Embed Size (px)
Citation preview
Managing Risk in Perinatal Care
Linda A. Hunter, CNM, EdDRobin Shields, RNC-OB
Disclosures- We have received financial support from
Laerdal to present this topic- We have no contractual relationship with
Laerdal
ObjectivesDiscuss the medical/legal environment in the
perinatal area.Identify issues specific to perinatal care.Describe the role of simulation in providing
safe, reliable care.Discuss collaboration with multidisciplanary
leadership.Describe how to plan and implement in-situ
simulation

“To Err is Human”Factors contributing to errors:
It’s NOT an “individual provider issue”Convergence of multiple contributing factors
Complexity of many health problemsLack of communicationIneffective interdisciplanary cooperation
IOM, 2000
IOM Key RecommendationsEstablish national focus to enhance
knowledge about patient safetyLeadership, research, tools, protocols
Identifying and learning from errors through mandatory reporting effortsEncourage voluntary non-punitive reporting
Raising standards and expectationsCreating safety systems within health care
organizations
Perinatal Safety IssuesNational Quality Forum:
National Voluntary Consensus Standards for Perinatal Care
Joint Commission: Perinatal Core Measures Set
March of Dimes:Toward improving the outcome of
pregnancy III.

Interprofessional & Interdisciplinary Education
Core competencies include working in teamsImproves collaboration and communicationIncreases understanding of differing rolesEnhances professional confidenceAvoids “professional silos”Improves attitudes and morale Improves quality of care
Reduces errors
Teamwork TrainingAviation Industry: Crew Resource
ManagementReplace hierarchal relationships with mutual
decision-making Organize individuals to think/act as a team
Structured Communication “SBAR”SituationBackgroundAssessmentRecommendationsReduces errors
Using Simulation for Team Training
Active interdisciplinary learning environmentIntegrates cognitive, affective, psychomotor
skillsAssesses team management of high risk
scenariosIncreases shared learning, interaction, and
collaboration
Reduces Errors
Importance of DebriefingSafeguard learning experienceConfidentiality agreementsNot part of performance evaluationRules of conduct
Constructive feedbackEvaluate team performanceFollow standards of care
EMTALAEmergency Medical Treatment and Labor
ActAny patient who presents to the ED must have
an appropriate medical screening examination to determine if an “emergency medical condition” exists
Pregnant women in active labor Must be examined Can they be sent home? Can they be safely transferred?
Emergency Deliveries Often chaoticSuboptimal locationMinimal patient infoLack of equipmentInexperienced birth
attendantsTraumatizing experience
Factors
Choice
Access
Time

Perinatal RisksMaternal
Shoulder dystocia
Postpartum hemorrhage
Serious lacerationsCervical/vaginalPerineum
3rd/4th degree
FetalFetal distressMeconium
aspirationLow Apgar scoresNeonatal injuryHypothermiaInfection
Maternal and family dissatisfaction
Making a Decision to TransferTo another facility
EMTALA rules applyTo another unit (ie Labor & Delivery)
Bed & provider availability
Judgment of the examining provider
Where is the safest location?
Establishing a ProtocolALL Emergency Departments
Training, simulation & practice drillsALL staff (MDs, APRNs, RNs, Unit secretaries etc)
Having equipment readyInfant warmerPrecipitous birth packs
Specialized documentationBirth summary

Implementing a Work in Progress

Crisis SituationThemes
Lack of Communication Between team Between family
Lack of Team LeadershipLack of Efficiency
Role delineation Access to necessary equipment
Lack of Patient Satisfaction
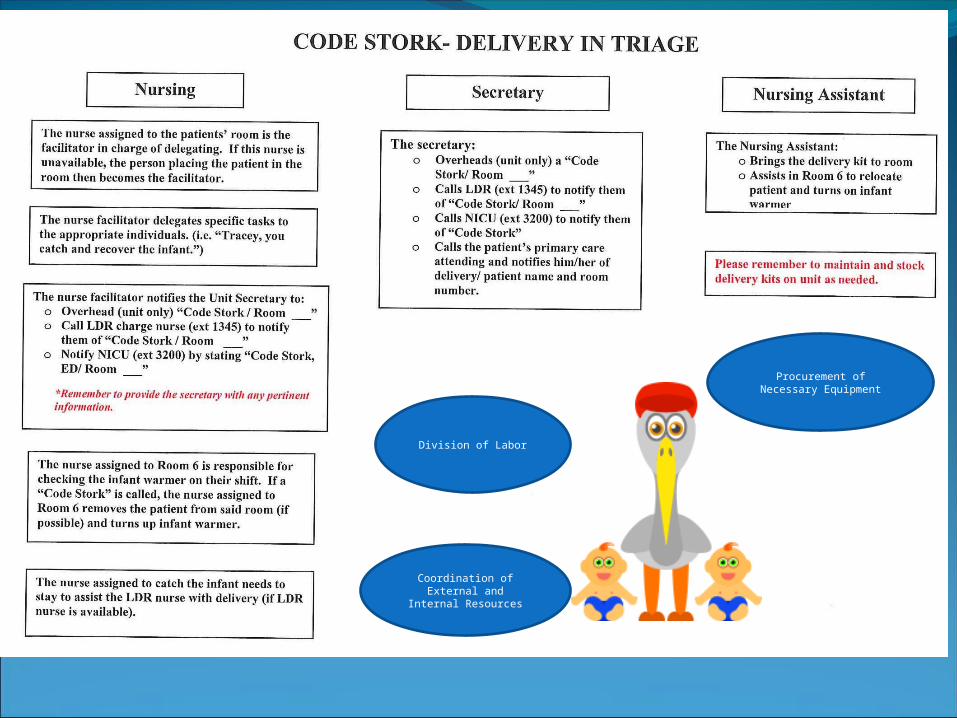
Division of Labor
Coordination of External and Internal
Resources
Procurement of Necessary Equipment

“Code Stork” Test Run • Goals: Assess knowledge and compliance with the policy• “Surprise” simulation• Realistic scenario• Failed home birth with meconium
Observations & DebriefingInadequate communication
Key questions not asked No SBAR No clear team leader No delegation of roles
No coordination Overhead “Code Stork” not called
Limited knowledge on standard of careSuspension of Disbelief
Improving ComplianceHigh Risk/Low Frequency event
Reading policy clearly not enoughCreating a visual example -> Educational
VideoTeam Preparation
Multidisciplinary (RNs, CNMs, MDs, support staff)
Intradepartmental (Triage, LDR, NICU)Scenario Creation
Established guidelines in policy
Learning ObjectivesFoster communication between the
teamEnhance communication with the
familyEstablish leadership in a crisis situationStandardize delivery of equipmentProvide efficiency in the delivery of
care
Implementation PlanDVD was shown to all triage staff
Managerial Staff monitored educational opportunity Allowed for Q+A from Staff Prompted discussion
Over next few weeks, surprise drills were conducted on each shift

Follow-Up Results• Policy awareness was raised• Staff knew the correct “steps”
• Some action steps were still inconsistent• Self identified
• Staff were much more vested in the debriefing process and open to learning/improving

Import DVD here
Achieving Our Objectives?Foster communication between the
teamEnhance communication with the
familyEstablish leadership in a crisis situationStandardize delivery of equipmentProvide efficiency in the delivery of
care
Thank You!
Questions?
ReferencesAngelini DA. Interdisciplanary and interprofessional
education. J Perinat Neonat Nurs. 2011;25:175-9.Arafeh JM, Hansen SS, Nichols A. Debriefing in
simulation-based learning: facilitating a reflective discussion. J Perinat Neonat Nurs. 2010;24:302-9.
Institute of Medicine: To err is human: building a safer health system. National Academy of Sciences,2000; accessed from http://www.nap.edu/catelog/9728.html on September 23,2011.
The Joint Commission. Perinatal core measures set. Oakbrook Terrace, Il. The Joint Commission; 2009.
National Quality Forum. National Voluntary Consensus Standards for Perinatal Care 2008: A Consensus Report. Washington, DC: National Quality Forum: 2008
Simpson, KR. Perinatal safety and quality. J Perinat Neonat Nurs, 2011; 25:103-7.
FAQ on EMTALA. What are the provisions for pregnant women in active labor? April 25, 2011. accessed from www.EMTALA.com/faq.html on September 23, 2011.
March of Dimes. Toward improving the outcome of pregnancy III. White Plains, NY: March of Dimes Foundation 2010. accessed from http://www.marchofdimes.com/professionals/medicalresources_tiop.html on September 23, 2011
Robinson L. Preparing for precipitous vaginal deliveries in the emergency department. J Emer Nurs, 2009; 35:256-8.





























