Embed Size (px)
Citation preview

Management of Upper GIT Bleeding
BY Reda ElWakil, MD
Prof.of Tropical MedicineAin Shams University
Cairo, Egypt
1

2
Upper GIT bleeding is defined as haemorrhage from any Source proximal to the ligament of Trietz.
It is estimated that greater than 350.000 hospital admissions for upper GITB occur annually with an overall mortality of approximately 10%
Yavorski et al.,Am J Gastroenterol.1995;22:723-36

NumberPercentage
Variceal70170.1
Non Variceal26126.1
Obscure causes383.8
Causes of Upper GIT bleeding in 1000 patients presenting to Emergency Endoscopy Unit Ain Shams University Hospital
from January 2007-January 2008
Elwakil et al,J. Egypt. Soc. Parasitol., 41 (2), 2011: 455 – 467 3

Varicealgroup
Non Varicealgroup
P value
Recurrence: N (%)Yes No
136 (19.4)565 (80.6)
17 (6.5)244 (94.5)
<0.001
Mortality: N (%)Yes No
30 (4.2)671 (95.8)
1 (0.4)260 (99.6)
0.001
Recurrence and Mortality in Variceal vs Non-Variceal groups of cases
Elwakil et al,J. Egypt. Soc. Parasitol., 41 (2), 2011: 455 – 467 4

Variceal bleeding is one of the most alarming life-threatening complications of cirrhosis.
60% of patients with cirrhosis develop esophageal varices 30% of these patients bleed within 2 years
50% bleed at some point during their lifetime.
The mortality rate for variceal bleeding is 30-50%
Corson and Williamson, eds: Surgery. London, UK: Mosby-Year Book; 2001
5
Variceal bleeding

Clinically significant bleeding:
1.Transfusion requirement of ≥ 2 units of blood
within 24 hours of time zero
2.Systolic blood pressure<100mmHg or a
postural change of >20mmHg,
3.And/or pulse rate >100/minute at time zero.
De Franchis ; Proceedings of the Third Baveno International Consensus Workshop 2001.
6

Therapeutic aims in acute variceal bleeding
• Correct hypovolaemia
• Stop bleeding as soon as
possible
• Prevent early rebleeding
• Prevent complications
associated with bleeding
• Prevent deterioration in liver
function
7

1. Assess and address the ABCs
2. Those patients at high risk of aspiration must be
intubated.
3. Bilateral 16-gauge upper extremity peripheral
intravenous lines are adequate for volume
resuscitative efforts.
4. Replace each milliliter of blood loss with 3 mL of
crystalloid fluid. .
Initial management
Silverstein et al. Gastrointest Endosc ,1981 May; 27(2): 80-93 8

5. Foley catheter placement is mandatory for
evaluation of the urinary output as a guide to renal
perfusion.
6. This labor-intensive management should be
performed only in an ICU setting.
7. Insert a nasogastric tube (NGT) and perform an
aspirate and lavage procedure.
Silverstein et al. Gastrointest Endosc 1981 May; 27(2): 80-93
9

Infection is one of the strongest prognostic indicators in AVB and is associated with early rebleeding and greater mortality[1].
Antibiotic prophylaxis significantly reduces the percentage of patients who develop infection and rebleeding and increases survival[2] .
All cirrhotic patients with upper GI bleeding must receive prophylactic antibiotic therapy at admission. The current recommended antibiotic schedule is oral norfloxacin at dose of 400 mg BID for 7 d although ciprofloxacin could also be used[3] .
Intravenous (IV) ceftriaxone (1 g/d) might be more effective than oral norfloxacin in preventing bacterial infections in Child B and C patients[4], in hospital settings with high prevalenceof quinolone-resistant bacterial infections and in patients on previous quinolone prophylaxis [5] .
Antibiotic Prophylaxis
1-Bernard et al., Gastroenterology.1995;108:1828–1834.2-Bernard et al.,Hepatology.1999;29:1655–1661.3-Sarin et al. Hepatol Int. 2008;2:429–439.4- Fernández et al. Gastroenterology.
2006;131:1049–1056.5-de Franchis. J Hepatol (2010),
10

Renal function
The development of renal failure in cirrhotic patients after an AVB which occur in approximately 11% of cases is associated with a dismal prognosis.1
Renal function should be supported by adequate fluid and electrolyte replacement (saline solutions should be avoided), and should be closely monitored.2
Urine output should be maintained at a minimum of 40 mL/h; an output below 20 mL/h indicates poor renal function and impending renal failure.
Nephrotoxic drugs should be avoided.
1-Cárdenas et al., Hepatology. 2001;34:671–676.
2-de Franchis . J Hepatol. 2005;43:167–176.
11

NutritionMalnutrition is frequent in cirrhosis and may contribute to an
increased susceptibility to infections and renal dysfunction .
Therefore, feeding should be resumed as soon as a 24 h interval free of rebleeding has been achieved. Enteral nutrition is always preferable due to lower cost and complications when compared to parenteral nutrition. 1
EncephalopathyVariceal bleeding can precipitate hepatic encephalopathy .
Prophylactic treatment of lactulose or lactitol can be given to patients who are liable to encephalopathy.2
1-Córdoba et al., J Hepatol. 2004;41:38–43.
2-de Franchis . J Hepatol. 2005;43:167–176.12

As a general rule, endoscopy should be performed as soon as the patient can tolerate it, i.e. when
haemodynamic stability has been achieved .
The presence of skilled personnel to assist during emergency endoscopy is essential .
It is doubtful whether vigorous gastric lavage prior to endoscopy may improve diagnostic accuracy.
De Franchis& Primignani (2001)
Endoscopy for Variceal Bleeding
13

Variceal hemorrhage is diagnosed on the basis of one of the following findings on endoscopy:
Active bleeding from a varix
“White nipple” overlying a varix
Clots overlying a varix
Varices with no other potential source of bleeding (Diagnosis is certain when blood is present in the stomachand/or endoscopy is done within 24 hours).
14
De Franchis ; Proceedings of the Third Baveno International Consensus Workshop 2001.

Vasopressin:
very powerful vasoconstrictor of the splanchnic circulation. Systemic vasoconstriction severe cardiovascular adverse disorders which reduced by glyceril –trinitrate (NTG).
Pharmacological Treatment
Terlipressin : long acting triglycyl lysine derivative of vasopressin Side effects are less frequent and terlipressin can be used without NTG.
15

Octreotide :
Synthetic octapeptide with pharmacologic actions
similar to the endogenous hormone somatostatin.
Octreotide has a much longer half-life, can be
administered subcutaneously.
Somatostatin:
Natural peptide inducing splanchnic vasoconstriction It lacks most of the adverse effects of vasopressin on systemic circulation
Calès et al.,N Engl J Med. 2001;344:23–28. 16

Somatostatin vasopressinvs
No difference in failure to control bleeding
Side effects are significantly less
Seven RCTs (301 patients)
Silvain 2001 Proceedings of the Third Baveno International Consensus Workshop 17

Three studies including (302) patients
Somatostatin Terlipressinvs
No significant differences were found in:
•Failure to control bleeding
•Rebleeding
•Mortality
•Side effects.
Silvain ,Proceedings of the Third Baveno International Consensus Workshop, 200118

Efficacy of terlipressin in treatment of acute oesophageal variceal haemorrhage.
Terlipressin was associated with a statistically significant reduction in all cause mortality compared to placebo (RR 0.66, 95% CI, 0.49 - 0.88).
No statistically significant difference was demonstrated between terlipressin and either somatostatin or endoscopic treatment
No difference was demonstrated in the number of adverse events between terlipressin and either balloon tamponade or octreotide or vasopressin
Ioannou et al. Cochrane Database Syst Rev. 2003;(1):CD002147. 19

octreotide is a safe and effective
adjunctive therapy after variceal
obliteration techniques.
Octreotide had comparable efficacy to immediate sclerotherapy for control of bleeding
Fewer major complications than vasopressin/terlipressin
a complication profile comparable to no intervention/placebo
Corley , et al. Gastroenterology. 2001 Mar;120(4):946-54.
Octreotide for Management of AVB
20

Vapreotide and lanreotide
Are two other synthetic analogues of somatostatin with comparable affinity for somatostatin receptors.1
They both have been shown to reduce portal pressure in animals but their clinical hemodynamic effect in humans is controversial.2
One study showed that, when used before endotherapy, vapreotide was more effective than placebo in controlling variceal bleeding.3
1-Abraldes & Bosch ,Hepatology. 2002;35:1305–1312. 2-Bosch et al .,Horm Res. 1988;29:99–102.3. Calès et al. N Engl J Med. 2001;344:23–28.
21

Summary of pharmacotherapy
Vasoactive drugs are effective and safe and should be used as first line treatment of AVB as soon as variceal bleeding is suspected.
Available data do not permit firm conclusions regarding the superiority of one drug over the others, although the efficacy and safety profile of either terlipressin or somatostatin seems to be the most adequate, rendering these two drugs as first choice.
Octreotide and vapreotide could also be used if combined with endoscopy.
22

Hemostasis was achieved in all the cases after
recombinant activated factor VII therapy. Rebleeding
and mortality rates were 25% and 50%, respectively.
Romero-Castro , Clin Gastroenterol Hepatol. 2004 Jan;2(1):78-84.
Recombinant-activated factor VII
Tried with 8 patients experiencing severe and active hemorrhage from esophageal varices unresponsive to pharmacologic therapy, endoscopic therapy, or balloon tamponade.
23

Endoscopic Treatment
• Injection Sclerotherapy Tissue adhesives Thrombin and Fibrin Glue
• Ligation Rubber band Endoloop (Snare)
24

Sclerotherapy
25

Four RCTs including (367 patients)
Somatostatin Emergency EVSvs
No significant differences were found in • Failure to control bleeding • Rebleeding • Mortality
Complications were significantly less frequent and less severe
Silvain 2001 Proceedings of the Third Baveno International Consensus Workshop
26

Emergency sclerotherapy Vasoactive drugs VS
•Available evidence does not support emergency
sclerotherapy as the first-line treatment of variceal bleeding in
cirrhosis when compared with vasoactive drugs• Endoscopic therapy might be added only in pharmacologic
treatment failures
D'Amico , Gastroenterology. 2003 May;124(5):1277-91.
A cochrane meta-analysis for 15 trials
Sclerotherapy was not superior to terlipressin, somatostatin, or octreotide for any outcome .
27

Multicenter RCT ( 219 patients)
Terlipressin Sclerotherapy vs
They are equally highly effective therapies achieving : •The initial control of variceal bleeding • Preventing early rebleeding. •Both treatments are safe, but terlipressin is better tolerated. • Terlipressin may represent a first-line treatment in acute variceal bleeding until the administration of elective therapy.
Escorsell et al., Hepatology. 2000 Sep;32(3):471-6.28

Complications of Sclerotherapy
• Retrosternal pain (45%)
• Dysphagia and heart burn (37%)
• Esophageal stricture (3.75%)
• Short term fever (25%)
•Prolonged fever (2.5%)
• Sclerosing ulcers (18%)
• Chest infection (10%)
• Persistent hiccough (3.75%)
• Cachexia (2.5%)
• Pleural effusion (5%)
• Significant bleeding from pucture site (6%)
• Paraplegia (1.5%) El-Wakil (1987) M.D. Thesis Ain Shams University. 29

30

EVS(N=89) EVL(N=90)
Failure to control bleeding 15% (P=0.02) 4%
Emergency endoscopic treatment added to somatostatin in acute variceal bleeding.
Side Effects 28% 14%
Conclusion:variceal ligation instead of sclerotherapy added to somatostatin for the treatment of acute variceal bleeding and significantly improved the efficacy and safety.
Six-week survival probability better
+
Somatostatin infusion (for 5 days).
Villanueva et al.J Hepatol. 2006 Oct;45(4):560-7.
or
31

Detachable Endoloop
Simple, safe and effective method for treatment of bleeding esophageal varices.
The loop consists of heat-treated elliptically shaped nylon thread and a silicone rubber stopper that maintains the tightness of the loop.
The transparent ligation chamber with no elastic bands or strings mounted on detachable miniloop gives a clear endoscopic view.
The problem of elastic band slippage off from the ligated varix does not exist.
32

33

Endoscopic ttt of bleeding osoephageal varices
Detachable endoloop Elastic band ligation
vs
No statistically significant difference was found in :• Recurrence of bleeding • Recurrence of varices • Number of the patients with eradicated varices • Number of sessions needed for eradication of varices
• Better field of vision• Tighter application• Good results with junctional varices• Lack of strain exerted by the device on the endoscope
Naga et al. Gastrointest Endosc. 2004 Jun;59(7):804-9.34

Gastric varices
35

Endoscopic treatment of acute gastric variceal hemorrhage
GVL GVO
No difference in survival No Severe complications
lower GV rebleeding rate.
Tan PC, et al Hepatology. 2006 Apr;43(4):690-7.36

37
World J Gastrointest Endosc. 2015 Apr 16; 7(4): 411–416.Published online 2015 Apr 16. doi: 10.4253/wjge.v7.i4.411PMCID: PMC4400631N-butyl-2-cyanoacrylate, iso-amyl-2-cyanoacrylate and hypertonic glucose with 72% chromated glycerin in gastric varicesReda Elwakil, Mohamed Fawzy Montasser, Sara M Abdelhakam, and Wesam A Ibrahim
Ninety patients with gastric varices presented to Endoscopy Unit of Ain Shams University Hospital were included .
They were randomly allocated into three groups; each group included 30 patients treated with intravariceal sclerosant injections in biweekly sessions till complete obturation of gastric varices; Group I (n-butyl-2-cyanoacrylate; Histoacryl®), Group II (iso-amyl-2-cyanoacrylate; Amcrylate®) and Group III (mixture of 72% chromated glycerin; Scleremo® with glucose solution 25%).
All the procedures were performed electively without active bleeding .

38
HistoacrylAmcrylateScleremo with glucose
χ2P value
Obturation of varices
1st month20 (66.6)16 (53.3)14 (46.6)1.4> 0.05 (NS) 2nd month26 (86.6)24 (80)22 (73.3)
3rd month28 (93.3)28 (93.3)30 (100)
No. of sessions
One10 (33.3)8 (26.6)6 (20)2.5> 0.05 (NS) Two20 (66.6)21 (70)20 (66.6)
Three0 (0)1 (3.3)4 (13.3)
Outcomes of gastric varices for rates of obturation and number of sessions

39
HistoacrylAmcrylateScleremo with glucose
P value
1st session42 cc80 cc126 cc< 0.05 (S)
2nd session20 cc28 cc74 cc< 0.05 (S)
3rd session02 cc10 cc> 0.05 (NS)
Total amount of sclerosant used per session

40
HistoacrylAmcrylateScleremo with glucose
Amount of one ampoule
0.5 cc0.5 cc5.0 cc
Total used amount62 cc110 cc210 cc
No. of all injected ampoules
12422042
Cost of one ampoule
88 EGP (14.6 USD)
44 EGP (7.3 USD)15 EGP (2.5 USD)
Cost of all injected ampoules
10912 EGP (1809 USD)
9680 EGP (1605 USD)
630 EGP (104.5 USD)
Amount of sclerosants and their cost

Human fibrin glue for endoscopic treatment of bleeding gastric varices.
Human thrombin forms a fibrin clot at the needle tip immediately upon injection through a double lumen needle in 10 patients.
Immediate hemostasis was achieved in 70% of patients with a single injection of human thrombin. There was no recorded episode of recurrent bleeding from gastric varices.1
Yang et al reported successful haemostasis in 75% of their patients (N=12) and a low rate of mortality and recurrence of bleeding ( 8% and 25%) respectively.2
1- Heneghan et al. Gastrointest Endosc. 2002 Sep;56(3):422-6 2-Yang et al. Hepatology. 2006 Apr;43(4):690-7.
41

Ectopic varices were reported in different abdominal
parts including enterostomy and surgical adhesions
varices, isolated gastric varices, duodenal varices,
small intestinal varices, colonic varices, sigmoid and
rectal varices, gall bladder varices, common bile
duct varices and rare varices on sites such as the
ovary , the vagina or the dorsal base of the tongue.
Ectopic Varices

Duodenal Varices
43

44

Second endoscopy
Balloon tamponade and esophageal stents
Shunting procedures
TIPS Surgical Shunts
Rescue Therapies
45

•These tubes can be a life-saving maneuver
•Recurrent bleeding with release of the tamponade
occurs in most patients.
•20% complication rate that includes airway
obstruction, aspiration, and esophageal necrosis with
rupture .
•The tubes act as a bridge to help stabilize the patient
until a time when the patient is prepared for either a
repeat endoscopy procedure or a portal pressure
decompression through a radiological or surgical
method.
Kupfer et al. Gastroenterol Clin North Am 2000 Jun; 29(2): 275-307
Balloon Tamponade
46

An alternative to balloon tamponade in the initial control of massive variceal hemorrhages .
Theoretically, they will have the advantage over tamponade of less severe complications and additional protection against early re-bleeding since they can be left in place for up to 14 d.
However, concerns do exist regarding the possibility of downstream migration (especially in patients with concomitant
hiatus hernia) .
Hubmann et al. Endoscopy. 2006;38:896–901.-Zehetner et al. Surg Endosc. 2008;22:2149–2152.106. -Wright et al. Gastrointest Endosc. 2010;71:71–78.
Esophageal SEMS
47

Stents for variceal tamponade
SEMS placement allows continuation of oral nutrition, does not mandate ongoing endotracheal intubation or impair patient mobility, and can be left in situ for as long as 2 weeks to allow
time for recovery and institution of definitive therapy .
An SEMS was recently designed for esophageal variceal tamponade and atraumatic removability (SX-Ella Danis stent; Ella-CS, Hradec Kralove, Czech Republic).
It is a fully covered, nitinol SEMS with variable pitches in stent braiding that conform to esophageal peristalsis in an effort to minimize migration. The stent (13.5 cm long; 30-/25-mm flare/body diameter) is constrained on a 9.4-mmdelivery catheter,
Hubmann et al. Endoscopy 2006;38:896-901.

49
The first Egyptian experience using new self-expandable metal stents in acute esophageal variceal bleeding: Pilot study
Mohamed S Zakaria1, Iman M Hamza1, Mohamed A Mohey1, Rainer G Hubamnn2
1 Department of Endemic Medicine, Cairo University, Cairo, Egypt2 Department of Internal Medicine, Allgemeines Krankenhaus der Stadt Linz, Linz, Austria
2013 | Volume : 19 | Issue : 4 | Page : 177-181
Twenty patients with acute variceal bleeding were included in the study and 16 of them were allocated to receive stent treatment. Results: Stent deployment was successful in 15 of 16 patients (93.75%). Technical errors were reported in 3 (18.75%) patients. Initial control of variceal bleeding was reported in 14 (out of 16) (87.5%) patients. The mean duration of the procedure was 10 (±6) min. Mortality was reported in 4 (25.0%) patients. Conclusion: SEMS is a safe and effective mean to control acute variceal bleeding.

50
SEMS for Variceal Bleeding
Zakaria et al.,Saudi J Gastroenterol.(2013) : 19 (4) :177-181

In a relatively large series(N 34), placement of the SX-Ella Danis stent resulted in hemostasis in all patients with active variceal bleeding in whom conventional therapy failed (banding,
n21; injection sclerotherapy, n 7; BT, n 6) .
The mean stent dwell time was 5 days (range 1-14 days) and allowed the majority of the patients to undergo more definitive
therapy during this time interval .
Stent migration occurredin 21% of patients, confirmed radiographically, but this did not result in bleeding. All migrated stents could be reconstrained and repositioned by using the extractor.
Stents for variceal tamponade
Zehetner et al.,Surg Endosc 2008;22:2149-52.

EUS-guided angiotherapy
Rationale for use. EUS-guided angiotherapy may play a role in the management of bleeding lesions that are refractory to
standard endoscopic and/or angiographic techniques .
EUS can identify feeding vessels that are not visible with a standard endoscope and are inaccessible with conventional
hemostatic techniques .
EUS may enable precise fine-needle injection (FNI) delivery of selected therapy to targeted vessels and assess treatment response with Doppler monitoring.
REPORT ON EMERGING TECHNOLOGY,Emerging technologies for endoscopic hemostasis. GASTROINTESTINAL ENDOSCOPY 75,. 5 : 2012 ,933-7.

EUS-guided angiotherapy
Various agents such as sclerosants,thrombins, and cyanoacrylates (glues) can be administered to targeted vessels by using standard EUSguidedFNI techniques.
The coils that are used currently for angiographic embolizationcan also be delivered to the target vessel through an FNA needle
by using the stylet as a pusher .
For gastric varices, FNI of coils followed by cyanoacrylate mayminimize the risk of glue embolizationt and decrease the amount of glue needed to achieve variceal obliteration. The coil diameter is selected to approximate that of the targeted varix, and coils of 8 to 20 mm in diameter have been delivered to gastric varices
REPORT ON EMERGING TECHNOLOGY,Emerging technologies for endoscopic hemostasis. GASTROINTESTINAL ENDOSCOPY 75,. 5 : 2012 ,933-7.

TIPS
TIPS controls variceal bleeding in more than 90% of
patients . The 30 day rebleeding rate is 25-30% due to Stenosis
or obstruction of the stent. Shunt dysfunction occurs in approximately 50-60% of
patients at 6 months. Chau et al.Gastroenterol1998;114:981-7
TIPS is considered the standard of therapy for bleeding esophagogastric varices that are unresponsive to endoscopic and pharmacologic first-line treatment.
Taniai, et al. Hepatogastroenterology. 2005 May-Jun;52(63):949-53 54

Extended polytetra-fluoroethylene- covered stents significantly improved the stent long term patency and reduced the incidence of encephalopathy when compared
with bare stents .
This may contribute to improve overall outcomes of patients receiving TIPS.1
An early TIPS within 72 h (ideally 24 h) should be considered in patients at high-risk of treatment failure (e.g. Child-Pugh class C <14 points or Child class B with active bleeding) after initial pharmacological and endoscopic therapy .2
1-Bureau et al. Gastroenterology. 2004;126:469–475.2-de Franchis R. Revising consensus in portal hypertension: Report of the Baveno V consensus workshop on methodology of diagnosis
and therapy in portal hypertension. J Hepatol (2010),
TIPS
55

BRTOArai et al. reported that 90.9% of gastric varices
were obliterated and 9.1% was diminished in size
after emergency B-RTO
No rebleeding or recurrence were found during the
mean follow-up period of 1136 days.
Survival rates were 90.9% and 70.7%, respectively,
at 1 year and 3 years.
Conclusion : Emergency B-RTO is an effective
treatment for the prevention of rebleeding from
ruptured gastric varices
Arai et al J Gastroenterol. 2005 Oct;40(10):964-71. 56

ligation--devascularization--splenectomy •They provide excellent results in patients with normal livers
and extrahepatic portal venous obstruction
•Rebleeding is a major complication (40-50%)
Total shunts Incidence of encephalopathy was high( 30%).
Selective shunts • Protection from rebleeding with less post-shunt encephalopathy.• Currently selective shunts are reserved for patients with good
liver function.
Surgical Treatment
57

Suggested Algorithm for Management of AVB
TIUCA & Sztogrin,J Med Life. 2011 November 14; 4(4): 395–39858

59
Non-Variceal Upper GIT Bleeding (NVUGIB)

60
Several validated risk-stratification schemes have been published.
Such a scheme should aid in making clinical decisions, as to both the need for urgent intervention and the prediction of continued or recurrent bleeding in the context of endoscopic therapy.
The latter point is important because alternative treatment strategies should be readily available to prevent recurrent bleeding.
Risk assessment

61
With the data generated from 4,185 admissions in the national UK audit, Rockall et al. derived a scoring scheme based on admission and post-endoscopy scores.
Rockall et al. (1996) Gut 38: 316–321
A total score of three or less is associated with an excellent prognosis, while a score of eight or more is associated with a high risk of death.
The Rockall Score is the most widely used method for risk assessment and it has been validated by independent studies.
Rockall Risk Scoring System
Vreeburg et al. (1999) Gut 44: 331–335,Church and Palmer (2001) Eur J Gastroenterol Hepatol 13: 1149–1152 ,Sanders et al. (2002) Am J Gastroenterol 97: 630–635

variablevariable
ScoreScore00112233
Age (years)Age (years)< 60< 6069-7969-79> 80> 80
ShockShockNo shockNo shockTachycardiaTachycardiahypotensionhypotension
Systolic BPSystolic BP>100>100>100>100<100<100
Pulse rate Pulse rate <100<100>100>100>100>100
Co-morbidity Co-morbidity NilNilCardiac failure, Cardiac failure, IHD, Other IHD, Other major co-major co-morbidity morbidity
Renal failure, Renal failure, liver failure, liver failure,
disseminated disseminated malignancy malignancy
DiagnosisDiagnosisMallory-Weiss Mallory-Weiss tear, without tear, without
SRH, no lesion SRH, no lesion
All other All other diagnosis diagnosis
Malignancy of Malignancy of upper GIT upper GIT
Stigma of Stigma of recent bleed recent bleed
(SRH) (SRH)
None or dark None or dark spotsspots
Blood in UGIT. Blood in UGIT. adherent clot, adherent clot,
visible or visible or spurting vessel. spurting vessel.
Rockall risk scoring system

Rockall Risk Score stratifies the risk of death and re-bleed
SCORE 0 Risk of rebleeding of 5%
SCORE >8 Risk of rebleeding of 40%
SCORE > 8 Mortality rate > 41%
SCORE 0-2 Mortality rate < 1%
Rockall et al. Gut 1996; 38 : 316-21.

In 2004, the American Society of Gastrointestinal Endoscopy recommended the use of PPIs in all patients with upper-gastrointestinal bleeding that was severe enough to require endoscopic therapy, and in patients with suspected peptic ulcer bleeding associated with hemodynamic instability.
The recommendation endorsed systematic use of PPIs in upper-gastrointestinal bleeding.
ASGE Guideline (2004) The role of endoscopy in upper gastrointestinal bleeding. Gastrointest Endosc 60: 497-504
PPI use with NVUGIB

The benefit of pre-emptive IV PPIs in patients with upper-gastrointestinal bleeding is supported by the interim analysis of a large-scale randomized study from Hong Kong.
Patients with symptoms and signs of upper-gastrointestinal bleeding who received intravenous PPIs were found to have less active bleeding on endoscopy, and hence were less likely to require endoscopic therapy.
Lau et al. (2005) placebo controlled randomized trial [abstract]. Gastroenterol 128 (Suppl 2): A50
PPI use with NVUGIB

A high-dose regimen (80 mg bolus followed by 8 mg/h infusion) has been used in most studies .
Two studies suggested that there might be room to reduce the infusion of intravenous omeprazole to the 'regular' dose of 20-80 mg per day.
Cheng HC et al. (2005) Dig Dis Sci 50: 1194-1201 Udd M et al. (2001) Scand J Gastroenterol 36: 1332-1338
The dose of intravenous PPI is debatable
But

67
Since the late 1980s, endoscopic hemostatic therapy has been widely accepted as the first-line therapy for upper-gastrointestinal bleeding.
Numerous clinical trials and two meta-analyses have confirmed the efficacy of endoscopic therapy in this setting.
Most clinical trials demonstrated a reduction in both recurrent bleeding and the need for surgical intervention when endoscopic hemostasis was used.
Sacks et al. (1990) JAMA 264: 494–499 Cook et al. (1992) Gastroenterology 102: 139–148
Endoscopic Management

Forrest classification of bleeding peptic ulcers
GradeUlcer appearance
Ia Spurting haemorrhage
Ib Oozing haemorrhage
IIa Non-bleeding visible vessel
IIb Adherent clot
IIc Flat pigmented spot
III Clean ulcer base
Forrest JA, et al. Lancet 1974;17:394–7

Forrest IIa8%
Forrest III
49%
Forrest IIc
23%
Forrest IIb
13%
Forrest I7%
Prevalence of Forrest grades amongpatients with peptic ulcer bleeding
I – active bleeding
IIa – non-bleeding visible vessel
IIb – adherent clot
IIc – flat pigmented spots
III – clean ulcer base
Grade and ulcer appearance
Lau JY, et al. Endoscopy 1998;30:513–18

Risk of re-bleeding by Forrest grade
Forrest I* Forrest IIa Forrest IIb Forrest IIc Forrest III
55
43
22
10 5
0
20
40
60
80
100
Patients with endoscopic or clinical re-bleeding(%)
Laine L & Peterson WL. N Engl J Med 1994;331:717–27 *Patients did not receive endoscopic therapy

Endoscopic modalities available for management of Bleeding Peptic Ulcer
InjectionThermalMechanical
Adrenaline (1:10,000 or 1:20,000)
Heater probeHemoclips
Fibrin glue Bicap probeBanding
Human thrombin Gold probeEndoloops
SclerosantsArgon plasma coagulation
Staples/sutures
AlcoholLaser therapy

Endoscopic haemostasis
Monotherapy with either epinephrine injection or thermal treatment (e.g. with a heater probe)
or A combination of epinephrine injection plus thermal treatment and/or haemoclips
Epinephrine injection HaemoclipHeater probe

NameCompositionMechanism of action
Regulatory clearance
Hemospray™MineralAbsorption of waterApproved in Europe and Canada1
Concentration of platelets and clotting factors
Under evaluation in United States
Mechanical tamponade
EndoClot™ PHSAbsorbable hemostatic polysaccharides
Absorption of waterApproved in Turkey, Europe, Malaysia and Australia
Concentration of platelets and clotting factorsMechanical tamponade
Ankaferd®Blood Stopper
Mixture of plantsEncapsulated protein network that provides focal points for erythrocyte aggregation
Approved in Turkey
Hemostatic powders currently availableFor non-variceal upper gastrointestinal bleeding.
Marco Bustamante-Balén and Gema Plumé.World J Gastrointest Pathophysiol.2014 August 15; 5(3): 284-292.

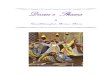
Hemospray™
The Hemospray™ package includes a delivering device with a powder syringe (20 g each), two catheters (7 and 10 F, suitable for a working channel of 2.8 and 3.7 respectively) and a CO2 cartridge .The latter is activated by turning a red knob placed at the base of the handle until it stops .
Blood must be removed as much as possible and the bleeding site must be identified. Then, air is flushed through the accessory channel and the catheter is slowly advanced through it until the catheter tip is visualized .
Care must be taken in not placing the catheter directly in contact with blood or the mucosa to avoid occlusion. It is advisable to maintain a 1-2 cm distance from the bleeding site during the procedure.
TC-325 is ready to be delivered by depressing the red trigger button in 1-2 s pulses. Following the manufacturer´s instructions, no more than 3 devices (60 g) should be applied per patient .
Sung et al. Endoscopy. 2011;43:291-295.

Hemospray™ package. 1: Spray catheters; 2: Powder cartridge; 3: Activation knob; 4: Security valve; 5: Trigger.
World J Gastrointest Pathophysiol.2014 August 15; 5(3): 284-292.

76
Leung Ki EL, Lau JY -Clin Endosc. 2012 Sep; 45(3): 224–229

Primary hemostatic methodAdjuvant therapy
Lesions with a difficult endoscopic access
Failure of conventional methods
Less experienced examiner
Malignant gastrointestinal bleeding
Massive bleeding as a mean to achieve an initial hemostasis
Possible indications for the use of hemostatic powders

A multicenter European trial has been published on the use of Hemospray™ in non-variceal upper GI bleeding.
In this trial, 63 patients with a variety of indications, including ulcers, tumors and post-therapeutic bleeding, were treated with Hemospray™ as either monotherapy or second-line therapy.
Primary hemostasis was achieved in 85% of patients when Hemospray was used as monotherapy. Seven patients rebled by the 7th day, therefore 15 patients (27%) failed to achieve sustained hemostasis.
The 3 patients who rebled from a peptic ulcer had a Forrest Ia lesion. Hemospray was used as a second-line therapy in 8 patients, with two early rebleedings.
Smith et al J Clin Gastroenterol. 2013;Dec 10
Clinical results of hemospray

Devices for mechanical closureThe over-the-scope clip (OTSC)(Ovesco Endoscopy AG, Tübingen, Germany) appears most suitable as a hemostatic tool for selected bleeding lesions.
The OTSC is significantly different in design compared with standard endoscopic clips, with higher compression force and capacity to capture a larger volume of tissue.
A study on an ex vivo porcine model for arterial bleeding showed the OTSC to be significantly more efficacious than traditional clips for vascular closure, which may translate into more durable and effective hemostasis.
Drawbacks: Technically challenging in the setting of acute hemostasis given device complexity, impaired visibility, longer procedure time, and limited maneuverability/access to certain locations.
Naegel et al. Gastrointest Endosc 2012;75:152-9.

80
OTSC

In 1 study (N 27), initial hemostasis was achieved in all patients for a variety of lesions, including peptic ulcer, Mallory-Weiss tear, gastric Dieulafoy lesion, diverticular bleeding, and postbiopsy or postpolypectomy bleeding. Recurrent bleeding occurred in 2 patients (7%).
In another study, the OTSC was applied to various bleeding lesions (duodenal ulcer, n 4; gastric ulcer, n 1; endoscopic mucosectomy site, n 1; colonic diverticulum,n 1) for which conventional clip placement or injection therapy failed. Hemostasis was achieved initially in all patients, but rebleeding (n 2) and perforation (n 1) were observed during the follow-up period.
Devices for mechanical closure Clinical applications
Kirschniak et al.,. Surg Endosc 2011;25:2901-5.Albert et al. Gastrointest Endosc .2011;74:389-97.

In Egypt, AVB represents more than two thirds of the cases UGIB.
Antibiotic prophylaxis must be regarded as integral part of the treatment of AVB and should be started at admission.
It can be currently recommended to combine pharmacological and endoscopic therapies for the initial treatment of AVB.
Vasoactive drugs (preferable somatostatin or terlipressin) should be started as soon as a variceal bleeding is suspected (ideally during transfer to hospital) and maintained afterwards for 2-5 d.
After stabilizing the patient with cautious fluid and blood support, an emergency diagnostic endoscopy should be done and, as soon as a skilled endoscopist is available, an endoscopic variceal treatment (ligation as first choice, sclerotherapy if EVL not feasible) should be performed.
82
Conclusions

Risk assessment is important for cases of NVUGIB.
The use of PPI intravenously is endorsed before endoscopy for the cases of NVUGIB
Several endoscopic modalities proved to be effective in treatment of NVUGIB. Their use depends on availability and local expertise
In case of failure to control the acute bleeding, rescue therapies that include SEMS and EUS guided injection for AVB besides hemostatic powders and OTSC for NVUGIB may be considered.
Shunt therapies (especially TIPS) are very effective at controlling treatment failures after AVB.
Conclusions
83

84
Thank You