Embed Size (px)
Citation preview

National I nstitute of JusticeIssues and Practices
U.S. Department of Justice
Office of Justice Programs
National Institute of Justice
DE
PA
RTMENT OF JUST
ICE
OF
FIC
E OFJUST I CE P
RO
GR
AM
S
BJ
AN
I JOJJDP
BJSO
VC
Program Focus
Managing MentallyIll Offenders in the
Community
Mil waukee’s CommunitySupport Program

2 National Institute of Justice
PROGRAM FOCUS
Managing Mentally Ill Offenders in the Community:Milwaukee’s Community Support Programby Douglas C. McDonald, Ph.D., and Michele Teitelbaum, Ph.D.
ersons suffering chronic mental illnesses are fre-quently caught up in the criminal justice system, butjustice agencies are usually ill equipped to respondeffectively to the problems they pose. Jailing themkeeps them off the streets, but this provides only ashort-term solution at a high price. Probation maybe warranted in some cases, but conventional supervi-sion and services are often insufficient. Many men-tally ill persons need the most elementary ofnecessities as well as medication, and they requiremore intensive monitoring than most probationdepartments are able to devote to them.
The Wisconsin Correctional Service(WCS), a private not-for-profit organi-zation in Milwaukee, has establishedan innovative Community SupportProgram (CSP) that adopts a “carrotand stick” approach to managing men-tally ill offenders in the community,most of whom are schizophrenic.Since many of the program’s clientscome to the attention of criminal jus-tice agencies, formal legal authority isused initially to get offenders into theprogram.
The program is also well suited toserving mentally ill persons who havenot yet come into the criminal justicesystem but may be at risk of doing so.Many WCS clients have run afoul ofthe law because they are actively psy-chotic and not medicated, and with thecourt’s authority most can be con-vinced to accept medications. Onceengaged in the program, many offend-ers comply willingly with its require-ments because they receive substantialbenefits, various needed social serv-ices, and life supports. Indeed, somechoose to stay in the program foryears, well beyond the cessation oftheir legal obligations.
The program was developed in 1978,when WCS noticed the growing num-bers of chronically mentally ill personscoming into Milwaukee’s courts andjails. Since then, the county has copiedthe basic design and has funded threeother community support programs,two under contract with private orga-nizations, and a third operated directlyby county officials. The programmodel includes the following fivedefining elements, all of which can be
P
agency, provides an alternative to incar-ceration for this population through a mixof coercion, incentives, and housingassistance, money management, and thera-peutic support services.
The program does this for $3,000 a yearper client—less than it would cost forintensive outpatient treatment in local men-tal health systems. This Program Focusdescribes how the program works andhow it gained community acceptance. It isan approach that offers a ray of hope tomunicipalities seeking a just, humane, andrealistic means of dealing with mentallyill offenders while protecting the widercommunity as well.
National Institute of Justice
Every day our crowded, overbur-dened jails and probationdepartments face yet another
challenge—dealing with offenders whoare mentally ill and require medication,close monitoring, and other services.Many of these persons have been in andout of jails and hospitals. Few havehomes or jobs, and more and more ofthem are drug-addicted as well. Theirown untreated, often psychoticbehavior may have been the cause oftheir being arrested in the first place.
Milwaukee faced up to the problem 15years ago when it developed a programto keep these offenders out of jail, out ofthe hospital, and under close communitysupervision. The Community SupportProgram, run by a private nonprofit

Program Focus 3
PROGRAM FOCUS
adapted quite readily to other jurisdic-tions. These include:
Medical and Therapeutic Services.Medication is prescribed, administered5 days a week, and closely monitoredby a pharmacy on the premises. Psy-chotherapy and group sessions are alsoavailable, and case management serv-ices are provided to all clients to helpthem obtain primary health care.
Money Management. The programarranges to be the legal recipient forthe client’s social security and otherdisability benefits. The client’s fixedexpenses (rent, for example) are paiddirectly by the program. The remain-der is given to the client in a dailyallowance—after the client has takenhis or her prescribed medicine.
Housing and Other Support Services.Intensive casework is undertaken toprovide for the client’s basic needs,either after arrest, or upon release fromjail or a hospital. This includes referralto other social service agencies, ifneeded. Housing in the community isarranged directly by the program, anddaily living is monitored by periodichome visits.
Day Reporting and Close Monitoring.Most clients are required to report tothe clinic daily, Monday through Fri-day, where they can stay either for abrief period to take their medicationsand get their money or for longer peri-ods. The daily observation and interac-tion with the clients enables the staffto monitor behavior and to spot whenchanges in medications are needed.Failure to report is noted, and clientsare located.
Participation. Although clients mustagree to enter the treatment program,their choice is constrained by otherless desirable alternatives, includingjail. Because many mentally ill per-sons are difficult to manage and resistbeing medicated, the combination ofsupportive services backed by firmlegal authority is effective in bringingthem into treatment.
Program administrators believe thatwhat keeps them in the program arethe benefits. Prior to coming into theprogram, many of the clients arehomeless and without any means ofsupport. By helping them get shelter,income, and medication, the programcreates a powerful incentive forstaying.
Program OperationsThe program operates out of a smallclinic located in a predominantly resi-dential neighborhood. The clinic has afriendly, relaxed feeling about it, with-out the trappings of a more institu-tional environment. Clients even havea room where they can socialize witheach other or just relax during thedaytime.
Clinic staff are readily available to allclients and offer a broad range of serv-ices. Three full-time nurses provideclinical support to clients who, in ad-dition to psychological distress, oftenneed primary health care evaluationand referral to medical services. Apart-time psychiatrist diagnoses cli-ents and prescribes them psychotropicmedications as needed. The pharmacystaff dispense all medications andmanage the required recordkeeping.
Four full-time case managers have acaseload of 60 clients each. Severalfinancial service staff members helpclients obtain government benefits andmanage their money. Daily allowancesare given out by a cashier. Two staffpersons work to obtain housing forthose who need it and to help manageclients’ ongoing relationships withtheir landlords. A small managementand administrative staff direct overalloperations.
The program has the capacity to serveapproximately 250 clients at any onetime, a number that has remained fairlystable over the past several years. Dur-ing 1992, a total of 312 clients at-tended the program. On any given day,program staff see about 200 clients,most of whom visit briefly to take theirmedicine and get their daily allowance.The others are on schedules that re-quire less than daily reporting.
The Community Support Program hasdeveloped a combination of coerciveelements, incentives, and support thatencourages clients to use services tohelp them live in the community with-out violating the law.
Entry Intothe ProgramClients come into the CSP throughvarious routes. Some are identified byworkers in other programs that WCSoperates for Milwaukee’s municipalcourts. Others are referred by proba-tion and parole officers or by privateattorneys. A small percentage comeinto the program on their own. Someare referred by psychiatric hospitals.

4 National Institute of Justice
PROGRAM FOCUS
A common entry channel is throughthe work of the associated programsrun by WCS in the criminal justicesystem. Two programs are based at thecourts: the Central Intake Unit and theMunicipal Court Intervention Pro-gram. The former is a pretrial servicesagency, similar to others elsewhere inthe Nation, although it provides amore expansive and comprehensiveset of services than many others do.These include a separate intensivepretrial supervision program and adrug testing program.
The Municipal Court InterventionProgram provides a structured alterna-tive to incarceration for persons con-victed in municipal courts. It aimsprincipally to keep in the communitypersons convicted of violating munici-pal ordinances who are in need of
mental health, alcohol, or drug treat-ment; indigent persons unable to payfines imposed by the municipal court;and those who are due to be trans-ferred to the local correctional facility.
Staff at the Central Intake Unit’sscreening center interview all defend-ants brought into the courts for ar-raignment to obtain informationneeded by the court for bail and cus-tody decisions. Each day, hundreds ofsuch defendants are interviewed. Inthe course of these interviews, intakescreeners also identify persons whoappear to be candidates for the pro-grams operated by WCS, including theCommunity Support Program. If staffsuspect that a defendant is mentally ill,he or she is interviewed more inten-sively and considered for the CSP.
Although such screening may exist inother jurisdictions, pretrial serviceagencies generally lack the capabilityto provide needed services directly.Instead, defendants are referred toservices, if they are at liberty, or theymust wait to be transferred elsewherefor services if they are in custody. Formentally ill persons, such delays intreatment can exacerbate their mentaland physical conditions. For that rea-son, the Central Intake Unit worksclosely with the courts to place appro-priate offenders and defendants intothe Community Support Program asquickly as possible.
Wisconsin Correctional Service staffalso canvass the populations in thelocal jails and prison for possible re-ferral to WCS programs. Again, thosedefendants or offenders who showsigns of mental illness are identifiedand given more intensive consider-ation to determine if referral to theCommunity Support Program isappropriate.
Once individuals are identified as suit-able for the Community Support Pro-gram, the courts are notified. In someinstances, judges may refer defendantsto the program as a condition of pre-trial release. If the potential clientshave already been convicted, thecourts may order offenders into theprogram and impose treatment obliga-tions as a condition of probation. Re-ferrals that represent a genuinealternative to incarceration are givenpriority. The close supervision andassistance that the program provides—and the fact that conditions are en-forced—gives judges and jailers the
The psychiatrist on duty has an open-door policy for clients who want to come in and talk or whohave questions about their medications.
Pho
to by
Por
ter G
iffor
d, N
ew Y
ork,
N.Y
.

Program Focus 5
PROGRAM FOCUS
confidence to release mentally ill per-sons to the program.
Another path into the program isthrough referral by probation and pa-role officers. For those mentally illoffenders in need of a blend of serv-ices—intensive supervision, dayreporting, and monitored medica-tions—participation in the programcan be imposed as a condition of re-lease. Staffs of probation, paroleagencies, and the program have devel-oped close working relationships tocreate a consistent set of rules andexpectations.
After entry into the program, theclient’s behavior is closely monitored,and the appropriate authorities areroutinely informed.
In recent years, about 1,000 arresteeshave been identified annually as beingmentally ill. Of those, approximately200 to 300 were both eligible for re-lease and deemed suitable for the pro-gram. Of the remaining 700 to 800,some were already in treatment pro-grams and were referred back to them.Others were hospitalized, and stillothers had their charges dropped. Notall those who appeared to need theprogram’s services and to meet theadmissions criteria could be servedimmediately because slots in the pro-gram were limited. During 1992, forexample, 67 new clients were admittedto the program. (See exhibit 1.) Thirtyothers were referred to other county-funded community support programs.Another 40 remained in custodythrough the end of the year and there-fore were not eligible for admission tothe program. Those who were released
but not admitted to any of the commu-nity support programs were put on awaiting list. Many of those placed onthe waiting lists were released fromdetention with the requirement thatthey report daily to mental healthcounselors/case workers in the CentralIntake Unit.
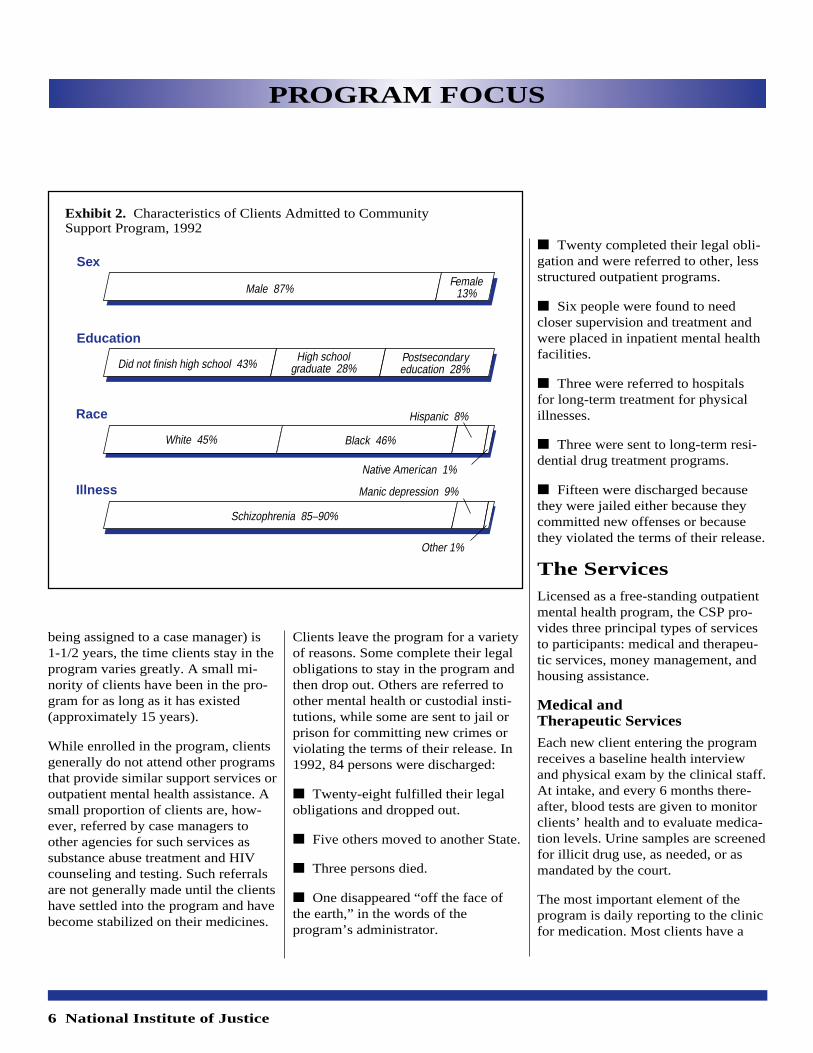
The ClientsThe typical CSP client is a male in hismid-thirties who has never been mar-ried, has some secondary education,and has a diagnosed major mentalillness. The majority had at least twoprior arrests on their record. Clientsentering the program in 1992 averaged75 days in psychiatric hospitals duringthe preceding 2 years. (See exhibit 2.)
Although the number of admitted per-sons has remained relatively constantover the past several years, the clinicalconditions of clients have changed.The Milwaukee area has seen an up-surge in mentally ill offenders who aredrug users (so-called dually diagnosedclients), paralleling the reported in-crease in cocaine use in the area.
Clinic staff say that these dually diag-nosed offenders are more difficult totreat, have more serious histories ofinstitutionalization, and demonstratemore frequent relapses and recidivismthan mentally impaired offenderswithout substance abuse problems.Program staff report that prior to theupsurge in cocaine use and duallydiagnosed clients in the area, fewerthan 10 percent of the offendersreleased from the program were re-institutionalized in either jails or psy-chiatric hospitals. Staff find that nowabout one-quarter of the offendersreleased from the program are lockedup again, an increase that they at-tribute to cocaine abuse.
The Community Support Program seesmany clients who have histories ofnoncompliance with outpatient treat-ment programs. Indeed, many clients(39 percent in 1992) returned to theCommunity Support Program, eithervoluntarily or through referral, after aperiod of not being enrolled. Althoughthe average length of stay in the pro-gram as an active case (defined as
Exhibit 1. Admissions to Community Support Program, 1992
Reason Number (Percent)
Pretrial release 27 (40%)
Probation 30 (45%)
Court order after trial 4 (6%)but before sentencing
Noncriminal, voluntary 6 (9%)
TOTAL 67 (100%)
6 National Institute of Justice
PROGRAM FOCUS
being assigned to a case manager) is1-1/2 years, the time clients stay in theprogram varies greatly. A small mi-nority of clients have been in the pro-gram for as long as it has existed(approximately 15 years).
While enrolled in the program, clientsgenerally do not attend other programsthat provide similar support services oroutpatient mental health assistance. Asmall proportion of clients are, how-ever, referred by case managers toother agencies for such services assubstance abuse treatment and HIVcounseling and testing. Such referralsare not generally made until the clientshave settled into the program and havebecome stabilized on their medicines.
Clients leave the program for a varietyof reasons. Some complete their legalobligations to stay in the program andthen drop out. Others are referred toother mental health or custodial insti-tutions, while some are sent to jail orprison for committing new crimes orviolating the terms of their release. In1992, 84 persons were discharged:
■ Twenty-eight fulfilled their legalobligations and dropped out.
■ Five others moved to another State.
■ Three persons died.
■ One disappeared “off the face ofthe earth,” in the words of theprogram’s administrator.
■ Twenty completed their legal obli-gation and were referred to other, lessstructured outpatient programs.
■ Six people were found to needcloser supervision and treatment andwere placed in inpatient mental healthfacilities.
■ Three were referred to hospitalsfor long-term treatment for physicalillnesses.
■ Three were sent to long-term resi-dential drug treatment programs.
■ Fifteen were discharged becausethey were jailed either because theycommitted new offenses or becausethey violated the terms of their release.
The ServicesLicensed as a free-standing outpatientmental health program, the CSP pro-vides three principal types of servicesto participants: medical and therapeu-tic services, money management, andhousing assistance.
Medical andTherapeutic Services
Each new client entering the programreceives a baseline health interviewand physical exam by the clinical staff.At intake, and every 6 months there-after, blood tests are given to monitorclients’ health and to evaluate medica-tion levels. Urine samples are screenedfor illicit drug use, as needed, or asmandated by the court.
The most important element of theprogram is daily reporting to the clinicfor medication. Most clients have a
Sex
Education
Race
Illness
Male 87%Female
13%
Did not finish high school 43%High school
graduate 28%Postsecondaryeducation 28%
White 45% Black 46%
Hispanic 8%
Native American 1%
Schizophrenia 85–90%
Manic depression 9%
Other 1%
Exhibit 2. Characteristics of Clients Admitted to CommunitySupport Program, 1992

Program Focus 7
PROGRAM FOCUS
history of stopping their medications,becoming actively psychotic, and, insome cases, aggressive. To ensure thatclients comply with their medicationschedules, the program has developedan efficient system for dispensingmedicines and monitoring their use.After the intake exams, a psychiatristprescribes medications. On each day,Monday through Friday, clients cometo the clinic, stand in medication linesat the pharmacy window, and taketheir medicines in front of nurses.They then receive a chit to turn in atthe cashier’s window, where they gettheir daily allowances.
This process is not rushed, and thenurses have time to strike up conversa-tions with clients. This provides themthe opportunity to observe clients’behavior and to spot any need for ad-justing the mix and dosage of drugs.Clients can be either overmedicated orundermedicated, or they can developside effects that can be moderated orsuppressed with other drugs. If a nursesuspects that an adjustment in themedications is needed or if there areother problems needing attention, theclient can be referred to the psychia-trist or other service specialists in theCSP.
The use of a registered nurse, licensedpractical nurses, and pharmacy assist-ants allows low-cost maintenance ofthe medication services. The pharmacydispenses medications to some 200clients a day. Although most clientsstarting the program visit daily, theprogram reduces this requirement forsome after a period of reliable attend-ance. Medication alone would be aninsufficient incentive to keep clients in
the program. Caseworkers in the clinicalso provide a number of valuableservices to patients who report faith-fully and maintain their medicationschedules. These benefits may be farmore compelling than the court orderthat initially motivated most of theclients.
Money Management
Clients receive considerable assistancein managing their money. Nearly allagree to have the Community SupportProgram serve as the payee for SocialSecurity and other government disabil-ity benefits. The program pays all ofthe clients’ fixed expenses, such asrent, and the remainder is doled out tothe clients daily—after they havetaken their medications. Failure tocomply with a treatment plan can re-sult in withholding a scheduled cashallowance. Clients interviewed at theclinic said that they appreciated thisservice. Many realize that they are notable to manage their money well, andmany are afraid of being preyed uponby thieves and con artists who knowwhen monthly disability checks aredelivered.
The program’s full-time financialservices advocate manages clients’entitlement claims. Additionally, full-time money managers assist clients inmaintaining their accounts, budgetingtheir funds, and scheduling paymentsand billings. A behind-the-scenes fi-nancial services coordinator overseesall accounts, keeping each client’sfunding stable.
Devising the internal money-manage-ment procedures was a challenge.Accounts have to be reconciled every
day because clients make approxi-mately 200 withdrawals of smallamounts daily. Accounting procedureshave been computerized, using a pro-gram that was written especially forthat purpose.
Upon enrollment, the client (or theprogram on behalf of the client) ap-plies for both general assistance/wel-fare and Social Security benefits,either Supplemental Security Income(SSI) or Social Security DisabilityInsurance (SSDI). However, someclients are eligible for both SSI andSSDI, and a small number are alsoeligible for veterans’ benefits. Thegeneral assistance benefit is usuallyapproved first, but because the SSI orSSDI benefit is retroactive from thedate of application, these Federalfunds are used to reimburse the gen-eral assistance agency.
Housing AssistanceHousing assistance is another majorcomponent of the program. Overthree-quarters of all clients lack stablehousing when they enter the program,and the Community Support Programfinds rental housing for them. Overtime, and by means of a variety ofstrategies (including newspaper adver-tisements and word of mouth), CSPofficials have enlisted the help of land-lords willing to house clients. Atpresent, the roster lists approximately425 landlords, making about 1,000apartments available to the CSP.Landlords like the program becausethey know that they will receive rentchecks regularly and directly from theprogram’s administrators. They arealso willing to accept security deposits

8 National Institute of Justice
PROGRAM FOCUS
in several installments. The housingservice has computerized part of itsoperations, so that rent checks arewritten and mailed out automatically,and an inventory of housing is main-tained and closely monitored. During1992, WCS found housing for ormoved 170 clients. The program evenprovides a truck and other assistancewhen clients have to move. In additionto organizing and managing fundingfor clients’ housing, the program solic-its donations of furniture and house-hold items from the public to helpclients achieve a decent, albeit mini-mal, standard of living. Caseworkersvisit clients’ households on a periodicbasis to assess their treatment needsand check on their welfare.
As an additional source of assistancefor the housing program, the programreceived a Housing Cost ReductionGrant in 1992 from the State govern-ment. This one-time grant was depos-ited in an interest-bearing account, andthe revenue generated by this accountenables the program to extend loans toclients for security deposits and firstmonth rents. Clients can then use theirmonthly benefit funds to buy essentialfurnishings for their households and topay the program back over time for theloans. Obtaining this additional sourceof funds, and using it for these pur-poses have proved a creative and suc-cessful venture by the program.
Success FactorsThe program’s primary objectives areto keep persons afflicted with chronicmental illnesses out of the local jailsand hospitals and to help them liveindependently. Although the programhas not been formally evaluated, itappears to be achieving its goals. In-deed, county officials are so persuadedof the program’s usefulness that theyhave dedicated scarce State and Fed-eral aid dollars to fund three othersimilar programs. By creating a sys-tem for identifying mentally ill per-sons brought into court and jail andcreating a programmatic alternativethat the courts use, the program isundoubtedly reducing the number ofmentally ill persons in jail. Theprogram’s administrators report that inrecent years the proportion of jail in-mates diagnosed as mentally ill hasbeen small—about 3 percent, on aver-age—and that the proportion wasmuch larger prior to the program’screation.
Further evidence of the program’ssuccess in accomplishing its objectiveof diverting mentally ill persons fromjail is seen in the tributes voiced bycourt officials. The judges, prosecu-tors, and defense attorneys interviewedstrongly support the program, as dothe court and jail staff. Relations withother agencies (including mentalhealth, parole and probation agencies,forensic services, and State hospitals)are positive, according to those offi-cials interviewed. One judge inter-viewed said that confidence in theprogram is “as high as it could be.”Another judge said that the court “can-not do without the program.”
agencies. Because the program was sup-porting clients in the interim, substantialcash-flow problems resulted. When theprogram lost a client before finally get-ting him or her registered, it was unableto collect the client’s past claims andsuffered a financial loss as a consequence.
The key was to get the various benefitagencies to let the Community SupportProgram do all the necessary paperworkfor applications. This occurred when of-ficials in the welfare department realizedthat the information the CSP providedwas always correct and that the difficul-ties of handling these clients in theiroffices could be avoided by having theCSP conduct the interviews and obtainthe needed data. Once an agreement wasreached to delegate these responsibilitiesto the CSP, the program made similararrangements with other benefit agen-cies. This has made registration and en-rollment much more efficient and hasreduced the program’s cash-flow prob-lems to a manageable level.
One of the program’s important innova-tions was to develop special arrange-ments with Federal, State, and countyagencies to conduct screening interviewswith clients for benefits. When the pro-gram first began, many clients were notreceiving benefits to which they werelegally entitled.
The program helped manage their enroll-ment and sent hundreds of mentally illpeople to government offices for inter-views. But for many clients these inter-views were a large stumbling block togetting registered. Many severely dis-turbed clients have neither the socialskills nor patience required for makingan appointment, showing up several daysor weeks later, bringing all the requireddocuments, waiting in line, communi-cating clearly with social service case-workers, and filling out forms.
It took months to get clients on the rollswith social security and county welfare
Avoiding Cash Flow Problems

Program Focus 9
PROGRAM FOCUS
Low CostCentral to the program’s success hasbeen its ability to provide this serviceat a low cost. The cost per serviceslot—about $3,000 per year—is aboutone-quarter to one-third the cost ofintensive outpatient treatment in theState and county mental health sys-tems. Costs are low because the pro-gram uses paraprofessionals to deliverservices whenever possible, ratherthan employing a large staff of certi-fied specialists with advanced degrees.(A majority of the program staff havebachelor’s degrees rather than higher,more specialized degrees.)
Perhaps the program’s greatest accom-plishment, therefore, is that it has de-vised an important support service thatdid not previously exist in a fiscalenvironment that has not encouragedpublic expenditures for the poor andneedy. The program has increased thelevel of services in a county that hashigh property taxes and great resist-ance to increased government spend-ing. According to the county’s budgetdirector, local government would notprovide these services if doing so re-quired the creation of new countyemployee positions funded by countytax revenues. Relying upon a privateentity, the Wisconsin CorrectionalService, and a low-cost model of serv-ice delivery made it unnecessary tocreate new government positions.
Financial support is obtained from twoprincipal sources. The most importantand largest is a grant from the Com-bined Community Services Board, aState government entity establishedto allocate and administer State and
Federal block grant funds for disabledpersons. The second most importantsource is the United Way, which hasbeen supporting the program for years.Additional sources of revenues includethe Community Options Programfunds from the State for long-termchronically mentally ill clients, as wellas medicaid, medicare, and privateinsurance payments for psychiatric,psychological, and pharmaceuticalservices.
Creating SimilarPrograms ElsewhereThe Community Support Programdoes not depend on unique conditionsin Milwaukee for its existence, and itcould be adapted elsewhere with onlyslight modifications. The program didtake advantage of the pretrial screen-ing procedures and organization al-ready in place. It also benefited fromits private rather than governmentaloperating authority. Neither are neces-sary preconditions, however.
Locating facilities for mentally ill per-sons is difficult in many communities,because residents and merchants fear thatthe concentrated presence of such per-sons will have a negative effect on theirproperty values and businesses. Despitethis resist-ance, the CSP has managed towin the support of its neighboring com-munity. This has resulted in part from theprogram’s working to accommodate theinterests of its neighbors. Initially, theprogram was located in the heart of thedowntown area, in a government officebuilding. Merchants were concerned thatclients milling about the clinic might scarecustomers away. The most effective solu-tions to this problem, devised after meet-ing with the merchants, were surprisinglysimple. Reporting times were spreadthroughout the day, so that an undulylarge number of clients would not becongregating around the clinic at anyparticular hour. The building was alsoopened and staffed 1-1/2 hours in ad-vance of the first scheduled reportingtime so that clients arriving early couldcongregate inside, rather than on the street.
When the program moved to its presentlocation, in a mixed residential and com-mercial area, citizen groups were con-
Gaining Community Acceptancecerned about the effects on their busi-nesses. To alleviate this anxiety, theprogram’s directors invited neighbors toan open house to see the facilities andobserve operations. Local residents wereinvited to join an ad hoc advisory com-mittee. Program staff also attend bi-monthly neighborhood coalition meet-ings and make themselves available torespond to any complaints or special con-cerns. Area businesses are given the namesand telephone numbers of project staff tobe contacted in the event that clients cre-ate problems in the neighborhood. Promptattention to residents’ requests has helpeddiffuse tensions as they arise. Althoughthe program still gets occasional com-plaints, it now appears to be operatinginconspicuously in the community.
Although these various outreach effortshave been important in bringing aboutgood community relations, the program’sadministrators believe that the most ef-fective strategy has been to address theclients’ basic needs (housing, moneymanagement, and medication) early andeffectively. If clients are well served,their anxieties are generally reduced; act-ing out is minimized; and the likelihoodof their drawing attention to themselvesin the community is lessened.

10 National Institute of Justice
PROGRAM FOCUS
offenders. However, most probationagencies are only brokers: officers donot provide services directly (otherthan supervision), and they mustrefer their charges to other serviceproviders.
Jurisdictions that already have pretrialscreening agencies or organizationswill be most able to develop a commu-nity support program economically.Because these agencies assess defend-ants’ likelihood to appear at trial, theyalso provide a convenient point foridentifying persons who might bementally ill. In jurisdictions lackingsuch pretrial screening capabilities,procedures would have to be devel-oped to identify the mentally ill in jail.While identification and referral in jailis preferable to no screening at all,identification at the pretrial stage isbetter, because then mentally ill de-tainees can be diverted from jail alto-gether if the charges are not seriousenough to warrant detention.
Private or PublicOperationSince the Community Support Pro-gram is privately operated in Milwau-kee, other local governments maywant to follow this model. In consider-ing where to locate responsibility fordevelopment and operation of a com-munity support program, governmentofficials should consider how existingstandards and practices in the candi-date agency might constrain its abilityto adopt all elements of the CSP’slow-cost design. For example, obliga-tions to meet more acute care (such asinpatient treatment) standards in anagency might raise costs substantially,because such standards require the
Because our knowledge of mental ill-nesses is limited, it is unrealistic to expectany program to cure these illnesses. Thebest one can realistically expect is thatmentally ill persons can be helped toachieve some stability in their living ar-rangements, to live independently in thecommunity rather than in a hospital orother custodial facility, to be protectedfrom persons who would prey upon them,and to be relieved to the extent possible ofthe anxieties, fears, and delusions thattorment them.
It is clear that the Community Support
Program is accomplishing these goals. Ifthe program did not exist, a large propor-tion of the clients would be homeless,living in a succession of temporary shel-ters, or cycling through hospitals. Manywould be actively psychotic, as mostwould not be medicated or under psychi-atric supervision. By managing their hous-ing and money, the program minimizesthe opportunities for swindlers and thievesto victimize clients. It is also likely thatthe clients’ own criminal behavior—mostly thefts, assaultive behavior, anddrug taking or selling—is also lessened.
Setting Realistic Expectations
The program’s money manager works with clients to budget their funds and to reach anagreement on how much money they will receive each day.
do some of this on an ad hoc basis toget an unruly prisoner out of a facility.In many jurisdictions, judges rely onprobation officers to assist them infashioning a useful and appropriateresponse to mentally ill defendants and
Pretrial Screening Capacity
In many jurisdictions, there are nospecific services for identifying men-tally ill persons in the criminal justicesystem and devising placements forthem, although jail administrators may
Pho
to by
Por
ter G
iffor
d, N
ew Y
ork,
N.Y
.

Program Focus 11
PROGRAM FOCUS
Opinions or points of view expressed inthis document are those of the authors anddo not necessarily reflect the official posi-tion or policies of the U.S. Department ofJustice.
use of professional, rather than para-professional, employees. However,governments willing to make the com-mitment could create a program simi-lar to CSP and avoid the issue ofrelying on local tax revenues to supplynew government services.
About This StudyThis document was written byDouglas McDonald, Ph.D., andMichele Teitelbaum, Ph.D., seniorsocial scientists at Abt Associates Inc.Elissa Weitzman, research analyst, andStacia Langenbahn, editorial assistantat Abt, assisted the authors.
Data for this report were obtainedfrom several sources. Site visits in-cluded interviews with directors andstaff of the Wisconsin CorrectionalService and its Community SupportProgram and Central Intake Unit; staffof the district attorney’s and publicdefender’s offices, and the local jail;judges of the State district and munici-pal courts and a court commissioner;representatives of the State’s Depart-ment of Health and Social Servicesand the county’s budget office; andtelephone interviews with representa-tives of the United Way (a fundingsource) and the State mental healthhospital. Several useful documentswere also provided by the WSC, in-cluding program descriptions, recentannual reports, and public presenta-tions of Bowne (Bob) J. Sayner,
Assistant Executive Director of theWisconsin Correctional Service.
Additional information about theCommunity Support Program can beobtained from the Wisconsin Correc-tional Service, 436 West WisconsinAvenue, Milwaukee, WI 53203,(414–271–2512).
Cover photo by Porter Gifford, NewYork, N.Y. Pictured are clients whoreport each day to the program’spharmacy window for their medica-tions, which they are required to takein front of a nurse.
The National Institute of Justice is acomponent of the Office of JusticePrograms, which also includes the Bureauof Justice Assistance, Bureau of JusticeStatistics, Office of Juvenile Justice andDelinquency Prevention, and the Office forVictims of Crime.
A client cooks his lunch in the apartment that the Community Support Program arranged forhim to rent.
Photo by P
orter Gifford, N
ew Y
ork, N.Y
.
NCJ 145330 March 1994

12 National Institute of Justice
PROGRAM FOCUSU.S. Department of JusticeOffice of Justice Programs
National Institute of Justice
Washington, D.C. 20531
Official BusinessPenalty for Private Use $300
BULK RATEPOSTAGE & FEES PAID
DOJ/NIJPermit No. G–91