Embed Size (px)
Citation preview

P1: JYSfm JWBK439-Banerjee January 15, 2010 19:1 Printer Name: Yet to Come
MANAGING DEMENTIA IN AMULTICULTURAL SOCIETY
Sube Banerjee and Vanessa Lawrence
The David Goldberg CentreThe Institute of Psychiatry
King’s College LondonLondon, UK
A John Wiley & Sons, Ltd., Publication
iii

P1: JYSfm JWBK439-Banerjee January 15, 2010 19:1 Printer Name: Yet to Come
ii
P1: JYSfm JWBK439-Banerjee January 15, 2010 19:1 Printer Name: Yet to Come
MANAGING DEMENTIA IN AMULTICULTURAL SOCIETY
i

P1: JYSfm JWBK439-Banerjee January 15, 2010 19:1 Printer Name: Yet to Come
ii

P1: JYSfm JWBK439-Banerjee January 15, 2010 19:1 Printer Name: Yet to Come
MANAGING DEMENTIA IN AMULTICULTURAL SOCIETY
Sube Banerjee and Vanessa Lawrence
The David Goldberg CentreThe Institute of Psychiatry
King’s College LondonLondon, UK
A John Wiley & Sons, Ltd., Publication
iii
P1: JYSfm JWBK439-Banerjee January 15, 2010 19:1 Printer Name: Yet to Come
This edition first published 2010, C© 2010 John Wiley & Sons, Ltd
Wiley-Blackwell is an imprint of John Wiley & Sons, formed by the merger of Wiley’sglobal Scientific, Technical and Medical business with Blackwell Publishing.
Registered OfficeJohn Wiley & Sons Ltd, The Atrium, Southern Gate, Chichester, West Sussex,PO19 8SQ, UK
Other Editorial Offices9600 Garsington Road, Oxford, OX4 2DQ, UK111 River Street, Hoboken, NJ 07030-5774, USA
For details of our global editorial offices, for customer services and for informationabout how to apply for permission to reuse the copyright material in this book pleasesee our website at www.wiley.com/wiley-blackwell
The right of the author to be identified as the author of this work has been asserted inaccordance with the Copyright, Designs and Patents Act 1988.
All rights reserved. No part of this publication may be reproduced, stored in a retrievalsystem, or transmitted, in any form or by any means, electronic, mechanical,photocopying, recording or otherwise, except as permitted by the UK Copyright,Designs and Patents Act 1988, without the prior permission of the publisher.
Wiley also publishes its books in a variety of electronic formats. Some content thatappears in print may not be available in electronic books.
Designations used by companies to distinguish their products are often claimed astrademarks. All brand names and product names used in this book are trade names,service marks, trademarks or registered trademarks of their respective owners. Thepublisher is not associated with any product or vendor mentioned in this book. Thispublication is designed to provide accurate and authoritative information in regard tothe subject matter covered. It is sold on the understanding that the publisher is notengaged in rendering professional services. If professional advice or other expertassistance is required, the services of a competent professional should be sought.
The contents of this work are intended to further general scientific research,understanding, and discussion only and are not intended and should not be relied uponas recommending or promoting a specific method, diagnosis, or treatment by physiciansfor any particular patient. The publisher and the author make no representations orwarranties with respect to the accuracy or completeness of the contents of this workand specifically disclaim all warranties, including without limitation any impliedwarranties of fitness for a particular purpose. In view of ongoing research, equipmentmodifications, changes in governmental regulations, and the constant flow ofinformation relating to the use of medicines, equipment, and devices, the reader isurged to review and evaluate the information provided in the package insert orinstructions for each medicine, equipment, or device for, among other things, anychanges in the instructions or indication of usage and for added warnings andprecautions. Readers should consult with a specialist where appropriate. The fact thatan organization or Website is referred to in this work as a citation and/or a potentialsource of further information does not mean that the author or the publisher endorsesthe information the organization or Website may provide or recommendations it maymake. Further, readers should be aware that Internet Websites listed in this work mayhave changed or disappeared between when this work was written and when it is read.No warranty may be created or extended by any promotional statements for this work.Neither the publisher nor the author shall be liable for any damages arising herefrom.
Library of Congress Cataloging-in-Publication DataBanerjee, Sube.
Managing dementia in a multicultural society / Sube Banerjee and VanessaLawrence.
p. ; cm.Includes bibliographical references and index.ISBN 978-0-470-72353-1 (pbk.)1. Dementia–Great Britain. 2. Transcultural medical care–Great Britain.
I. Lawrence, Vanessa. II. Title.[DNLM: 1. Dementia–therapy–Great Britain. 2. Cultural Competency–Great
Britain. 3. Cultural Diversity–Great Britain. 4. Dementia–ethnology–Great Britain.5. Health Policy–Great Britain. WM 220 B215m 2010]
RC521.B36 2010362.196′83–dc22
2009049246
ISBN: 978-0-470-72353-1
A catalogue record for this book is available from the British Library.
Typeset in 9.5/11.5pt Times by Aptara Inc., New Delhi, IndiaPrinted in Great Britain by Antony Rowe Ltd., Chippenham, Wilts
First impression 2010
iv
P1: JYSfm JWBK439-Banerjee January 15, 2010 19:1 Printer Name: Yet to Come
CONTENTS
Preface ix
1 Dementia – a brief overview 1What is dementia? 1Historical development of terms 2Scientific terminology and understandings 2Sub-types of dementia 5Alzheimer’s disease 6Vascular dementia 7Dementia with Lewy Bodies 8Frontotemporal dementia 9Clinical presentation of dementia 10
2 The current state of dementia care inthe UK 11Dementia – an emerging priority 11The policy framework 13The National Dementia Strategy for England 17
3 Why a cultural perspective? 19Race, ethnicity and culture 20Black Caribbean and south Asian populations
in the UK 21Structure of black Caribbean and south Asian
populations in the UK 24Epidemiology 25
4 Health beliefs, culture and service use 27The role of health beliefs and illness behaviour 27Social and cultural influences on the
pathway to care 31Cultural differences in health beliefs 33
v
P1: JYSfm JWBK439-Banerjee January 15, 2010 19:1 Printer Name: Yet to Come
vi CONTENTS
5 Whose illness is it anyway? 37Society – policy in relation to ethnicity
and culture 37Black and minority ethnic organisations 38Use of services 42The experience of the person with dementia 43The care giver experience 45
6 The perspective of the personwith dementia 47A neglected perspective 47Self-identity in dementia 50Impact of dementia on the sense of self
of the person with dementia 51Coping strategies and adaptation 52Attitudes towards care 55
7 The perspective of the family carers ofpeople with dementia 57Patterns of care giving 58The impact of care giving 60The stress process 60Ethnicity and culture and the stress process 64Appropriateness of services 67Understanding of dementia across
ethnic groups 68Cultural knowledge, attitudes and beliefs
about formal support 69
8 Qualitative enquiry in the experiences ofpeople with dementia and their familycarers 73New research 73Data collection 74Data analysis 76Results 76One research project, two theories 86Biographical disruption: a common theme 87An anthropological perspective 88
P1: JYSfm JWBK439-Banerjee January 15, 2010 19:1 Printer Name: Yet to Come
CONTENTS vii
9 Implications for practice and policy 91People with dementia 91Increased public awareness of dementia 95Increased public awareness of
services and support 96Supporting people with dementia and carers
in accessing services 98Discussing the diagnosis 99Discussing the future 100Promoting valued elements of life of the
person with dementia 101Repositioning the care giver role 105
10 One size fails all – dementia, agediscrimination and specialist olderpeople’s mental health services 109What does good look like? 110Age discrimination in service commissioning 110Why consider older adults separately from
adults of working age? 111Policy development for older people with
mental disorders 113Liaison services in general hospitals 121In-patient care for older people with
mental disorders 125
References 129Index 153

P1: JYSfm JWBK439-Banerjee January 15, 2010 19:1 Printer Name: Yet to Come
viii
P1: JYSfm JWBK439-Banerjee January 15, 2010 19:1 Printer Name: Yet to Come
PREFACE
Dementia: The 21st CenturyChallenge
There can be no doubt that dementia is one of the great-est societal challenges that we face as we start the 21st cen-tury. Its personal and societal impacts are greater than thoseof health conditions such as cancer and heart disease whichpreoccupied the second half of the last century. It is a chal-lenge that transcends barriers of health, social and familycare. It is also a challenge that acts at international, national,regional and local levels as well as the personal. It is in allways exceptional—in terms of size, cost and current and fu-ture impact. The Dementia UK Report (Knapp et al., 2007)estimates that there are currently 700,000 people with de-mentia in the UK and that this figure will double in just30 years, with the overall cost trebling from the current$17 billion p.a. to over $50 billion (Comas-Herrera et al.,2007).
There is no doubt that dementia is a worldwide phe-nomenon. Reliable projections suggest that there are around24.3 million people with dementia worldwide, which will riseto 81.1 million by 2040 (Ferri et al., 2006) and 106.8 mil-lion by 2050 (Brookmeyer et al., 2007). This is an issue forthe developing world as well as the developed: even now,about half of these cases are in Asia and that proportionwill rise swiftly with time. The profound negative effects ofthis devastating illness on the people with dementia them-selves, their families, and on health and social services arenot in doubt. Dementia is highly stigmatised and universallyfeared: Patrick et al. (1994) reported that it is one of the veryfew illnesses rated as ‘worse than death’.
ix
P1: JYSfm JWBK439-Banerjee January 15, 2010 19:1 Printer Name: Yet to Come
x PREFACE
It is equally the case that there is a widespread under-estimation of the positive things that can be done to helppeople with dementia have a good quality of life. In the lastdecade, it has become clear that there are a multiplicity ofpositive interventions that can promote independence andimprove the quality of life for people with dementia andtheir carers. These can enable individuals and their friendsand families to adapt to the challenges of dementia andsteer a course, in the 7 to 12 years that they might be livingwith dementia, that avoids crises and harm and promoteswell being for all involved.
Unfortunately, the large majority of people with demen-tia and their family carers do not benefit from these positiveinterventions. In fact, systems often seem to have been de-signed to result in the avoidance of diagnosis and the con-sequent denial of care. A fundamental flaw in the currentsystem is that only about a third of people with dementia re-ceive a diagnosis of dementia, usually late in the time courseof the disorder, often at a time of crisis when it is too lateto prevent the harm that has been caused to the person withdementia and their family.
Finally, it appears that if a person with dementia comesfrom a minority group, be that by ethnicity, by having young-onset dementia, by having a learning disability, or by havingsensory impairment, they are even less likely to gain accessto good quality care. The subject of this book is managingdementia in a multicultural society. However, in consider-ing how best to meet the needs of people with dementiafrom minority ethnic groups, the question of what consti-tutes good quality care for all must be addressed first. Eventhe most cursory of reviews of the literature and analysesof services in the UK show that it is not the case that peoplefrom minority ethnic groups get a poor service while those ofwhite European ethnicity receive good quality care. In factboth, unless they are very lucky, get poor quality care, if anycare at all, with the possibility that for those from a minoritygroup the care could be even worse than that given to thewhite majority.
The recently published National Dementia Strategy (De-partment of Health, 2009) presents a high level five-yearplan for quality improvement in dementia care in England.
P1: JYSfm JWBK439-Banerjee January 15, 2010 19:1 Printer Name: Yet to Come
PREFACE xi
Its scope is comprehensive and its intention is to provide apolicy framework for local service development. This bookhas a different focus. It is intended to have a practical rel-evance, weighing the data available in a critical sense, andgenerating ideas for practical solutions to improve the qual-ity of care for those suffering from dementia. We considerwhat it is about dementia that means that services have beenallowed to remain so poor and fragmented. We investigatewhat constitutes good quality care for all, before turning toexamine the particular barriers presented to people with de-mentia from minority groups. Finally, we identify strategiesthat can help all who require help and support in dementiato receive it.
A note on language used� The terms ‘carers’, ‘care givers’, ‘family carers’ and ‘in-
formal carers’ are used interchangeably to refer to un-paid supporters of people with dementia (i.e. family andfriends). When referring to the work of others, the pre-ferred terminology of the original authors is used.
� The expression ‘formal carers’ is used to indicate paid careprofessionals who work with people with dementia. Theterm ‘formal services’ encompasses statutory health andsocial services as well as services provided by the privateor voluntary sector.
� The term ‘minority ethnic’ is used in preference to ‘ethnicminority’ as it places the emphasis on the minority statusand recognises that everyone has an ethnicity.
� Throughout the book, the categories ‘black Caribbean’,‘south Asian’ and ‘white British’ are used to denote thethree main ethnic groups considered. The terms ‘blackCaribbean’ and ‘south Asian’ refer to people who de-fine themselves as originating from the Caribbean andthe Indian sub-continent respectively. The category ‘southAsian’ includes individuals who originated in the Indiansub-continent and migrated to the UK via East Africa.
Sube BanerjeeVanessa Lawrence

P1: JYSfm JWBK439-Banerjee January 15, 2010 19:1 Printer Name: Yet to Come
xii
P1: VGF/OSW P2: TIXc01 JWBK439-Banerjee January 15, 2010 20:36 Printer Name: Yet to Come
1DEMENTIA – A BRIEF
OVERVIEW
WHAT IS DEMENTIA?
What do we mean by dementia? One of the particular chal-lenges in seeking to understand medical problems, but par-ticularly those associated with the mind and brain, is thatthe technical language used to define specific illnesses mayalso be part of the common lay vocabulary. The problemis that the meanings and definitions attached are seldom thesame. So schizophrenia, a devastating disorder characterisedby hallucinations, delusions, anxiety and fear, becomes asynonym for doing something contradictory. Depression be-comes an understandable normal sadness rather than a pro-found illness robbing people of their ability to enjoy life,interfering with eating, sleeping, energy and concentrationand resulting in excess mortality including death by suicide.In this, dementia becomes a state of frenzied lack of controlor one of total lack of function and total dependency, ratherthan a slow neurodegenerative disorder where people in thefirst few years of the illness are almost indistinguishable fromthose without it.
Managing Dementia in a Multicultural Society Sube Banerjee and Vanessa LawrenceC© 2010 John Wiley & Sons, Ltd
1
P1: VGF/OSW P2: TIXc01 JWBK439-Banerjee January 15, 2010 20:36 Printer Name: Yet to Come
2 MANAGING DEMENTIA IN A MULTICULTURAL SOCIETY
HISTORICAL DEVELOPMENT OF TERMS
So what of dementia? Etymologically the root of the worddementia is the Latin word ‘demens’ meaning insane or be-ing out of one’s mind. There are references to disorders ofmemory and function occurring in later life from ancientEgyptian sources (Boller and Forbes, 1998). A connectionbetween old age and error of judgement (and therefore cog-nitive impairment) was identified by the Greek jurist Solonaround 600BC, along with pain, drugs, violence and ‘the per-suasion of a woman’.
The roots of the use of the word in English and thedevelopment of the concept are well traced by Huppertand colleagues in their book Dementia and Normal Ageing(Huppert et al., 1994). They trace the word dementia backto the mid seventeenth century with an entry in Blancard’sPhysical Dictionary ascribing a generic meaning of ‘extinc-tion of the imagination and judgement’. Prior to this, in thefifteenth century, the word demency was in use as a generalterm for mental illness. By the mid eighteenth century it ap-pears that the word takes on a medical meaning denotinga form of mental disorder different from ‘mania’ which in-cluded schizophrenia and bipolar behaviours, and ‘delirium’which included acute states of confusion. What is less clearis the growth of its lay meaning (that is, ‘wild and irrational’)but this was in use by the end of the nineteenth century andhas continued since.
SCIENTIFIC TERMINOLOGY ANDUNDERSTANDINGS
Spending time on use of language prepares for understand-ing the next set of terminology. ‘Alzheimer’s Disease’ is in-creasingly used in a lay sense, as a synonym for dementia asa whole, rather than as a technical term for a specific sub-type of dementia. The reasons for this start at the turn of thenineteenth and twentieth centuries when the aetiology andpathology of the dementia were engaging some of the finestscientific minds of the day, as they are again now.
One of the most common causes of dementia at this timewas end-stage syphilis which resulted in widespread brain
P1: VGF/OSW P2: TIXc01 JWBK439-Banerjee January 15, 2010 20:36 Printer Name: Yet to Come
DEMENTIA – A BRIEF OVERVIEW 3
cell death and dementia. Using microscopy on post mortembrain tissue and new developments in technology of stainingcells and cellular components, the dementias that were dueto syphilis were differentiated from a group considered tobe caused by cerebrovascular disease such as small strokes.This was termed ‘senile dementia’ since it tended to be morecommon in older people than syphilitic dementia (who gen-erally died before they could become old).
Following this, other pathology was observed in the se-nile dementia group, the first plaques were identified (nowknown to be made of a protein called amyloid) and it wassuggested that these were a pathological feature of seniledementia. The eponymous Alois Alzheimer’s advance wasto use a silver stain on brain tissue taken from a 51-year-old woman who had died after developing an unusual andrapidly progressing dementia. He described a novel pathol-ogy, neurofibrilary tangles, in the bodies of nerve cells thatseemed to have destroyed the internal architecture of thecells themselves, resulting in cell death. These tangles werepresent along with large numbers of the plaques mentionedabove. Alzheimer suggested that this might be a disease thatwas separate from senile dementia and a further 11 casesof young-onset dementia with plaques and tangles on neu-ropathological examination post mortem were reported inthe next five years.
This led his boss, the pre-eminent psychiatrist of theday, Emil Kraepelin to include ‘Alzheimer’s Disease’ inhis definitive textbook of 1910. Having a disease namedafter you was a great honour at the time and it has beensuggested that the rapidity of Kraepelin coining the eponymAlzheimer’s Disease was motivated to ensure that someoneworking in his own academic department at Munich gotthis honour, rather than rivals at Prague such as Fischerand Pick who had been involved in the first identificationof the plaques (Amaducci et al., 1986). So, the first meaningof Alzheimer’s Disease was as a young-onset dementiaseparate from that which affected older people. However,from the beginning it was acknowledged that there wasan intrinsic unlikelihood that something magic happensat the age of 65 that differentiates, at a neuropathologicallevel, between clinical states that are very similar (except
P1: VGF/OSW P2: TIXc01 JWBK439-Banerjee January 15, 2010 20:36 Printer Name: Yet to Come
4 MANAGING DEMENTIA IN A MULTICULTURAL SOCIETY
in terms of age) and where the cases happening in later lifeoutnumbered the young-onset cases by at least 100 to one,if the syphilitic cases were removed.
Careful study over the twentieth century has shown usthat the cardinal pathological features of young-onset de-mentia (the original Alzheimer’s Disease) and late-onset de-mentia (the original senile dementia) are precisely the same.Both have general atrophy of brain tissue with amyloidplaques and neurofibrilary tangles on pathological study. Inboth, certain parts of the brain appear to be affected earlyand prominently including the fronto-temporal lobes (thesides of the brain) and the hippocampus (a nucleus at thebase of the brain important in the neural circuits involvedin memory with a complicated curved shape that sixteenth-century anatomists thought looked like a seahorse, hencethe name). The same clinical course is observed and, by the1960s, it was accepted that they were the same disease. Withthe characteristic elegance of the age, the term ‘Senile De-mentia of the Alzheimer Type’ was coined.
In the past 25 years there has been a tremendousamount of work trying to elucidate the causes of demen-tia, the pathological pathways leading to dementia, andways of treating dementia. The consistent finding that thereare deficiencies in cholinergic pathways in the brain hasled to the first generation of treatments for dementia, thecholinesterase inhibitors, whose action is to increase theamount of the neurotransmitter acetylcholine available inthe brain. Terminology has also evolved so that there is nowwidespread consensus that Alzheimer’s Disease is clinicallythe same in younger or older patients so that the term ‘se-nile’ has been dropped from all sensible descriptions of thedisorder. There are, however, issues that make living withdementia different in your fifties than in your eighties. Theprovision of good quality care for those who develop demen-tia relatively early in their lives is therefore a legitimate areaof concern. The terminology used to identify this group usedhere is ‘young-onset dementia’. While this may be somewhatgrammatically cumbersome it makes the point that thesepeople develop dementia while relatively young (usually de-fined as under 65) but does not confuse age of onset with theseverity of dementia at any particular time.
P1: VGF/OSW P2: TIXc01 JWBK439-Banerjee January 15, 2010 20:36 Printer Name: Yet to Come
DEMENTIA – A BRIEF OVERVIEW 5
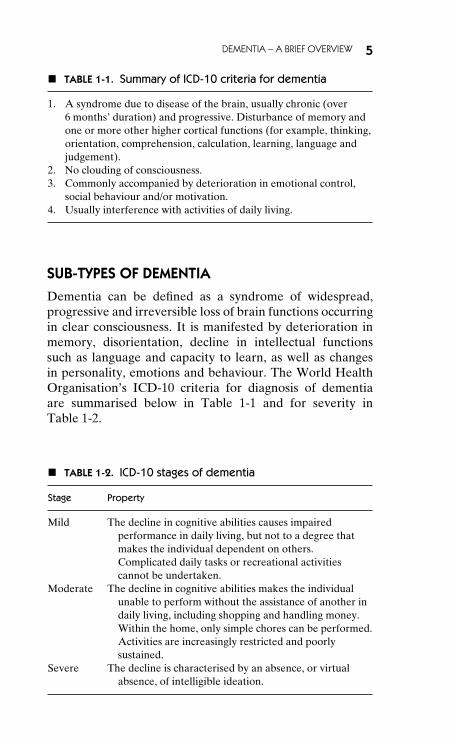
� TABLE 1-1. Summary of ICD-10 criteria for dementia
1. A syndrome due to disease of the brain, usually chronic (over6 months’ duration) and progressive. Disturbance of memory andone or more other higher cortical functions (for example, thinking,orientation, comprehension, calculation, learning, language andjudgement).
2. No clouding of consciousness.3. Commonly accompanied by deterioration in emotional control,
social behaviour and/or motivation.4. Usually interference with activities of daily living.
SUB-TYPES OF DEMENTIA
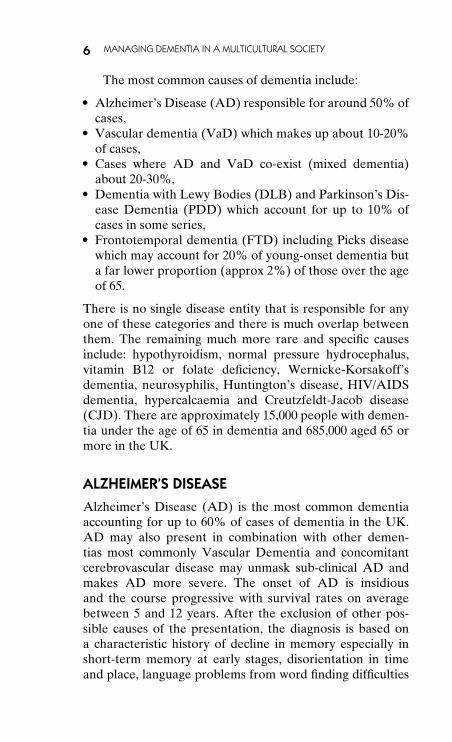
Dementia can be defined as a syndrome of widespread,progressive and irreversible loss of brain functions occurringin clear consciousness. It is manifested by deterioration inmemory, disorientation, decline in intellectual functionssuch as language and capacity to learn, as well as changesin personality, emotions and behaviour. The World HealthOrganisation’s ICD-10 criteria for diagnosis of dementiaare summarised below in Table 1-1 and for severity inTable 1-2.
� TABLE 1-2. ICD-10 stages of dementia
Stage Property
Mild The decline in cognitive abilities causes impairedperformance in daily living, but not to a degree thatmakes the individual dependent on others.Complicated daily tasks or recreational activitiescannot be undertaken.
Moderate The decline in cognitive abilities makes the individualunable to perform without the assistance of another indaily living, including shopping and handling money.Within the home, only simple chores can be performed.Activities are increasingly restricted and poorlysustained.
Severe The decline is characterised by an absence, or virtualabsence, of intelligible ideation.
P1: VGF/OSW P2: TIXc01 JWBK439-Banerjee January 15, 2010 20:36 Printer Name: Yet to Come
6 MANAGING DEMENTIA IN A MULTICULTURAL SOCIETY
The most common causes of dementia include:� Alzheimer’s Disease (AD) responsible for around 50% of
cases,� Vascular dementia (VaD) which makes up about 10-20%
of cases,� Cases where AD and VaD co-exist (mixed dementia)
about 20-30%,� Dementia with Lewy Bodies (DLB) and Parkinson’s Dis-
ease Dementia (PDD) which account for up to 10% ofcases in some series,
� Frontotemporal dementia (FTD) including Picks diseasewhich may account for 20% of young-onset dementia buta far lower proportion (approx 2%) of those over the ageof 65.
There is no single disease entity that is responsible for anyone of these categories and there is much overlap betweenthem. The remaining much more rare and specific causesinclude: hypothyroidism, normal pressure hydrocephalus,vitamin B12 or folate deficiency, Wernicke-Korsakoff’sdementia, neurosyphilis, Huntington’s disease, HIV/AIDSdementia, hypercalcaemia and Creutzfeldt-Jacob disease(CJD). There are approximately 15,000 people with demen-tia under the age of 65 in dementia and 685,000 aged 65 ormore in the UK.
ALZHEIMER’S DISEASE
Alzheimer’s Disease (AD) is the most common dementiaaccounting for up to 60% of cases of dementia in the UK.AD may also present in combination with other demen-tias most commonly Vascular Dementia and concomitantcerebrovascular disease may unmask sub-clinical AD andmakes AD more severe. The onset of AD is insidiousand the course progressive with survival rates on averagebetween 5 and 12 years. After the exclusion of other pos-sible causes of the presentation, the diagnosis is based ona characteristic history of decline in memory especially inshort-term memory at early stages, disorientation in timeand place, language problems from word finding difficulties
P1: VGF/OSW P2: TIXc01 JWBK439-Banerjee January 15, 2010 20:36 Printer Name: Yet to Come
DEMENTIA – A BRIEF OVERVIEW 7
to dysphasia (difficulty understanding or formulating lan-guage), dyscalculia (difficulty with numbers), impairedability to carry out activities of daily living such as mealpreparation and dressing and impaired skills such as drivingto dyspraxia (difficulty with complex tasks) and variousmanifestations of misidentification to agnosia (difficulty inidentifying people or things). Delusions, hallucinations anddepression also occur in a significant proportion of cases.There are some rare hereditable causes with simple geneticsthat occur early, a very small proportion of those with veryyoung-onset AD have autosomal dominant inherited forms.The family tree will usually show a tragically large numberof affected people, on average half in each and everygeneration. The genes causing most inherited dementias,including early onset familial AD, have been identified.Susceptibility genes alter risk of all other AD in conjunctionwith environmental risk factors. Only one such gene hasbeen unequivocally identified to date, APOE, the ε4 allele,which modestly increases risk. However, the use of this genein answer to the common concern about inheriting diseaseis not advised due to low predictive power.
VASCULAR DEMENTIA
Vascular Dementia (VaD) is the second most commoncause of dementia in the UK and may be responsible forup to 20% of cases. It results from a variety of condi-tions that can cause vascular damage to the brain althoughcommonly atherosclerotic thrombo-embolic disease (nar-rowed arteries with small blood clots forming inside them).It commonly coexists with AD in that one third of VaDhave significant AD pathology and 60–90% of AD caseshave cerebrovascular pathology. It classically has a fluc-tuating course with patchy neuropsychological deficits de-pending on the pattern of underlying brain tissue damage.Survival is also variable and depends on the extent of un-derlying disease and its response to treatment as well asthe control of the familiar cardiovascular risk factors of:hypertension; cigarette smoking; obesity; hypercholestero-laemia; diabetes mellitus and atrial fibrillation. It is from
P1: VGF/OSW P2: TIXc01 JWBK439-Banerjee January 15, 2010 20:36 Printer Name: Yet to Come
8 MANAGING DEMENTIA IN A MULTICULTURAL SOCIETY
this association that the possibility of preventing an elementof dementia by promoting good cardiovascular health hascome. In the National Dementia Strategy this is summarisedin the line: ‘what’s good for your heart is good for yourhead’.
Although VaD historically has been characterised by astepwise progression, it may have a clinical course that is in-distinguishable from AD. Features like sudden onset, emo-tional lability (rapidly changing mood or being easily upset)and night time confusion may be suggestive of a vascularcause, but diagnosis depends on evidence of dementia witha temporal relationship to vascular damage. Focal neuro-logical symptoms and signs, along with evidence of cerebraldamage on CNS imaging can be very useful in supporting thediagnosis. History of other end organ damage e.g. myocar-dial infarction can raise suspicions and longstanding cardiacdisorders are associated with cognitive impairment.
DEMENTIA WITH LEWY BODIES
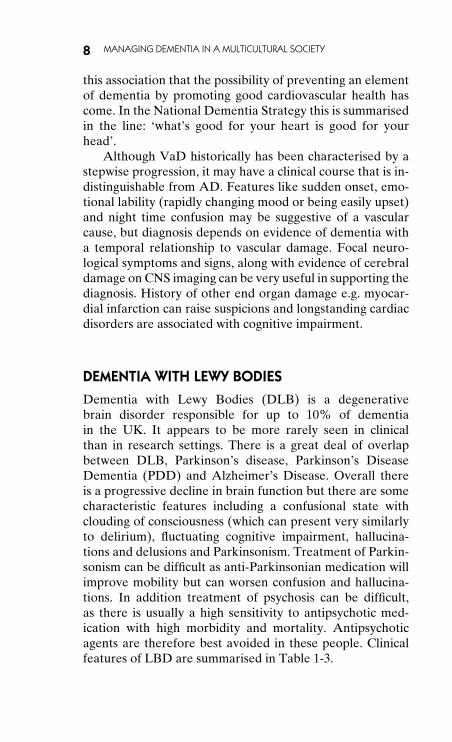
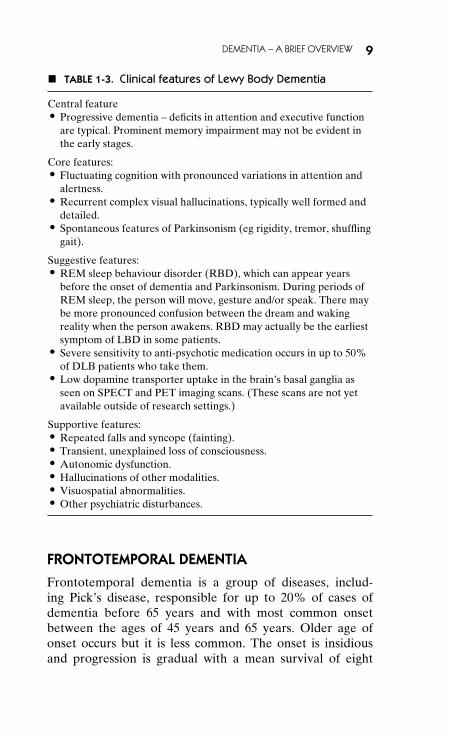
Dementia with Lewy Bodies (DLB) is a degenerativebrain disorder responsible for up to 10% of dementiain the UK. It appears to be more rarely seen in clinicalthan in research settings. There is a great deal of overlapbetween DLB, Parkinson’s disease, Parkinson’s DiseaseDementia (PDD) and Alzheimer’s Disease. Overall thereis a progressive decline in brain function but there are somecharacteristic features including a confusional state withclouding of consciousness (which can present very similarlyto delirium), fluctuating cognitive impairment, hallucina-tions and delusions and Parkinsonism. Treatment of Parkin-sonism can be difficult as anti-Parkinsonian medication willimprove mobility but can worsen confusion and hallucina-tions. In addition treatment of psychosis can be difficult,as there is usually a high sensitivity to antipsychotic med-ication with high morbidity and mortality. Antipsychoticagents are therefore best avoided in these people. Clinicalfeatures of LBD are summarised in Table 1-3.
P1: VGF/OSW P2: TIXc01 JWBK439-Banerjee January 15, 2010 20:36 Printer Name: Yet to Come
DEMENTIA – A BRIEF OVERVIEW 9
� TABLE 1-3. Clinical features of Lewy Body Dementia
Central feature� Progressive dementia – deficits in attention and executive function
are typical. Prominent memory impairment may not be evident inthe early stages.
Core features:� Fluctuating cognition with pronounced variations in attention and
alertness.� Recurrent complex visual hallucinations, typically well formed and
detailed.� Spontaneous features of Parkinsonism (eg rigidity, tremor, shuffling
gait).
Suggestive features:� REM sleep behaviour disorder (RBD), which can appear years
before the onset of dementia and Parkinsonism. During periods ofREM sleep, the person will move, gesture and/or speak. There maybe more pronounced confusion between the dream and wakingreality when the person awakens. RBD may actually be the earliestsymptom of LBD in some patients.
� Severe sensitivity to anti-psychotic medication occurs in up to 50%of DLB patients who take them.
� Low dopamine transporter uptake in the brain’s basal ganglia asseen on SPECT and PET imaging scans. (These scans are not yetavailable outside of research settings.)
Supportive features:� Repeated falls and syncope (fainting).� Transient, unexplained loss of consciousness.� Autonomic dysfunction.� Hallucinations of other modalities.� Visuospatial abnormalities.� Other psychiatric disturbances.
FRONTOTEMPORAL DEMENTIA
Frontotemporal dementia is a group of diseases, includ-ing Pick’s disease, responsible for up to 20% of cases ofdementia before 65 years and with most common onsetbetween the ages of 45 years and 65 years. Older age ofonset occurs but it is less common. The onset is insidiousand progression is gradual with a mean survival of eight
P1: VGF/OSW P2: TIXc01 JWBK439-Banerjee January 15, 2010 20:36 Printer Name: Yet to Come
10 MANAGING DEMENTIA IN A MULTICULTURAL SOCIETY
years. Early features include changes in personality andbehaviour, usually seen as a decline in social interpersonalskills and emotional blunting. There may be increased men-tal rigidity and a decline in personal hygiene with decline inmemory, spatial orientation and dysphasia occurring later inthe illness. Other features include disinhibition, aggression,hyperorality, distractibility and stereotyped behaviour withearly loss of insight. Diagnosis is by a suggestive historyand can be supported by neuropsychological testing. Brainimaging may show frontal and/or temporal abnormality.
CLINICAL PRESENTATION OF DEMENTIA
Individual cases of dementia can vary greatly in terms oftheir clinical presentation depending on the type and stageof dementia, the presence of behavioural and psychologi-cal symptoms, the presence of co-morbid physical illness,personality and the social context. There are, however, fea-tures that are commonly reported. People with dementiamay complain of forgetfulness or a decline in intellectualfunctioning but may also report mood disturbance such asdepression. However, they may also have no concerns aboutthemselves and so it is often carers who report changes inmemory, personality and behaviour, such as poor personalhygiene and deteriorating social interaction.
Occasionally, both patients and their closest contacts areunaware of or unconcerned about apparent disorientation,poor memory and deterioration in function that may seemobvious to the outside observer. This may be because thechanges have been gradual, and are attributed to normalaging, or it may be the result of denial of a highly anxietyprovoking problem. Some cases present with dangerous be-haviour, such as wandering outside exposing themselves tothe risk of accidents or the weather, or the misuse of cookersand heaters with the potential for fires and explosions.
P1: VGF/OSW P2: TIXc02 JWBK439-Banerjee January 14, 2010 14:22 Printer Name: Yet to Come
2THE CURRENT STATE OF
DEMENTIA CARE INTHE UK
DEMENTIA – AN EMERGING PRIORITY
So dementia is one of the most severe and devastating ill-nesses we face. It is also very common, with approximately700 000 people with dementia in England (Knapp et al.,2007). It is predominantly a disorder of later life, but at least15 000 people under the age of 65 have the illness. Its inci-dence (the number of new cases per year) and prevalence(the number of cases at any one time) rises exponentiallywith age, and it affects men and women from all social andethnic groups. Around 15 000 people from minority ethnicgroups have some form of dementia, but this number is setto rise sharply as these populations age.
The Dementia UK report estimates the cost of dementiafor the UK as a whole to be £17 billion per year, and projectsthat the number of people with dementia will double to 1.4million in the next 30 years. In the same brief period, thecosts associated with dementia are set to treble to over £50billion per year (Comas-Herrera et al., 2007). Dementia hasa devastating impact on those with the disorder, but it alsohas profound, negative effects on the family members whoprovide the majority of all care. Family carers are often oldand frail themselves, and suffer high levels of care burden,
Managing Dementia in a Multicultural Society Sube Banerjee and Vanessa LawrenceC© 2010 John Wiley & Sons, Ltd
11
P1: VGF/OSW P2: TIXc02 JWBK439-Banerjee January 14, 2010 14:22 Printer Name: Yet to Come
12 MANAGING DEMENTIA IN A MULTICULTURAL SOCIETY
depression and physical illness, and a diminished qualityof life.
Dementia is a terminal disorder, but people can livewith it for 7–12 years after diagnosis. The challenge we haveis how to enable people with dementia and their carersto live as well as possible, maximising their quality of life.The National Audit Office has identified problems in thecurrent systems of health and social care for dementia.Its report Improving services and support for people withdementia estimates that approximately two-thirds of peoplewith dementia do not receive a formal diagnosis – or havecontact with specialist services – at any time in their illness(National Audit Office, 2007). It is also of concern that suchdiagnosis and contact, when made, often only occurs late inthe illness and when the person with dementia is in crisis –so the opportunities for harm prevention and maximisingquality of life are limited. If dementia is not diagnosed, theperson with the illness and their family carers are denied thepossibility of making choices themselves. They are unableto plan for their future and don’t have access to the help,support and treatments (social and psychological, as well aspharmacological) that are available.
Contrary to popular belief, a great deal can be done toprovide help for people with dementia and their carers (thishas been well summarised in the NICE/SCIE clinical guide-line on dementia). While there are undoubtedly potentialnegative reactions to diagnoses (Iliffe et al., 2003), the bal-ance is very much in favour of making these early – theearlier they are made, the better (National Institute of Clin-ical Evidence and Social Care Institute of Excellence, 2006).There is clear evidence that providing people with a di-agnosis decreases their levels of depression and anxiety(Carpenter et al., 2008).
There is a real problem in service planning in terms ofthe lack of routinely collected data on dementia servicesin the UK. The data available is limited, but UK activityin terms of the diagnosis and treatment of people withdementia is generally low with a 30-fold variation in activitybetween the lowest and highest functioning PCTs. Thereare also significant variations between areas that are notexplained by the numbers of people with dementia in those
P1: VGF/OSW P2: TIXc02 JWBK439-Banerjee January 14, 2010 14:22 Printer Name: Yet to Come
THE CURRENT STATE OF DEMENTIA CARE IN THE UK 13
areas. International comparisons suggest that the UK isin the bottom third of European performance (Waldemaret al., 2007), with less than half the activity of France,Sweden, Ireland and Spain. The National Audit Office’sreport recommended that services need to be redesigned sothat dementia is diagnosed early and well, and people withdementia and their family carers can receive the treatment,care and support that will enable them to live as well aspossible with dementia. Transforming the quality of lifeof people with dementia is also about empowering thosepeople to make choices about what they want, and enablingthem to care for themselves. Services need to put peoplewith dementia and their carers at the heart of planning theirlives. In addition to adequate services being in place, peopleneed to be informed and supported to make choices. Thereare clear suggestions that this is not happening in the UK atthe present time.
THE POLICY FRAMEWORK
The realisation that all is not well in the health and socialcare provided for people with dementia has developedclarity and momentum over the past decades. Services forpeople with dementia are complex, and include primaryhealth care, specialist services in mental health (e.g. old-agepsychiatry), care provided in general hospitals (e.g. geri-atrics and neurology), as well as social care commissionedand provided by both local authorities, the voluntary andindependent sectors, and for-profit providers of home careand care homes. There are examples of excellent dementiacare provided by all of these agencies, and also problematiccare within each. The last decade has seen a growing ac-knowledgement of the challenge posed by dementia and theneed for service improvement. Details of relevant reportsand policy include:
� The Audit Commission’s report Forget me not: Mentalhealth services for older people (Audit Commission,2000) – published in 2000 key findings included:� Only a half of GPs considered it important to look ac-
tively for signs of dementia and to make an early diag-nosis.
P1: VGF/OSW P2: TIXc02 JWBK439-Banerjee January 14, 2010 14:22 Printer Name: Yet to Come
14 MANAGING DEMENTIA IN A MULTICULTURAL SOCIETY
� Less than half of GPs felt that they had received suffi-cient training in how to diagnose dementia.
� There was a lack of clear information, counselling, ad-vocacy and support for people with dementia and theirfamily carers.
� There was insufficient supply of specialist home care.� There were poor assessments and treatment, with little
joint health and social care planning and working.� They found little improvement when reviewing change
two years later (Audit Commission, 2002).� The National Service Framework for Older People (De-
partment of Health, 2001) – published in 2001, it includeda chapter on mental health and older people. This in-cluded a consideration of dementia, advocating:� Early diagnosis and intervention.� That the NHS and local authorities should review ar-
rangements for health promotion, early detection anddiagnosis, assessment, care and treatment planning, andaccess to specialist services.
� The provision of ‘integrated’ and ‘comprehensive’ ser-vices.
� Reviewing progress, this appears to have had little pos-itive impact on services for people with dementia andtheir families.
� The Care Services Improvement Partnership’s (CSIP) Ev-erybody’s business: Integrated mental health services forolder adults: a service development guide (Care ServicesImprovement Partnership, 2005) – published in 2005, thisset out the essentials for a service that works for older peo-ple’s mental health in general including:� Memory assessment services to enable the early diagno-
sis of dementia for all.� Integrated community mental health teams whose role
includes the management of people with dementia withcomplex behavioural and psychological symptoms.
� The National Institute for Health and Clinical Excellence(NICE) and Social Care Institute for Excellence (SCIE)Dementia: Supporting people with dementia and their car-ers in health and social care, a joint clinical guideline on themanagement of dementia (National Institute of Clinical
P1: VGF/OSW P2: TIXc02 JWBK439-Banerjee January 14, 2010 14:22 Printer Name: Yet to Come
THE CURRENT STATE OF DEMENTIA CARE IN THE UK 15
Evidence and Social Care Institute of Excellence, 2006) –published in 2006, key recommendations included:� Integrated working across all agencies.� Provision of memory assessment services as a point of
referral for diagnosis of dementia.� Assessment, support and treatment (where needed) for
carers.� Assessment and treatment of non-cognitive symptoms
and behaviour that challenges.� Dementia care training for all staff working with older
people.� Improvement of care for people with dementia in gen-
eral hospitals.� The Alzheimer’s Society Dementia UK report (Knapp
et al., 2007) – published in February 2007 the report’s keyfindings included:� The number of people with dementia in the UK –
700 000.� The projected number of people with dementia in the
UK – doubling in 30 years.� The costs of dementia £17 billion per year.� Low level of diagnosis and management of dementia in
the UK.� High variation in activity between areas in the UK.� The recommendation that dementia should be made an
explicit national health and social care priority.� The need to improve the quality of services provided for
people with dementia and their carers.� The National Audit Office’s (NAO) report Improving ser-
vices and support for people with dementia (National Au-dit Office, 2007) – published in July 2007, this report wasprofoundly critical of the quality of care received by peo-ple with dementia and their families. Its findings included:� The size and availability of specialist community mental
health teams was extremely variable.� The confidence of GPs in spotting the symptoms of de-
mentia was poor and lower than it had been in 2000.� Deficiencies in carer support.� Services are not currently delivering value for money to
taxpayers or people with dementia and their families.
P1: VGF/OSW P2: TIXc02 JWBK439-Banerjee January 14, 2010 14:22 Printer Name: Yet to Come
16 MANAGING DEMENTIA IN A MULTICULTURAL SOCIETY
� That too few people are being diagnosed or being diag-nosed early enough.
� That early diagnosis and intervention is needed to im-prove quality of life.
� Services in the community, care homes and at the endof life are not delivering consistently or cost-effectivelyagainst the objective of supporting people to liveindependently as long as possible in the place of theirchoosing.
� The need for a ‘spend to save’ approach, with upfrontinvestment in services, for early diagnosis and interven-tion and improved specialist services, community ser-vices and in general hospitals resulting in long-term costsavings from prevention of transition into care homesand decreased length of hospital stay.
� The subsequent report of the Public Accounts CommitteeImproving services and support for people with dementia(Public Accounts Committee, 2008) – published in 2008,the NAO report was submitted for consideration by theHouse of Commons Public Accounts Committee (PAC),and at the committee’s public hearing on 15 October 2007the NHS Chief Executive and others from the Depart-ment of Health were questioned on the NAO’s criticismsand recommendations.� That dementia should be made a high priority for the
NHS and Social Care.� The need for explicit national ownership and leader-
ship.� Early diagnosis.� Improving public attitudes and understanding.� Co-ordinated care.� All improvements to benefit carers too.� Improvements in care in care homes.� Improvements in care in general hospitals.
The Government’s response to the PAC report is avail-able at www.official-documents.gov.uk/document/cm73/7323/7323.pdf. The response accepted virtually all theconclusions and recommendations of the committee,
P1: VGF/OSW P2: TIXc02 JWBK439-Banerjee January 14, 2010 14:22 Printer Name: Yet to Come
THE CURRENT STATE OF DEMENTIA CARE IN THE UK 17
emphasising that their findings would be fully addressed inthe National Dementia Strategy.
The size of the population affected by dementia and thepervasiveness of the condition in health and social care set-tings mean that the development of policy and services forpeople with dementia and their families is also affected bythe wider policy context. This currently includes initiatives,guidance and policy statements such as: Our NHS, Our Fu-ture; Putting People First: A shared vision and commitment tothe transformation of adult social care; the Carers’ Strategy;and the National End of Life Care Strategy. Getting servicesright for people with dementia would make a positive con-tribution to all of these.
In response to this increasing clarity on the nature ofthe health and social care challenge posed, the Governmenthas made improving dementia care a national priority, acommitment confirmed in the 2008/9 NHS OperatingFramework. A one-year programme to develop a NationalDementia Strategy and implementation plan was announcedby Ivan Lewis, the then Parliamentary Under-Secretary ofState for Care Services, in August 2007.
THE NATIONAL DEMENTIA STRATEGYFOR ENGLAND
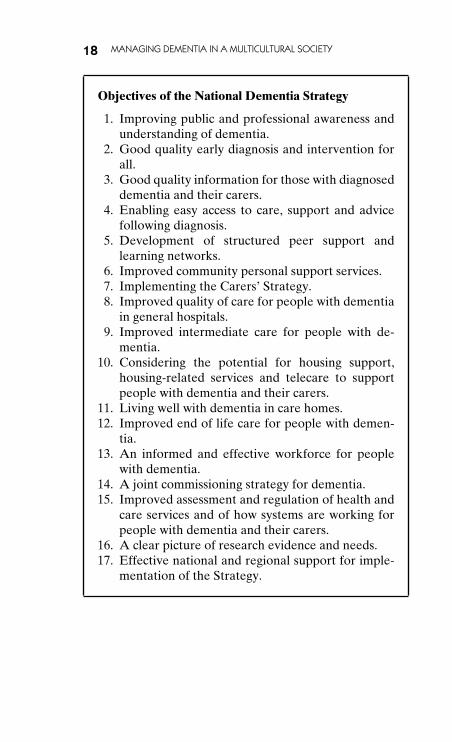
Work to develop a National Dementia Strategy includeda two-phase formal consultation and this was published inFebruary 2009 (Department of Health, 2009). The Strategyis an ambitious five-year plan which, if implemented, wouldresult in the positive transformation of health and social carefor dementia in England. It presents a comprehensive criti-cal analysis of the current systems of providing health andsocial care for people with dementia and their carers andsets out the actions needed to enable people to live well withdementia. It is structured into three broad themes (improv-ing public and professional awareness and understanding;providing early specialist diagnosis and support for all withdementia; and improving the quality of care from diagnosisright through to the end of life) and 17 specific objectives:
P1: VGF/OSW P2: TIXc02 JWBK439-Banerjee January 14, 2010 14:22 Printer Name: Yet to Come
18 MANAGING DEMENTIA IN A MULTICULTURAL SOCIETY
Objectives of the National Dementia Strategy
1. Improving public and professional awareness andunderstanding of dementia.
2. Good quality early diagnosis and intervention forall.
3. Good quality information for those with diagnoseddementia and their carers.
4. Enabling easy access to care, support and advicefollowing diagnosis.
5. Development of structured peer support andlearning networks.
6. Improved community personal support services.7. Implementing the Carers’ Strategy.8. Improved quality of care for people with dementia
in general hospitals.9. Improved intermediate care for people with de-
mentia.10. Considering the potential for housing support,
housing-related services and telecare to supportpeople with dementia and their carers.
11. Living well with dementia in care homes.12. Improved end of life care for people with demen-
tia.13. An informed and effective workforce for people
with dementia.14. A joint commissioning strategy for dementia.15. Improved assessment and regulation of health and
care services and of how systems are working forpeople with dementia and their carers.
16. A clear picture of research evidence and needs.17. Effective national and regional support for imple-
mentation of the Strategy.
P1: SQX/OSW P2: TIX
c03 JWBK439-Banerjee January 14, 2010 14:26 Printer Name: Yet to Come
3WHY A CULTURAL
PERSPECTIVE?
It is well documented that the UK population is ageing, andthe proportion of older people within black and minorityethnic groups is expected to increase dramatically over thecoming decade, as first generation migrants from the 1950s,1960s and 1970s reach retirement age (Lowdell, 2000). Ac-cordingly, while the number of people with dementia is pro-jected to double overall over the next 30 years (Knapp andPrince, 2007), there will be a much steeper increase in thenumbers of people from minority ethnic groups with demen-tia. This is likely to have a profound impact on the livesof older people and their families within minority ethniccommunities, yet there remains a fundamental knowledgegap regarding how dementia is understood, experienced andmanaged among black and minority ethnic groups in the UKand elsewhere (Milne, 2005).
Epidemiological research on ‘ethnicity’ and ‘health’ hasexamined risk factors for physical and mental illnesses,and ethnic differences in morbidity, mortality and patternsof service use. This has simultaneously demonstrated highlevels of need among ethnic minority groups (e.g. blackCaribbean and certain sub-groups of the south Asian pop-ulation appear at increased risk of Vascular dementia com-pared with the white British population (Richards, 1999))
Managing Dementia in a Multicultural Society Sube Banerjee and Vanessa LawrenceC© 2010 John Wiley & Sons, Ltd
19
P1: SQX/OSW P2: TIX
c03 JWBK439-Banerjee January 14, 2010 14:26 Printer Name: Yet to Come
20 MANAGING DEMENTIA IN A MULTICULTURAL SOCIETY
and low levels of service use in comparison with the ma-jority group (Adelman and Livingston, 2008). Evidencesuggests that ethnic elders with dementia are less likelyto receive a diagnosis of dementia (Yeo and Gallagher-Thompson, 1997) or access specialist mental health care(Rait and Burns, 1998) or social care services (Social Ser-vices Directorate, 2001). This highlights the importance ofgenerating services that meet the needs of those from ethnicminorities.
RACE, ETHNICITY AND CULTURE
Much of the research examining differential service useamong minority ethnic groups has used the terms ‘race’and ‘ethnicity’ interchangeably. However, these are separateconstructs that require elaboration, alongside the term ‘cul-ture’, which is equally pertinent to this discussion. Smedleyand Smedley (2005) pointed out that there is no one def-inition of race, but those that have been offered generallyrest upon phenotypic (what you look like) and social charac-teristics. Racial groups have been construed as biologicallydiscrete entities that are marked by particular physical char-acteristics. The term race remains widely recognised in theUS, where it signifies a social division that encompasses adimension akin to socio-economic status. However, the con-cept of race has lost credibility in the UK. When the termis used it tends to be accompanied by inverted commas thatacknowledge that it is a socially constructed categorisation,used to represent social groups that are purported to holddistinctive cultural behaviours (Ahmad, 2008). Academicshave rejected racial distinctions on the basis that they are notgenetically discrete, not reliably measurable and not scien-tifically meaningful. Smedley and Smedley (2005) conclude,‘Race essentializes and stereotypes people, their social sta-tuses, their social behaviours, and their social ranking’.
In contrast to race, ethnicity is not fixed, but open andsubject to change. Ethnicity operates as a marker of iden-tity, referring to an individual’s affiliation to a culturally dis-tinct community. People who share the same language, placeof origin, religion, sense of history, traditions, values, may
P1: SQX/OSW P2: TIX
c03 JWBK439-Banerjee January 14, 2010 14:26 Printer Name: Yet to Come
WHY A CULTURAL PERSPECTIVE? 21
constitute an ethnic group. It is self-defined and has no nec-essary connection to an individual’s physical characteristicsor genetic heritage (Smedley and Smedley, 2005).
Culture can be defined as a set of shared symbols, be-liefs, and customs that shape individual and group behaviour(Goodenough, 1999). In research, culture is often used asan overarching label for contextual variables (social, histor-ical, political, etc) that are thought to influence particularbehaviours (Segall et al., 1998). One example of this is theconcept of individualism-collectivism as a cultural character-istic, which enables predictions about behaviour to be made.Ahmad (1996) argues that both culture and ethnicity shouldbe treated as a context, which interacts with other social andstructural contexts of people’s lives.
BLACK CARIBBEAN AND SOUTH ASIANPOPULATIONS IN THE UK
The two largest minority ethnic groups in terms of numbersof older adults in the UK are those of Black Caribbean andsouth Asian ethnicity and we will focus on these groupshere in this book. The English speaking countries of theCaribbean comprise 12 independent countries of whichJamaica is the largest, followed by Trinidad and Tobago andGuyana. The smallest islands (e.g. Montserrat, Anguilla,Turks and Caicos, the British Virgin Islands and the CaymanIslands) have populations of only a few thousand. Guilford(1994) reports that over 95% of these populations are ofAfrican origin, brought to the Caribbean as slaves. Religionis often considered one of most important aspects of thetraditional Caribbean community. Catholicism is the mostwidely practiced religion, although Protestant beliefs tend todominate the English speaking islands. A small proportiontypically found on French and Spanish speaking islandspractice Creole religions. English is the most widely spokenlanguage of the Caribbean, although other official languagesinclude Spanish, French and Dutch. There are also numer-ous regional dialects spoken solely by the island natives.
Geographically, South Asia includes the countries ofIndia, Pakistan, Sri Lanka, Bangladesh, Nepal, Bhutan, and
P1: SQX/OSW P2: TIX
c03 JWBK439-Banerjee January 14, 2010 14:26 Printer Name: Yet to Come
22 MANAGING DEMENTIA IN A MULTICULTURAL SOCIETY
the Maldives, although the term ‘South Asian’ is often ap-plied to those who have migrated from India and Pakistan.Hindu and English are the official languages of India. Over80% of the Indian population practice Hinduism, and likethe 12% who practice Islam, this represents a way of life.Hindus hold the concept of unity of life, such that all lifeforms are interdependent and life continues after death (i.e.reincarnation). Good deeds in this life lead to re-birth in ahigher life form. Due to the colonisation of part of Indiaby the Portuguese and some evangelism, 2% of the popu-lation practice Christianity. Sikhism was founded in Punjabin Northern India and is practiced by 2% of the Indian pop-ulation, although the significant roles that they have playedin the armed forces and public affairs have afforded IndianSikhs greater prominence in society.
As recently as 1939, the population of ‘Asians’ and‘blacks’ living permanently in the UK was as low as 7000(Ghosh and Khan, 2005). High levels of migration started inGreat Britain in the 1950s as post-war labour shortages cre-ated job opportunities for Commonwealth citizens. A largeproportion of migrants came from south Asia and the WestIndies. For many, the arrival of 417 Jamaicans on the EmpireWindrush in 1948 symbolised the start of mass colonial im-migration to Britain. The most rapid period of migration toBritain from the Caribbean islands occurred between 1955and the Commonwealth Immigration Act of 1962, which re-stricted entry to the UK to those with government issuedemployment vouchers. This had the paradoxical effect of in-creasing the levels of immigration in the rush to beat the ban(Peach, 1988). Records show that in 1966 around 60% of theCaribbean population in Britain was from Jamaica (Rose,1969).
During this original wave of migration large numbers ofmen in their twenties and thirties arrived from India andPakistan. Many came from rural and economically unde-veloped areas where there was poor health care and loweducation standards. The majority did not intend to settlepermanently, but viewed migration as an interlude beforereturning to their families in their country of origin. Thus,wives and children often did not follow until the1970s, and it
P1: SQX/OSW P2: TIX
c03 JWBK439-Banerjee January 14, 2010 14:26 Printer Name: Yet to Come
WHY A CULTURAL PERSPECTIVE? 23
is commonly argued that the ‘myth’ of returning home con-tributed to restricted contact with the wider society (Bhachu,1985). In the 1970s, migrants sought refuge from hostilesituations in East Africa, including Uganda, Kenya andTanzania. As the British East African colonies gained in-dependence in the 1960s, those of south Asian backgroundwere faced with the choice of opting for local or British cit-izenship and many chose the latter in case the political sit-uation worsened. During the era of the British Raj, semi-skilled Sikhs from the Punjab were transported to BritishEast Africa to help build the railways. In addition, Indianmigrants had entered East Africa in the early part of thetwentieth century to work as part of the civil service andhad come to belong to the middle class business commu-nity. A large proportion was fluent in English, well educatedand enjoyed a good standard of living. In contrast to othersouth Asian immigrants, East Africans typically viewed theirmigration to Britain as permanent and arrived in completefamily units, often consisting of three generations.
The majority of early migrants were employed in lowpaid and menial jobs with many directly recruited towork within transport systems, mills and factories, althoughskilled workers played an important role in the creation andgrowth of the new National Health Service. In 1971 it wasestimated that 11% of doctors working in the UK were bornin the Indian subcontinent (Robinson and Carey, 2000). Ahigh level of black Caribbean women without children alsomigrated to the UK to fill vacancies in the caring professions(Ahmad and Atkin, 1996), although often at the State En-rolled rather than State Registered nursing level, with lowerstatus and pay. This has been identified as one of the firstlabour movements in which Caribbean women migrated inan almost equal proportion to Caribbean men and it offeredthe opportunity for women to participate in wage genera-tion in Britain independently of male migrants (Chamber-lain, 1998).
Many of those who migrated to the UK in the 1950s tothe 1980s suffered from racial prejudice and discriminationand did not have access to the same employment and hous-ing opportunities as the majority white community (Modood
P1: SQX/OSW P2: TIX
c03 JWBK439-Banerjee January 14, 2010 14:26 Printer Name: Yet to Come
24 MANAGING DEMENTIA IN A MULTICULTURAL SOCIETY
et al., 1994). These ethnic groups brought with them a dis-tinct ethnic identity, with a variety of languages, religions,customs and traditions. Despite the pervasive assumptionthat immigrants would assimilate to the British way of life(Ahmad and Bradby, 2007), there is still clear evidence ofdifferences in cultural practices, particularly with respect tofamily and social patterns.
STRUCTURE OF BLACK CARIBBEAN AND SOUTHASIAN POPULATIONS IN THE UK
It is largely due to differential migration patterns that theage structure among the Caribbean and Indian popula-tion in the UK is older than within other minority ethnicgroups (Ballard and Kalra, 1994). The 1991 Census revealedthat the median ages of individuals from minority ethnicgroups were highest in the South East and Greater Londonwhere older black Caribbean and Indian ethnic groups pre-dominated (Owen, 1993). Census data from 1991 (Officeof Population Censuses and Surveys, 1993) indicated thatthe white ethnic group formed the majority of older peo-ple in London, accounting for over 95% of over 65s. Thebiggest single minority groups in Greater London were In-dian and black Caribbean, each accounting for approxi-mately a third of London’s non-white elders (Lowdell et al.,2000). Within London, the black Caribbean population hastraditionally populated inner city areas (Peach, 1996). Peachnotes many black Caribbeans originally settled in ClaphamJunction/Brixton (the borough of Lambeth has one of thehighest Caribbean populations) and there is evidence of aprogressive outward diffusion, with the Caribbean popu-lation of Wandsworth-Lambeth-Southwark moving south-wards into Croydon. Many Indian migrants settled in theWest Midlands and East Midlands. The London ward withthe highest Indian population is Northcote in Ealing, whereover two-thirds of the population is Indian (Peach, 1996).However, the 1991 Census reported a unique shift in thegeographical distribution of the Indian population, with adramatic increase in the number of Indians living in OuterLondon and a decrease in the number of Indian residents in
P1: SQX/OSW P2: TIX
c03 JWBK439-Banerjee January 14, 2010 14:26 Printer Name: Yet to Come
WHY A CULTURAL PERSPECTIVE? 25
inner boroughs. The Census showed that two thirds of theEast African population live in the South East, with almosthalf residing in Outer London boroughs. However, this pop-ulation remains more difficult to describe, as they were clas-sified as part of the heterogeneous ‘Other-Asian’ category.
In terms of social class, the 1991 Census indicated thata higher proportion of Indians and ‘Asian Others’ were en-gaged in non-manual occupations than the white majority,and almost twice the number were represented in SocialClass 1 (Professional employment). The employment pat-terns of black Caribbean adults mirrored the white major-ity in every social class category, apart from Social Class 1where they were underrepresented (Ballard and Kalra,1994). Data from the 2001 Census demonstrated that the av-erage number of persons per household is higher among theIndian than the black Caribbean or white British population(Office for National Statistics). Black Caribbean householdsare striking in the high proportion of adults and older adultswho live alone, which is greater than in the white majoritypopulation (Office for National Statistics, 2003).
EPIDEMIOLOGY
There is evidence to suggest that within the UK the preva-lence of dementia is significantly higher among older peopleborn in Africa or the Caribbean than in the white British ma-jority population (Livingston et al., 2001). This may be be-cause black Caribbean older adults have higher rates of car-diovascular disease (Wild and McKeigue, 1997) than the in-digenous white population. Population based studies in theUnited States have typically found higher rates of Vascu-lar dementia and Alzheimer’s Disease in African Americansthan the white American majority (Yeo, 2006). Larger cross-sectional surveys are needed to confirm the increased rate ofdementia in the British, African and Caribbean populations(Adelman et al., 2009). Overall, the evidence base regardingthe prevalence of psychiatric disorders among south Asianimmigrants in the UK is highly limited. One population-based study found dementia in 4% of immigrants fromthe Indian sub-continent living in Bradford (Bhatnagar and
P1: SQX/OSW P2: TIX
c03 JWBK439-Banerjee January 14, 2010 14:26 Printer Name: Yet to Come
26 MANAGING DEMENTIA IN A MULTICULTURAL SOCIETY
Frank, 1997), while prevalence rates of 0% and 20% werefound among Gujarati elders in the age bands 65–74 and 75+respectively (Lindesay et al., 1997).
Census data reveals that the proportion of black and mi-nority ethnic individuals over the age of 65 increased from3% in the 1991, to over 8% in 2001 (Shah et al., 2005). There-fore, it appears inevitable that the numbers of people withdementia in minority ethnic groups, and the challenges thatthis presents to health and social services in the UK will rise(McCracken et al., 1997).
There is limited research into the socio cultural contextof dementia, which is epitomised by the dearth of researchwithin minority ethnic groups (Downs, 2000). It has alsobeen argued that a preoccupation with discrepancies in ser-vice use between population groups has overshadowed thedevelopment of evidence-based guidelines for culturally ap-propriate care (Mackenzie et al., 2006). There is some evi-dence to suggest that the burden of care giving differs acrossethnic groups and that concepts of dementia vary acrossgenerations and cultures (Dilworth-Anderson et al., 2002).However, further research is needed to explore how cultureand ethnicity influence the way people with dementia andcarers experience and respond to the condition (Yeo andGallagher-Thompson, 2006).
P1: PXY/OSW P2: TIXc04 JWBK439-Banerjee January 14, 2010 14:27 Printer Name: Yet to Come
4HEALTH BELIEFS,
CULTURE ANDSERVICE USE
THE ROLE OF HEALTH BELIEFS ANDILLNESS BEHAVIOUR
How are we to understand the internal processes that lead toone person or one group seeking help and accepting it, andanother person or group with the same problems not seek-ing help or seeking help but refusing it? In an attempt tounderstand this, illness behaviour has long been the focus ofsociological and anthropological research. First introducedas a term by Mechanic in the 1960s, ‘illness behaviour’ hasbeen defined as the way in which individuals and significantothers perceive, evaluate and respond to the symptoms ofillnesses (Mechanic, 1982). As such, the study of illness be-haviour can be useful in understanding utilisation of healthcare services and other sources of support.
At this point it may be useful to clarify terms again. Weneed to note the distinction between ‘disease’, which refersto a malfunctioning of biological and/or physiological pro-cesses, and ‘illness’, which refers to the psychosocial experi-ence and meaning of experienced disease (Kleinman, 1980).Thus, unlike disease, illness is essentially a subjective experi-ence, which involves processes of attention, perception, cog-nitions and values.
Managing Dementia in a Multicultural Society Sube Banerjee and Vanessa LawrenceC© 2010 John Wiley & Sons, Ltd
27
P1: PXY/OSW P2: TIXc04 JWBK439-Banerjee January 14, 2010 14:27 Printer Name: Yet to Come
28 MANAGING DEMENTIA IN A MULTICULTURAL SOCIETY
The literature on illness behaviour has been divided intomicrosociological and macrosociological models (Young,2004). Microsociological models within social psychol-ogy and socio-cultural research focus on the individual.Macrosociological models have looked at the role of eco-nomics, the proximity of services and socio-demographicvariables among others in determining access to health ser-vices (Young, 2004). Much of the research has fallen intothe latter category of macrosociological models and has ex-amined the effect of socio-economic status, education, age,gender, religion and ethnicity on health service utilisation.Using epidemiological methods and large national surveys,socio-demographic characteristics have been correlated withthe outcomes of interest. However, this approach has beencriticised for failing to explicate individual experiences orthe causal mechanisms behind the observed associations(Young, 2004, Morgan et al., 2004). We have consideredmacrosociolgical factors earlier, here we focus on dominantsocial psychological models that have prioritised the role ofhealth beliefs. Within this illness behaviour is studied as adecision making process. The health belief model (HBM)and the self-regulation model (SRM) are of promising util-ity. These models consider health beliefs broadly in relationto how individuals respond to symptoms.
In the 1950s Rosenstock and colleagues formulated thehealth belief model (HBM) in response to growing concernabout the failure of people to accept disease prevention orscreening tests (Rosenstock, 1974). Although initially devel-oped to predict individual health behaviour, i.e. those ac-tions taken by ‘healthy’ individuals to prevent disease, it hassince proved a valuable resource in understanding illness be-haviour (Kirscht, 1974). Significantly, the model stresses theimportance of the individual’s subjective interpretation. Itstates that an individual’s readiness to take a health actionis a function of the perceived threat (i.e. perceived suscepti-bility and perceived severity) and perceived benefit (i.e. per-ceived probability that the threat will be reduced minus theperceived cost of action) and that cues to action, such as theperception of symptoms or health education programmes,will trigger health behaviour.
P1: PXY/OSW P2: TIXc04 JWBK439-Banerjee January 14, 2010 14:27 Printer Name: Yet to Come
HEALTH BELIEFS, CULTURE AND SERVICE USE 29
Werner (2003) used the health belief model to examinethe factors associated with seeking a cognitive examinationin the presence of memory problems. Only cues to actionand perceived benefits were found to be significant predic-tors of intentions. The perceived benefits were affected bythe dual belief that cognitive assessment and possible diag-nosis would have significant psychological costs and that ap-propriate treatments did not exist. The extent to which ‘sig-nificant others’ would support them in seeking a cognitiveexamination also predicted intentions. Critics of the HBMhave stated that component variables are poorly defined,inconsistently operationalised and lack specification withregards to the relationship between them (Wallston andWallston, 1984). Werner (2003) pointed out that the HBMpositions health decisions as static and that future studiesmight benefit from adopting a more dynamic approach, suchas the self-regulatory model (Leventhal et al., 2003).
For the last 20 years the self-regulation model (SRM),also known as the common sense model of self-regulation(Leventhal et al., 2003), has focused on cognitive factors thatinfluence illness coping behaviours and outcomes. It hypoth-esises that individuals create mental representations of theirillness, relating to its cause, consequence, illness identity (i.e.beliefs about the illness label and knowledge/ experience ofsymptoms), course, and control/cure. These, in conjunctionwith the individual’s emotional state, determine coping andhelp seeking behaviour. The adaptive function of this be-haviour is then appraised, which feeds back into the illnessrepresentation and coping strategies. The model states thatthe meaning assigned to the symptoms reflects an individ-ual’s past experience with the illness, societal expectationsand information from family, friends, the media and med-ical practitioners. Central to this theory is the assumptionthat perceived threat motivates active health behaviour.
A meta-analysis of empirical studies using the SRMfound significant relationships between illness cognition andcoping behaviour. Viewing the illness as uncontrollable,chronic and highly symptomatic was positively associatedwith avoidance/denial (i.e. cognitive or behavioural attemptsto ignore or avoid the existence of problems or illness) and
P1: PXY/OSW P2: TIXc04 JWBK439-Banerjee January 14, 2010 14:27 Printer Name: Yet to Come
30 MANAGING DEMENTIA IN A MULTICULTURAL SOCIETY
expressing emotions (i.e. coping by venting or expressing re-actions to illness). Viewing the illness as controllable waspositively associated with problem focused coping strategies(i.e. active attempts to directly address the illness/problem),seeking social support and strategies that help them re-appraise the importance of their condition. Correlationshave also been found between illness representations and ill-ness outcomes. Higher perceived consequences, a strongerillness identity, and in particular, perception of symptoms,was associated with psychological distress (Hagger andOrbell, 2003). Loban et al. (2003) concluded that the SRMmay have a particular utility for understanding severe men-tal illnesses and this could include dementia.
Diseases can elicit different expectations and responsesat different points in the lifespan; there is a propensityamong older adults to misattribute symptoms to ageing anddowngrade the seriousness of symptoms via comparisonswith peers (Leventhal and Crouch, 1997). The majority ofstudies that have adopted the SRM have focused on ill-ness representations in chronic illnesses including: diabetes,heart disease and hypertension. Few studies have exam-ined illness representations among older adults and fewerstill dementia. In an exploratory qualitative study, Clareet al. (2006) elicited the five key dimensions of illness rep-resentation (i.e. relating to cause, consequence, illness iden-tity, course, control/cure) in people with mild dementia,suggesting the applicability of the SRM within this popula-tion. A study of illness representations of Alzheimer’s Dis-ease among first degree relatives suggested that a lack ofawareness of available medications and treatment (i.e. be-liefs relating to control/cure) and the attribution of symp-toms to normal ageing (i.e. beliefs relating to cause) coulddiscourage family members from pursuing help (Robertsand Connell, 2000).
The 1980 publication, Mental Illness in the Community(Goldberg and Huxley, 1980) provided one of the first in-vestigations into the routes taken by people seeking help fora mental illness. The model confirmed that only a small pro-portion of those with psychiatric conditions in the commu-nity access specialist mental health services. They proposed
P1: PXY/OSW P2: TIXc04 JWBK439-Banerjee January 14, 2010 14:27 Printer Name: Yet to Come
HEALTH BELIEFS, CULTURE AND SERVICE USE 31
a hierarchical model of levels and filters that determinewhether and at what stage people access specialist care.They argued that people’s beliefs and attributions about ill-nesses are fundamental to the way they respond to symp-toms; they inform individuals’ decisions to seek help and themanner in which they present to services. It provides a usefulframework for understanding the help-seeking process andthe different stages at which attitudes and beliefs might actas a barrier to care. The identification of need and decisionto seek help, the presentation of the condition and the abilityof the physician to identify psychiatric morbidity/offer ap-propriate treatment, and the individual’s decision to accepttreatment/referral all have the potential to act as barrier offacilitators to services (Commander et al., 1997). So, access-ing formal health and social care for dementia is likely torest upon the conceptualisation of dementia held by the in-dividual and the family, and beliefs surrounding appropriatehelp seeking and accepting behaviour.
SOCIAL AND CULTURAL INFLUENCES ON THEPATHWAY TO CARE
Social networks comprising family and friends play an im-portant role in determining illness behaviour. For exam-ple, strong social networks with a negative view of formalhealth care may contribute to the under utilisation of ser-vices (McKinlay, 1973). Pescosolido (1992) described thepathway to care as a dynamic social process, arguing thatthe meaning of symptoms is constructed within a social net-work and that health decisions are negotiated with signifi-cant others. Consequently, families and peers modulate ac-cess to care and the level of satisfaction with the care thatthey receive. Inevitably, the progressive impairment of cog-nitive function that characterises dementia will affect therelative influence of the person with dementia and the fam-ily carer in the help-seeking process. Family members playan increasingly pivotal role as the dementia progresses. Theperson with dementia may become unable to make decisionsat which point the knowledge, attitudes and beliefs of infor-mal carers may become decisive. However, it is important
P1: PXY/OSW P2: TIXc04 JWBK439-Banerjee January 14, 2010 14:27 Printer Name: Yet to Come
32 MANAGING DEMENTIA IN A MULTICULTURAL SOCIETY
to note that throughout the course of the illness all healthdecisions are made within a network of relationships. Thisis consistent with anthropological research that views illnessbehaviour as a product of a complex interplay of individual,social and cultural factors (Kleinman, 1980).
Models of illness behaviour have also recognised thatsocial-cultural factors, including ethnicity, influence theidentification of and response to illness (Mechanic, 1968).In the HBM, ethnicity is considered one of a number of de-mographic variables that influences the perceived threat ofthe condition and the perceived benefits and costs of tak-ing action (Becker, 1974), while the SRM considers culturalbackground relevant to the meaning ascribed to symptoms(Leventhal et al., 1982). Goldberg (1999) acknowledged thatculture and ethnicity are likely to be influential at multiplestages on the ‘pathway to care’. Bhui and Bhugra (2002)identified the role of cultural beliefs in determining theappraisal and expression of distress in the community andprimary care, and expanded the pathway to care model toinclude traditional healers, voluntary organisations, and re-ligious worship, arguing that this better reflected the helpseeking narratives of black and south Asian people.
Kleinman’s Health Care System model (1980), informedby an anthropological perspective, has been central inadvancing understanding of how illness responses andinteractions with health care are informed by the culturalframework in which individuals make sense of their expe-rience. Kleinman coined the term, ‘explanatory model’ todescribe the notions that individuals hold about a specificillness and its treatments. Loban (2003) argued that ex-planatory models incorporate similar key beliefs to thoseidentified in the self-regulatory model. Kleinman positedthat explanatory models are embedded in larger cognitivesystems of illness beliefs, norms and experiences, which arein turn anchored in the social and cultural context. Althoughexplanatory models draw upon belief systems, Kleinmanargues that they are formed in response to particular illnessepisodes and need to be analysed in that concrete setting.Health care systems are conceived as cultural systemsthat integrate all aspects of society concerned with health.
P1: PXY/OSW P2: TIXc04 JWBK439-Banerjee January 14, 2010 14:27 Printer Name: Yet to Come
HEALTH BELIEFS, CULTURE AND SERVICE USE 33
These are experienced and responded to in three differentarenas:
� the popular sector,� the folk sector and� the professional sector.
The popular sector comprises individuals, families, socialnetworks, and community beliefs and activities. Kleinmanargued that therapeutic measures will often remain withinthe family, but if this is deemed insufficient, professionals orfolk practitioners may be consulted.
The folk sector comprises healers and practitioners ofcomplementary and alternative medicine who are not partof the established medical system.
The professional sector mainly comprises Western med-ical organisations, although indigenous medical systemsare sometimes included (e.g. in India, Indian Systems ofMedicine exists alongside the Western biomedical model).
How people interact with the local health care systemwill in part depend upon the explanatory models that existwithin these different sectors. Conflict in explanatory mod-els may impede health care. Thus, as argued by Bhugra(1999), a thorough exposition of help seeking behaviour re-quires an understanding of cognitive processes within the so-cial and cultural context.
CULTURAL DIFFERENCES IN HEALTH BELIEFS
People coming to the UK from the Caribbean and southAsia will have experienced different health care systems,which include ‘patterns of belief about the causes of ill-ness; norms governing choice and evaluation of treatment’(Kleinman, 1980). Religious missions played an importantpart in introducing Western medicine to the Caribbeanthrough installing hospitals in urban centres and taking med-ical services to remote indigenous settlements (Pedersonand Baruffati, 1985). Much of the Caribbean now has anetwork of modern medical care. Primary care is largelyprovided through government run health centres, which arepredominantly staffed by nurses and attended by doctors for
P1: PXY/OSW P2: TIXc04 JWBK439-Banerjee January 14, 2010 14:27 Printer Name: Yet to Come
34 MANAGING DEMENTIA IN A MULTICULTURAL SOCIETY
specific clinical sessions (e.g. diabetes clinics, chronic diseaseclinics). Many doctors also run private practices that are of-ten considered to provide a higher quality of care, and ‘doc-tor shopping’, whereby patients attend a mixture of publicand private clinics for the same and different complaints, iscommon (Gulliford, 1994).
Cultural beliefs about mental illness have been shownto influence help seeking behaviour in the Caribbean. In-deed, the concept of ‘mental illness’ has traditionally beenregarded as a misnomer, as such conditions were consid-ered to be beyond the knowledge and treatments of doctors(Littlewood, 1988). Traditional beliefs include the attribu-tion of mental illness to ‘Obeah’ (sorcery or black magic),the intrusion of spirits, excessive worries or an untreatabledisturbance of the head, which place the condition out-side the domain of traditional medical practice (Littlewood,1988, Kiev, 1963). The few studies to examine these con-ceptualisations in the UK suggest that they exist in anattenuated form and that psychiatric illnesses remain stig-matised among the Caribbean community (Cinnirella andLoewenthal, 1999, Kiev, 1963, Lawrence et al., 2006a,Marwaha and Livingston, 2002). The centrality of religiousbeliefs and practice in the cause, prevention and treatmentof mental illness has been strongly expressed in this group(Cinnirella and Loewenthal, 1999). However, others havesuggested that Caribbean countries share the beliefs andpractices of the Western medical model and that this co-exists with the perceived value of religious and spiritual re-sources (Peluso and Blay, 2004). A cross-cultural study ofhelp seeking for depression in minority ethnic groups in theUK found that black Caribbean older adults advocated con-versing with God through prayer and consulting one’s GP asequally valid ways of accessing help (Lawrence et al., 2006b).
Western medical forms of practice were established inIndia during the British rule when indigenous models ofhealth care were suppressed. Today, India has a plural-istic medical system and the Western biomedical modelexists alongside the government sanctioned, ‘Indian Sys-tems of Medicine’. These include Ayurveda, which is of-ten described as the oldest health care system in the world,
P1: PXY/OSW P2: TIXc04 JWBK439-Banerjee January 14, 2010 14:27 Printer Name: Yet to Come
HEALTH BELIEFS, CULTURE AND SERVICE USE 35
and variations on Ayurveda such as Siddha and Unani. InAyurvedic medicine the mind and body are regulated by‘doshas’, which are endowed at birth and which are a combi-nation of the five elements: space, air, fire, water, and earth.Life can cause imbalances in doshas, which can lead to ill-ness. Treatments are holistic and focus on the person ratherthan the disease; thus they target the mind (e.g. transcen-dental meditation), body (e.g. herbs, purification techniques,exercise), behaviour (sleeping, working habits) and environ-ment (e.g. collective practice of transcendental meditation).More recent therapies, including yoga and homeopathy, arealso widely practiced throughout India.
Western and Indian systems of medicine are consideredcomplementary and are utilised in different sequences andcombinations. However, there is limited availability and useof psychiatric treatment in India. Admission to a psychi-atric institution signifies an individual’s insanity and familymembers are keen to avoid this label at all costs (Laungani,1999). There is also an absence of formal services such ascare homes and families and other informal carers are themainstay of support (Shaji et al., 1996). Research indicatesthat there is also a stark under-provision of services to sup-port people with dementia and carers within the commu-nity (Shaji et al., 2003). In addition to the use of Ayurvedicmedicine, it is also accepted practice to visit shrines, tem-ples or faith healers, as mental illness can be attributed tomalevolent gods or evil spirits (Laungani, 1999). A smallscale study with ‘healthy’ Asians in a community setting inGlasgow revealed that the knowledge of Asian health con-cepts, remedies and healers was high, but that there wereeven greater barriers to accessing Asian medicine than theNational Health Service. The use of Asian medicine didnot affect general practice consultation rates in this group(Singh-Bhopal, 1986). However, this picture is likely to havechanged in the last 20 years; pressures on waiting lists andappointment times may have increased barriers to main-stream care in the UK, while the revival of ‘alternative sys-tems’ of care are likely to have made them more accessible.

P1: PXY/OSW P2: TIXc04 JWBK439-Banerjee January 14, 2010 14:27 Printer Name: Yet to Come
36
P1: PXY/OSW P2: TIXc05 JWBK439-Banerjee January 14, 2010 14:30 Printer Name: Yet to Come
5WHOSE ILLNESS IS IT
ANYWAY?
From the previous chapters it can be seen that there are atleast three perspectives that can be taken:
� that of society including its dominant modes of health andsocial care
� that of the person with dementia� that of family carers of the person with dementia.
These all act and interact to determine whether services aredeveloped, funded, offered, requested and accepted. In thischapter we will consider the available evidence in each ofthese perspectives.
SOCIETY – POLICY IN RELATION TO ETHNICITYAND CULTURE
At the heart of government guidelines and recommenda-tions for people with dementia is the principle that olderadults have a right to person-centred care that acknowl-edges and responds to their individual needs. By definition,equality of access and individualised care requires careprofessionals and service providers to take account of thepatient’s social and cultural background (Audit Commis-sion, 2000, Audit Commission, 2002). Standard Seven of the
Managing Dementia in a Multicultural Society Sube Banerjee and Vanessa LawrenceC© 2010 John Wiley & Sons, Ltd
37
P1: PXY/OSW P2: TIXc05 JWBK439-Banerjee January 14, 2010 14:30 Printer Name: Yet to Come
38 MANAGING DEMENTIA IN A MULTICULTURAL SOCIETY
National Service Framework for Older People (Departmentof Health, 2001) included a focus on the need for accessibleand appropriate mental health services for individuals fromblack and minority ethnic groups. The last 20 years has seena considerable shift in policy, and this stance is far removedfrom the previously espoused expectation that membersof minority ethnic groups should simply ‘fit in’ with themajority culture (Royal College of Psychiatrists, 1990). Thequestion of whether dementia services for older people fromminority ethnic groups should be located in mainstreamor specialist provision remains the subject of considerabledebate. In a document with the best title of any governmentdocument in the last century (not that that’s much of acompetition) They look after their own, don’t they? (SocialServices Directorate, 1998) contended that Social ServicesDepartments should support both the provision of in-houseculturally appropriate services that are capable of meetingthe needs of all communities, as well as specialist serviceswithin the voluntary sector. Assessment of culturally ap-propriate services and the dissemination of examples ofgood practice would benefit both voluntary and mainstreamproviders (Care Services Improvement Partnership, 2005).
BLACK AND MINORITY ETHNICORGANISATIONS
Separate dementia services for ethnic minority older peo-ple may not represent the solution to unmet needs in thisgroup, but it is arguable that voluntary organisations servingblack and minority groups have acquired a great deal of ex-perience supporting people with dementia within these com-munities. Since its inception in 1998, the Policy ResearchInstitute of Ageing and Ethnicity has successfully focussedattention on the prominent role that minority voluntary ser-vices have played in providing dementia care and informa-tion. Certainly, many organisations have established rep-utations for providing innovative and responsive services,which offer a valuable insight into culturally sensitive care.Consequently, they present an important learning resourcefor mainstream service providers. It is therefore highly
P1: PXY/OSW P2: TIXc05 JWBK439-Banerjee January 14, 2010 14:30 Printer Name: Yet to Come
WHOSE ILLNESS IS IT ANYWAY? 39
unfortunate that little formal evidence exists regarding thenature of these services, their effectiveness, and even theirprevalence. The information that does exist tends to be lim-ited to local directories and internal reports and it is with thisimportant caveat that we now discuss some of the availableservices and consider what lessons can be drawn from theapproaches to care that they provide.
Many projects, groups and organisations, which wereoriginally established to enhance interaction and shared ex-periences within the local community, have since developedstructured services that aim to meet specific needs withinthe ethnic minority group. This includes day-care for olderpeople with dementia, within which the core values of re-specting individual’s cultural and background remain. Thisincorporates sensitivity to dietary rules and preferences, ev-eryday customs, linguistic needs and religious practice aswell as culturally appropriate leisure activities and hobbies.For example, older adults are provided with a kosher mealat the ‘The Dennis Centre’, part of Jewish care, while ‘AgeConcern Haringey’ acquires Turkish food from a nearbyrestaurant, and the ‘Calabash centre’ in southeast Londontakes pride in providing high quality Caribbean meals thatmembers can enjoy with others. In some centres bathing ser-vices exist, in which an awareness of cultural preferences andneeds are paramount, while other organisations offer assis-tance with personal care within the individual’s own home.As part of the ‘Lambeth Chinese Community Association’Home-Care Project, bi-lingual care workers assist older peo-ple with dementia with cleaning, personal care, meal prepa-ration, feeding, etc. Language represents a major barrier tothe majority of Chinese older people, and as such, only avery small proportion access mainstream services. Conse-quently, bi-lingual staff represent a basic requirement withinthis group. Alternatively, as part of the ‘The Red Sea Healthand Community Care Association’ in West London, staff actas interpreters to Somali older people during appointmentsat GP surgeries and hospitals.
Although, there is no firm consensus on the issue, manyof these organisations employ staff predominantly from thesame ethnic group as their membership. It is the policy
P1: PXY/OSW P2: TIXc05 JWBK439-Banerjee January 14, 2010 14:30 Printer Name: Yet to Come
40 MANAGING DEMENTIA IN A MULTICULTURAL SOCIETY
of ‘Alzheimer’s Concern Ealing’, a well-established char-ity within the ethnically diverse borough of Ealing, that thebackground of its staff should reflect the community as awhole. However, the service places equal emphasis on re-cruiting staff that are skilled in working with people with de-mentia. ‘The Dekh Bhall Project’, launched in the Londonborough of Newham, represents a novel initiative that aimedto address the shortage of Asian care workers adequatelytrained in dementia. A 14-week programme and placementscheme was developed for the purposes of advancing the de-mentia knowledge and skills of Asian domiciliary care work-ers. On the other hand, employers of Alzheimer’s Scotlandoffer advice on culturally appropriate care to professionalsin mainstream settings that are working with clients of East-ern European background. This underlines the joint neces-sity of these two areas of expertise.
A number of voluntary organisations have also recog-nised that the ethnic and cultural background of caregiversmay affect their experiences and needs. For instance mem-bers of ethnic minority groups may consider it more ac-ceptable to utilise home respite services than to use respiteplacements in local care homes. As part of a 3 year HealthAction Zone project, the ‘Bradford Dementia Group’ devel-oped and implemented a 10-week support group for southAsian and Eastern European carers of people with demen-tia. The project aimed to adopt a person-centred approachthat explored the experience and needs of minority care-givers from the individual’s perspective. Through a processof interviews and observation, culturally appropriate sup-port materials were developed for use with future groups.Voluntary organisations have pioneered a range of inno-vative strategies to advance the understanding of dementiawithin ethnic minority communities, and to raise awarenessof available services (both statutory and voluntary). This isimportant as conventional leaflets and posters have beenshown to have limited success in this domain. Videos suchas ‘Dementia does not discriminate’ and ‘Dementia Ki Hai’[Alzheimer’s Concern Ealing, London] use interviews withethnic minority carers and staff to explain how dementia canaffect the individual, how this may be influenced by culture,
P1: PXY/OSW P2: TIXc05 JWBK439-Banerjee January 14, 2010 14:30 Printer Name: Yet to Come
WHOSE ILLNESS IS IT ANYWAY? 41
and what help is available. Similarly, Dementia Plus in theWest Midlands has successfully developed multi-media edu-cational programmes for African Caribbean and Asian pop-ulations.
Notably, among the support groups provided by the‘Bradford Dementia Group’, one was specifically arrangedfor Pakistani carers who did not wish to participate in anethnically mixed group, and another was attended by bothPakistani and Indian carers. This raises the question of howculturally specific a service should be. ‘Alzheimer’s ConcernEaling’ clearly states that they are not a culturally specificagency, but one that reflects the ethnic make-up of the com-munity. However, a ‘Help the Aged’ produced booklet ofagencies for minority ethnic older people in London illus-trates how challenging this can be. It details the difficultiesexperienced by a Cypriot agency in Haringey, which at-tempted to serve both the local Greek Cypriot and TurkishCypriot populations. Despite providing culturally appropri-ate food and prayer facilities for each community, theyfound that historical and religious differences prevented thepredominantly Muslim Turkish speaking elders from usingthe service. The ‘Help the Aged’ booklet also observedthat older people with dementia risk being marginalised inunder-resourced centres that aim to meet the diverse needsof people of all ages and abilities within a particular ethnicgroup.
Services benefited from successful links with othergroups and organisations working with similar client groups.This allows projects to share information and expertise andto create a unified voice for the ethnic group and their organ-isations. However, it is equally important that these projectswork in partnership with statutory agencies. For example,despite providing a high standard of culturally sensitive daycare for Jewish older people with dementia, ‘Jewish Care’found that many older people were being referred to thecentre at too late a stage. They are now working proactivelyto raise awareness of their service among health and so-cial care professionals and to encourage referrals at an ear-lier stage in the illness. In conclusion, it is undeniable thatvoluntary organisations represent an invaluable resource to
P1: PXY/OSW P2: TIXc05 JWBK439-Banerjee January 14, 2010 14:30 Printer Name: Yet to Come
42 MANAGING DEMENTIA IN A MULTICULTURAL SOCIETY
many older people and their carers within ethnic minoritygroups. They are restricted by limited resources and furtherinvestment is needed to sustain innovative projects and en-able them to operate to their full potential. However, thelack of independent evaluations of these services must beaddressed.
Like dementia services as a whole, (National Audit Of-fice, 2007), a partnership is needed between service commis-sioners, voluntary organisations, and older people and theircarers from minority ethnic groups. Delivering Race Equal-ity in Mental Health Care (Department of Health, 2005) ispart of a wider programme to bring about equal quality inhealth and social care for all people from black and minoritygroups. Although this is not specific to older adults, the keymessages of more appropriate and responsive services, com-munity engagement and better dissemination of informationand good practice, have obvious relevance.
USE OF SERVICES
Research conducted in 1995 indicated that only 15–20% ofpeople with dementia were ever referred to specialist men-tal health services (Holmes et al., 1995). More recent figuressuggest that less than half of older adults with dementia inthe United Kingdom have their condition diagnosed at anystage in their illness (Knapp et al., 2007) despite the likelytherapeutic benefits. Furthermore, a considerable amountof research has indicated that people with dementia and caregivers do not always utilise available community supportservices including respite care, day centres and domiciliarycare (Brodaty et al., 2005, Braithwaite, 1998, Casserta et al.,1987, Collins et al., 1991, Gwyther, 1994, Lawton et al.,1989a, Strain and Blandford, 2002, Thomson et al., 2005).
It appears that older people from minority ethnic groupsare more likely to receive the diagnosis of Alzheimer’s Dis-ease at later stages of the disease, and following a long anddebilitating course (Yeo and Gallagher-Thompson, 1997).They are therefore, less likely to access interventions earlyand so to benefit from available services and treatments.Research suggests that south Asian (Patel et al., 1998, Rait
P1: PXY/OSW P2: TIXc05 JWBK439-Banerjee January 14, 2010 14:30 Printer Name: Yet to Come
WHOSE ILLNESS IS IT ANYWAY? 43
and Burns, 1997) and Caribbean (Nelson et al., 2004) olderpeople are under-represented in referrals to psychiatricservices and in the use of social care services (Social Ser-vices Directorate, 1998, Social Services Directorate, 2001) inthe UK. Research conducted in the United States had indi-cated lower levels of service use among minority care giverscompared with non-Hispanic white care givers (Dilworth-Anderson et al., 2002). UK studies similarly suggest that peo-ple with dementia and their carers from ethnic minorities arenot using services at the same rate as the majority popula-tion (Brownlie, 1991, Brownfoot, 1998). In response to this,councils are now required to monitor whether older peoplefrom black and minority ethnic groups are fairly representedin referrals to and use of social services (The Home Office,2000).
It is important for us to observe such apparent disparityof service use. However, knowing that there is a differenceis only one step on the road to finding a solution. Whilequantitative studies are good for answering the questions‘how many?’ and ‘is there a difference between. . .?’ theyare not as good at telling us ‘why?’ It is this that we needto understand if we are to formulate an effective responseat a service and individual level. In order to start to addresssuch questions there is value in looking to qualitativemethodologies that can tap the experience of people withdementia and their carers directly, providing insights intoknowledge, attitudes and behaviour. In the next chapterswe will therefore consider the background to help seeking,offering and accepting for people with dementia and theircarers separately. Following this we will present the datafrom cross-cultural qualitative studies designed to take ourunderstanding in these areas further.
THE EXPERIENCE OF THE PERSONWITH DEMENTIA
As noted above, understanding the preferences, interests,values, relationships and achievements of the individual withdementia is pivotal to providing care that enhances qualityof life (Woods, 2001). Until recently, however, people with
P1: PXY/OSW P2: TIXc05 JWBK439-Banerjee January 14, 2010 14:30 Printer Name: Yet to Come
44 MANAGING DEMENTIA IN A MULTICULTURAL SOCIETY
dementia have been likened to ‘hidden victims’, not just be-cause of the effects of the disease, but because their perspec-tive has been largely overlooked (Woods, 1997). In the 1980sand 1990s, the person with dementia was sidelined as socialresearch focused on the attitudes and experiences of familycarers (Bartlett, 2007). Yet over the last 20 years the dis-course surrounding dementia has begun to change and thefocus of the medical model on dementia as a disease entityhas broadened to include an awareness of the individualityof the person with dementia (Innes, 2002). Through the con-cept of ‘personhood’, Kitwood (1997) acknowledged aspectsof self that are not bound to the preservation of memory,including feelings, emotions and reactions that can be sus-tained in relationships with others. Qualitative studies haverevealed that people with dementia are able to express feel-ings and concerns articulately (Pearce et al., 2002) and that alevel of awareness is retained, even in the later stages of thedisease (Clare et al., 2008). The recent growth of researchexploring the perspective of the person with dementia hasstarted to redress the traditional lack of attention in this area(Steerman, 2006). Previously, research had relied upon theperspective of care givers, which may not reflect the expe-rience of the individual sufferers themselves. Indeed, a dis-crepancy may exist between the needs and preferences ofthe care giver and care recipient (Lyons, 2002).
However, this is an emerging field and questions remainregarding how people with dementia appraise their situa-tion and conceptualise aspects of their lives. The existingknowledge base is predominantly underpinned by researchwith people in the early stages of dementia who are oftenrecruited through memory clinics. It is important that olderpeople in the moderate to severe stages of dementia alsohave an opportunity to express their views. Most striking,however, is the stark absence of research with people withdementia from minority ethnic groups. Two recent reviewsidentified 28 qualitative studies (Steeman et al., 2006) and 50articles (de Boer et al., 2007) that examined the perspectiveof the person with dementia, yet none reported experienceswithin minority ethnic populations. Kitwood (1997) con-ceptualised dementia as a socially embedded phenomenon
P1: PXY/OSW P2: TIXc05 JWBK439-Banerjee January 14, 2010 14:30 Printer Name: Yet to Come
WHOSE ILLNESS IS IT ANYWAY? 45
in which the person’s neurological impairment interactswith the surrounding social environment. Accordingly, itis important to consider the experience of dementia withinits socio-cultural context (Downs, 2000). Downs (2000)emphasised that cultural meanings of changed cognitiveabilities are likely to influence the subjective experienceof dementia and the manifestation and response to thecondition. The recognition of the perspective of the personwith dementia within research, policy and practice, marksan important development in dementia care (Woods, 2001).However, the continued lacuna in research within ethnicminority groups also needs to be addressed.
THE CARE GIVER EXPERIENCE
The 1990s saw a focus on research exploring ethnic andcultural variations in the dementia care giving experience.The Stress Process Model (Chapter 7) underpinned themajority of this work and has provided valuable insights intothe problems that families face over the course of the caregiving career (Aneshensel, 1995). A review of the literaturereveals not only negative findings; African American caregivers have been found to report less stress, burden anddepression than white care givers and to derive more benefitand meaning from the care giver experience (Connell, 1997).Researchers have posited that variation in informal support,coping responses and attitudes towards the care giving rolemay mediate the relationship between ethnicity and caregiver strain/gain. Understanding the psychosocial processesthat account for difference in care giver outcomes shouldassist us in the development of supportive services and inter-ventions for minority carers (Janevic, 2001) and the popula-tion as a whole (Montgomery, 2001). However, the majorityof research in this area has been quantitative and theemphasis has been on measuring outcomes rather than on‘understanding’ the subjective experience of care givers. Forexample, the data suggest a relationship between caregivers’ cultural attitudes and care giver well being, but tellus little about how this process operates. Again, qualitativemethodology may be best placed to uncover the complexity
P1: PXY/OSW P2: TIXc05 JWBK439-Banerjee January 14, 2010 14:30 Printer Name: Yet to Come
46 MANAGING DEMENTIA IN A MULTICULTURAL SOCIETY
of the cultural differences in care giver values, beliefs andmeanings. The dominance of the Stress Process Modelhas been linked to an emphasis on the negative outcomesof caring for a person with dementia. Research into thepositive aspects of care giving offers advantages, includinggenerating direct help for clinicians to work more effectivelywith carers (Kramer, 1997). Lastly, it is important to pointout that the bulk of this research has been conducted inAmerica; in UK populations comparatively little is known.
Inevitably, a major consideration is why people withdementia and their carers do not utilise available formalsupport. The majority of research undertaken within ethnicminority groups in the UK has concentrated upon carers’ at-titudes towards formal services and how they conceptualisethe condition. This has suggested that concepts of dementiaand the perceived appropriateness of services may differacross ethnic groups. Some researchers have contendedthat health care providers are inclined to adopt the viewthat ethnic minority groups ‘take care of one’s own’, as itmitigates their own responsibility to provide care (Atkinsand Rollins, 1992). However, the current evidence base ischaracterised by small-scale studies that lack an underlyingtheoretical framework. Research is largely confined tosouth Asian communities and the absence of research withthe black Caribbean population represents an overarchingdeficit (Milne, 2005). The diversity within and between eth-nic groups, and the temporality of cultural beliefs, presentfurther difficulties to clinicians, who have been challengedto avoid making stereotypical generalisations (Yeo andGallagher-Thompson, 2006).
P1: IFM/OSW P2: TIXc06 JWBK439-Banerjee January 14, 2010 14:31 Printer Name: Yet to Come
6THE PERSPECTIVE OF THEPERSON WITH DEMENTIA
There has been a recent growth in research exploring thesubjective experience of the person with dementia that hasstarted to redress the traditional lack of attention in thisarea. This literature is not that well known and so we willnow focus on summarising this growing body of research.This will start with a discussion of its emergence within theresearch field, followed by a review of the main topics cov-ered in the literature:
� impact of dementia on the sense of self;� practical and emotional impact of dementia;� coping strategies and adaptation by the person
with dementia;� attitudes towards services.
A distinctive feature of this research, in contrast to that ofthe care giving literature which we will consider in the nextchapter, is the absence of research within minority ethnicgroups.
A NEGLECTED PERSPECTIVE
As noted above, people with dementia have been likenedto hidden victims, not because of the effects of the disease,
Managing Dementia in a Multicultural Society Sube Banerjee and Vanessa LawrenceC© 2010 John Wiley & Sons, Ltd
47
P1: IFM/OSW P2: TIXc06 JWBK439-Banerjee January 14, 2010 14:31 Printer Name: Yet to Come
48 MANAGING DEMENTIA IN A MULTICULTURAL SOCIETY
but because their perspective has been largely overlooked(Woods, 1997). Despite, or perhaps due to the intense focuson care givers, the person with dementia has been sidelinedand usually implicitly positioned in the literature as a bur-den or root cause of the problem (Bartlett and O’Conner,2007). The subjective experience of living with dementia hastended to be limited to the perspective of family care givers.Yet there may well be discrepancy between the needs andpreferences of the care giver and care recipient (Lyons et al.,2002). Moreover, it cannot, unfortunately, be assumed thatcare givers are always motivated by the best interest of theperson with dementia. Until recently, research into the ex-perience of dementia has been dominated by quantitativestudies that have often focused upon the behavioural andpsychological symptoms of dementia. Again, these have re-lied upon the perspective of carers, which may not reflectthe experience of the individuals themselves (Hoe et al.,2007).
In the late 1980s the notion of ‘personhood’ was intro-duced into the dementia literature as a critical componentof the dementia experience (Bartlett and O’Conner, 2007).Tom Kitwood, one of the principal proponents of this ap-proach, argued that the person with dementia’s neurologicalimpairment interacts with the social environment, person-ality, biography, physical health and social psychology toinform the clinical presentation of the condition (Kitwood,1993). This focused attention on the impact of the surround-ing social environment by suggesting that a ‘malignant socialpsychology’ could depersonalise the person with dementiaand be deeply damaging to personhood. Kitwood definedpersonhood as, ‘a standing or status that is bestowed uponone human being, by others, in the context of relationshipand social being’ (Kitwood, 1997). This describes a senseof self-identity that is created in relationships with othersand can persist throughout the course of dementia. Thischallenges the pervasive assumption that cognitive abilitiesunderpin personhood and that one cannot meaningfullyexist if cognition is impaired (Woods, 1999). Cotrell andSchulz (1993) insisted that people with dementia should
P1: IFM/OSW P2: TIXc06 JWBK439-Banerjee January 14, 2010 14:31 Printer Name: Yet to Come
THE PERSPECTIVE OF THE PERSON WITH DEMENTIA 49
be seen not as objects, but as individuals who are uniquelysituated to help us better understand the illness and itstreatment.
As clinicians have always known, research has nowshown that people with mild-moderate dementia are gen-erally able to express feelings and concerns articulately(Cohen and Eisendorfer, 1986, Phinney, 2002) and respondconsistently to questions about preferences, choices anddecisions regarding daily care (Feinberg and Whitlatch,2001). Recent research has also disputed traditional opinionthat a lack of awareness of one’s condition is a clinicalfeature of dementia. Clare (2003) found that efforts toprotect self-esteem contributed to apparent variations inawareness and that individuals who use coping strategiessuch as denial and minimisation risk being mislabeled asunaware or lacking insight. It has also been suggested thatdemonstrable sadness and despair in people with dementiabelie lack of insight (Howorth and Saper, 2003). Clare(2004) presented a biopsychosocial model of awarenessthat is compatible with person-centred approaches toresearch and clinical practice. This model proposes thatcognitive functioning interacts with individual psychologicalresponses and the social context to influence expressions ofawareness.
Research has predominantly focused on people in theearly stages of dementia (Downs, 1997) and the voices ofindividuals in the more severe stages have received littleattention. The majority of research participants have beenrecruited from memory clinics (Steeman et al., 2006) wherepatients are likely to be more independent and have lowerlevels of cognitive impairment (Jolley et al., 2006, Luceet al., 2001). Although no estimates exist, it is likely thatonly a tiny minority of people with dementia access suchservices. It is also vital to note that in most research a focuson the person with dementia within minority ethnic groupshas barely started (Bowes and Wilkinson, 2002). Concep-tualising dementia as a socially embedded phenomenon(Kitwood, 1997) demands that we explore the impact ofethnicity and culture on the experience of dementia.
P1: IFM/OSW P2: TIXc06 JWBK439-Banerjee January 14, 2010 14:31 Printer Name: Yet to Come
50 MANAGING DEMENTIA IN A MULTICULTURAL SOCIETY
SELF-IDENTITY IN DEMENTIA
Ultimately, as with any chronic illness, the physical, social,psychological and financial implications of dementia form athreat to the self, as individuals struggle to sustain valuedattributes, activities and roles (Charmaz, 1987). Indeed, de-mentia has been described as leading to ‘the inexorable dis-solution of the self’ (Cohen and Eisendorfer, 1986), and it isthis loss of identity that underlies much of the fear attachedto the disease (Basting, 2003). However, vivid personal ac-counts of living with Alzheimer’s Disease communicate anenduring sense of self that is not bound to the preservationof memory (Basting, 2003).
Sabat and Harre (1992) differentiated two forms ofidentity: the personal self, which persists into the final stagesof dementia, and social selves, which may or may not be lostdepending upon how the individual is viewed and treatedin social interactions. Sabat and Harre’s (1992) socialconstructionist model and Kitwood’s (1997) person-centredcare model both look beyond the neurological effects of thedisease to the role that significant others play in maintainingor undermining the self and well-being. They argue that theexistence of the self requires social co-operation and that thetendency to position the individual as helpless and confused,and to overemphasise the symptoms of dementia, is detri-mental (Sabat and Harre, 1992). As previously mentioned,Kitwood (1997) termed this a ‘malignant social psychology’,and proposed that constructive interaction requires that caregivers recognise, respect and provide opportunity for theindividual’s self-expression. Empirical research has begunto analyse the change in self-identity throughout dementia(Cohen-Mansfield et al., 2000, Cohen-Mansfield et al.,2006a), as well as the role that interpersonal relationships(Orona, 1990; Surr, 2006) and therapeutic interventions(Cohen-Mansfield et al., 2006a, Romero and Wenz, 2001)can play in promoting continuity. In some ways the def-inition of personhood as ‘a standing or status bestowedupon one human being, by others’ (Kitwood, 1997) situatespeople with dementia as passively dependent on others foraffirmation. Yet, research has also begun to suggest that
P1: IFM/OSW P2: TIXc06 JWBK439-Banerjee January 14, 2010 14:31 Printer Name: Yet to Come
THE PERSPECTIVE OF THE PERSON WITH DEMENTIA 51
people with dementia themselves play an active role inmaintaining their sense of self (Harris and Sterin, 1999).
IMPACT OF DEMENTIA ON THE SENSE OF SELFOF THE PERSON WITH DEMENTIA
People with dementia often report problems with theirmemory when asked about their condition (Aggarwal et al.,2003, Clare et al., 2005, Van Dijkhuizen et al., 2006). Othershave spoken about losing skills and the ability to performparticular activities (Cohen-Mansfield et al., 2000, Gillies,2000, Sabat, 2002). People with dementia have also de-scribed difficulties with communication and feelings of lossof control, autonomy and independence (Harris and Sterin,1999, Gillies, 2000, Aggarwal et al., 2003, MacQuarrie,2005).
There is a substantial amount of evidence to suggestthat the prevalence of depression is high in people with de-mentia (Ballard et al., 1996). However, instruments that as-sess mood and behaviour in the person with dementia havetended to rely heavily on carer reports and interpretation(Brod et al., 1999). Similarly, the impact of dementia on thequality of life of those afflicted has been rated and describedusing proxy measures in various quantitative studies. Whereboth perspectives have been sought, quantitative studies in-dicate a tendency for informal carers to report more healthrelated quality of life problems than the people with demen-tia themselves (Smith et al., 2005, Sneeuw et al., 2002). Thisrequires an exploration of how people with dementia them-selves experience and value their situation.
Qualitative studies have begun to elucidate the psycho-logical and emotional impact of dementia on the individ-ual. The onset of dementia has been found to evoke feelingsof confusion, shock and anxiety (MacQuarrie, 2005, Gillies,2000, Howorth and Saper, 2003). Research has also indi-cated that people with dementia can experience irritation,frustration and anger in response to memory loss (Gillies,2000, MacQuarrie, 2005, Aggarwal et al., 2003) as well asfeelings of worthlessness and stupidity (Sabat, 1998, Harrisand Sterin, 1999). Individuals have expressed fear regarding
P1: IFM/OSW P2: TIXc06 JWBK439-Banerjee January 14, 2010 14:31 Printer Name: Yet to Come
52 MANAGING DEMENTIA IN A MULTICULTURAL SOCIETY
the progressive nature of the condition and of becoming aburden in the future (Clare, 2002, Clare, 2003, Pearce et al.,2002). There is evidence that people with dementia are of-ten concerned about how they are perceived by others andsome prefer to keep their diagnosis private (Gillies, 2000,Husband, 2000) for fear of stigmatisation (Sabat, 2002). Arecent review of quantitative and qualitative research fromthe person with dementia’s perspective found only a smallnumber of positive accounts whereby the individual wasunconcerned or relatively ‘happy’ with his or her situation(de Boer et al., 2007). The findings from one study indicatethat good contact with other people and a feeling of being ofuse contributes to a good quality of life (Droes and Boelens-Van Der Knoop, 2006). However, the review reported thatqualitative accounts with people with dementia regardingtheir quality of life remain scarce.
COPING STRATEGIES AND ADAPTATION
A substantial area of research relates to coping strategiesand adaptation by the person with dementia. Theoreticalmodels of coping have posited that individuals adopt cog-nitive or behavioural methods to manage demands or emo-tions that are appraised as stressful (Lazarus and Folkman,1984). Strategies have traditionally been categorised ac-cording to function (i.e. emotion focused, problem focused(Lazarus and Folkman, 1984), avoidance coping and ap-proach coping (Suls and Fletcher, 1985). These differentiatebetween coping strategies that actively manage the situation(i.e. problem-focused coping, approach coping), and thosethat manage the meaning ascribed to it (i.e. emotion-focusedcoping, avoidance coping). As will be discussed next, cop-ing among care givers of people with dementia has predomi-nantly been viewed from the perspective of the stress-copingtheory (Pearlin et al., 1990b, Zarit, 1989). This draws atten-tion to coping styles aimed at managing symptoms of stressproduced by the situation. Although extensive research hasexamined coping in care givers, until recently comparativelylittle had been published on coping in dementia by peo-ple with dementia. Previous work has tended to draw upon
P1: IFM/OSW P2: TIXc06 JWBK439-Banerjee January 14, 2010 14:31 Printer Name: Yet to Come
THE PERSPECTIVE OF THE PERSON WITH DEMENTIA 53
clinical observation and experience, rather than on sys-tematic empirical research with the person with dementia(Droes, 2007). This not only marks the recognition of indi-viduals’ invaluable contribution to research, but also theiractive role in managing the changes that they are experienc-ing (Cotrell and Schulz, 1993).
Evidence suggests that people with dementia adoptstrategies aimed at managing the situation such as:� using external memory aids such as calendars and lists
(Keady and Nolan, 1995b, Gillies, 2000, Clare, 2002,Preston et al., 2007, Harris and Sterin, 1999, Gilmour andHuntington, 2005);
� finding out more about dementia (Clare, 2002, Younget al., 2002);
� talking about one’s memory deficits (Clare, 2002, Prestonet al., 2007, Harris, 2002); and
� relying on others or seeking informal or formal support(Harris and Sterin, 1999, Gillies, 2000, MacQuarrie, 2005,Pearce et al., 2002, Clare, 2003).
In one of the first studies of its kind, Keady et al. (1995) ob-served that people with dementia ‘cover up’ memory lapses,but also demonstrate acceptance and positive coping. Sub-sequent research has found evidence of a range of strategiesaimed at managing the meaning ascribed to the situation,including:� denial of problems (Gillies, 2000, Norman et al., 2004,
MacQuarrie, 2005);� normalising perceived changes (Gillies, 2000, MacQuar-
rie, 2005, Clare, 2002, Pearce et al., 2002, Clare and Shake-speare, 2004, Van Dijkhuizen et al., 2006, Preston et al.,2007);
� minimising problems (Clare, 2002, Pearce et al., 2002, VanDijkhuizen et al., 2006, Preston et al., 2007, MacQuarrie,2005); and
� engaging in positive social comparisons (Gillies, 2000,Clare, 2002, Pearce et al., 2002).
Finally, research has observed individuals acceptingtheir difficulties and viewing them in the wider context
P1: IFM/OSW P2: TIXc06 JWBK439-Banerjee January 14, 2010 14:31 Printer Name: Yet to Come
54 MANAGING DEMENTIA IN A MULTICULTURAL SOCIETY
(MacQuarrie, 2005, Clare, 2002, Pearce et al., 2002, VanDijkhuizen et al., 2006, Preston et al., 2007). The latterstrategies appear to alleviate distress by helping individualsto readjust negative appraisals of their condition. Lazarus(1993) observed a tendency among researchers to cate-gorise problem focused strategies as adaptive, but to viewemotional focused strategies as having an adverse effecton individuals’ mental and physical health. However, emo-tional focused strategies such as acceptance may representthe best coping choice where nothing useful can be done tochange the situation (Lazarus, 1993).
Keady (1995) proposed that people with dementia adoptdifferent coping strategies at different stages in the illness.Others have positioned coping on a continuum, with ‘self-protective’ strategies that protect an individual’s prior senseof self at one end, and ‘self-integrative’ strategies that adjustthe sense of self to dementia related changes at the other(Harris and Sterin, 1999, Clare, 2002, Pearce et al., 2002).The tension between maintaining and reconstructing iden-tity emerges as a dominant theme, and achieving equilibriumbetween self-protective strategies (e.g. holding on to rolesand abilities, compensating for deficits) and self-integrativestrategies (e.g. developing a fighting spirit, coming to termswith lost abilities) has been identified as a key adaptive taskfaced by people with dementia (Clare, 2002). More recently,it has been hypothesised that acknowledgement and denialoperate in parallel (MacQuarrie, 2005). MacQuarrie (2005)argued that people with dementia face threats to their au-tonomy, and that the desire to stay in control causes indi-viduals at times to acknowledge, and at other times to resist,aspects of their disease. Thus, stories of seeking help for de-mentia were juxtaposed with minimisation and normalisa-tion strategies, as both enabled individuals to assert agencyin the face of the condition. Similarly, Steeman et al. (2007)reported that in order to maintain a sense of value, peoplewith dementia balance an acknowledgement of difficultieswith an emphasis on remaining competencies.
So our insights into how individuals adjust to dementiahave grown over the last ten years. It is evident that somecoping strategies are more helpful than others, with some
P1: IFM/OSW P2: TIXc06 JWBK439-Banerjee January 14, 2010 14:31 Printer Name: Yet to Come
THE PERSPECTIVE OF THE PERSON WITH DEMENTIA 55
associated with depression and others underlying success-ful adjustment (Harris, 2002). However, the efficacy of cop-ing behaviour in people with dementia is highly complex.No linear correlation appears to exist between depressionand emotion focused strategies such as wishful thinking, ashas been suggested among care givers (Pruchno and Kleban,1993). Clare and colleagues (2006) explored the feasibilityof applying the self-regulatory model of illness (Leventhalet al., 1984) to dementia, which proposes that the use ofproblem focused or emotion focused coping behaviours me-diates the relationship between illness representations andhealth outcomes. Although predominantly focused on thenature of illness representations among people with demen-tia, the study also suggested that a limited repertoire of cop-ing strategies and a belief that nothing could be done to in-fluence their situation, could be related to higher levels ofanxiety and depression. However, the advantages and dis-advantages of the varied strategies require further consid-eration, as do their practical implications for help seekingand accepting. The stress and coping theory (Lazarus, 1966)highlights that the cognitive process through which individ-uals appraise their situation is central to his or her emo-tional response, yet few studies (Droes, 1997) have exploredhow people with dementia assess the significance that thechanges hold for their lives. Research has not yet begun toaddress coping behaviour among people with dementia fromminority ethnic groups, thus the influence of cultural atti-tudes and beliefs on cognitive appraisal, coping strategiesand adaptation is unknown.
ATTITUDES TOWARDS CARE
Exploring the perspective of the person with dementia is es-sential to developing care that enhances quality of life. Itpromises insight into how individuals perceive their needsand how they perceive the ability of services to meet them(Sabat, 2002). However, the attitudes of people with demen-tia towards services remain poorly understood. It is unclearhow people with dementia benefit from the introduction offormal services or what role they themselves play in that
P1: IFM/OSW P2: TIXc06 JWBK439-Banerjee January 14, 2010 14:31 Printer Name: Yet to Come
56 MANAGING DEMENTIA IN A MULTICULTURAL SOCIETY
introduction (Zarit et al., 1999). One area that has begunto receive attention is patient preferences towards receivingthe diagnosis of dementia. Despite evidence that GPs for-mally disclose the diagnosis to less than half of their patients(Van Hout et al., 2000), research has indicated that peoplewith dementia want to be told the truth (Pratt and Wilkin-son, 2001), even in the severe stages of the illness (Jha et al.,2001). Receiving diagnostic information can help to validatethe individual’s experience and allow them to express feel-ings of loss and grief (Derksen et al., 2006). A recent qualita-tive evaluation of satisfaction with a specific memory servicerevealed that people with dementia valued the clear com-munication and continuity of care that they received (Williset al., 2009).
Few studies have involved the evaluation of services bypeople with dementia, yet there is some evidence of positiveaccounts of day centres, which have been praised for provid-ing stimulation through word games and quizzes (Aggarwalet al., 2003) and for offering opportunities for social inter-action (Reid et al., 2001). Spending time with other olderpeople with dementia also provides opportunities to shareand normalise the experience (Preston et al., 2007). Con-versely, care homes have been associated with a lack of in-dependence, choice and stimulation (Aggarwal et al., 2003,Van Dijkhuizen et al., 2006). People with mild dementiahave cited memory groups as helpful in adapting positivelyto changes (Keady and Nolan, 1995a) and research suggeststhat people with dementia have mixed expectations regard-ing whether medication can help them (Lindstrom et al.,2006). Although a small number of studies have suggestedthat they are to explore attitudes to services among peo-ple with dementia from minority ethnic groups (Bowes andWilkinson, 2003, Brownfoot, 1998), the research findings aredominated by the views of carers. As previously suggested,the person with dementia’s service preferences may be in-compatible with their relatives’, and deserve at least equalattention (Moriarty, 1999).
P1: IFM/OSW P2: TIXc07 JWBK439-Banerjee January 15, 2010 17:38 Printer Name: Yet to Come
7THE PERSPECTIVE OF THE
FAMILY CARERS OFPEOPLE WITH DEMENTIA
Family carers have assumed centre stage in the researchagenda for almost 30 years, reflecting the pivotal rolethat they play, both in providing direct assistance and inaccessing formal support (Pearlin et al., 2001). In the UK,two thirds of people with dementia live in the community(National Audit Office, 2007) and family members continueto represent the most important source of care (Pickardet al., 2000). This is especially true among minority ethnicpopulations who are less likely to contemplate residentialcare (Adamson, 2001, Seabrooke and Milne, 2004) orto access specialist health or social care services in thecommunity (Social Services Directorate, 2001). Culture andethnicity have emerged as influential in multiple domains,including psychosocial research that has focused upon theimpact of care giving on mental and physical health, andresearch exploring the appropriateness of services, whichhas focused on variations in care preferences and serviceuse. Before considering this, the chapter will focus onpatterns of care giving within the different ethnic groups.
Managing Dementia in a Multicultural Society Sube Banerjee and Vanessa LawrenceC© 2010 John Wiley & Sons, Ltd
57
P1: IFM/OSW P2: TIXc07 JWBK439-Banerjee January 15, 2010 17:38 Printer Name: Yet to Come
58 MANAGING DEMENTIA IN A MULTICULTURAL SOCIETY
PATTERNS OF CARE GIVING
Supporting relatives with tasks and activities can be a nor-mal part of family life, yet assisting individuals with personalcare activities such as bathing, dressing and toileting is moreclearly associated with care giving (Lewis and Meredith,1988). Schulz and Quittner (1998) suggest that the practicaltasks assumed by carers reflect extraordinary care that ex-ceeds the bounds of what is normative. Carers of people withdementia face numerous and diverse everyday problems (dela Cuesta, 2005). Much of care giving extends beyond hands-on care to include anticipating future support needs, moni-toring and supervising, preserving the individual’s sense ofself and helping the individual to develop new and valuedroles (Nolan, 1995). There are also extensive emotional as-pects of care giving, which will be discussed later. Anesh-ensel and colleagues (1995) contend that care giving shouldnot be viewed as a fixed set of experiences, but as evolvingcircumstances that represent different stages in a ‘care givingcareer’.
Across ethnic groups the main responsibilities for day-to-day care tend to fall to one family member, usually awoman. Research has consistently shown that of all rela-tives, daughters are the most likely to provide care (Qureshiand Walker, 1989). Qureshi and Walker (1989) were the firstto suggest the existence of a hierarchy of preferred sourcesof support among British older people. This hierarchy de-scribed (with typical sociological elegance) as a ‘traditionalWestern normative preference structure’, assumed thefollowing order:
� spouse;� daughter;� daughter-in-law;� son, other relative; and� non-relative.
A study of care giving responsibilities observed similaritiesin the norms of social obligations between white and Asianpopulations, although one difference was that care givingwas more likely to fall to sons and daughters-in-law than to
P1: IFM/OSW P2: TIXc07 JWBK439-Banerjee January 15, 2010 17:38 Printer Name: Yet to Come
THE PERSPECTIVE OF THE FAMILY CARERS OF PEOPLE WITH DEMENTIA 59
daughters in the Asian community (Finch and Mason, 1993).One studies found that within south Asian families, personalcare tended to fall to daughters or daughters-in-law, whilemale carers assumed responsibility for organising care andmaking decisions (Townsend and Godfrey, 2001).
There is very limited published research on patterns ofcare giving within black Caribbean communities in the UK(Milne and Chryssanthopoulou, 2005). Our knowledge ofcare giving and family structures predominantly consists ofinferences drawn from Census data and from descriptiveand speculative accounts. There has also been a tendencyto rely upon research within African American communi-ties. This research has suggested that a distinctive featureof African American informal support networks is that theyare often comprised of both family and non-family memberssuch as friends and neighbours (Atkin and Rollings, 1996,Daker-White et al., 2002). The nature of the ties between thenon-family care giver and person with dementia within thispopulation, which might be classified as low down on the hi-erarchy of preferred support, has not been shown to affectthe quality of care (Lawton et al., 1992). However, impor-tant differences exist between African American and Britishblack Caribbean populations that necessitate caution whendrawing parallels of this sort. For instance, in comparisonwith America, the growth in minority ethnic groups in theUK has been rapid and recent, and the older generation tendto represent first generation immigrants (Adelman et al.,2009). It is also proposed that levels of segregation are con-siderably higher among African Americans than in Britishblack Caribbeans (Peach, 1999). Yet, the two populationsshare a number of characteristics, such as high unemploy-ment rates and a high proportion of households headed by asingle female (Peach, 1999), and the shared African heritagecan be expected to inform cultural values and beliefs.
Changing socio-economic and demographic factors, suchas smaller family sizes and women’s increased partici-pation in the workforce, may be limiting the ability ofAsian families to provide care (Ahmad, 1996a). Ahmad(1996b) queried the existence of the ‘extended family’ withinthe south Asian population, arguing that within the UK
P1: IFM/OSW P2: TIXc07 JWBK439-Banerjee January 15, 2010 17:38 Printer Name: Yet to Come
60 MANAGING DEMENTIA IN A MULTICULTURAL SOCIETY
relationships of intimacy within the nuclear family are moretypical. A qualitative study with first generation and secondgeneration Caribbean and south Asian participants in theUK reported contrasting perceptions of the current role ofthe extended family (Modood et al., 1994). It was found thatunlike first generation south Asians, the second generationplaced a greater emphasis on the nuclear rather than theextended family. However, the findings also indicated thatextended family networks were considered to have weak-ened a great deal less within the south Asian, than withinthe Caribbean community. The roles of south Asian womenliving in Western countries appear to be changing; they nowhave the same educational opportunities as men and makea greater contribution to family decisions. Some commen-tators have referred to a dualistic role in that they displayWestern characteristics in an occupational context, yet con-tinue to adopt traditional behaviour within the home andsocial settings (Chandarana and Pellizzari, 2001).
THE IMPACT OF CARE GIVING
Research into care giving began to grow in the 1980s, reflect-ing an increasing awareness that the American populationwas ageing and that care giving was becoming an increas-ingly typical experience. Attention turned to the economic,social and psychological impact of caring for a relative orfriend with dementia. An accumulating body of evidencesuggested that dementia care givers were more likely to ex-perience anxiety, stress and depression than non-care givers(Cooper et al., 2007, Pinquart and Sorensen, 2003).
THE STRESS PROCESS
The negative outcomes of care giving attracted the inter-est of stress researchers and Stress Process Models domi-nate care giver research (Pearlin et al., 1990a). These wereadapted from the stress and coping model of Lazarus andFolkman (1984). This gave precedence to the process ofappraisal, stating that individuals first evaluate the poten-tial threat of external stressors and then assess their ability
P1: IFM/OSW P2: TIXc07 JWBK439-Banerjee January 15, 2010 17:38 Printer Name: Yet to Come
THE PERSPECTIVE OF THE FAMILY CARERS OF PEOPLE WITH DEMENTIA 61
to cope with them. Stress was conceptualised as a state ofarousal that resulted from conditions that taxed or exceededthe usual resources of the person. The demands associatedwith care giving can lead to strain, which the gerontologicalliterature has come to refer to as ‘care giver burden’ (Hoff-man and Mitchell, 1998). The Stress Process Model arguedthat the demands imposed by cognitive impairment, func-tional abilities and the behaviour problems associated withdementia were not the sole determinants of care giver bur-den (Zarit et al., 1980). The model acknowledged these ob-jective demands of care giving as ‘objective primary stres-sors’, but theorised that these could also prompt certainsubjective states (i.e. ‘subjective primary stressors’) such asfeeling overwhelmed or trapped in the care giver role. Theprimary stressors of care giving could also proliferate ‘sec-ondary stressors’ including strains in domains outside of caregiving such as family and work, as well as intrapsychic strainssuch as loss of self (Aneshensel et al., 1995). Thus, provid-ing care may jeopardize social relationships, employment,health, activities and interests (Harris, 1993, Opie, 1994) andthis, alongside the level and type of impairment, contributesto the mental and physical health of the care giver. TheStress Process Model is presented in Figure 7-1.
At the heart of the Stress Process Model is the obser-vation that care givers can experience seemingly similarobjective demands, yet demonstrate different levels ofsubjective burden and depression. The Stress ProcessModel hypothesises that mediators explain a large amountof this outcome variability. Coping and social support aregenerally regarded as the primary mediators, which canoperate to constrain the proliferation of stressors (Pearlinet al., 1990a). For example, care givers have been found tobenefit from coping strategies including acceptance, prob-lem focused coping styles that concentrate on managing thesituation, and self-efficacy, i.e. care givers’ confidence inmanaging the situation, as well as the perception of socialsupport (Chappell and Reid, 2002, Gilliam and Steffen,2006, Kneebone and Martin, 2003). The Stress ProcessModel teases apart the direct and indirect role of copingstrategies and social support in alleviating or increasing
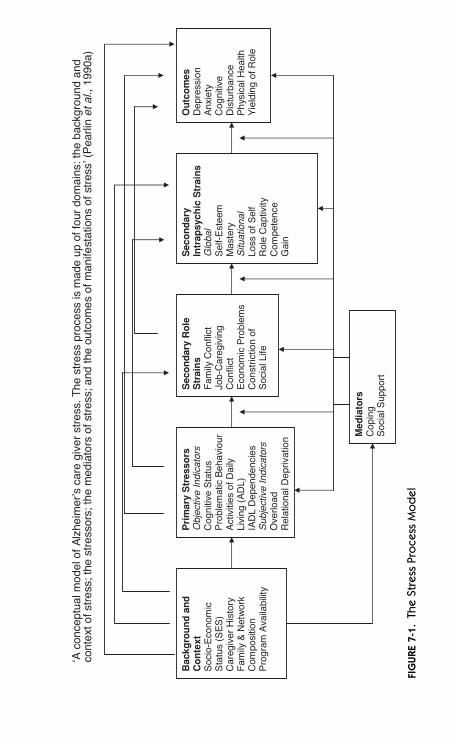
P1: IFM/OSW P2: TIXc07 JWBK439-Banerjee January 15, 2010 17:38 Printer Name: Yet to Come
‘A c
once
ptua
l mod
el o
f A
lzhe
imer
’s c
are
give
r st
ress
. The
str
ess
proc
ess
is m
ade
up o
f fou
r do
mai
ns: t
he b
ackg
roun
d an
dco
ntex
t of s
tres
s; th
e st
ress
ors;
the
med
iato
rs o
f str
ess;
and
the
outc
omes
of m
anife
stat
ions
of s
tres
s’ (
Pea
rlin
et a
l., 1
990a
)
Bac
kgro
un
d a
nd
C
on
text
S
ocio
-Eco
nom
ic
Sta
tus
(SE
S)
Car
egiv
er H
isto
ry
Fam
ily &
Net
wor
k C
ompo
sitio
n P
rogr
am A
vaila
bilit
y
Pri
mar
y S
tres
sors
Obj
ectiv
e In
dica
tors
Cog
nitiv
e S
tatu
s P
robl
emat
ic B
ehav
iour
A
ctiv
ities
of D
aily
Li
ving
(A
DL)
IA
DL
Dep
ende
ncie
s S
ubje
ctiv
e In
dica
tors
O
verlo
ad
Rel
atio
nal D
epriv
atio
n
Sec
on
dar
y R
ole
S
trai
ns
Fam
ily C
onfli
ct
Job-
Car
egiv
ing
Con
flict
E
cono
mic
Pro
blem
s C
onst
rictio
n of
S
ocia
l Life
Sec
on
dar
y In
trap
sych
ic S
trai
ns
Glo
bal
Sel
f-E
stee
m
Mas
tery
S
ituat
iona
l Lo
ss o
f Sel
f R
ole
Cap
tivity
C
ompe
tenc
e G
ain
Ou
tco
mes
Dep
ress
ion
Anx
iety
C
ogni
tive
Dis
turb
ance
P
hysi
cal H
ealth
Y
ield
ing
of R
ole
Med
iato
rs
Cop
ing
S
ocia
l Sup
port
FIG
URE
7-1.
The
Stre
ssPr
oce
ssM
od
el
62
P1: IFM/OSW P2: TIXc07 JWBK439-Banerjee January 15, 2010 17:38 Printer Name: Yet to Come
THE PERSPECTIVE OF THE FAMILY CARERS OF PEOPLE WITH DEMENTIA 63
carers’ emotional distress. Not only can they limit therelationship between aggregated stressors and outcomes,but also the progression of objective primary stressors tosubjective primary stressors, primary stressors to secondarystressors and so on (Aneshensel et al., 1995). By recognisingthat social and psychological resources can reduce stressproliferation, the Stress Process Model introduces valuableopportunities for clinical interventions (Aneshensel et al.,1995). For example, role training interventions aimed atadjusting care givers’ appraisal of their ability to managetheir situation have successfully reduced care giving burdenand depression (Hepburn et al., 2001). Formal services suchas respite care also promise to contain care giving stressesby limiting their intrusion into other areas of carers’ lives.
Aneshensel and colleagues (1995) also acknowledgedthat the stresses and strains of care giving do not occur in avacuum and that contextual variables such as gender, socio-economic resources, kin relationship, age and ethnicitymay also inform the care giving experience. For example,research has suggested that women experience higher levelsof burden and depression than male care givers, although itwould seem that this is subject to social change, as smallerdifferences appear in more recent studies (Pinquart andSorensen, 2006). There is also evidence that low socio-economic resources are associated with greater care giverdistress (Covinsky et al., 2003), although they have also beenassociated with less distress in African American carers(Roff et al., 2004, Lawton et al., 1992). The effects of cultureand ethnicity on care giving experiences will be discussedbelow. Notably, this will take the sociocultural stress andcoping model (Knight et al., 2000) as its starting point. Thismodel extends previous interpretations that have tradition-ally viewed the influence of ethnicity as being limited to thatof structural status characteristics akin to low income or lackof education. Instead, it suggests that ‘ethnicity as culture’influences are likely to affect each stage of the Stress ProcessModel simultaneously, and potentially, in different direc-tions (Knight et al., 2000). This model helps to explain whyAfrican American care givers have reported lower levelsof burden than white American care givers, despite their
P1: IFM/OSW P2: TIXc07 JWBK439-Banerjee January 15, 2010 17:38 Printer Name: Yet to Come
64 MANAGING DEMENTIA IN A MULTICULTURAL SOCIETY
disadvantaged socio-economic status (Knight et al., 2000).For instance, low socio-economic status among AfricanAmerican care givers might contribute to an experience ofadversity that helped to reframe difficult life experiencessuch as care giving more positively (Roff et al., 2004)
For over 20 years, the dominance of the Stress ProcessModel focused attention on the negative outcomes of car-ing for a person with dementia. However, evidence that car-ers can experience personal fulfilment, an improved sense ofself-worth, pride at developing skills, and a greater closenessin the relationship with the person with dementia (Motenko,1989, Braudy Harris, 1993, Murray et al., 1999) has grad-ually accumulated, and calls have been made for a morebalanced approach to investigating the care giving experi-ence (Motenko, 1989, Kramer, 1997, Lambardo, 2003). Un-derstanding these positive elements offers advantages, in-cluding helping clinicians to work more effectively with caregivers, providing insight into quality of care and advancingtheory on care giver adaptation (Kramer, 1997). A consen-sus has emerged that the positive and negative aspects ofcare giving are conceptually distinct (Lawton et al., 1991),and researchers have identified the need to study the pro-cesses separately (Long Foley et al., 2002). The focus onthe positive aspects of care giving has underlined the impor-tance of enhancing care giver rewards as well as amelioratingcare giver strains (Kramer, 1997). While there remains am-biguity regarding the determinants of care giver gain (Millerand Lawton, 1997), findings suggest that attitudinal vari-ables such as motivation for providing care (Kramer, 1997,Motenko, 1989) may play an important role.
ETHNICITY AND CULTURE AND THESTRESS PROCESS
The 1990s saw an increase in research exploring ethnicand cultural variations in dementia care giving. Culturalvariation exists in both the negative and positive out-comes of care giving (Janevic and Connell, 2001, Dilworth-Anderson et al., 2002). African American care givers havebeen found to experience less stress, burden and depression
P1: IFM/OSW P2: TIXc07 JWBK439-Banerjee January 15, 2010 17:38 Printer Name: Yet to Come
THE PERSPECTIVE OF THE FAMILY CARERS OF PEOPLE WITH DEMENTIA 65
than white care givers, and derive more benefit and meaningfrom the care giver experience (Haley et al., 1996, Arandaand Knight, 1997, Haley et al., 1995, Haley et al., 2004, Law-ton et al., 1992, Hinrichsen and Ramirez, 1992). Buildingupon a review of the literature on minority ethnic care givers(Aranda and Knight, 1997), Knight et al. (2000) proposed asocio-cultural stress and coping model, which hypothesisedthat the relationship between ethnicity and culture and theoutcomes of care giving was mediated by variation in in-formal support, coping strategies and appraisal of potentialstressors.
It has frequently been suggested that African Americancare givers experience lower levels of burden because of thesupport provided by tightly knit extended families (Woodand Parham, 1990). However, Levkoff et al. (1999) foundthat African American care givers often felt isolated in theircare giver role and that their psychosocial needs were unmetby church groups or extended family. Indeed, research hasincreasingly discounted the argument that extended kin andsocial networks protect African Americans from negativeconsequences (Wood and Wan, 1993, Haley et al., 1995, Foxet al., 1999, Dilworth-Anderson et al., 2002). Researchersin the UK have similarly challenged the assumption thatsouth Asian and black Caribbean carers are assured of sup-port from extended families (Bowes and Wilkinson, 2003,Katbamna et al., 2004, Milne and Chryssanthopoulou, 2005).However, there is evidence of variation in coping responsesacross ethnic groups: white care givers have been shownto use more avoidance and approach coping (Haley et al.,1995, Wykle and Seagall, 1991), while black care givers havebeen reported as relying on prayer, religion and faith (Segallet al., 1998, Wood and Parham, 1990). There is evidencethat African American care givers regard God as an equalsource of informal support to family and friends (Wood andParham, 1990, Sterritt and Pokorny, 1998). Lastly, researchsuggests that ethnicity influences the appraisal of stressors.Black care givers have been shown to appraise specific mem-ory and behavioural issues as being less stressful than whitecare givers (Haley et al., 1996, Farran et al., 1997, Miller et al.,1995).
P1: IFM/OSW P2: TIXc07 JWBK439-Banerjee January 15, 2010 17:38 Printer Name: Yet to Come
66 MANAGING DEMENTIA IN A MULTICULTURAL SOCIETY
This is helpful in building a picture of the differentvariables that influence the relationship between ethnicityand care giver well being. Unfortunately, it tells us littleabout why ethnicity is related to differences in appraisaland coping mechanisms. A common explanation for theseethnic differences is that African American care givers aremore likely to hold the care giver ideology of ‘taking care ofone’s own’ (Wood and Wan, 1993). This has been identifiedas a heavily quoted, yet essentially untested hypothesis(Toth-Cohen, 2004). A growing body of literature revealsa cluster of cultural beliefs that shape the appraisal of caregiving and choice of coping behaviours. In 1992, Lawtonassociated favourable care giving appraisals among blackcare givers with what he termed a ‘traditional care givingideology’, which he defined as a wish to:
� repay the care recipient for previous actions;� continue family traditions;� fulfil personal values; and� set a good example to children.
Subsequently, research has hypothesised that black caregivers are more likely to:� view care giving as a culturally normative process (Haley
et al., 1996);� have a stronger preference for family care (Long Foley
et al., 2002);� have higher levels of “familism” (Kim et al., 2006, Rozario
and DeRienzis, 2009); and� have a stronger cultural justification for care giving
(Dilworth-Anderson et al., 2005).
Others have speculated that cultural differences in identityand definitions of the self may underlie the choice of copingbehaviours (Aranda and Knight, 1997, Pyke and Bengston,1996, Landrine and Klonoff, 1992). Dilworth-Andersonet al. (2005) approach variability within cultural groups byadopting the concept of a ‘cultural frame’ (Goodenough,1999), which acknowledges that individuals’ characteristicsand experiences interact with the norms and expectationsperceived to exist within the wider group. This is useful when
P1: IFM/OSW P2: TIXc07 JWBK439-Banerjee January 15, 2010 17:38 Printer Name: Yet to Come
THE PERSPECTIVE OF THE FAMILY CARERS OF PEOPLE WITH DEMENTIA 67
considering that cultural attitudes towards care giving mayrepresent a generational phenomenon (Long Foley et al.,2002), and that acculturation may lead to conflicting val-ues and beliefs within ethnic groups (Burton and Sorensen,1993, Youn et al., 1999).
In the UK, research has supported the view that care giv-ing is positioned as the ‘norm’ within south Asian families(Bowes and Wilkinson, 2003, Adamson, 2001). In one of thefew studies of its kind, Adamson and Donovan (2005) con-cluded that south Asian and black Caribbean carers drawupon their ethnic identity to make sense of their situation.Yet how cultural values and beliefs effect the wider care giv-ing experience has rarely been explored in the UK. Little at-tention has been given to the implications that they may holdfor health and social care providers, despite suggestions thatfamilial attitudes towards care giving, and the ensuing wayin which they appraise and adjust to the role, should informthe support that is offered (Murray and Livingston, 1998).
In-depth discussions with African American care giverssuggest that ‘the symbolic figure of the African Americancare giver as an unconditionally loyal, self-satisfied, less bur-dened servant’ was a myth (Fox et al., 1999). The assump-tion of the same characteristics in south Asian and blackCaribbean families in the UK is likely to be similarly mythic,however comforting for those planning, purchasing and de-livering services.
APPROPRIATENESS OF SERVICES
How appropriate are health and social care services for peo-ple with dementia and care givers across ethnic groups? Whydo people with dementia and care givers not use availableformal support services (Collins et al., 1994, Gwyther, 1994,Lawton et al., 1989a) that have proven efficacy in reliev-ing stress in family care givers and delaying or preventinginstitutionalisation of the person with dementia (Maslow,1990, Zarit et al., 1999)? It is well established that familycare givers play a pivotal role in initiating and maintainingservice use not only for themselves, but also for their cog-nitively impaired relatives. Why are members of minority
P1: IFM/OSW P2: TIXc07 JWBK439-Banerjee January 15, 2010 17:38 Printer Name: Yet to Come
68 MANAGING DEMENTIA IN A MULTICULTURAL SOCIETY
ethnic groups even less likely to access dementia care (Raitand Burns, 1997) or social care services (Social ServicesDirectorate, 1998, Social Services Directorate, 2001) thantheir white counterparts?
UNDERSTANDING OF DEMENTIA ACROSSETHNIC GROUPS
As previously indicated the meanings that individuals attachto symptoms are influential in their evaluation and deter-mine the action that is taken. Indeed the perception of illnesscan be considered the first step in help seeking behaviour(Young, 2004). The meaning of symptoms and help seekingdecisions are constructed within social networks comprisingfamily and friends (Pescosolido, 1992). It is widely acceptedthat this is especially so in the case of dementia and thatfamily care givers play a crucial role in initiating service use(Adamson, 2001). Culture and ethnicity are also highly in-fluential in this illness labelling process (Angel and Thoits,1987). Relatives may attribute symptoms such as memoryloss to old age (Pollitt, 1996) or may not consciously considerthe possibility of dementia out of respect for their spouseor parent (Antonelli et al., 1992). It has been suggested thatsouth Asian and black Caribbean families in the UK are lesslikely to identify symptoms of dementia than the populationas a whole (Adamson, 2001, Bowes and Wilkinson, 2003).Health care professionals have described a ‘cultural clash’with south Asian relatives who often conceptualise symp-toms of dementia as a ‘normal’ part of the ageing process(Patel and Mirza, 2000), and as such, natural and untreat-able (Milne, 2002).
However, there is also evidence that dementia isassociated with stigma and shame within south Asiancommunities, and this may account for an unwillingnessto acknowledge dementia (Bowes and Wilkinson, 2003)and the desire to minimise contact between people withdementia and health care providers and even membersof the wider family (Seabrooke and Milne, 2004). Carersin a Gujarati community in north London feared that de-mentia would have negative repercussions on the marriage
P1: IFM/OSW P2: TIXc07 JWBK439-Banerjee January 15, 2010 17:38 Printer Name: Yet to Come
THE PERSPECTIVE OF THE FAMILY CARERS OF PEOPLE WITH DEMENTIA 69
prospects of their children (Brownfoot, 1998). Older adultsin Goa attributed dementia to abuse, neglect, or lack oflove on the part of children towards a parent (Patel andPrince, 2001). The apparent propensity among BritishAsian (Patel et al., 1998) and African American populations(Gallagher et al., 2000) to interpret dementia as ‘an act ofGod’ may similarly limit service use. In the US, AfricanAmericans have been found to attribute cognitive deficits toexcessive worrying or ‘thinking too much’ (Gaines, 1989).These varied conceptualisations and attributions serve toposition formal support as either irrelevant or undesirable.Conversely, a study of help seeking across minority ethnicgroups revealed that African American care givers fre-quently adopted a biomedical model of attribution (Levkoffet al., 1999). Despite this, many only sought help followingdangerous incidents whereby the person with dementia hadplaced himself or herself at risk, e.g. wandering at night.
CULTURAL KNOWLEDGE, ATTITUDES ANDBELIEFS ABOUT FORMAL SUPPORT
Preference for family care has been cited as the most power-ful component of care giver attitudes in predicting the use offormal services within the community (Collins et al., 1991).Families may feel it is their responsibility to support theirrelative and feel guilty about potentially relinquishing careto others (Aneshensel et al., 1995). The propensity withinminority ethnic groups to identify care giving as a duty islikely to propagate these concerns. It has also been sug-gested that some south Asian carers interpret offers of ser-vice support as a criticism of the quality of care that they areproviding (Jewson et al., 2003).
Carers make subtle judgements about the costs and ben-efits of accepting help and are likely to reject services thatare incompatible with their own perceived needs (Nolanet al., 2002). Zarit and Leitsch (2001) identified the needfor researchers to enter into a ‘meaningful dialogue’ withcarers in an effort to understand their complex needs andthe process by which they access services. It is highly likelythat perceived appropriateness of services will indeed differ
P1: IFM/OSW P2: TIXc07 JWBK439-Banerjee January 15, 2010 17:38 Printer Name: Yet to Come
70 MANAGING DEMENTIA IN A MULTICULTURAL SOCIETY
across ethnic groups. Traditional and complementarymedicines are practised in the UK alongside the establishedWestern medical approach, and cultural beliefs around ap-propriate treatment may prompt members of minority eth-nic groups to consult a healer rather than a GP about theirillness (Campion and Bhugra, 1998). In relation to care op-tions, there is considerable evidence that residential homesare considered inappropriate to the needs of south Asianpeople by south Asians themselves (Bowes and Wilkinson,2003, Seabrooke and Milne, 2004). However south Asiancarers, like those in the majority population, have also ex-pressed a desire for respite breaks (Patel and Mirza, 2000,Seabrooke and Milne, 2004). In an exploration of the viewsand experiences of south Asian families living in Scotland,families stated a strong preference for caring for their rela-tives at home, but communicated a serious need for servicesupport to do this (Bowes and Wilkinson, 2003).
Gujarati carers in North London have described theirunsatisfactory experiences of statutory services. They statedthat home help provided through social services lackedawareness of cultural practices and many opted instead topay for their own Asian domiciliary assistance privately(Brownfoot, 1998). Gujarati carers communicated a desireto have culturally sensitive Asian organised and staffed ser-vices that were separate from the mainstream provision. Incontrast Caribbean carers expressed concern that this mightlead to a marginalized, segregated service. However, theytoo wanted services to be culturally sensitive (Brownfoot,1998). Levkoff found that African American care givers re-lied on mainstream services, but expressed dissatisfactionwith the support due to cultural misunderstandings (Levkoffet al., 1999). Furthermore, it has been argued that amongstAfrican American care givers, distrust of mainstream careproviders may preclude their seeking help outside the family(Elliot et al., 1996). Research also suggests a fear of psychi-atric services within south Asian and black Caribbean com-munities in the UK (Patel and Mirza, 2000).
The availability of services, how accessible they areand individual’s knowledge of their existence and how toaccess them is likely to set parameters on the use of formal
P1: IFM/OSW P2: TIXc07 JWBK439-Banerjee January 15, 2010 17:38 Printer Name: Yet to Come
THE PERSPECTIVE OF THE FAMILY CARERS OF PEOPLE WITH DEMENTIA 71
services. There is evidence that carers are not always awareof the services available to them (Toseland et al., 1999)and that a lack of knowledge can create extra barriers forminority ethnic older people and their families (Ahmad andAtkin, 1996, Boneham et al., 1997, Katbamna et al., 2004).Language and communication difficulties can also make itdifficult for some south Asian family members to organisesocial care (Katbamna et al., 2004). Beattie et al. (2005)highlight the absence of choice as a fundamental issue forpeople with dementia within minority ethnic groups. Thereare reports of limited availability of culturally sensitiverespite services (Jewson et al., 2003) and difficulties withtransport often prohibit their use. A shortage of specialistservices for people with dementia in general (Audit Com-mission, 2000) means that people with dementia are often‘shoved in where there is a vacancy’ (Beattie et al., 2005).

P1: IFM/OSW P2: TIXc07 JWBK439-Banerjee January 15, 2010 17:38 Printer Name: Yet to Come
72
P1: TIX/OSW P2: TIXc08 JWBK439-Banerjee January 14, 2010 14:34 Printer Name: Yet to Come
8QUALITATIVE ENQUIRY IN
THE EXPERIENCES OFPEOPLE WITH DEMENTIA
AND THEIR FAMILYCARERS
NEW RESEARCH
In the light of the gaps in the evidence base identifiedabove, we completed a qualitative study to attempt to ex-plore the subjective reality of living with dementia and car-ing for a person with dementia within multicultural Britain.A grounded theory approach was used to investigate the di-versity of experiences of black Caribbean, south Asian andwhite British people with dementia and their carers withinSouth London. In-depth individual interviews were con-ducted with 30 people with dementia (11 black Caribbean,9 south Asian and 10 white British) and 32 carers of peoplewith dementia (10 black Caribbean, 10 south Asian and 12white British). Constant comparison analysis of the data ledto the emergence of separate theories for people with de-mentia and their carers. The interviews with the people withdementia centred on the main problem, ‘threat to valued el-ements of life’. This involved a process of appraisal in which
Managing Dementia in a Multicultural Society Sube Banerjee and Vanessa LawrenceC© 2010 John Wiley & Sons, Ltd
73
P1: TIX/OSW P2: TIXc08 JWBK439-Banerjee January 14, 2010 14:34 Printer Name: Yet to Come
74 MANAGING DEMENTIA IN A MULTICULTURAL SOCIETY
the individual’s ‘understanding of the condition’ and ‘atti-tudes surrounding support needs’ determined the perceivedthreat to ‘valued elements of life’. Participants used copingstrategies that focused on ‘constancy’ and ‘change’ in val-ued elements of life to manage the threat that the conditionposed. Cultural values and beliefs were influential at eachstage in this process. Carers were categorised as holding ei-ther a traditional or non-traditional ‘care giving ideology’ ac-cording to whether or not they conceptualised care giving asnatural, expected and virtuous. This informed the ‘continu-ity and rewards’ experienced in the care giving role, ‘cop-ing strategies’, ‘informal support’, ‘nature of the care givingrole’ and attitudes towards ‘formal support’. These will bediscussed further below considering their joint implicationsfor providing culturally appropriate care.
DATA COLLECTION
In-depth individual interviews were conducted with blackCaribbean, south Asian and white British people with de-mentia and their carers. The lack of information in this areaprompted the use of the grounded theory approach, whichoffers a rigorous, orderly guide for generating theory fromdata (Glaser and Strauss, 1967). People with dementia wererecruited from a diverse range of sources including Com-munity Mental Health Teams for Older Adults, a memoryclinic, a south Asian community mental health programmeand a faith-based mental health project for ethnic minorityolder adults. Participants either had a formal diagnosis ofdementia or were attending a dementia specific day-centreor group. The research team was mindful that membersof ethnic minority groups (or the white British majority)might not frame their experience of dementia within thewestern medical model. Therefore, the expression ‘memoryproblems’ was used in place of ‘dementia’, as this did notrequire participants to be aware of a formal diagnosis oridentify with a potentially stigmatising and/or western con-cept. Recruitment was conducted within four socially andethnically diverse south London boroughs. Caregivers wererecruited through Community Mental Health Teams forOlder Adults, carer services and organisations (eg Lambeth
P1: TIX/OSW P2: TIXc08 JWBK439-Banerjee January 14, 2010 14:34 Printer Name: Yet to Come
QUALITATIVE ENQUIRY IN THE EXPERIENCES OF PEOPLE 75
Crossroads, Alzheimer’s Society Croydon), and communityservices aimed at serving black and minority ethnic groups(eg Charisma, a Croydon based project for older adults fromethnic minority groups with mental health problems and de-mentia). Recruitment continued until theoretical saturationwas reached, that is until no significant new themes wereemerging.
Qualitative interviews – people with dementia
The combination of structure and flexibility that charac-terises in-depth interviews promised to help orientate theolder adults, but also to allow the researchers to adjust thepace and complexity of the interview to each participant.A set of open-ended questions was devised in consultationwith experts in dementia and cross-cultural psychiatry. Theinterview guide was amended iteratively and aimed to fol-low the participants’ own concerns. Initial topics included:the experience, impact and understanding of the conditionand participant’s priorities and fears. Questions loosely fellinto three clusters:
� The first related to a vignette, which depicted a man withmoderate dementia: this was used to facilitate discussionon this sensitive topic and provided a culturally unbiasedsituation to which everyone could respond.
� Second, participants were asked questions regarding theirown condition.
� Third, generic questions were posed in relation to ‘demen-tia’ and ‘Alzheimer’s Disease’.
Individuals’ responses to the vignette and dementia pro-vided additional layers of insight into how they conceptu-alised their own situation. In instances where participantswere judged to lack capacity to consent, we sought the as-sent of their main carer and only proceeded if the personwith dementia was happy to do so.
Qualitative Interviews – carers
The interview guide was generated from a review of the lit-erature and expert consultation. Initial topics included: the
P1: TIX/OSW P2: TIXc08 JWBK439-Banerjee January 14, 2010 14:34 Printer Name: Yet to Come
76 MANAGING DEMENTIA IN A MULTICULTURAL SOCIETY
help-seeking pathway, nature of the care giving role, copingstrategies, attitudes towards the future, informal support,service use and evaluation. Questions were open-ended andrevised iteratively, allowing further exploration of the issuesraised e.g. the theme ‘fulfilment’ was introduced by partici-pants and subsequently explored. Interviews were con-ducted in people’s homes, unless participants stated apreference to be seen elsewhere. They lasted around onehour and were conducted in the participants’ preferredlanguage. Interviews were recorded on audiotape andtranscribed verbatim.
DATA ANALYSIS
Three of the researchers (VL, JM, KS) read the first fivetranscripts repeatedly to immerse themselves in the data;they then independently separated the data into meaningfulfragments and emerging themes were identified and labelledwith descriptive codes. They compared their individual cod-ing frames until a consensus was reached. VL then appliedthe constant comparison method to delineate the similar-ities and differences between codes; from this, conceptualcategories were formed (e.g. ‘continuity in relationship/life’,‘care giving rewards’, ‘level of responsibility’). Data collec-tion and analysis occurred simultaneously and different per-spectives were purposefully sought to test and refine theemergent theory e.g. ethnic minority carers born in the UKwere purposefully recruited on the basis that they may pos-sess less traditional attitudes towards the care giving role.Throughout the analysis, ideas about themes and their rela-tionships were recorded in theoretical memos and discussedat regular intervals with the research team.
RESULTS
Thirty people with dementia were interviewed: 11 wereblack Caribbean (3 male, 8 female), 9 south Asian (5 male,4 female) and 10 white British (5 male, 5 female). Thirty-twocarers participated in an interview: 10 were black Caribbean(9 female, 1 male), 10 south Asian (5 female, 5 male) and
P1: TIX/OSW P2: TIXc08 JWBK439-Banerjee January 14, 2010 14:34 Printer Name: Yet to Come
QUALITATIVE ENQUIRY IN THE EXPERIENCES OF PEOPLE 77
12 white British (11 female, 1 male). The sample captureda variety of caring relationships and ages (ranging from 33to 87). Their characteristics are presented in Tables 8-1 and8-2.
Priority was given to uncovering the participants’ mainconcerns and the emphasis shifted away from identifying at-titudes and beliefs that prevented service use.
Findings – people with dementia
It became evident that the interviews with the people withdementia were centred on the main problem, ‘threat to val-ued elements of life’. Three key findings emerged:
1. The people with dementia appeared to engage in a pro-cess of appraisal in which they assessed the threat thatdementia related changes held for their lives. This wasinformed by the person with dementia’s ‘understandingof the condition’, ‘attitudes surrounding support needs’and the individual’s ‘valued elements of life’. Within ‘un-derstanding of the condition’, the belief that the condi-tion was serious, progressive and stigmatised, increasedthe threat to valued elements of life. Within ‘attitudessurrounding support needs’, the belief that the supportwas unavailable, unacceptable, and that alternatives werenecessary, yet undesirable, compounded this threat. Ulti-mately, the level of threat varied from individual to indi-vidual, as participants appraised how their condition andsupport needs might interfere with the valued elementsof life.
2. The findings indicated that people with dementia ac-tively sought to manage the ‘threat to valued elementsof life’. Older adults used two groups of coping strate-gies to manage the threat of dementia: the first focussedon constancy, the second on change. Identifying past andpresent abilities/roles, normalisation and minimisationhelped participants to focus on the valued elements oflife that remained unchanged. Participants displayed ac-knowledgment of the changes that had occurred in theirknowledge, feelings, and behavioural response to their
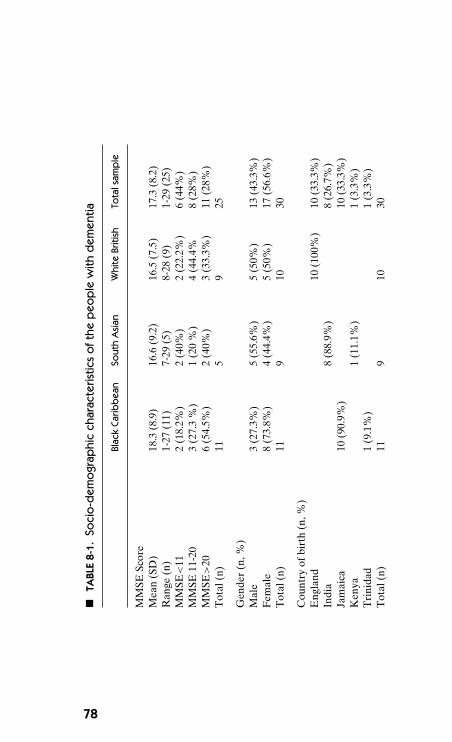
P1: TIX/OSW P2: TIXc08 JWBK439-Banerjee January 14, 2010 14:34 Printer Name: Yet to Come
�TA
BLE
8-1.
Soci
o-d
emo
grap
hic
char
acte
ristic
so
fthe
peo
ple
with
dem
entia
Blac
kCa
ribb
ean
Sout
hA
sian
Whi
teBr
itish
Tota
lsam
ple
MM
SESc
ore
Mea
n(S
D)
18.3
(8.9
)16
.6(9
.2)
16.5
(7.5
)17
.3(8
.2)
Ran
ge(n
)1-
27(1
1)7-
29(5
)8-
28(9
)1-
29(2
5)M
MSE
<11
2(1
8.2%
)2
(40%
)2
(22.
2%)
6(4
4%)
MM
SE11
-20
3(2
7.3
%)
1(2
0%
)4
(44.
4%8
(28%
)M
MSE
>20
6(5
4.5%
)2
(40%
)3
(33.
3%)
11(2
8%)
Tot
al(n
)11
59
25
Gen
der
(n,%
)M
ale
3(2
7.3%
)5
(55.
6%)
5(5
0%)
13(4
3.3%
)F
emal
e8
(73.
8%)
4(4
4.4%
)5
(50%
)17
(56.
6%)
Tot
al(n
)11
910
30
Cou
ntry
ofbi
rth
(n,%
)E
ngla
nd10
(100
%)
10(3
3.3%
)In
dia
8(8
8.9%
)8
(26.
7%)
Jam
aica
10(9
0.9%
)10
(33.
3%)
Ken
ya1
(11.
1%)
1(3
.3%
)T
rini
dad
1(9
.1%
)1
(3.3
%)
Tot
al(n
)11
910
30
78
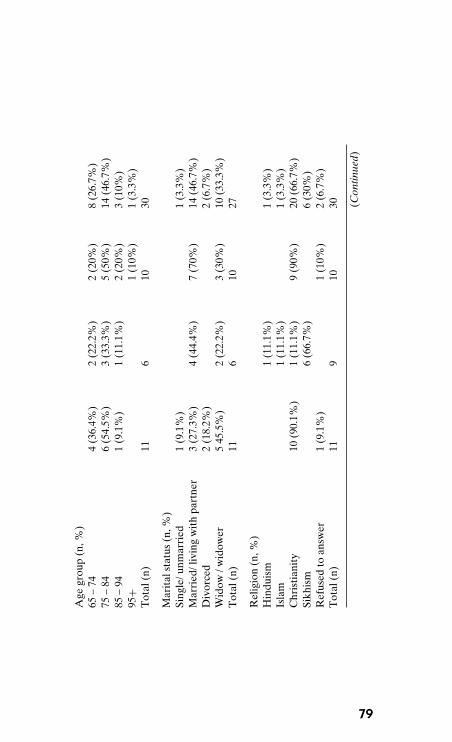
P1: TIX/OSW P2: TIXc08 JWBK439-Banerjee January 14, 2010 14:34 Printer Name: Yet to Come
Age
grou
p(n
,%)
65–
744
(36.
4%)
2(2
2.2%
)2
(20%
)8
(26.
7%)
75–
846
(54.
5%)
3(3
3.3%
)5
(50%
)14
(46.
7%)
85–
941
(9.1
%)
1(1
1.1%
)2
(20%
)3
(10%
)95
+1
(10%
)1
(3.3
%)
Tot
al(n
)11
610
30
Mar
ital
stat
us(n
,%)
Sing
le/u
nmar
ried
1(9
.1%
)1
(3.3
%)
Mar
ried
/liv
ing
wit
hpa
rtne
r3
(27.
3%)
4(4
4.4%
)7
(70%
)14
(46.
7%)
Div
orce
d2
(18.
2%)
2(6
.7%
)W
idow
/wid
ower
545
.5%
)2
(22.
2%)
3(3
0%)
10(3
3.3%
)T
otal
(n)
116
1027
Rel
igio
n(n
,%)
Hin
duis
m1
(11.
1%)
1(3
.3%
)Is
lam
1(1
1.1%
)1
(3.3
%)
Chr
isti
anit
y10
(90.
1%)
1(1
1.1%
)9
(90%
)20
(66.
7%)
Sikh
ism
6(6
6.7%
)6
(30%
)R
efus
edto
answ
er1
(9.1
%)
1(1
0%)
2(6
.7%
)T
otal
(n)
119
1030 (C
ontin
ued)
79
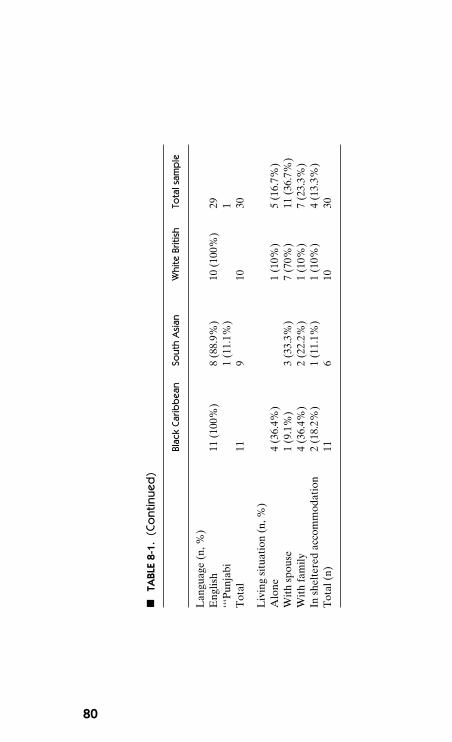
P1: TIX/OSW P2: TIXc08 JWBK439-Banerjee January 14, 2010 14:34 Printer Name: Yet to Come
�TA
BLE
8-1.
(Co
ntin
ued
)
Blac
kCa
ribb
ean
Sout
hA
sian
Whi
teBr
itish
Tota
lsam
ple
Lan
guag
e(n
,%)
Eng
lish
11(1
00%
)8
(88.
9%)
10(1
00%
)29
‘‘‘P
unja
bi1
(11.
1%)
1T
otal
119
1030
Liv
ing
situ
atio
n(n
,%)
Alo
ne4
(36.
4%)
1(1
0%)
5(1
6.7%
)W
ith
spou
se1
(9.1
%)
3(3
3.3%
)7
(70%
)11
(36.
7%)
Wit
hfa
mily
4(3
6.4%
)2
(22.
2%)
1(1
0%)
7(2
3.3%
)In
shel
tere
dac
com
mod
atio
n2
(18.
2%)
1(1
1.1%
)1
(10%
)4
(13.
3%)
Tot
al(n
)11
610
30
80
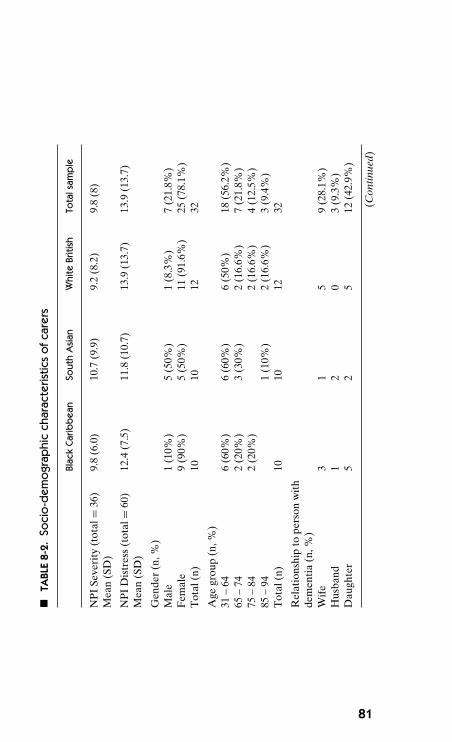
P1: TIX/OSW P2: TIXc08 JWBK439-Banerjee January 14, 2010 14:34 Printer Name: Yet to Come
�TA
BLE
8-2.
Soci
o-d
emo
grap
hic
char
acte
ristic
so
fcar
ers
Blac
kCa
ribb
ean
Sout
hA
sian
Whi
teBr
itish
Tota
lsam
ple
NP
ISe
veri
ty(t
otal
=36
)M
ean
(SD
)9.
8(6
.0)
10.7
(9.9
)9.
2(8
.2)
9.8
(8)
NP
ID
istr
ess
(tot
al=
60)
Mea
n(S
D)
12.4
(7.5
)11
.8(1
0.7)
13.9
(13.
7)13
.9(1
3.7)
Gen
der
(n,%
)M
ale
1(1
0%)
5(5
0%)
1(8
.3%
)7
(21.
8%)
Fem
ale
9(9
0%)
5(5
0%)
11(9
1.6%
)25
(78.
1%)
Tot
al(n
)10
1012
32
Age
grou
p(n
,%)
31–
646
(60%
)6
(60%
)6
(50%
)18
(56.
2%)
65–
742
(20%
)3
(30%
)2
(16.
6%)
7(2
1.8%
)75
–84
2(2
0%)
2(1
6.6%
)4
(12.
5%)
85–
941
(10%
)2
(16.
6%)
3(9
.4%
)T
otal
(n)
1010
1232
Rel
atio
nshi
pto
pers
onw
ith
dem
enti
a(n
,%)
Wif
e3
15
9(2
8.1%
)H
usba
nd1
20
3(9
.3%
)D
augh
ter
52
512
(42.
9%)
(Con
tinue
d)
81
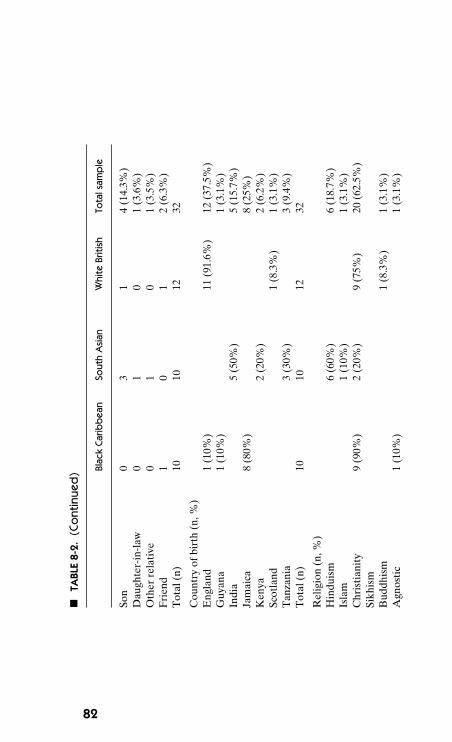
P1: TIX/OSW P2: TIXc08 JWBK439-Banerjee January 14, 2010 14:34 Printer Name: Yet to Come
�TA
BLE
8-2.
(Co
ntin
ued
) Blac
kCa
ribb
ean
Sout
hA
sian
Whi
teBr
itish
Tota
lsam
ple
Son
03
14
(14.
3%)
Dau
ghte
r-in
-law
01
01
(3.6
%)
Oth
erre
lati
ve0
10
1(3
.5%
)F
rien
d1
01
2(6
.3%
)T
otal
(n)
1010
1232
Cou
ntry
ofbi
rth
(n,%
)E
ngla
nd1
(10%
)11
(91.
6%)
12(3
7.5%
)G
uyan
a1
(10%
)1
(3.1
%)
Indi
a5
(50%
)5
(15.
7%)
Jam
aica
8(8
0%)
8(2
5%)
Ken
ya2
(20%
)2
(6.2
%)
Scot
land
1(8
.3%
)1
(3.1
%)
Tan
zani
a3
(30%
)3
(9.4
%)
Tot
al(n
)10
1012
32
Rel
igio
n(n
,%)
Hin
duis
m6
(60%
)6
(18.
7%)
Isla
m1
(10%
)1
(3.1
%)
Chr
isti
anit
y9
(90%
)2
(20%
)9
(75%
)20
(62.
5%)
Sikh
ism
Bud
dhis
m1
(8.3
%)
1(3
.1%
)A
gnos
tic
1(1
0%)
1(3
.1%
)
82
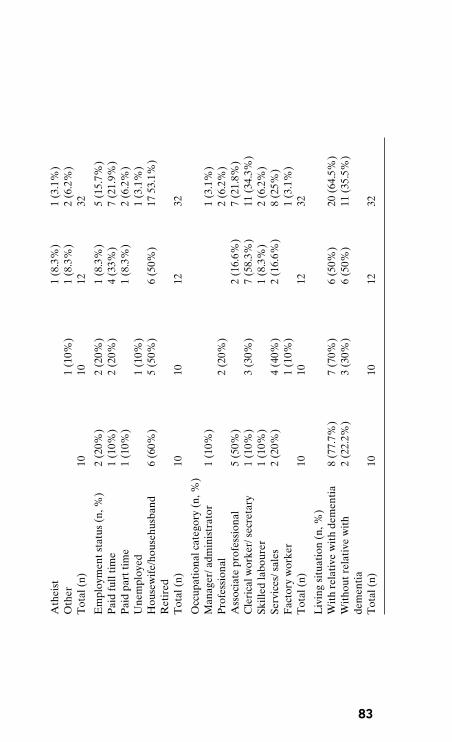
P1: TIX/OSW P2: TIXc08 JWBK439-Banerjee January 14, 2010 14:34 Printer Name: Yet to Come
Ath
eist
1(8
.3%
)1
(3.1
%)
Oth
er1
(10%
)1
(8.3
%)
2(6
.2%
)T
otal
(n)
1010
1232
Em
ploy
men
tsta
tus
(n,%
)2
(20%
)2
(20%
)1
(8.3
%)
5(1
5.7%
)P
aid
full
tim
e1
(10%
)2
(20%
)4
(33%
)7
(21.
9%)
Pai
dpa
rtti
me
1(1
0%)
1(8
.3%
)2
(6.2
%)
Une
mpl
oyed
1(1
0%)
1(3
.1%
)H
ouse
wif
e/ho
useh
usba
ndR
etir
ed6
(60%
)5
(50%
)6
(50%
)17
53.1
%)
Tot
al(n
)10
1012
32
Occ
upat
iona
lcat
egor
y(n
,%)
Man
ager
/adm
inis
trat
or1
(10%
)1
(3.1
%)
Pro
fess
iona
l2
(20%
)2
(6.2
%)
Ass
ocia
tepr
ofes
sion
al5
(50%
)2
(16.
6%)
7(2
1.8%
)C
leri
calw
orke
r/se
cret
ary
1(1
0%)
3(3
0%)
7(5
8.3%
)11
(34.
3%)
Skill
edla
bour
er1
(10%
)1
(8.3
%)
2(6
.2%
)Se
rvic
es/s
ales
2(2
0%)
4(4
0%)
2(1
6.6%
)8
(25%
)F
acto
ryw
orke
r1
(10%
)1
(3.1
%)
Tot
al(n
)10
1012
32
Liv
ing
situ
atio
n(n
,%)
Wit
hre
lati
vew
ith
dem
enti
a8
(77.
7%)
7(7
0%)
6(5
0%)
20(6
4.5%
)W
itho
utre
lati
vew
ith
dem
enti
a2
(22.
2%)
3(3
0%)
6(5
0%)
11(3
5.5%
)
Tot
al(n
)10
1012
32
83
P1: TIX/OSW P2: TIXc08 JWBK439-Banerjee January 14, 2010 14:34 Printer Name: Yet to Come
84 MANAGING DEMENTIA IN A MULTICULTURAL SOCIETY
condition. Strategies focussing on constancy and changewere most effective when used concurrently, yet the dataindicated that people with dementia struggled to obtainthe necessary equilibrium. Informal and formal care alsohad the potential to threaten or support valued elementsof life.
3. The findings revealed that the ‘threat to valued elementsof life’ differed across ethnic groups, as the individual’sconcept of the condition, attitudes towards support needs,and valued elements of life were firmly rooted in the in-dividual’s cultural background. Cultural values were sim-ilarly reflected in the person with dementia’s response tothe condition.
Findings – carers
Within the caregiver data, ‘caregiver ideology’ emerged asthe main theme that accounted for most of the variation incaregiver experiences. In summary:
1. Carers were categorised as holding either a traditional ornon-traditional caregiving ideology according to whetheror not they conceptualised caregiving as natural, expectedand virtuous. The majority of south Asian, half the blackCaribbean and a minority of white British participantswere found to possess a traditional ideology.� Identifying caregiving as natural helped ‘traditional’
carers to accommodate change, which in turn helpedthem to maintain continuity and rewards in their rela-tionship with the person with dementia and their livesas a whole. Conversely, ‘non-traditional’ carers experi-enced a pervasive sense of conflict and were less likelyto derive rewards from the caregiving relationship orfrom the caregiving role itself.
� Those with a traditional approach to caregiving viewedaccepting change as a precursor to adapting to it. Theyoften held strong religious beliefs, demonstrated a ten-dency to reconcile caregiving with their stage in life,and were concerned that circumstances might preventthem from continuing in the caregiving role. Among
P1: TIX/OSW P2: TIXc08 JWBK439-Banerjee January 14, 2010 14:34 Printer Name: Yet to Come
QUALITATIVE ENQUIRY IN THE EXPERIENCES OF PEOPLE 85
carers with non-traditional ideologies, acceptance wasmore closely aligned to resignation and endurance, anda number were worried about the indefinite nature ofcaregiving.
� Carers’ ideologies seemed to influence, as well as tobe shaped by, the perception of informal support.‘Non-traditional’ carers frequently reported that familymembers were unsupportive and critical of their deci-sion to provide care. Carers with traditional ideologieswere more likely to feel supported in the role.
� Carers with a non-traditional ideology attached greaterimportance to protecting non-caregiving roles, whichled to both fulfilment and role conflict. Many felt over-whelmed and trapped in the caregiver role. Many ‘tra-ditional’ carers implicitly prioritised the care recipients’needs over their own, and a small number of southAsian carers construed help seeking as a failure to fulfiltheir personal responsibility.
� As with informal support, carers with a traditionalideology expressed greater confidence than ‘non-traditional’ carers in the availability of formal support.The perception of support provided greater comfortthan actual support, which they were keen to limit.However, both ‘traditional’ and ‘non-traditional’ car-ers likened the initial help seeking process to a battlein which they were required to fight to receive informa-tion, advice, and practical assistance. Carers with non-traditional ideologies often lacked the resources to pur-sue the help they needed.
� There was consensus across the sample regarding whatconstituted good care. Carers wanted services and sup-port that listened and responded to their individualneeds. Carers evaluated services on the basis of fourcriteria: whether they served an emotional or practicalfunction for the person with dementia or themselves.Home respite services, e.g. Crossroads, and on occa-sion, day centres, met all four of these criteria; how-ever, in most cases, carers were forced to weigh up theperson with dementia’s needs and wants against theirown.
P1: TIX/OSW P2: TIXc08 JWBK439-Banerjee January 14, 2010 14:34 Printer Name: Yet to Come
86 MANAGING DEMENTIA IN A MULTICULTURAL SOCIETY
2. Caregiving ideology was conceived as a philosophy ofcaregiving that was embedded in cultural values (Lawtonet al., 1989) and this is reinforced by the findings of thisresearch, which views caregiving ideology as originat-ing in the collectivism-individualism dimension. This isa widely studied concept of cultural differences that hasbeen shown to differ across ethnic groups.
Thus, the research proposed two models for understand-ing the behaviour of people with dementia and their carerswithin black Caribbean, south Asian and white British com-munities. The two theories have identified processes that ap-ply across the ethnic groups and cultural patterns that occurwithin them, both of which can help to shape culturallyappropriate care.
ONE RESEARCH PROJECT, TWO THEORIES
The data from the interviews with the people with demen-tia and the data from the interviews with care givers weretreated separately, as the two groups of participants raisedseparate worries and concerns. The interviews with the peo-ple with dementia, but not the care givers, revolved aroundthe threat that the condition posed to their identity. Con-versely, the interviews with the care givers revolved aroundperforming the care giving role. Put simply, the focus of theinterviews was on ‘living with dementia’ and ‘living with caregiving’ respectively. Thus, the data are informative in high-lighting two parallel sets of experiences in relation to thecommon experience of dementia. The two theories sharesimilarities and these will be considered, but they cannotusefully be explained by one overarching theme.
The findings are unequivocal that people with demen-tia and carers of people with dementia each have their ownneeds and concerns that should be addressed separately.This is supportive of UK policy, as set out in the Carersand Disabled Children Act, 2000 (Office of Public SectorInformation, 2000), which states that all carers have a rightto a needs assessment that is independent of the person forwhom they are caring. Although the attitudes, experiences
P1: TIX/OSW P2: TIXc08 JWBK439-Banerjee January 14, 2010 14:34 Printer Name: Yet to Come
QUALITATIVE ENQUIRY IN THE EXPERIENCES OF PEOPLE 87
and beliefs of the person with dementia and the care giverare heavily intertwined, it should not be assumed that theyshare the same worries or that both members of the caregiving dyad are coping equally. However, the grounded the-ory that emerged from the people with dementia data andthe grounded theory that emerged from the care giving databoth have implications for each other, as well as for care pro-fessionals and service providers.
BIOGRAPHICAL DISRUPTION:A COMMON THEME
At the heart of this project is the importance of maintainingcontinuity in the person with dementia’s valued elements oflife. The experience of dementia threatens to disrupt conti-nuity and, to a large degree, coping strategies were aimed atsustaining it. This also emerged as a major sub-theme in thecare giving data, as the findings highlighted how importantit was for carers to be able to maintain continuity in theirown biographies. Continuity was valuable in the lives of caregivers and enabled those with traditional ideologies to de-rive ongoing rewards from their relationship with the personwith dementia and their lives as a whole. In ‘non-traditional’care givers the care giving role conflicted with participants’expectations and concept of themselves and their relation-ships. Their valued elements of life lay not in care giving,but in their own jobs, social lives and families, and thesewere now threatened by dementia. In this sense, dementia,as with any chronic illness, can be seen to represent a ‘bi-ographically disruptive’ experience to both people with de-mentia and their care givers (Bury, 1982). The data gener-ated suggests that to a large extent people with dementiaand carers are preoccupied by different concerns and holddifferent fears for the future. Yet it is clear that both groupsshare the need to maintain a sense of value and meaning inlife.
In this respect the two separate grounded theories ap-pear interrelated. There is a risk that the biographical dis-ruption experienced by care givers may have a negativeeffect on the person with dementia’s efforts to maintain
P1: TIX/OSW P2: TIXc08 JWBK439-Banerjee January 14, 2010 14:34 Printer Name: Yet to Come
88 MANAGING DEMENTIA IN A MULTICULTURAL SOCIETY
continuity in valued elements of life. Many of the carers witha non-traditional ideology appeared to experience a sense ofalienation from the care giving role and from the person thatthey were looking after. They struggled to recognise the per-son with dementia as their mother or wife, often stating thatthe relationship they had known and valued had been lost.It is likely that carers in this context would find it difficult toidentify and sustain the uniqueness of the individual. Yet, itis widely accepted that people with dementia depend uponsignificant others to reinforce their sense of self. It is impor-tant to recognise this disparity, especially as white Britishparticipants predominantly displayed a non-traditional ide-ology, thus it can be assumed that this experience is moretypical of the wider UK population.
AN ANTHROPOLOGICAL PERSPECTIVE
The two theories outlined underline the potential value ofconsidering the experience of dementia from an anthropo-logical perspective. The findings support the argument thatnotions of the self are constituted cross-culturally and arefundamental to constructions of dementia and the care thatindividuals receive (Hashmi, 2009). Within the present re-search, culture informed the person with dementia’s under-standing of the condition and the perceived implications,while the cultural construction of the self was reflected inthe individual’s ‘valued elements of life’. Similarly, the caregiver experience was rooted in collectivist-individualist con-cepts of self, which varied across the ethnic groups. To alarge extent the people with dementia and care giver datacan be understood in light of the individualistic view of theself, considered typical of Western cultures, and the collec-tivist view of the self, considered typical of non-Western cul-tures (Triandis, 1995). In Western societies where the selfis defined by individuality, agency and autonomy (Hashmi,2009), the priority that white British people with dementiaattach to remaining independent of others and being ableto account for oneself, and the tendency of white Britishcarers to construe care giving as an intrusion in their lives,is perhaps unsurprising. Impaired cognitive functioning
P1: TIX/OSW P2: TIXc08 JWBK439-Banerjee January 14, 2010 14:34 Printer Name: Yet to Come
QUALITATIVE ENQUIRY IN THE EXPERIENCES OF PEOPLE 89
undermined autonomy and this was associated with a lossof selfhood among white British people with dementia andcarers.
In contrast, the interdependent view of the self thatis considered characteristic of non-Western cultures is re-flected in the expectation of south Asian people with demen-tia to receive family support and the expectation of southAsian carers to provide it. Unlike the white British par-ticipants, south Asian people with dementia and carers at-tached value to maintaining and fulfilling their role withinthe family. The picture also appeared consistent across thepeople with dementia and carers within the black Caribbeansample. Both the people with dementia and the carersunderlined the importance of independence, yet this oftencoexisted with strong religious beliefs and a tradition ofworking within the caring professionals. Notably, this ap-peared to have contradictory implications, as experienceworking within the caring professions reinforced the tradi-tional ideology in care givers, but made it more difficult forthe person with dementia to receive care that previouslythey had provided. Hashmi (2009) concludes, ‘It is our verynotions of selfhood that are a major determining factor incross-cultural constructions of dementia, and the care thatsufferers ultimately receive’. The present data support thisposition and argue that the provision of culturally sensitivecare requires an understanding of these cultural differences.

P1: TIX/OSW P2: TIXc08 JWBK439-Banerjee January 14, 2010 14:34 Printer Name: Yet to Come
90
P1: TIX/OSW P2: TIXc09 JWBK439-Banerjee January 14, 2010 14:36 Printer Name: Yet to Come
9IMPLICATIONS FOR
PRACTICE AND POLICY
PEOPLE WITH DEMENTIA
These data argue that the loss or maintenance of the personwith dementia’s valued roles, relationships and activities ispivotal in determining the level of distress that they expe-rience. This has important implications, as informal carers,care professionals and service providers are in a position toprotect and promote these aspects of the individual’s life.This would benefit from a dual approach:
1. Reducing the threat to valued elements of life throughaddressing beliefs relating to individuals’ ‘understandingof the condition’ and ‘attitudes towards support needs’.
2. Promoting valued roles, relationships and activitiesthrough interaction, the environment, services and inter-ventions.
Cultural insights
The data revealed that black Caribbean, south Asian andwhite British people with dementia were likely to hold dif-ferent fears, as they tended to conceptualise their conditionand support needs in distinctive ways e.g. fear or being anirritation to others, fear of being ‘mad’, fear of care homes.
Managing Dementia in a Multicultural Society Sube Banerjee and Vanessa LawrenceC© 2010 John Wiley & Sons, Ltd
91
P1: TIX/OSW P2: TIXc09 JWBK439-Banerjee January 14, 2010 14:36 Printer Name: Yet to Come
92 MANAGING DEMENTIA IN A MULTICULTURAL SOCIETY
This has implications for the information, advice and reas-surance that they require. Ethnic variation in valued roles,relationships and activities helped to highlight the uniformprocess through which individuals across ethnic groups ap-praise and respond to their condition. However, the findingscan also help to sensitise practitioners to cultural variationin valued elements of life, which can help facilitate their rolein sustaining them.
Care givers
The care givers in this study could be classified as holdingeither a traditional or non-traditional care giver ideology(Lawrence et al., 2009). A traditional ideology was definedby the presence of three core, interrelated beliefs: care giv-ing is natural, care giving is expected, and care giving is vir-tuous. Conversely, a non-traditional care giver ideology wastypified by the absence of these beliefs. Carers occupied po-sitions on a continuum from highly traditional to highly non-traditional ideologies. However, each carer was categorisedinto one of two groups according to whether they held a pre-dominantly traditional or non-traditional ideology (see Ta-ble 9-1). We found that five black Caribbean, nine southAsian, and three white British participants held a tradi-tional ideology, while five black Caribbean, one south Asianand nine white British participants held a non-traditionalideology.
The data indicated that the attitudes of carers towardsthe care giving role, or more specifically their care givingideology, had direct implications for how carers could bestbe supported. The findings are consistent with the argumentthat carers are a heterogeneous group that experiences dif-ferent difficulties and distress and has different resourcesand priorities (Zarit and Femia, 2008). Zarit and Femia hy-pothesised that this diversity helped to explain weak effectsobserved overall in studies examining the efficacy of psy-chosocial interventions for care givers and necessitated theprovision of individualised interventions. The findings of thepresent research offer guidance on how to tailor services andsupport to the needs of the care giver.
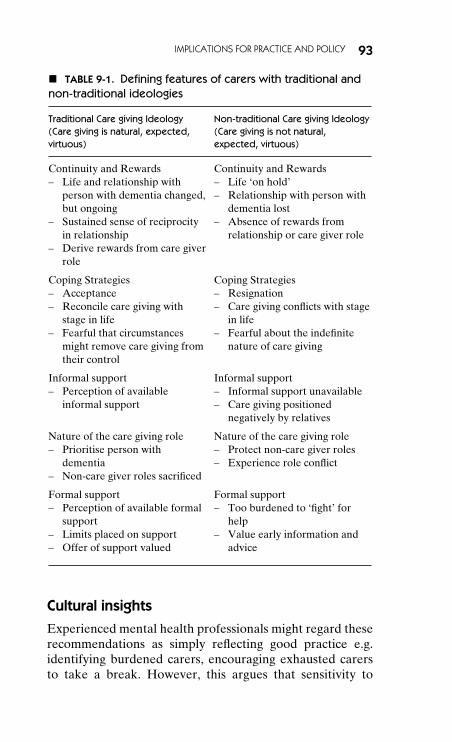
P1: TIX/OSW P2: TIXc09 JWBK439-Banerjee January 14, 2010 14:36 Printer Name: Yet to Come
IMPLICATIONS FOR PRACTICE AND POLICY 93
� TABLE 9-1. Defining features of carers with traditional andnon-traditional ideologies
Traditional Care giving Ideology(Care giving is natural, expected,virtuous)
Non-traditional Care giving Ideology(Care giving is not natural,expected, virtuous)
Continuity and Rewards– Life and relationship with
person with dementia changed,but ongoing
– Sustained sense of reciprocityin relationship
– Derive rewards from care giverrole
Continuity and Rewards– Life ‘on hold’– Relationship with person with
dementia lost– Absence of rewards from
relationship or care giver role
Coping Strategies– Acceptance– Reconcile care giving with
stage in life– Fearful that circumstances
might remove care giving fromtheir control
Coping Strategies– Resignation– Care giving conflicts with stage
in life– Fearful about the indefinite
nature of care giving
Informal support– Perception of available
informal support
Informal support– Informal support unavailable– Care giving positioned
negatively by relatives
Nature of the care giving role– Prioritise person with
dementia– Non-care giver roles sacrificed
Nature of the care giving role– Protect non-care giver roles– Experience role conflict
Formal support– Perception of available formal
support– Limits placed on support– Offer of support valued
Formal support– Too burdened to ‘fight’ for
help– Value early information and
advice
Cultural insights
Experienced mental health professionals might regard theserecommendations as simply reflecting good practice e.g.identifying burdened carers, encouraging exhausted carersto take a break. However, this argues that sensitivity to
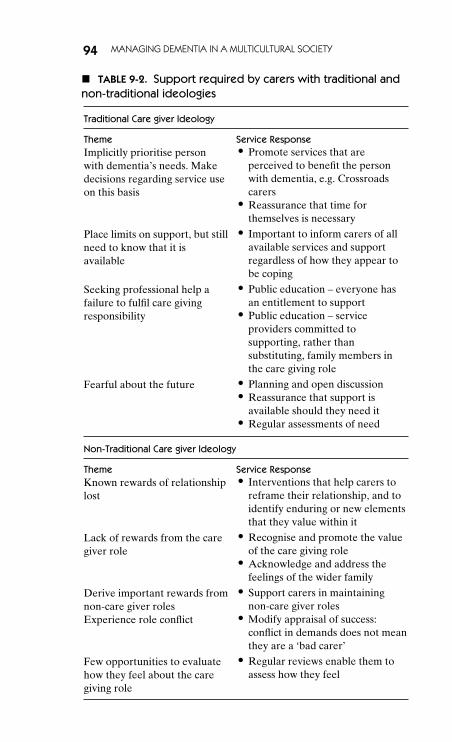
P1: TIX/OSW P2: TIXc09 JWBK439-Banerjee January 14, 2010 14:36 Printer Name: Yet to Come
94 MANAGING DEMENTIA IN A MULTICULTURAL SOCIETY
� TABLE 9-2. Support required by carers with traditional andnon-traditional ideologies
Traditional Care giver Ideology
Theme Service ResponseImplicitly prioritise personwith dementia’s needs. Makedecisions regarding service useon this basis
� Promote services that areperceived to benefit the personwith dementia, e.g. Crossroadscarers
� Reassurance that time forthemselves is necessary
Place limits on support, but stillneed to know that it isavailable
� Important to inform carers of allavailable services and supportregardless of how they appear tobe coping
Seeking professional help afailure to fulfil care givingresponsibility
� Public education – everyone hasan entitlement to support
� Public education – serviceproviders committed tosupporting, rather thansubstituting, family members inthe care giving role
Fearful about the future � Planning and open discussion� Reassurance that support is
available should they need it� Regular assessments of need
Non-Traditional Care giver Ideology
Theme Service ResponseKnown rewards of relationshiplost
� Interventions that help carers toreframe their relationship, and toidentify enduring or new elementsthat they value within it
Lack of rewards from the caregiver role
� Recognise and promote the valueof the care giving role
� Acknowledge and address thefeelings of the wider family
Derive important rewards fromnon-care giver rolesExperience role conflict
� Support carers in maintainingnon-care giver roles
� Modify appraisal of success:conflict in demands does not meanthey are a ‘bad carer’
Few opportunities to evaluatehow they feel about the caregiving role
� Regular reviews enable them toassess how they feel
P1: TIX/OSW P2: TIXc09 JWBK439-Banerjee January 14, 2010 14:36 Printer Name: Yet to Come
IMPLICATIONS FOR PRACTICE AND POLICY 95
attitudes towards care giving, which originate in cultural dif-ferences along the collectivism-individualism dimension, canusefully guide their approach. Foremost, it provides careprofessionals with a deeper understanding of why carersacross ethnic groups behave in certain ways and evidenceto suggest a specifically tailored approach.
Joint implications for policy and practice
The two sets of data provide complementary insights intohow dementia care might be improved. The following dis-cussion of policy and practice implications will be organisedaround the relevant services and interventions.
INCREASED PUBLIC AWARENESS OF DEMENTIA
Reducing stigma
A priority of the National Dementia Strategy is to addressthe stigma associated with the condition (Department ofHealth, 2009). The data from the interviews with the peoplewith dementia underline the necessity of helping individu-als and their partners to view forgetfulness as a symptom ofdementia, rather than ‘obstinacy’, ‘stupidity’ or ‘madness’.This is consistent with cognitive therapy interventions thatsuggest that examining dysfunctional illness beliefs in theperson with dementia may lead to improvements in mood(Scholey and Woods, 2003). Societal attitudes are likely toinfluence the illness representations that people with de-mentia hold (Clare et al., 2006). These findings indicate thatpublic education campaigns are needed to challenge stigma-tising beliefs and that these may benefit from a culturallytailored approach. Meanwhile, the findings offer support forthe role of memory services, which offer assessment, diag-nostic and treatment services while avoiding much of thestigma attached to old age psychiatry services. The evidencebase remains limited, yet research does suggest that mem-ory services are also more accessible to members of minorityethnic groups than traditional psychiatric services (Banerjeeet al., 2007).
P1: TIX/OSW P2: TIXc09 JWBK439-Banerjee January 14, 2010 14:36 Printer Name: Yet to Come
96 MANAGING DEMENTIA IN A MULTICULTURAL SOCIETY
Negotiating a shared understandingof dementia
A parallel aim of the National Dementia Strategy is to chal-lenge the ‘false belief’ that dementia is a normal part of age-ing, as this can result in an unwillingness to seek or accepthelp (Department of Health, 2009). The findings here re-veal the complexity of this issue. In many ways, the propen-sity of the south Asian older people to conceptualise theircondition as a normal part of ageing, rather than as a dis-ease entity, helped them to cope with their situation. Edu-cational campaigns aimed solely at modifying these beliefsmay constitute an oversimplified response and risk alien-ating people with dementia and their families within mi-nority ethnic groups. A recent award-winning programme(‘The Meri Yaadain project’) aimed at raising awareness ofdementia among south Asian communities in Bradford at-tributed its success to focusing on memory loss rather thanmental illness. Outreach workers gradually introduced dis-cussion of mental health and issues affecting older people.Again, memory services may provide a solution, as thereis potential for eliciting the patients’ and the family’s cul-tural understanding of dementia in this context. Practition-ers would then ‘be in a better position to negotiate a wayof talking about the illness and a therapeutic approach thatreflects the values of biomedicine and of families’ (Hintonet al., 2005). The research indicated that medication is rarelyconceived as an appropriate response to memory problems.This confirms the importance of developing a shared ex-planatory model, particularly with regards to expectationsand treatment goals. It also highlights the importance of hav-ing specialist professionals with skills in assessing and deliv-ering a diagnosis of dementia.
INCREASED PUBLIC AWARENESS OF SERVICESAND SUPPORT
The data from the people with dementia and the data fromcare givers with traditional and non-traditional ideologiesunderline the necessity, albeit in different ways, of raising
P1: TIX/OSW P2: TIXc09 JWBK439-Banerjee January 14, 2010 14:36 Printer Name: Yet to Come
IMPLICATIONS FOR PRACTICE AND POLICY 97
awareness of formal support. Among the people with de-mentia, the view that GPs were unable to help was oftenjuxtaposed against the value placed on the varied health andsocial services that GPs enabled them to access. Therefore,it might be expedient to provide education regarding the ex-istence of these services and of the GP’s role in providing ac-cess to support and specialist care. The findings prioritise theimportance of defining what help is available and of promot-ing awareness of day centres, home helps, befrienders, etc.,alongside that of pharmacological and non-pharmacologicalinterventions.
Although a large proportion of ‘traditional’ carers hadaccessed services at the time of interview, many south Asiancarers admitted that they only became aware of what wasavailable when their situation reached crisis point. It is alsoimportant to note that some south Asian carers with tradi-tional ideologies identified asking for professional help as afailure to fulfil their responsibilities. In part, this appeareddue to the tendency to equate formal care with care homes.This highlights the importance of raising awareness amongminority ethnic groups, in particular, of the range of servicesavailable to support carers and people with dementia in theirown homes. Services might be considered more acceptable ifthey could communicate their commitment to respecting in-dividual preferences for care, and to supporting, rather thansuperseding, family members in the care giving role (Sin,2006). Despite placing limits on the level of support that theyasked for and received, many ‘traditional’ carers drew enor-mous comfort from the perceived availability of services andoffers of assistance assumed equal importance throughoutthe carer sample.
There was also a consensus among ‘traditional’ and ‘non-traditional’ carers that acquiring information, advice andpractical assistance could be time consuming and tiring. Car-ers were equally clear that they wanted guidance as soonas possible and for there to be one person to whom theycould turn with their queries and concerns. This is consistentwith the identified need for continuity of support, informa-tion and advice outlined in the National Dementia Strategy(Department of Health, 2009). Thus, the data support the
P1: TIX/OSW P2: TIXc09 JWBK439-Banerjee January 14, 2010 14:36 Printer Name: Yet to Come
98 MANAGING DEMENTIA IN A MULTICULTURAL SOCIETY
proposed introduction of ‘dementia care advisors’ whowould act as an identifiable point of contact with knowl-edge and access to the whole range of local services avail-able. Alternatively, the findings support the expansion ofexisting services committed to providing information andco-ordinating practical support for carers of people with de-mentia for as long as they require.
SUPPORTING PEOPLE WITH DEMENTIA ANDCARERS IN ACCESSING SERVICES
Communicating the importance of care giverwell being
Lack of knowledge is not the only factor preventing peo-ple with dementia and their families from accessing avail-able help. Care giver ideology informs attitudes towards for-mal care that necessitate specific advice and reassurance. Itemerged that children and spouses with a traditional ide-ology appeared resigned to sacrificing certain elements oftheir lives and many implicitly prioritised the care recipients’needs over their own physical and mental health. Conse-quently, many of these carers suffered from exhaustion andfatigue. It is important that professional care staff reassurecarers that it is both natural and necessary to require timefor themselves. Staff should stress that services that allowcarers to recuperate their emotional and physical strengthultimately benefit the person with dementia (Gallagher-Thompson, 2006). The 2008 carers’ strategy stipulated thatcarers should be supported so that caring does not adverselyaffect their health (Department of Health, 2008a). This maymean providing services and support that specifically targetcarers’ health needs, e.g. replacement care to allow carers toattend hospital appointments and screenings.
Identifying burdened care givers
The data also support suggestions that carers with highlevels of burden often need help to seek help (Gafstromand Winblad, 1995). The findings indicated that carers withnon-traditional ideologies experienced a greater urgency of
P1: TIX/OSW P2: TIXc09 JWBK439-Banerjee January 14, 2010 14:36 Printer Name: Yet to Come
IMPLICATIONS FOR PRACTICE AND POLICY 99
need (e.g. many were juggling demands, lacking support andhighly distressed) than ‘traditional’ carers, yet often lackedthe necessary resources to pursue the help they needed.Buono et al. (1999) concluded that general practitionersshould be encouraged to identify family members with highlevels of burden and to provide them with additional supportand information as well as the opportunity to access help fortheir own personal needs (Buono et al., 1999).
Responding to symptoms of dementia acrossethnic groups
It was striking that over half of the black Caribbean peo-ple with dementia, in contrast to the south Asian and whiteBritish participants, had faith in the GP’s ability to assistthem. A lack of informal support, an emphasis on self-help,and a belief in GPs appeared to prompt black Caribbeanolder adults to personally seek help in the early stages oftheir condition. It is vital that GPs respond sensitively tothese concerns and avoid the pervasive assumption that sub-jective memory complaints indicate depression or normalageing rather than dementia (Iliffe et al., 2005). One of theproposed strengths of specialist memory clinics is that theywill provide a simple single focus for referrals from primarycare (Department of Health, 2009). However, this hinges ontheir availability and the willingness of GPs to make appro-priate referrals. It is essential that GPs are sensitive to cul-tural and ethnic variations in patterns of presentation andhow older people and their families are likely to frame theircondition, e.g. impaired functioning of the brain in the blackCaribbean population and irritation among white Britisholder adults. This should form a constituent part of the na-tional training that has been proposed by the National De-mentia Strategy to enable all GPs to recognise early symp-toms of dementia (Department of Health, 2009).
DISCUSSING THE DIAGNOSIS
Accurately identifying dementia as serious and progressiveevokes fear for the future. This highlights the tension be-tween avoiding harm and promoting a patient’s autonomy
P1: TIX/OSW P2: TIXc09 JWBK439-Banerjee January 14, 2010 14:36 Printer Name: Yet to Come
100 MANAGING DEMENTIA IN A MULTICULTURAL SOCIETY
through the provision of full, clear information (Woods andPratt, 2005). It is well documented that some families (andpractitioners) fear that providing the person with demen-tia with a diagnosis and full information can cause unnec-essary distress (Holroyd et al., 2002). However, research hasalso suggested that opportunities to discuss their experiencemight reduce anxiety (Carpenter et al., 2008) and help in-dividuals make sense of their illness (Pearce et al., 2002).Although the older adults in this sample were reassured bythe apparent propensity of GPs to frame their condition inthe context of normal ageing, many also appeared confusedand concerned that this did not entirely explain their con-dition. The findings suggest that despite patients’ apprehen-sions they would benefit from an open discussion about theirdifficulties and concerns, as this would help to validate theirexperience, reduce the surrounding taboo, and ultimatelyhelp them to acknowledge their condition. Thus, the find-ings support the argument that people with dementia shouldreceive a diagnosis if it is made (Pearce et al., 2002, Derksenet al., 2006). GPs have been found to experience difficulty indiscussing the diagnosis of dementia; many feel constrainedby the limited consultation period (Van Hout et al., 2000)and believe that dementia diagnosis belongs within the spe-cialist’s domain, rather than that of general practice (Turneret al., 2004). Discussing the individual’s condition requirestime and skill and the data highlight the advantages of de-livering a diagnosis of dementia within specialist memoryclinics. The findings are unequivocal that individuals requiresupport in managing these difficult beliefs.
DISCUSSING THE FUTURE
The inclusion of Advance Care Planning in recent govern-ment initiatives (Department of Health, 2008b) has firmlyplaced the emphasis on enabling people to articulate theirconcerns and preferences for the future. This should ap-ply no less to people with dementia. The findings of thepresent research indicate that people with dementia requirethe opportunity to voice their fears and anxieties and ex-plore possible solutions. For example, a large number of
P1: TIX/OSW P2: TIXc09 JWBK439-Banerjee January 14, 2010 14:36 Printer Name: Yet to Come
IMPLICATIONS FOR PRACTICE AND POLICY 101
black Caribbean participants conceptualised care homes asan undesirable, yet unavoidable part of their future. En-tering into a dialogue with family and professionals abouttheir options may dissipate some of these fears and assistthem in working to find a satisfactory solution. Similarly, itis important to reassure white British people with demen-tia that there are alternatives to care homes and burden-ing family members. Moreover, a distinctive level of distresswas evident in the few south Asian participants who lackedconfidence in family support. If this is a developing trend(Katbamna et al., 2004) the experience of dementia is likelyto evoke increasing levels of fear among south Asian olderpeople with dementia.
The findings also demonstrate the need for professionalsto support family members in addressing their concerns forthe future. There was a propensity across the sample for car-ers to focus on the present and avoid acknowledging theirfears. Open discussion, and planning for the future, mightinstall a greater sense of control. This would help alleviatethe fears of carers with traditional ideologies, many of whomwere terrified that their own health might deteriorate, thusremoving care giving from their control. Critically, it wouldalso reassure them that support was available should theyrequire it in the future. Lastly, formal mechanisms such asregular reviews are needed to provide carers with an oppor-tunity to evaluate how they feel about the current situation.Few ‘non-traditional’ carers had identified a threshold forrelinquishing the role and many persevered despite feelingincreasingly overwhelmed. In this context, family membersmay require support in stepping back from the care givingrole.
PROMOTING VALUED ELEMENTS OF LIFE OFTHE PERSON WITH DEMENTIA
Reinforcing individual biographies
One of the core messages here is the importance of sus-taining the person with dementia’s valued elements of life.Sabat and Harre’s (1992) social constructionist model and
P1: TIX/OSW P2: TIXc09 JWBK439-Banerjee January 14, 2010 14:36 Printer Name: Yet to Come
102 MANAGING DEMENTIA IN A MULTICULTURAL SOCIETY
Kitwood’s (1997) person-centred care model offer impor-tant insights into how this can be achieved. Both highlightthe role that significant others play in maintaining or under-mining the self in people with dementia. In the present re-search, some older adults were comforted by the reassuranceand kindness that family members provided, while negativeinteractions threatened to compound fears of inadequacyamong others. Kitwood proposed that constructive interac-tion requires that care givers recognise, respect and provideopportunity for the individual’s self-expression (Kitwood,1997). Family carers are uniquely positioned to reinforce theindividual’s identity as they have expert knowledge of theperson for whom they care. Research has demonstrated thatsome relatives engage in a daily struggle to ‘maintain ves-tiges of the person as once known’ (Orona, 1990). However,as previously discussed, it is striking that many of the car-ers within the present research did not describe their role inthis way. A defining characteristic of many of the carers withnon-traditional ideologies was that they struggled to recog-nise the person with dementia as the relative whom they hadknown and valued. The data suggest a need for interventionsthat support carers in seeing beyond the illness. These car-ers may also benefit from interventions that help to reframetheir relationship, and to identify new or enduring elementsthat they value within it.
Evidence has also demonstrated that interactions withformal care givers are critical. Golander and Raz (1996) de-scribed the important role that care givers played in remind-ing, constructing and re-editing past biographies in nursinghome residents. Surr (2006) observed that people with de-mentia endeavour to recount a life story and noted thatcommunicating life events and experiences played an im-portant role in preserving the self. Knowledge of the indi-vidual’s biography can help carers to engage in these storiesand assist them in finding metaphorical meaning in accountsthat may present as disjointed or time confused to oth-ers. Thus, it is important that staff take a personal inter-est in the background of the person with dementia if theyare to sustain person and social selves in dementia (Smallet al., 1998). Cohen-Mansfield acknowledged that gaining
P1: TIX/OSW P2: TIXc09 JWBK439-Banerjee January 14, 2010 14:36 Printer Name: Yet to Come
IMPLICATIONS FOR PRACTICE AND POLICY 103
information about the past identity and roles of peoplewith dementia would take additional staff time, but thatthe benefits of individualised activities, including a reduc-tion of problem behaviours, should be acknowledged as acost saving (Cohen-Mansfield et al., 2006b) and a qualityimprovement.
Providing opportunities to pursue valuedroles, relationships and activities
Harris and Sterin (1999) concluded that if a person’s inter-ests and valued roles are understood, then it should be pos-sible to adjust the psychosocial environment to affirm theindividual’s sense of self. Personal accounts of living with de-mentia suggest that a sense of personal identity is retained,but that individuals may lack ‘avenues for self-expression’(Basting, 2003). Surr (2006) found that permitting nursinghome residents to pursue their own desirable roles e.g. socialrelationships, being part of a family, working, caring for oth-ers, helped preserve the person with dementia’s sense of self.In one example, staff supported a female resident in main-taining meaningful occupation by asking her to do smalltasks around the home. Individualised interventions that tar-get salient role identities have been shown to have a positiveimpact on the person with dementia’s emotional and psycho-logical well being (Cohen-Mansfield et al., 2006b, Romeroand Wenz, 2001). Modifying or substituting activities thatpeople with dementia previously enjoyed also promises tohelp preserve continuity in their lives (Romero and Wenz,2001).
Offering services that reinforce rather thanchallenge valued roles
Among the white British people with dementia, helping withpractical tasks around the house or relieving loved ones byaccepting service support, played an important part in help-ing older adults maintain a sense of reciprocity within themarital relationship. Many black Caribbean people with de-mentia described social interaction as an integral part of
P1: TIX/OSW P2: TIXc09 JWBK439-Banerjee January 14, 2010 14:36 Printer Name: Yet to Come
104 MANAGING DEMENTIA IN A MULTICULTURAL SOCIETY
their lives and day centres and lunch clubs afforded oppor-tunities to pursue this. Supporting south Asian older adultsin maintaining active roles within the community might alsoprove valuable in preserving their sense of self. There is aneed to be sensitive to the person with dementia’s hopesand fears and to offer services in a way that does not un-dermine integral roles, e.g. assistance with household tasksshould not evoke feelings of failure as a housewife. Instead,the provision of services should reinforce valued identities,e.g. day centres as an opportunity to pursue social interac-tion or reciprocate the support of one’s spouse. These arevery general examples based on the cultural trends observedwithin the data. However, core values are unique to each in-dividual and informal and formal carers are required to elicitthe roles, relationships and activities that each person withdementia values.
As previously stated, many carers with traditional ide-ologies appeared to prioritise the care recipients’ needs overtheir own, and made decisions regarding service use on thisbasis. Services that are perceived as benefiting the personwith dementia through providing individualised care, such asCrossroads carers, offer an important solution. The knowl-edge that the person with dementia was safe and happywould relieve carers’ concerns, thus enabling them to enjoya complete break without fear that they are compromisingthe person with dementia’s well being. This would of coursebe equally beneficial for ‘non-traditional’ carers who on oc-casion felt similarly forced to weigh up the person with de-mentia’s needs and wants against their own.
Psychosocial interventions
The findings point towards the value of reminiscence ther-apy, which involves the discussion of past experiences,events and activities. In particular, people with dementiamay benefit from the more structured and individually tar-geted intervention, life review. Life review has the powerto promote an enduring sense of self through reviewingone’s entire history. As Haight points out (2003), ‘this his-tory is the core of uniqueness of individuals’. Few systematic
P1: TIX/OSW P2: TIXc09 JWBK439-Banerjee January 14, 2010 14:36 Printer Name: Yet to Come
IMPLICATIONS FOR PRACTICE AND POLICY 105
evaluations exist, yet descriptive and observational studieshave reported favourable outcomes (Woods et al., 2005).Preliminary findings have suggested that completing life sto-rybooks with people with dementia and carers can improvemood in the person with dementia and decrease reportedbehavioural problems and burden in family carers (Haightet al., 2003).
Supporting people with dementia in balancingconstancy with change
Participants used two groups of coping strategies to man-age the threat of dementia: the first focused on constancy,the second on change. Focusing on valued elements of lifethat remained unchanged and acknowledging changes invalued elements of life both had the potential to managethe threat that dementia posed, but participants struggledto achieve equilibrium between the two. It is important toemphasise that the need to maintain the feeling of continu-ous identity existed alongside the need to adjust to demen-tia related changes. Acknowledgement conferred importantadvantages such as helping to diffuse the stigma and fearattached to the condition, enabling the person with demen-tia to discuss worries and concerns, utilise behavioural cop-ing strategies and seek and accept help. People with demen-tia may find it easier to acknowledge some of the changesthat they are experiencing if significant others are helping tomaintain a sense of identity.
REPOSITIONING THE CARE GIVER ROLE
Promoting the care giving role
Carers with non-traditional ideologies were less likely to de-rive rewards from the care giving role itself, as they oftenlacked the conviction that it represented virtuous behaviour.Health and social care providers are in a position to recog-nise the value of the care that families provide. This is inagreement with the 2008 carers’ strategy, which stresses thatcarers must be universally recognised and valued for the
P1: TIX/OSW P2: TIXc09 JWBK439-Banerjee January 14, 2010 14:36 Printer Name: Yet to Come
106 MANAGING DEMENTIA IN A MULTICULTURAL SOCIETY
support that they provide to individuals and society as awhole (Department of Health, 2008a). It argues, specifically,that professionals should recognise that carers are expertin the care of the person they are looking after, and moregenerally, that society must encourage and support thoseindividuals who are willing to take on caring responsibili-ties. However, there is also scope for a change in govern-mental policy and the benefits system to directly supportand promote the role of family carers. Specific grants ortargeted benefits would publicly acknowledge the value ofthe care giving role as well as directly help those who care.There is a level of recognition within the carers’ strategythat the Carer’s Allowance is an inadequate reflection ofthe work that goes into caring and that the current struc-ture of benefits should be reviewed (Department of Health,2008a).
Involving the wider family
It may be insufficient for care professionals to work withthe primary care giver alone, given that the findings suggestthat siblings, spouses and children are pivotal in informingcarers’ attitudes towards the role. Instead, it may be bene-ficial to adopt a systemic approach that acknowledges thefeelings of the wider family. Previous research has arguedthat interventions that address the family unit are neededwithin collectivist care giving systems (Dilworth-Andersonet al., 2006). The data from this study suggest that such inter-ventions may be of even greater importance in individualistcare giving systems, where the attitudes and beliefs of sig-nificant others may undermine the individual’s approach tothe care giving role. There is evidence that it is possible tomodify spouses’ satisfaction with social support and that thiscan reduce appraisals of stressfulness and depression (Roth,2005). Roth (2005) found that spouses benefited from indi-vidual and family counselling sessions that focused on mo-bilising existing natural social support resources. Increasesin objective indicators of support were not found to predictreduced depression, prompting the authors to speculate thatimproved quality of relationships, rather than an increase in
P1: TIX/OSW P2: TIXc09 JWBK439-Banerjee January 14, 2010 14:36 Printer Name: Yet to Come
IMPLICATIONS FOR PRACTICE AND POLICY 107
the amount of assistance received, may underlie satisfactionwith social support and improvements in mood.
Supporting carers in maintaining non-caregiving roles
An absence of intrinsic rewards from the care giving rela-tionship or the care giving role may explain why individualswith non-traditional ideologies appeared to attach greaterimportance to remaining in their jobs and protecting theirsocial lives. These roles provided fulfilment, yet also ledto role conflict, as previously demonstrated among ‘non-traditional’ carers (Long Foley et al., 2002). It is importantthat service providers appreciate the benefits of maintain-ing non-care giver roles (Dautzenberg et al., 1999), and offeras much practical support as possible. This is in accordancewith the carers’ strategy, which asserts that carers must beenabled to have a life of their own alongside the care giv-ing role (Department of Health, 2008a). The report pledges£150 million to increase the availability of short breaks fromcare giving. However, for this to succeed the provision ofcare must be perceived to be of adequate quality and tobe suited to the individual needs of both the carer and theperson with dementia. The carers’ strategy also stipulatesthat employers have a crucial role to play in offering flexibleworking and in recognising that carers have specific needs,e.g. understanding that there may be occasions where theyneed to leave suddenly. It may also be necessary to modifythe way carers appraise their success: they should not expectto perform multiple roles faultlessly, and need to understandthat they can still be a ‘good carer’ even if they experienceconflict in the needs of those around them.

P1: TIX/OSW P2: TIXc09 JWBK439-Banerjee January 14, 2010 14:36 Printer Name: Yet to Come
108
P1: IFM/OSW P2: TIXc10 JWBK439-Banerjee January 14, 2010 14:37 Printer Name: Yet to Come
10ONE SIZE FAILS
ALL – DEMENTIA, AGEDISCRIMINATION AND
SPECIALIST OLDERPEOPLE’S MENTALHEALTH SERVICES
One important element of good quality care for people withdementia is specialist older people’s mental health services.In this final chapter we will address the question of whatsuch services should do and problems in their provisionincluding the role of age discrimination in generating thecurrent state of service provision. The disparity in termsof quality and quantity of care provided for older peoplewith mental disorders including dementia compared withthat provided for adults of working age has led some, moreor less benignly, to advocate that services for older peopleshould be closed and there should be a single service foradults of all ages, since the presence of an age-definedservice is age discrimination. In this chapter we will explorehow and why such an approach would result in decreasedservice quality, decreased patient safety and decreaseddeployment of evidence-based care.
Managing Dementia in a Multicultural Society Sube Banerjee and Vanessa LawrenceC© 2010 John Wiley & Sons, Ltd
109
P1: IFM/OSW P2: TIXc10 JWBK439-Banerjee January 14, 2010 14:37 Printer Name: Yet to Come
110 MANAGING DEMENTIA IN A MULTICULTURAL SOCIETY
WHAT DOES GOOD LOOK LIKE?
So what does good quality specialist mental health care forolder adults look like? A simplistic reading of the situationin the context of the need to provide services that do notdiscriminate on the basis of age, might suggest that thereshould be a single service for all adults with mental disorder,or a single service for all adults with functional disorderand a separate dementia service. However, with a closerconsideration of the clinical situation it becomes clear thatthere are systematic differences between the needs of olderpeople and those of working age and that a specific serviceresponse is needed. On balance, there appears to be nobetter case for combining services for working age adults(be they functional or organic) with those for older adultsthan there are for combining services for working ageadults with those for children.
AGE DISCRIMINATION IN SERVICECOMMISSIONING
Age discrimination is addressed in the NHS Constitutionwhose first principle is ‘ the NHS provides comprehensiveservice, available to all irrespective of gender, race, disabil-ity, age, sexual orientation, religion or belief’, and furtherthat the NHS ‘ has a wider duty to promote equality throughthe services it provides and to pay particular attention togroups or sections of society where improvements in healthand life expectancy are not keeping pace with the rest of thepopulation’. This is a fair description of the current state ofspecialist mental health services for older adults. The Equal-ity Bill will outlaw age discrimination in all health and careservices
There can be no doubt that there is age discriminationin the development, commissioning and provision of mentalhealth services. The Healthcare Commission report Olderpeople’s mental health services: a national study published in2009, found that older people’s services were falling behindthose for adults, with clear evidence of age discrimination inaccess to services, a lack of age appropriateness and lack ofspecialist input. Recommendations included suggesting that
P1: IFM/OSW P2: TIXc10 JWBK439-Banerjee January 14, 2010 14:37 Printer Name: Yet to Come
ONE SIZE FAILS ALL – MENTAL HEALTH SERVICES 111
commissioners and providers assess all services for discrimi-nation in access and deal with this. They were clear that thiscould not be achieved by simply providing access to servicesdesigned for younger adults. These are complex systems andsimple answers may generate more discrimination and lowerquality for older people rather than addressing these impor-tant issues.
A ‘one size fits all ages’ approach is more likely to in-crease age discrimination than it is to address it. This is be-cause age here is a proxy for a different set of needs andtherefore skills. The aim of the age equality agenda is to gen-erate services of equivalently good quality for people of allages. The nature of risk and need in older people with men-tal disorders means that, in order to provide services that areof equivalent quality to those available to adults of workingage, specific provision needs to be made in terms of thesedifferent needs and skills. Delivering equivalent quality ofcare is therefore likely to require enhancing current olderpeople’s mental health teams to have higher levels of func-tionality in terms of the capacity for assertive outreach, forexample.
WHY CONSIDER OLDER ADULTS SEPARATELYFROM ADULTS OF WORKING AGE?
The implications for our health and social care systems ofpopulation ageing are well articulated in the National Ser-vice Framework for Older People and form a major partof the rationale for the development of such age specificpolicy by DH and across government. We live at a time ofworldwide population ageing and this has generated con-cerns about the ability of social systems and health careservices to meet the needs of older people (World HealthOrganization, 1991). This is as active an issue in the develop-ing world where countries are projected to experience a mas-sive increase in the numbers of older people both in relativeand absolute terms (Kalache, 1991; Prince et al., 2007), as it isin the developed world. The demographic projections in theUK, as in much of the developed world, are for an increasein the oldest old (those over 75 and those over 85) who havethe highest levels of physical and psychiatric morbidity and
P1: IFM/OSW P2: TIXc10 JWBK439-Banerjee January 14, 2010 14:37 Printer Name: Yet to Come
112 MANAGING DEMENTIA IN A MULTICULTURAL SOCIETY
therefore the greatest need. Particular concern has been fo-cused in the developed world on the funding of long termcare for the elderly, with dementia being a major determi-nant of need for this type of care. In the UK around 3.6% ofgross domestic product is spent on long term care at present(Bone, 1997) with some projecting that this may need to riseto 10.8% in the next 30 years (Nuttall et al., 1994).
In terms of service activity in psychiatry, older peopleare an important group. People over the age of 65 makeup around a third of all mental health activity in the UK interms of admissions, readmissions and community contacts(Philpot and Banerjee, 1997). However, the profile of disor-der and needs does differ from that in younger age groups.The challenges presented by dementia and co-morbid physi-cal illness and disability require particular professional skillsand services need to be able to deal with the complex mix ofsocial, psychological, physical and biological factors found inthe elderly mentally ill.
Old age psychiatry was developed within the UK healthand social care system for two main reasons.
� The needs and risks presented by older people with men-tal disorder systematically differ from those presented byadults of working age. So a different set of skills is neededin the multidisciplinary teams charged with their care anda differentiated service response needed to meet theseneeds.
� It was clear that undifferentiated adult psychiatry servicesprovided a poor quality service for those older adults thatcame under their remit in terms of diagnosis and manage-ment.
Different needs and risks
The special needs of the elderly include:
� a pattern of multiple pathology;� complex co-morbidity of physical and mental health with
social care needs;� different patterns of social care and family support;
P1: IFM/OSW P2: TIXc10 JWBK439-Banerjee January 14, 2010 14:37 Printer Name: Yet to Come
ONE SIZE FAILS ALL – MENTAL HEALTH SERVICES 113
� the particular challenge of mental disorder in care homes;and
� dementia.
These were identified as requiring specialist training andmultidisciplinary working with effective joint working withcarers, primary health care, geriatric medicine and social ser-vices (Arie, 1971; Royal College of Psychiatrists and BritishGeriatric Society, 1979; Wertheimer, 1997).
Development from undifferentiated services
Moves to develop specialist older people’s mental healthservices out of undifferentiated adult psychiatry started inthe late 1960s and by the mid-1990s there was a nationwidenetwork of such services, albeit a network that had majorvariation in terms of resource available. These services weremostly staffed by full time consultants in old age psychia-try with community teams and wards dedicated to work-ing with older people specifically (Lindsay and Banerjee,1992). As a discipline it defined itself from the first as hav-ing a primary community focus, insisting on the importanceof home-based assessment and care (Arie and Issacs, 1978).More recently, the World Health Organisation (WHO) con-sensus statement on psychiatry for the elderly has affirmedthat assessments should be carried out in the patient’s home(Wertheimer, 1997). Unlike many principles, these appearto be the reality of clinical practice in old age psychiatry,with nine out of ten referrals seen at home rather than inout-patient clinics (Wattis et al., 1981). However, its devel-opment and differentiation has been based not only on ide-ology and the specific unmet needs of the elderly but also ona practical need to overcome institutional age-related preju-dice within psychiatry (Murphy and Banerjee, 1993).
POLICY DEVELOPMENT FOR OLDER PEOPLEWITH MENTAL DISORDERS
The National Service Framework for mental health was ex-plicitly targeted at working age adults, the validity of this
P1: IFM/OSW P2: TIXc10 JWBK439-Banerjee January 14, 2010 14:37 Printer Name: Yet to Come
114 MANAGING DEMENTIA IN A MULTICULTURAL SOCIETY
decision can be debated but it was decided that general prin-ciples and specific services for working age adults shouldbe addressed by the mental health NSF and specialist olderpeople’s mental health services by the older people’s NSF.Here we need to consider some of the consequences in thatproblems for older people mental health services have be-come clear with the successes of the mental health NSF. Themental health NSF resulted in major investment and sub-sequent quality improvement of in-patient and communitymental health services for working age adults. Across thecountry, it has become evident that these developments andimprovements have not been matched by similar develop-ment or investment in older people’s mental health services,which have in a sense been ‘left behind’. This differentialinvestment by commissioners, widening discrimination, wasan unforeseen and unwanted consequence of the success ofthe mental health NSF.
The National Service Framework for Older People(NSFOP) was a success in terms of embedding its genericgoals of the need for dignity and respect to be at the heart ofthe National Health Service’s response to older people. Thespecific clinical areas that it identified as needing particularattention have also been acknowledged to be correct andthese include mental disorder in later life. However, dueto the particular nature of the NSFOP’s implementation,it has been necessary for there to be further policy devel-opment in order to achieve quality improvement in thesespecific areas. To date these include the development ofthe National Stroke Strategy and the National DementiaStrategy. There is now a need for similar work to bedone for older people’s mental health not least to workto eliminate age discrimination which is in itself a majorpriority.
In 2005 DH through the Care Services ImprovementPartnership published the good practice guide Everybody’sBusiness: integrated mental health services for older people.This stated that services should deliver:
� non-discriminatory mental health and care services avail-able on the basis of need, not age;
P1: IFM/OSW P2: TIXc10 JWBK439-Banerjee January 14, 2010 14:37 Printer Name: Yet to Come
ONE SIZE FAILS ALL – MENTAL HEALTH SERVICES 115
� holistic, person-centred older people’s health and careservices which address mental as well as physical healthneeds.
The National Dementia Strategy on specialistolder people’s mental health services
The National Dementia Strategy clearly covers services fordementia outside specialist older people’s mental health ser-vices. As with mental health care in general, dementia careis an issue for the health and social care system as a whole,rather than simply being the responsibility of specialist olderpeople’s mental health services. However, the interface witholder people’s mental health services is one of particular im-portance.
The consultation exercise for the National DementiaStrategy revealed strong concern from multiple sourcesabout the future of specialist older people’s mental healthservices and how they might be affected by the dementiastrategy. In particular concerns were raised that this strat-egy might mean that there would be a push for the divisionof specialist older people’s mental health services into or-ganic and functional elements.
The National Dementia Strategy identified that special-ist older people’s mental health services are a vital com-ponent part of service provision for people with demen-tia. It concluded that, in order to work well for dementia,this requires strong, well resourced and effective specialistolder people’s mental health teams. Finally it suggested thatthese teams needed to continue to have a role that extendsbeyond dementia, to include responsibility for older adultswith schizophrenia, depression and mania so that they havethe capacity and skills to provide the range of care neededfor people with dementia. This was made on the basis thatthe separation of ‘organic’ and ‘functional’ disorders is es-sentially a false dichotomy for specialist mental health ser-vice provision, and one that is likely to disadvantage peoplewith dementia with complex needs and their family carers.Specialist mental health services are needed that can de-liver good-quality care that is attuned to the specific needs
P1: IFM/OSW P2: TIXc10 JWBK439-Banerjee January 14, 2010 14:37 Printer Name: Yet to Come
116 MANAGING DEMENTIA IN A MULTICULTURAL SOCIETY
of older people. The natural history of dementia means thata substantial proportion of those affected will develop chal-lenging behaviour, including symptoms such as depression,hallucinations and delusions. These are likely to require carefrom specialist older people’s mental health services. For thesystem as a whole to work for people with dementia andtheir carers, these services need to be effective and avail-able. This means services that work for older people withboth functional and organic disorders and therefore a mix-ture of both.
Eliminating age discrimination in mental healthservice provision
As noted above there can be no doubt that there is agediscrimination in the development and provision of mentalhealth services.
There is a need to think very carefully through the op-tions for action in response to age discrimination in order toensure that we can be clear about the consequences of ac-tions and to make sure that these result in the best qualityoutcomes for older people with mental disorders and theirfamily carers. Accepting that age in itself is no marker ofthe need for a specific service and that services should beprovided on the basis of need, proposals have been made to‘open’ working adult services to older adults either by creat-ing a single undifferentiated service for all adults or an un-differentiated service for adults with functional disorder anda separate service for people with dementia.
Such service change is often offered benignly in an ac-knowledgement of differential investment and growth andan attempt to:
� remove discrimination on the basis of age; and� enable older people to have access to the services avail-
able for working age adults such as assertive outreachteams.
There are also other potential motivations for generatingundifferentiated or dementia-only services that are worth
P1: IFM/OSW P2: TIXc10 JWBK439-Banerjee January 14, 2010 14:37 Printer Name: Yet to Come
ONE SIZE FAILS ALL – MENTAL HEALTH SERVICES 117
articulating here in order to identify potential flaws in thereasoning. These include:
Motivation Potential flaws
Cost containment orminimisation
Combining services to save money. Cost savingshould not be the reason for closing specialistolder people’s mental health services andcost saving should not be presented asservice improvement, especially since qualityis likely to decrease for older people.
Convenience Combining services for administrativesimplicity. This should not be a driver for theamalgamation of services.
A sense of neatness Splitting into functional and organic servicesappears neat and sensible. This ignores realclinical overlap both between disorder and inthe skill set needed to manage the conditionsin later life.
Implementing thedementia strategy
The creation of dementia-only specialist mentalhealth services is the opposite of what is setout in the National Dementia Strategy.
Improving dementiacare
There is no room for improving the quality ofdementia care at the expense of older adultswith other mental disorder.
Removing agediscrimination bybeing ‘age blind’
There is ample evidence that adopting aposition where one is ‘blind’ todiscrimination will only entrench thatdiscrimination.
Opening working age adult services to olderpeople – one size does not fit all
There are two main flaws in opening existing working ageadult services. The first is that these services (be they gen-eral community mental health teams, assertive outreach, cri-sis resolution and home treatment teams) have been de-signed and developed to understand and meet the needs ofworking age adults with severe mental illness. This will re-sult in what Age Concern (2009) has termed ‘indirect agediscrimination’, this is an ‘apparently neutral practice thatdisadvantages people of a certain age, e.g. designing services
P1: IFM/OSW P2: TIXc10 JWBK439-Banerjee January 14, 2010 14:37 Printer Name: Yet to Come
118 MANAGING DEMENTIA IN A MULTICULTURAL SOCIETY
around the needs of young people without taking older peo-ple’s needs into account’. As discussed above, the needs ofthe two age groups are significantly different and it may notbe possible to meet them in the same place with the samestaff group. This is as true for the majority of older peoplewith functional severe mental illness as well as those with or-ganic disorder. It is striking that where services have openedtheir doors to older people how very few older people aretaken on by these teams. However, there is a small groupof older people with severe mental disorder who have needsthat are indistinguishable from those of adults of workingage and these may well be well served by these services andshould not be denied them.
The second flaw is that the team may well not havethe skills needed to assess, understand need, and plan anddeliver effective care for older people with severe mentalillness. This is because there are systematic differences interms of complexity and co-morbidity which means that adifferent skill set is needed by staff of all professions in theseteams. Skills developed with and for working age adults willoften fail older people with similar disorders. The CSIP ageequality guidance note states: ‘an ageing population has par-ticular needs and it is essential that care is aimed at thosewho most need it. . .The mental health needs of older peo-ple are often multi-factorial and frequently complicated byfailing physical health. This complexity requires the skillsof specialist practitioners. . .Specialist mental health servicesfor this group should be the bedrock on which other servicescan rely for clinical advice, support and practical help’. Thisis not simply a matter of training, it also involves attitudesand orientation.
Is an older adults service necessarily discriminatory interms of age?
The short answer to this question is ‘no’. The slightlylonger answer is ‘no, and not providing an older adults ser-vice is highly likely to result in care that is discriminatoryon the basis of age’. The problem here is largely one of lan-guage.
The basic principle must be that services should be pro-vided on the basis of need not age. However, age is a reason-able marker of different need especially in mental health,
P1: IFM/OSW P2: TIXc10 JWBK439-Banerjee January 14, 2010 14:37 Printer Name: Yet to Come
ONE SIZE FAILS ALL – MENTAL HEALTH SERVICES 119
where the majority of incident cases of serious mental ill-ness are in the 20-45 year age group, with a second peakfrom age 65 onwards with a second tranche of incident casesincluding those with dementia. There is a need for agree-ments between working age adults and older adult servicesthat acknowledge that age is a guide rather than an absolutemarker of service need. Such agreements have been reachedin the majority of mental health trusts and common featuresinclude:
� Those who grow old with enduring mental health prob-lems should stay under the care of the working age adultservice they are familiar with unless their needs would bebetter met by the older people’s service.
� Those with first episodes of mental illness after the age of65 will be seen in the first instance by the older people’sservice.
� Those with first episodes of mental illness before the ageof 65 will be seen in the first instance by the working ageadult service.
� Those with dementia of any age will be seen by the olderpeople’s service.
� Referrals of ‘graduate’ patients who are over the age of 65who need continuing psychiatric input and who may havea specific need for specialist older people’s psychiatricservices will be assessed and taken over, this will mostcommonly be because of physical frailty, co-morbidsevere complex medical disorder, or the advent of a pro-gressive dementia. In addition the older person’s servicewill receive referrals of patients under the age of 65 whoseneeds would be better met their services for the samereasons.
� Older people whose primary need is for specialist ser-vices such as substance misuse services or forensic mentalhealth care will not be denied access and care from suchservices on the basis of age.
� Where patients would benefit from joint working thisshould be provided.
� The mechanism for resolution of dispute where agree-ment is not reached lies ultimately with the Trust MedicalDirector as an issue of clinical governance.
P1: IFM/OSW P2: TIXc10 JWBK439-Banerjee January 14, 2010 14:37 Printer Name: Yet to Come
120 MANAGING DEMENTIA IN A MULTICULTURAL SOCIETY
Such a system is not discriminating on the basis of age but isusing age as a marker of difference in need so that differentservices are needed to provide services of equal quality tothose with different needs.
Addressing age discrimination by providingequal quality of care
So the ‘one size fits all ages’ approach is more likely toincrease age discrimination than it is to address it. This isbecause age here is a useful proxy for a different set of needsand therefore skills. The aim of the age equality agenda is togenerate services of equivalent good quality for people of allage. Delivering equivalent quality of care is therefore likelyto require enhancing current older people’s mental healthteams to have higher levels of functionality in terms of thecapacity for assertive outreach, for example. This wouldbenefit those with dementia as well as those older peoplewith functional disorder. In summary, the nature of risk andneed in older people with mental disorders means that, inorder to provide services that are of equivalent quality tothose available to adults of working age, specific provisionneeds to be made in terms of specialist community mentalhealth teams and inpatient services for older people withmental disorder.
Multi-functional community teams for mentalhealth in older adults
The focus of these teams should be on the ‘serious mentalillness’ element of older people’s mental health dealingwith urgent and complex disorders providing assessmentand care in the community for older people with functionaland organic disorders. The role of the memory servicesdiscussed above and in the National Dementia Strategy isa complementary one of early intervention and harm pre-vention in dementia and needs to be provided in a separateteam. Delivering equivalent quality of care to that providedby community mental health services for working age adultsis also likely to require enhancing current older people’s
P1: IFM/OSW P2: TIXc10 JWBK439-Banerjee January 14, 2010 14:37 Printer Name: Yet to Come
ONE SIZE FAILS ALL – MENTAL HEALTH SERVICES 121
mental health teams to have higher levels of functionalityin terms of the capacity for assertive outreach, for example.This would benefit those with dementia as well as thoseolder people with functional disorder.
LIAISON SERVICES IN GENERAL HOSPITALS
Up to 70% of acute hospital beds are currently occupiedby older people and up to a half of these may be peoplewith cognitive impairment, including those with dementiaand delirium. Levels of depression in general hospital wardsare also high (around 30%) and interfere with treatment andrehabilitation. The majority of these patients are not knownto specialist mental health services, and are undiagnosed.General hospitals are particularly challenging environmentsfor people with memory and communication problems, withcluttered ward layouts, poor signage and other hazards. Peo-ple with dementia and depression in general hospitals haveworse outcomes in terms of length of stay, mortality and in-stitutionalisation. This impact is not widely appreciated byclinicians, managers and commissioners. The NAO has esti-mated the excess cost of dementia to be more than £6 millionper year in an average general hospital.
There are marked deficits in the knowledge and skills ofgeneral hospital staff who care for older people with mentaldisorder. Often, insufficient information is sought from rela-tives and carers. This means that person-centred care is notdelivered and it can lead to under-recognition of delirium,dementia, and depression. Poor care can lead to malnutri-tion and dehydration for people with dementia, an outcomehighlighted in the Age Concern England report Hungry tobe Heard. The National Dementia Strategy presents threeways to deliver improvement:
� the identification of a senior clinician within the generalhospital to take the lead for quality improvement in de-mentia care in the hospital;
� the development of an explicit care pathway for the man-agement and care of people with dementia in hospital, ledby that senior clinician; and
P1: IFM/OSW P2: TIXc10 JWBK439-Banerjee January 14, 2010 14:37 Printer Name: Yet to Come
122 MANAGING DEMENTIA IN A MULTICULTURAL SOCIETY
� commissioning specialist liaison older people’s mentalhealth teams to work in general hospitals.
Here we will focus on the commissioning of specialist liai-son older people’s mental health teams working in generalhospitals. They are advocated by the NICE/SCIE guidelineon dementia services and can provide rapid high-quality spe-cialist assessment and input into care planning for those withall possible mental health needs admitted to general hospi-tals, including input into ongoing care and discharge plan-ning. They will generally consist of a multidisciplinary teamof three to four members of staff (part-time consultant, staffgrade doctor, nurse and psychologist/therapist) with admin-istrative support and a base in the general hospital. They cancover the whole range of mental health problems in olderadults, not just dementia, but are likely to be of major valueto people with dementia.
These teams could work closely with the designated gen-eral hospital lead to build skills and improve care throughthe hospital. They need to have good links with the socialwork assessment teams based in or linked to the hospital.They are already provided in some but by no means all hos-pitals and there is major variation in composition and qualityof the services provided across the country. Hitherto invest-ment in mental health liaison services has focused on acuteassessments in accident and emergency departments and isoften focused on self-harm and acute psychosis in adults ofworking age rather than older people on the wards. There isalso a clear need for specialist older people’s mental healthliaison services to be commissioned by PCTs to work on thewards with skills in the diagnosis and management of de-mentia and other mental disorder in later life.
Specialist dementia care services into carehomes – looked after adults, the nextbattleground for quality
One-third of people with dementia live in care homes andover two-thirds of all people living in care homes havedementia and up to a half have depression. This state of
P1: IFM/OSW P2: TIXc10 JWBK439-Banerjee January 14, 2010 14:37 Printer Name: Yet to Come
ONE SIZE FAILS ALL – MENTAL HEALTH SERVICES 123
affairs has not been planned for, either through commis-sioning services or through workforce planning. In the past30 years the proportion of people with dementia in carehomes has increased by two to three-fold. The severity andcomplexity of needs of those admitted to care homes hasalso increased without changes in the ways that medical careis provided to homes. It is striking that while people in carehomes, by definition, have the most severe and complexhealth problems in society, they receive less specialist com-munity health services than those living at home. Equallyas these health problems have grown there has been noincrease in primary care skills and input into these homes.The need for workforce development in health and socialcare is profound, and training in this area is covered in theNational Dementia Strategy. Compared to the energy andeffort that society puts into ‘looked after children’, it isstriking that so little resource is committed to these ‘lookedafter adults’ who are amongst the most socially excludedand disadvantaged in the community.
There is no doubt that residential care may be the mostappropriate and effective way of meeting the needs of some-one with dementia. There are care homes that provide ex-cellent care, paying close attention to leadership and staffmanagement, staff training and development, and person-centred care planning. They can also provide a physicalenvironment that enables people with dementia to movearound the home safely and an active social environmentwith purposeful activities that relate to individual prefer-ences. However, evidence from the Alzheimer’s Society’sHome from Home report and other sources show that inmany homes, residents have little to do and there is immensesocial poverty with the typical person in a care home hav-ing just two minutes interaction with staff or other residentsover a six-hour period of observation (excluding time spenton care tasks). The mental health needs of people living incare homes are extensive and generally not well met. Be-havioural disturbance in dementia in these settings is bothvery common and a cause of stress to residents and staff.It is striking that there is very little in the way of activenon-pharmacological management of these problems in care

P1: IFM/OSW P2: TIXc10 JWBK439-Banerjee January 14, 2010 14:37 Printer Name: Yet to Come
124 MANAGING DEMENTIA IN A MULTICULTURAL SOCIETY
homes, despite accumulating evidence of the effectiveness ofold age psychiatric intervention. Current input from mentalhealth services is generally on an ad-hoc basis or reactivewith referrals at times of crisis.
An issue of particular concern is the use of anti-psychoticmedication in care homes for the management of be-havioural and psychological symptoms in those residentswith dementia. Those who have criticised current prac-tice include the Parliamentary Accounts Committee, theAlzheimer’s Society, the National Dementia Strategy andthe All-Party Parliamentary Group on Dementia. It appearsthat there are particular risks that are serious and negativein the use of anti-psychotic medications for people with de-mentia, including increased mortality and stroke. There isaccumulating evidence that in care homes they are initiatedtoo freely, they are not reviewed appropriately following ini-tiation, and they are not withdrawn as quickly as they couldbe. Improving the quality of care in care homes requiresthese issues to be addressed effectively.
In the course of developing the National DementiaStrategy, one means suggested to address these problemshas been the commissioning of a system of regular specialistmental health assessment following admission, and regularspecialist review for this vulnerable population. This wouldenhance the quality of care by providing a regular forumfor discussion between nursing staff, GPs and specialistolder people’s mental health teams to identify and managethe mental health problems of care home residents. Anyintervention would need to be in partnership with the GPsresponsible for care within care homes. In this system thequality of mental health care for residents in care homescould be improved by:
� specialist assessment of mental health needs following alladmissions;
� regular six-monthly mental health reviews of residents inconjunction with the GP and nursing home staff;
� providing access to specialist advice for problems arisingbetween reviews to prevent problems by means of a regu-lar pattern of visiting;
P1: IFM/OSW P2: TIXc10 JWBK439-Banerjee January 14, 2010 14:37 Printer Name: Yet to Come
ONE SIZE FAILS ALL – MENTAL HEALTH SERVICES 125
� the formulation and deployment of non-pharmacologicalmanagement strategies for behavioural disorder in de-mentia, so avoiding the initiation of anti-psychotic med-ication;
� specialist input into decision making concerning the initia-tion, review and cessation of anti-psychotic medication forpeople with dementia;
� rapid specialist review of all those with dementia initiatedon anti-psychotic medication;
� rapid specialist response to problems as they occur withinhomes; and
� assessment of the residential care provided and the poten-tial for improvement to create a more therapeutic envi-ronment.
Commissioners could achieve this by commissioning an ex-tension of the existing role of the old age community men-tal health teams building on existing capacity, rather thanby setting up a separate service. Joint commissioning of in-reach services from other professionals, such as communitypharmacists, community dentists, arts therapists and geri-atricians, could also improve support to care homes andenhance their environment.
IN-PATIENT CARE FOR OLDER PEOPLE WITHMENTAL DISORDERS
Sometimes older people with dementia and other mentalhealth problems, due to the nature and severity of their ill-ness or risk to themselves or others, will require a period ofin-patient care. There are questions similar to those posedby the provision of community mental health care above,which need to be answered in terms of how good quality,safe, in-patient care can be provided for older people that isnot discriminatory on the basis of age. Most mental healthtrusts will have specialist old age psychiatric wards that arestaffed by specialist nurses and medical staff working as partof a multi-disciplinary team. Very few cases are admitted di-rectly to such wards in that most people are assessed and
P1: IFM/OSW P2: TIXc10 JWBK439-Banerjee January 14, 2010 14:37 Printer Name: Yet to Come
126 MANAGING DEMENTIA IN A MULTICULTURAL SOCIETY
managed in the community in the first instance and admit-ted only when there is absolutely no alternative.
In almost all areas there has been a decrease in the num-bers of such acute assessment beds and the numbers aresmaller than the numbers of general adult wards. In manyunits there will be only a single older people’s mental healthward. There are three issues that are of particular concern atthis time:� the value of separating organic patients from functional
patients;� the need for a specialist functional ward for older people;� the value of separating male from female patients.
There is clinical heterogeneity in whether ‘organic’ patientsare cared for in a separate ward from ‘functional’ patients.Such a division is attempted in some units but not others.There is no clear consensus about whether it is better to havesegregated or mixed wards and this can cause confusion forcommissioners and for trust management. The argument formixed wards are that many people who are admitted havecomplex mixed disorders or uncertain diagnoses which iswhy they are admitted. Also running two wards can be moreexpensive than running a mixed unit and ‘organic’ wards canbecome gloomy places taking on the negative attributes ofsome care homes. Advocates of separation would report thatmany people complain that they do not like being on a wardwith people with dementia. However, it is often people withdementia who are lacking in insight that make such com-ments and they would be on the dementia-only ward in asegregated system. Also the individuals they complain aboutmay well be people with psychosis or depression whose be-haviour is disturbed. There is a need for the faculty of oldage psychiatry to produce definitive guidance in this area.
One possible consequence of separating organic fromfunctional wards for older people is that the older people’sfunctional ward is closed and that older adults with func-tional disorders are admitted to the same wards as workingage adults. This can be seen as a cost-saving exercise orthe logical extension of abandoning a missed system. Theproblems with this are that older people often find wards
P1: IFM/OSW P2: TIXc10 JWBK439-Banerjee January 14, 2010 14:37 Printer Name: Yet to Come
ONE SIZE FAILS ALL – MENTAL HEALTH SERVICES 127
filled with adults of working age with serious mental illnessvery intimidating environments. Also, the same issues withrespect to the need for a different skill set in order to delivergood quality care applies in this case. Older people havea different pattern of risk and need and so may not meetcriteria for admission or may be discharged more quicklythan would be best. There are few examples of this approachworking well but again there is a need for the faculty of oldage psychiatry to produce definitive guidance in this area.
Finally gender separation at a ward level is seen as agood thing in working age adult services and generally in thehealth services. Why might this be a problem for older peo-ple with mental problems? The answer is that there is oftenonly a single ward in a particular area. If there is gender sep-aration then it may be that the male or the female ward willbe in a neighbouring PCT, thus increasing markedly the dis-tance that visitors (who are often old and frail themselves)need to travel. Older people have long stay lengths and thiscan prove problematic. This is not such a problem for work-ing age services where there are usually multiple wards in asingle area allowing such separation. The issues become am-plified if one separates on the basis of diagnosis and well asgender. One way ahead is for older people’s mental healthwards to be built so that everyone has their own bedroomwith their own en suite bathing facilities. This enables ev-erybody to have their own space and avoids the need forseparation by gender or diagnosis.

P1: IFM/OSW P2: TIXc10 JWBK439-Banerjee January 14, 2010 14:37 Printer Name: Yet to Come
128
P1: IFM/OSW P2: TIXref JWBK439-Banerjee January 14, 2010 11:12 Printer Name: Yet to Come
REFERENCES
ADAMSON, J. (2001) Awareness and understanding of demen-tia in African-Caribbean and South Asian families. Health andSocial Care in the Community, 9, 391–396.
ADELMAN, S., BLANCHARD, M. & LIVINGSTON, G. (2009)A systematic review of the prevalence and covariates of dementiaor relative cognitive impairment in the older African-Caribbeanpopulation in Britain. International Journal of Geriatric Psychia-try, Forthcoming.
AGE CONCERN (2009) Age of equality? Outlawing age discrimi-nation beyond the workplace, London, Age Concern England.
AGE CONCERN (2006) Hungry to be heard. The scandal ofmalnourished older people in hospital, London, Age ConcernEngland.
AGGARWAL, N., VASS, A. A., MINARDI, H. A., WARD, R.,GARFIELD, C. & CYBYK, B. (2003) People with dementia andtheir relatives: personal experiences of Alzheimer’s and of theprovision of care. Journal of Psychiatric and Mental Health Nurs-ing, 10, 187–197.
AHMAD, W. (1996a) Family obligations and social change amongAsian communities. IN AHMAD, W. & ATKIN, K. (Eds.) Raceand Community Care, Buckingham, Open University Press.
AHMAD, W. & ATKIN, K. (1996) Race and Community Care,Buckingham, Open University Press.
AHMAD, W. & BRADBY, H. (2007) Locating ethnicity andhealth: exploring concepts and contexts. Sociology of Health andIllness, 29, 795–810.
ALZHEIMER’S SOCIETY (2007) Home from home. A reporthighlighting opportunities for improving standards of dementiacare in care homes, London, Alzheimer’s Society.
AMADUCCI, L, A., ROCCA, W, A., & SCHOENBERG, B, S.(1986) Origin of the distinction between Alzheimer’s disease andsenile dementia: How history can clarify nosology. Neurology, 36,1497–1499.
Managing Dementia in a Multicultural Society Sube Banerjee and Vanessa LawrenceC© 2010 John Wiley & Sons, Ltd
129
P1: IFM/OSW P2: TIXref JWBK439-Banerjee January 14, 2010 11:12 Printer Name: Yet to Come
130 REFERENCES
ANESHENSEL, C.S., PEARLIN, L.I., MULLAN, J.T., ZARIT,S.H. & WHITLACH, C.J. (1995) Profiles in Caregiving: TheUnexpected Career, California, Academic Press.
ANGEL, R. & THOITS, P. (1987) The impact of culture on thecognitive structure of illness. Culture, Medicine and Psychiatry,11, 465–494.
ANTONELLI, I. R., MARRA, C., GEMMA, A., CAPPARELLA,O. & CARBONIN, P. U. (1992) Unrecognised dementia: socio-demographic correlates. Aging (Milano), 4, 301–304.
ARANDA, M. P. & KNIGHT, B. G. (1997) The influence of eth-nicity and culture on the caregiver stress and coping process: asociocultural review and analysis. The Gerontologist, 37, 342–354.
ARIE, T. (1971) Morale and the planning of Psychogeriatric ser-vices. British Medical Journal, 3, 166–170.
ARIE, T. & ISSACS, A, D. (1978). The development of Psy-chogeriatric services for the elderly in Britain. IN ISSACS,A, D. & POST, F. (Eds.) Studies in Geriatric Psychiatry,Chichester, Wiley.
ARMSTRONG, T. L. & SWARTZMAN, L. C. (2001) Cross-cultural differences in illness models and expectations for thehealth care provider-client/patient interaction. IN KAZARIAN,S. S. & EVANS, D. R. (Eds.) Handbook in Cultural HealthPsychology, Ontario, Academic Press.
ATKIN, K. & ROLLINGS, J. (1996) Looking after their own?Family care-giving among Asian and Afro-Caribbean communi-ties. IN AHMAD, W. & ATKIN, K. (Eds.) Race and CommunityCare, Buckingham, Open University Press.
AUDIT COMMISSION (2000) Forget Me Not: Mental Health Ser-vices for Older People, London, Audit Commission.
AUDIT COMMISSION (2002) Forget Me Not 2002: DevelopingMental Health Services for Older People in England, London,Audit Commission.
BALLARD, C. G., BANNISTER, C. & OYEBODE, F. (1996)Depression in dementia sufferers – a review. International Jour-nal of Geriatric Psychiatry, 11, 507–515.
BALLARD, R. & KALRA, V. S. (1994) The Ethnic Dimensions ofthe 1991 Census: A Preliminary Report. Manchester, ManchesterCensus Group.
BANERJEE, S., WILLIS, R., MATTHEWS, D., CONTELL, F.,CHAN, J. & MURRAY, J. (2007) Improving the quality of carefor mild to moderate dementia: an evaluation of the CroydonMemory Service Model. International Journal of Geriatric Psy-chiatry, 22, 782–788.
P1: IFM/OSW P2: TIXref JWBK439-Banerjee January 14, 2010 11:12 Printer Name: Yet to Come
REFERENCES 131
BARTLETT, R. & O’CONNER, D. (2007) From personhood tocitizenship: broadening the conceptual base for dementia prac-tice and research. Journal of Aging Studies, 21, 107–118.
BASTING, A. (2003) Looking back from loss: views of the self inAlzheimer’s disease. Journal of Aging Studies, 17, 87–99.
BECKER, M. H. (1974) The health belief model and sick role be-havior. Health Education Monographs, 2, 409–419.
BHACHU, P. (1985) Twice Migrants: East African Sikh Settlers inBritain, London, Tavistock Publishers.
BHATNAGAR, K. & FRANK, J. (1997) Psychiatric disorders inelderly from the Indian sub-continent living in Bradford. Inter-national Journal of Geriatric Psychiatry, 12, 907–912.
BOLLER, F., FORBES, M. (1998) History of dementia and de-mentia in history: an overview. Journal of the Neurological Sci-ences. 158, 125–133.
BONEHAM, M. A., WILLIAMS, K. E., COPELAND, J. R. M.,MCKIBBIN, P., WILSON, K., SCOTT, A. & SAUNDERS,P. A. (1997) Elderly people from ethnic minorities in Liverpool:mental illness, unmet need and barriers to service use. Health andSocial Care in the Community, 5, 173–180.
BOWES, A. & WILKINSON, H. (2002) South Asian people withdementia: research issues. IN WILKINSON, H. (Ed.) The Per-spectives of People with Dementia: Research Methods and Moti-vations, London, Jessica Kingsley.
BOWES, A. & WILKINSON, H. (2003) ‘We didn’t know it wouldget that bad’: South Asian experiences of dementia and the ser-vice response. Health and Social Care in the Community, 11,387–396.
BRAITHWAITE, V. (1998) Institutional respite care: breakingchores or breaking social bonds. The Gerontologist, 38, 610–717.
BRAUDY HARRIS, P. (1993) The misunderstood caregiver? Aqualitative study of the male caregiver of Alzheimer’s disease vic-tims. The Gerontologist, 33, 551–556.
BROOKMEYER, R., JOHNSON, E., ZIEGLER-GRAHAM,K., ARRIGHI, H (2007) Forecasting the global burden ofAlzheimer’s disease. Alzheimer’s and Dementia: the Journal ofthe Alzheimer’s Association, 3: 186–191.
BROD, M., STEWART, A. L. & SANDS, L. (1999) Conceptu-alisation and measurement of quality of life in dementia: theDementia Quality of Life Instrument (Dqol). The Gerontologist,39, 25–35.
BRODATY, H., THOMSON, C., THOMPSON, C. & FINE, M.(2005) Why caregivers of people with dementia and memory loss
P1: IFM/OSW P2: TIXref JWBK439-Banerjee January 14, 2010 11:12 Printer Name: Yet to Come
132 REFERENCES
don’t use services. International Journal of Geriatric Psychiatry,20, 537–546.
BROWNFOOT, J. (1998) The needs of people with dementia andtheir carers within three ethnic groups in Haringey. London,Haringey Housing and Social Services and the London RegionalOffice of the Alzheimer’s Disease Society.
BROWNLIE, J. (1991) A hidden problem?: Dementia amongstminority ethic groups. Stirling, Dementia Services DevelopmentCentre.
BUONO, M. D., BUSATO, R., MAZZETTO, M., PACCA-GNELLA, B., ALEOTTI, F., ZANETTI, R., BIANCHETTI,A., TRABUCCHI, M. & DE LEO, D. (1999) Community carefor patients with Alzheimer’s Disease and non-demented elderlypeople: use and satisfaction with services and unmet needs infamily caregivers. International Journal of Geriatric Psychiatry,14, 915–924.
BURTON, L. & SORENSEN, S. (1993) Temporal context andthe caregiving role: perspectives from ethnographic studies ofmultigeneration African American families. IN ZARIT, S. H.,PEARLIN, L. I. & SCHAIE, K. W. (Eds.) Caregiving Systems:Informal and Formal Helpers, New Jersey, Erlbaum.
BURY, M. (1982) Chronic illness as biographical disruption. Soci-ology of Health and Illness, 4, 167–182.
CAMPION, J. & BHUGRA, D. (1998) Religious and indigenoustreatment of mental illness in South India – a descriptive study.Mental Health, Religion & Culture, 1, 21–29.
CARE SERVICES IMPROVEMENT PARTNERSHIP (2005)Everybody’s Business. Leeds, Care Services Improvement Part-nership.
CARPENTER, B. D., XIONG, C., PORENSKY, E. K., LEE, M.M., BROWN, P. J., COATS, M., JOHNSON, D. & MORRIS,J. C. (2008) Reaction to a dementia diagnosis in individuals withAlzheimer’s disease and mild cognitive impairment. Journal ofAmerican Geriatrics Society, 56, 405–412.
CASSERTA, M. S., LUND, D. A., WRIGHT, S. D. & RED-BURN, D. E. (1987) Caregivers to dementia patients: the uti-lization of community services. The Gerontologist, 27, 209–214.
CHAMBERLAIN, M. (1998) Caribbean Migration: GlobalisedIdentities, London, Routledge.
CHANDARANA, P. & PELLIZZARI, J. R. (2001) Health psy-chology: South Asian perspectives. IN KAZARIAN, S. S. &EVANS, D. R. (Eds.) Handbook of Cultural Health Psychology,Ontario, Academic Press.
P1: IFM/OSW P2: TIXref JWBK439-Banerjee January 14, 2010 11:12 Printer Name: Yet to Come
REFERENCES 133
CHARMAZ, K. (1987) Struggling for a self: identity levels ofthe chronically ill. Research in the Sociology of Health Care, 6,283–321.
CINNIRELLA, M. & LOEWENTHAL, K. M. (1999) Religiousand ethnic group influences on the beliefs about mental illnesses:A qualitative study. British Journal of Medical Psychology, 72,505–524.
CLARE, L. (2002) We’ll fight it as long as we can: coping withthe onset of Alzheimer’s disease. Aging and Mental Health, 6,139–148.
CLARE, L. (2003) Managing threats to self: awareness in earlystage Alzheimer’s disease. Social Science & Medicine, 57,1017–1029.
CLARE, L., GOATER, L. & WOODS, R. T. (2006) Illness rep-resentations in early-stage dementia: a preliminary investigation.International Journal of Geriatric Psychiatry, 21, 761–767.
CLARE, L., ROTH, I. & PRATT, R. (2005) Perceptions ofchange over time in early-stage Alzheimer’s disease. Dementia,4, 487–520.
CLARE, L., ROWLANDS, J., BRUCE, E. & DOWNS, M. (2008)‘I don’t do like I used to do’: a grounded theory approach toconceptualising awareness in people with moderate to severe de-mentia living in long-term care. Social Science & Medicine, 66,2366–2377.
CLARE, L. & SHAKESPEARE, S. (2004) Negotiating the impactof forgetting: dimensions of resistance in task-oriented conversa-tions between people with early-stage dementia and their part-ners. Dementia, 3, 211–232.
COHEN-MANSFIELD, J., GOLANDER, H. & ARNHEIM, G.(2000) Self-identity in older persons suffering from demen-tia: preliminary results. Social Science & Medicine, 51, 381–394.
COHEN-MANSFIELD, J., PARPURA-GILL, A. & GOLAN-DER, H. (2006a) Salience of self-identity roles in persons withdementia: differences in perceptions among elderly persons,family members and caregivers. Social Science & Medicine, 62,745–757.
COHEN-MANSFIELD, J., PARPURA-GILL, A. & GOLAN-DER, H. (2006b) Utilization of self-identity roles for designinginterventions for persons with dementia. Journal of Gerontology:Psychological Sciences, 61B, 202–212.
COHEN, C. I. (1993) The biomedicalization of psychiatry: a criticaloverview. Community Mental Health Journal, 29, 509–521.
P1: IFM/OSW P2: TIXref JWBK439-Banerjee January 14, 2010 11:12 Printer Name: Yet to Come
134 REFERENCES
COHEN, D. & EISENDORFER, C. (1986) The Loss of Self: AFamily Resource for the Caregiver of Alzheimer’s Disease and Re-lated Disorders, New York, W. W. Norton & Company.
COLLINS, C., KING, S. & KOKINAKIS, C. (1994) Communityservices issues before nursing home placement of persons withdementia. Western Journal of Nursing Research, 16, 40–52.
COLLINS, C., STOMMEL, M., KING, S. & GIVEN, C. W. (1991)Assessment of the attitudes of family caregivers toward commu-nity services. The Gerontologist, 31, 756–761.
COMAS-HERRERA, A., WITTENBERG, R., PICKARD, L. &KNAPP, M. (2007) Cognitive impairment in older people: futuredemand for long-term care services and the associated costs. In-ternational Journal of Geriatric Psychiatry, 22, 1037–1045.
COMMANDER, M. J., DHARAN, S. P. S., ODELL, S. M. &SURTEES, P. G. (1997) Access to mental health care in aninner-city health district. II: Association with demographic fac-tors. British Journal of Psychiatry, 170, 317–320.
COOPER, C., BALAMURALI, T. B.S. & LIVINGSTON, G.(2007) A systematic review of the prevalence and covariates ofanxiety in caregivers of people with dementia. International Psy-chogeriatics, 19, 175–195.
COTRELL, V. & SCHULZ, R. (1993) The perspective of the pa-tient with Alzheimer’s disease: a neglected dimension of demen-tia research. The Gerontologist, 33, 205–211.
COVINSKY, K. E., NEWCOMER, R., FOX, P., WOOD, J.,SANDS, L., DANE, K. & YAFFE, K. (2003) Patient and care-giver characteristics associated with depression in caregivers ofpatients with dementia. Journal of General Internal Medicine, 18,1006–1014.
DAKER-WHITE, G., BEATTIE, A., GILLIARD, J. & MEANS,R. (2002) Minority ethnic groups in dementia care: a review ofservice needs, service provision and models of good practice. Ag-ing and Mental Health, 6, 101–108.
DAUTZENBERG, M. G H., DIEDERIKS, J. P. M., PHILIPSEN,H. & TAN, F. E. S. (1999) Multigenerational caregiving and well-being: distress of middle-aged daughters providing assistance toelderly parents. Women & Health, 29, 57–74.
DE BOER, M. E., HERTOGH, C. M., DROES, R. M., RIPHA-GEN, I. I., JONKER, C. & EEFSTING, J. A. (2007) Sufferingfrom dementia – the patient’s perspective: a review of the litera-ture. International Psychogeriatrics, 19, 1021–1039.
DE LA CUESTA, C. (2005) The craft of care: family care of rel-atives with advanced dementia. Qualitative Health Research, 15,881–896.
P1: IFM/OSW P2: TIXref JWBK439-Banerjee January 14, 2010 11:12 Printer Name: Yet to Come
REFERENCES 135
DEPARTMENT OF HEALTH (2001) National Service Frame-work for Older People. London, Department of Health.
DEPARTMENT OF HEALTH (2005) Delivering race quality inmental health care. London, Department of Health.
DEPARTMENT OF HEALTH (2008a) Carers at the heart of the21st century families and communities: a caring system on yourside, a life of your own. London, Department of Health.
DEPARTMENT OF HEALTH (2008b) End of Life CareStrategy – promoting high quality care for all adults at the endof life. London, Department of Health.
DEPARTMENT OF HEALTH (2009) Living Well With Demen-tia: A National Dementia Strategy. London, Department ofHealth.
DERKSEN, E., VERNOOIJ-DASSEN, M., GILLISSEN, F.,RIKKERT, M., O. & SCHELTENS, P. (2006) Impact of diag-nostic disclosure in dementia on patients and carers: qualitativecase series analysis. Aging and Mental Health, 10, 525–531.
DILWORTH-ANDERSON, P., WILLIAMS, I. C. & GIBSON, B.E. (2002) Issues of race, ethnicity, and culture in caregiving re-search. The Gerontologist, 42, 237–272.
DILWORTH-ANDERSON, P., BRUMMETT, B. H., GOOD-WIN, P., WALLACE WILLIAMS, S., WILLIAMS, R. B. &SIEGLER, I. C. (2005) Effect of race for cultural justificationsfor caregiving. Journal of Gerontology: Social Sciences, 60B,257–262.
DILWORTH-ANDERSON, P., GIBSON, B.E., & BURKE, J.D.(2006) Working with African American families. IN YEO, G. &GALLAGHER-THOMPSON, D. (Eds) Ethnicity and the De-mentias, Second Edition, New York, Routledge.
DOWNS, M. (1997) The emergence of the person in dementia re-search. Ageing & Society, 17, 597–607.
DOWNS, M. (2000) Dementia in a socio-cultural context: an ideawhose time has come. Ageing & Society, 20, 369–375.
DROES, R. M. (1997) Psychomotor group therapy for dementedpatients in the nursing home. IN MIESEN, B. (Ed.) Care-givingin Dementia, London, Routledge.
DROES, R. M. (2007) Insight in coping with dementia: listening tothe voice of those who suffer from it. Aging and Mental Health,11, 115–118.
DROES, R. M. & BOELENS-VAN DER KNOOP, E. (2006)Quality of life in dementia in perspective: an explorative studyof variations in opinions among people with dementia and theirprofessional caregivers, and in literature. Dementia, 5, 533–558.
P1: IFM/OSW P2: TIXref JWBK439-Banerjee January 14, 2010 11:12 Printer Name: Yet to Come
136 REFERENCES
ELLIOT, K., DIMINNO, M. & LAM, D. (1996) Working withChinese families in the context of dementia. IN YEO, G. &GALLAGHER-THOMPSON, D. (Eds.) Ethnicity and the De-mentias, Washington DC, Taylor and Francis.
FARRAN, C. J., MILLER, B., KAUFMAN, J. E. & DAVIS, L.(1997) Race, finding meaning, and caregiver distress. Journal ofAging and Health, 9, 316–333.
FEINBERG, L. F. & WHITLATCH, C. J. (2001) Are personswith cognitive impairment able to state consistent choices? TheGerontologist, 41, 374–382.
FERRI, C., PRINCE, M., BRAYNE, H., BRODATY, H.,FRATIGLIONI, L., GANGULI, M., HALL, K., HASEGAWA,H., HENDRIE, H., HUANG, Y. (2006) Global prevalence ofdementia: a Delphi consensus study. The Lancet, 366, 9503,2112–2117.
FINCH, J. & MASON, J. (1993) Negotiating Family Responsibili-ties, London, Sage Publications.
FOX, K., HINTON, W. L. & LEVKOFF, S. (1999) Take up thecaregiver’s burden: stories of care for urban African Ameri-can elders with dementia. Culture, Medicine and Psychiatry, 23,501–529.
GAFSTROM, M. & WINBLAD, B. (1995) Family burden in thecare of the demented and nondemented elderly – a longitudinalstudy. Alzheimer Disease and Associated Disorders, 2, 78–86.
GAINES, A. D. (1989) Alzheimer’s disease in the context of black(Southern) culture. Health Matrix, 6, 33–38.
GALLAGHER-THOMPSON, D. (2006) The family as the unitof assessment and treatment in work with ethnically diverseolder adults with dementia. IN YEO, G. & GALLAGHER-THOMPSON, D. (Eds.) Ethnicity and the Dementias, SecondEdition, New York, Taylor and Francis Group.
GALLAGHER, T. J., AREAN, P. A. & COON, D. (2000) Devel-opment and implementation of intervention strategies for cultur-ally diverse caregiving populations. IN SCHULZ, R. (Ed.) Hand-book on Dementia Caregiving: Evidence-Based Interventions forFamily Caregivers, New York, Springer.
GHOSH, P. & KHAN, S. A. (2005) Transcultural Geriatrics: Caringfor Elderly People of Indo-Asian Origin Authors, Oxford, Rad-cliffe Publishing.
GILLIAM, C. M. & STEFFEN, A. M. (2006) The relationshipbetween caregiving self-efficacy and depressive symptoms in de-mentia family caregivers. Aging and Mental Health, 10, 79–86.
GILLIES, B. A. (2000) A memory like clockwork: accounts of liv-ing through dementia. Aging and Mental Health, 4, 366–374.
P1: IFM/OSW P2: TIXref JWBK439-Banerjee January 14, 2010 11:12 Printer Name: Yet to Come
REFERENCES 137
GILMOUR, J. A. & HUNTINGTON, A. D. (2005) Finding thebalance: living with memory loss. International Journal of Nurs-ing Practice, 11, 118–124.
GLASER, B. & STRAUSS, A. (1967) The Discovery of GroundedTheory: Strategies for Qualitative Research, Chicago, Aldine.
GOLDBERG, D. & HUXLEY, P. (1980) Mental Illness in theCommunity: The Pathway to Psychiatric Care, London, TavistockPublications.
GOODENOUGH, W. H. (1999) Outline of a framework for a the-ory of cultural evolution. Cross-Cultural Research, 33, 84–107.
GULLIFORD, M. C. (1994) Health and health care in the En-glish speaking Caribbean: a British public health physician’s viewof the Caribbean. Journal of Public Health Medicine, 16, 263–269.
GWYTHER, L. (1994) Service delivery and utilisation: Re-search directions and clinical implications. IN LIGHT, E.,NIEDERECHE, G. & LEBOWITZ, B. (Eds.) Stress Effects onFamily Caregivers of Alzheimer’s Patients: Research and Inter-ventions. New York, Springer.
HAGGER, M. S. & ORBELL, S. (2003) A meta-analytic review ofthe common-sense model of illness representations. Psychologyand Health, 18, 141–184.
HAIGHT, B. K., BACHMAN, D. L., HENDRIX, S., WAGNER,M. T., MEEKS, A. & JOHNSON, J. (2003) Life review: treatingthe dyadic family unit with dementia. Clinical Psychology andPsychotherapy, 10, 165–174.
HALEY, W. E., GITLIN, L. N., WISNIEWSKI, S. R.,MAHONEY, D. F., COON, D. W. & WINTER, L. (2004)Well-being, appraisal and coping in African American andCaucasian dementia caregivers: findings from the REACHstudy. Aging and Mental Health, 8, 316–329.
HALEY, W. E., ROTH, D. L., COLETON, M. I., FORD, G. R.,WEST, C. A. C., COLLINS, R. P. & ISOBE, T. L. (1996) Ap-praisal, coping and social support as mediators of well-being inblack and white caregivers of patients with Alzheimer’s disease.Journal of Consulting and Clinical Psychology, 64, 120–129.
HALEY, W. E., WEST, C. A. C., VADLEY, V. G., FORD, G. R.,WHITE, F. A., BARRETT, J. J., HARRELL, L. E. & ROTH,D. L. (1995) Psychological, social and health impact of caregiv-ing: a comparison of Black and White family caregivers and non-caregivers. Psychology and Ageing, 10, 540–552.
HARRIS, P. (1993) The misunderstood caregiver? A qualitativestudy of the male caregiver of Alzheimer’s disease victims. TheGerontologist, 33, 551–556.
P1: IFM/OSW P2: TIXref JWBK439-Banerjee January 14, 2010 11:12 Printer Name: Yet to Come
138 REFERENCES
HARRIS, P. B. & STERIN, G. J. (1999) Insider’s perspective:defining and preserving the self in dementia. Journal of MentalHealth and Aging, 5, 241–256.
HASHMI, M. (2009) Dementia: an anthropological perspective. In-ternational Journal of Geriatric Psychiatry, 24, 207–212.
HEPBURN, K. W., TORNATORE, J., CENTER, B. & OST-WALD, S. W. (2001) Dementia family caregiver training: affect-ing beliefs about caregiving and caregiver outcomes. Journal ofthe American Geriatrics Society, 49, 450–457.
HINRICHSEN, G. A. & RAMIREZ, M. (1992) Black and whitedementia caregivers: a comparison of their adaptation, adjust-ment, and service utilization. The Gerontologist, 29, 328–332.
HOE, J., KATONA, C., ORRELL, M. & LIVINGSTON, G.(2007) Quality of life in dementia: care recipient and caregiverperceptions of quality of life in dementia: the LASER-AD study.International Journal of Geriatric Psychiatry, 22, 1031–1036.
HOFFMAN, R. L. & MITCHELL, A. M. (1998) Caregiver burden:historical development. Nursing Forum, 33, 5–12.
HOLMES, C., COOPER, B. & LEVY, R. (1995) Dementia knownto mental health services: first finding of a case register for a de-fined elderly population. International Journal of Geriatric Psy-chiatry, 10, 875–881.
HOLROYD, S., TURNBULL, Q. & WOLF, A. M. (2002) Whatare patients and their families told about the diagnosis of demen-tia? Results of a family survey. International Journal of GeriatricPsychiatry, 17, 218–221.
HOWORTH, P. & SAPER, J. (2003) The dimensions of insight inpeople with dementia. Aging and Mental Health, 7, 113–122.
HUSBAND, H. J. (2000) Diagnostic disclosure in dementia: an op-portunity for intervention. International Journal of Geriatric Psy-chiatry, 15, 544–547.
HUPPART, F. A., BRAYNE, C. & O’CONNOR, D. W. (1994)Dementia and Normal Aging, Cambridge, Cambridge UniversityPress.
ILIFFE, S., MANTHORPE, J. & EDEN, A. (2003) ‘Sooner orlater? Issues in the early diagnosis of dementia in general prac-tice: a qualitative study. Family Practice, 20, 376–8.
ILIFFE, S., DE LEPELEIRE, J., VAN HOUT, H., KENNY,G., LEWIS, A., VERNOOIJ-DASSEN, M. & THE DIADEMGROUP (2005) Understanding obstacles to the recognitionof and response to dementia in different European countries:a modified focus group approach using multinational, multi-disciplinary expert groups. Aging and Mental Health, 9, 1–6.
P1: IFM/OSW P2: TIXref JWBK439-Banerjee January 14, 2010 11:12 Printer Name: Yet to Come
REFERENCES 139
JANEVIC, M. R. & CONNELL, C. M. (2001) Racial, ethnic, andcultural differences in the dementia caregiving experience: recentfindings. The Gerontologist, 41, 334–347.
JEWSON, N., JEFFERS, S. & KALRA, V. (2003) ‘In our blood’:respite services, family care and Asian communities in Leicester.University of Leicester.
JHA, A., TABET, N. & ORRELL, M. (2001) To tell or not totell – comparison of older patients’ reaction to their diagnosis ofdementia and depression. International Journal of Geriatric Psy-chiatry, 16, 879–885.
JOLLEY, D., BENBOW, S. M. & GRIZZELL, M. (2006) Memoryclinics. Postgraduate Medical Journal, 82, 199–206.
KALACHE, A. (1991) Ageing is a third world problem too. Inter-national journal of Geriatric Psychiatry, 6, 617–618.
KATBAMNA, S., AHMAD, W., BHAKTA, P., BAKER, R. &PARKER, G. (2004) Do they look after their own? Informal sup-port for South Asian carers. Health and Social Care in the Com-munity, 12, 398–406.
KEADY, J. & NOLAN, M. (1995a) IMMEL 2: working to augmentcoping responses in early dementia. British Journal of Nursing, 4,377–380.
KEADY, J. & NOLAN, M. (1995b) IMMEL: assessing coping re-sponses in the early stages of dementia. British Journal of Nurs-ing, 4, 309–314.
KIEV, A. (1963) Beliefs and delusions of West Indian immigrantsto London. British Journal of Psychiatry, 109, 356–363.
KIM, J., KNIGHT, B. & LONGMIRE, C. V. F. (2006) Therole of familism in stress and coping processes among AfricanAmerican and white dementia caregivers: effects on men-tal health and physical health. Health Psychology, 26, 564–576.
KIRSCHT, J. P. (1974) The health belief model and illness behav-ior. Health Education Monographs, 2, 387–408.
KITWOOD, T. (1997) Dementia Reconsidered: The Person ComesFirst, Buckingham, Open University Press.
KLEINMAN, A. (1980) Patients and Healers in the Context ofCulture: An Exploration of the Borderland between Anthropol-ogy, Medicine and Psychiatry, California, University of Califor-nia Press
KNAPP, M., PRINCE, M., ALBANESE, E., BANERJEE, D.,DHANASIRI, S., FERNANDEZ, J., FERRI, C., MCCRONE,P., SNELL, T. & STEWART, R. (2007) Dementia UK. London,Alzheimer’s Society.
P1: IFM/OSW P2: TIXref JWBK439-Banerjee January 14, 2010 11:12 Printer Name: Yet to Come
140 REFERENCES
KNEEBONE, I. I. & MARTIN, P. R. (2003) Coping and caregiversof people with dementia. British Journal of Health Psychology, 8,1–17.
KNIGHT, B. G., SILVERSTEIN, M., MCCULLUM, T. J. & FOX,L. S. (2000) A sociocultural and coping model for mental healthoutcomes among African American caregivers in southern Cal-ifornia. Journal of Gerontology: Psychological Sciences, 55B,142–150.
KRAMER, B. J. (1997) Gain in the caregiving experience: whereare we? What next? The Gerontologist, 37, 218–232.
LAMBARDO, S. (2003) Caregiving role satisfaction: my mother’sfinal gift. Home Healthcare Nurse, 21, 68.
LANDRINE, H. & KLONOFF, E. A. (1992) Culture and health-related schemas: a review and proposal for interdisciplinary inte-gration. Health Psychology, 11, 267–276.
LAUNGANI, P. (1999) Understanding mental illness in India andBritain. International Journal of Health Promotion and Educa-tion, 37, 144–157.
LAWRENCE, V., BANERJEE, S., BHUGRA, D., SANGHA, K.,TURNER, S. & MURRAY, J. (2006a) Coping with depressionin later life: a qualitative study of help-seeking in three ethnicgroups. Psychological Medicine, 36, 1375–1383.
LAWRENCE, V., MURRAY, J., BANERJEE, S., TURNER,S., SANGHA, K., BYNG, R., BHUGRA, D., HUXLEY, P.,TYLEE, A. & MACDONALD, A. (2006b) Concepts and cau-sation of depression: a cross-cultural study of the beliefs of olderadults. The Gerontologist, 46, 23–32.
LAWTON, M. P., BRODY, E. M. & SAPERSTEIN, A. R.(1989a) A controlled study of respite services for caregivers ofAlzheimer’s patients. The Gerontologist, 29, 8–16.
LAWTON, M. P., KLEBAN, M. H., MOSS, M., ROVINE, M. &GLICKSMAN, A. (1989b) Measuring caregiving appraisal. Jour-nal of Gerontology: Psychological Sciences, 44, 61–71.
LAWTON, M. P., MOSS, M., KLEBAN, M. H., GLICKSMAN,A. & ROVINE, M. (1991) A two-factor model of caregivingappraisal. Journal of Gerontology: Psychological Sciences, 46,61–71.
LAWTON, M. P., RAJAGOPAL, D., BRODY, E. & KLEBAN,M. H. (1992) The dynamics of caregiving for a demented elderamong black and white families. Journal of Gerontology: SocialSciences, 27, 156–164.
LAZARUS, R. S. (1966) Psychological Stress and the Coping Pro-cess, New York, McGraw-Hill.
P1: IFM/OSW P2: TIXref JWBK439-Banerjee January 14, 2010 11:12 Printer Name: Yet to Come
REFERENCES 141
LAZARUS, R. S. (1993) Coping theory and research: past, presentand future. Psychosomatic Medicine, 55, 234–247.
LAZARUS, R. S. & FOLKMAN, S. (1984) Stress, Appraisal andCoping, New York, Springer.
LEVENTHAL, E., A. & CROUCH, M. (1997) Are there differ-ences in perceptions of illness across the lifespan? IN PETRIE,K. J. & WEINMAN, J. (Eds.) Perceptions of Health and Illnes,Amsterdam, Harwood Academic.
LEVENTHAL, H., BRISSETTE, I. & LEVENTHAL, E. A.(2003) The common-sense model of self-regulation of health andillness. IN CAMERON, L. D. & LEVENTHAL, H. (Eds.) TheSelf-Regulation of Health and Illness Behaviour, London, Rout-ledge.
LEVENTHAL, H., NERENZ, D. & STRAUS, A. (1982) Self-regulation and the mechanisms for symptom appraisal. INMECHANIC, D. (Ed.) Symptoms, illness behavior, and help-seeking, New Jersey, Rutgers University Press.
LEVENTHAL, H., NERENZ, D. R. & STEELE, D. J. (1984) Ill-ness representations and coping with health threats. IN BAUM,A., TAYLOR, S. E. & SINGER, J. E. (Eds.) Handbook of Psy-chology and Health, New Jersey, Lawrence Erlbaum Associates.
LEVKOFF, S., LEVY, R. & FLYNN WEITZMAN, P. (1999) Therole of religion and ethnicity in the help seeking of family care-givers of elders with Alzheimer’s disease and related disorders.Journal of Cross-Cultural Gerontology, 14, 335–356.
LEWIS, L. E. & MEREDITH, B. (1988) Daughters who Care:Daughters Caring for Mothers at Home, London, Routledge.
LINDESAY, J., JAGGER, C., MLYNIK-SZMID, A.,SINORWALA, A., PEET, S. & MOLEDINA, F. (1997)The mini-mental state examination (MMSE) in the elderly immi-grant Gujarati population in the United Kingdom. InternationalJournal of Geriatric Psychiatry, 12, 1155–1167.
LINDSTROM, H. A., SMYTH, K. A., SAMI, S. A., DAWSON,N. V., PATTERSON, M. B., BOHINC, J. H., POST, S. G.,BARBER, M. J., OLLERTON, S., SINGER, M. & WHITE-HOUSE, P. J. (2006) Medication use to treat memory loss indementia. Perspectives of persons with dementia and their care-givers. Dementia, 5, 27–50.
LITTLEWOOD, R. (1988) From vice to madness: the semantics ofnaturalistic and personalistic understandings in Trinidadian localmedicine. Social Science & Medicine, 27, 129–148.
LIVINGSTON, G., LEAVEY, G., KITCHEN, G., MANELA, M.,SEMBHI, S. & KATONA, C. (2001) Mental health of migrant
P1: IFM/OSW P2: TIXref JWBK439-Banerjee January 14, 2010 11:12 Printer Name: Yet to Come
142 REFERENCES
elders – the Islington study. British Journal of Psychiatry, 179,361–366.
LONG FOLEY, K., TUNG, H. & MUTRAN, E. J. (2002) Self-gainand self-loss among African American and White caregivers.Journal of Gerontology: Social Sciences, 57B, 14–22.
LOWDELL, C., EVANDROU, M., BARDSLEY, M., MORGAN,D. & SOLJAK, M. (2000) Health of Ethnic Minority Elders inLondon: Respecting Diversity. The Health of Londoners Project.London, East London & The City Health Authority.
LOWIN, A., KNAPP, M. & MCCRONE, P. (2001) Alzheimer’sdisease in the UK; comparative evidence on cost of illness andvolume of health services research funding. International Journalof Geriatric Psychiatry, 16, 1143–1148.
LYONS, K. S., ZARIT, S. H., SAYER, A. G. & WHITLACH, C.J. (2002) Caregiving as a dyadic process: perspectives from care-giver and receiver. Journal of Gerontology: Psychological Sci-ences, 57B, 195–204.
MACKENZIE, J., BARTLETT, R. & DOWNS, M. (2006) Mov-ing towards culturally competent dementia care: have we beenbarking up the wrong tree? Reviews in Clinical Gerontology, 15,39–46.
MACQUARRIE, C. (2005) Experiences in early stage Alzheimer’sdisease: understanding the paradox of acceptance and denial. Ag-ing and Mental Health, 9, 430–441.
MARWAHA, S. & LIVINGSTON, G. (2002) Stigma, racism, andchoice: Why do depressed ethnic elders avoid psychiatrists? Jour-nal of Affective Disorders, 72, 257–265.
MASLOW, K. (1990) Formal long term care services and settings.IN MARC, N. (Ed.) Dementia Care: Patient, Family and Com-munity, Baltimore, Johns Hopkins University Press.
MCCRACKEN, C. F., BONEHAM, M. A., COPELAND, J. R.M., WILLIAMS, K. E., WILSON, K., SCOTT, A., MCKIBBIN,P. & CLEAVE, N. (1997) Prevalence of dementia and depres-sion among elderly people in black and ethnic minorities. BritishJournal of Psychiatry, 171, 269–273.
MCKINLAY, J. (1973) Social networks, lay consultation and help-seeking behaviour. Social Forces, 51, 275–291.
MECHANIC, D. (1968) Medical Sociology, New York, Free Press.MECHANIC, D. (1982) Symptoms, Illness Behaviour, and Help
Seeking, New York, Prodist.MILLER, B., CAMPBELL, R. T., FARREN, C. J., KAUFMAN,
J. E. & DAVIS, L. (1995) Race, control, mastery, and caregiverdistress. Journal of Gerontology: Social Services, 50B, 374–382.
P1: IFM/OSW P2: TIXref JWBK439-Banerjee January 14, 2010 11:12 Printer Name: Yet to Come
REFERENCES 143
MILLER, B. & POWELL LAWTON, M. (1997) Positive aspectsof caregiving. The Gerontologist, 37, 216–217.
MILNE, A. J. (2002) Ethnic minority populations and dementia.Research and Policy Briefings from the Mental Health Founda-tion. London.
MILNE, A. & CHRYSSANTHOPOULOU, C. (2005) Dementiacare-giving in Black and Asian populations: reviewing and refin-ing the research agenda. Journal of Community & Applied SocialPsychology, 15.
MODOOD, T., BEISHON, S. & VIRDEE, S. (1994) ChangingEthnic Identities, London Policy Studies Institute.
MORGAN, C., MALLETT, R., HUTCHINSON, G. & LEFF, J.(2004) Negative pathways to psychiatric care and ethnicity: thebridge between social science and psychiatry. Social Science &Medicine, 58, 739–752.
MORIARTY, J. (1999) Use of community and long-term care bypeople with dementia in the UK: a review of some issues in ser-vice provision and carer and user preferences. Aging and MentalHealth, 3, 311–319.
MOTENKO, A. (1989) The frustrations, gratifications, and well-being of dementia caregivers. The Gerontologist, 29, 166–172.
MURRAY, J. & LIVINGSTON, G. (1998) A qualitative study ofadjustment to caring for an older spouse with psychiatric illness.Ageing & Society, 18, 659–671.
MURRAY, J., SCHNEIDER, J., BANERJEE, S. & MANN, A. H.(1999) Eurocare: a cross-national study of co-resident spouse car-ers for people with Alzheimer’s disease: II – a qualitative analysisof the experience of caregiving. International Journal of GeriatricPsychiatry, 14, 662–667.
MURPHY, E., & BANERJEE, S. (1993) The organisation ofold-age psychiatry services. Reviews in Clinical Gerontology, 3,367–378.
NATIONAL AUDIT OFFICE (2007) Improving services and sup-port for people with dementia. London, National Audit Office.
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EX-CELLENCE & SOCIAL CARE INSTITUTE OF EXCEL-LENCE (2006) Dementia: supporting people with dementia andtheir carers in health and social care. London, National Collabo-rating Centre for Mental Health.
NELSON, T., FERNANDEZ, J., LIVINGSTON, G., KNAPP, M.& KATONA, C. (2004) Does diagnosis determine delivery? TheIslington study of older people’s needs and health care costs. Psy-chological Medicine, 34, 147–155.
P1: IFM/OSW P2: TIXref JWBK439-Banerjee January 14, 2010 11:12 Printer Name: Yet to Come
144 REFERENCES
NOLAN, M. (1995) Developing a typology of family care: implica-tions for nurses and other service providers. Journal of AdvancedNursing, 21, 256–265.
NOLAN, M., RYAN, T., ENDERBY, P. & REID, D. (2002) To-wards a more inclusive vision of dementia care practice and re-search. Dementia, 1, 193–211.
NUTTALL, S, R., BLACKWOOD, R, J, L., BUSSELL, B, M, H.,CLIFF, J, P., CORNALL, M, J., COWLEY, A., GATENBY, P,L. & WEBBER, J, M. (1994) Financing long-term care in GreatBritain. Journal of the Institute of Actuaries, 121, 1–68.
OFFICE FOR NATIONAL STATISTICS (2003) UK Census 2001,London, The Stationary Office.
OFFICE OF POPULATION CENSUSES AND SURVEYS(1993) 1991 Census: Ethnic Group and Country of Birth GreatBritain. London, Office of Population Censuses and Surveys.
OFFICE OF PUBLIC SECTOR INFORMATION (2000) Carersand Disabled Children Act. Office of Public Sector Information.
OPIE, A. (1994) The instability of the caring body: gender and care-givers of confused older people. Qualitative Health Research, 4,31.
ORONA, C. (1990) Temporality and identity loss due toAlzheimer’s disease. Social Science & Medicine, 30, 1247–1256.
PATEL, N. & MIRZA, N. (2000) Care for ethnic minorities:the professional’s view. Journal of Dementia Care, Jan/Feb, 27–28.
PATEL, N., MIZRA, N., LINDBLAD, P., AMASTRUP, K. &SAMOLI, O. (1998) Dementia and Minority Ethnic Older Peo-ple, Lyme Regis, Russell House Publishing Ltd.
PATEL, V. & PRINCE, M. (2001) Ageing and mental health ina developing country: who cares? Qualitative studies from Goa,India. Psychological Medicine, 31, 29–38.
PATRICK, D, L., STARKS, H, E., CAIN, K, C., UHLMANN, R.,PEARLMAN, R. (1994) Measuring preferences for health statesworse than death. Medical Decision Making. 14, 9–18.
PEACH, C. (1988) Trends in levels of Caribbean segrega-tion, Great Britain, 1961–91. IN CHAMBERLAIN, M. (Ed.)Caribbean Migration: Globalised Identities, London, Routledge.
PEACH, C. (1996) Ethnicity in the 1991 Census, Volume 2: TheEthnic Minority Populations of Great Britain Office for NationalStatistics, London, The Stationary Office.
PEACH, C. (1999) London and New York: contrasts in British andAmerican models of segregation. International Journal of Popu-lation Geography, 5, 319–351.
P1: IFM/OSW P2: TIXref JWBK439-Banerjee January 14, 2010 11:12 Printer Name: Yet to Come
REFERENCES 145
PEARCE, A., CLARE, L. & PISTRANG, N. (2002) Managingsense of self: coping in the early stages of Alzheimer’s disease.Dementia, 1, 173–192.
PEARLIN, L. I., HARRINGTON, C., POWELL, J. L., MONT-GOMERY, R. J. V. & ZARIT, S. H. (2001) An overview of thesocial and behavioural consequences of Alzheimer’s disease. Ag-ing and Mental Health, 5, 3–6.
PEARLIN, L. I., MULLAN, J. T., SEMPLE, S. J. & SKAFF, M.M. (1990a) Caregiving and the stress process: an overview of con-cepts and their measures. The Gerontologist, 30, 583–594.
PEARLIN, L. I., TURNER, H. & SEMPLE, S. (1990b) Cop-ing and the mediation of caregiver stress. IN LIGHT, E. &LEBOWITZ, B. (Eds.) Alzheimer’s Disease Treatment and Fam-ily Stress, Rockville, Hemisphere Publishing Corporation.
PEDERSON, D. & BARUFFATI, V. (1985) Health and tradi-tional medicine cultures in Latin America and the Caribbean.Social Science & Medicine, 21, 5–12.
PELUSO, E. T. P. & BLAY, S. L. (2004) Community perceptionof mental disorders: a systematic review of Latin American andCaribbean studies. Social Psychiatry and Psychiatric Epidemiol-ogy, 39, 955–61.
PESCOSOLIDO, B. A. (1992) Beyond rational choice: the socialdynamics of how people seek help. The American Journal ofSociology, 97, 1096–1138.
PHILPOT, M. & BANERJEE. S. (1997) Mental health services forolder people in London. IN JOHNSON, S., RAMSAY, R., ÞICROFT, G. (Ed.) The Report for the King’s FundLondon Commission, London: King’s Fund Publishing.
PHINNEY, A. (2002) Fluctuating awareness and the breakdown ofthe illness narrative in dementia. Dementia, 1, 329–244.
PICKARD, L., WITTENBERG, R., COMAS-HERRERA, A.,DAVIES, B. & DARTON, R. (2000) Relying on informal carein the new century? Informal care for elderly people in Englandto 2031. Ageing and Sociey, 20, 745–772.
PINQUART, M. & SORENSEN, S. (2003) Differences betweencaregivers and noncaregivers in psychological health and physicalhealth: a meta-analysis. Psychology and Aging, 18, 250–267.
PINQUART, M. & SORENSEN, S. (2006) Gender differencesin caregiver stressors, social resources, and health: an updatedmeta-analysis. Journal of Gerontology: Social Sciences, 61B,33–45.
POLLITT, P. (1996) Dementia in old age: an anthropological per-spective. Psychological Medicine, 26, 1061–1074.
P1: IFM/OSW P2: TIXref JWBK439-Banerjee January 14, 2010 11:12 Printer Name: Yet to Come
146 REFERENCES
PRATT, R. & WILKINSON, H. (2001) ‘Tell me the truth’: the ef-fect of being told the diagnosis of dementia from the perspectiveof the person with dementia. London, The Mental Health Foun-dation.
PRESTON, L., MARSHALL, A. & BUCKS, R. (2007) Investigat-ing the ways that older people cope with dementia: a qualitativestudy. Aging and Mental Health, 11, 131–143.
PRINCE, M., LIVINGSTON, G. & KATONA, C. (2007) Mentalhealth care for the elderly in low-income countries: a health sys-tems approach. World Psychiatry, 6, 5–13.
PRUCHNO, R. & KLEBAN, M. H. (1993) Caring for an institu-tionalized parent: the role of coping strategies. Psychology andAging, 8, 18–25.
PUBLIC ACCOUNTS COMMITTEE (2008) Improving servicesand support for people with dementia, London, TSO.
PYKE, K. D. & BENGSTON, V. L. (1996) Caring more or less: in-dividualistic and collectivist systems of family eldercare. Journalof Marriage and the Family, 58, 379–392.
QURESHI, H. & WALKER, A. (1989) The Caring Relationship.Elderly People and Their Families, Philadelphia, Temple Univer-sity Press.
RAIT, G. & BURNS, A. (1997) Appreciating background and cul-ture: the South Asian elderly and mental health. InternationalJournal of Geriatric Psychiatry, 12, 973–977.
REID, D., RYAN, T. & ENDERBY, P. (2001) What does it meanto listen to someone with dementia? Disability & Society, 16,377–392.
ROBERTS, J. S. & CONNELL, C. M. (2000) Illness representa-tions among first-degree relatives of people with Alzheimer dis-ease. Alzheimer Disease and Associated Disorders, 14, 129–136.
ROBINSON, V. & CAREY, M. (2000) Peopling skilled interna-tional migration: Indian doctors in the UK. International Migra-tion, 38, 89–101.
ROMERO, B. & WENZ, M. (2001) Self-maintenance therapyin Alzheimer’s disease. Neuropsychology Rehabilitation, 11,333–355.
ROSE, E. J. B. (1969) Colour and Citizenship: A Report on BritishRace Relations, London, Oxford University Press.
ROSENSTOCK, I. M. (1974) The historical origins of the healthbelief model. Health Education Monographs, 2, 328–335.
ROTH, D. L. (2005) Changes in social support as mediators ofthe impact of a psychosocial intervention for spouse caregiversof persons with Alzheimer’s disease. Psychology and Aging, 20,634–644.
P1: IFM/OSW P2: TIXref JWBK439-Banerjee January 14, 2010 11:12 Printer Name: Yet to Come
REFERENCES 147
ROYAL COLLEGE OF PSYCHIATRISTS (1990) PsychiatricPractice and Training in a British Multi-Ethnic Society. London,Royal College of Psychiatrists.
ROYAL COLLEGE OF PSYHCIATRISTS & BRITISH GERI-ATRIC SOCIETY (1979) Guidelines for collaboration betweengeriatric physicians and psychiatrists in the care of the el-derly. Bulletin of the Royal College of Psychiatrists, 1979, 168–169.
ROZARIO, P. A. & DERIENZIS, D. (2009) Familism beliefs andpsychological distress among African American women care-givers. The Gerontologist, 48, 772–780.
SABAT, S. R. (1998) Voices of Alzheimer’s disease sufferers: a callfor treatment based on personhood. Journal of Clinical Ethics, 9,35–48.
SABAT, S. R. (2002) Epistemological issues in the study of insightin people with Alzheimer’s disease. Dementia, 1, 279–293.
SABAT, S. R. & HARRE, R. (1992) The construction and decon-struction of the self in Alzheimer’s disease. Ageing & Society, 12,443–461.
SCHOLEY, K. A. & WOODS, R. T. (2003) A series of briefcognitive therapy interventions with people experiencing bothdementia and depression: a description of techniques and com-mon themes. Clinical Psychology and Psychotherapy, 10, 175–185.
SEABROOKE, V. & MILNE, A. (2004) Culture and care in de-mentia. A study of the Asian community in north west Kent.Kent, Alzheimer’s and Dementia Support Services.
SEGALL, M. H., LONNER, W. J. & BERRY, J. W. (1998) Cross-cultural psychology as a scholarly discipline. American Psycholo-gist, 53, 1101–1110.
SHAH, A., OOMMEN, G. & WUNTAKAL, B. (2005) Cross-cultural aspects of dementia. Psychiatry, 4, 103–106.
SHAJI, K. S., SMITHA, K., PRAVEEN LAL, K. & PRINCE, M.(2003) Caregivers of people with Alzheimer’s disease: a qualita-tive study from the Indian 10/66 Dementia Research Network.International Journal of Geriatric Psychiatry, 18, 1–6.
SHAJI, S., PROMODU, K., ABRAHAM, T., ROY, J. & VERGH-ESE, A. (1996) An epidemiological study of dementia in a ruralcommunity in Kerala, India. British Journal of Psychiatry, 168,745–749.
SIN, C. (2006) Expectations of support among White British andAsian-Indian older people in Britain: the interdependence of for-mal and informal spheres. Health and Social Care in the Commu-nity, 14, 215–224.
P1: IFM/OSW P2: TIXref JWBK439-Banerjee January 14, 2010 11:12 Printer Name: Yet to Come
148 REFERENCES
SINGH-BHOPAL, R. (1986) The inter-relationship of folk, tra-ditional and Western medicine within an Asian community inBritain. Social Science & Medicine, 22, 99–105.
SMITH, S. C., LAMPING, D. L., BANERJEE, S., HARWOOD,R., FOLEY, B., SMITH, S., COOK, J. C., MURRAY, J.,PRINCE, M., LEVIN, E., MANN, A. & KNAPP, M. (2005)Measurement of health-related quality of life for people with de-mentia: development of a new instrument (DEMQOL) and anevaluation of current methodology. Health Technology Assess-ment 9.
SNEEUW, K. C. A., SPANGERS, M. A. G. & AARONSON, N.K. (2002) The role of health care providers and significant othersin evaluating the quality of life of patients with chronic disease.Journal of Clinical Epidemiology, 55, 1130–1143.
SOCIAL SERVICES DIRECTORATE (1998) ‘They look aftertheir own, don’t they?’ Inspection of community care services forblack and ethnic minority older people. London, Department ofHealth.
SOCIAL SERVICES DIRECTORATE (2001) Improving olderpeople’s services. Inspection of social care services for older peo-ple. London, Department of Health.
STEEMAN, E., DIERCKX DE CASTERLE, B., GODDERIS, J.& GRYPDONCK, M. (2006) Living with early stage of demen-tia: a review of qualitative studies. Journal of Advanced Nursing,54, 722–738.
STERRITT, P. F. & POKORNY, M. E. (1998) African Americancaregiving for a relative with Alzheimer’s disease. Geriatric Nurs-ing, 19, 127–134.
STRAIN, L. A. & BLANDFORD, A. A. (2002) Community-basedservices for the taking but few takers: reasons for nonuse. Journalof Applied Gerontology, 21, 220.
SULS, J. & FLETCHER, B. (1985) The relative efficacy ofavoidant and nonavoidant coping strategies: a meta-analysis.Health Psychology, 4, 249–288.
SURR, C. A. (2006) Preservation of self in people with dementialiving in residential care: a socio-biographical approach. SocialScience & Medicine, 62, 1720–1730.
TOSELAND, R., MCCALLION, P., GERBER, T., DAWSON,C., GIERYIC, S. & GUILAMO-RAMOS, V. (1999) Use ofhealth and human services by community-residing people withdementia. Social Work, 44, 535–548.
TOTH-COHEN, S. (2004) Factors influencing appraisal of up-set in Black caregivers of persons with Alzheimer disease and
P1: IFM/OSW P2: TIXref JWBK439-Banerjee January 14, 2010 11:12 Printer Name: Yet to Come
REFERENCES 149
related dementia. Alzheimer Disease and Associated Disorders,18, 247–255.
TOWNSEND, J. & GODFREY, M. (2001) Asian experiences ofcare-giving for older relatives with dementia: an exploration ofthe barriers to uptake of support services. Leeds, Nuffield Insti-tute for Health.
TRIANDIS, H. C. (1995) Individualism and Collectivism, Col-orado, West View Press.
TURNER, S., ILIFFE, S., DOWNS, M., WILCOCK, J., BRYANS,M., LEVIN, E., KEADY, J. & O’CARROL, R. (2004) Generalpractitioners’ knowledge, confidence and attitudes in the diag-nosis and management of dementia. Age and Ageing, 33, 461–467.
VAN DIJKHUIZEN, M., CLARE, L. & PEARCE, A. (2006)Striving for connection. Appraisal and coping among womenwith early stage Alzheimer’s disease. Dementia, 5, 73–94.
VAN HOUT, H., VERNOOIJ-DASSEN, M., BAKKER, K.,BLOM, M. & GROL, R. (2000) General practitioners on demen-tia: tasks, practices and obstacles. Patient Education and Coun-selling, 39, 219–225.
WALDEMAR, G., KIEU, T., PHUNG, T., BURNS, A.,GEORGES, J., RONHOLT HANSEN, F., MARKING, C.,OLDE RIKKERT, M., SELMES, J., STOPPE, G. & SARTO-RIUS, N. (2007) Access to diagnostic evaluation and treatmentfor dementia in Europe. International Journal of Geriatric Psy-chiatry, 22, 47–54.
WALLSTON, B. S. & WALLSTON, K. A. (1984) Social psy-chological models of health behaviour: an examination and in-vestigation. IN BAUM, A. (Ed.) Handbook of Psychology andHealth. Volume IV: Social Psychological Aspects of Health, Cam-bridge, Cambridge University Press.
WATTIS, J, P., WATTIS, L. & ARIE, T. (1981) Psychogeriatrics:a national survey of a new branch of psychiatry. British MedicalJournal, 283, 1529–1533.
WERTEIMER, J. (1997) Psychiatry of the elderly: a consen-sus statement. International Journal of Geriatric Psychiatry, 12,432–435.
WILD, S. & MCKEIGUE, P. (1997) Cross-sectional analysis ofmortality by country of birth in England and Wales, 1970–1972.British Medical Journal, 214, 705–710.
WOOD, J. B. & PARHAM, I. A. (1990) Coping with perceivedburden: ethnic and cultural issues in Alzheimer’s family caregiv-ing. Journal of Applied Gerontology, 9, 325–329.
P1: IFM/OSW P2: TIXref JWBK439-Banerjee January 14, 2010 11:12 Printer Name: Yet to Come
150 REFERENCES
WOOD, J. B. & WAN, T. T. H. (1993) Ethnicity and minority issuesin family caregiving to rural Black elders. IN BARRESI, C. M. &STULL, D. E. (Eds.) Ethnic Elderly and Long-Term Care, NewYork, Springer.
WOODS, R. T. (1997) Talking point: Kitwood’s ‘The experience ofdementia’. Aging and Mental Health, 1997, 11–12.
WOODS, R. T. (1999) The person in dementia care. Generations,Fall, 35–39.
WOODS, R. T. & PRATT, R. (2005) Awareness in dementia: eth-ical and legal issues in relation to people with dementia. Agingand Mental Health, 9, 423–429.
WOODS, R. T., SPECTOR, A., JONES, C., ORRELL, M.& DAVIES, S. (2005) Reminiscence therapy for dementia.Cochrane Database of Systematic Reviews, 2.
WORLD HEALTH ORGANIZATION (1992) The ICD-10 Clas-sification of Mental and Behavioural Disorders: Clinical Descrip-tions and Diagnostic Guidelines, Geneva, World Heath Organi-zation.
WYKLE, M. & SEAGALL, M. (1991) A comparison of black andwhite family caregivers experience with dementia. Journal of theNational Black Nurses Association, 5, 29–41.
YEO, G. (2006) Prevalence of dementia among different ethnicpopulations. IN YEO, G. & GALLAGHER-THOMPSON, D.(Eds.) Ethnicity and the Dementias, Second Edition, New York,Routledge.
YEO, G. & GALLAGHER-THOMPSON, D. (1997) Ethnicity &the Dementias, Washington DC, Taylor and Francis.
YEO, G. & GALLAGHER-THOMPSON, D. (2006) Ethnicity andthe Dementias, Second Edition, New York, Routledge.
YOUN, G., KNIGHT, B. G., JEONG, H. & BENTON, D. (1999)Differences in familism values and caregiving outcomes amongKorean, Korean American, and white American dementia care-givers. Psychology and Aging, 14, 355–364.
YOUNG, H. M., MCCORMICK, W. C. & VITALIANO, P. (2002)Attitudes toward community-based services among JapaneseAmerican families. The Gerontologist, 42, 814–825.
YOUNG, J. T. (2004) Illness behaviour: a selective review and syn-thesis. Sociology of Health & Illness, 26, 1–31.
ZARIT, J. M. (1989) Issues and directions in family inter-vention research. IN LIGHT, E. & LEBOWITZ, B. (Eds.)Alzheimer’s disease treatment and family stress: Directions forresearch, Rockville, MD, Department of Health and HumanServices.

P1: IFM/OSW P2: TIXref JWBK439-Banerjee January 14, 2010 11:12 Printer Name: Yet to Come
REFERENCES 151
ZARIT, S. H. & FEMIA, E. E. (2008) A future for family careand dementia intervention research? Challenges and strategies.Aging and Mental Health, 12, 5–13.
ZARIT, S. H., GAUGER, J. E. & JARROTT, S. E. (1999) Use-ful services for families: research findings and directions. Interna-tional Journal of Geriatric Psychiatry, 14, 161–181.
ZARIT, S. H., REEVER, K. E. & BACH-PETERSON, J. (1980)Relatives of impaired elderly: correlates of feelings of burden.The Gerontologist, 20, 649–655.

P1: IFM/OSW P2: TIXref JWBK439-Banerjee January 14, 2010 11:12 Printer Name: Yet to Come
152
P1: OTE/OTE/SPH P2: OTEInd JWBK439-Banerjee January 15, 2010 19:47 Printer Name: Yet to Come
INDEX
AD see Alzheimer’s Diseaseadaptive strategies 52–5Advance Care Planning 100–1African American populations
59, 63–9Age Concern 117, 121age discrimination in service
commissioning 110–11,113, 116–17, 120
All-Party ParliamentaryGroup on Dementia 124
Alzheimer’s Disease (AD)6–7
clinical features 3–4culture and ethnicity 25family carers 62health beliefs 30incidence and prevalence 6presentation and aetiology
6–7qualitative research 75social perspective 40–1, 42terminology and
understandings 2–3Alzheimer’s Society, The 11,
15, 123–4amyloid plaques 3–4anthropological perspective
88–9antipsychotics 8–9, 124–5
APOE gene 7approach coping 52Audit Commission 13–14avoidance coping 52Ayurvedic medicine 34–5
biographical disruption 87–8,101–3
bipolar disorders 2black Caribbean populations
21–6family carers 59–60, 65–71,
76–7, 81–6health beliefs 33–4policy framework 91–2, 99,
101, 103quality of life 76–80, 84
care giverscommunicating importance
of wellbeing 98culture and ethnicity
39–41, 45–6dementia care in the UK
11–12, 15, 18extended family support
106–7identifying burden 98–9maintaining non-care giving
roles 107
Managing Dementia in a Multicultural Society Sube Banerjee and Vanessa LawrenceC© 2010 John Wiley & Sons, Ltd
153
P1: OTE/OTE/SPH P2: OTEInd JWBK439-Banerjee January 15, 2010 19:47 Printer Name: Yet to Come
154 INDEX
care givers (Cont.)policy framework 92–5,
97–9, 101promoting role 105–6psychosocial interventions
105quality of life 47–8reinforcing valued roles 104repositioning 105–7service use 46Stress Process Model 45–6support for service access
98–9see also family carers
care giving ideology 74, 85–6care homes 122–5Care Services Improvement
Partnership (CSIP) 14,38, 114, 118
Carer’s Allowance 106Carers and Disabled Children
Act 86–7cell death 2–3cholinesterase inhibitors 4Community Mental Health
Teams 74–5complementary therapies
34–5, 70coping strategies
care givers 93family carers 61–3, 66quality of life 52–5, 77
Crossroads carers 104CSIP see Care Services
Improvement Partnershipculture and ethnicity 19–26
anthropological perspective88–9
appropriateness of services67–8
attitudes/beliefs aboutformal support 69–71
black/minority ethnicorganisations 38–42
care givers 39–41, 45–6definitions 20–1dementia care 11demographics in the UK
24–5epidemiology 19–20, 25–6family carers 26, 57, 59–60,
63–71health beliefs 31–5policy framework 37–8,
91–2, 93–5, 97–8, 99population structures 24–5qualitative research 73–4,
76–86quality of life 49race 19, 20–1service use 42–3, 46Stress Process Model 64–7understanding of dementia
68–9voluntary organisations
38–41
data collection 74–6delirium 2Dementia: Supporting people
with dementia and theircarers in health and socialcare 14–15
dementiaaetiology 6clinical presentation 10historical development of
terms 2ICD-10 criteria and stages
5
P1: OTE/OTE/SPH P2: OTEInd JWBK439-Banerjee January 15, 2010 19:47 Printer Name: Yet to Come
INDEX 155
incidence and prevalence 6misconceptions 1terminology and
understandings 2–4dementia care 109–27
age discrimination in servicecommissioning110–11, 113, 116–17,120
appropriateness of services67–8
current state in the UK11–18
demographics 111–12ethnicity 11in-patient care 125–7incidence and prevalence
11liaison services in general
hospitals 121–5multi-functional community
teams 120–1National Dementia Strategy
17–18needs and risks of older
adults 112–13, 120,127
older adults 109–27one size fits all approach
109, 111, 120organic/functional patients
126–7policy framework 13–17,
113–21quality of life 12–13, 43–5,
55–6quality versus quantity 109specialist mental health care
110, 113, 115–16,118–19, 122–5
working age adult services117–20
see also care givers; familycarers
dementia with Lewy bodies(DLB) 6, 8–9
Dementia UK 11, 15denial 53depression
dementia care for olderadults 115–16, 122,126
family carers 63, 106misconceptions 1quality of life 55
DLB see dementia with Lewybodies
emotion-focused strategies52, 55
end-stage syphilis 2–3Equality Bill 110ethnicity see culture and
ethnicityEverybody’s business:
Integrated mental healthservices for older adults14, 114
explanatory models 32–3
family carers 57–71anthropological perspective
88–9appropriateness of services
67–8attitudes/beliefs about
formal support69–71
biographical disruption87–8
P1: OTE/OTE/SPH P2: OTEInd JWBK439-Banerjee January 15, 2010 19:47 Printer Name: Yet to Come
156 INDEX
family carers (Cont.)culture and ethnicity 26,
45–6, 57, 59–60, 63–71data analysis 76data collection 74–6dementia care in the UK
11–12demographics 59–60extended family support
106–7health beliefs 30, 31–3hierarchy of care giving
58–9impact of care giving 60patterns of care giving
58–60psychosocial interventions
105qualitative research 73–7,
81–6quality of life 48reinforcing individual
biographies 102Stress Process Model 60–7theoretical outcomes 86–7
Forget me not: Mental healthservices for older people13–14
frontotemporal dementia(FTD) 6, 9–10
functional wards 126–7
general hospitals 121–5general practitioners (GPs)
dementia care for olderadults 124–5
dementia care in the UK13–14, 15
policy framework 97,99–100
health belief model (HBM)28–9, 32
health beliefs 27–35complementary therapies
34–5culture and ethnicity 31–5health belief model 28–9,
32Health Care System model
32–3illness behaviour 27–31macro/microsociological
models 28pathway to care 31–3self-regulation model 28,
29–30, 32social networks 31–3terminology and
understandings 27–8Health Care System model
32–3Healthcare Commission
110–11hierarchy of care giving 58–9Home from Home 123Hungry to be Heard 121
ICD-10 criteria and stages 5illness behaviour 27–31Improving services and
support for people withdementia 12, 16
in-patient care 125–7
late-onset dementia 3–4Lewy body dementia (LBD) 6,
8–9liaison services in general
hospitals 121–5life review 104
P1: OTE/OTE/SPH P2: OTEInd JWBK439-Banerjee January 15, 2010 19:47 Printer Name: Yet to Come
INDEX 157
macrosociological models 28malignant social psychology
48, 50mania 2, 115memory aids 53Mental Illness in the
Community 30–1microsociological models 28minimisation strategies 54mixed dementia 6multi-functional community
teams 120–1
National Audit Office (NAO)12–13, 15–16, 121
National Dementia Strategy17–18
dementia care for olderadults 115–17, 120–1,123–4
public awareness ofdementia 95
public awareness of servicesand support 97–8
shared understanding ofdementia 96
support for service access99
vascular dementia 8National Institute of Clinical
Excellence (NICE) 12,14–15, 122
National Service Frameworkfor Older People 14, 38,111–14
neurofibrilary tangles3–4
NICE see National Institute ofClinical Excellence
normalisation strategies 54
Obeah 34objective primary stressors
61–3Older people’s mental health
services: a national study110–11
organic wards 126–7outreach workers 96
PAC see Public AccountsCommittee
Parkinsonism 8Parkinson’s disease dementia
(PDD) 6Parliamentary Accounts
Committee 124pathway to care 31–3PDD see Parkinson’s disease
dementiaperson-centred care model
102personhood 44, 48–9Pick’s disease 6, 9–10policy framework 13–17,
91–107balancing constancy with
change 105care givers 92–5, 97–9, 101,
105–7communicating importance
of wellbeing 98culture and ethnicity 37–8,
91–2, 93–5, 97–8, 99dementia care for older
adults 113–21discussing diagnoses
99–100discussing the future 100–1extended family support
106–7
P1: OTE/OTE/SPH P2: OTEInd JWBK439-Banerjee January 15, 2010 19:47 Printer Name: Yet to Come
158 INDEX
policy framework (Cont.)identifying burdened care
givers 98–9implications for practice
95maintaining non-care giving
roles 107promoting care giving role
105–6promoting valued elements
of life 101–5psychosocial interventions
104–5public awareness of
dementia 95–6public awareness of services
and support 96–8quality of life 91–2, 99,
101–5reinforcing individual
biographies 101–3reinforcing valued roles
103–4responding to symptoms
across ethnic groups99
shared understanding ofdementia 96
stigmatisation 95support for service access
98–9Policy Research Institute of
Ageing and Ethnicity 38problem-focused strategies
52, 55, 61psychosis 126psychosocial interventions
104–5Public Accounts Committee
(PAC) 12, 16
public awarenessof dementia 95–6of services and support
96–8
qualitative researchanthropological perspective
88–9biographical disruption
87–8data analysis 76data collection 74–6family carers 73–7, 81–6interviews 75–6quality of life 73–5, 76–80,
84results 76–86socio-demographic
characteristics 78–83theoretical outcomes
86–7quality of life 43–5, 47–56
adaptive strategies 52–5anthropological perspective
88–9attitudes towards care
55–6balancing constancy with
change 105biographical disruption
87–8, 101–3care givers 47–8coping strategies 52–5culture and ethnicity 49data analysis 76data collection 74–5dementia care in the UK
12–13, 16family carers 64personhood 48–9
P1: OTE/OTE/SPH P2: OTEInd JWBK439-Banerjee January 15, 2010 19:47 Printer Name: Yet to Come
INDEX 159
policy framework 91–2, 99,101–5
promoting valued elementsof life 101–5
psychosocial interventions104–5
qualitative research 73–5,76–80, 84
reinforcing individualbiographies 101–3
reinforcing valued roles103–4
responding to symptomsacross ethnic groups99
self-identity/sense of self47, 50–2
support for service access 99theoretical outcomes 86–7
race 19, 20–1REM sleep behaviour disorder
(RBD) 9residential care 122–5role training interventions 63
schizophrenia 1, 2, 115SCIE see Social Care Institute
of Excellenceself-identity 47, 50–2self-integrative strategies 54self-protective strategies 54self-regulation model (SRM)
28, 29–30, 32senile dementia see late-onset
dementiasense of self 47, 50–2Social Care Institute of
Excellence (SCIE) 12,14–15, 122
social constructionist model101–2
social networkscare givers 58–9, 65, 68health beliefs 31–3
social perspectiveblack/minority ethnic
organisations 38–42policy framework 37–8service use 42–3, 46voluntary organisations
38–41Social Services Directorate
38socio-cultural stress/coping
theory 63, 65south Asian populations
21–6anthropological perspective
89family carers 60, 65–71,
76–7, 81–6health beliefs 33–5policy framework 91–2,
96–7, 101, 103quality of life 76–80, 84
SRM see self-regulation modelstigmatisation
culture and ethnicity 68, 74public awareness of
dementia 95sense of self 52
Stress Process Model 45–6,60–7
stress-coping theory 52, 55,63, 65
subjective primary stressors61–3
suicidality 1syphilis 2–3
P1: OTE/OTE/SPH P2: OTEInd JWBK439-Banerjee January 15, 2010 19:47 Printer Name: Yet to Come
160 INDEX
They look after their own,don’t they? 38
valued elements of life 73–4,77, 84, 101–5
vascular dementia (VaD) 7–8culture and ethnicity
19–20, 25incidence and prevalence 6presentation and aetiology
7–8
voluntary organisations38–41
working age adult services117–20
World Health Organization(WHO) 111, 113
young-onset dementia3–4
see also Alzheimer’s disease





























