Embed Size (px)
Citation preview

Management of Type 2 Diabetes
Dr.Gayotri GoswamiAttending Physician,
Jacobi-North Central Bronx Hospital April 29th, 2009



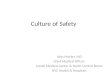
Stages of Type 2 Diabetes Related to Beta-Cell Function
Adapted from Lebovitz HE. Diabetes Reviews. 1999;7(3).
212 210 6 0 6 10 14
BetaCellFunction
(%)
0
50
100
75
25
Type2Phase1IGT
YearsfromDiagnosis
Type2Phase2
Type2Phase3
Postprandial
Hyperglycemia


TREATMENTOFT2DMISNOTJUSTTREATINGHYPERGLYEMIA
PREVENTION AND TREATMENT OF MACROVASCULAR DISEASEREQUIRES ADDRESSING ALL
CARDIOVASCULAR RISK FACTORS

HbA1c
Retinopathy
Nephropathy
NeuropathyMacrovascular disease
DCCTDCCT9 7%
76%
54%
60%
41%*
Kumamoto9 7%
69%
70%
-
-
UKPDS8 7%
17-21%
24-33%
-
16%*
*notstatisticallysignificant
Good Glycemic Control (Lower HbA1c) Reduces ComplicationsGood Glycemic Control (Lower HbA1c) Reduces Complications
UKPDS Study Group: Lancet 352:837-53, 1998Ohkubo Y: Diabetes Res Clin Prac 28:103-17, 1995DCCT Study Group: N Engl J Med 329:977-86, 1993


14
Targets for Glycemic Control*Normal Goal
AmericanDiabetesAssociation1
A1C (%)Preprandial plasma glucose (mg/dL) Peak postprandial plasma glucose (mg/dL)
<6.0<110
<7.090-130<180
EuropeanDiabetesPolicyGroup2
A1C (%)Preprandial plasma glucose (mg/dL) Postprandial glucose (mg/dL)
<6.0<110
<6.5<110<135
AmericanAssociationofClinicalEndocrinologists3
A1C (%)Preprandial plasma glucose (mg/dL) Postprandial glucose (mg/dL)
<6.0<110
<6.5<110<140
*More stringent goal of <6.0% should be considered for individual patients. Generally, A1C goal for each patient is an A1C as close to normal as possible without significant hypoglycemia.A1C = glycosylated hemoglobin A1C.1. ADA. Diabetes Care. 2006;29(suppl 1):S4-S42. 2. European Diabetes Policy Group 1999. Diabet Med. 1999;16:716-730. 3. Feld S. Endocr Pract. 2002;8(suppl 1):40-82.

Major components for patient centered care
International Diabetes Center model of patient-centered team care

Metabolic Management of type 2 DM
Nathan et al, A Consensus Statement from the American Diabetes Association and the European Association for the Study of Diabetes. Diabetes Care,29:759-764,2006

NON-PHARMACOLOGICMEASURES
Diabetes Self Management Training (DSMT)
Lifestyle Interventions • Ongoing Patient Education• Medical Nutrition Therapy (MNT)• Physical Activity• SMBG
Behavioral Health• Emotional assessment• Support Needs

Medical Nutrition Therapy
• A1c has been shown to decrease by 1% in a RCT in Type 1 Diabetics
• In Type 2, a decrease in A1c of 2% in newly diagnosed cases and 1% in cases of 4 years duration
• Most effective during the early stages after diagnosis of Type 2 when insulin resistance is the highest
• Messages on physical activity and MNT should be the most aggressive during the early stages

‘Healthy Plate Concept’

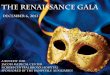
Contributions of FPG and PPG to Overall Glycemia in T2DM
PPG+FPG=A1C(%)
01020304050607080
1 2 3 4 5
A1CQuintiles
Contribution(%)
PPG
FPG
FPG = fasting plasma glucose. PPG: Post prandial glucoseAdapted with permission from Monnier L et al. Diabetes Care. 2003;26:881-885.
<7.3 7.3- 8.4 8.5 - 9.2 9.3- 10.2 >10.2

PHARMACOLOGICMEASURES

Sites of Action of Oral Antidiabetic Agents
Muscleandadiposetissue:PeripheralglucoseuptakeTHIAZOLIDINEDIONES
Liver:GlucoseproductionBIGUANIDES
Pancreas:InsulinsecretionSULFONYLUREASMEGLITINIDESAmylinsecretion
Intestine:Digestionandabsorptionofcarbohydrates-GLUCOSIDASEINHIBITORS
GIT:IncreaseglucosestimulatedinsulinsecretionINCRETINMIMETICS

Effect of Oral Therapies on A1c

Biguanides: inhibits hepatic glucose production, slow titration dose
• Glucophage(metformin) 500 mg
850 mg1000 mg 500 to 2550 mg daily (b.i.d.)
• GlucophageXR(extendedreleasedeliverysystem)500mg750mg 500to2000mgdaily(q.d.orb.i.d.)

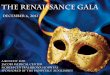
-1.2
-1.7
-2.0
-1.6
-0.9
-2.5
-2
-1.5
-1
-0.5
0
0.5
MeanDifferenceinHbA1c(%)vs.PlaceboatEndofStudy(14weeks)
500mg
(n=73)
1000mg
(n=73)
1500mg
(n=76)
2000mg
(n=73)
2500mg
(n=77)
*
*
*
*
*
*P<0.001
Metformin Dose-Response Study
Mean HbA1c Reductions
Garber AJ et al., Am J Med 1997.

-32
-42-36
-39-50
-40
-30
-20
-10
0
%Risk
Reduction
American Diabetes Association. Diabetes Care. 1999;22(suppl 1):S27-S31.
UK Prospective Diabetes Study (UKPDS) Group. Lancet. 1998;352:854-865.
*Comparedwithconventionaltreatment;†P=0.0023;‡P=0.017;§P=0.011;¶P=0.01
‡
§¶
AnyDiabetes- Diabetes- Related Related All-Cause Endpoint Mortality Mortality MI
UKPDS:Effects of Intensive (Metformin)
Treatment*
†

Sulphonylureas
• Lower BG by increasing insulin secretion from the pancreatic beta cells
• The glucose lowering effect usually plateaus at approximately one half of the maximum recommended dose *
• Should be used cautiously in the elderly and those with hepatic or renal impairment
*Simonson et al.Diabetes care,1997;20:597-606 Stenman et al. Ann.Int.Med, 1993;118:169-172

Sulfonylureas (insulin secretagogues)
• FIRST GENERATION AGENTS- lower binding affinity to the SFU receptor and must be given in higher doses
• SECOND GENERATION AGENTS– Glucotrol(glipizide) 2.5to20mgdaily(b.i.d.)– GlucotrolXL(glipizideGITS) 2.5to20mgdaily(q.d.)– Micronase,DiaBeta(glyburide)2.5to20mgdaily(q.d.)– Glynase(micronizedglyburide)1.5to6mgdaily(q.d.)– Amaryl(glimepiridescoretabs)0.5to8mgdaily(q.d.)

Thiazolidinediones
• Pharmacological ligands for a nuclear receptor known as the PPAR
• When activated, this receptor binds to response elements on DNA and alters transcription in various genes to regulate carbohydrate and lipid metabolism
• Through this process increase insulin stimulated glucose uptake in the skeletal muscle cells

MolecularTargetsofPPAR&PPARaction
NEJM 2004; 351:1106-18

Thiazolidinediones
• Indicated as monotherapy and in combination with SFU, metformin & insulin
• Weight gain & edema are commonly seen when used with insulin
• Contraindicated in patients with CHF and hepatic impairment
• Additionally combining 2 sensitizers produces and additive effect*
*Einhorn et al.Clin.Ther.2000;22:1395-1409

Glinides(Nateglinide and Repaglinide)
• Rapid but short lived release of insulin that lasts 1 to 2 hours
• Attenuate post prandial glucose excursions, therefore should be used to target PP blood glucose levels
• Repaglinide (Prandin) is more potent ,is minimally cleared by the kidneys and can be used safely with severe renal impairment

Insu
lin (µ
U/m
L)In
sulin
(µU
/mL)
00 44 88 1212 1616 2020
Time (hours post-morning dose)Time (hours post-morning dose)
Nateglinide: Meal-Related Insulin Levels in type 2 diabetes
NAT 120 mg ac x 3*NAT 120 mg ac x 3*Placebo ac x 3Placebo ac x 3
(n = 10) After 1 Wk Tx(n = 10) After 1 Wk Tx
120120
100100
8080
6060
4040
2020
00
MealMeal MealMeal SnackSnack
*No dose taken with snack.*No dose taken with snack.Walter YH, et al. Walter YH, et al. Eur J Clin Pharm. Eur J Clin Pharm. 2000;56:129–133.2000;56:129–133.
MealMeal

-Glucosidase Inhibitors delays digestion of carbohydrates and slows
glucose absorption, slow titration dose• Precose (acarbose)
– 25 mg– 50 mg– 100 mg 75 to 300 mg daily (t.i.d.) before meals
• Glyset (miglitol) – 25 mg– 50 mg– 100 mg 75 to 300 mg daily (t.i.d.) before meals

-Glucosidase Inhibitors
• Long history of use• Good safety profile• No weight gain• Mild stool softening • No substantial
systemic drug-drug interaction
• Good adjunctive therapy
• Require high-carbohydrate diet
• Must be taken before every meal
• Modest efficacy
• Flatulence and GI side effects
• Elevated LFT’s have been reported
LebovitzHE,Diabetes Reviews1998.
Advantage Disadvantage

INCRETINS
GLP 1 – Glucagon like peptide 1GIP – Glucose dependant insulinotropic polypeptide

GLP-1 GIP IsreleasedfromLcellsinileumandcolon1,2
IsreleasedfromKcellsinduodenum1,2
Stimulatesinsulinresponsefrombetacellsinaglucose-dependentmanner1
Stimulatesinsulinresponsefrombetacellsinaglucose-dependentmanner1
Inhibitsgastricemptying1,2 Hasminimaleffectsongastricemptying2
Reducesfoodintakeandbodyweight2
Hasnosignificanteffectsonsatietyorbodyweight2
Inhibitsglucagonsecretionfromalphacellsinaglucose-dependentmanner1
Doesnotappeartoinhibitglucagonsecretionfromalphacells1,2
1. Meier JJ et al. Best Pract Res Clin Endocrinol Metab. 2004;18:587–606. 2. Drucker DJ. Diabetes Care. 2003;26:2929–2940.

42
Modulation of Insulin and Glucagon Levels: The Enteroinsular Axis
alphacellsalphacellsbetacellsbetacells
Pancreas
GutInsulin (GLP-1,GIP)
Glucagon(GLP-1)
Nutrientsignals
Hormonalsignals•GLP-1•GIP
Neuralsignals
AdaptedwithpermissionfromCreutzfeldtW.Diabetologia.1979;16:75–85.Copyright©1979Springer-Verlag.DruckerDJ.Diabetes Care.2003;26:2929–2940.KiefferTetal.Endocr Rev.1999;20:876–913.NauckMAetal.Diabetologia.1993;36:741–744.

43
Time,min
IRInsulin,m
U/L n
mol/L
0.6
0.5
0.4
0.3
0.2
0.1
0
80
60
40
20
0
18060 1200
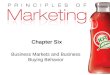
TheIncretinEffectinSubjectsWithoutandWithType2Diabetes
ControlSubjects(n=8)
PatientsWithType2Diabetes(n=14)
Time,min
IRInsulin,m
U/L n
mol/L
0.6
0.5
0.4
0.3
0.2
0.1
0
80
60
40
20
0
18060 1200
Oralglucoseload
Intravenous(IV)glucoseinfusion
IncretinEffect
Theincretineffectisdiminished
intype2diabetes.
AdaptedwithpermissionfromNauckMetal.Diabetologia.1986;29:46–52.Copyright©1986Springer-Verlag.

GLP-1 and GIP Are Degraded by the DPP-4 Enzyme
Meal
IntestinalGIPandGLP-1
release
GIPandGLP-1Actions
DPP-4Enzyme
GIP-(1–42)GLP-1(7–36)
Intact
GIP-(3–42)GLP-1(9–36)Metabolites
RapidInactivation
Half-life*GLP-1~2minutesGIP~5minutes
DeaconCFetal.Diabetes.1995;44:1126–1131.*MeierJJetal.Diabetes.2004;53:654–662.

EffectiveGLP1therapies:
Exenatide (Byetta)– binds to and activates the GLP 1 receptor and resists degradation by DPP-4 (April 2005)
Sitagliptin (Januvia) – resistant to DPP-4 degradation (October 2006)
Vildagliptin – inhibits the DPP-4 enzyme (Under review by FDA)

Byetta (Exenatide)
• Indicated as an adjunctive therapy in patients withType 2 DM who are taking Metformin, SFU or a combination and TZDbut has not achieved adequate control
• Not recommended for use in patients with ESRD, severe renal impairment, or severe gastrointestinal disease and in Type 1 Diabetics

Byetta (Exenatide)
• Major side effect is nausea.
Recent FDA warning of acute pancreatitis being associated with Byetta.
• Prescribed as a subcutaneous injection given within 1 hour before the morning and evening meal
• Starting dose is 5 ug BID and can be increased to 10 ug BID

Sitagliptin (Januvia)DDP-4 inhibitor
• Monotherapy or in combination with Metformin, TZD, Glimepiride ± Metformin
• Mainly target PPG but have been shown to decrease FBG levels
• Daily recommended dose is 100mg orally once a day
• Dose adjustment is required in moderate to severe renal insufficiency

“Although insulin therapy has not traditionally been implemented early
in the course of Type 2 diabetes, there is no reason why it should not
be…”
Nathan DM. NEJM. Oct 24, 2002;347(17):1342-1349.

Physiologic Blood Insulin Secretion Profile
PlasmaPlasmaInsulinInsulin((µU/mL)U/mL)
4:004:00
2525
5050
7575
8:008:00 12:0012:00 16:0016:00 20:0020:00 24:0024:00 4:004:00
Breakfast Lunch Dinner
Time
8:008:00
Adapted from White JR, Campbell RK, Hirsch I. Postgraduate Medicine. June 2003;113(6):30-36.

HoursAfterGlucoseIngestion
PatientsWithType2DiabetesHealthySubjects
PlasmaInsulin
0
20
40
60
–1 0 1 2 3 4 5
90
180
270
360
–1 0 1 2 3 4 5
PlasmaGlucose
Mitrakou A, et al. Diabetes. 1990;39:1381–1390.
Loss of Early Insulin Release Leads to Postprandial Hyperglycemia
(mU/L)(mg/dL)

INSULINS Peak(duration)hrs
• RAPID-ACTINGINSULINANALOGS– Humalog(lispro) 1-2 (2-6)– Novolog(aspart) 1-2 (2-6)– Glulisine(epidra) 1-2(2-6)
• SHORT-ACTING-Regular 2-4 (3-6)
• INTERMEDIATE-ACTING
– NPH 6-12 (10-24)
• LONGACTING– Lantus/glargine none (10-24)– Levemir/detemir -

Fixed dose insulin mixes
HUMULIN(NPH/REG)
–70/30
–50/50
HUMALOG(Prot-lispro/freelispro)
–75/25
NOVOLIN(NPH/REG)
–70/30
NOVOLOGMIX(Prot-aspart/aspart)
–70/30

Insulin delivery devices


OPTIONS………
1. Once daily background or basal insulin if fasting BG is elevated but glucose values remain stable during the day,
2. Once daily or twice daily pre-mixed insulin analogue, orally administered drugs may or may not be continued
3. Basal bolus therapy…..first initiate basal along with 1 bolus injection before the largest meal and eventually at each meal ,if needed

What doses to start with……..
• With HbA1c <8%, begin 0.1U/Kg body weight
• HbA1c 8-10%, start 0.2U/kg body weight
• HbA1c >10%, start 0.3U/Kg body weight
• With pre-mixes can divide the total dose by 2 if used twice a day
• With insulin glargine, adjust dose every 3-7 days until target fasting dose is reached
Bergenstal Endocrine Practice,Jan 2006

Advantages of rapid acting insulin analogs
• Restores the early insulin peak in combination with meal ingestion
• Prevents the hyperinsulinemia resulting from the late absorption of regular insulin and thereby protects against hypoglycemia

Human Insulin Time-Action Patterns
Time(hours) SCinjection
Normalinsulinsecretionatmealtime
Changeinseruminsulin
BaselineLevel
Theoreticalrepresentationofexpectedinsulinreleaseinnondiabeticsubjects

Human Insulin Time-Action Patterns
Time(hours) SCinjection
Normalinsulinsecretionatmealtime
Regularinsulin(human)
BaselineLevel
TheoreticalrepresentationofprofileassociatedwithRegularInsulin(human)
Changeinseruminsulin

Analog Insulin Time-Action Patterns
Time(hours) SCinjection
Normalinsulinsecretionatmealtime
BaselineLevel
Theoreticalrepresentationofexpectedinsulinreleaseinnondiabeticsubjects
Changeinseruminsulin

Analog Insulin Time-Action Patterns
Time(hours) SCinjection
Normalinsulinsecretionatmealtime
BaselineLevel
Theoreticalrepresentationofprofileassociatedwithrapid-actingInsulinAnalog
Changeinseruminsulin
Rapid-ActingInsulinAnalog

Human Insulin Time-Action Patterns
Time(hours) SCinjection
Normalinsulinsecretionatmealtime
NPHinsulin(human)
BaselineLevel
TheoreticalrepresentationofprofileassociatedwithNPHInsulin
Changeinseruminsulin

Human Insulin Time-Action Patterns
Time(hours) SCinjection
Normalinsulinsecretionatmealtime
HumanPremix70/30(70%NPH&30%Regular)
BaselineLevel
TheoreticalrepresentationofprofileassociatedwithHumanPremix70/30
Changeinseruminsulin

Analog Insulin Time-Action Patterns
Time(hours) SCinjection
Normalinsulinsecretionatmealtime
QD(basal)AnalogInsulin
BaselineLevel
TheoreticalrepresentationofprofileassociatedwithBasalAnalogInsulin
Changeinseruminsulin

Analog Insulin Time-Action Patterns
Time(hours) SCinjection
Normalinsulinsecretionatmealtime
BaselineLevel
TheoreticalrepresentationofprofileassociatedwithInsulinAnalogPremix
Changeinseruminsulin
InsulinAnalogPremix

USE COMBINATION THERAPY AND GET PATIENTS TO GOAL AS SOON AS POSSIBLE

COMBINATION THERAPYAACE Guidelines, Endocrine Practice, May/June 2007

• Finally, Type 2 DM is a progressive disease with worsening glycemia over time.
• Therefore, addition of medications is the rule, not the exception, if treatment goals are to be met over time.