Embed Size (px)
Citation preview

Management of Special Situations in Inpatient Hyperglycemia:Case Studies in ActionModule B
1

Learning Objectives
• Assess the impact of special situations on glucose control, eg, an increased risk for either hyperglycemia or hypoglycemia
• Identify potential risks for insulin errors to implement risk reduction strategies that improve patient safety
• Develop treatment strategies to manage special situations affecting glucose control in the inpatient setting
2

Current Recommendations for Hospitalized Patients: Critically Ill and Noncritically Ill Patients
ICU
• BG level 140–180 mg/dL • IV insulin preferred
Non‐Critical Care Settings
• Premeal BG level <140 mg/dL• All BG levels <180 mg/dL
4
BG = blood glucose; IV = intravenous.Moghissi ES et al; American Association of Clinical Endocrinologists; American Diabetes Association. Endocr Pract. 2009;15(4):353–369. Umpierrez GE et al; Endocrine Society. J Clin Endocrinol Metab. 2012;97(1):16–38.
Reassess the regimen if BG level is <100 mg/dLModify the regimen if BG level is <70 mg/dL

Causes of Hospital‐related Hyperglycemia
5
Known diabetes (uncontrolled, undertreated)
Known diabetes (uncontrolled, undertreated)
Undiagnosed diabetesUndiagnosed diabetes
Stress hyperglycemia (transient physiologic response to the stress of
acute illness or injury)
Stress hyperglycemia (transient physiologic response to the stress of
acute illness or injury)
Iatrogenic (corticosteroids, catecholamines, parenteral and enteral nutrition, reduced exercise)
Iatrogenic (corticosteroids, catecholamines, parenteral and enteral nutrition, reduced exercise)
“New Hyper‐
glycemia”

Hospitalization: Multiple Transitions, Shifting Clinical Situations
7
Adapted from Low Wang CC, Draznin B. Hosp Pract (1995). 2013;41(2):45–53.
Rehabilitation Facility
Primary Care
Provider
Skilled Nursing Facility
HospitalWard ICU
Surgery
Perioperative Management
Parenteral Nutrition
Enteral Nutrition
Steroid Therapy
Insulin Pump
U‐500Insulin

Basic Paradigm for Management of Inpatient Hyperglycemia in Patients With Pre‐existing Diabetes
Adequate planning for discharge
Evaluation of the daily BG patterns or the daily adjustments of insulin dose and type as needed
Outlining clear parameters for the management of hypoglycemia
Ordering scheduled point‐of‐care monitoring and scheduled insulin dosing while keeping the patient’s inpatient glucose goals in mind
Discontinuation of non‐insulin glucose‐lowering medications(in most cases)
Evaluation of patient’s preadmission glycemic control with a quick review of glucose patterns
8
Low Wang CC, Draznin B. Hosp Pract (1995). 2013;41(2):45–53.

Special Hospitalized Populations with Altered Insulin Sensitivity as Compared to the General Population
• Decreased insulin sensitivity– Infected– Acute organ injury (AMI, stroke)– Postsurgical– Glucocorticoid therapy– Pressor therapy (esp. epinephrine)– Transplant patients– TPN/PPN– Enteral (tube) feeding– ESRD, pre‐dialysis*– Severe burns– Hyperglycemia (glucotoxicity)
9
AMI = acute myocardial infarction; ESRD = end‐stage renal disease; PPN = peripheral parenteral nutrition; TPN = total parenteral nutrition.Adapted from Low Wang CC, Draznin B. Hosp Pract (1995). 2013;41(2):45–53.
• Increased insulin sensitivity– Hypoadrenal– Hypopituitary– Malnourished– ESRD, post‐dialysis– Post‐hyperglycemia correction
(reversal of glucotoxicity)
* may still be hypoglycemia prone

Transition From IV to SC insulin
10

Use of IV Insulin in the Inpatient Setting
In the intensive care unit
Patients with DKA
Patients with HHS
During/ after major surgery
11
DKA = Diabetic ketoacidosis; HHS = hyperglycemic hyperosmolar state.Moghissi ES et al; American Association of Clinical Endocrinologists; American Diabetes Association. Endocr Pract. 2009;15(4):353–369.

Transition From IV Insulin to SC Insulin
• IV insulin should be transitioned to SC basal‐bolus insulin therapy– When patient begins to eat and BG levels are stable
• Because of short half‐life of IV insulin, SC basal insulin should be administered at least 2–3 hours prior to discontinuing the drip– If short‐acting insulin also administered, IV insulin may be able to be stopped sooner, eg, after 1 hour
SC = subcutaneous.Umpierrez GE et al; Endocrine Society. J Clin Endocrinol Metab. 2012;97(1):16–38.
12

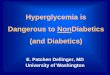
Rationale for Starting SC Insulin Prior to Discontinuation of IV Insulin
SC insulin prior to d/c of IV insulin keeps BG levels within target range
Failing to give SC insulin prior to d/c of IV insulin leads to rebound hyperglycemia
Low Wang CC, Draznin B. Hosp Pract (1995). 2013;41(2):45–53.
13
Bloo
d Glucose
–5 –4 –3 –2 –1 0 +1 +2
+3 +4Time (hours)
SC insulin dose
IV insulin infusion
Bloo
d Glucose
–5 –4 –3 –2 –1 0 +1 +2
+3 +4Time (hours)
No SC insulin
IV insulin infusion

SC Insulin Administration
14
Long‐acting insulin Rapid‐acting insulin
“Scheduled” (Sliding-scale insulin only uses this component)
Basal Nutritional Correction
Correction
Basal Nutritional
Total daily insulin needs
Moghissi ES et al; American Association of Clinical Endocrinologists; American Diabetes Association. Endocr Pract. 2009;15(4):353–369.Clement S et al. Diabetes Care. 2004;27(2):553–591.

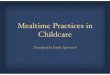
Basal‐bolus Therapy Is Effective for the Maintenance of Glycemic Control
1. Moghissi ES et al; American Association of Clinical Endocrinologists; American Diabetes Association. Endocr Pract. 2009;15(4):353–369. 2. Bray B. Consult Pharm. 2008;23(suppl B):17–23. 3. Roberts G et al. Med J Aust. 2012;196(4):266269. 4. Umpierrez GE et al. Diabetes Care. 2011;34(2):256–261.
Basal‐bolus is more effective at glycemic control vs sliding‐scale therapy in medical and surgical patients.3,4
Effective insulin therapy may contain basal, bolus, and supplemental doses to achieve target goals.1
Adapted from Bray.2
0
25
50
75
0 8:00 12:00 16:00 20:00 24:00 4:00 8:00
Breakfast Lunch Dinner Bolus insulin
Basal insulin
Plasma Insulin
(U/m
L)
Time
Correction insulin
15

Sliding‐scale Insulin
• Definition– Use of a mealtime insulin, typically regular insulin, as the sole insulin for managing a patient’s diabetes
– i.e., no scheduled basal insulin or prandial insulin• Potential problems
– Poor control of hyperglycemia (does not address basal insulin needs); also does not address premealneeds
– Insulin “stacking”– Hypoglycemia
• Not preferred method of SC insulin delivery
16
American Diabetes Association. Diabetes Care. 2014;37(suppl 1):S14–S80.Browning LA, Dumo P. Am J Health Syst Pharm. 2004;61(15):1611–1614.Hirsch IB. JAMA. 2009;301(2):213–214.

Converting From IV to SC Insulin
• Endocrine Society guidelines conservatively recommend the following:– Establishing the 24‐hour insulin requirement by averaging the IV insulin dose required over the previous 6–8 hours
– Using a fraction of that (ie, 75%–80%) as the total daily dose (TDD) of SC insulin
• Giving half of that as basal and dividing the other half among rapid‐acting insulin before meals
• Clinical trial support using 80% of the TDD to achieve 80–140 mg/dL
17
Umpierrez GE et al; Endocrine Society. J Clin Endocrinol Metab. 2012;97(1):16–38. Schmeltz LR et al. Endocr Pract. 2006;12(6):641–650.

Case Study Example: Moving to Step‐down Unit
• Patient is stable, will be moved out of the CCU and will begin scheduled meals
• The average dose of IV insulin was 1.5 units/hour over the past 8 hours
• TDD: ~40 units– 80% of 40 = 32 units
• Basal insulin = 50% of TDD = ~16 units (glargine/detemir) or 8 units NPH bid
• Nutritional = 50% of TDD = ~5 units per meal (x 3 meals) (lispro/glulisine/aspart; = 15 units)
Doses are then titrated against actual glucose levels.
18

(Reference: Mean BG 100–110 mg/dL)
Kosiborod M et al. Circulation. 2008:117(8):1018–1027.
Mean Glucose and In‐hospital Mortality in Patients With AMI: Hypoglycemia and Hyperglycemia Both Associated with Increased Mortality, Especially in Patients with No Diabetes
19
No diabetesAll patientsDiabetes
Odd
s Ratio
15
20
10
5
10
Mean BG Level (mg/dL)

Tight Glycemic Control in Critically IllAdults: Risk of Severe Hypoglycemia
A Meta‐analysis of 26 Randomized Controlled Trials (13,567 patients)
20
Severe Hypoglycemia(≤40 mg/dL)
StudyVan den Berghe et al.8Henderson et al.31
Bland et al.25
Van den Berghe et al.9Mitchell et al.35
Azevedo et al.22
De La Rosa et al.12
Devos et al.13
Oksanen et al.36
Brunkhorst et al.11
Iapichino et al.32
Arabi et al.10
Mackenzie et al.33
NICE-SUGAR18
OverallRisk Ratio (95% CI)
Favors IIT Favors conventional control
0.1 1 10
Overall Severe Hypoglycemia
RR 5.99 (4.47–8.03)
CI = confidence interval.Griesdale D et al. CMAJ. 2009;180(8):821–827.

MANAGING HYPOGLYCEMIA IN THE HOSPITAL
21

Hypoglycemia was a predictor of higher mortality in patients not treated with insulin, but not in patients treated with insulin.
Hypoglycemia and Mortality in AMI Patients, Stratified by Insulin Therapy
No Insulin Treatment0
10
Insulin Treatment
Mortality (%
)
60
Kosiborod M et al. JAMA. 2009;301(5):1556–1564.
18.4
9.2
P <0.001
10.210.4
P <0.92
HypoglycemiaNo hypoglycemia
Hypoglycemia was a predictor of higher mortality in patients not treated with insulin, but not in patients
treated with insulin.
N = 7338 no hypo
N = 482 hypo(BG <60 mg/dL)
22

Hypoglycemia and Risk of Death in Critically Ill Patients: NICE‐SUGAR Study
23
NICE‐SUGAR Study Investigators. N Engl J Med. 2012;367(12):1108–1118.
No hypoglycemiaModerate hypoglycemiaInsulinNo insulin
Severe hypoglycemiaInsulinNo insulin
726
545136
5722
3089
2066378
18637
1.00
1.22 (1.03–1.44)1.64 (1.34–2.01)
1.68 (1.23–2.29)3.84 (2.37–6.23)
0.12 1.00 8.00
IncreasedRisk of Death
DecreasedRisk of Death
Hazard Ratio (95% Cl)
0.007
0.003
P ValuePopulationDeathsno.
Subgroup
Median Time From Hypoglycemia to
Death (IQR)
9 (3–23)5 (1–22)
10 (4–15)1 (0–9)
days

Deleterious Impact of Hypoglycemia
• Sympathoadrenal response • Cardiac dysrythmias• Neuroglycopenia
– Altered sensorium and vision– Falls– Aspiration
• ? Pro‐inflammatory state• ? Procoagulant state• ? Endothelial dysfunction
24
Seaquist ER et al. Diabetes Care. 2013;36(5):1384–1395. Cryer PE. N Engl J Med. 2013;369(4):362–372. Goto A et al. BMJ. 2013;347:f4533.Rubin DJ, Golden SH. Hosp Pract. 2013;41(1):109–116. Hanefeld M et al. Cardiovasc Diabetol 2013;12:135.

The Hidden Costs of Inpatient Hypoglycemia
• Prolonged length of stay• Malpractice suits• CMS and “never events”
25
CMS = Centers for Medicare and Medicaid Services

CMS and “Never Events”
• In 2008, the Centers for Medicare and Medicaid Services (CMS) implemented a provision that denies Medicare payment for hospital‐acquired conditions (HACs)
• This provision brings attention to the quality of patient care and the financial impact associated with "never events" occurring during a patient's hospitalization
• Examples include:– Stages III and IV pressure ulcers– Catheter‐associated urinary tract infection– Vascular catheter‐associated infection– Falls resulting in fractures, dislocations, and/or intracranial
injuries– Manifestations of poor glycemic control
• Complications associated with hypoglycemia (death/disability)
26
Sand H et al. Neurohospitalist. 2012;2(1):18–27.

Causes of Treatment‐related Hypoglycemia
27
Elliott MB et al. J Diabetes Sci Technol. 2012;6(2):302–309.
Incidence percentage of proximate causes of hypoglycemia
0
Excess insulin
50 60 70
Inadequate monitoring
Diet change
Administration error
Hyperkalemia treatment
Physician computer entry error
20 30 4010

Scenarios Prompting Increased Monitoring and Possible Decreases in Insulin Dose
• Patient is switched to NPO status• Reduction in food intake• Discontinuation of enteral feeding or TPN• Discontinuation or reduction in IV dextrose• Timing of premeal insulin if meal disrupted due to medical procedures or patient transport
• Reduction in corticosteroid administration
28
NPO = nothing by mouth.

Special Situations
Hypoglycemia<70 mg/dL <40 mg/dL (severe)
• Can take PO Give 15 g carb (4 oz. orange juice)• NPO Give 12.5 g carb IV (1/2 amp D50)• MS changes Give 25 g carb IV (1 amp D50)
Rule of thumb: 25 g carb will BG 25–50 mg/dL • Document in chart• Assess reason for hypoglycemia (food, insulin dose,
sepsis, renal failure, hepatic failure) • Re‐evaluated regimen; usually decrease insulin
29

Patients Receiving Enteral or Parenteral Nutrition
30

Case Study: Total Parenteral Nutrition
• 55‐year‐old obese male is admitted with enterocutaneous fistula, no prior history of diabetes
• On admission, his BG level = 200 mg/dL • A1C level: 7.5% (previously unrecognized DM)• Patient is not eating, and it is anticipated that he will not be able to eat for 1 week
• TPN is started
31
DM = diabetes mellitus.

Prevalence of Hyperglycemia in Patients Receiving Specialized Nutritional Support
• Prevalence of hyperglycemia in patients receiving enteral nutrition is up to 30%
• May be >50% in patients receiving parental nutrition
32
Gosmanov AR, Umpierrez GE. Curr Diab Rep. 2013;13(1):155–162.Pleva M et al. Nutr Clin Pract. 2009;24(5):626–634.Arinzon Z et al. Arch Gerontol Geriatr. 2008;47(3):383–393.Pancorbo‐Hidalgo PL et al. J Clin Nurs. 2001;10(4):482–490.

20
12 1318
3328
1217
26
46
19
31
25
35
43 42
0
10
20
30
40
50
60 Pre‐TPN Max within 24 hrs During TPN10 days
p = 0.038
Admission
Pasquel FJ et al. Diabetes Care. 2010;33(4):739–741.
<120
BG Level (mg/dL)
p = 0.0007p = 0.010 p = 0.038
Hyperglycemia During TPN: Marker of Poor Outcomes and Mortality in the Hospital
33
121–150
150–180
>180
Mortality (%
)
<120 121–150
150–180
>180 <120 121–150
150–180
>180 <120 121–150
150–‐180
>180

Adverse Outcomes Significantly Associated With Hyperglycemia in Patients Receiving TPN
N BG Level (mg/dL) Odds Ratio P <0.05
Death Any Infection Renal Failure
Cheung et al. 111 <125 vs >164 10.9 3.9 10.9
Lin et al. 457 <114 vs 137–180 2.3 2.7 NS
Pasquel et al. 276 ≤120 vs >180 2.8 3.6* 2.2
Sarkisian et al. 100 ≤180 vs >180 7.22 NS NS
Olveira et al. 605 >180 vs <140 5.6 NR NR
34
*Data reported for pneumonia only.
Cheung NW et al. Diabetes Care. 2005;28(10):2367–2371. Lin LY et al. Am J Med Sci. 2007;333(5):261–265.Pasquel FJ et al. Diabetes Care. 2010;33(4):739‐741. Sarkisian S et al. Can J Gastroenterol. 2010;24(7):453–457.Olveira G et al. I. 2013;36(5):1061–1066.

Case Study: Total Parenteral Nutrition
What is the insulin treatment you would recommend for a DM patient on TPN?
1. IV insulin, separate from TPN2. Insulin added to TPN3. Basal‐bolus insulin
35

Approach to the Management of Hyperglycemia in Patients Receiving Enteral or Parenteral Nutrition
36
EN = enteral nutrition; PN = parenteral nutrition; POC = point of care.Gosmanov AR, Umpierrez GE. Curr Diab Rep. 2013;13(1):155–162.
Enteral Nurition (EN)
or Parenteral
Nutrition (PN) is initiated
Patient on ENUse diabetes‐specific formula. Start insulin therapy: basal insulin 0.15–0.25 U/kg (NPH q8h, glargine qd, detemir qd, bid).
Supplemental short‐acting insulin q4–6h
Patient on PNConsider limiting load in
TPN to 150–200 g/dL/day.Start insulin therapy.
Mix regular insulin with PN or use supplemental short‐acting insulin
q4–6h.
Titrate daily insulin therapy per glycemic.
Request notifications if
nutrition support
regimen is changed.Initiate
appropriate discharge planning.
Start (no diabetes) or continue (known diabetes) POC BG
monitoring q4–6h
BG >180 mg/dL x1
or BG = 140–180 mg/dL
x2

General Recommendations: Hyperglycemia Associated With Parenteral Nutrition (PN)
For patients receiving PN, regular insulin administered as part of the PN formulation can be both safe and effective.– A BG level >120 mg/dL before PN predicts the need for insulin
SC correction‐dose insulin is often used, in addition to insulin that is mixed with the IV nutrition.
• When starting PN, the initial use of a separate insulin infusion can help in estimating the TDD of insulin that will be required
• Separate IV insulin infusions may be needed to treat marked hyperglycemia during PN
Umpierrez GE et al; Endocrine Society. J Clin Endocrinol Metab. 2012;97(1):16–38. Moghissi ES et al; American Association of Clinical Endocrinologists; American Diabetes Association. Endocr Pract. 2009;15(4):353–369. Roehl KA et al. JPEN J Parenter Enteral Nutr. 2013;37(6):755–762.
37

Case Study:Insulin Needs and Enteral Nutrition
• 70‐year‐old woman admitted with a stroke– She has a prior history of T2DM, controlled on oral agents
– BG level on admission = 150 mg/dL, A1C level = 7%– Currently she is unable to swallow– Continuous EN is started on hospital day 2
38
T2DM = type 2 diabetes mellitus.

Case Study:Insulin Needs and Enteral Nutrition
What insulin treatment would you recommend for a DM patient on enteral tube feedings? (BG >200 mg/dL)1. Sliding scale only with rapid‐acting insulin2. IV insulin, variable‐rate infusion3. NPH and regular insulin every 8 hours4. Glargine qd or detimir qd/bid5. Supplemental short‐acting insulin every 4–6 hours
39

Glycemic Management of the Patient Receiving Enteral Nutrition (EN)
Continuous EN• Basal insulin: 40%–50% of TDD as long‐ or intermediate‐acting insulin given once or twice a day
• Short‐acting insulin: 50%–60% of TDD given q6h
Cycled EN• Intermediate‐acting insulin given together with a rapid‐ or short‐acting insulin with start of TF
• Rapid‐ or short‐acting insulin administered q4–6h for duration of EN administration
• Correctional insulin given for BG level above goal range
Bolus EN• Rapid‐ or short‐acting insulin given prior to each bolus
40
Umpierrez GE et al; Endocrine Society. J Clin Endocrinol Metab. 2012;97(1):16–38.

Limited Clinical Trial Data Comparing Insulin Therapy During Enteral Nutrition (EN)
• One prospective RCT has evaluated different insulin regimens in hospitalized patients receiving EN support
• 50 patients with and without history of DM with BG levels >140 mg/dL randomized to sliding scale with regular insulin (SSRI) alone vs with long‐acting insulin glargine once daily
• Results– “No difference” in glucose control but 48% of SSRI group required rescue with NPH due to persistent hyperglycemia
41
RCT = randomized controlled trial.Korytkowski MT et al. Diabetes Care. 2009;32(4):594–596.

Cautions With Insulin and Enteral Feedings
• Unexpected interruptions in enteral feeding occur frequently!– Administration of long‐acting insulin independent of enteral feeding may increase the risk of hypoglycemia
• Consider ordering D10 infusion (to provide calories) to be administered if tube feeding is discontinued or interrupted to prevent hypoglycemia
– Some data suggest that the use of “biphasic” analogs (premixed 70/30, 70/25) may be less likely to cause hypoglycemia because of their shorter durations of action
42
Low Wang CC, Draznin B. Hosp Pract (1995). 2013;41(2):45–53.Hsia E et al. Nutr Clin Pract. 2011;26(6):714–717.

Preventing Hypoglycemia in Patients Receiving Enteral and Parenteral Nutrition
If tube feeding is interrupted: If tube feeding is interrupted: • Start IV 10% dextrose infusion 50 mL/hour• Consider reducing next dose of long‐ or intermediate‐acting insulin, and • Increase frequency of bedside glucose monitoring
If parenteral nutrition is interrupted: If parenteral nutrition is interrupted: • Consider reducing next dose of long‐ or intermediate‐acting insulin (if used)
Reduce dose of scheduled insulin if: Reduce dose of scheduled insulin if: • Renal insufficiency• Discontinuation or reduction in steroids• Discontinuation of vasopressors • Decrease in carbohydrate intake
43
Gosmanov AR, Umpierrez GE. Curr Diab Rep. 2013;13(1):155–162.

Limited Clinical Trial Studying Insulin Protocols for Total Parenteral Nutrition (TPN)
An insulin protocol for management of hyperglycemia in patients receiving TPN was superior to ad hoc management
• Initiation of insulin at rate of 1 unit:20 g of dextrose with further up‐titration to ratio of 1 unit:15 g if BG >140 mg/dL was effective in nondiabetic patients in ICU (or average total daily insulin dose of 0.3 ± 0.2 u/kg)
44
Jakoby MG, Nannapaneni N. JPEN J Parenter Enteral Nutr. 2012;36(2):183–188.

Managing Hypoglycemia (BG <70 mg/dL) in Patients Receiving Enteral or Parenteral Nutrition
Administer IV dextrose 50% 25–50 mL Administer IV dextrose 50% 25–50 mL • If repeat BG is <70 mg/dL in 15 minutes, repeat dextrose IV push and start IV 10% dextrose infusion 50 mL/hour
• If repeat BG is ≥70 mg/dL in 15 minutes, measure BG in 1 hour and repeat treatment until BG is >100 mg/dL
Administer intramuscular 1 mg glucagon if there is no IV accessAdminister intramuscular 1 mg glucagon if there is no IV access
Reduce or hold next dose of long‐ or intermediate‐acting insulin (if used) Reduce or hold next dose of long‐ or intermediate‐acting insulin (if used)
45
Gosmanov AR, Umpierrez GE. Curr Diab Rep. 2013;13(1):155–162.

Perioperative Glucose Control
46

Examples of Perioperative Hyperglycemia and Poor Outcomes
Independent of diabetes status, increases the risk of perioperative morbidity and mortality.1
Preoperative BG >200 mg/dL is associated with deep sternal wound infections among patients undergoing CABG.2
Preadmission hyperglycemia independent risk factor for inpatient symptomatic pulmonary embolism after major orthopedic surgery.3
Hyperglycemia before carotid endarterctomy is associated with increased perioperative stroke, transient ischemic attack, myocardial infarction, and death.4
47
CABG = coronary artery bypass grafting.1. Lipshutz AK, Gropper MA. Anesthesiology. 2009;110(2):408–421. 2. Trick WE et al. J Thorac Cardiovasc Surg. 2000;119(1):108–114.3. Mraovic B et al. J Arthroplasty. 2010;25(1):64–70. 4.McGirt MJ et al. Neurosurgery. 2006;58(6):1066–1073.

Importance of Perioperative Glycemic Control in General Surgery
48
Kwon S et al. Ann Surg. 2013;257(1):8–14.
• Study evaluated relationship of perioperative hyperglycemia (>180 mg/dL) and insulin administration on mortality, preoperative interventions, and infections for patients undergoing elective colorectal and bariatric surgery at 47 participating hospitals between 4th quarter of 2005 and4th quarter of 2010
• If preoperative hyperglycemia was corrected with insulin, outcomes were better– NO significant increase in
• infections • preoperative interventions• or death
– Worst outcomes: BG >180 mg/dL– Best outcomes: BG <130 mg/dL

Glycemic Control (<180 mg/dL) in Patients With Diabetes During Cardiac Surgery
Reduces mortality Reduces morbidity
Lowers the incidence of
wound infections
Reduces hospital LOS
Enhances long‐term survival
Lazar HL et al; Society of Thoracic Surgeons Blood Glucose Guideline Task Force. Ann Thorac Surg. 2009;87(2):663–669.
49

IV Insulin Infusions: A Treatment Consideration During Surgery for Patients With T1DM
In the critically ill, glycemic control is best achieved with continuous insulin infusions rather than intermittent SC insulin injections or intermittent IV insulin boluses
All patients with diabetes undergoing cardiac surgical procedures should receive an insulin infusion postoperatively for at least 24 hours to keep BG <180 mg/dL
In patients with T1DM and labile T2DM patients on insulin, it is advisable to begin insulin infusion preoperatively or intraoperatively to facilitate better postoperative control
50
Lazar HL et al; Society of Thoracic Surgeons Blood Glucose Guideline Task Force. Ann Thorac Surg. 2009;87(2):663–669.

Preoperative Management and Assessment for Patients With Diabetes
Obtain A1C level prior to surgery in patients with DM or those at risk for postoperative hyperglycemia to characterize level of glycemic control
Initiate scheduled insulin therapy, using a combination of long‐ and short‐acting SC insulin, to achieve glycemic control for in‐hospital patients awaiting surgery
Consider insulin infusion protocol in selected T1DM patients or T2DM patients with labile control
Hold nutritional insulin after dinner the evening prior to surgery; consider modest 10%–20% reduction in evening long‐acting insulin
51
Lazar HL et al; Society of Thoracic Surgeons Blood Glucose Guideline Task Force. Ann Thorac Surg. 2009;87(2):663–669.

Oral Agents
• All oral hypoglycemic agents and non‐insulin diabetes medications should be held starting the night before surgery– Especially those that stimulate insulin secretion, such as sulfonylureas and meglitinides, because of their potential for producing hypoglycemia during fasting prior to surgery
– Potential for decreased renal function and metformin considerations
• …but stopping antidiabetic therapy too early may compromise glucose control perioperatively
52

Early Postoperative Period
If an IV insulin infusion is initiated in the preoperative period, it should be continued throughout the intraoperative and early postoperative period according to institutional protocols to maintain serum glucose levels ≤180 mg/dL.
53
Lazar HL et al; Society of Thoracic Surgeons Blood Glucose Guideline Task Force. Ann Thorac Surg. 2009;87(2):663–669.

Glucocorticoid‐induced Diabetes
54

Steroid Case Study
• 65‐year‐old patient with T2DM is admitted for severe COPD exacerbation. – His outpatient medications include insulin glargine 32 units SC at bedtime and insulin aspart 9 units SC before meals.
– He is started on prednisone 60 mg orally every morning as part of his treatment regimen.
– What do you expect the impact will be on his BG level, – How might you adjust his Inpatient regimen?
55
COPD = chronic obstructive pulmonary disease.

Steroid Case Study: Which of the following is most likely to occur?
1. All insulin requirements are likely to increase; therefore, his insulin glargine and insulin aspart doses should be increased by approximately 30%
2. His fasting BG level is likely to increase significantly; will need to increase his insulin glargine dose by approximately 30%
3. His postprandial glucoses are likely to increase significantly; will need to increase his premeal insulin aspart by approximately 30%
56

Glucocorticoids and Glycemic Control
• Glucose elevation is predominantly postprandial with relative lack of fasting hyperglycemia• Treatment often requires large doses of rapid‐acting insulin before meals (usually before lunch and dinner)
• Significant increase in basal insulin should be avoided as overnight hypoglycemia may be induced
Administration of glucocorticoidsAdministration of glucocorticoids
57
Low Wang CC, Draznin B. Hosp Pract (1995). 2013;41(2):45–53.

Prandial vs Fasting Glycemia
58
Iwamoto T. Pharmacotherapy. 2004:24(4):508–514.
Plasma Glucose Con
centratio
n (m
g/dL)
Prednisolone administeredPrednisolone not administered
300
400
200
100
0Before
Breakfast2 Hours After
Breakfast
BeforeLunch
2 Hours AfterLunch
BeforeDinner
2 Hours After Dinner

High Incidence of Steroid‐induced Hyperglycemia in the Hospital
86.0%
70%
0.0%
10.0%
20.0%
30.0%
40.0%
50.0%
60.0%
70.0%
80.0%
90.0%
100.0%
>144 mg/dL >180 mg/dL
At least one BG level
59
48
14
0
10
20
30
40
50
60
144 mg/dL 180 mg/dL
Mean BG levels
Fong AC, Cheung NW. Diabetes Res Clin Pract. 2013;99(3):277–280.
Percen
tage of P
atients
Percen
tage of p
atients
80 nondiabetic patients treated with high‐dose steroids

Frequency of Hyperglycemia in Patients Receiving High‐dose Corticosteroids
High dose defined as a dose equivalent of at least 40 mg/day of prednisone.Donihi AC et al. Endocr Pract. 2006;12(4):358–362.
Percen
t
Episodes
60

General Recommendations: Hyperglycemia Associated With Steroids
• Initiate SC basal‐bolus insulin therapy is recommended– Starting insulin dose and timing of administration individualized depending on severity of hyperglycemia and duration/dosage of steroid therapy
– Suggested starting dosage of 0.3–0.5 U/kg • day• For patients receiving high‐dose glucocorticoids and in those with severe hyperglycemia that is difficult to control, the use of continuous insulin infusion may be appropriate
61
Umpierrez GE et al; Endocrine Society. J Clin Endocrinol Metab. 2012;97(1):16–38. Moghissi ES et al; American Association of Clinical Endocrinologists; American Diabetes Association. Endocr Pract. 2009;15(4):353–369.

Basal‐bolus Therapy with Emphasis on Nutritional Insulin
• Medium‐dose glucocorticoids (40–60 mg/day) tend to cause minimal increase in FPG and marked elevation in PPG.
62
FPG = fasting plasma glucose; PPG = postprandial glucose. Clement S et al. Diabetes Care. 2004;27(2):553–591. Moghissi ES et al; American Association of Clinical Endocrinologists; American Diabetes Association. Endocr Pract. 2009;15(4):353–369.
“Scheduled” Supplemental/Correction*Basal Nutritional*
• Insulin drip • NPH • Long-acting insulin
analog (glargine, detemir)
Emphasis onregular or rapid-acting
insulin analog
Regular or rapid-acting insulin
analogq4–6h
Analog Mixes
*Rapid analog preferred.

Hyperglycemia and Glucocorticoid Therapy: Summary
• Institute glucose monitoring for at least 48 hours in all patients
• Prescribe insulin therapy as needed according to results of bedside BG monitoring
During initiation and taper of steroid therapy, proactive adjustment of insulin therapy can help
avoid uncontrolled hyperglycemia and hypoglycemia.
63
Umpierrez GE et al; Endocrine Society. J Clin Endocrinol Metab. 2012;97(1):16–38. Moghissi ES et al; American Association of Clinical Endocrinologists; American Diabetes Association. Endocr Pract. 2009;15(4):353–369.

Concentrated Forms of Insulin: The Example of U‐500
64

U‐500 Case Study
• 58‐year‐old male complaining of right toe pain and foot infection admitted to rule osteomyelitis– Height = 5′11″; weight = 257 lb; BMI = 36 kg/m2
– A1C level = 10.9%– Patient states that he is on insulin human injection U‐500 (concentrated) insulin 30 units before breakfast and dinner at home
– Started on vancomycin 1g IV q12h
65

Essential Prescribing Information
• Insulin human injection U‐500 contains 500 units of insulin in each milliliter (5 times more concentrated than traditional insulin human injection U‐100)
• Extreme caution must be observed in the measurement of dosage because inadvertent overdose may result in serious adverse reaction or life‐threatening hypoglycemia
• To reduce the risk of dosing errors, the actual dose in units, corresponding unit marking on U‐100 insulin syringe or mL markings on volumetric (TB or allergy) syringe with accompanying conversion chart
66

When a U‐500 Insulin Patient Is Admitted to the Hospital, Several Safety Issues Arise
67
– U‐500 insulin syringes do not exist, so patients use regular U‐100 insulin syringes to draw up their insulin at home.
– As the corresponding units on a regular insulin syringe are not comparable, there is misrepresentation of actual dose given. Dosed in tenths of milliliters.
– Pharmacy should interview the patient on admission to verify correct dose by having the patient demonstrate drawing up actual home dose.
Samaan KH et al. Am J Health Syst Pharmacy. 2011;68(1):63–68.

U‐500 Case Study
• When Pharmacy interviews the patient, he demonstrates that he draws the insulin to the 30 mark on the U‐100 syringe. What is the actual dose the patient is receiving at home?1. 30 units of R U‐500 insulin before meals2. 150 units of R U‐500 insulin before meals3. 6 units of R U‐500 insulin before meals
68

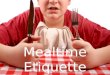
Comparison of U‐100 mL Syringe With Insulin Human Recombinant U‐100 and Insulin Human Recombinant U‐500 Dose
69
Although both are drawn to the 5‐unit mark, the syringe with U‐500 contains 25 units, whereas the syringe with U‐100 contains
5 units of insulin.
U‐500 Regular U‐100 Regular

Safety Measures Required to Reduce the Risk of Dosing Errors
Standardized CPOE, with alerts to Pharmacist and Diabetes Educator
Pharmacy home dose verification of R U‐500 insulin on admission
Patient’s R U‐500 sent home or stored in Pharmacy
Pharmacy dispenses prefilled volumetric syringe to the unit
U‐500 insulin dose and volume documented in the “MAR”
70

Continuous Subcutaneous Insulin Infusions (CSII), Also Known as
Insulin Pump Therapy, in the Hospital Setting
71

Insulin Pumps
• Electronic devices that deliver insulin through a subcutaneously inserted catheter: basal rate (variable) + bolus delivery for meals
• Used predominantly in T1DM• Pump patients are fastidious about their BG control and
reluctant to yield control to the inpatient medical team• Hospital personnel tend to be unfamiliar with pumps • Hospitals do not stock pump supplies• Need policies to allow pump patients to manage their
own diabetes during hospitalizations (many ethical/ medicolegal considerations!)
72

Insulin Pumps
73

74

Hours
InsulinLevel
0 2 4 6 8 10 12 14 16 18 20 22 24
Mealtime boluses
Basal rates
0.8 U/h 0.7 U/h0.9 U/h 0.6 U/h
1.1 U/h
8 U
5 U
10 U
2 U
Physiological Insulin Delivery From an Insulin Pump
75

Inpatient CSII Protocol
76
• Patients who have been well controlled with CSII at home can self‐manage their pumps during hospitalization– Patients should confirm in
writing their willingness and ability to use insulin pumps
• Nurses should verify and document all administered basal rates and bolus doses– If pump is interrupted for
>1 hour, another source of insulin (either IV or SC) MUST be given 30 minutes prior to discontinuation
• eg, Insulin pumps must be discontinued for an MRI
Patient AttestationI confirm that I have been fully trained on the use of my insulin pump prior to this hospitalization and that I am capable and willing to manage it independently during my hospital stay.If at any time I feel that I am unable to manage the pump, I will alert my medical team.
________ ________Patient Witness
CSII = continuous SC insulin infusion; MRI = magnetic resonance imaging.Noschese ML et al. Endocr Pract. 2009;15(5):415–424; EL3, review of medical records; EL4, expert opinion.

Transitioning Insulin Pump Therapy From the Outpatient to the Inpatient Setting: A Review of 6 Years' Experience With 253 Cases
• Data show that adherence to core process measures improved over time– 100% of cases had an endocrinology consultation– 100% had insulin pump order set completed– 94% had documentation of signed agreement specifying patient
responsibilities for continued use of pump technology while hospitalized– 64% had documentation of insulin pump flow sheet
• Clinical outcomes– Episodes of severe hyperglycemia (>300 mg/dL) and hypoglycemia
(<40 mg/dL) were significantly less common among pump users– No pump site infections, mechanical pump failures, or episodes of diabetic
ketoacidosis were observed among patients remaining on therapy
77
Cook CB et al. J Diabetes Sci Technol. 2012;6(5):995–1002.

Resources
American Association of Clinical Endocrinologists Inpatient Glycemic Resource Center
http://www.aace.com/resources/igcrc/Institute for Safe Medication Practices
http://www.ismp.org/default.aspAmerican Society of Hospital Pharmacists: Safe Use of Insulin in Hospitals
hhtp://www.ashop.org/s_ashp/docs/files_Safe_Use_of_Insulin.pdfSociety for Hospital Medicine Resource Center
http://www.hospitalmedicine.org/ResourceRoomRedesign/GlycemicControl.cfm
Samaan KH et al. Addressing safety concerns about U‐500 insulin in a hospital setting. Am J Health Syst Pharmacy. 2011 Jan 1;68(1):63–68.
78