Embed Size (px)
Citation preview

The 16th Malaysian Cardiovascular Interventional
Symposium with Live Transmission
25th – 27th July 2019, Sheraton Petaling Jaya
Managing High Bleeding Risk patients with
short DAPT
DR AL FAZIR OMAR MBCHB FNHAM FAsCC FSCAI
CONSULTANT CARDIOLOGIST GLENEAGLES KUALA LUMPUR

The 16th Malaysian Cardiovascular Interventional
Symposium with Live Transmission
25th – 27th July 2019, Sheraton Petaling Jaya
I will start my last slide as my first slide
• How long would you keep his DAPT
– 1 month
– 3 months
– 12 months
– >12 months

The 16th Malaysian Cardiovascular Interventional
Symposium with Live Transmission
25th – 27th July 2019, Sheraton Petaling Jaya
• 67 yrs
• Diabetes Mellitus
• ESKD – Renal replacement therapy
• IHD

The 16th Malaysian Cardiovascular Interventional
Symposium with Live Transmission
25th – 27th July 2019, Sheraton Petaling Jaya
• IHD – PCI RCA in Jan 2013 – CTO LAD – told to manage medically unless
symptomatic as very complex and then patient defaulted
– Multiple NSTEMI since end of last year with deteriorating LV function
– Recent admission with NSTEMI 7/5/2019 with Trop T 1500

The 16th Malaysian Cardiovascular Interventional
Symposium with Live Transmission
25th – 27th July 2019, Sheraton Petaling Jaya
24th May 2019
• Admitted with drowsiness, weak, hypotensive
• Right middle zone/ lower zone pneumonia
• IV meropenem / IV insulin / IV Norad

The 16th Malaysian Cardiovascular Interventional
Symposium with Live Transmission
25th – 27th July 2019, Sheraton Petaling Jaya

The 16th Malaysian Cardiovascular Interventional
Symposium with Live Transmission
25th – 27th July 2019, Sheraton Petaling Jaya
ECG

The 16th Malaysian Cardiovascular Interventional
Symposium with Live Transmission
25th – 27th July 2019, Sheraton Petaling Jaya

The 16th Malaysian Cardiovascular Interventional
Symposium with Live Transmission
25th – 27th July 2019, Sheraton Petaling Jaya

The 16th Malaysian Cardiovascular Interventional
Symposium with Live Transmission
25th – 27th July 2019, Sheraton Petaling Jaya
• LVDD 6.4cm • LVSD 5.3cm • IVSD 1.4cm
• LV severely reduced • Simpson 23% Visual EF 30% • Mild moderate MR

The 16th Malaysian Cardiovascular Interventional
Symposium with Live Transmission
25th – 27th July 2019, Sheraton Petaling Jaya
Called by a colleague May 2019 to discuss about revascularization

The 16th Malaysian Cardiovascular Interventional
Symposium with Live Transmission
25th – 27th July 2019, Sheraton Petaling Jaya
Code Blue in HDU during dialysis

The 16th Malaysian Cardiovascular Interventional
Symposium with Live Transmission
25th – 27th July 2019, Sheraton Petaling Jaya
Discussed with hematologist Dr Jay Suria – started hydrocortisone plus Eltrombopag 50mg od for ITP

The 16th Malaysian Cardiovascular Interventional
Symposium with Live Transmission
25th – 27th July 2019, Sheraton Petaling Jaya

The 16th Malaysian Cardiovascular Interventional
Symposium with Live Transmission
25th – 27th July 2019, Sheraton Petaling Jaya

The 16th Malaysian Cardiovascular Interventional
Symposium with Live Transmission
25th – 27th July 2019, Sheraton Petaling Jaya

The 16th Malaysian Cardiovascular Interventional
Symposium with Live Transmission
25th – 27th July 2019, Sheraton Petaling Jaya
What is the plan?
• Issues:
• Low platelets
• However, becoming hemodynamically unstable
• Complex anatomy

The 16th Malaysian Cardiovascular Interventional
Symposium with Live Transmission
25th – 27th July 2019, Sheraton Petaling Jaya
• Duration of DAPT ?

DAPT Duration:
It’s all about balance
Ischemic
events Bleeding
MI Stroke ST
Death Death
GI Access ICH

Study
Year
Randomization
DAPT
duratio
n
median
Primary
Endpoin
t* Exp
Arm
Primary
Endpoin
t* Cnt
Arm
(PCI-) ASA/Clopidogrel x12m
CURE 2001 vs. 9 mo 4.5% 6.4%
(n=2658) ASA/Clopidogrel x1m
+ ASA alone x11m
TRITON ASA/Prasugrel
(n=13,608) 2007 vs. 14 mo 9.9% 12.1%
ASA/Clopidogrel
PLATO ASA/Ticacrelor
(n=18,624) 2009 vs. 9 mo 9.8% 11.7%
ASA/Clopidogrel
12-Month DAPT Duration After PCI with
Stents: What is the evidence? 3 RCTs in ACS
*CVD, MI or urgTVR in PCI-CURE; CVD, MI or stroke in TRITON and PLATO

Why Short DAPT? The high bleeding risk pt
Elderly
Rx with OAC or NOAC
Previous bleeding
Anemia or other
hematologic disorders
Coagulation disorders
Chronic Rx with
steroids or NSAIDs
Renal dysfunction
Bleeding
Risk Factors
VKA NOACs

PCI-CURE BMS (n=2658)
STOPDAPT-2 (n=3009)
SENIOR (n=1200)
SMART-CHOICE (n=2993)
REDUCE (n=1496)
RESET (n=2117)
OPTIMIZE (n=3119) IVUS-XPL (n=1400)
SECURITY (n=1399)
EXCELLENT (n=1443)
ISAR-SAFE (n=4000) I LOVE IT 2 (n=1829)
OPTIMA-C (n=1367)
SMART-DATE (n=2712)
NIPPON (n=3307)
ITALIC (n=1850)
PRODIGY (n=2014)
ARCTIC-Interruption (n=1259) DAPT BMS (n=1687)
DAPT DES (n=9961)
DES Late (n=5045)
OPTIDUAL (n=1385)
0 3 6 9 12 15 18 21 24 27 30 33 36 39 42 45 48
Months after PCI
22 RCTs of DAPT Duration after DES/BMS Timing of SAPT vs. DAPT
*1 vs. 12 mo in SIHD; 6 vs. 12 mo in ACS; **Primary endpoint at 12 mo
**
57,250 randomized pts!
*

Network Meta-analysis of Short (≤6 mo) vs. Standard
(12 mo) vs. Long (≥12 mo) Duration DAPT After DES
17 RCTs and 46,864 Pts
Yin SHL et al.
BMJ 2019;365:l2222
Short DAPT
(3-6 mo; n=13,234)
Standard DAPT
(12 mo; n=18,473)
Long DAPT
(>12 mo; n=15,157)
3-6 mo vs >12 mo
• Greater MI and ST
• Less bleeding and
non-cardiac death
• No ∆ in cardiac or
all-cause death
3-6 mo vs 12 mo
• Less bleeding
• No ∆ in MI, ST,
non-cardiac,
cardiac or all-cause
death
Odds ratio
(95% CI)
DAPT duration comparisons
>12 mo vs 3-6 mo
All cause mortality
Cardiac death Non-cardiac death
Major bleeding
Any bleeding
MI
Definite or probable stent thrombosis
Odds ratio
(95% CI)
1.18 (0.93 to 1.49)
1.28 (0.88 to 1.86)
1.63 (1.03 to 2.59)
1.78 (1.27 to 2.49)
2.13 (1.46 to 3.10)
0.63 (0.46 to 0.86)
0.57 (0.34 to 0.95)
1.08 (0.77 to 1.51)
0.88 (0.67 to 1.15) Stroke
Net adverse clinical events
12 mo vs 3-6 mo
All cause mortality
Cardiac death
Non-cardiac death
Major bleeding
Any bleeding
MI
Definite or probable stent thrombosis
Stroke
Net adverse clinical events
1.08 (0.82 to 1.43)
1.12 (0.80 to 1.58)
1.09 (0.67 to 1.77)
1.28 (0.91 to 1.80)
1.39 (1.01 to 1.92)
0.92 (0.70 to 1.21)
0.98 (0.59 to 1.64)
1.04 (0.74 to 1.47)
0.91 (0.77 to 1.08)
0.2 0.4 0.8 1 Favors longer duration
1.6 3.2 5 Favors shorter duration

Utility of Risk
Scores
Short-term
1 vs. 3 vs. 6 vs. 12 months
Long-term
1 year vs. longer
Key Factors That Affect
Optimal DAPT Duration after PCI

Risk Scores for DAPT Duration
Capodanno D et al. Lancet 2017;389:987-9
Score
Setting
Predicted
outcome(s)
Developme nt
cohort (design,
pts)
Number of
variables in the
risk score
Validation cohort(s) (c-
index, pts)
DAPT
PCI patients on
DAPT who were
event- free at 12
months
Ischemia and
bleeding
between 12
and 30 months
after PCI
RCT
(N=11,648)
Ischemia: 8
clinical and
procedural
Major
bleeding: 1
clinical
0.64 for ischemia
0.64 for bleeding
(N=8,136)
PARIS
PCI patients on
DAPT at
discharge
Ischemia and
bleeding at 24
months after PCI
Multicenter
registry
(N=4,190)
Ischemia: 6
clinical
Major
bleeding: 6
clinical
0.65 for ischemia
0.64 for bleeding
(N=8,665)
PRECIS
E-DAPT
PCI patients on
DAPT at
discharge
Bleeding at 12
months after PCI
Pooled RCTs
(N=14,963)
5 clinical
0.70 for bleeding
(N=8,595)
0.66 for bleeding
(N=6,172)

DAPT Trial: Continued Thienopyridine vs.
Placebo According to High vs. Low DAPT Score
-0,66%
0,92%
-3,02%
0,37%
-2,70%
-4,0%
-3,0%
-2,0%
-1,0%
0,0%
1,0%
2,0%
3,0%
4,0%
DAPT Score < 2
DAPT Score ≥ 2
ST or MI
NNT NNT
153 34
GUSTO mod/sev bleed Net adverse events
NNH NNH NNH NNT
109 37
P<0.001
64 272
P=0.02
1,55%
P<0.001
Ris
k D
iffere
nce (
Co
ntinued T
hie
nopyri
din
e
– P
lacebo
), 1
2-3
0M
Yeh R et al. JAMA. 2016;315:1735-1749

Yeh R et al. JAMA 2016;315:1735-1749
Pa
tie
nts
, %
7 8 9 10
30
25
20
15
10
5
0
Clinical Prediction Score
Variable Points
Age, years
≥75 -2
65-<75 -1
<65 0
Cigarette smoking 1
Diabetes mellitus 1
MI at presentation 1
Prior PCI or prior MI 1
Paclitaxel-eluting
stent
1
Stent diameter <3 mm 1
CHF or LVEF <30% 2
Vein graft stent 2
Total score range: -2 to 10
1 2 3 4 5 6
Clinical Prediction Score
-2 -1 0
DAPT Score: Multivariable prediction models unified
into a single integer score to predict clinical benefit
- N = 11,648 -

Prior
bleed
WBC
Age
CrCl
0 pt
26 pt
0 pt
15 pt
0 pt
0 pts
19 pt
25 pts
0 pt Hgb
15 pt
100 pts 0 pts
Costa F et al. Lancet 2017;389:1025-34
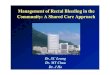
PRECISE-DAPT Score: Post-discharge
bleeding risk prediction model (n=14,963) multiple RCTs

PRECISE-DAPT Score: Post-discharge
bleeding risk prediction model (n=14,963)
Very low
Bleeding score quartiles
# o
f P
ati
en
ts
1-Y
ear B
lee
din
g R
isk
(%)
TIMI major o(rC mindienx o= 0r.7b1)leeding (C index = 0.73)
TIMI major bleeding
>4.15
3.85
2.67
1.84
1.27
0.88
0.60 0.42
0.26 0.37 0.51
0.71
0.99
1.38
>2.05
1.93
700
525
350
175
0 0 5 10 15 20
Low Mod
25 30
High
35 ≥36 0
1
2
3
4
5 Risk factors and score
derivation 0 2 4 6 8 10 12 14 16 18 20 22 24 26 28 30
Points
≤90
Creatinine clearance (mL/min)
20 0
≥12.0 11.5 11.0 10.5 ≤10.0
Hemoglobin (g/dL)
≤5 8 10 12 14 16 18 ≥20
White blood cell (x103 cells per µL)
≥50 60 70 80
Age (years)
≥100 80 60 40
Previous Bleed
No Yes
Costa F et al. Lancet 2017;389:1025-34
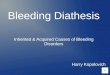
PRECISE-DAPT SCORE
Calculation
July 23, 2019, 4:24 pm
Patient ID number: Stent implanted (type): DES
Stent implanted (brand):
Total number of stent implanted: 3
Intended DAPT duration: 6
Antiplatelet agents implemented: ASA+Clopidogrel
Did score calculation change
your treatment duration strategy? Yes
Haemoglobin value 11.3 (g/dl)
Age 63 (years)
White blood cell count 9.1 (units/mcL)
Creatinine clearance 15 (ml/min)
Prior Bleeding No
PRECISE-DAPT Score 33
Risk category High
DISCLAIMER
This risk scoring tool is intended for use by clinicians, in conjunction with individual patient assessment.
We assume no responsibility for how you use or interpret the PRECISE-DAPT score or any other information provided on this website.

ACS (troponin +)
vs. Stable CAD
Key Factors That Affect
Optimal DAPT Duration after PCI

The 16th Malaysian Cardiovascular Interventional
Symposium with Live Transmission
25th – 27th July 2019, Sheraton Petaling Jaya

The 16th Malaysian Cardiovascular Interventional
Symposium with Live Transmission
25th – 27th July 2019, Sheraton Petaling Jaya

Stent Type
Key Factors That Affect
Optimal DAPT Duration after PCI

Extended Duration DAPT After DES:
Second vs. First Generation DES
Giustino G et al. JACC 2015;65:1298–310
Stent Thrombosis Trial Name
Shorter DAPT Better Longer DAPT Better
Subtotal heterogeneity; p=0.21
Odds Ratio (95% CI)
Overall
Pint = 0.008
1
Second Generation DES
DAPT
ITALIC
SECURITY
PRODIGY
EXCELLENT
OPTIMIZE
First Generation DES
DAPT
PRODIGY EXCELLENT
Subtotal heterogeneity; p=0.59
2.64 (1.17, 5.98)
7.01 (0.36, 135.86)
0.70 (0.12, 4.20)
0.25 (0.03, 2.25)
3.01 (0.31, 28.99)
1.08 (0.49, 2.37)
1.54 (0.96, 2.47)
4.44 (2.22, 8.87)
2.30 (0.70, 7.56)
7.12 (0.37, 138.77)
3.94 (2.20, 7.05)
2.33 (1.63, 3.34)

DAPT Duration According to Ds Complexity Individual patient data meta-analysis comparing short-term (3 or 6 months) vs. long-term
(≥12 mo) DAPT from 6 RCTs; 9,577 randomized pts; 1,680 (17.5%) underwent complex
PCI (3 vessels or ≥3 lesions treated or ≥3 stents implanted or total stent length >60 mm
or 2-stent bifurcation or CTO). Median 392 day FU.
Impact of DAPT duration on MACE (CD, MI or ST):
0
No. at risk
0
90 180
Days After Procedure
270 360
Non-complex PCI – Short DAPT 3938 3875 3816 3782 3511
Non-complex PCI – Long DAPT 3932 3874 3824 3794 3520
Complex PCI – Short DAPT 802 777 768 759 668
Complex PCI – Long DAPT 840 816 805 796 693
Non-complex PCI –
Short DAPT
Non-complex PCI –
Long DAPT
Complex PCI –
Short DAPT
Complex PCI –
Long DAPT
MA
CE
(%
)
2
4
6
8
10
Complex PCI
Non-complex PCI
Long
DAPT
2.8%
2.0%
Short
DAPT
4.4%
2.0%
Adjusted HR
∆ (95% CI)
-1.6% 0.56 (0.35-0.89)
+0.0% 1.01 (0.75-1.35) int
Giustino G et al. JACC 2016;68:1851-64
P =0.01

2000 patients*
Up to 90 global sites
1:1 randomization
1m
o
2mo 6 mo 1 yr 2 yr
Prospective, multicenter, single-blind
randomized trial in high bleeding-risk
patients undergoing PCI*
Resolute ONYX DES
with 1-month DAPT
(N=1000)
BioFreedom DCS with
1-month DAPT
(N=1000)
Onyx ONE Global RCT Short-Term (1-Month) DAPT
*Pts with ACS and stable angina undergoing PCI who are at increased risk of bleeding
or in whom DAPT >1 month is undesirable (criteria similar to LEADERS FREE)
Antiplatelet Therapy: DAPT for 1 month, SAPT after 1 month
Follow-up:
Primary endpoint: Composite of cardiac death, MI or stent thrombosis (def/prob) at 1 year
Major secondary endpoint (powered): Target lesion failure at 1 year
Other secondary endpoints: Acute procedural, device and lesion success; BARC bleeding;
target vessel failure; all death, MI, stroke, revascularizations, TLF and MACE at all timepoints
Principal Investigator: Stephan Windecker
Co-principal Investigators: Elvin Kedhi and Azeem Latib Study Chair: Gregg W. Stone
Sponsor: Medtronic

The 16th Malaysian Cardiovascular Interventional
Symposium with Live Transmission
25th – 27th July 2019, Sheraton Petaling Jaya

The 16th Malaysian Cardiovascular Interventional
Symposium with Live Transmission
25th – 27th July 2019, Sheraton Petaling Jaya

© AstraZeneca 2019
TWILIGHT
Ticagrelor With aspIrin or aLone In hiGH-risk patients after coronary inTervention

© AstraZeneca 2019
TWILIGHT: Study Design Overview1
cOther secondary ischemic endpoints included time to first occurrence of: (i) CV death, non-fatal MI, ischemic stroke or clinically-driven revascularization; (ii) CV death, non-fatal MI or ischemic stroke; (iii) definite or probable stent thrombosis; (iv) CV death.
1. Baber U et al. Am Heart J. 2016;182:125-134; 2. Mehran R et al. Online ahead of print. N Engl J Med. 2019.
Primary composite endpoint (ITT): Clinically relevant (BARC type 2, 3, or 5) bleeding during months 3-15 Key secondary endpoint (per protocol): Composite of all-cause death, non-fatal MI, stroke during months 3-15c
aHigh-risk patients must meet ≥1 criteria from both clinical and angiographic criteria (Inclusion criteria):
• Clinical: ≥65 years of age, female, troponin positive ACS, established vascular disease (previous MI, documented PAD or CAD/PAD revascularization),
DM treated with medications, CKD (eGFR <60 mL/min/1.73 m2 or CrCl <60 mLmin)
• Angiographic: multivessel CAD, target lesion total stent length >30 mm, thrombotic target lesion, bifurcation lesions with Medina X, 1, 1 classification requiring ≥2 stents, left main ≥50%
or proximal LAD ≥70% lesion, calcified target lesion requiring atherectomy
Open-label ticagrelor; double-blinded ASA or placebo
Ticagrelor 90 mg BID + PBO
Ticagrelor Monotherapy
(Ticagrelor 90 mg BID
+ Placebo)
Standard of care therapy at
the discretion of treating
physician
Observation period Open-label after index PCI
Ticagrelor 90 mg
BID + ASA 81-100
mg QD
Randomized if event-
freeb and adherent
(N=7119)2
Enrollment
(N=9006)2
Ticagrelor DAPT
(Ticagrelor 90 mg BID
+ ASA 81-100 mg QD)
High-riska
patients aged
≥18 years
undergoing
PCI with
≥1 DES
placement
15 mo 18 mo 3 mo
42
bEvent-free if none of the following:
• Major bleeding (BARC type 3b); ischemic event after PCI (eg, non-fatal MI, definite or probable stent thrombosis, ischemic stroke, coronary revascularization with DES); no longer
taking DAPT with ticagrelor + ASA; non physician-guided cessation of ASA or ticagrelor of 5 consecutive days; current indication for oral anticoagulation or high dose ASA; renal failure
requiring dialysis; woman of child bearing potential; refusal of randomization by patient or treating physician; withdrawal of consent; lost to follow-up
Exclusion Criteria

© AstraZeneca 2019
TWILIGHT: Primary Endpoint1
43
Note: The primary endpoint analysis was performed in the ITT cohort, including those who were successfully randomized at the 3-month visit.2
1. Mehran R et al. Online ahead of print. N Engl J Med. 2019; 2. Baber U et al. Am Heart J. 2016;182:125-134.
0
2
4
6
8
10
3555 3474 3424 3366 3321 Ticagrelor Monotherapy
3564 3454 3357 3277 3213 Ticagrelor DAPT
Number at risk
0 3 6 9 12
BARC 2, 3 or 5 Bleeding
Monotherapy vs. DAPT
HR 0.56 (95% CI 0.45-0.68)
p<0.001
Cu
mu
lati
ve In
cid
en
ce (
%)
Months Since Randomization
Ticagrelor Monotherapy 4.0%
Ticagrelor DAPT 7.1%
Definitions of BARC Bleeding

© AstraZeneca 2019
Note: The key secondary endpoint was performed in the per protocol cohort, including those who were randomized and completed all study-related contacts without any major protocol deviations.2 aNon-inferiority was tested at a one-sided alpha level of 0.025 using 1.6% as the absolute upper limit of the 95% CI.2
1. Mehran R et al. Online ahead of print. N Engl J Med. 2019; 2. Baber U et al. Am Heart J. 2016;182:125-134.
TWILIGHT: Key Secondary Endpoint1
44
Cu
mu
lati
ve
In
cid
en
ce
(%
)
0
2
4
6
8
10
0 3 6 9 12
Ticagrelor Monotherapy: 3.9%
Ticagrelor DAPT: 3.9%
Composite of All-Cause Death, MI or Stroke
Monotherapy vs. DAPT
HR 0.99 (95% CI 0.78-1.25)
Non-inferiority p<0.001a
3524 3457 3412 3365 3330
3515 3466 3415 3361 3320
Ticagrelor Monotherapy
Ticagrelor DAPT
Number at risk Months Since Randomization

The 16th Malaysian Cardiovascular Interventional
Symposium with Live Transmission
25th – 27th July 2019, Sheraton Petaling Jaya
GAIA 2 changes to Conquest PRO

The 16th Malaysian Cardiovascular Interventional
Symposium with Live Transmission
25th – 27th July 2019, Sheraton Petaling Jaya

The 16th Malaysian Cardiovascular Interventional
Symposium with Live Transmission
25th – 27th July 2019, Sheraton Petaling Jaya

The 16th Malaysian Cardiovascular Interventional
Symposium with Live Transmission
25th – 27th July 2019, Sheraton Petaling Jaya
Multiple predilatation balloons 1.0, 1.5, 2.0, 2.5 NSE Balloon 2.5, 3.0 NC balloons 3.0, 3.5 Used Guide extension

The 16th Malaysian Cardiovascular Interventional
Symposium with Live Transmission
25th – 27th July 2019, Sheraton Petaling Jaya

The 16th Malaysian Cardiovascular Interventional
Symposium with Live Transmission
25th – 27th July 2019, Sheraton Petaling Jaya

The 16th Malaysian Cardiovascular Interventional
Symposium with Live Transmission
25th – 27th July 2019, Sheraton Petaling Jaya
3 DES ONYX 2.75mmx26 ONYX 3.5x38mm ONYX 3.5x38mm


DAPT Duration: Factors to be weighed
HIGH
ISCHEMIC RISK
•High-risk ACS
•Recurrent ischemic events on DAPT
•Peripheral vascular disease
•Prior MI
•Diabetes
•Chronic renal dysfunction
•Complex/multivessel CAD
•Stent-related factors (multiple stents, overlapping stents,
long stents, small-sized stents,
double stents in bifurcations)
•First generation DES
PCI with DES
HIGH
BLEEDING
RISK
LOW
ISCHEMIC
RISK
•Clinically significant bleeding
on DAPT
•Bleeding diathesis
•Prior bleeding
•Female gender
•Elderly
•Liver disease
•Chronic renal dysfunction
•Anemia or thrombocytopenia
•Chronic anticoagulation therapy
•Diabetes
•Second generation DES
• Stable CAD
• Troponin negative ACS
• Single vessel disease
• Simple stenting
(single, short, large stent)
INTERMEDIATE
ISCHEMIC RISK
•Troponin positive ACS
Favors 3 or 6-month DAPT Favors 1-year DAPT Favors >1-year DAPT
When assessing ischemic and bleeding risk, clinical presentation (ACS vs SIHD),
age, disease/PCI complexity and stent type are important factors to consider
Palmerini T and Stone GW. Eur Heart J 2016;37:353-64

The 16th Malaysian Cardiovascular Interventional
Symposium with Live Transmission
25th – 27th July 2019, Sheraton Petaling Jaya
Recently seen 12th July 2019
• Tolerating dialysis well
• Current platelets 200 (eltrombopag 50mg od)
• Still on DAPT – 2 months now

The 16th Malaysian Cardiovascular Interventional
Symposium with Live Transmission
25th – 27th July 2019, Sheraton Petaling Jaya
I will start my last slide as my first slide
• How long would you keep his DAPT
– 1 month
– 3 months
– 12 months
– >12 months

The 16th Malaysian Cardiovascular Interventional
Symposium with Live Transmission
25th – 27th July 2019, Sheraton Petaling Jaya
Thank you

The 16th Malaysian Cardiovascular Interventional
Symposium with Live Transmission
25th – 27th July 2019, Sheraton Petaling Jaya