence or absence of vaginal bleeding.

Braxton-Hicks contractions, which are often irregular and which do not increase in frequency with increasing intensity, must be differentiated from true contractions. Braxton Hicks contractions often resolve with ambulation or a change in activity. However, true labor contractions tend to be long and intense, and they tend to lead to cervical change. True labor is defined as uterine contractions leading to cervical changes. If contractions occur without cervical changes, it is not true labor. Other causes for the cramping should be diagnosed. Gestational age is not a part of the definition of labor.

In addition, Braxton-Hicks contractions occur occasionally, usually no more than 1-2 per hour, and they often occur just a few times per day. Labor contractions are persistent, they may start as infrequently as every 10-15 minutes, but they accelerate over time, increasing to 1 every 2-3 minutes.
Patients may also describe what has been called lightening, ie, physical changes felt because the fetus' head is advancing into the pelvis. The mother may feel that her baby has become light or that it as started to drop and the shape of her abdomen may change to reflect descent of the fetus. Her breathing may be relieved because tension on the diaphragm is reduced, whereas urination may become frequent because of added pressure on the bladder.

*General examination: Physical examination should include
documentation of the patient's height, weight, vital signs, the fetus' presentation, and the fetus' wellbeing. The frequency, duration, and intensity of uterine contractions should be assessed.

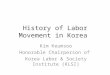
*Abdominal examination begins with inspection, and the Leopold maneuvers described below.
The initial maneuver involves the examiner placing both of his or her hands on each upper quadrant of the patient's abdomen and gently palpating the fundus with the tips of the fingers to define which fetal pole is present in the fundus. If it is the fetus' head, it should feel hard and round. In a breech presentation, a large, nodular body is felt.


The second maneuver involves palpation in the paraumbilical regions with both hands by applying gentle but deep pressure. The purpose is to differentiate the fetal spine (a hard, resistant structure) from its limbs (irregular, mobile small parts) to determinate the fetus' position.
The third maneuver is suprapubic palpation by using the thumb and fingers of the dominant hand. As with the first maneuver, the examiner ascertains the fetus' presentation and estimates its station. If the presenting part is not engaged, a movable body (usually the fetal occiput) can be felt. This maneuver also allows for an assessment of the fetal weight and of the volume of amniotic fluid.

The fourth maneuver involves palpation of bilateral lower quadrants with the aim of determining if the presenting part of the fetus is engaged in the mother's pelvis. The examiner stands facing the mother's feet. With the tips of the first 3 fingers of both hands, the examiner exerts deep pressure in the direction of the axis of the pelvic inlet. In a cephalic presentation, the fetus' head is considered engaged if the examiner's hands diverge as they trace the fetus' head into the pelvis.

• *Vaginal examination is performed in a sterile fashion to decrease the risk of infection. Use of sterile gloves is preferred. If membrane rupture is suspected, examination with a sterile speculum is performed to visually confirm pooling of amniotic fluid in the posterior fornix. The examiner also looks for fern on a dried sample of the vaginal fluid under a microscope and checks the pH of the fluid by using a nitrazine stick or litmus paper, which turns blue if the amniotic fluid is alkalotic. If frank bleeding is present, pelvic examination should be deferred until placenta previa is excluded with ultrasonography. Furthermore, the pattern of contraction and the patient's presenting history may provide clues about placental abruption.

Digital examination of the vagina allows the clinician to determine the following: (1) the degree of cervical dilatation, which ranges from 0 cm (closed or fingertip) to 10 cm (complete or fully dilated), (2) the effacement (assessment of the cervical length, which is often reported as a percentage of the normal 3- to 4-cm-long cervix), (3) the position, ie, anterior or posterior, and (4) the consistency, ie, soft or firm. Palpation of the presenting part of the fetus allows the examiner to establish its station, by quantifying the distance of the body (-5 to +5 cm) that is presenting relative to the maternal ischial spines, where 0 station is in line with the plane of the maternal ischial spines).

The shape of the mother's pelvis can also be assessed and classified into 4 broad categories. Gynecoid, anthropoid, android, and platypelloid. Although the gynecoid and anthropoid pelvic shapes are thought to be most favorable for vaginal delivery, many women can be classified into 1 or more pelvic types, and the distinctions can be arbitrary.

*ADMISSION MANAGEMENT Identification of labor and differentiation
between true and false labor. True labor: contractions regular, intervals
shortens increase intensity. Cervix dilates. Discomfort in the back and abdomen. Discomfort is not stopped by sedation.

Fetal assessment in labor (intrapartum fetal monitoring)
After admission to the labor room, a review of history risk factors as hypertension, D.M, APH and others. Examination reveal breech, IUGR, oligohydramnios, twins, etc. admission CTG is recommended—if all are reassuring so woman mobilization for the next few hours is recommended with intermittent auscultation of fetal heart using fetal stethoscope this can be done at intervals of 15-30 minutes. If there is any abnormality then electronic monitoring is undertaken.




Information about fetal condition from clinical and electronic assessment:
*Meconium and liquor volume: color, consistency and amount of amniotic fluid are used to assess the fetus. Reduced liquor may predispose to cord occlusion, fetal hypoxia.
The appearance of meconium staining of the amniotic fluid is important it could be due to maturity or fetal compromise. The appearance of meconium is an indication for electronic fetal monitoring, and the possibility that the fetus may develops meconium aspiration intrapartum or after delivery with the onset of breathing. This is why some advise ARM early in labor. The healthy fetus is able to withstand the stresses of labor; head compression, umbilical cord compression and reduced placental blood flow. But on occasion may become distressed which can be diagnosed with electronic fetal monitoring and fetal scalp PH measurement.

*Cardiotocography: The CTG records the fetal heart rate on a paper strip. This is carried out either by external abdominal transducer or fetal scalp attachment through the vagina.
Uterine contractions are felt with the palm of the hand and also recorded on the strip by external or internal monitoring.
The recorded rate may be the mother's heart rate, this may occur in obese women or with polyhydramnious or with fetal movements.

Components of CTG: *Baseline rate: 110-150 bpm. *Baseline variability: it is variation in
baseline rate over 1 minute normal value is 10-25 bpm.



*Accelerations (reactivity): increase in fetal heart rate with an amplitude > 15 bpm for at least 15 seconds, normally 2 accelerations per 15 minutes.
*Decelerations: slowing of fetal heart rate from the baseline, they are significant when they are 15 bpm less than the baseline for at least 15 seconds. They are described in amplitude, duration, shape (v or u shape) and lag time of the deceleration in relation the peak of contraction. The u decelerations whose lag time is relatively long (late deceleration) are significant, while deceleration with contraction and with short lag time (early deceleration), and v shaped are less significant.
Continuous fetal heart monitoring is better than intermittent auscultation. Whenever there is concern about fetal heart rate, fetal acid base measurement is indicated.

*Fetal scalp blood sampling: hypoxia in the fetus leads to increase vagal tone which lead to fetal bradycardia, prolonged hypoxia results in increase catecholamines from the adrenal gland it will overcome the vagal bradycardia so fetal heart rate increase. Fetal hypoxia leads to fetal academia. Saling in the 1960s described a method by puncturing the fetal skin to get a blood sample, to measure the capillary PH. Normal PH level is 7.28-7.34 and a value of 7.2 is the lower limit of fetal blood PH accepted during labor.
*Fetal pulse oximetry *Fetal ECG

Management of nonreassuring fetal heart rate pattern:
-Repositioning of the patient -Stop oxytocic agents -Vaginal examination -Correct maternal hypotension -Oxygen to the mother -Fetal heart rate monitoring -Request for newborn care -Emergency delivery

Vaginal examination: cervical effacement, dilatation, position of cervix, station of presenting part.
Detection of ruptured membranes: leakage of fluid from the vagina, speculum examination, or PH of the vagina is 4.5-5.5 while of amniotic fluid it is 7-7.5or finding arborization on a slide of vaginal fluid or the use of nitrazine.
Vital signs and review of pregnancy recordRecording vital signs, pulse and bl. pr hourly
and temperature every 3 hours.

• Preparation of the vulva and perineum
• Enema: is not routinely used.• Laboratory: hematocrit or Hb
concentration, blood group, urine sample for sugar, ketones, proteins and blood.

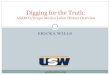
The partogram: it is a graphic record of labor; it allows visual assessment of the progress of labor so active management can be instituted if progress is slow.
It has been introduced by Friedman in 1954. The gradual rise in the latent phase (0-3 cm dilatation) is followed by the steep slope of the active phase (4-9 cm) and then short steep curve to full dilatation. The latent phase last between 3 and 8 hours, the active phase last between 2 and 6 hours depending on parity and other factors.

The rate of cervimetric progress (cervical dilatation), and the descent of the presenting part represent the measure of progress of labor. The descent is observer through the rule of five abdominally and the level of the presenting part in relation to the ischial spine vaginally.
Records of uterine contractions and its frequency and strength.
Ultrasound scan during labor: portable U/S is now present for bedside diagnosis in the labor room.
Pain relief The use of pethidin, epidural analgesia and others
will be discussed in other lecture.

Management of normal labor
The first stage of laborFrom diagnosis till full dilatation. The principles of management are:Care and supportProgress of laborMonitor fetal well being Pain relief as the patient wish Adequate hydration.

Average duration of the first stage of labor in nulliparous women is about 7 hours and in parous women is 4 hours, there are marked individual variations.
The variability is more in the latent phase depending on the cervical effacement and the Bishop score.
The membranes may be ruptured or not, intermittent monitoring of fetal heart rate, maternal BP, pulse, temperature also monitored.
In a normal first stage, encourage mobilization; eat light diet, vaginal examination every 4 hours. Progress of labor is plotted on a Partogram, bladder emptying every few hours.

If abnormal labor; continuous CTG, antacid to the mother, epidural and urinary catheter.
Maternal vital signs at least every 3 hours, if membranes are ruptured check the temperature every hour and start antimicrobial in cases with prolonged rupture membranes.
Periodic vaginal examination every 2-3 hours to evaluate the progress of labor.
Liquid oral intake may need intravenous fluid to administer oxytocin.
Maternal position: allow the women to lie in the lateral position or any position she is comfortable.
Analgesia: the timing, method of administration, and size of initial and subsequent doses of systematically acting analgesic agents are based on the anticipated interval of time until delivery.
Amniotomy: artificial rupture of membranes may be indicated.
Urinary bladders function: encourage voiding.

Second stageWith full dilatation of the cervix the woman begins to
bear down and with the descent of the presenting part she develops the urge to defecate. Uterine contractions and the expulsive forces may last for 1 and 1/2 minutes and recur after myometrial resting of no more than a minute.
Duration of the second stage is 50 minutes in nulliparous and 20 minutes in multiparous, but with analgesia it may be prolonged to more than 2 hours.
Fetal heart rate may be slowed due to cord and head compression.
Auscultation in the second stage may be every 15 minutes in low risk group and every 5 minutes in high risk group.

Maternal tachycardia which is common in the second stage may be mistaken for fetal heart.
Expulsive forces: in most cases bearing down is reflex and spontaneous during the second stage, instruction should be given to the mother regarding the bearing down with contraction and resting in between, also the position the recumbent or the squatting position or the dorsal lithotomy position.
Preparation for labor: the position, cleaning the vulva and the perineum.
Descent and delivery of the head: it is judged by watching the perineum, when the head no longer recedes between contractions (crowning), this indicates that the head has passed through the pelvic floor and delivery is imminent. The midwife must control head delivery to prevent sudden birth, so with crowning the patient should take rapid shallow breaths, carefully deliver the head by applying pressure through the perineum onto the forehead. Episiotomy is sometimes needed to prevent perineal tear it is done with crowning.

Delivery of the shoulders and rest of the body: after the birth of the fetal head check the cord round the neck if it is tight around the neck so clamping is indicated, if there is meconium nasopharyngeal suction is mandatory to prevent aspiration. External rotation occur we apply gentle pull on the head downwards and forwards until the anterior shoulder appears, the head is now lifted until the posterior shoulder appears then deliver the body and legs.

Immediate care to the neonateAfter delivery the fetus takes its first breath within
seconds. No need for immediate clamping because about 80 ml of blood will go to the baby from the placenta before cord pulsation cease. Keep the head in dependent position to allow the drainage of secretions. After clamping the cord, I minute Apgar score assessed then place the fetus on the mother's abdomen. Give vitamin K and do general examination for the baby for any abnormality and a wrist label attached for identification.
Apgar score: is the clinical evaluation of the newborn it is usually recoded at I and 5 minutes.

Sign 0 1 2 Heart rate Absent Below 100 beat Over 100 beat Respiratory effort Absent Weak Good strong cry Muscle tone Limp Some flexion Active motion, well flexed extremities Reflex irritability No response Grimace Cry Color Blue, pale Body pink; Completely pink extremities blue

Third stage of labor
Delivery of the placenta

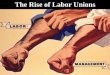
SEPARATION OF AMNIOCHORION. PLACENTAL EXTRUSION. The retroplacental hematoma either follows the placenta or is found within the
inverted sac. In this process, known as the Schultze mechanism of placental
expulsion, blood from the placental site pours into the inverted sac, not escaping externally until after extrusion of the

placenta. In the other method of placental extrusion, known as the Duncan mechanism, separation of the placenta occurs first
at the periphery, with the result that blood collects between the membranes and the uterine wall and escapes from the vagina





Third stage It is from delivery of fetus to the expulsion of the
placenta and membranes. It takes 5-10 minutes normally. If longer than 30 minutes it is prolonged. Separation of placenta occurs due to reduction of uterine volume due to contraction and retraction. Cleavage plane develops and the placenta lies in the lower segment of the uterus.
Signs of separation are: lengthening of the cord.Gush of bloodRising of the uterine fundus, it becomes hard and
globular. *Traditionally; we wait for signs of separation of the
placenta then expel it by pressing down on the fundus. This takes 20 minutes and is associated with 5% PPH.

*The modern management of the 3rd stage of labor is active management and involves a procedure called controlled cord traction. This technique is as follows:
1-Synthetic oxytocin 10 IU or syntometrine (5 IU oxytocin, 0.5 mg ergometrine) is given by im injection following delivery of the anterior shoulder. Syntometrine gives a more sustained contraction but must not be used with hypertension.
2-after delivery the attendant should place the left hand on the uterus to identify contraction. During this time observe any bleeding, clamp the cord after 1-2 minutes after delivery of the baby, and identify lengthening of the cord.


3-when contraction is felt the left hand should be put suprapubically to elevate the fundus with the palm facing the mother, at the same time the right hand grasping the cord and exert traction steadily to deliver the placenta gently. In 2% of cases the placenta will not be expelled, if no bleeding further attempt is tried after 10 minutes. If this fails we need evacuation in the theater. After completion inspect the placental cotyledons and examine the vulva for tears or lacerations.





•Fourth stage of labor• Examine the placenta and
membranes and for vaginal and perineal tears. The hour immediately following delivery is critical, the uterus is frequently evaluated and the perineum also should be inspected.

• Active management of labor•The active management of labor refers to
active control, rather than passive observation, over the course of labor by the obstetrical provider .
•There are three essential elements to active management: Careful diagnosis of labor by strict criteria, Constant monitoring of labor with specific standards for normal progression, Prompt intervention (eg, amniotomy, high dose oxytocin) according to established guidelines if progress is unsatisfactory
• •

•It was introduced during the 1960's to shorten the length of labor in nulliparous
women
•POPULATION — The active management of labor is generally limited to women who
meet the following criteria :
•Nulliparous, Term pregnancy, Singleton infant in cephalic presentation, No pregnancy complications, Experiencing
spontaneous onset of labor .