Embed Size (px)
Citation preview

70 Sebha Medical Journal, Vol. 6(1), 2007.
Management of Tibial Deformities by Using
of Mono-tube External Fixator
Abdulrazag Shakshuki,* Sedig ben Dalla,* Abdelhakim Zanati,*
Abstract:
The aim of this study is to evaluate the results of dome-shaped tibial osteotomy with mono-tub external
fixator in treatment of genovarus and other tibial deformities with or without leg length discrepancy.
And to understand the system of external fixator ... advantages, disadvantages and complications.
And is it a better solution that replaces other methods which used in treatment of tibial deformities.
Key words: Tibial deformities, external fixation, mono-tube.
Introduction:
These deformities are very common conditions
Which often worries the mother of her 1st
baby, and account for a substantial percentage
of referrals to the pediatric orthopaedic clinics.
Careful explanation of this condition to the
mothers is important at their initial stage. At
this stage of early life the varus knee or the
bowed leg appearance might be worse
specially when accompanied by some internal
rotation of the lower limb with increased
anteversion of the femoral neck.
Basically, these early deformities were called
normal physiological changes that happen
during childhood; geno-varum and tibial bow
added to mild degree of rotation start to appear
during the first year of life, and continue
during the toddler stage until the age of 4-5
years, were reversal to geno-valgum and of
course developed into beautiful straight legs
eventually.
It's important to stress the normality of this
state not only to the parents but also to the
following doctors in polyclinics. The problem
of deciding when the normal varus or
angulated leg becomes pathological is very
difficult,1 and widespread abnormalities can be
discussed as the primary pathology e.g :
1. Epiphyseal dysplasia.
2. Metaphyseal dysplasia of Blount's disease.
3. Osteogenesis imperfecta.
4. Postero-medial tibial angulation.
5. Antero-lateral tibial angulation (pre
pseudoarthrosis tibia).3
6. post-trumatic physis injuries.
Among this short four –year- experience study,
we review our acknowledgment and out come
treatment of tibial deformities referred to our
department by using mono tube external
fixator.
Regarding their physio-pathological and
therapeutic aspect, our treatment plan follow
the type of deformity, age of patient and
severity of angles measured (staging). The
treatment to correct this deformity started for a
long time by using Ializrov,4 and Wagner
external fixator.
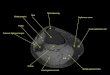
Aetiology Pathogenesis: As the most other idiopathic congenital
anomalies of the extremities no clear causative
factor was determined. In deed, many
attributers suppose different aetiology, the
congenital postero-medial tibial angulation, in
fact, is related to abnormal intrauterine
position of the fetus which usually occur in the
middle and distal third of the tibia dominantly
unilateral deformity and often skin dimple over
the angle of bow (approximately 50%) as in
"fig. 1" added to proximity to the ankle makes
the deformity mimic calcaneo-valgus footl
,while antero-lateral tibial bowing is often
correlate to pseudoarthrosis of tibia. And
supposed primary due to abnormal vascular
system of tibial shaft or secondary to zone 2
{Streeter) congenital constriction band of the
leg as2 in "fig. 2". Pathological changes of
bony sclerosis and cystic changes or dysplasia
might support that. Neurofibromatosis is
associated with deformity in 30% of the cases.
*) Orthopeadic Department, Central Hospital, Tripoli, Libya.

Management of Tibial Deformities …… Abdulrazag Shakshuki, et al.
71 Sebha Medical Journal, Vol. 6(1), 2007.
fig. 1: skin dimple fig. 2: congenital constriction band
Tibia vara (Blount's disease) of infantile
variety is more clearly defined by
developmental abnormalities as a result of
growth disturbance of the medial side of the
upper tibial growth plate. It's presence with
high incidence in west Africa and west
Indians. Those children are noted to walk
earlier and they also have lax ligaments and
joints.3 Cvolding and McNiel (1963) conclude
that this type of tibia vara is caused by failure
of growth of the postero-medial part of upper
tibial epiphysis. The other adolescent variety
developed at age of 8-13 years and those
children are above the 95th
percentile for height
and weight and usually unilateral.4
The post traumatic physis injury is another
cause of varus deformity (Tibia vara).
Excessive loading on mechanical axis of the
knee by early walking of overweight child with
physiological bowed legs may contributes to
the development of the infantile Blount's
disease, but this hypothesis has not been
proved.
Langenskiold (l964)5 Has classified tibia vara
into six stages (Table 1) according to
pathological changes seen on the radiographs.
That is very helpful to decide treatment should
be undertaken.
Table 1: (Langinskiold staging) and treatment regimens
Age Stage Treatment
<18mo 1-2 None
18-24mo 1-2 Frame/ blount brace (night)
2-3yr 1-2 Modified locked KAF*
3-8yr 3-5 Orthosis
3-8yr 6 Valgus rotational osteotomy
Resection of bony bridge
*KAF-Knee, Ankle, Foot.
Plan of Treatment and Follow-up:
Treatment methods as ordinary are described
into:
(1) Conservative regimen that includes all
cases younger than (3 years) and some cases
older than (3 years) with mild deformity. It is
processed in a way of short period casting
followed by long time bracing until the age
near the puberty.
(2) Surgical regimen includes:
a- cases do not respond to bracing with
progressive deformation.
b- For cases which primarily present with
sever deformity at late age and adults.
Physiological geno varum and tibial bow
rarely require treatment rather than family
education and regular observation, during
which radiographic angles and leg length
discrepancy are recorded. According to a chart
based on (Green-Andersoit) growth tables can
guides the time of possible surgical treatment.

Management of Tibial Deformities …… Abdulrazag Shakshuki, et al.
72 Sebha Medical Journal, Vol. 6(1), 2007.
In general tibio-femoral angle exceeds
(32degree), anatomical tibial angulation more
than (25 degree) with {Boyd) signs of
morbidity or significant cosmetic deformity
guiding toward the corrective surgery.
Despite dramatic appearance, the postero-
medial angular deformity is corrected
spontaneously in nearly all cases, some authors
recommend casting to hold the dorsiflexed foot
down to plantigrade position, but as actual
deformity is not related to the foot, this
maneuver was not logical and patients who are
never casted resolve as quickly as those who
are suffering from tibial curvature remodels
enough by the age of three that the leg appears
cosmetically acceptable, even if little bowing
may be evident on radiograph at 5-8 years.
Although this deformity needs no treatment,
long term follow-up indicates few numbers of
cases that will necessitate surgical correction
with the external fixator device, especially
with those complicated by leg length
discrepancy.6
Specific attention must be taken for the antero-
lateral tibial deformity as their critical outcome
might end by amputation of the limb, the
possibility of the fracture from birth until the
age of 8-10 years is still important prognostic
factor, (Boy d) classification is based on
bowing and the presence of cystic bone
changes, sclerosis, or dysplasia helps to prove
treatment time. Early treatment includes a total
contact brace to protect from fracture, and later
surgical corrective osteotomies with excision
of hamartomatous tissue or constriction band
and fixation with Mono Tube External Fixators
can improve the prognosis, bone grafting
insertion advised by many authors if fracture
occurs to minimize the high risk of tibial
pseudoarthrosis.6
Treatment of (Blount's) tibia vara is more
practical with high success rate regarding the
long term follow-up control.
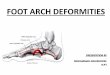
Langinskiold staging-Table 1) shows two
groups of patient according to the affected part
of tibial physis, physial plate depression
recorded by radiographs "fig. 3"7.. Those
groups; in children under 3 years with stage 1
or 2 disease complete correction can be
achieved using long leg brace that exert valgus
force and unload the medial tibial physis.
Fig. 3: Epiphseal-methaphyseal angle in Blount's disease
while in stage 3 or more and even in failed
bracing of more than one year, the corrective
surgical osteotomy is indicated with long term
post-operative bracing until the age of maturity
is recommended.
In stage 6, tibia vara with depression of medial
articular surface an osteotomy to elevate the
entire medial platue is necessary. Also a
combination with epiphysiodesis and
lengthening may be required for sever cases.7
Over all these different management ways, the
only surgical option that involves such
deformities is the corrective osteotomy to re
aligned the angulation apart from fixation
device or casting procedure.
Material and Methodology:
This study started four years ago in
orthopaedic department central hospital-
Tripoli. It's applied for (33) cases of tibial
deformities ("7" cases with antero-lateral and
postero-medial angular deformity, "20" cases
of Blount's disease, "3" cases post-traumatic
geno-varum "3" cases of geno-varum due to
achondroplasia and metaphysial dysplasia ).
As in "fig.4", all of them were Libyans; male
to female ratio was about 5:1. The age
category is grouped into: below (3 years),
above (3 years), and adults. The diagnostic
tools obtained from clinical observation with

Management of Tibial Deformities …… Abdulrazag Shakshuki, et al.
73 Sebha Medical Journal, Vol. 6(1), 2007.
condition of the skin overlying deformities and
associated anomalies and by 2nd
tool which is
the radiographs on both A-P and Lat views and
control X-ray of the normal side in unilateral
cases. Three major angles were measured;
(Drennan's) metaphyseal-diaphyseal angle in
tibia vara, which is the angle between
metaphyseal beaks is perpendicular to the long
axis of tibia which is abnormally more than
(16 degree), another tibio-femoral angle is
between the anatomical axis of the tibia and
femur (Levin), which is normally less than (32
degree) in children "fig. 5".
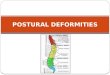
The (3rd
) angle of tibial shaft deformities is the
angle drawn between the anatomical axis of
proximal and distal parts of tibia which isn't
more than (25 degree) for better prognosis.6
Fig. 4: •Blount's disease • Post. Traumatic geno.varus Fig. 5: Tibio-femoral angle (Levine)
• Antero-lateral & postero-medial angulation Meta-diaphyseal angle (Drennan’s)
• Achondroplasia & metaphysial dysplasia
Surgical Technique:
The correction of deformity carried out using
Mono Tube External Fixator starts by
osteotomy of the fibula first then insertion of
two parallel pins in the tibia just below the
joint line in adults and below epiphyseal plate
in children and insertion of another two
longitudinal pins distal to the osteotomy line
on the tibia.
Distal and proximal pins are fixed together by
a bar of Mono Tube External Fixator.
The dome shape osteotomy was done just
below the proximal pins of external fixator.
Then we can correct the angle of deformity by
moving of distal tibia (anterior or posterior and
medial or lateral). After correction of the
angle, we can fix the external fixator.
N.B.: we can adjust the deformity even after
surgery (postoperative) by manipulation of
external fixator and we can do the surgery
under image intensifier screen (TV. Screen).
Results:
Among (33) cases of pathological Tibial
deformities:
(a) Tibial vara (Blount's disease).
(b) Postero-medial tibial angulation.
(c) Antero-lateral tibial angulation.
(d) Other geno-varus.
(27) cases were males and (6) females of
different geographical distribution along Great
Jamahiria, age-severity relationship recorded
as 31% less than "3 years" old of mild and
moderate deformity, while 69% more than "3
years" and adults of moderate and sever
deformity.
(16 cases) were treated conservatively.
(17 cases~19 legs) were treated surgically.
Two of them were treated bilaterally (we
treated both legs) by using Mono Tube
External Fixator are shown as:
(12 cases) good correction
(3 cases) incomplete correction + leg length
discrepancy less than 4cm.
(2 cases) delayed union + no correction.
(2 cases) did not complete their follow-up.
0
5
10
15
20
Blount's disease A. L. & P. M.angulation
Post. Traumaticgeno.varus
Achondroplasia

Management of Tibial Deformities …… Abdulrazag Shakshuki, et al.
74 Sebha Medical Journal, Vol. 6(1), 2007.
0
5
10
15
20
25
30
35
40
45
Blount's disease P.M. bow A.L. bow other G.V.
corrective tibial osteotomy+monotube E.F outcome
Good
Fair
Bad
11%
11%
16% 62%
post. Operative complication with monotube E.F.
D. wound healing D. bone union leg length discrepancy no complication
* E.F- external fixator * P.M- postero-medial
* A.L- antero-lateral * G.V- geno-varus
Complications:
(1). Delayed wound healing: two cases.
(2). Delayed bone union: two cases.
(3). Leg length discrepancy less the 4cm: three cases.
(4). Compartment syndrome: no cases recorded.
(5). Bone infection: none.
(6). Neuro-vascular injury: none.
* E.F- external fixator
* D- delayed

Management of Tibial Deformities …… Abdulrazag Shakshuki, et al.
75 Sebha Medical Journal, Vol. 6(1), 2007.
Conclusion:
The most orthopaedic attributers agreed that
lower extremities disorders in general usually
can be easily diagnosed with a thorough
history and examination apart from speciality
unit, laboratory and radiographic studies
facilitate both diagnosis and treatment
planning, as many of these deformities in
children are physiologically normal and
require only family reassurance, instructions
closed to regular follow-up and observation.
By the way the adolescent tibia vara with
(Drennan's) angle of more than (16 degree)
should be corrected carefully to avoid early
progressive degenerative arthritis at adulthood.
The surgical treatment preferred in adults and
adolescent and recently many authors prefer
surgical treatment even in early life (4-5) years
old.1
The (Mono Tube External Fixator) can be
used to treat these deformities.
This method gives us more flexibility to
correct the deformities even after surgery
(post-operative) by re adjustment of external
fixator, and gives rapid return of joint motion,
earlier weight bearing and walking. By using
Mono Tube External Fixator we can correct
leg length discrepancy. Also Mono Tube
External Fixator augmented by autogenous
bone graft can be one of the best options.
Some cases:
(Preoperative) (Dome- osteotomy + monotube Ex. Fix.)
(Blount's disease) (Blount's disease) Preoperative Postoperative

Management of Tibial Deformities …… Abdulrazag Shakshuki, et al.
76 Sebha Medical Journal, Vol. 6(1), 2007.
Using of Mono-Tube External Fixator in correction bf postero-medial tibial angulation deformity
with leg length discrepancy.
Pre. Operative Post. Operative after healing & removal of Ex. Fix
Congenital anterior angulation of the tibia corrected with Mono-Tube External Fixator.
References:
1. Pappas AM. Congenital postero-medial
bowing of the tibia and fibula. J pediatric
ortho, 1984.
2. Morrissey RT. Congenital pseudoarthrosis
tibiae factors that effect Results dine ortho,
1982.
3. Johnston CE. Infantile tibia vara. clinc
ortho, 1990.
4. Tudisco C et al. Functional results at the end
of skeletal growth in 30 patients affected
by congenital ps tibiae. J pediatric ortho,
2000.
5. Langinskiold. Tibia vara, osteochondrosis
deformans tibiae, Blount's Dis clinic ortho,
1981.
6. Review of orthopaedics. Mark D. Miller,
M.D 4th
Edition, 2004.
7. Bwen JR-Lealy JL, Zahng Z. Partiale
epiphyseodesis at the knee to Correct the
angle deformities, clinc ortho, 1985.
8. Feldman MD, Schooenecker PL use of the
metaphyseal-epiphyseal Angle in
evaluation of the bowed legs. J Bone Jr
Surg, 1993.