Embed Size (px)
Citation preview
Management of side effects
Rafael Esteban Liver Unit.
Hospital General Universitari Vall Hebron. Barcelona.
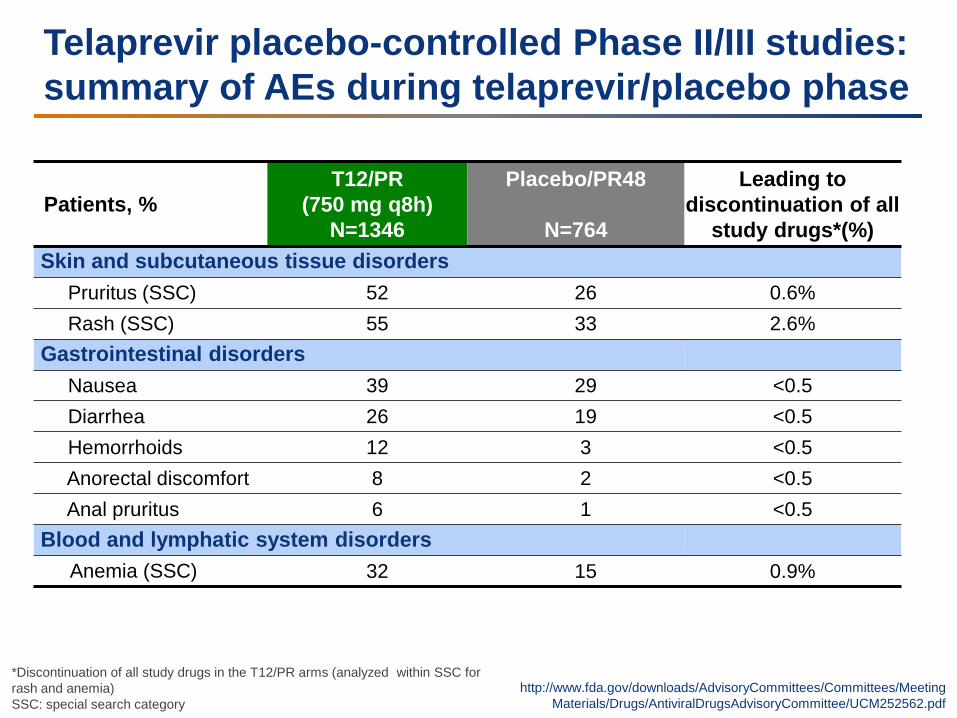
Telaprevir placebo-controlled Phase II/III studies: summary of AEs during telaprevir/placebo phase
Patients, % T12/PR
(750 mg q8h) N=1346
Placebo/PR48
N=764
Leading to discontinuation of all
study drugs*(%) Skin and subcutaneous tissue disorders Pruritus (SSC) 52 26 0.6% Rash (SSC) 55 33 2.6% Gastrointestinal disorders Nausea 39 29 <0.5 Diarrhea 26 19 <0.5 Hemorrhoids 12 3 <0.5 Anorectal discomfort 8 2 <0.5 Anal pruritus 6 1 <0.5 Blood and lymphatic system disorders Anemia (SSC) 32 15 0.9%
http://www.fda.gov/downloads/AdvisoryCommittees/Committees/Meeting Materials/Drugs/AntiviralDrugsAdvisoryCommittee/UCM252562.pdf
*Discontinuation of all study drugs in the T12/PR arms (analyzed within SSC for rash and anemia) SSC: special search category
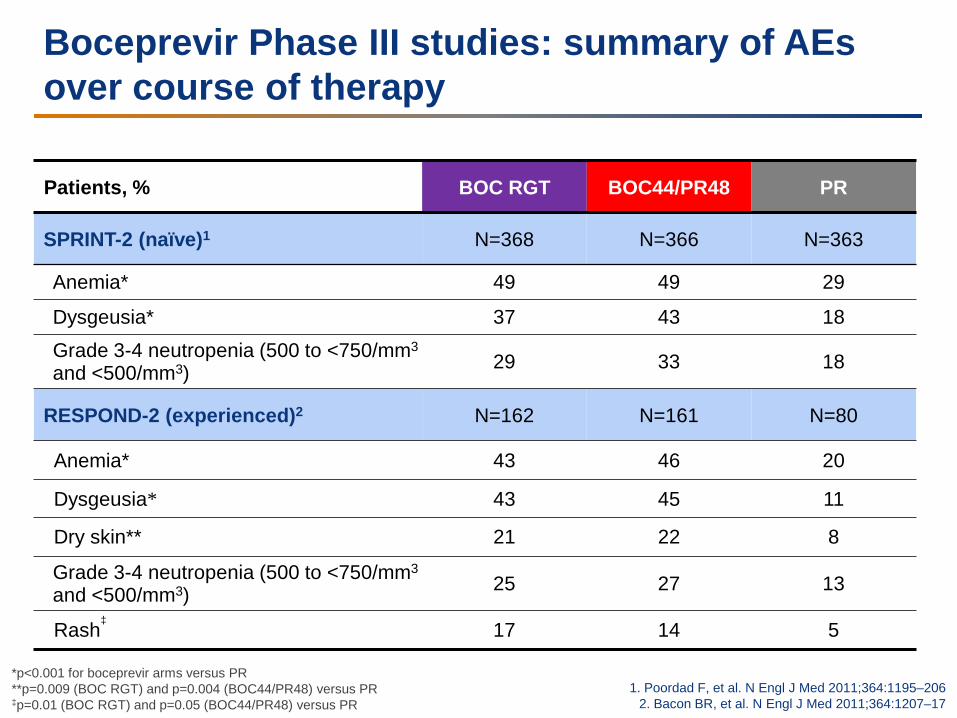
Boceprevir Phase III studies: summary of AEs over course of therapy
Patients, % BOC RGT BOC44/PR48 PR
SPRINT-2 (naïve)1 N=368 N=366 N=363
Anemia* 49 49 29
Dysgeusia* 37 43 18
Grade 3-4 neutropenia (500 to <750/mm3
and <500/mm3) 29 33 18
RESPOND-2 (experienced)2 N=162 N=161 N=80
Anemia* 43 46 20
Dysgeusia* 43 45 11
Dry skin** 21 22 8
Grade 3-4 neutropenia (500 to <750/mm3
and <500/mm3) 25 27 13
Rash‡ 17 14 5
1. Poordad F, et al. N Engl J Med 2011;364:1195–206 2. Bacon BR, et al. N Engl J Med 2011;364:1207–17
*p<0.001 for boceprevir arms versus PR **p=0.009 (BOC RGT) and p=0.004 (BOC44/PR48) versus PR ‡p=0.01 (BOC RGT) and p=0.05 (BOC44/PR48) versus PR
Specific AEs with DAAs: anemia
Telaprevir EU SmPC
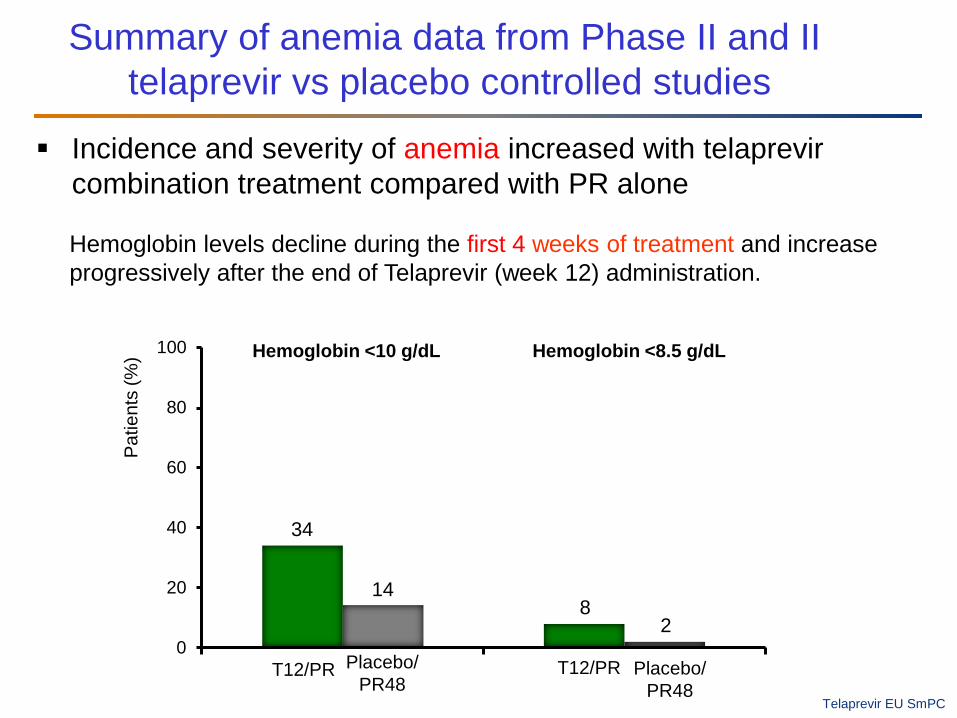
Incidence and severity of anemia increased with telaprevir combination treatment compared with PR alone
34
814
20
20
40
60
80
100
T12/PR Placebo/ PR48
T12/PR Placebo/ PR48
Hemoglobin <10 g/dL Hemoglobin <8.5 g/dL
Pat
ient
s (%
)
Hemoglobin levels decline during the first 4 weeks of treatment and increase progressively after the end of Telaprevir (week 12) administration.
Summary of anemia data from Phase II and II telaprevir vs placebo controlled studies
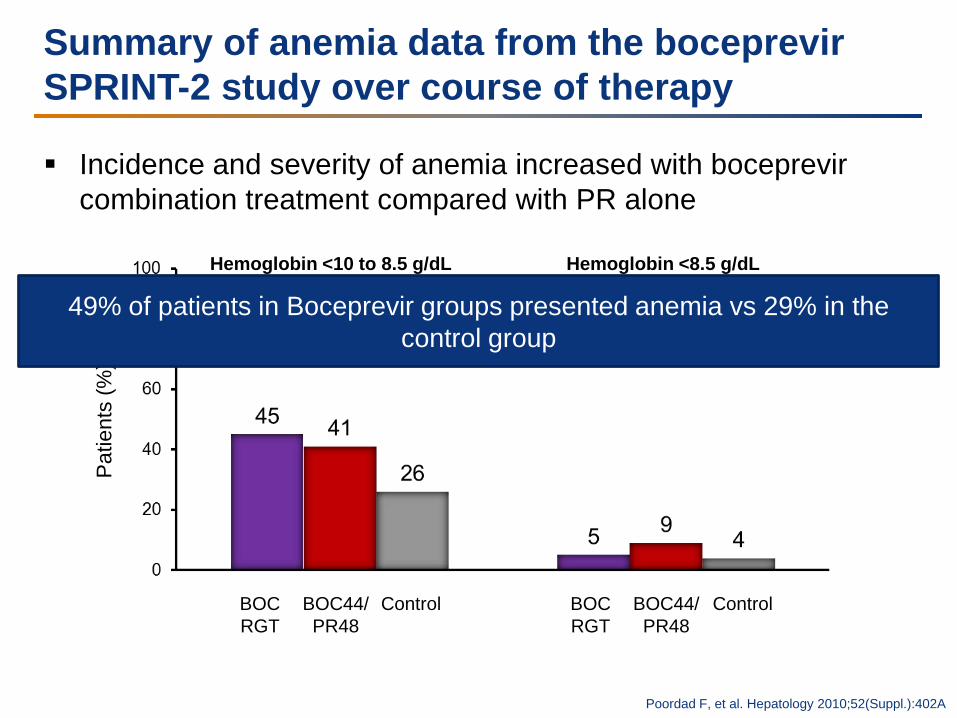
Summary of anemia data from the boceprevir SPRINT-2 study over course of therapy
Incidence and severity of anemia increased with boceprevir combination treatment compared with PR alone
BOC RGT
Control
Hemoglobin <10 to 8.5 g/dL Hemoglobin <8.5 g/dL
Pat
ient
s (%
)
BOC44/ PR48
BOC RGT
Control BOC44/ PR48
Poordad F, et al. Hepatology 2010;52(Suppl.):402A
49% of patients in Boceprevir groups presented anemia vs 29% in the control group
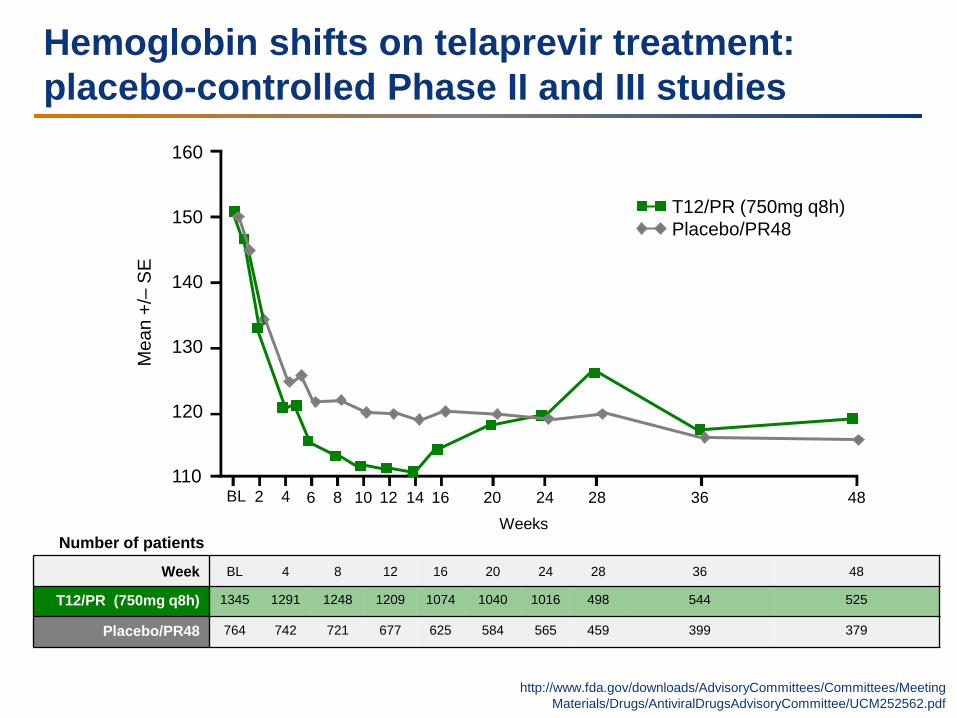
Hemoglobin shifts on telaprevir treatment: placebo-controlled Phase II and III studies
http://www.fda.gov/downloads/AdvisoryCommittees/Committees/Meeting Materials/Drugs/AntiviralDrugsAdvisoryCommittee/UCM252562.pdf
Number of patients
Week BL 4 8 12 16 20 24 28 36 48
T12/PR (750mg q8h) 1345 1291 1248 1209 1074 1040 1016 498 544 525
Placebo/PR48 764 742 721 677 625 584 565 459 399 379
160
150
140
130
120
110
Mea
n +/
– S
E
T12/PR (750mg q8h) Placebo/PR48
2 4 6 8 10 12 14 16 20 24 28 36 48 BL
Weeks
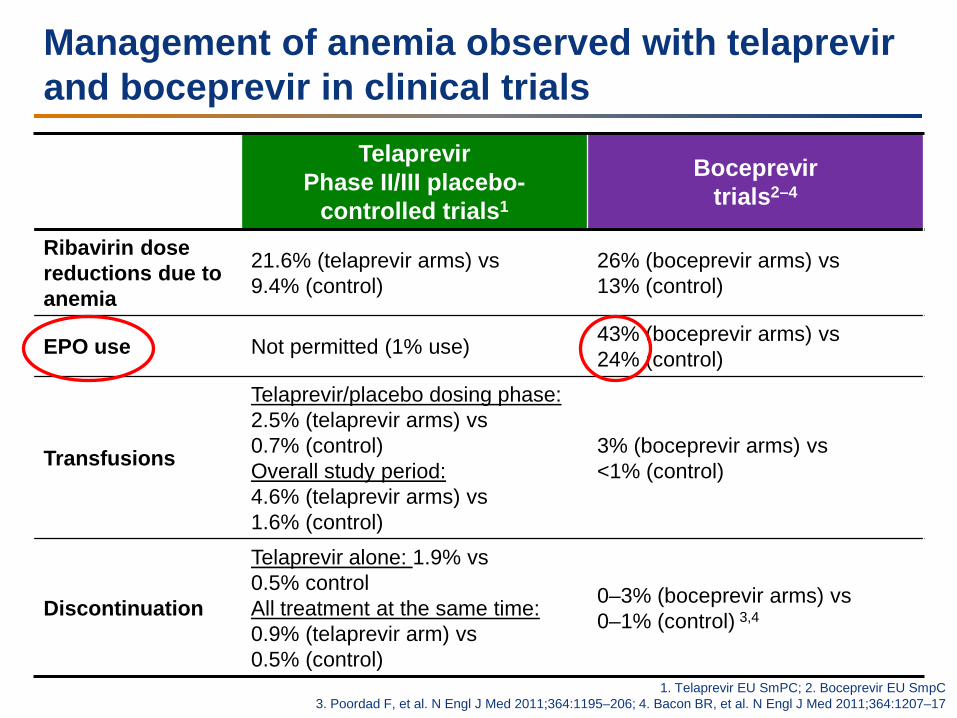
Management of anemia observed with telaprevir and boceprevir in clinical trials
Telaprevir Phase II/III placebo-
controlled trials1
Boceprevir trials2–4
Ribavirin dose reductions due to anemia
21.6% (telaprevir arms) vs 9.4% (control)
26% (boceprevir arms) vs 13% (control)
EPO use Not permitted (1% use) 43% (boceprevir arms) vs 24% (control)
Transfusions
Telaprevir/placebo dosing phase: 2.5% (telaprevir arms) vs 0.7% (control) Overall study period: 4.6% (telaprevir arms) vs 1.6% (control)
3% (boceprevir arms) vs <1% (control)
Discontinuation
Telaprevir alone: 1.9% vs 0.5% control All treatment at the same time: 0.9% (telaprevir arm) vs 0.5% (control)
0–3% (boceprevir arms) vs 0–1% (control) 3,4
1. Telaprevir EU SmPC; 2. Boceprevir EU SmpC 3. Poordad F, et al. N Engl J Med 2011;364:1195–206; 4. Bacon BR, et al. N Engl J Med 2011;364:1207–17
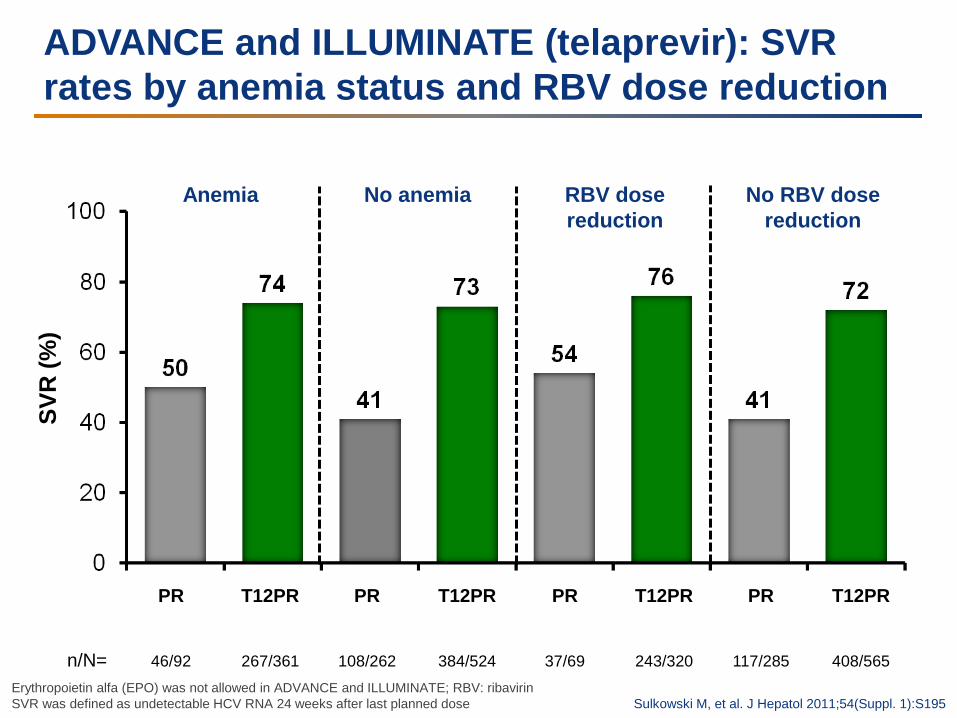
ADVANCE and ILLUMINATE (telaprevir): SVR rates by anemia status and RBV dose reduction
SVR
(%)
n/N=
T12PR
267/361
PR
46/92
Anemia
PR
108/262
T12PR
384/524
No anemia
Sulkowski M, et al. J Hepatol 2011;54(Suppl. 1):S195
T12PR
243/320
PR
37/69
PR
117/285
T12PR
408/565
RBV dose reduction
No RBV dose reduction
Erythropoietin alfa (EPO) was not allowed in ADVANCE and ILLUMINATE; RBV: ribavirin SVR was defined as undetectable HCV RNA 24 weeks after last planned dose
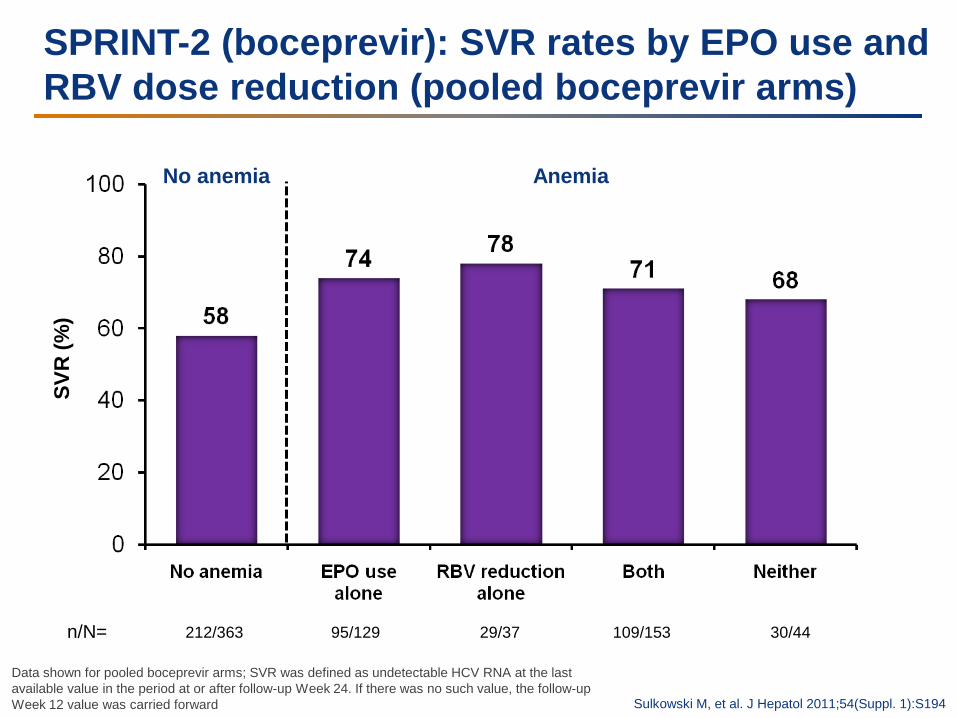
95/129
SPRINT-2 (boceprevir): SVR rates by EPO use and RBV dose reduction (pooled boceprevir arms)
Sulkowski M, et al. J Hepatol 2011;54(Suppl. 1):S194
SVR
(%)
No anemia Anemia
212/363
29/37
109/153
30/44 n/N=
Data shown for pooled boceprevir arms; SVR was defined as undetectable HCV RNA at the last available value in the period at or after follow-up Week 24. If there was no such value, the follow-up Week 12 value was carried forward
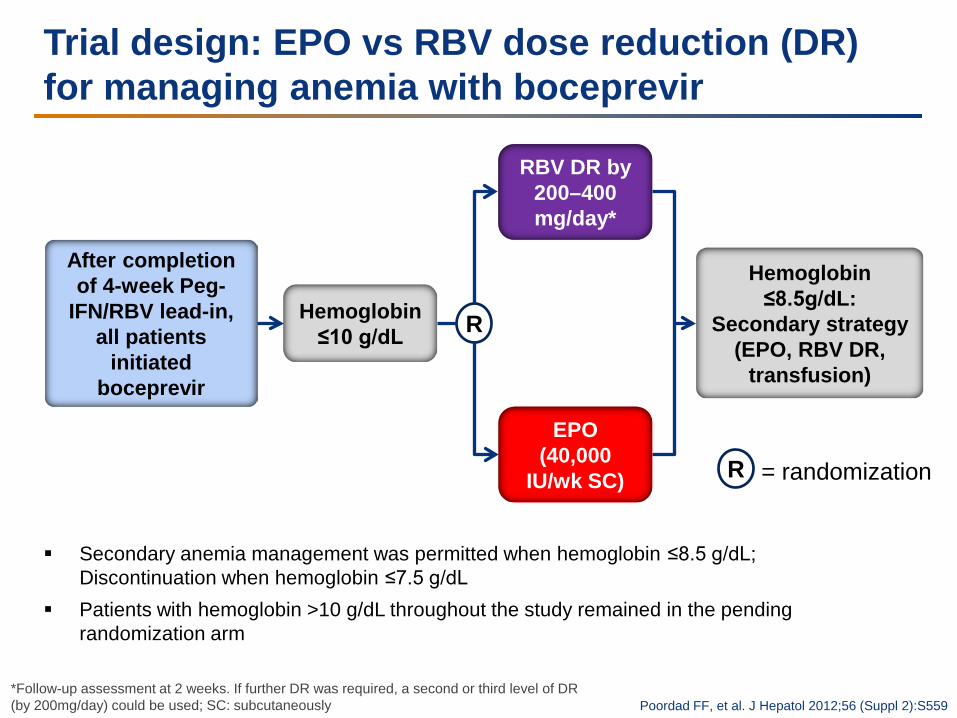
Trial design: EPO vs RBV dose reduction (DR) for managing anemia with boceprevir
After completion of 4-week Peg-
IFN/RBV lead-in, all patients
initiated boceprevir
Hemoglobin ≤10 g/dL
RBV DR by 200–400 mg/day*
EPO (40,000
IU/wk SC)
Hemoglobin ≤8.5g/dL:
Secondary strategy (EPO, RBV DR,
transfusion)
R
R = randomization
*Follow-up assessment at 2 weeks. If further DR was required, a second or third level of DR (by 200mg/day) could be used; SC: subcutaneously Poordad FF, et al. J Hepatol 2012;56 (Suppl 2):S559
Secondary anemia management was permitted when hemoglobin ≤8.5 g/dL; Discontinuation when hemoglobin ≤7.5 g/dL
Patients with hemoglobin >10 g/dL throughout the study remained in the pending randomization arm
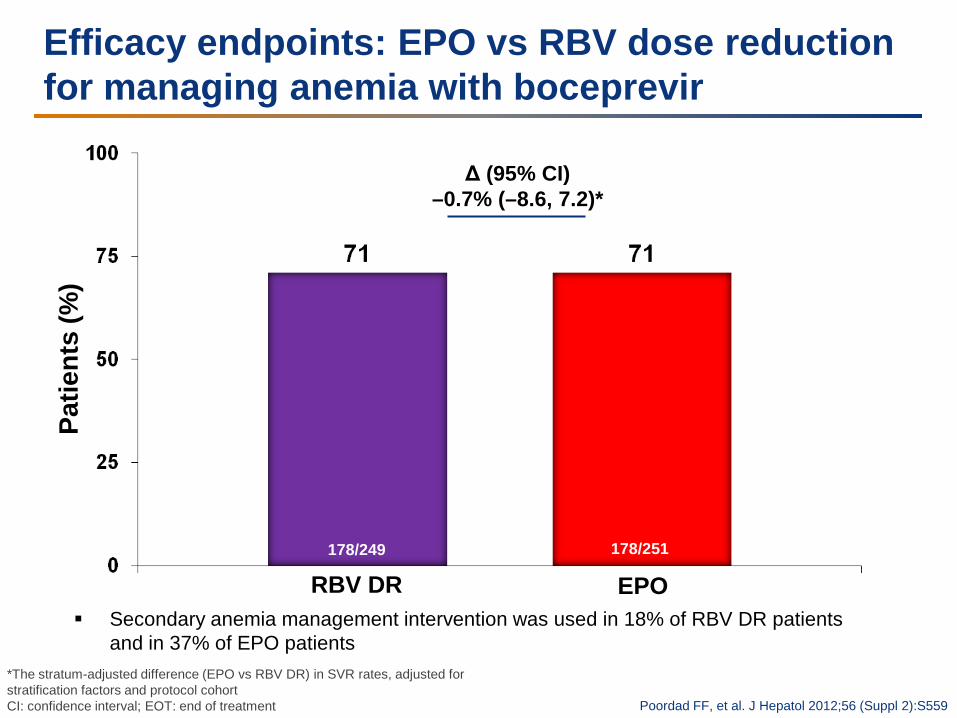
Efficacy endpoints: EPO vs RBV dose reduction for managing anemia with boceprevir
*The stratum-adjusted difference (EPO vs RBV DR) in SVR rates, adjusted for stratification factors and protocol cohort CI: confidence interval; EOT: end of treatment
Patie
nts
(%)
Δ (95% CI) –0.7% (–8.6, 7.2)*
178/249 178/251
Poordad FF, et al. J Hepatol 2012;56 (Suppl 2):S559
RBV DR EPO Secondary anemia management intervention was used in 18% of RBV DR patients
and in 37% of EPO patients
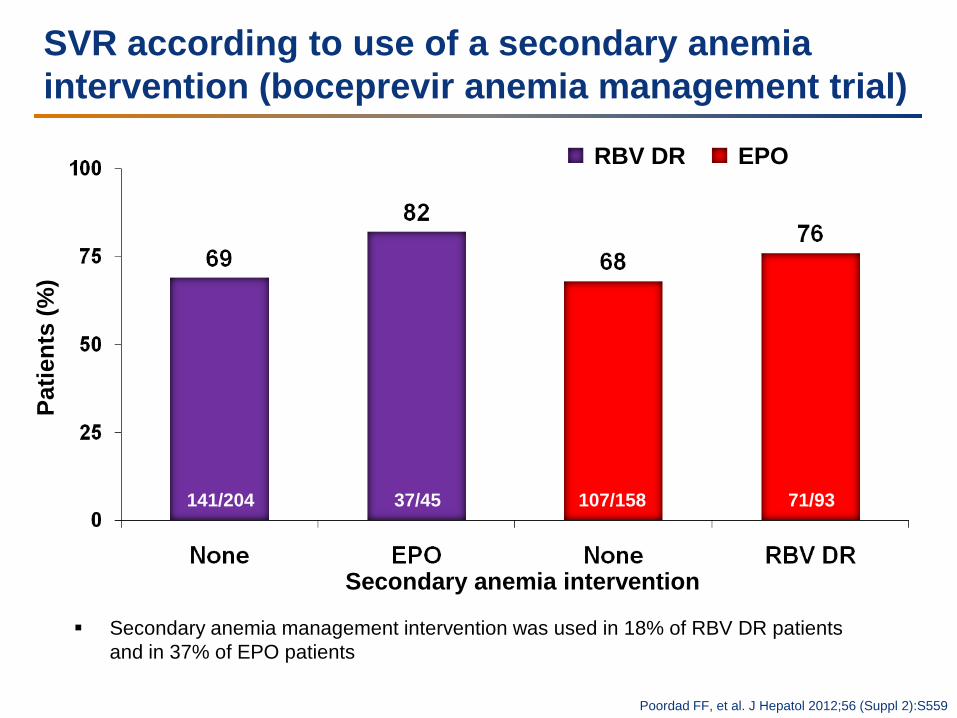
SVR according to use of a secondary anemia intervention (boceprevir anemia management trial)
Patie
nts
(%)
Secondary anemia intervention
141/204 37/45 107/158 71/93
Poordad FF, et al. J Hepatol 2012;56 (Suppl 2):S559
RBV DR EPO
Secondary anemia management intervention was used in 18% of RBV DR patients and in 37% of EPO patients
Specific adverse events with DAAs: rash
Optimal management
of dermatological reactions
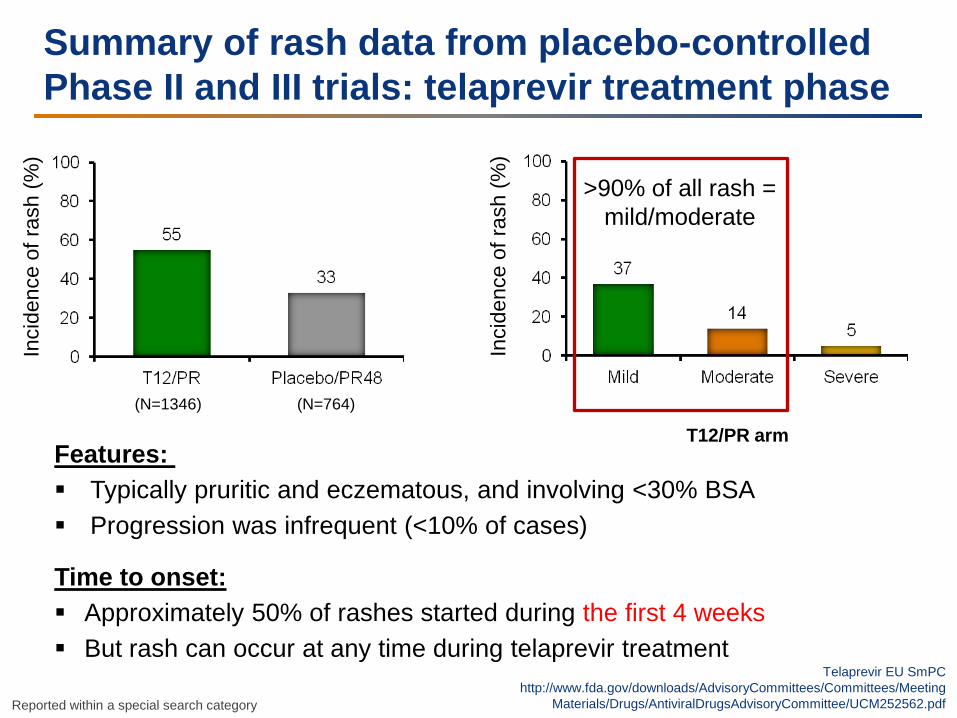
Summary of rash data from placebo-controlled Phase II and III trials: telaprevir treatment phase
>90% of all rash = mild/moderate
Inci
denc
e of
rash
(%)
Features: Typically pruritic and eczematous, and involving <30% BSA Progression was infrequent (<10% of cases)
Time to onset: Approximately 50% of rashes started during the first 4 weeks But rash can occur at any time during telaprevir treatment
Inci
denc
e of
rash
(%)
Telaprevir EU SmPC http://www.fda.gov/downloads/AdvisoryCommittees/Committees/Meeting
Materials/Drugs/AntiviralDrugsAdvisoryCommittee/UCM252562.pdf
(N=1346) (N=764)
Reported within a special search category
T12/PR arm
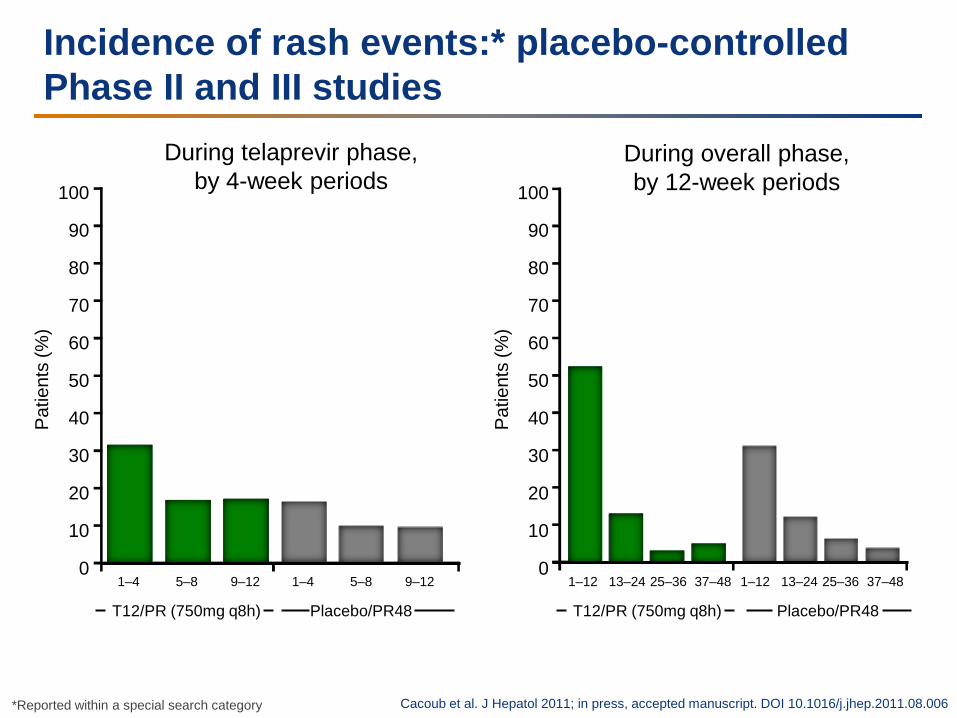
Incidence of rash events:* placebo-controlled Phase II and III studies
During telaprevir phase, by 4-week periods
During overall phase, by 12-week periods 100
90
80
70
60
50
40
30
20
10
0
100
90
80
70
60
50
40
30
20
10
0
Pat
ient
s (%
)
Pat
ient
s (%
)
1–4 5–8 9–12
T12/PR (750mg q8h)
1–4 5–8 9–12
Placebo/PR48
1–12 13–24 25–36
T12/PR (750mg q8h)
37–48
Placebo/PR48
1–12 13–24 25–36 37–48
Cacoub et al. J Hepatol 2011; in press, accepted manuscript. DOI 10.1016/j.jhep.2011.08.006 *Reported within a special search category
Grading of skin eruption severity
Mild: localized skin eruption and/or a skin eruption with limited distribution (up to several isolated sites on the body)
Moderate: diffuse rash involving ≤50% of body surface area
Severe: extent of rash >50% of body surface area or associated with significant systemic symptoms, mucous membrane ulceration, target lesions, epidermal detachment
SCAR: Collective term for severe drug-related skin conditions that can be associated with significant morbidity
SCAR: Severe Cutaneous Adverse Reaction Telaprevir EU SmPC
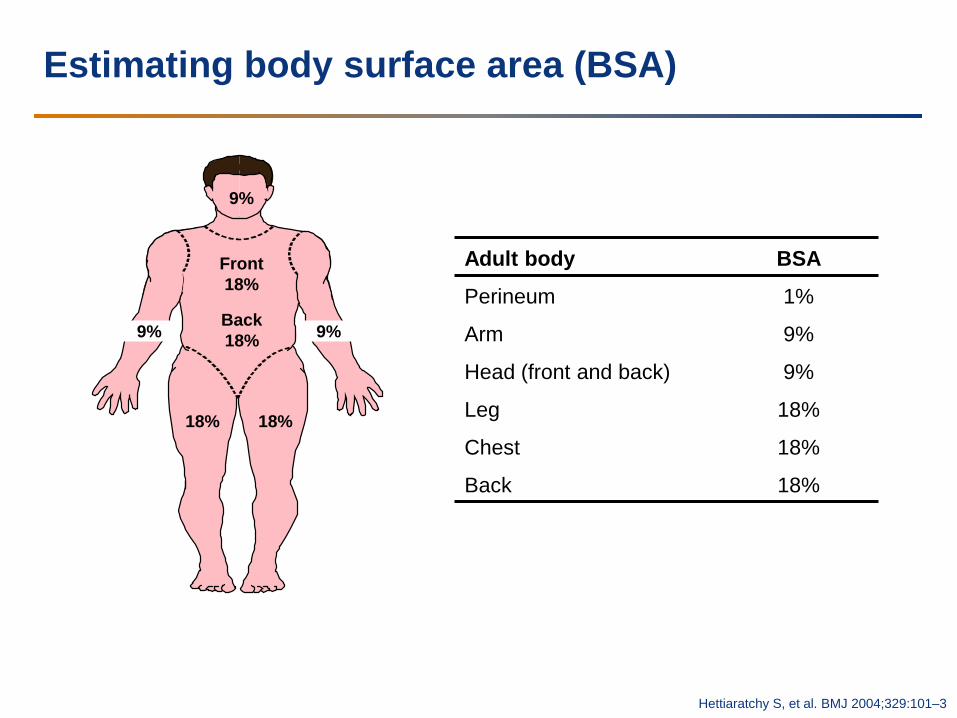
Estimating body surface area (BSA)
9%
9%
Front 18%
Back 18% 9%
18% 18%
Hettiaratchy S, et al. BMJ 2004;329:101–3
Adult body BSA
Perineum 1%
Arm 9%
Head (front and back) 9%
Leg 18%
Chest 18%
Back 18%
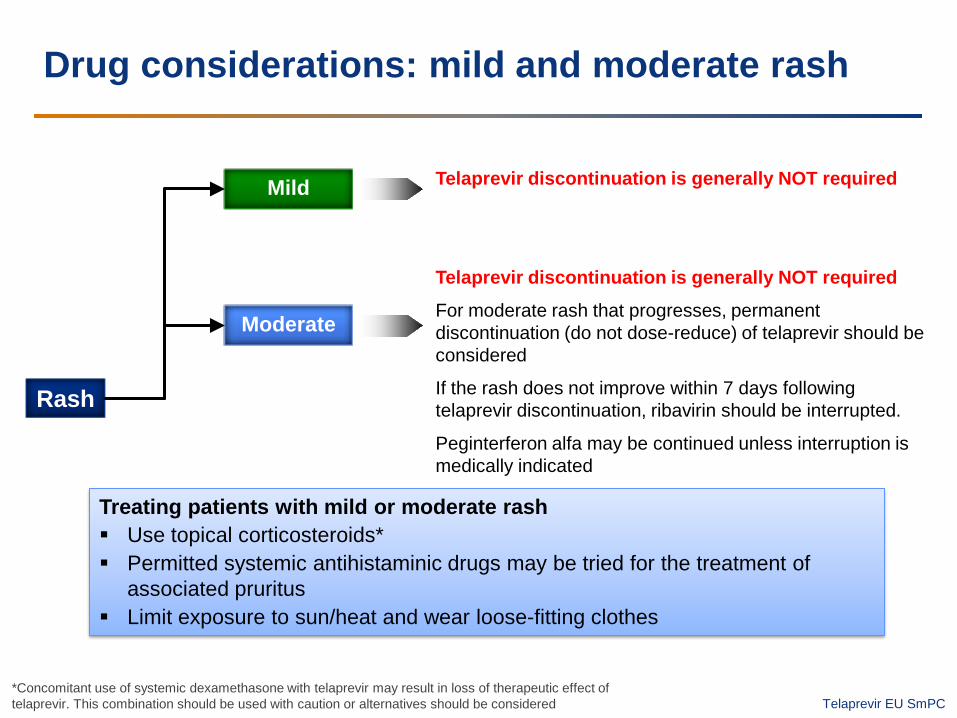
Drug considerations: mild and moderate rash
Treating patients with mild or moderate rash Use topical corticosteroids* Permitted systemic antihistaminic drugs may be tried for the treatment of
associated pruritus Limit exposure to sun/heat and wear loose-fitting clothes
Rash
Mild
Moderate
Telaprevir discontinuation is generally NOT required
Telaprevir discontinuation is generally NOT required
For moderate rash that progresses, permanent discontinuation (do not dose-reduce) of telaprevir should be considered
If the rash does not improve within 7 days following telaprevir discontinuation, ribavirin should be interrupted.
Peginterferon alfa may be continued unless interruption is medically indicated
*Concomitant use of systemic dexamethasone with telaprevir may result in loss of therapeutic effect of telaprevir. This combination should be used with caution or alternatives should be considered Telaprevir EU SmPC

Mild rush (Grade 1 Dermatitis)
Mild rash is defined as localized skin eruption and/or a skin eruption with limited distribution (up to several isolated sites on the body)
Cacoub, P., Bourlière, M., Lübbe, J., Dupin, N., Buggisch, P., Dusheiko, G., Hézode, C.,Picard, O., Pujol, R., Segaert, S., Thio, B., Roujeau, J-C., Dermatological side effects of hepatitis c and its treatment: Patient management in the era of direct-acting antivirals, Journal of Hepatology (2011), doi: 10.1016/j.jhep. 2011.08.006. Grade 1 dermatitis,
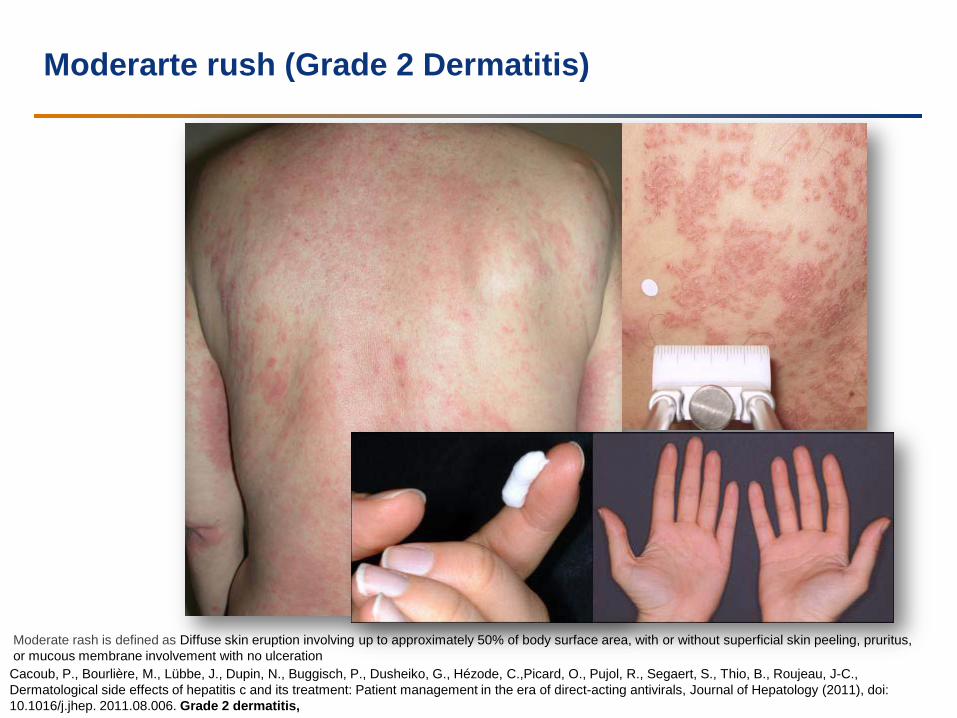
Moderarte rush (Grade 2 Dermatitis)
Cacoub, P., Bourlière, M., Lübbe, J., Dupin, N., Buggisch, P., Dusheiko, G., Hézode, C.,Picard, O., Pujol, R., Segaert, S., Thio, B., Roujeau, J-C., Dermatological side effects of hepatitis c and its treatment: Patient management in the era of direct-acting antivirals, Journal of Hepatology (2011), doi: 10.1016/j.jhep. 2011.08.006. Grade 2 dermatitis,
Moderate rash is defined as Diffuse skin eruption involving up to approximately 50% of body surface area, with or without superficial skin peeling, pruritus, or mucous membrane involvement with no ulceration
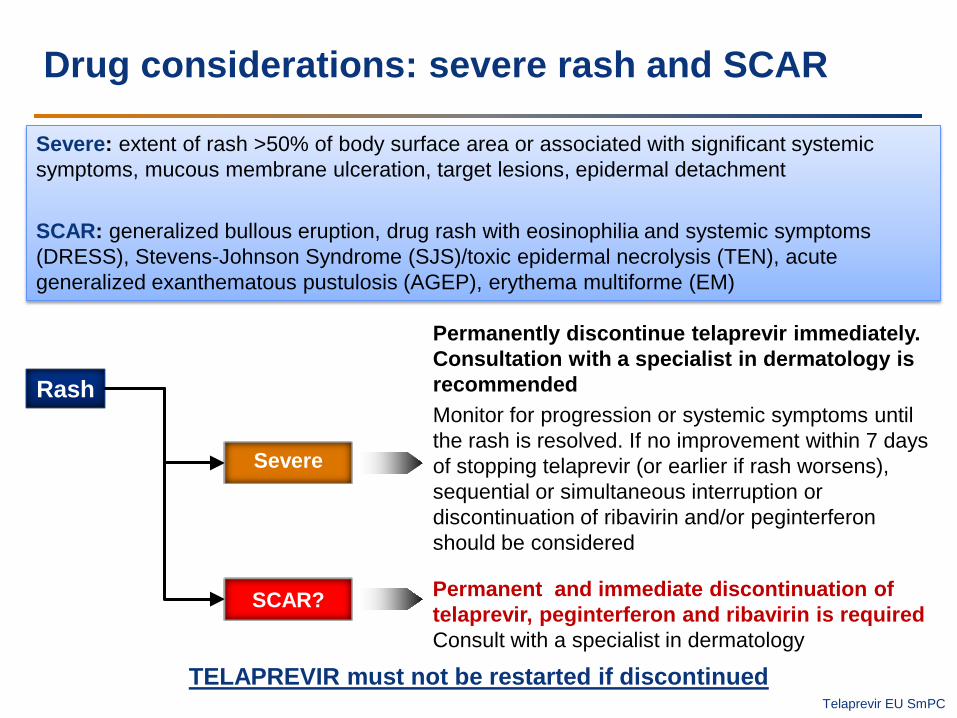
Drug considerations: severe rash and SCAR
Severe: extent of rash >50% of body surface area or associated with significant systemic symptoms, mucous membrane ulceration, target lesions, epidermal detachment SCAR: generalized bullous eruption, drug rash with eosinophilia and systemic symptoms (DRESS), Stevens-Johnson Syndrome (SJS)/toxic epidermal necrolysis (TEN), acute generalized exanthematous pustulosis (AGEP), erythema multiforme (EM)
TELAPREVIR must not be restarted if discontinued
Rash
Severe
SCAR?
Permanently discontinue telaprevir immediately. Consultation with a specialist in dermatology is recommended Monitor for progression or systemic symptoms until the rash is resolved. If no improvement within 7 days of stopping telaprevir (or earlier if rash worsens), sequential or simultaneous interruption or discontinuation of ribavirin and/or peginterferon should be considered
Permanent and immediate discontinuation of telaprevir, peginterferon and ribavirin is required Consult with a specialist in dermatology
Telaprevir EU SmPC
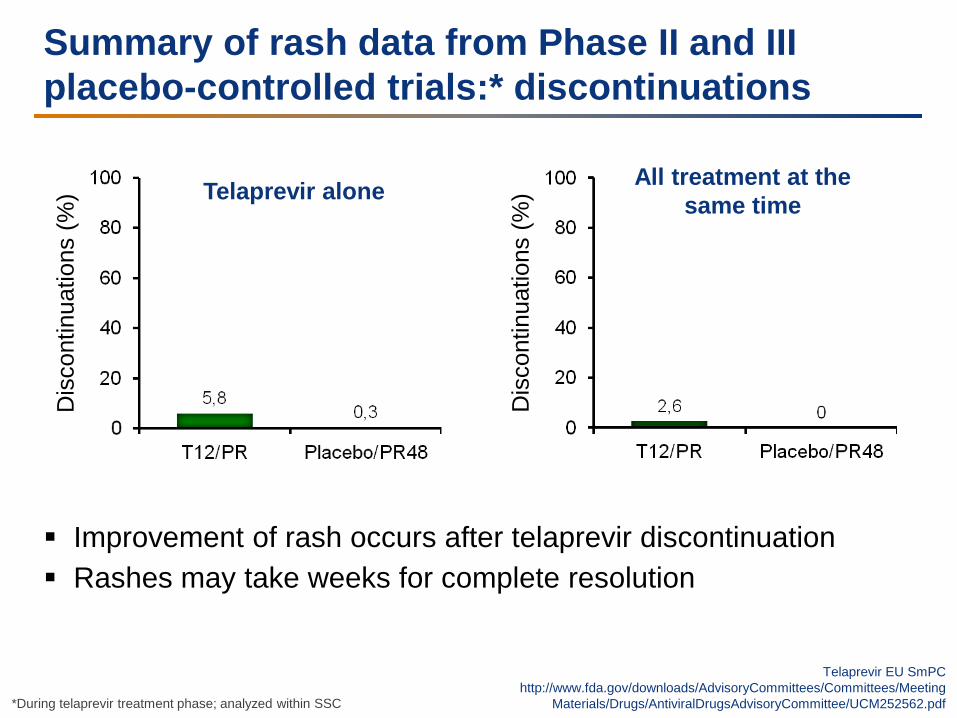
Summary of rash data from Phase II and III placebo-controlled trials:* discontinuations
*During telaprevir treatment phase; analyzed within SSC
Improvement of rash occurs after telaprevir discontinuation Rashes may take weeks for complete resolution
Dis
cont
inua
tions
(%)
Dis
cont
inua
tions
(%) Telaprevir alone All treatment at the
same time
Telaprevir EU SmPC http://www.fda.gov/downloads/AdvisoryCommittees/Committees/Meeting
Materials/Drugs/AntiviralDrugsAdvisoryCommittee/UCM252562.pdf
Dermatological side effects of hepatitis C and its treatment: Patient management in the era of direct-acting antivirals
Patrice Cacoub et al. J Hepatol 2012
Proper skin care: - at least 15 min and should become a daily habit in order to become effective. - after a shower/bath - Emollient creams and lipid-rich lotions, rather than aqueous lotions or ointments, are effective and well-accepted by patients and should be prescribed as prophylactic baseline skin treatment If grade 1-2 dermatitis: - potent topical corticosteroids can be used (hands, feet, skin around the large joints, large skin surfaces)
Anorectal Symptoms
In telaprevir trials: – 29% of patients receiving triple therapy vs 7% of patients receiving
standard therapy
Most of these adverse events: - hemorrhoids, anorectal discomfort, anal pruritus, rectal burning However, most of them were mild to moderate, and < 1% resulted in
treatment discontinuation
Management: short-term topical corticosteroids, topical lidocaine-type agents, antihistamines before bedtime, and trying to control bowel movements with loperamide or diphenoxylate
and atropine.
is not believed to be related to levels of telaprevir, and the cause remains enigmatic
Summary and conclusions
Side effects remain a problem (Peg-IFN/RBV side effects dominant) Additional side effects with DAAs include
– Telaprevir:1–4 rash, anemia, anorectal itching – Boceprevir:5,6 anemia, dysgeusia, neutropenia
Rash:1–4,7 – Most rashes (>90%) are mild, responsive to treatment (compatible with
‘treating-through’) – Treat rash early and monitor patient closely – Few cases of severe cutaneous reactions (SJS, DRESS) (resolved with
treatment discontinuation) Anemia
– Increased with telaprevir and boceprevir (EPO use only allowed in boceprevir trials)
– Anemia with telaprevir is limited (12 weeks) – Strategies for treating anemia include EPO, RBV dose reduction and blood
transfusions 1. Jacobson IM, et al. N Engl J Med 2011;364:2405–16; 2. Sherman KE, et al. Hepatology 2010;52(Suppl.):401A
3. Zeuzem S, et al. N Engl J Med 2011;364:2417–28; 4. Telaprevir EU SmPC 5. Poordad F, et al. N Engl J Med 2011;364:1195–206; 6. Bacon BR, et al. N Engl J Med 2011;364:1207–17
7. http://www.fda.gov/downloads/AdvisoryCommittees/Committees/MeetingMaterials/Drugs/AntiviralDrugsAdvisoryCommittee/UCM252562.pdf
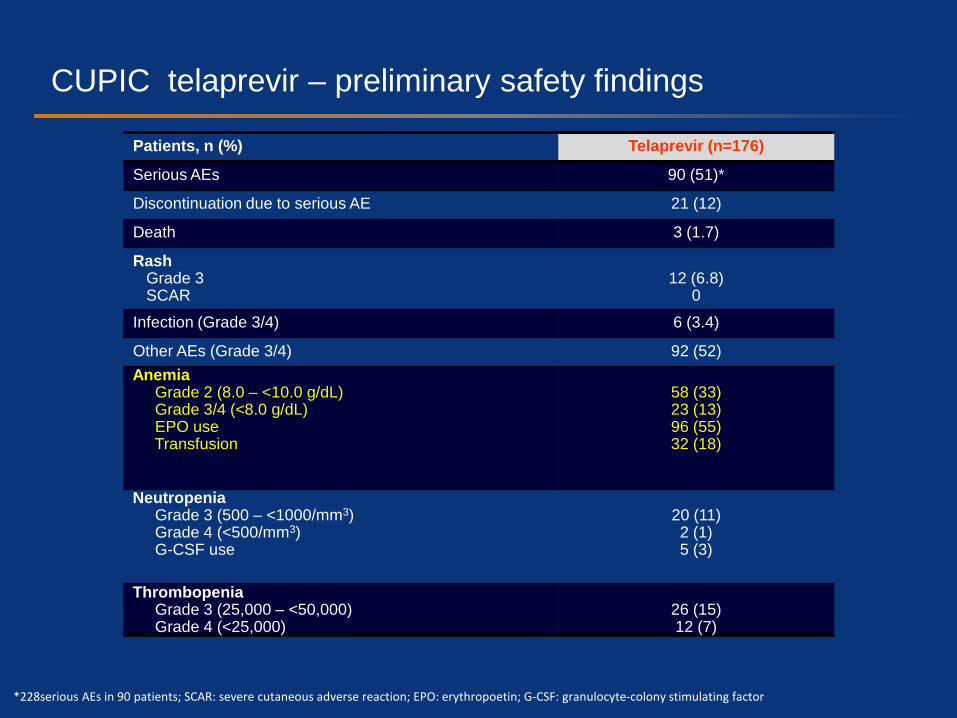
CUPIC: telaprevir – preliminary safety findings
Patients, n (%) Telaprevir (n=176)
Serious AEs 90 (51)*
Discontinuation due to serious AE 21 (12)
Death 3 (1.7)
Rash Grade 3 SCAR
12 (6.8)
0
Infection (Grade 3/4) 6 (3.4)
Other AEs (Grade 3/4) 92 (52) Anemia Grade 2 (8.0 – <10.0 g/dL) Grade 3/4 (<8.0 g/dL) EPO use Transfusion
58 (33) 23 (13) 96 (55) 32 (18)
Neutropenia Grade 3 (500 – <1000/mm3) Grade 4 (<500/mm3) G-CSF use
20 (11) 2 (1) 5 (3)
Thrombopenia Grade 3 (25,000 – <50,000) Grade 4 (<25,000)
26 (15) 12 (7)
*228serious AEs in 90 patients; SCAR: severe cutaneous adverse reaction; EPO: erythropoetin; G-CSF: granulocyte-colony stimulating factor
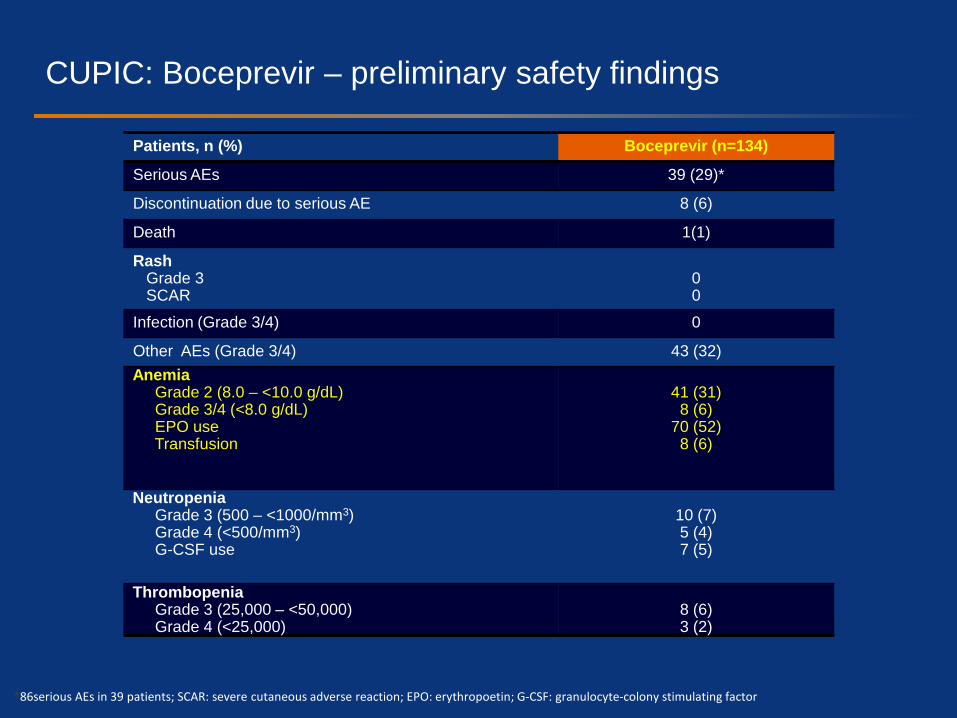
CUPIC: Boceprevir – preliminary safety findings
Patients, n (%) Boceprevir (n=134)
Serious AEs 39 (29)*
Discontinuation due to serious AE 8 (6)
Death 1(1)
Rash Grade 3 SCAR
0 0
Infection (Grade 3/4) 0
Other AEs (Grade 3/4) 43 (32) Anemia Grade 2 (8.0 – <10.0 g/dL) Grade 3/4 (<8.0 g/dL) EPO use Transfusion
41 (31)
8 (6) 70 (52)
8 (6)
Neutropenia Grade 3 (500 – <1000/mm3) Grade 4 (<500/mm3) G-CSF use
10 (7) 5 (4) 7 (5)
Thrombopenia Grade 3 (25,000 – <50,000) Grade 4 (<25,000)
8 (6) 3 (2)
*86serious AEs in 39 patients; SCAR: severe cutaneous adverse reaction; EPO: erythropoetin; G-CSF: granulocyte-colony stimulating factor
Summary
Anemia is a common event associated with DAAs – Reducing the dose of RBV is considered the best initial approach
for managing anemia with DAAs
Most rash associated with telaprevir therapy is mild/moderate – Typically pruritic and eczematous, progression is infrequent (<10% of
cases)
Follow recommendations for treatment discontinuation and rash management – Mild/moderate rash can be treated with topical corticosteroids or systemic
antihistamines without discontinuation of DAA therapy
29





























