Embed Size (px)
Citation preview
Management of perioperative frailty
Dr K TealeConsultant anaesthetist
Clinical Lead PreopSRFT
What is frailty?
Common issues
• Complex patients being listed for surgery based on an X-Ray review or investigation
• No shared decision making
• Failure to assess for markers of frailty
• Failure to identify, counsel or plan for predictable complications- AKI, cardiorespiratory issues, delirium
• Referral tennis
Definition of frailty
• “Decreased physiological reserve across multiple organ systems leading to increased vulnerability to seemingly minor external stressors.”
Eg UTI, URTI, minor surgery, new medication
Not all old people are frail, but most frail people are old
Why is it important?
• High Frailty score predictably associated with adverse outcomes
• Frailty can be modified if recognised
CEPOD 2010 “An age old problem”
• “….comorbidity, disability and frailtyneed to be clearly recognized as independent markers of risk in the elderly. This requires skill & multidisciplinary input including early involvement of Medicine for the Elderly”.
• BGS recommends all encounters between health staff and older people should include assessment for frailty.
Have we made progress
• 2014 survey of 160 acute trusts – 12% had formal arrangements for geriatric review preop, and 20% postop
• NELA – 14% of trusts had preoperative geriatric review
• How do we recognise it?
• What can we do about it?
frailty• may present acutely eg falls/delirium/sudden
immobility
• May not always be recognised if not actively sought
• Requires a different approach from organ-specific disease
• We may not be as familiar with how to get help or advice about frailty
BGS – recognising frailty
• Gait speed - >5 seconds to walk 4 meters
• TUGT – 10s to stand, walk 3 meters, turn and sit
• PRISMA 7 - >85• Male
• Health problems limiting activity
• Need someone to help regularly
• Health problems meaning stay at home
• Can you count on someone close to help
• Regularly use stick or walking aid to get about
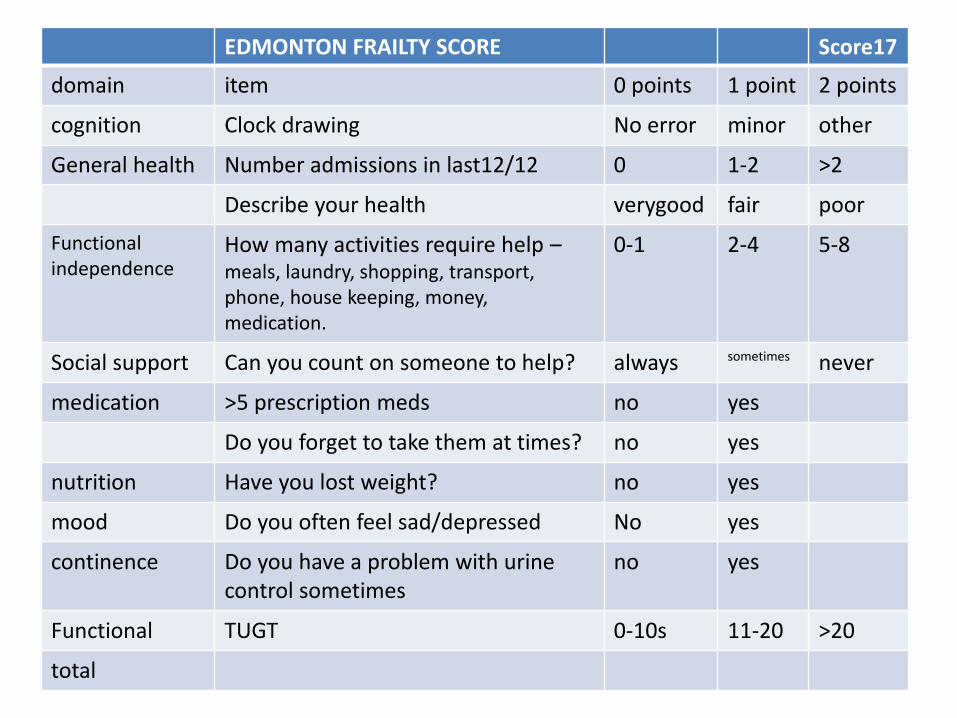
Edmonton frailty scoreEDMONTON FRAILTY SCORE Score17
domain item 0 points 1 point 2 points
cognition Clock drawing No error minor other
General health Number admissions in last12/12 0 1-2 >2
Describe your health verygood fair poor
Functional independence
How many activities require help –meals, laundry, shopping, transport, phone, house keeping, money, medication.
0-1 2-4 5-8
Social support Can you count on someone to help? always sometimes never
medication >5 prescription meds no yes
Do you forget to take them at times? no yes
nutrition Have you lost weight? no yes
mood Do you often feel sad/depressed No yes
continence Do you have a problem with urine control sometimes
no yes
Functional TUGT 0-10s 11-20 >20
total
Management in the community
• No evidence that routine population screening improves health outcomes
• All frail patients should be holistically reviewed in primary care – Comprehensive Geriatric Assessment
• Treat medical conditions
• Personalised care and support plan
• Consider referral – COTE, psychiatry
• Regular medication review
Perioperative management – LOOK FOR IT
• Surgical patients – up to 40-50%
• In Community – 8.5% women, 4.1% men
• Care home residents
– 400,000 care home residents in UK
– “majority” deemed to be frail
Current pathways…
• Preop service concentrates on “single organ” referrals
• Often binary “fit or unfit” outcome
• GP/specialist physicians not always aware of research on periop risk
• Delays, sometimes exclusion from surgery
• POPS model
• Proactive referral – clear referral criteria
• Clinic MDT – interventions – geriatrician, anaesthetist, surgeon,OT, physio, SW, sec
• Hospital admission – postop COTE input, discharge planning
• Post-discharge – links with primary care, intermediate care, specialist clinic FU
POPS referral
• AGE > 65 (flexible) with one or more– Dementia/cognitive impairment
– 2 or more uncontrolled comorbidities
– Functional dependence
– > 6 prescription medications
– Multiple hospital admissions 12/12 12/12in in last 12/12
– Concerns about low BMI
– Poor exercise tolerance
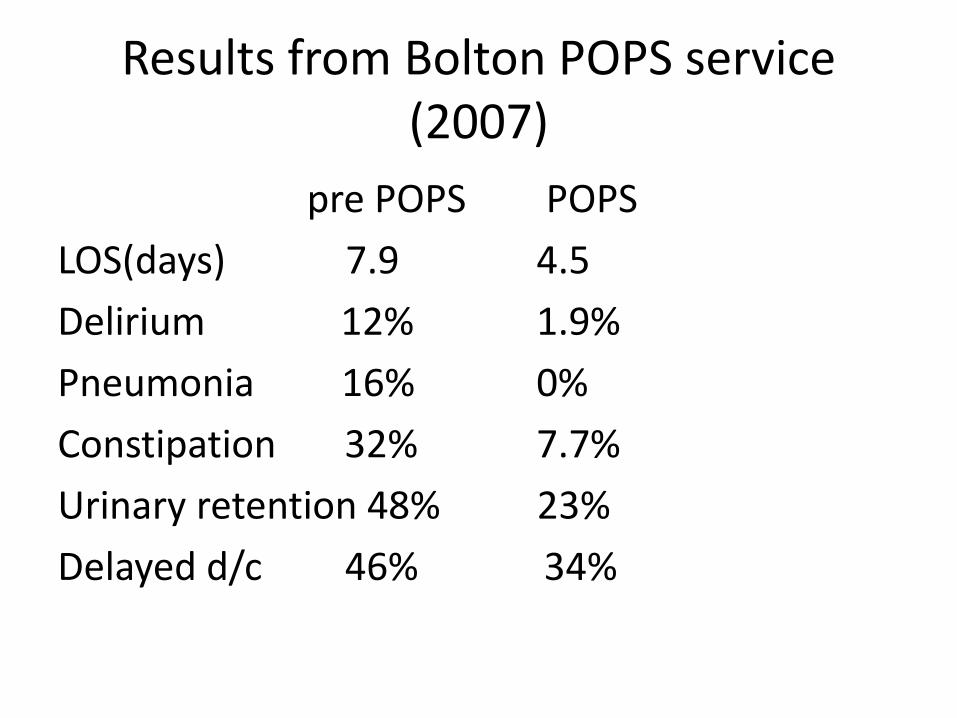
Results from Bolton POPS service (2007)
pre POPS POPS
LOS(days) 7.9 4.5
Delirium 12% 1.9%
Pneumonia 16% 0%
Constipation 32% 7.7%
Urinary retention 48% 23%
Delayed d/c 46% 34%
“A multifactorial interdisciplinary intervention reduces frailty in older people” BMC medicine, 2013, 11;65 Cameron et al
• Weight loss – dietician, meal provision
• Low activity levels – physiotherapy
• Social isolation – community engagement
• Chronic disease management and regular review
• All takes time

In hospital
• Early mobilisation
• Nutritional assistance
• Orientating communication
• Regular detailed review including medication
Case study
• 83 year old lady, retired office worker
• Idiopathic Parkinson’s Disease
– Levodopa QDS, Rivastigmine patch
• Dementia syndrome
– Visual and musical hallucinations
• Severe OA both knees
• Hypertension
Background
• Hallucinations much better since rivastigminepatch started
• Increased falls with knee giving way
• Very keen for surgery to help pain and mobility
Social Background
• Lives alone in a bungalow
• Carers QDS and “Care On Call”
• Adapted shower room
• Assistance with all ADL’s
• Occasional urinary incontinence
• Mobile short distances with zimmer frame
• Friend Terry, personal carer
Medications
Losartan 25mg OD
Rivastigmine patch 9.5mg/24 hours
Co-careldopa 250mg MR QDS (8, 13, 18, 22)
Amlodipine 5mg OD
Adcal D3 BD
Paracetamol
Codeine phosphate
Assessment
• ACE-R 72/100
• EFS 13/17 (Severe frailty syndrome)
• BMI 21.6
• Bloods unremarkable
• Normal spirometry
• CT Brain- old occipital infarcts
Outcome
• Spinal anaesthesia with aim of not interfering with oral levodopa
• Proactive management of constipation
• Counselling regarding delirium risk and delirium measures
• Joint preoperative plan with Parkinson’s team
• Suspension of antihypertensives
Post-operative period
• Mild postoperative delirium
• AKI avoided
• Pain an issue initially but optimised
• Discharged home with care package
• Seen in clinic- mood much improved, mobility better
• Very pleased with outcome from surgery, wants 2nd knee doing
conclusion
• Frailty syndrome is a distinct entity and a clear predictor of complications
• Frailty is often not recognised
• It should be specifically looked for at preop
• Frailty can be modified by appropriate preoperative multidisciplinary interventions





























