Embed Size (px)
Citation preview

Hemangioma and Vascular Malformations CenterHemangioma and Vascular Malformations Center
Pediatric Disciplines:Pediatric Disciplines:Hematology and OncologyHematology and OncologyOtolaryngologyOtolaryngologyDermatologyDermatologyGeneral SurgeryGeneral SurgeryPlastic SurgeryPlastic SurgeryInterventional RadiologyInterventional Radiology
Retrospective Chart ReviewRetrospective Chart ReviewA database of patients diagnosed with hemangiomas at the A database of patients diagnosed with hemangiomas at the Hemangioma and Vascular Anomalies Clinic was examined for patienHemangioma and Vascular Anomalies Clinic was examined for patients ts with lesions in a beard distribution from 2004with lesions in a beard distribution from 2004--2007.. Patients were 2007.. Patients were identified and their charts were subsequently explored for identified and their charts were subsequently explored for demographics, birth history, presenting signs and symptoms, medidemographics, birth history, presenting signs and symptoms, medical cal work up, imaging studies, operative reports, and medical and surwork up, imaging studies, operative reports, and medical and surgical gical management.management.
Criteria for Study AdmissionCriteria for Study AdmissionBased on previously reported classification of Based on previously reported classification of ““beardedbearded”” segmental segmental hemangiomas.hemangiomas.11 Patients were required to have four out of five prePatients were required to have four out of five pre--selected facial segments involved with disease. Segments qualifyselected facial segments involved with disease. Segments qualifying ing included the chin, included the chin, submentumsubmentum, neck, , neck, preauricularpreauricular (cheek) areas and (cheek) areas and lower lip.lower lip.
WorkWork--upupHead and neck imaging (MRI or CT scan) examined Head and neck imaging (MRI or CT scan) examined posteriorposterior cranial cranial fossaefossae abnormalities, abnormalities, hhemangioma distribution, and vascular anomalies. emangioma distribution, and vascular anomalies. Echocardiographs were conducted to investigate Echocardiographs were conducted to investigate ccardiac and great ardiac and great vessel aberrations. Consultation with ophthalmology was preformevessel aberrations. Consultation with ophthalmology was preformed to d to explore ocular abnormalities. explore ocular abnormalities. SSternalternal and abdominal defects were and abdominal defects were discovered on physical exam. See Table 1discovered on physical exam. See Table 1
ManagementManagementSpecific disorders of the skin, head and neck, and airway could Specific disorders of the skin, head and neck, and airway could thereby thereby be addressed, while surgical and reconstructive needs were be addressed, while surgical and reconstructive needs were accomplished, by practitioners invested in the teamaccomplished, by practitioners invested in the team’’s treatment plan. s treatment plan. Systemic medical therapy was administered and regulated primarilSystemic medical therapy was administered and regulated primarily by y by the pediatric hematologist and oncologist on the team. the pediatric hematologist and oncologist on the team. MicrolaryngoscopyMicrolaryngoscopy and and bronchoscopybronchoscopy was performed by a pediatric was performed by a pediatric otolaryngologistotolaryngologist using standard techniques previously described. using standard techniques previously described.
lower lip, neck(+)noLower lip, chin, neck, preauricularTerm4F11 lower lip, bil-ear(+)noLower lip, chin, neck, bil-preauricularTerm1.5F10
lower lip, left ear(+)yesLower lip, chin, neck, bil-preauricularTerm3F9
(-)(+)yesLower lip, chin, neck, bil-preauricularTerm10 yrF8
right ear(+)yesLower lip, chin, neck, left-preauricularTerm1.25F7 left ear, neck(+)noChin, neck, bil-preauricualrTerm0.75F6
upper lip(-)yesLower lip, chin, neck, left-preauricularTerm1.25F5 (-)(-)yesChin, neck, bil-preauricularTerm1.25F4
right ear(+)noLower lip, chin, neck, bil-preauricularTerm1.75F3
lower lip(+)noLower lip, chin, neck, bil-preauricular381.5F2
upper lip(+)yesLower lip, chin, neck, left preauricular331.25F1 UlcersUpper Aero lesionsPHACESBeard SitesGestAge Pres (mos)GenderPt #
19 mos6 mosSubmucous resection/ssLTP a/p ccg
Steroid/dilation x2-kenalog injectionsBilateralPharynx, Supraglottis, subcordal, subglottis11
n/a(-)(-)Steroid/vincristine(-)Pharynx, Vallecula10n/a(-)(-)Steroid(-)Pharynx, supraglottis9n/a(-)(-)SteroidScatteredTracheal8n/a(-)(-)SteroidScatteredSupraglottis, subglottis7
Pend6 mosThyroid Ala graftPost Cricoid split
Steroid /vincristineAirway dilation
Posteriorw/ulcer
Pharynx, subcordal, supraglottis, subglottis, trachea6
n/a(-)(-)n/a(-)(-)5
n/a(-)Thyroid Ala graftPost Cricoid split
Steroid / vincristine/ Airway dilationAcquired SGS(-)4
n/a(-)(-)Steroid/laserbilateralSubcordal, subglottis3n/a(-)PendSteroid / vincristineBilateral (left>right)Pharynx, subcordal, supraglottis, subglottis2
32 mos5 wk(-)Steroid / vincristineRight anteriorSubglottis, trachea1DecanTrachOpen/LTPMedical/EndoscopicSubglottic siteLocationsPT #
Subglottic ManagementAerodigestive tract involved
STUDY DESIGN
RESULTS
CONCLUSIONS
Table 3. PHACES abnormalities identified in patients with Beard distribution segmental facial hemangiomas at one institution over a 3 year period. Most common abnormalities were vascular. (pt=patient, Optho=ophthalmologic abnormality, (-)=none)
REFERENCES
RESULTS
Table 4. The location of airway disease in patients with beard distribution segmental hemangiomas. Medical and surgical interventions for airway disease are listed. Subglottic disease has been currently managed effectively with systemic treatment in 5 patients without the need for tracheostomy. One patient is awaiting single stage laryngoytrachealreconstruction (LTP). (trach=tracheostomy, decan=decannulation, pend-pending, (-)=none, n/a=not applicable)
Gresham T. Richter1, Denise M. Adams2, Roshni DasGupta3, Anna W. Lucky4, Richard G. Azizkhan3, and Ravindhra G. Elluru1
Hemangioma and Vascular Malformations Center1Department of Pediatric Otolaryngology-Head and Neck Surgery; Department of Pediatric Hematology and Oncology;
3Department of Pediatric Surgery; 4Department of Pediatric DermatologyCincinnati Children’s Hospital Medical Center, Cincinnati, OH
Management of Patients with Beard Hemangiomas and their Associated Anomalies
Table 1. Hemangioma sites and associated syndromes of 11 patients with beard segmental hemangiomas seen Hemangioma and Vascular Malformations Clinic. 55% of patients had PHACES syndrome, 82% had upper aerodigestive tract involvement (64% subglottic Disease) and 81% developed ulcers at hemagiomassites (Ear and lower lip). (mos=months, Aero-aerodigestive, F=female, yr=year, bil=bilateral, Gest=gestation)
(-)(-)(-)
Aortic Coarctation, Aberrent
Subclavian(-)(-)8
(-)(-)(-)
Tortuous ICA, Persistent stapedial
artery(-)Irregular Vermis9
Protein losing
enterophathy
Optic Nerve Hypoplasia
Sternal CleftSupra-umbilical
RapheTortuous ICA
PDAPatent Foramen
Ovale(-)7
(-)Optic Nerve
Atrophy(-)none(-)(-)5
Intraabdominal
Hemangioma(-)(-)
Aortic Coarctation, Absent ICA and
VAPatent Foramen
Ovale(-)4
(-)ProptosisSternal Raphe
Abdominal RapheAortic hypoplasia
ICA stenosisMitral Stenosis(-)1
OtherOphthoMidline DeformitiesVascularCardiacPosterior FossaePt #
INTRODUCTIONSegmental (or Segmental (or ““diffusediffuse””) hemangiomas are large, broad based lesions ) hemangiomas are large, broad based lesions spanning several anatomic regions with an affinity for the spanning several anatomic regions with an affinity for the neurocutaneousneurocutaneous course of the trigeminal nerve. With simultaneous course of the trigeminal nerve. With simultaneous involvement of the chin, lower lip, parotid and involvement of the chin, lower lip, parotid and preauricularpreauricular regions, regions, these are baptized as segmental hemangiomas in a these are baptized as segmental hemangiomas in a ““beardbeard”” distribution. distribution. Subglottic involvement has been reported to occur in over 60% ofSubglottic involvement has been reported to occur in over 60% ofpatients with beard hemangiomas and has stimulated early endoscopatients with beard hemangiomas and has stimulated early endoscopic pic airway surveillance in symptomatic children.1 The aggressive groairway surveillance in symptomatic children.1 The aggressive growth wth and disfigurement of beard hemangiomas and the risk morbidity frand disfigurement of beard hemangiomas and the risk morbidity from om subglottic lesions warrants early intervention. Therapeutic apprsubglottic lesions warrants early intervention. Therapeutic approaches oaches to both lesions are numerous and comprise the use of systemic anto both lesions are numerous and comprise the use of systemic and d intralesionalintralesional steroids, chemotherapeutic agents, and surgical steroids, chemotherapeutic agents, and surgical extirpation. The unusual and prolonged course of these lesions extirpation. The unusual and prolonged course of these lesions compared to their focal counterparts has further complicated thecompared to their focal counterparts has further complicated their ir management. Treatment decisions in patients with beard hemangiommanagement. Treatment decisions in patients with beard hemangiomas, as, especially those with subglottic involvement, remain complex andespecially those with subglottic involvement, remain complex andrequire the coordinated effort of several pediatric disciplines.require the coordinated effort of several pediatric disciplines.
PHACE syndrome is PHACE syndrome is neurocutaneousneurocutaneous disorder with 100% incidence of disorder with 100% incidence of facial segmental hemangiomas. The disorder includes one or more facial segmental hemangiomas. The disorder includes one or more aberrations of the posterior fossa, large arteries, cardiac struaberrations of the posterior fossa, large arteries, cardiac structures and ctures and eye (Table 1). The identification of eye (Table 1). The identification of sternalsternal clefts in these patients has clefts in these patients has changed the acronym to PHACES. Regardless, 70% of PHACES changed the acronym to PHACES. Regardless, 70% of PHACES patients have only one anomaly in addition to their facial hemanpatients have only one anomaly in addition to their facial hemangioma. gioma. Associations between segmental hemangiomas and new anomalies areAssociations between segmental hemangiomas and new anomalies arealso emerging in the literature. Distribution of the hemangioma also emerging in the literature. Distribution of the hemangioma has has been suspected to be predictive of associated anomalies but thisbeen suspected to be predictive of associated anomalies but thiscurrently remains unclear. Interestingly, PHACES often occurs wicurrently remains unclear. Interestingly, PHACES often occurs with th the involvement of only one facial segment hemangioma. The the involvement of only one facial segment hemangioma. The relationship between beard hemangiomas and PHACES anomalies has relationship between beard hemangiomas and PHACES anomalies has not been elucidated. This present study examines patients with not been elucidated. This present study examines patients with hemangiomas in a beard distribution with a report on less commonhemangiomas in a beard distribution with a report on less commonly ly known associated anomalies that are important to evaluate upon known associated anomalies that are important to evaluate upon presentation. The object is to increase awareness of otolaryngolpresentation. The object is to increase awareness of otolaryngologists ogists of the disorders associated with beard hemangiomas, draw patternof the disorders associated with beard hemangiomas, draw patterns to s to their involvement, and discuss management options based upon clitheir involvement, and discuss management options based upon clinical nical experience and literature review. experience and literature review.
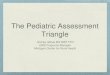
Figure 1: Three infants with typical “beard” distribution hemangiomas with involvement of the chin, lips, neck, and pre-auricular areas.
Pt #10 Pt #12Pt #6
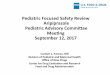
Figure 3. Representative images of upper aerodigestive tract involvement of hemangiomas in patients with hemangiomas in a beard distribution. 82% (n=9) revealed evidence of aerodigestive lesions with 64% (n=7) harboring subglottic disease (B). Lesions beyond the subglottic lumen were flat, bright red and non-obstructive (A, C, E). One patient only had lesions along the undersurface of their true vocal cords (D, arrow). Figure (E) illustrates a patient with aerodigestive hemangiomas in involution phase.
AA EEDDCCBB
Presenting Symptoms and Demographics
From years 2004-2007, eleven patients presented to the Hemangioma and Vascular Malformation Center for evaluation and management of Hemangiomas in a Beard Distribution. Presenting symptoms included stridor (n=8), ulcerations and bleeding (n=9), and aggressive proliferating hemangiomas (n=11). All patients were female and ten presented to the clinic within four months of age. One patient presented at ten years ofage with persistent head and neck disease in search of surgical management. Previous reports were sufficient to gleam infantile and medical information along with procedures previously conducted on this patient. The racial distribution of the patient population with beard hemangiomas included Caucasian (n=7, 64%), Hispanic (n=1), Asian (n=1), and Arabic (n=1). Birth and medical surveys were completed by parents prior to their first clinical visit. Gestational age was at or near term in all but one patient. Eight patients (64%) were born to mothers with 2 or more prior pregnancies. Suspicion for vascular anomalies was present in each patient within 2 weeks of birth due to head and neck areas indicating persistent vascular blush and growth. The distribution of hemangiomas for each patient is listed in Table 1. Four patients had segmental hemangiomas contiguous but extending beyond the confines of the beard distribution that included periorbital, intraorbital, chest, forehead and temporal-parietal scalp locations. Intraoral involvement was identified in 7 patients with tongue, buccal mucosal and palatal lesions.
Figure 2: Ulcers identified at the lower lip and left ear of an infant with beard distribution hemangioma. 82% of patients with these lesions had ulcers at one of these sites.
Figure 4: Patient with beard hemangioma at 6 month (A), and 27 months (B) treated with oral steroids and tailored tapering dose.
RESULTS
A multidisciplinary approach is necessary in A multidisciplinary approach is necessary in patients with segmental beard hemangiomas. patients with segmental beard hemangiomas. Formal neurological, cardiac, great vessel, Formal neurological, cardiac, great vessel, ophthalmic, and airway evaluation and ophthalmic, and airway evaluation and management should be performed due to the management should be performed due to the frequent involvement of PHACES anomalies and frequent involvement of PHACES anomalies and airway disease. Preventative and proactive airway disease. Preventative and proactive management of ear and lip ulcers are necessary in management of ear and lip ulcers are necessary in the majority of this patient population Systemic the majority of this patient population Systemic therapy with steroids and therapy with steroids and VincristineVincristine can subvert can subvert late progressive, airway and recalcitrant disease late progressive, airway and recalcitrant disease with minor risks for complication.with minor risks for complication.
1.Adams DM. The nonsurgical management of vascular lesions. Facial plastic surgery clinics of North America 2001;9:601-608.2.Chan YC. Current treatment practices in the management of cutaneoushaemangioma. Expert opinion on pharmacotherapy 2004;5:1937-1942.3.Fawcett SL, Grant I, Hall PN, Kelsall AW, Nicholson JC. Vincristine as a treatment for a large haemangioma threatening vital functions. British journal of plastic surgery 2004;57:168-171.4.Haggstrom AN, Drolet BA, Baselga Eet al. Prospective study of infantile hemangiomas: clinical characteristics predicting complications and treatment. Pediatrics 2006;118:882-887.5.Metry DW, Haggstrom AN, Drolet BAet al. A prospective study of PHACE syndrome in infantile hemangiomas: demographic features, clinical findings, and complications. American journal of medical genetics 2006;140:975-986.6.Orlow SJ, Isakoff MS, Blei F. Increased risk of symptomatic hemangiomas of the airway in association with cutaneous hemangiomas in a "beard" distribution. The Journal of pediatrics 1997;131:643-646.
RESULTS
Beard Beard HemangiomasHemangiomas
Surgical ConsultPhysical ExamSternal anomalies
Ophthalmology RxOphthalmologic ExamEye abnormalities
Cardiology EvaluationCardiac and great vessel anomalies
Surgical ConsultArtery anomalies
Ulcers and Airway obstructionMicrolaryngoscopy and Bronchoscopy
Hemangiomas (Segmental Facial)
Neurologic evaluationDevelopmental assessment
MRI/MRA-Head, neck and mediastinum
Posterior fossae malformations
ManagementManagementWorkWork--upupAcronymAcronymPHACESPHACES
MANAGEMENT ALOGRITHM
Airway DistributionAirway Distribution
UlcersUlcers
HemangiomasHemangiomas
Subglottic Subglottic lesionslesions
Supraglottic Supraglottic lesionslesions
1. Symptomatic (1. Symptomatic (Stridor/StertorStridor/Stertor))
2. Obstructing Disease2. Obstructing Disease
3. Proliferation Phase (Ave 13. Proliferation Phase (Ave 1--9 9 mosmos))
Asymptomatic (often)Asymptomatic (often)
Asymptomatic (rare)Asymptomatic (rare)
MLB MLB AirwayAirway TherapyTherapy
If Surgical interventions If Surgical interventions required for anomaliesrequired for anomalies
(ex. (ex. CoarctationCoarctation Repair, Repair, LarygotracheoplastyLarygotracheoplasty))
Wean Steroids. If Active disease then begin Wean Steroids. If Active disease then begin VincristineVincristine (0.05 mg/kg/wk)(0.05 mg/kg/wk)
EndoscopicEndoscopic
SurgicalSurgical
MedicalMedical
1. Begin with Steroids (1. Begin with Steroids (PredisosonePredisosone 22--3 mg/kg)3 mg/kg)
2. Slow tapered dose2. Slow tapered dose
3. If complications occur3. If complications occur--(HTN, (HTN, immunosuppressionimmunosuppression) then ) then begin begin VincristineVincristine (0.05mg/kg/wk) if surgery not an option(0.05mg/kg/wk) if surgery not an option
Laser Therapy (CO2 or Argon) Laser Therapy (CO2 or Argon) and and IntubateIntubate 22--3 day Vs.3 day Vs.
Steroid Injection (Steroid Injection (kenalogkenalog) and ) and IntubateIntubate 22--3 3 daysVsdaysVs..
Combined ApproachCombined Approach
Follow symptoms Repeat MLB Follow symptoms Repeat MLB prnprn
Follow symptoms Repeat MLB Follow symptoms Repeat MLB prnprn
Open ApproachOpen ApproachTracheostomy vs.Tracheostomy vs.
SubmucosalSubmucosal Resection Alone vs.Resection Alone vs.
LaryngotrachealLaryngotracheal Reconstruction Reconstruction with with SubmucosalSubmucosal ResectionResection
1. Rapidly proliferating with deformity1. Rapidly proliferating with deformity
2. Ulcerations2. Ulcerations
3. Symptomatic Airway Disease3. Symptomatic Airway Disease
AnomaliesAnomalies
1. Begin Steroids (1. Begin Steroids (PredisosonePredisosone 22--3 mg/kg)3 mg/kg)
2. Slow tapered dose adjusted to disease 2. Slow tapered dose adjusted to disease response during response during proliferativeproliferative phasephase
Preventative management of common sites Preventative management of common sites (ear and lower lip) with (ear and lower lip) with AquaforAquafor BID BID UlcersUlcers——bactroban/bacitracin/aquaforbactroban/bacitracin/aquafor
FPDL to promote FPDL to promote epithelializaionepithelializaion
Bimonthly evaluationBimonthly evaluation--PEPE
Wean steroids (0.2Wean steroids (0.2--0.3 ml weekly) If 0.3 ml weekly) If responsive (graying overlying skin) responsive (graying overlying skin) then Maintain dosethen Maintain dose
Steroid Complications:HTN, Growth disturbance, FTT, Immunosuppression, Cushingoid, Irritability
(N=10) 91%(N=10) 91%
(N=6) 55%(N=6) 55%
(N=9) 82%(N=9) 82%
(N=9) 82%(N=9) 82%
(N=7) 64%(N=7) 64%
1. Wean Steroids (weekly 1. Wean Steroids (weekly evaleval))
2. Begin 2. Begin VincristineVincristine (0.05mg/kg/wk) (0.05mg/kg/wk) (N=5, 45%)(N=5, 45%)
3. Wean 3. Wean VincristineVincristine to Hemangioma responseto Hemangioma responseTherapyTherapy
N=number in N=number in our seriesour series
AA BB
Surgical ManagementSurgical ManagementDuring InvolutionDuring InvolutionFPDLFPDL--Red Red MaculesMaculesExcision Bulky LesionsExcision Bulky Lesions