Embed Size (px)
Citation preview

MANAGEMENT OF NORMAL LABOUR AND DELIVERY
Dr Nabeel Bondagji
Consultant Perinatologist
KAUH&KFSH

LECTURE OVERVIEW
• Definitions • Anatomy of the fetal head and maternal
pelvis• Management of 1st, 2nd and 3rd stages of
normal labour– monitoring of maternal well being– monitoring of fetal well-being– monitoring progress of labour

NORMAL LABOUR: Definitions
Onset of regular involuntary coordinated, painful uterine contractions associated with cervical effacement and dilatation
• Delivery is the expulsion of the product of the conception after fetal viability.

TRUE LABOURVX FALES LABOUR
• Regular contractions• Increase in frequency
and intensity• Cervix dilate• No relive with
sedation• Abd and back pain
• Irregular• Remain the same
• Unchanged• relive
• Lower abd

STAGES OF LABOUR 4
• First stage cervical dilatation and effacement
• Second stage is the expulsion of the fetus
• Third stage is the delivery of the placenta
• Fourth stage is the early recovery

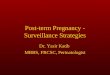
FRIEDMAN’S CURVE

Management of Normal Labour
• Monitor maternal well-being
• Monitor fetal well-being
• Monitor the progress of labour

MECHANICS OF LBOUR, OR,
HOW DOES THE HEAD NEGOTIATE THE PELVIS?
(1) change it’s shape and size (moulding)
(2) change it’s position (flexion and rotation)

ANATOMY OF THE FETAL HEAD
• Largest and least compressible part of the fetus– therefore the most important obstetrically
• Comprises of– (1) base of skull (ossified, non compressible, protecting brain
stem)– (2) cranium
• (a) bones: occipital, 2 parietal, 2 frontal and 2 temporal interconnected with membrane; therefore compressible
• (b) sutures (where the bones meet): saggital, lambdoid, coronal• © fontanelles (where the sutures meet): ant and post
• The compressibility of the fetal skull means the bones can overlap (moulding) in order for the skull to change shape negotiating the maternal pelvis