Embed Size (px)
DESCRIPTION
林口長庚醫院 內科部 感染醫學科 吳丁樹 醫師. Management of Occupational Exposures to HIV. 一位 23 歲林姓護士在照顧一位末期愛滋病人時不慎被 IC 針所刺傷食指 請問如何處理 ? 需要吃抗病毒藥物嗎 ? 吃幾種藥物 ? 吃多久 ?. Post-exposure prophylaxis (PEP). Definitions Exposures Risks Timing and duration of PEP Selection of HIV PEP Regimens - PowerPoint PPT Presentation
Citation preview
林口長庚醫院 內科部 感染醫學科吳丁樹 醫師
一位 23 歲林姓護士在照顧一位末期愛滋病人時不慎被 IC 針所刺傷食指
請問如何處理 ? 需要吃抗病毒藥物嗎 ? 吃幾種藥物 ? 吃多久 ?
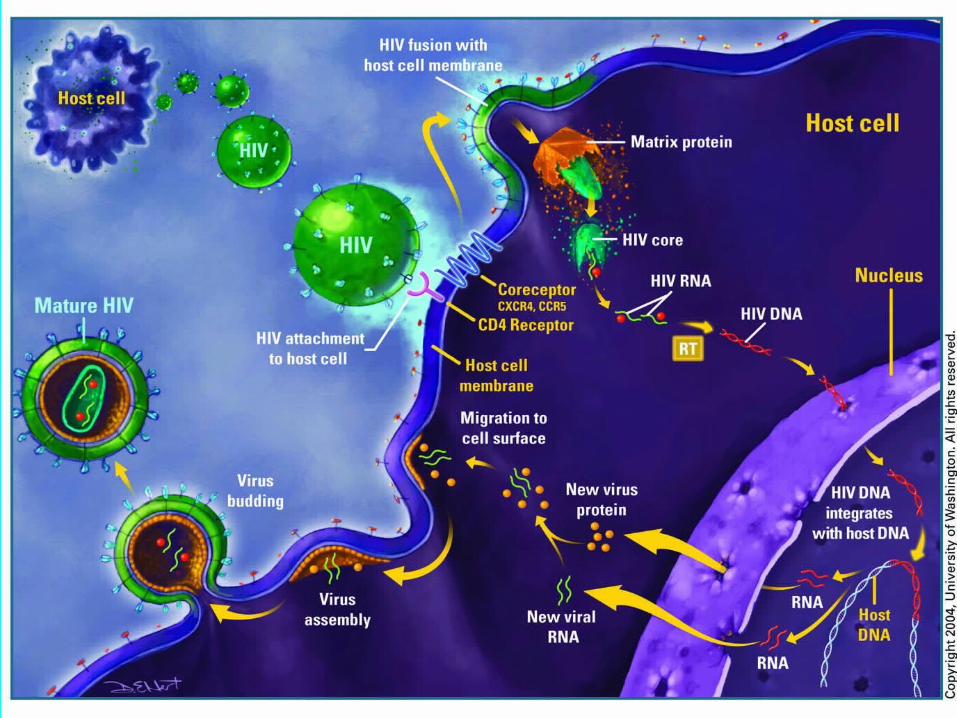
Post-exposure prophylaxis (PEP) Definitions Exposures Risks Timing and duration of PEP Selection of HIV PEP Regimens Special issue in pregnancy Follow-up Post-contact seroconversion in HCWs Infection control strategies
Definition
Health-care personnel (HCP) : all paid and unpaid persons working in health-care settings who have the potential for exposure to infectious materials (e.g., blood, tissue, and specific body fluids and medical supplies, equipment, or environmental surfaces contaminated with these substances).
Exposures Percutaneous injury (e.g., a needlestick or
cut with a sharp object) or Contact of mucous membrane or nonintact
skin (e.g., exposed skin that is chapped, abraded, or afflicted with dermatitis) with blood, tissue, or other body fluids that are potentially infectious.
Visibly bloody body fluids, semen and vaginal secretions also are considered potentially infectious
Exposures
Cerebrospinal fluid, synovial fluid, pleural fluid, peritoneal fluid, pericardial fluid, and amniotic fluid. The risk for transmission of HIV infection from these fluids is unknown.
Feces, nasal secretions, saliva, sputum, sweat, tears, urine, and vomitus are not considered potentially infectious unless they are visibly bloody.
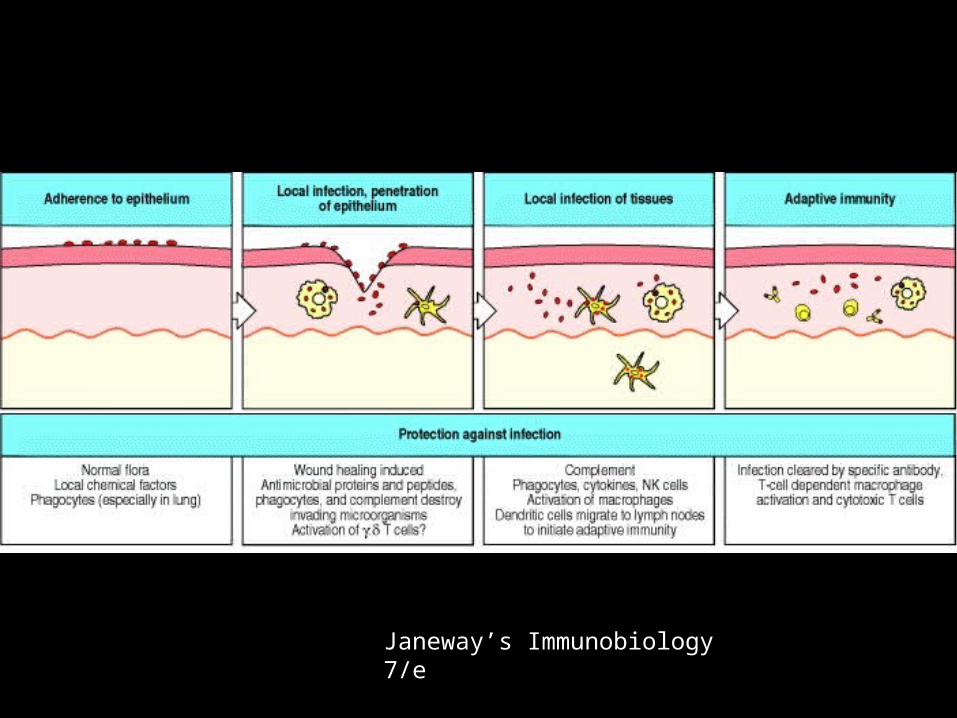
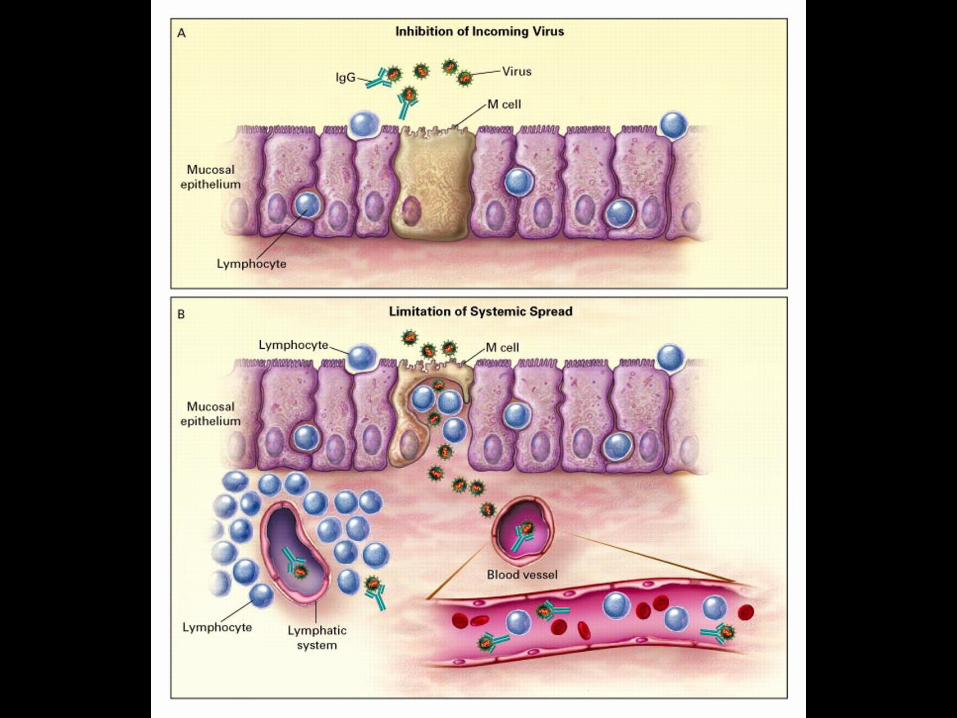
Janeway’s Immunobiology 7/e
Risks the average risk for HIV transmission after a
percutaneous exposure to HIV-infected blood has been estimated to be approximately 0.3%
after a mucous membrane exposure, approximately 0.09%
larger quantity of blood a device (e.g., a needle) visibly contaminated with
the patient’s blood a procedure that involved a needle being placed
directly in a vein or artery a deep injury Terminal HIV-related illness in the source patient.
Controversy
lower viral load (e.g., <1,500 RNA copies/ mL) or one that is below the limits of detection probably indicates a lower titer exposure, it does not rule out the possibility of transmission
Timing and Duration of PEP as soon as possible, preferably within hours
rather than days of exposure Because 4 weeks of ZDV appeared protective
in occupational and animal studies, PEP should be administered for 4 weeks, if tolerated.
Reevaluation of exposed HCP should be strongly encouraged within 72 hours postexposure, especially as additional information about the exposure or source person becomes available.
Science. 1995 Nov 17;270(5239):1197-9. Prevention of SIV Infection in Macaques by (R)-9-(2-
Phosphonylmethoxypropyl)adenine Che-Chung Tsai (1), Kathryn E. Follis, Alexander Sabo, Thomas
W. Beck, Richard F. Grant, Norbert Bischofberger, Raoul E. Benveniste, Roberta Black
The efficacy of pre- and postexposure treatment with the antiviral compound (R)-9-(2-phosphonylmethoxypropyl)adenine (PMPA) was tested against simian immunodeficiency virus (SIV) in macaques as a model for human immunodeficiency virus (HIV). PMPA was administered subcutaneously once daily beginning either 48 hours before, 4 hours after, or 24 hours after virus inoculation. Treatment continued for 4 weeks and the virologic, immunologic, and clinical status of the macaques was monitored for up to 56 weeks. PMPA prevented SIV infection in all macaques without toxicity, whereas all control macaques became infected. These results suggest a potential role for PMPA prophylaxis against early HIV infection in cases of known exposure.
Tenofovir
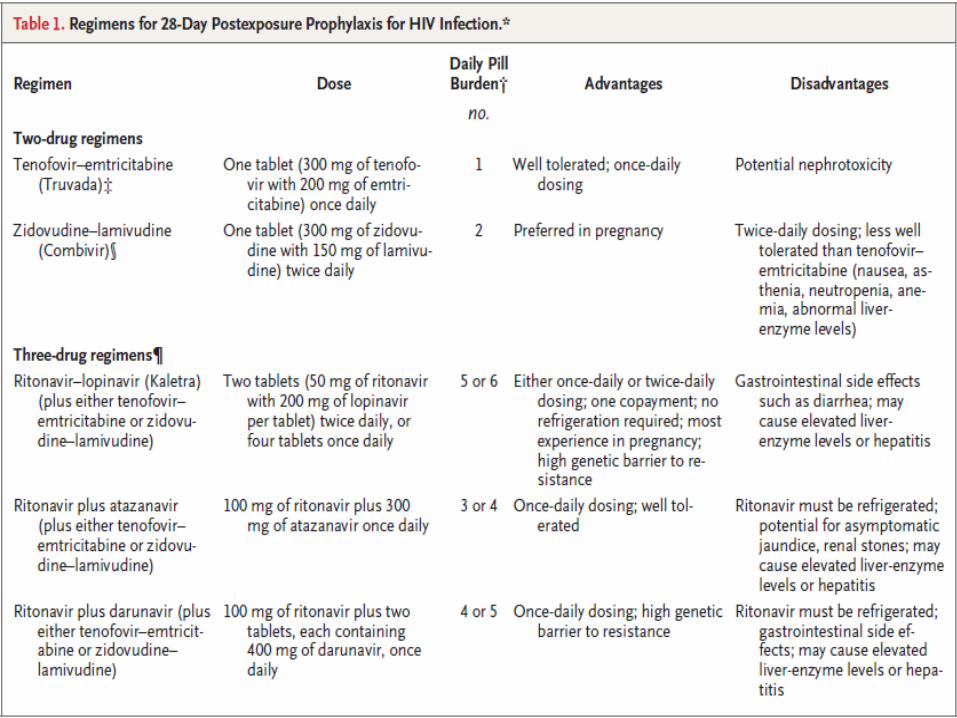
Selection of HIV PEP Regimens 2 drugs or 3 drugs? The main arguments in favour of two-drug PEP
(fewer side effects, better adherence and course completion rates) are being addressed through switching to better-tolerated agents with lower pill burdens.
At the same time, a potent three-drug PEP regimen is preferred because resistance to antiretroviral drugs is found at significant levels in both treated and untreated infected individuals in the UK.
Selection of HIV PEP Regimens the source of the occupational exposure (e.g.,
possible treatment history or antiretroviral drug resistance)
history of and response to antiretroviral therapy based on clinical response, CD4+ T-cell counts, viral load measurements, and current disease stage.
The addition of a third (or even a fourth) drug should be considered for exposures that pose an increased risk for transmission or that involve a source in whom antiretroviral drug resistance is likely.
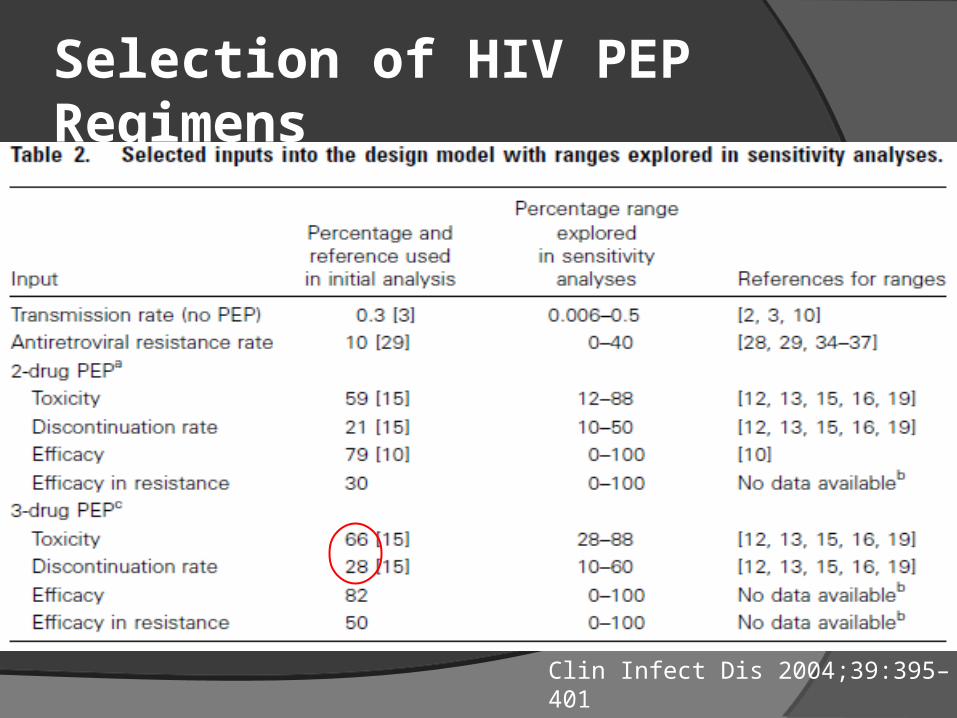
Selection of HIV PEP Regimens
Clin Infect Dis 2004;39:395–401
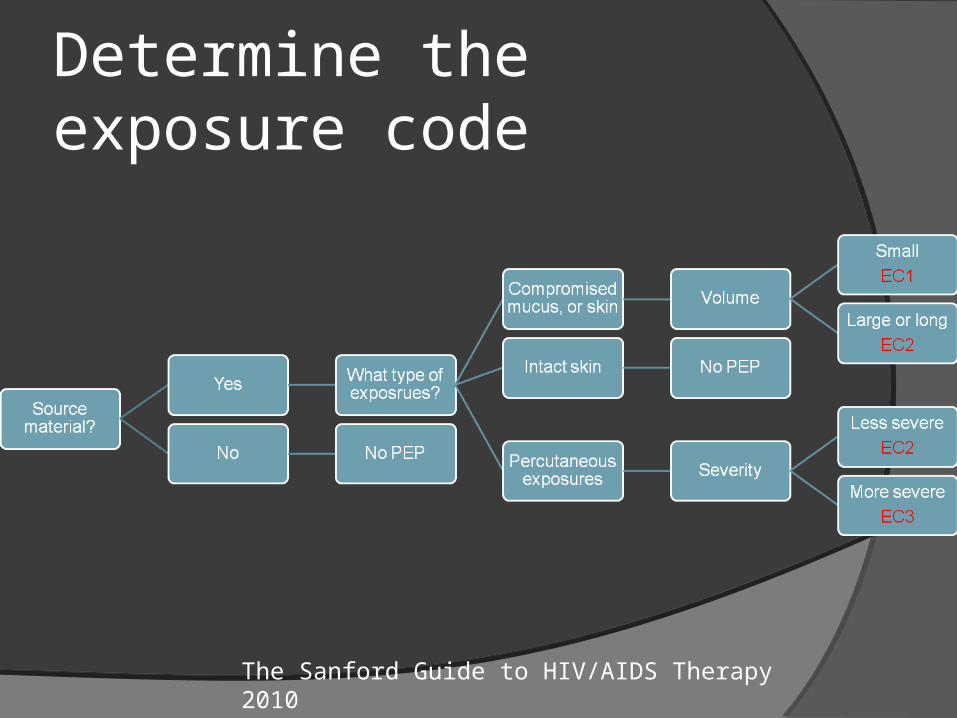
Determine the exposure code
The Sanford Guide to HIV/AIDS Therapy 2010
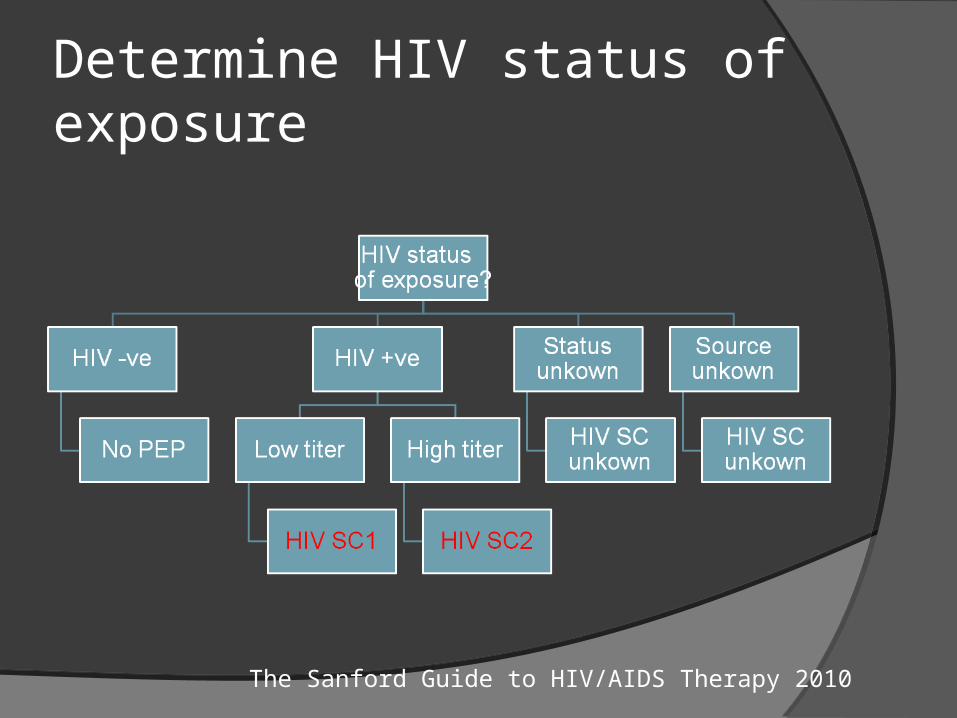
Determine HIV status of exposure
The Sanford Guide to HIV/AIDS Therapy 2010
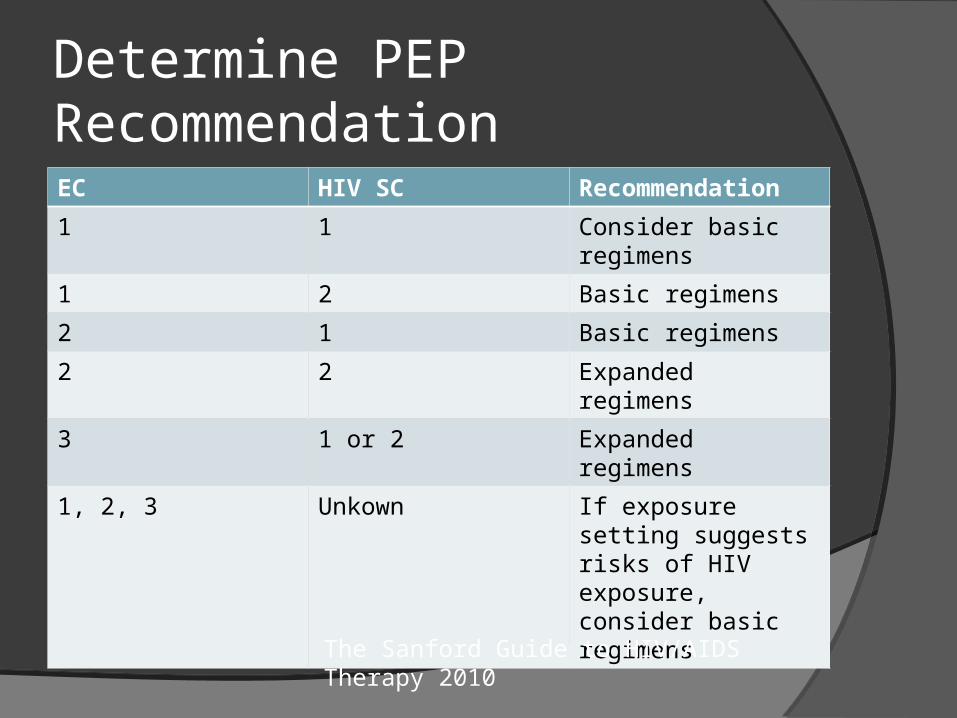
Determine PEP RecommendationEC HIV SC Recommendation
1 1 Consider basic regimens
1 2 Basic regimens
2 1 Basic regimens
2 2 Expanded regimens
3 1 or 2 Expanded regimens
1, 2, 3 Unkown If exposure setting suggests risks of HIV exposure, consider basic regimens
The Sanford Guide to HIV/AIDS Therapy 2010
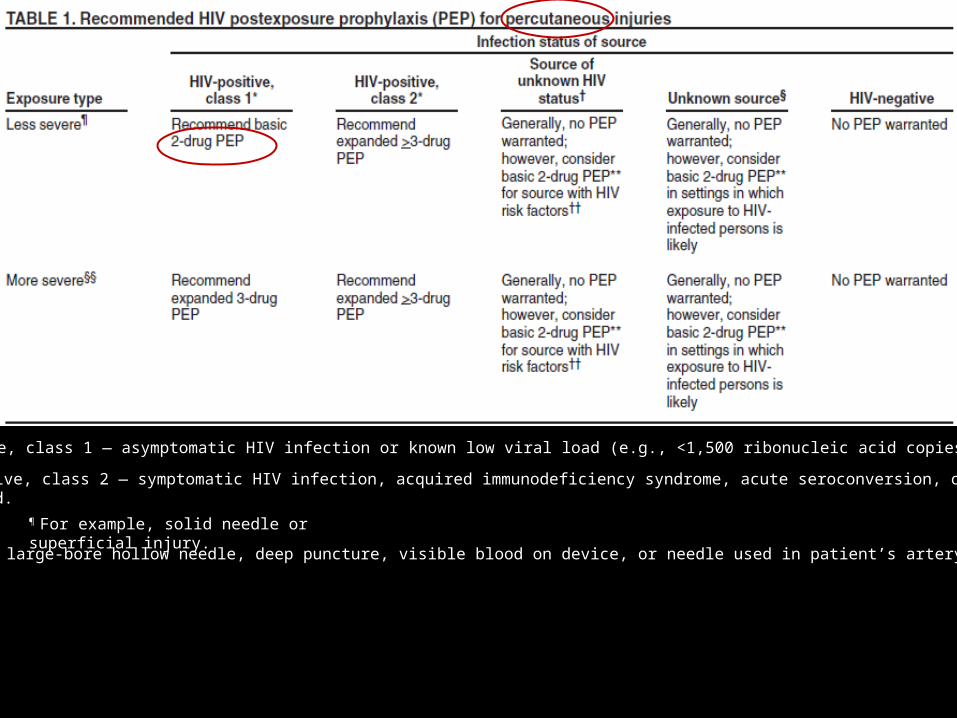
HIV-positive, class 1 — asymptomatic HIV infection or known low viral load (e.g., <1,500 ribonucleic acid copies/mL).
HIV-positive, class 2 — symptomatic HIV infection, acquired immunodeficiency syndrome, acute seroconversion, or known highviral load.
¶ For example, solid needle or superficial injury.
§§ For example, large-bore hollow needle, deep puncture, visible blood on device, or needle used in patient’s artery or vein.
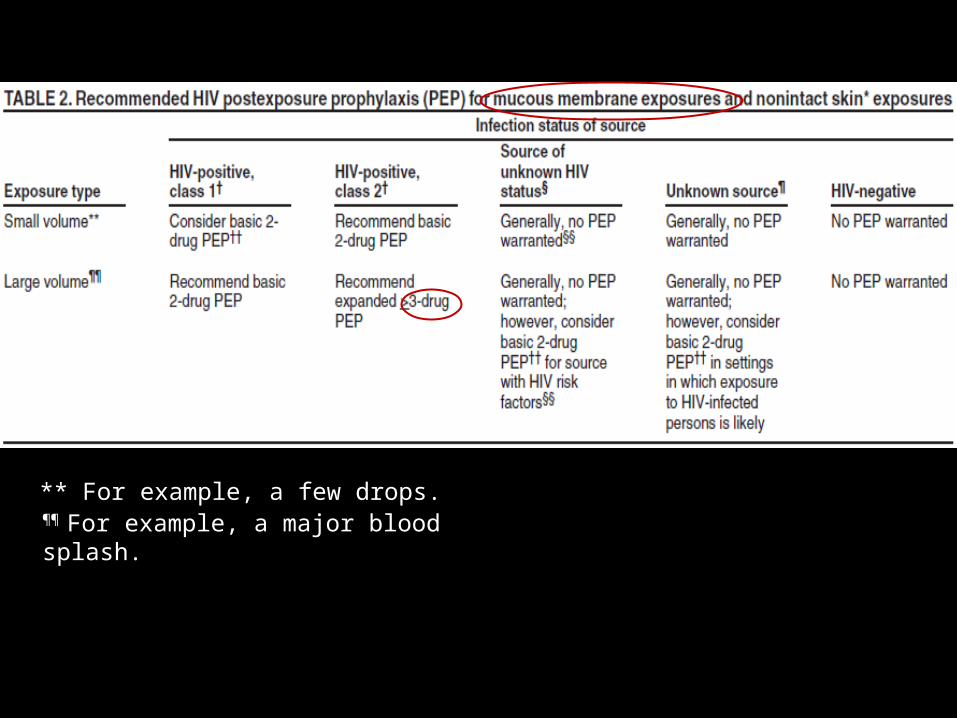
** For example, a few drops. ¶¶ For example, a major blood splash.
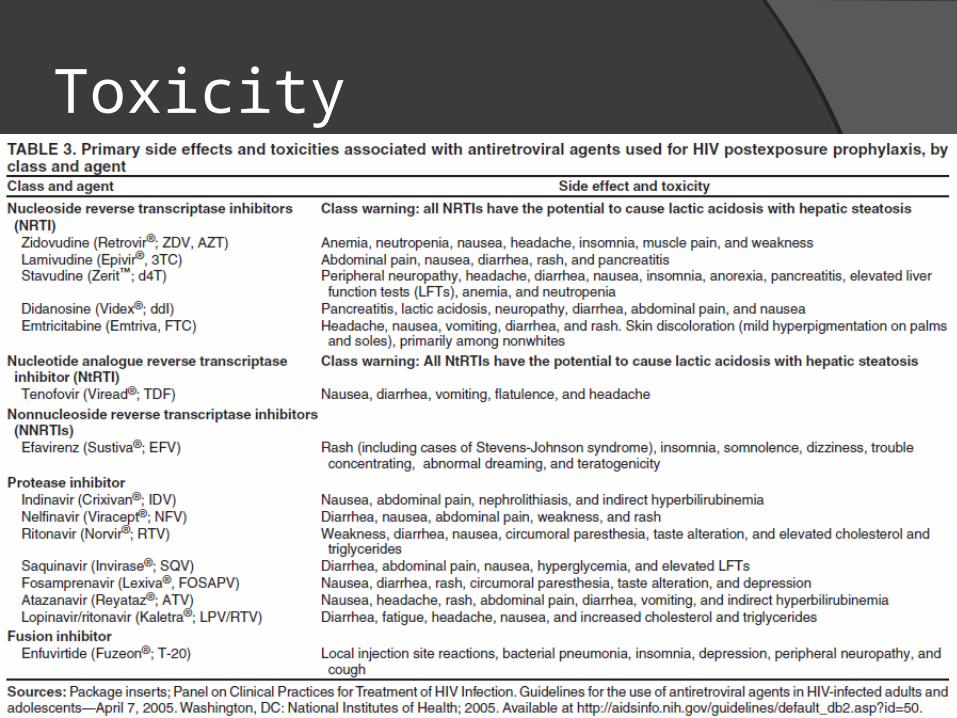
Toxicity
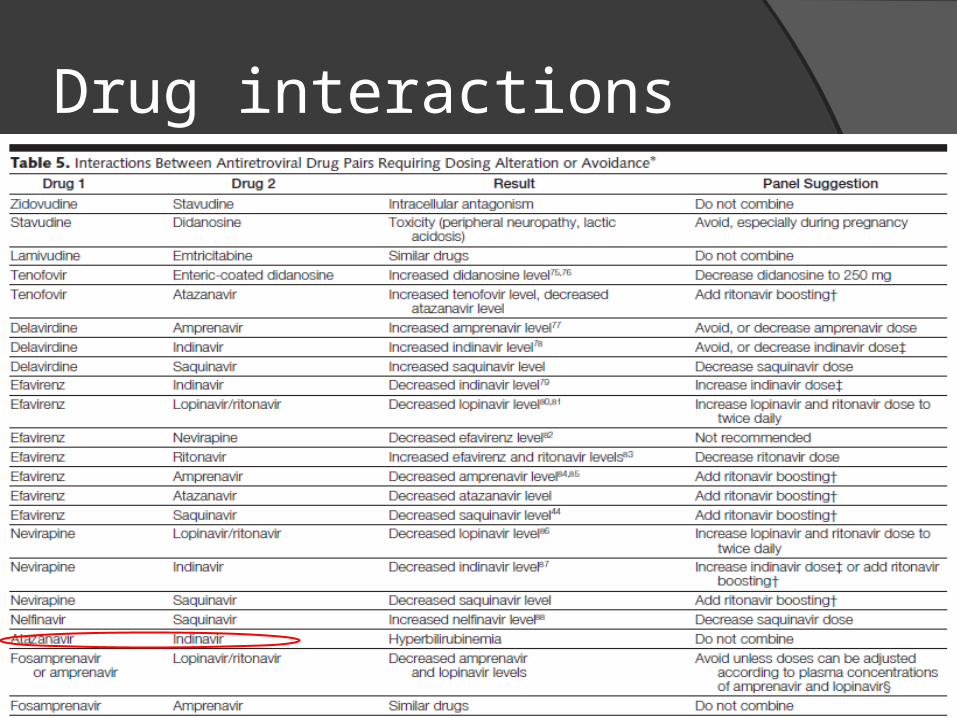
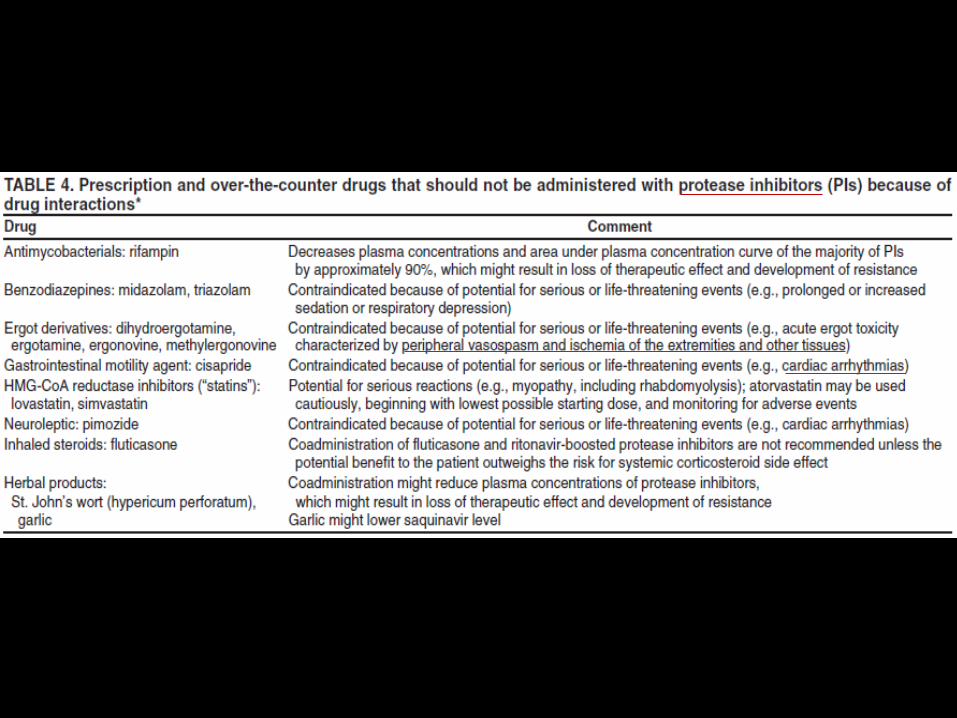
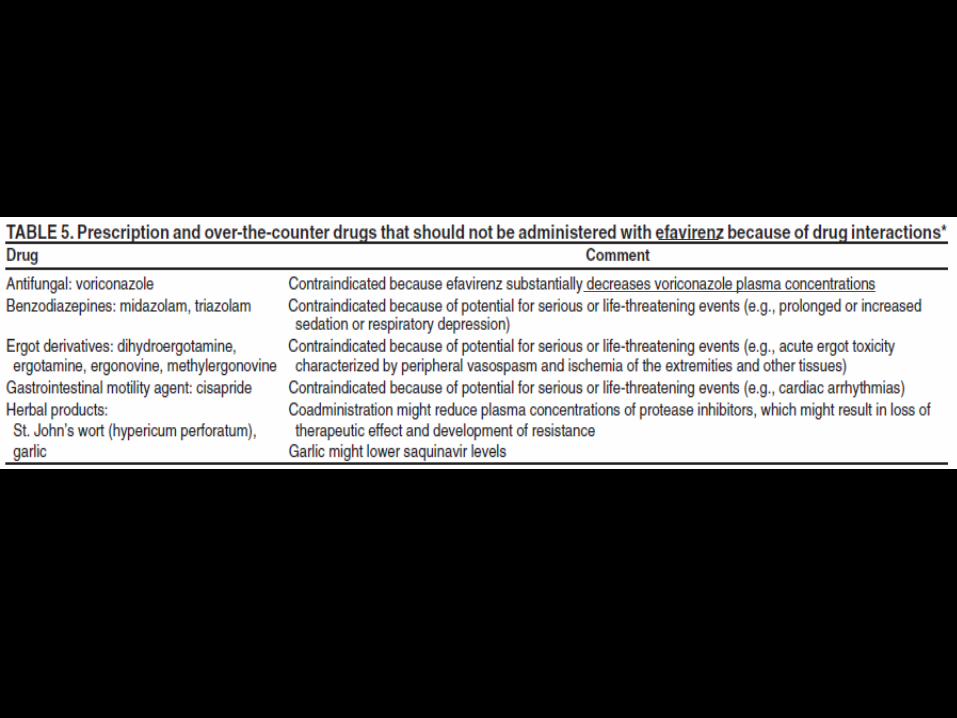
Drug interactions
Drug resistance hitherto undiagnosed; in this case, prevalence of
resistance to any class of drug can be estimated as 5–10%;
already diagnosed, and untreated; these patients are increasingly likely to have had a resistance test undertaken, since baseline testing is recommended;
on treatment with undetectable viral load; they will be of very low infectivity, and will also probably have had a baseline resistance test;
on treatment with detectable viral load; they are likely to have resistant virus and also a recent resistance test.
Pregnancy Urgent pregnancy testing should be arranged for any female
worker who cannot rule out the possibility of pregnancy should be counselled about the risks of HIV infection, about
the risks for transmission to her baby, and about what is known and not known about the potential benefits and risks of antiretroviral therapy for her and her baby
drugs that may cause nausea may exacerbate pregnancy associated nausea
Efavirenz is contraindicated in pregnancy and not recommended for inclusion in PEP regimens
Indinavir (IDV) is associated with infrequent side effects in adults (i.e., hyperbilirubinemia and renal stones) that could be problematic for a newborn.
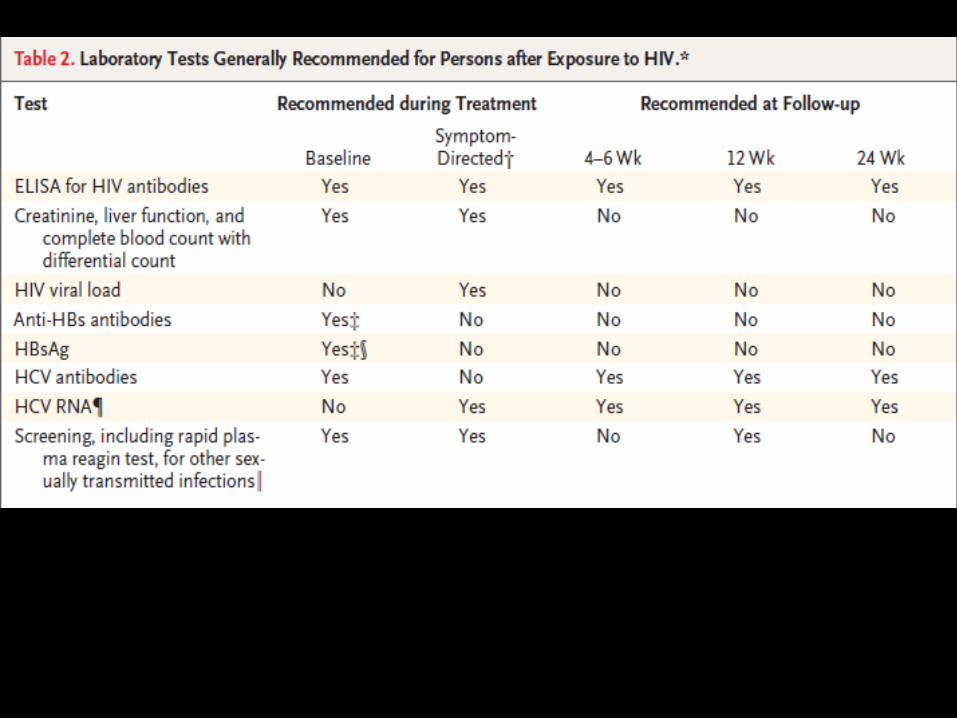
Follow-up
Extended HIV follow-up (e.g., for 12 months) is recommended for HCP who become infected with HCV after exposure to a source coinfected with HIV and HCV.
Am J Med. 1997 May 19;102(5B):115-6.
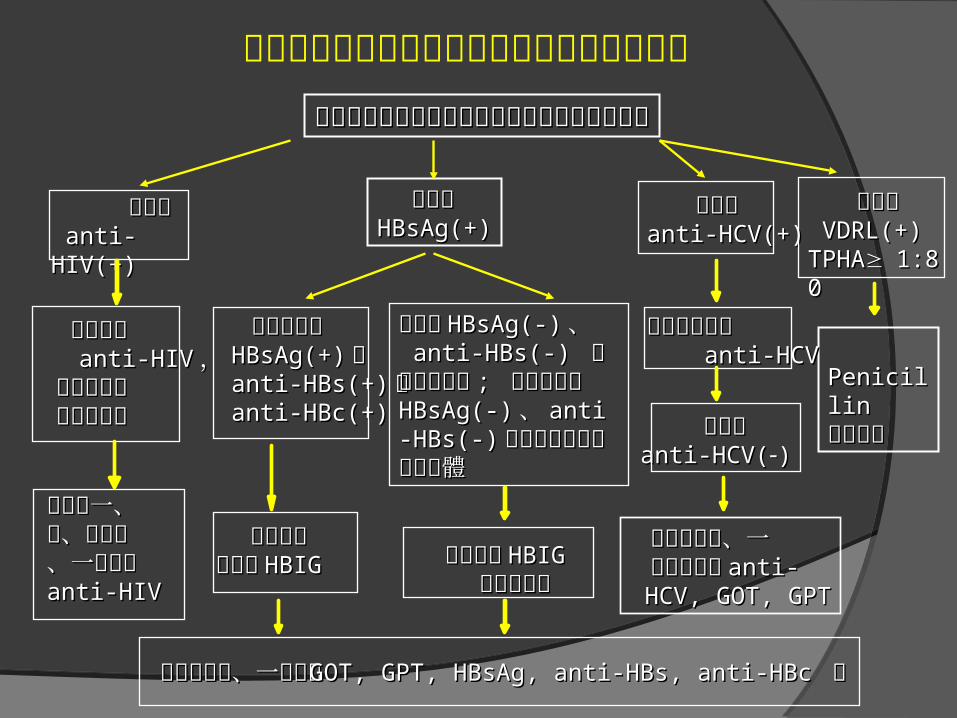
員工污染性尖銳器械傷害後感染追蹤檢驗流程發生被感染病人使用過之物品扎傷或割傷等情況發生被感染病人使用過之物品扎傷或割傷等情況
病人為病人為HBsAg(+)HBsAg(+)
病人為病人為 anti-HIV(+) anti-HIV(+)
病人為病人為anti-HCV(+)anti-HCV(+)
病人為病人為 VDRL(+) VDRL(+) TPHATPHA1:801:80
員工檢驗員工檢驗 anti-HIVanti-HIV ,, 視情況服用視情況服用 抗愛滋藥物抗愛滋藥物
員工本人為員工本人為 HBsAg(+)HBsAg(+) 或或 anti-HBs(+)anti-HBs(+) 或或 anti-HBc(+)anti-HBc(+)
PenicillinPenicillin預防注射預防注射
員工為員工為anti-HCV(anti-HCV())
不需注射不需注射疫苗或疫苗或 HBIGHBIG 儘快注射儘快注射 HBIGHBIG
並接種疫苗並接種疫苗
扎傷後半年、一扎傷後半年、一 年抽血檢驗年抽血檢驗 anti- anti- HCV, GOT, GPTHCV, GOT, GPT
扎傷後半年、一年追蹤扎傷後半年、一年追蹤 GOT, GPT, HBsAg, anti-HBs, anti-HBcGOT, GPT, HBsAg, anti-HBs, anti-HBc 等等
扎傷後一、扎傷後一、三、六個月三、六個月、一年追蹤、一年追蹤anti-HIVanti-HIV
員工抽血檢驗員工抽血檢驗 anti-HCVanti-HCV
員工為員工為 HBsAg(-)HBsAg(-) 、、 anti-HBs(-) anti-HBs(-) 且未注且未注射疫苗射疫苗 ; ; 員工本人為員工本人為HBsAg(-)HBsAg(-) 、、 anti-anti-HBs(-)HBs(-) 已完成注射但已完成注射但未產生抗體未產生抗體
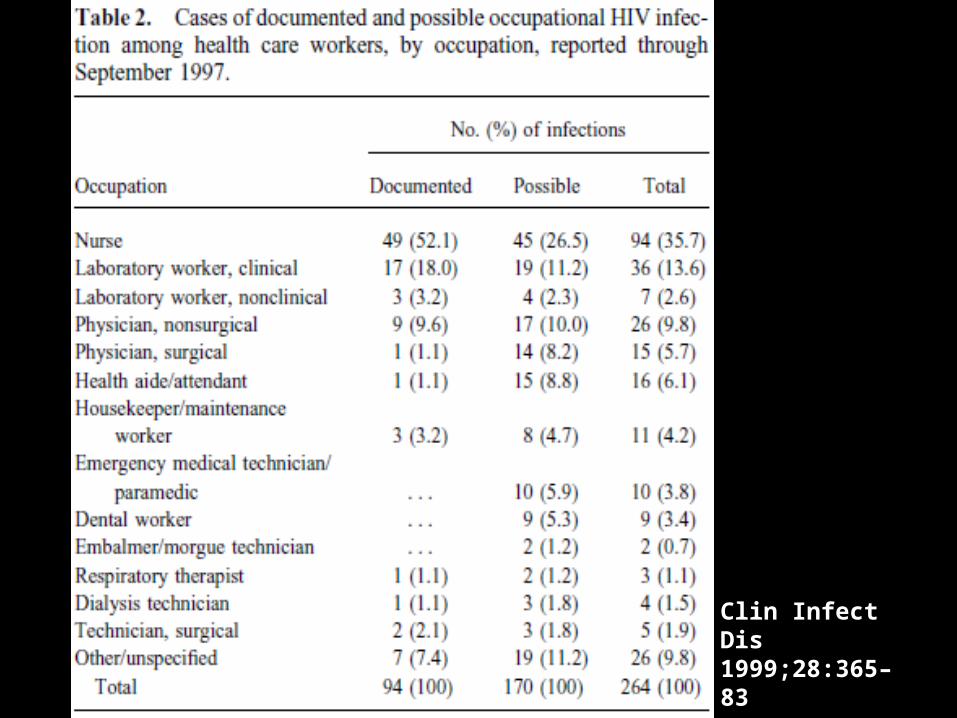
Clin Infect Dis 1999;28:365–83
Occupational HIV infection The majority of documented infections occurred in
nurses or clinical laboratory workers (66 of 94; 70.2%) after contact with infected blood (84 of 94; 89.4%) from a patient with with infected blood (84 of 94; 89.4%) from a patient with AIDS (40 of 52; 76.5%), by percutaneous exposure (83 of 94; 88.3%) during a procedure involving the placement of a device in an artery or vein (43 of 63; 68%).
Clin Infect Dis 1999;28:365–83
Occupational HIV infection Some job categories for which a high exposure
risk has been demonstrated, such as midwives and surgeons.
Eighteen cases of documented HIV infection occurred despite PEP with zidovudine.
Four of these patients had a negative HIV test at 6 months following exposure.
However, testing the HCW again at 1 year post-exposure can be considered for additional reassurance.
Clin Infect Dis 1999;28:365–83
Standard Precautions to Prevent HIV Transmission
Standard precautions (body substance isolation plus universal precautions)core elements:
○ hand washing ○ barrier precautions
barrier precautions to prevent direct contact with all body fluids, except sweat, and tissues
○ minimal manual manipulation of sharp instruments and devices
○ disposal of these items in puncture-resistant containers
Other Measures to Prevent HIV Transmission
Personal protective barriersgloves; gowns; goggles
Safety devicesblunt-tip suture needleneedleless systems
Work techniques Sterilization and disinfection
References Updated U.S. Public Health Service Guidelines for the Management of Occupational Exposures to
HIV and Recommendations for Postexposure Prophylaxis MMWRSeptember 30, 2005 / Vol. 54 / No. RR-9
HIV post-exposure prophylaxis: Guidance from the UK Chief Medical Officers’ Expert Advisory Group on AIDS, Sep, 2008, Department of Health, UK
Tsai CC, Follis KE, Sabo A, Beck TW, Grant RF, Bischofberger N, Benveniste RE, Black R. Prevention of SIV infection in macaques by (R)-9-(2-phosphonylmethoxypropyl)adenine. Science. 1995 Nov 17;270(5239):1197-9.
Bassett IV, Freedberg KA, Walensky RP. Two drugs or three? Balancing efficacy, toxicity, and resistance in postexposure prophylaxis for occupational exposure to HIV. Clin Infect Dis. 2004 Aug 1;39(3):395-401. Epub 2004 Jul 16.
Raphael J. Landovitz, and Judith S. Currier. Postexposure Prophylaxis for HIV Infection. N Engl J Med 2009;361:1768-75.
Cardo DM, Culver DH, Ciesielski CA, Srivastava PU, Marcus R, Abiteboul D, Heptonstall J, Ippolito G, Lot F, McKibben PS, Bell DM. A case-control study of HIV seroconversion in health care workers after percutaneous exposure. Centers for Disease Control and Prevention Needlestick Surveillance Group. N Engl J Med. 1997 Nov 20;337(21):1485-90.
Giuseppe Ippolito, Vincenzo Puro, Julia Heptonstall, Janine Jagger, Gabriella De Carli, and Nicola Petrosillo. Occupational Human Immunodeficiency Virus Infection in Health Care Workers: Worldwide Cases Through September 1997. Clinical Infectious Diseases 1999;28:365–83.
Initiation of Antiretroviral Therapy CD4 count < 350 cells/mm3
Pregnancy, HIV-associated nephropathy, and hepatitis B virus (HBV) coinfection when treatment of HBV is indicated.
Preferred regimens Efavirenz/tenofovir/emtricitabine;
ritonavir-boosted atazanavir + tenofovir/emtricitabine; ritonavir-boosted darunavir + tenofovir/emtricitabine; and raltegravir + tenofovir/emtricitabine.
Lopinavir/ritonavir-based regimens are now listed as “Alternative” instead of “Preferred” regimens, except in pregnant women, where twice-daily lopinavir/ritonavir + zidovudine/lamivudine remains a “Preferred” regimen.
PLASMA HIV RNA TESTING The minimal change in viral load considered to be
statistically significant (2 standard deviations) is a threefold, or a 0.5 log10 copies/mL change.
One key goal of therapy is suppression of viral load to below the limits of detection (below 40–75 copies/mL by most commercially available assays).
For most individuals who are adherent to their antiretroviral regimens and who do not harbor resistance mutations to the prescribed drugs, viral suppression is generally achieved in 12–24 weeks, even though it may take a longer time in some patients.
CD4+ T-CELL COUNT
increase in CD4 count in the range of 50–150 cells/mm3 per year, generally with an accelerated response in the first 3 months.
increase of approximately 50–100 cells/mm3 per year.
Severely depleted CD4 count may have a blunted increase in their count despite virologic suppression.
Drug resistance testing
Genotypic testing is recommended as the preferred resistance testing to guide therapy in patients with suboptimal virologic responses or virologic failure while on first or second regimens
Addition of phenotypic testing to genotypic testing is generally preferred for persons with known or suspected complex drug resistance mutation patterns, particularly to protease inhibitors









![Occupational Exposures in Europe · exposures the characteristics and risk factors of accidents that have led to infection by [HIV, hepatitis B and hepatitis C] will be reviewed,](https://img.pdfslide.net/doc/110x75/5fd3f8b0a832d948220d0dbe/occupational-exposures-in-europe-exposures-the-characteristics-and-risk-factors.jpg)