Embed Size (px)
Citation preview

Material published in this supplement has been peer-reviewed under the supervision of the Editors in accordance with the guidelinespublished in the Advice to contributors and editorial statements published previously [Volume 19 (1987), pp. 711–2 and Volume 25(1990), pp. 731–2].
Managing skin and soft tissue infections: expert panel recommendations on key decision points
Edited by
Kate Gould
Freeman Hospital NHS Trust, Newcastle upon Tyne, UK
David Reeves
Journal of Antimicrobial Chemotherapy, Birmingham, UK
This supplement has been sponsored by F. Hoffmann-La Roche Ltd
The Expert Panel was supported by an unrestricted educational grant from F. Hoffmann-La Roche Ltd
Dow
nloaded from https://academ
ic.oup.com/jac/article/52/suppl_1/i3/2473489 by guest on 11 January 2022

Dow
nloaded from https://academ
ic.oup.com/jac/article/52/suppl_1/i3/2473489 by guest on 11 January 2022

Journal of Antimicrobial Chemotherapy (2003) 52, Suppl. S1, i3–i17DOI: 10.1093/jac/dkg466
i3. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
© The British Society for Antimicrobial Chemotherapy 2003; all rights reserved.
Managing skin and soft tissue infections: expert panel recommendations on key decision points
Lawrence J. Eron1*, Benjamin A. Lipsky2, Donald E. Low3, Dilip Nathwani4, Alan D. Tice1 and
Gregory A. Volturo5
1University of Hawaii, John A. Burns Medical School, Honolulu, HI; 2University of Washington School of Medicine, Antimicrobial Research Clinic, Seattle, WA; 5University of Massachusetts, Medical School, Worcester, MA, USA; 3University of Toronto, Microbiology and Medicine, Toronto, Ontario, Canada; 4Ninewells Hospital and Medical
School, Dundee, UK
Introduction
Skin and soft tissue infections (SSTIs) are suppurative microbialinvasions of the epidermis, dermis and subcutaneous tissues thatinduce a host response. They are characterized by induration, erythema,warmth, and pain or tenderness. Local manifestations may be accom-panied by systemic signs and symptoms, such as fever, chills, malaiseand, at times, haemodynamic instability. SSTIs can sometimes leadto disseminated infection via the circulatory and lymphatic systems,especially in patients with various forms of immune suppression.1
These infections affect various tissues, are caused by a variety ofmicroorganisms and present with wide-ranging clinical manifestations.
By virtue of their incidence and severity, SSTIs represent a majorclinical problem. While the majority of cases are mild and may betreated with oral drugs, moderate or severe cases of SSTI may requirehospitalization and parenteral therapy. In 1995, an estimated 330 000patients in the USA and 4300 patients in Scotland required hospitaltreatment for SSTIs, representing about 0.1% of the adult population.2,3
SSTIs can pose considerable diagnostic and therapeutic challenges.Culturing the causative organisms is often difficult and takes severaldays. Host factors that contribute to the development and recurrenceof SSTIs may not be apparent initially. When parenteral therapy isutilized, patients are frequently hospitalized, making treatment costlyfrom both personal and financial perspectives.4
In February 2003, a panel of clinicians and researchers with interestand expertise in infectious diseases, microbiology and emergencymedicine gathered to discuss the classification and optimal treatmentof SSTIs. The aim of the meeting was to develop practical recom-mendations that aid the clinical decision-making process in dealingwith these infections, and thus optimize patient care. Five keydecision points in the handling of SSTI patients were identified andwill be addressed: (1) whether to hospitalize or to treat in an out-patient setting; (2) which type and route of antimicrobial agents to useinitially; (3) when to switch from parenteral to oral therapy; (4) whento discharge the hospitalized patient; and (5) when to discontinueantimicrobial treatment.
In many areas of SSTI management, there is little in the way ofhigh-level evidence available from randomized clinical trials. Therecommendations and statements given in this document are there-
fore based on published clinical trials where available, and on con-sensus opinion based on the clinical experiences of the faculty. Thesystems of care delivery described here may appear to have a NorthAmerican flavour. However, while regional variations in health careinfrastructure and care delivery may alter the actual method or styleof care delivery, we believe that the underlying philosophies andgeneric principles discussed are applicable globally.5–8
Classification
SSTIs can be divided into four classes according to the severity oflocal and systemic signs and symptoms of infection, and the presenceand stability of any comorbidities (Table 1 and Figure 1). This classifi-cation system serves as a useful guide to admission and treatmentdecisions for patients with SSTIs.9
Class 1 patients have no signs or symptoms of systemic toxicity,have no uncontrolled comorbidities that may complicate treatment,and usually can be managed with topical or oral antimicrobials on anoutpatient basis. Class 2 patients are either systemically ill, but anycomorbidities they may have are stable, or are systemically well, buthave one or more comorbidities (e.g. peripheral vascular disease,diabetes mellitus, chronic venous insufficiency, morbid obesity) thatmay complicate or delay the resolution of their SSTI. Some class 2patients may improve with a course of oral antimicrobials. For thoserequiring parenteral therapy, outpatient parenteral antimicrobialtherapy (OPAT) has the potential to greatly reduce costs and improvepatient satisfaction, with outcomes that are equivalent or superiorto those of inpatient treatment.10–12 Some class 2 patients may requireshort-term hospitalization or observation in an infusion centre oremergency department. Class 3 patients may appear toxic, e.g. havingchanges in mental status, tachycardia, tachypnoea or hypotension, orthey may appear non-toxic but have unstable comorbidities that mayinterfere with their response to therapy. Class 3 patients usuallyrequire initial inpatient treatment with parenteral antimicrobials, butmany can be quickly discharged on OPAT or oral therapy. Someclass 3 patients with limb-threatening infections due to vascular com-promise may need to be hospitalized for vascular evaluation andremediation. Class 4 patients have sepsis syndrome or serious life-threatening infections, such as necrotizing fasciitis, and are always
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
*Corresponding author. Tel: +1-808-432-7848; Fax: +1-808-432-8141; E-mail: [email protected]
Dow
nloaded from https://academ
ic.oup.com/jac/article/52/suppl_1/i3/2473489 by guest on 11 January 2022

L. J. Eron et al.
i4
admitted, often to the intensive care unit or a critical care facility.Many class 4 patients will require surgical intervention. Once class 4patients are stabilized, they may also be candidates for OPAT or oraltherapy.9 Examples of cases from each of these classes are presentedin Figure 1, and the treatment pathways are summarized in Figure 2.
This manuscript focuses on the management and treatment ofpatients with class 2 and 3 SSTIs.
Microbiology
The majority of SSTIs are caused by aerobic Gram-positive cocci,specifically Staphylococcus aureus and streptococci. In specificclinical or epidemiological circumstances, a number of other infec-tious agents also cause infection (Table 2).13 Owing to the difficultiesof isolating organisms from cellulitis cases, most of which are causedby streptococci, these agents may be under-represented in publisheddata.
Streptococci can be classified into several groups; those causingSSTIs are predominantly of groups A and B. Group A streptococciare particularly associated with necrotizing fasciitis, while group Bstreptococci are often the causative agents of infections in diabeticpatients.
Necrotizing soft tissue infections and wounds due to human bitesare more often caused by a mixture of aerobic and anaerobic micro-organisms; in the case of animal bite wounds, these are caused mostfrequently by Pasteurella multocida and rarely by Capnocyto-phaga.13 Vibrio vulnificus infections, acquired from sea water, oftenoccur in patients with cirrhosis or other deficiencies.14 Pseudomonasaeruginosa is often isolated from lower extremity infections,13 par-ticularly in patients who sustain nail puncture injuries of the plantarsurfaces of their feet, but may also be seen in patients with comorbidi-ties, such as peripheral vascular disease, chronic renal insufficiencyor diabetes. P. aeruginosa infection is often associated with preced-ing hydrotherapy. Synergic gangrene in diabetic patients is causedby polymicrobial flora, including S. aureus, group B streptococci,anaerobes and Gram-negative bacilli.
Decision point 1: assessment, classification and admission decision
The first decision point is whether or not to hospitalize a patient withan SSTI. Financially, this is by far the most important decision. Itdepends largely on the severity of the illness at presentation and the
Table 1. Eron9 classification system for patients with SSTIs
Class Patient criteria
1 afebrile and healthy, other than cellulitis2 febrile and ill appearing, but no unstable comorbidities3 toxic appearance, or at least one unstable comorbidity, or a limb-threatening infection4 sepsis syndrome or life-threatening infection, e.g. necrotizing fasciitis
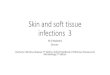
Figure 1. Examples of typical cellulitis case presentations according to class. Class 1: (a) Carbuncle. A 48-year-old man with no history of trauma developed a swelling in his lower leg over a 24 h period. He otherwise felt well and his temperaturewas 37.3°C (99.1°F). This is a class 1 patient. He was successfully treated with five days of oral dicloxacillin. (b) Infected insect bite. A 16-year-old boy presented 5days after an insect bite. Immediately after the bite there was ∼1 cm of erythema and the area was pruritic. Now the area is swollen and tender with lymphangitic streak-ing. There are no systemic signs or symptoms of infection. This class 1 case can be treated with oral outpatient antibiotic therapy active against aerobic Gram-positivecocci.Class 2: (c) Erysipelas. A 72-year-old man presented with a swollen leg for the past 4 days. He has been on cefalexin for 3 days with continued worsening of the infec-tion. His temperature is 39.2°C (102.6 °F), blood pressure is 100/70 mm Hg (normally 130/85 mm Hg), heart rate 120 beats/min. Laboratory tests showed a white bloodcell count of 23 000 cells/mm3; the haematocrit, platelet count, renal function and other tests were within normal limits. This is a class 2 patient. Because of the severityof the infection and failure to respond to oral antibiotic therapy, he could be managed on OPAT following an observation period in the hospital. A skin aspirationculture of the leading edge of his cellulitis was sterile, but there was a 4-fold rise in convalescent titres of his streptococcal DNAase B antibodies, suggesting group Astreptococci as the causative organism. (d) Leg wound. A 23-year-old woman with a history of substance abuse who presented about 30 hours after sustaining an injuryto her right leg. No care has been provided to the wound. Her entire lower leg was oedematous with erythema from mid calf to approximately 8 cm above the knee, andshe had a fever of 38.7°C (101.6 °F). This class 2 patient was discharged on OPAT after drainage of her abscess. (e) Recurrent cellulitis. An 82-year-old diabeticwoman with chronic venous stasis and recurrent cellulitis of the lower extremities presented with a fever, increased erythema and bullae on the lower extremities. Herdiabetes is well controlled and she is eating. Because of her systemic signs and co-morbidities, she is a class 2 patient. She was discharged to stay with her family onOPAT with compressive dressings covering her infected areas, with follow-up scheduled in 3 days.Class 3: (f) Haemorrhagic bullae. A 34-year-old man sustained a bite to his index and middle finger while playing with a dog. On presentation, he was stable and hadhaemorrhagic bullae on his index finger. Laboratory tests revealed leucocytosis with a left shift, evidence of disseminated intravascular coagulation, elevated creatinekinase levels, and abnormal liver function studies. Blood cultures were later positive for Capnocytophaga canimorsus. He has a severe bacteraemic cellulitis andshould be hospitalized for observation of his Class 3 sepsis syndrome. (g) Diabetic foot infection. This 62-year-old man with diabetes, peripheral neuropathy and per-ipheral vascular disease, stepped on a tack one week previously. He has had increased swelling of his foot for the last 5 days. His temperature is 38.3°C (101 °F), he wasmildly tachycardic but normotensive, and he has no palpable foot pulses. His white blood cell count was 23 000 cells/mm3, and his blood glucose was 450 mg/dL, butother blood tests were normal. This is a class 3 patient who needs hospitalization for surgical debridement, blood sugar control, and vascular remediation. His deepwound tissue specimens grew S. aureus and group B streptococci.Class 4: (h) Necrotizing fasciitis. A 45-year-old man with diabetes presented with a painful, swollen foot that began 3 days ago several days after stubbing his toe. Hecomplained of pain in his foot and was disoriented. His temperature was 39.9°C (103.8°F), he is hypotensive and tachycardic, his white blood cell count was 30 300cells/mm3, his platelet count was 70 000 platelets/mm3, and his creatinine was 2.4 mg/dL. This is a class 4 patient who needs to be admitted to the hospital, probably toan ICU. Cultures of his foot grew only group A streptococci.
Dow
nloaded from https://academ
ic.oup.com/jac/article/52/suppl_1/i3/2473489 by guest on 11 January 2022

Managing skin and soft tissue infections
i5
Dow
nloaded from https://academ
ic.oup.com/jac/article/52/suppl_1/i3/2473489 by guest on 11 January 2022

L. J. Eron et al.
i6
likelihood of disease progression. These factors are assessed on thebasis of the history, the presence of comorbidities, the physicalexamination, and the results of laboratory studies and other tests.15
This decision should also consider the patient’s ability to understandtheir disease and comply with instructions, the amount of supportthey can expect at home from friends or family, their ability to returnfor outpatient visits, and the availability of home nursing services.
Economic considerations may also influence the admissiondecision. In the UK, for example, SSTIs account for up to 10% ofadmissions to infection units and the mean length of hospital stay is5 days. This represents a considerable occupancy of the unit’s beds
and generates substantial costs.16 Furthermore, some data suggestthat hospitalization may have other adverse consequences. Patientswith community-acquired pneumonia treated as outpatients hadsimilar clinical outcomes, yet returned to normal daily activitiesmuch sooner, than patients with similar severity of disease who werehospitalized (8 versus 25 days; P = 0.0001).11
History
Clinicians should particularly seek concomitant medical conditionsthat may predict rapid disease progression or poor response to treat-ment. These include advanced age, chronic liver disease, chronicrenal disease, asplenia, alcohol abuse or the use of an antimicrobial inthe previous 2 weeks.13,17–19 The risk of a poor outcome for chronicwounds, such as lower extremity ulcers, is greater in patients withreduced arterial perfusion or neuropathy. Chronic venous insuffi-ciency, diabetes, obesity, malnutrition, advanced age and compro-mised immune function have also been reported to delay woundhealing.13
Information about underlying illnesses and vocational or avoca-tional exposure may also help to determine the causative agent andthus the appropriate treatment (Table 2). In immunocompromisedpatients, Gram-negative bacteria and atypical mycobacteria are seenat higher incidences than in the general population.20 Other factors,e.g. exposure to salt water, may predispose to less common infectiousorganisms, as listed in Table 2. Clinicians should inquire aboutfactors such as hobbies, job duties and travel, because they may influ-ence the aetiological agents, and thus the decision whether or not toculture the wound and the choice of an empirical antimicrobial regimen.
The use of medications by the patient should also be considered.Recent antimicrobial therapy can alter the aetiological agents or theirantimicrobial susceptibilities. High-dose corticosteroids can increasethe risk, and alter the manifestations, of SSTIs. Tumour necrosisFigure 2. Algorithm for managing cellulitis: site of care and route of therapy.
Table 2. Risk factors for specific pathogens causing SSTIs13,119
Risk factor Characteristic pathogens
Diabetes S. aureus, group B streptococci, anaerobes, Gram-negative bacilli
Cirrhosis Campylobacter fetus, Klebsiella pneumoniae, Escherichia coli, Capnocytophaga canimorsus, other Gram-negative bacilli, V. vulnificus
Neutropenia P. aeruginosa
Bite woundshuman oral flora (Eikenella corrodens)cat P. multocidadog C. canimorsus, P. multocidarat Streptobacillus moniliformis
Animal contact Campylobacter spp.
Reptile contact Salmonella spp.
Hot tub exposure/loofah sponges P. aeruginosa
Fresh water exposure Aeromonas hydrophila
Sea (or fish tank) water exposure V. vulnificus, Mycobacterium marinum
Drug abuseintravenous MRSA, P. aeruginosasubcutaneous anaerobes, especially Eikenella corrodens
Dow
nloaded from https://academ
ic.oup.com/jac/article/52/suppl_1/i3/2473489 by guest on 11 January 2022

Managing skin and soft tissue infections
i7
factor inhibitors, such as infliximab, are associated with the reactiva-tion of infections such as tuberculosis.21,22
Physical examination
The physical examination helps determine the severity of the infec-tion. Local signs of serious SSTI include bullae, haemorrhagiclesions, and anaesthesia or pain out of proportion to the objectivefindings. Fluctuance suggests an abscess that may require drainage.Crepitus should raise concerns about a gas-forming infection thatmay require surgical intervention. With infections of extremities(especially the foot), severe ischaemia may mask erythema, and neu-ropathy may reduce tenderness.
Systemic manifestations suggest a more severe infection. Specificfeatures identified as predictors of outcome include hypotension,tachycardia, body temperature <35°C or >40°C, and confusion ordecreased levels of consciousness.15,17,19 The presence of two or moreof these factors is associated with particularly poor outcome orresponse to treatment.17
Extreme pain or tenderness, especially out of proportion to object-ive findings, may be a sign of necrotizing infection.23 Anaesthesiaaround a wound may indicate tissue necrosis. The size and location ofthe lesion influence the severity, need for observation and surgicalconsultation, and thus the hospitalization decision; lesions on thethighs, digits, head or genitals are more likely to be serious. Largeareas of infection (e.g. more than several centimetres) may warrantadmission, especially in diabetic patients. Lymphangitis, or cellulitiswith a raised indurated border (as in erysipelas), is usually caused bya more superficial group A streptococcus infection, and hospital-ization may be unnecessary. A fetid odour suggests anaerobic infec-tion, while greenish exudate is typical of Pseudomonas infection.
Laboratory and ancillary studies
A complete blood count (white blood cell count and differential,haematocrit, platelet count) may assist in assessing the severity of ill-ness. Marked leucocytosis (or leucopenia), an extreme left shift in thewhite cell differential, new onset anaemia (caused by haemolysis) orthrombocytopenia may suggest sepsis syndrome. Elevated levels ofblood urea nitrogen and creatinine suggest intravascular volumedepletion or renal failure, while elevated creatine kinase levels mayindicate myonecrosis caused by necrotizing fasciitis or a compart-ment syndrome.24–26 Serological tests (streptozyme, anti-DNase B,anti-hyaluronidase) for streptococcal infection are generally not help-ful except as paired acute and convalescent titres. Certain cases maywarrant additional tests, such as X-rays (to look for foreign bodies orgas in the tissues), ultrasound or computed tomography (to look fordrainable collections), or Doppler vascular exam (to rule out deepvenous thrombosis or arterial insufficiency). Magnetic resonanceimaging is useful to investigate suspected fasciitis or osteomyelitis.Radionuclide scans are generally not helpful in the acute situation,because they lack specificity.
Obtaining culture specimens
There has been considerable debate about the benefits, timing andmethods used to sample a lesion for microbiological analysis. Culturingthe skin in cases of cellulitis infrequently yields a pathogen. Obtainingspecimens from other wounds for Gram-stained smear and culture isalmost always useful, especially if there is reason to believe that thepathogen is methicillin-resistant S. aureus (MRSA).13 The likelihood
of infection with MRSA depends largely on the local prevalence andprevious antibiotic use by the patient.27,28 Local antibiotic resistancepatterns should be considered when deciding whether to obtain speci-mens for culture and sensitivity: the lower the prevalence of resistantstrains, the less the need to culture.
For cultures, tissue specimens are generally preferable to swabs,especially for open wounds. Depending on the type of wound, culturesamples may be obtained by tissue biopsy or curettage (scraping witha dermal curette or scalpel blade) of ulcerated areas. If there is noopen wound, needle aspiration of fluid from the skin at the leadingedge of infection may be helpful.13 Collection of an adequate aspirateis facilitated by using a large-bore needle (18 gauge) and drawingair into the barrel of the syringe before aspiration to later help expelany tissue fluid collected.29 Blood cultures should be obtained frompatients with a severe infection or sepsis syndrome, although theyield of a pathogen may be <10%.30–32 Anaerobes are often difficultto culture, and require special handling (such as the use of anaerobictransport media). However, Gram-stained specimens may suggesttheir presence when analysed in conjunction with culture results.Anaerobes should be suspected if the wound is foul smelling ornecrotic, even if they have not been recovered on culture.13
Observation status
In some hospitals, low-risk patients are treated initially in an obser-vation unit, or are observed in the emergency department. Thisallows time (usually up to 24 h) to treat patients and observe theirresponse to therapy. If a patient appears to be responding, then theymay be treated as an outpatient, either at home or in an infusioncentre. Patients whose symptoms do not improve are admitted forinpatient treatment. Observation units should follow standardizedtreatment protocols to maintain good clinical outcomes, as well aspatient safety and satisfaction.33
SSTIs are among the most frequently treated conditions in anobservation setting. In one published study, SSTI was the third mostcommon diagnosis (8% of patients), behind chest pain and asthma.34
In this study, 85% of patients were discharged home from the obser-vation unit within 23 h.34 Similar results were seen in another study,in which 73% of patients were discharged from the observation unit,thus avoiding the need for admission.35 The average length of stay inthe observation unit was about 15 h.35
Good candidates for observation status are patients who are likelyto respond to empirical therapy, are expected to require a short stay,and have a low likelihood of infection with resistant organisms. Class2 patients, who are moderately ill, often meet these criteria. Someclass 1 patients may be suitable for observation, especially if theyhave a non-supportive home environment or require pain control.Although most class 3 patients require hospitalization, some (e.g. thosewho are not systemically toxic) may be adequately treated in anobservation unit.
Circumstances that would require hospitalization rather than anobservational unit include the presence of tissue necrosis, sepsis,severe pain, altered mental status, immunocompromise (e.g. AIDS,cancer), or liver or renal failure.34 Bite wounds and SSTIs on thehands, periorbital area, joints, scrotum and neck, which require carefulobservation or respond poorly to treatment, are not usually appro-priate in an observation unit.34 Successfully managing patients in anobservation unit requires early consultation with primary care phys-icians and specialists, as well as with social services and visitingnurse associations.
Dow
nloaded from https://academ
ic.oup.com/jac/article/52/suppl_1/i3/2473489 by guest on 11 January 2022

L. J. Eron et al.
i8
Indications for referral
Certain cases require not only hospitalization, but also urgent referralfor subspecialty consultation. Limb-threatening diabetic foot infec-tions are best treated by a multidisciplinary team, including infec-tious disease, podiatry and/or surgical (e.g. orthopaedic, vascular)specialists.13,36,37 Necrotizing fasciitis, synergic gangrene and some-times osteomyelitis or septic arthritis require prompt surgical consul-tation. An infectious disease consultant may assist in discussingthe choice of antimicrobial agents, adjunctive therapies and generalpatient care.
Decision point 2: initial antimicrobial selection
Once the severity of a patient’s infection has been classified and adecision has been made about admission, the next step is to choosethe initial antimicrobial regimen. Considerations in selecting anappropriate antimicrobial should include the spectrum of its anti-microbial activity, the route of delivery, antimicrobial resistanceissues, side effects profile, drug interaction potential, patient allergies,pharmacodynamics and cost.
Route and timing of administration
The choice between oral and parenteral therapy is governed by manyof the same factors that determine the class of the infection: thepatient’s clinical presentation, the results of laboratory analysesand the presence of comorbidities. There are, however, additionalconsiderations.
Many physicians prefer to prescribe oral therapy because of itsgreater patient convenience. Moreover, some studies have shownthat clinical outcomes with oral therapy are not statistically worsethan with parenteral therapy. However, such studies have not beensufficiently powered to show significant differences, nor have theystratified the patients according to disease severity. Furthermore,data from the OPAT Outcomes Registry (A. D. Tice & D. Nathwani,unpublished data) indicate that 22% of patients who were started onparenteral antimicrobial therapy had been treated initially with oral
antimicrobials and were switched because of treatment failure.Parenteral therapy is more likely to result rapidly in elevated serum(and thus tissue) antimicrobial levels than oral therapy, which isparticularly important in seriously ill patients. Parenteral therapy isalso preferred in patients for whom either gastrointestinal problems(e.g. nausea, vomiting, gastroparesis) or medication compliance is anissue.
In general, outpatient oral therapy is most appropriate in the treat-ment of class 1 patients (Table 3), who are less likely to be infectedwith unusual or drug-resistant organisms. Some class 2 patients mayrespond well to oral therapy, but there is no reliable way to predictwhich ones. Therefore, parenteral therapy should be preferred, atleast initially, for class 2 patients. In addition, most patients withmore severe cases of SSTI (classes 3 and 4) require at least initialparenteral therapy. Parenteral antimicrobial therapy should be initiatedin the hospital’s emergency department, observation unit or infusionclinic.
The first dose of antimicrobial is considered to be the mostimportant one and should be administered without delay as soon asculture specimens are obtained.38 Studies on patients with community-acquired pneumonia have shown that prompt antimicrobial adminis-tration reduces mortality, shortens the hospital stay and reduces costs.Substantial clinical benefits can result from saving just a few hours intime to drug delivery.38,39 For patients in whom early or immediatedischarge is anticipated, an initial dose of parenteral therapy with anantimicrobial that has an appropriate spectrum of activity against thecommonly encountered organisms and a long half-life that provides24 h coverage is ideal.40
Dosing considerations
Appropriate antimicrobial dosing requires an understanding ofpharmacokinetics and pharmacodynamics. It is largely related to thedrug concentration in tissues and body fluids and the MIC for theinfecting organism. Dosing is also influenced by patient character-istics, such as body weight and renal or hepatic function. The mostimportant factor in choosing an antimicrobial is the drug’s activityagainst the targeted organism, but it must achieve levels at the
Table 3. Recommended drug therapy for outpatient oral treatment of uncomplicated SSTIs (excluding MRSA infections)
ClassRecommended antimicrobial agents
Alternative antimicrobial agents Comments
Class 1 dicloxacillin–flucloxacillin taste or gastrointestinal disturbances
cefalexin concurrent treatment with acid-suppressive therapy may cause failures
benzyl penicillin (or phenoxymethylpenicillin)
for infection likely caused only by streptococci
co-amoxiclav more expensive; diarrhoea often a problem; good choice for bite wounds; covers most anaerobes
macrolides may be used in patients with penicillin allergies; however, resistance issues must be considered
tetracyclines minocycline may be useful for some community-acquired MRSA strains
clindamycin for patients with severe penicillin allergies; covers anaerobes and some community-acquired MRSA
Dow
nloaded from https://academ
ic.oup.com/jac/article/52/suppl_1/i3/2473489 by guest on 11 January 2022

Managing skin and soft tissue infections
i9
infected site exceeding the MIC for the infecting organism. Anti-microbial concentrations that kill the infecting organisms also pre-vent the selection of resistant mutants.41–43
Tissue penetration of drugs has been measured in blister fluids andin interstitial fluids of muscle and fat using microdialysis techniques.The best predictor of the achievable drug concentration in theseperipheral compartments appears to be free-drug concentration inserum. For most drugs, penetration into blister or interstitial fluidis delayed, and elimination from this compartment is slower thanfrom the serum. The higher serum concentrations achieved withparenteral drugs ensures improved penetration compared with mostoral agents.44–59 In patients with impaired arterial supply, e.g. withdiabetic limb infections, antimicrobial penetration is a particular prob-lem.60 Fluoroquinolones, which have high bioavailability and tissuepenetration, are therefore often used in such cases.
All drugs require three to five half-lives to reach their steady state.Consideration should be given to the use of a loading dose (abouttwice the usual dose) for oral drugs with a long half-life in order torapidly achieve serum levels above the MIC for the pathogen.Although azithromycin is the only oral antimicrobial with a loadingdose approved by the US Food and Drug Administration, other drugsmay be administered this way. It is also prudent to use a loading dosewhen treating a relatively resistant organism. A loading dose shouldbe avoided if it is likely to cause nausea or vomiting. In such a case, orwith agents with low bioavailability, a parenteral loading dose maybe appropriate with a subsequent switch to oral therapy.
Drug spectrum and activity
The spectrum of the antimicrobial chosen for initial therapy must bebroad enough to cover the suspected infecting organisms, but notoverly broad such that it also kills normal colonizing flora. In com-munities where the rate of antimicrobial resistance is high, coverage
may need to account for strains with reduced antimicrobial suscep-tibility, such as MRSA. Because most cases of SSTI are caused byβ-haemolytic streptococci and/or S. aureus, appropriate choices forempirical therapy include cephalosporins, semi-synthetic penicillinsand clindamycin, or macrolides in penicillin-allergic patients.13,15
Specific drug recommendations for SSTI classes 2 and 3 are shown inTable 4.
For class 2 patients, ceftriaxone is commonly prescribed becauseof its appropriate antimicrobial spectrum and favourable pharmaco-kinetics, which allow once-daily infusion.3,61,62 Moreover, adverseeffects are relatively infrequent.61 Ertapenem is a new once-dailycarbapenem, for which limited clinical data are available. Its spec-trum may be appropriate for complicated polymicrobial skin infec-tions, such as diabetic foot infections or pressure ulcers, because itis active against most aerobic Gram-positive and Gram-negativepathogens, and also anaerobes. Unlike other carbapenems, it is noteffective against Pseudomonas species and has decreased activityagainst staphylococci.63 Nafcillin and cefazolin each have a morelimited spectrum but excellent activity against S. aureus (non-MRSAstrains) and streptococci. Nafcillin may cause phlebitis, and becauseit must be administered four times daily, it is limited to hospitalizedpatients. While cefazolin is normally administered three times daily,some studies have shown that it can be given once-daily when com-bined with probenecid to prolong its serum half-life.62,64,65 Probene-cid may cause various adverse events and should therefore be usedwith caution. Cefazolin and semi-synthetic penicillins are appropri-ate choices for class 3 patients. It is advisable to treat patients whoare expected to be discharged early on OPAT with the same drugduring their hospital stay. For patients in an observation unit, anti-microbials that may be administered once daily are particularly useful.
If MRSA infection is suspected, several points must be considered(Table 5). First, community-acquired MRSA is typically susceptibleto several classes of antimicrobials [clindamycin, quinolones, tetra-
Table 4. Recommended parenteral antimicrobial therapy for class 2 and 3 SSTIs (excluding MRSA infections)
For additional information and special cases, see text.
ClassRecommended antimicrobial agents
Alternative antimicrobial agents Comments
Class 2 ceftriaxone appropriate range of antimicrobial activity, once-daily dosing
cefazolin ± probenecid probenecid may be associated with adverse events
flucloxacillin ± benzyl penicillin
taste or gastrointestinal disturbances
clindamycin for patients allergic to penicillin and for sensitive community-acquired MRSA strains
Class 3 cefazolin
semi-synthetic penicillins phlebitis may be a problem
flucloxacillin ± benzyl penicillin taste or gastrointestinal disturbances may be a problem
ceftriaxone ceftriaxone is recommended for class 3 patients on observation status who are subsequently admitted (for a short period of time) with the expectation that OPAT will be utilized upon discharge
clindamycin for patients allergic to penicillin and for sensitive community-acquired MRSA strains
Dow
nloaded from https://academ
ic.oup.com/jac/article/52/suppl_1/i3/2473489 by guest on 11 January 2022

L. J. Eron et al.
i10
cyclines and trimethoprim–sulfamethoxazole (co-trimoxazole)] towhich hospital-acquired MRSA strains are not.27 Because of itspotentially toxic side effects and the need to not overuse the drug,vancomycin should be reserved for MRSA acquired in health carefacilities, or for infections associated with dialysis or intravenousdrug use. Linezolid is virtually 100% bioavailable orally, can also begiven parenterally and is highly active against MRSA. It has beenshown to be effective in treating complicated skin infections, includingdiabetic foot infections.66,67 However, linezolid is expensive, andhas been associated with haematological toxicity, particularly whengiven for more than 2 weeks.68,69
In patients who report serious allergies (e.g. hives or anaphylaxis)with β-lactam antimicrobials, clindamycin is an appropriate choice.For those with only a non-specific maculopapular eruption due topenicillin, cephalosporins can usually be used safely, provided thatthe patient is observed for a few hours thereafter. Fluoroquinolones(especially agents more active against Gram-positive cocci) havebeen used for SSTIs, but we discourage using them for this indicationbecause of the potential for the development of resistance, exceptperhaps in diabetic foot infections.70 They may be appropriate forpatients with a penicillin allergy who cannot tolerate clindamycin.
In class 4 patients with necrotizing fasciitis or sepsis syndrome,urgent surgical consultation and follow-up is paramount. Theseinfections usually require debridement, and occasionally amputation.Because they can be caused by a variety of pathogens, and there is notime to correct errors, broad-spectrum antimicrobial therapy shouldbe used initially in most cases. Depending on the type of infection, thepatient may require coverage for group A streptococci only (necrotizingfasciitis) or for polymicrobial flora, including S. aureus, group Bstreptococci, anaerobes and Gram-negative bacilli (synergic gangrenein diabetic patients). Clindamycin is the drug of choice in most casescaused by group A streptococci.71 When necrotizing fasciitis is com-plicated by toxic shock syndrome, many clinicians use intravenousgamma globulin to neutralize the causative streptococcal pyrogenicexotoxin.72,73 Intravenous fluids and pressors are usually necessary,and drotrecogin alpha (activated) may be useful for severe sepsis
syndrome.74 For some anaerobic infections, especially those causedby Clostridium perfringens, hyperbaric oxygen may be useful.75,76
Adjunctive procedures and medications
Patients with necrotic tissue or an undrained abscess should be seenby a surgeon. Compression dressings can be useful for SSTIs compli-cated by chronic venous insufficiency.77 Reducing oedema helpsresolve the infection and prevent recurrences. In patients with a limbinfection and peripheral vascular disease, revascularization pro-cedures may be necessary.78
In patients with SSTI on therapy with antimicrobials, concomitantcorticosteroids or non-steroidal anti-inflammatory drugs (NSAIDs)may shorten the intensity and duration of inflammatory signs andfacilitate earlier discharge. A randomized study of 112 patients witherysipelas found that adding oral prednisolone to penicillin therapysignificantly shortened the time to complete resolution of fever,as well as the duration of intravenous therapy and hospital stay (adifference of 1 day versus placebo for each measure).79 There wasalso a non-significant trend towards fewer relapses of SSTIs in theprednisolone-treated group during a 1 year follow-up.80 Becausesteroids (and to a lesser extent NSAIDs) are associated with variousadverse effects, and may mask signs of worsening infection, furtherdata are required before their routine use can be recommended. Simi-larly, other adjunctive therapies, such as hyperbaric oxygen andgranulocyte colony-stimulating factor,76,81,82 have shown promise,but these expensive therapies cannot be recommended routinely untilfurther, properly conducted, supportive studies are available.
Resistance patterns among SSTI pathogens
Community-acquired MRSA is now the greatest antimicrobial prob-lem in treating SSTIs. Although still infrequent in most locations, theprevalence is increasing in some areas of the world.27,83 The averageprevalence of methicillin resistance among community-acquiredS. aureus isolated in the USA is at least 20%, and growing. Some
Table 5. Recommended parenteral therapy for class 2 and 3 SSTIs caused by MRSA
For additional information and special cases, see text.
Recommended antimicrobial agent
Alternative antimicrobial agents Comments
Clindamycin suitable for certain community-acquired MRSA strains
Daptomycin once daily; iv only; highly bactericidal
Linezolid suitable for hospital- or nursing-home-acquired MRSA; oral bioavailability almost 100%
Teicoplanin once-daily iv or im administration; loading doses may be necessary for severe infections
Vancomycin appropriate for hospital- or nursing home-acquired MRSA
quinupristin + dalfopristin must be administered with a peripherally inserted central catheter line, twice daily
fusidic acid + rifampicin for class 1 patients
minocycline paucity of data and experience; for class 1 patients
rifampicin + … only used in combination with other drugs
Dow
nloaded from https://academ
ic.oup.com/jac/article/52/suppl_1/i3/2473489 by guest on 11 January 2022

Managing skin and soft tissue infections
i11
centres have reported rates as high as 50%.27,83 Clinicians should beaware of the local community and hospital resistance trends, andconsider the presence of risk factors associated with community-acquired MRSA (Table 6).22,79 MRSA has been reported in somecases to be disseminated from the hospital to the community.84
Macrolide resistance has risen rapidly among group A and Bstreptococci in the last few years, but they remain susceptible topenicillins and cephalosporins.85–87 On the other hand, staphylococcihave developed several types of resistance to β-lactams, glyco-peptides and other antimicrobials.27,83 Vancomycin should not beused empirically, except in the most seriously ill patients or whenMRSA rates are high. Clindamycin is highly effective against moststaphylococcal or streptococcal strains. However, it should not beused alone against strains that are resistant to erythromycin, even ifthey appear to be clindamycin susceptible, because this may induceresistance.88–90 Reports of increasing resistance of MRSA strains toclindamycin have further complicated the antimicrobial selectionprocess.27 Where available, teicoplanin is a useful alternative tovancomycin for treating moderate to severe SSTIs due to MRSAinfection. It offers the advantage of once daily intravenous or intra-muscular therapy. Loading doses may be required in severe infec-tions.91 Agents active against MRSA may be associated with toxicity(vancomycin) or high costs (linezolid, quinupristin/dalfopristin).Thus, there is renewed interest in treating MRSA with older anti-microbials, such as minocycline, co-trimoxazole or doxycycline.92
In a randomized double-blind trial of 101 intravenous drug userswith S. aureus infections, co-trimoxazole showed similar efficacy tovancomycin against MRSA.93 Minocycline has also been shown tobe effective in treating MRSA,94,95 but extensive studies with mino-cycline monotherapy have not been reported.
Diabetic foot infections
Foot ulcers in diabetic patients are usually caused by sensory andmotor neuropathy and consequent excessive pressure or trauma.These ulcers often become infected, especially when complicated byarterial insufficiency. SSTIs can then extend to the skin surroundingthe infected ulcer, to deep spaces, or to bone or joint. Most acuteinfections in patients not recently treated with antimicrobials arecaused by S. aureus and/or β-haemolytic streptococci. In these cases,relatively narrow-spectrum therapy is sufficient.96 However, in pre-viously treated patients, or those with chronic or necrotic wounds,polymicrobial infections are more likely and require broad-spectrumantimicrobials (Table 7). Most cases also require adjunctive therapies,such as pressure relief, wound debridement or drainage, control ofhyperglycaemia and vascular evaluation.13,97 Granulocyte colony-stimulating factor and hyperbaric oxygen may be useful in selectedpatients. Vacuum dressings may help the healing of uninfectedwounds that do not show vascular compromise, but data on theirsafety or efficacy in treating infections are not yet available.
Recurrent infections
Recurrent bouts of SSTI are most commonly seen in patients withchronic lymphoedema, e.g. in those who have undergone saphenousvenectomy for coronary artery bypass grafting, pelvic surgery orirradiation, lymphadenectomy, mastectomy, or node dissection.98
Microbiologically, it is important to distinguish between persistentinfection (i.e. not successfully eradicated), and a new infection due toeither the same organism (relapse) or a different one (reinfection).Reducing or eliminating the predisposing conditions (e.g. oedema,dermatophytosis) is crucial to preventing relapse. Recurrent skininfection caused by S. aureus may be prevented by eradicating anteriornasal carriage with nasal mupirocin ointment.99 Recurrent SSTI isoften caused by β-haemolytic streptococci (groups A, B, C or G);long-term antimicrobial prophylaxis may reduce these recurrences.100
In patients with recurrent leg cellulitis, the entry portal for bacteriamay be sites of toe dermatophytosis.101 Special attention should bepaid to eradicating any coexistent tinea pedis.
Safety and tolerability
Although most antimicrobials are safe and well tolerated when givenin proper dosage, adverse effects occur and may occasionally beserious. In patients with a history of drug allergies, it is usually safestto avoid using those agents. In patients with a questionable historyof penicillin allergy, those at risk can usually be identified by ante-cedent penicillin skin testing with penicilloyl polylysine.102,103 Cross-reactivity between penicillins and cephalosporins is low (<5%), butcephalosporins should be avoided when a previous penicillinreaction was severe (e.g. anaphylaxis, laryngeal oedema or hives).103
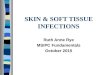
Data on antimicrobial side effects have been gathered by theOPAT Outcomes Registry from 44 centres in the USA, Canada, Italyand the UK on >14 000 courses of outpatient antimicrobial therapy.The most common antimicrobial used in the OPAT Outcomes Registrynetwork is ceftriaxone (Figure 3).104 In this database, drug discontin-uation due to adverse effects was most common with piperacillin–tazobactam, nafcillin and gentamicin, and least common with ceftri-axone (Figure 4).105 Rash, diarrhoea, nausea/vomiting and fever areamong the most common antimicrobial-related adverse events.
Treating SSTIs with OPAT
OPAT has the potential to greatly reduce costs and improve patientsatisfaction, with outcomes that are equivalent or superior to thoseof inpatient treatment.10–12 In the OPAT Outcomes Registry, SSTIis the most common infection treated, accounting for about 19% ofdiagnoses.104 OPAT, however, remains under-utilized, and could bene-fit many more patients. Its advantages include documented excel-lent clinical and bacteriological outcomes in appropriately selectedpatients, reduced cost and length of stay for hospitalized patients,
Table 6. Factors increasing the likelihood of isolating MRSA in community-acquired SSTIs27,28
Recent antimicrobial therapyRecent hospitalization or health care institutionalizationFrequent device use in the community (e.g. home haemodialysis, intravenous catheters)High rates of MRSA in institution or communityPrevious MRSA colonization
Dow
nloaded from https://academ
ic.oup.com/jac/article/52/suppl_1/i3/2473489 by guest on 11 January 2022

L. J. Eron et al.
i12
potential avoidance of nosocomial infections, improved patient andcaregiver satisfaction, and earlier return to usual daily activities.10,12,106
In the OPAT Outcomes Registry, 22% of patients are started onOPAT after oral therapy, the two most common reasons for this beingfailure of the patient to tolerate oral medication and progression of theinfection despite the patient receiving oral therapy for several days.The reasons for the lack of efficacy of oral treatment may be inadequatedrug levels due to dosing, absorption or compliance problems.
Class 2 patients, who are moderately ill but do not require hospital-ization, are ideal candidates for OPAT. Other candidates includeclass 3 patients for whom continued intravenous antimicrobial therapyis considered useful following a short stay in hospital or on obser-vation status. For OPAT to succeed, there must be adequate homesupport, and an understanding of, and willingness to follow, theinstructions. The patient must be able to return to the hospital or infu-sion centre when necessary, or otherwise access home health care orvisiting nurse services.
In hospitals or emergency departments without an OPAT system,patients can be instructed to return as frequently as necessary forcontinued injections/infusions. Alternatively, arrangements may bemade for their own physicians to administer the antimicrobials in
the office. In our experience, this is most easily accomplished witha once-daily drug that is well tolerated and can be administered byeither an intramuscular or intravenous route.
Decision point 3: antimicrobial switch
Limited research and much clinical experience on the timing of theswitch from parenteral to oral antimicrobial therapy suggest thatmost patients with uncomplicated SSTI may be safely switched tooral agents after 3–4 days.10,107–109 The timing is guided by thepatients’ response to parenteral antimicrobials, the culture andsusceptibility results, and the patients’ readiness for oral therapy.Therefore, each case needs to be assessed on a daily basis. Signs andsymptoms of infection should be improving, with decreases inerythema and induration. Skin wrinkling at the infected site suggestsreduced swelling. Body temperature and white blood cell count anddifferential should show an improving trend, and comorbiditiesshould have stabilized.
A randomized, double-blind trial of hospitalized patients withcomplicated SSTIs demonstrated that switching from intravenous to
Table 7. Recommended parenteral therapy for class 2 and class 3 diabetic limb infections
For additional information, see text.Only add anti-anaerobic agents when anaerobic infection is suspected or proven.
ClassRecommended antimicrobial agents
Alternative antimicrobial agents Comments
Class 2 ceftriaxone ± metronidazole add metronidazole if anaerobic infection suspected orconfirmed
fluoroquinolone + clindamycin broad spectrum coverage with easy oral switch
co-trimoxazole ± metronidazole
not recommended for observation patients; add metronidazoleif anaerobic infection suspected or confirmed
fluoroquinolone ± metronidazole
oral drugs with good bioavailability; can be givenintravenously if the patient is vomiting; Staphylococcus and Streptococcus coverage may be suboptimal
co-amoxiclav widely used drug with proven efficacy in clinical trials
ertapenem limited data available to date
fusidic acid used in some countries due to perceived (but unconfirmed) high penetration into tissue
Class 3 ceftriaxone ± metronidazole
fluoroquinolone + clindamycin
meropenem
piperacillin/tazobactam
semi-synthetic penicillins+ metronidazole
must be administered multiple times daily; appropriate forcommunity-acquired infections not previously treated withantimicrobial agents
cefepime ± metronidazole use for Pseudomonas infections
linezolid ± aztreonam linezolid is a useful alternative to vancomycin in the treatmentof MRSA infection; aztreonam is a useful alternative to β-lactams in the treatment of Gram-negative infections
vancomycin ± ceftriaxone when MRSA infection suspected or confirmed
Dow
nloaded from https://academ
ic.oup.com/jac/article/52/suppl_1/i3/2473489 by guest on 11 January 2022

Managing skin and soft tissue infections
i13
oral linezolid (n = 400) or from intravenous oxacillin to oral dicloxa-cillin (n = 419) resulted in satisfactory clinical cure rates (70% versus65%, respectively).108 For both regimens, the mean duration ofparenteral therapy was 4.7 days, and the total duration of therapy was13.4 days.108 Another study evaluated the oral switch in 40 hospitalizedpatients with SSTIs. The most commonly used intravenous drugswere ampicillin–sulbactam, cefazolin and ticarcillin–clavulanate,and the most commonly used oral drugs were cefradine, cipro-floxacin or co-amoxiclav. The mean duration of intravenous therapywas 3 days, and treatment was successful in 95% of cases.109
Patients treated with OPAT using ceftriaxone or cefazolin mayoften be safely switched to oral dicloxacillin or cefalexin after 3–4days to complete their treatment.10 Data from one observational studysuggest that the efficacy of cefalexin may be less than that of othercommonly prescribed antimicrobials.110 Another commonly usedagent for the oral switch is clindamycin, which is available forboth oral and intravenous therapy. In patients with clindamycin-resistant MRSA, therapy with intravenous vancomycin, linezolid orquinupristin–dalfopristin may be switched to oral linezolid, orperhaps co-trimoxazole, with or without rifampicin.
Use of intravenous therapy for longer than 3–4 days does notcorrelate with better outcomes.30 Data from the OPAT OutcomesRegistry support these findings. Moreover, the Registry data indicatethat oral therapy after a prolonged course of OPAT does not signifi-cantly improve outcomes, and may therefore be unnecessary in manypatients (see also Decision point 5). Further studies on the timing ofthe oral switch and the need for oral drugs after initial parenteraltherapy are required.
Decision point 4: discharge
The criteria for discharging hospitalized patients with SSTI parallelthe conditions for switching from parenteral to oral antimicrobials.Although in-hospital observation after discontinuation of intra-venous antimicrobials was previously common, patients can besafely discharged as soon as they discontinue intravenous therapy.111–113
Moreover, by using OPAT, it is possible to discharge patients evenbefore they are switched to oral antimicrobials. In our experience,before discharge, the infected area should be clinically improving,while systemic signs of infection should be resolving and any comor-bidities should be stabilized. Indications that the patient is not readyfor discharge are listed in Table 8.
Many physicians delay discharge until fever and other signs ofinflammation have completely resolved, but this is usually unnecessary.Fever is mediated by cytokines, which may persist, even thoughthe pathogen load is greatly diminished.10 Similarly, erythema mayincrease somewhat in the first day after starting antimicrobial treat-ment before it subsequently recedes. In a separate study of 50 patientswith SSTIs treated with OPAT, almost 50% defervesced within 24 hof initiating antimicrobial therapy, and about 70% did so within 48 h.However, the remaining patients took 48–96 h to become afebrile(L. J. Eron, unpublished results). In a study of 92 patients with SSTIs,the area and intensity of erythema took 3–4 days to decrease by 50%,and the area initially increased in 11% of patients (L. J. Eron, P. King& M. Marineau, unpublished results).
In a case-controlled study of patients hospitalized with SSTIs,community-acquired pneumonia or pyelonephritis, 111 patients who
Figure 3. Antimicrobial agents used most commonly to treat skin and soft tissueinfections, as gathered by the OPAT Outcomes Registry.104 Pip/Tazo, piperacillin–tazobactam.
Figure 4. Percentage of antimicrobial courses terminated early due to adverseevents in the OPAT Outcomes Registry.105 Pip/Tazo, piperacillin–tazobactam.
Table 8. Indications to delay hospital discharge in patients hospitalized with SSTIs
Severe infection (e.g. ischaemic foot, necrotizing fasciitis)Sepsis syndrome (including hypotension) or toxic appearanceUncontrolled infection-related painUncontrolled nausea or vomitingUnstable comorbidities or metabolic parameters (e.g. azotaemia, congestive heart failure, hyperglycaemia)Need for complex wound care, multiple diagnostic or surgical proceduresInadequate home support structure
Dow
nloaded from https://academ
ic.oup.com/jac/article/52/suppl_1/i3/2473489 by guest on 11 January 2022

L. J. Eron et al.
i14
were discharged prior to defervescence were compared with 112patients who were not discharged until defervescence. In the earlydischarge group, the mean length of hospital stay was 1.7 daysshorter, patient satisfaction was significantly greater and patientsreturned to normal daily activities earlier. Furthermore, none of thepatients required readmission.10 In a subsequent study of 92 patientsin the emergency department, discharge was further acceleratedthrough the use of ceftriaxone. In our experience, of patients whoreceived ceftriaxone, 98% were discharged immediately on OPAT,compared with only 39% of patients who received the comparatordrug, cefazolin.
Before discharge, a plan should be established for follow-up carein the outpatient setting. Early discharge can cause considerableanxiety in patients, who may still feel ill, as well as for their familymembers, who may have to learn to administer wound care and intra-venous antimicrobials. The health care team should be prepared tohelp patients and their families cope with these fears, and to managethe challenges of home care.
Decision point 5: antimicrobial discontinuation
The duration of antimicrobial therapy needed for SSTI has not beenwell studied. Therapy may be discontinued upon the resolution ormarked improvement in the clinical signs and symptoms of inflam-mation. Most cases of uncomplicated SSTI can be successfullytreated with 1–2 weeks of therapy, although serious or complicatedcases, such as diabetic foot infections, often require one or twoadditional weeks of treatment. Patients with associated osteomyelitismay require 6 weeks or more of antimicrobial therapy.97 Factors thatsuggest the need for more prolonged antimicrobial therapy are listedin Table 9. Local factors, such as the presence of lymphoedema,chronic venous insufficiency or poor arterial supply to the infectedlimb, may necessitate longer treatment and adjunctive therapies. Thepresence of bacteraemia should be considered in deciding when todiscontinue therapy, but does not in itself indicate that prolongedtreatment is necessary.
Shorter courses of therapy have been shown to be as effective aslonger ones for urinary tract and upper respiratory tract infec-tions.114,115 Moreover, several studies of various infectious diseases(e.g. urinary tract infections, otitis media) have demonstrated that asingle dose of parenteral antimicrobial is sufficient.116,117 However,there are no published data available on the efficacy of short coursesor single doses of antimicrobial therapy in SSTI patients, and furtherstudies are therefore needed.
About 20% of patients with a first episode of SSTI will developsubsequent episodes.17 Therefore, measures should be considered toprevent recurrence. Underlying conditions that predispose to SSTImust be addressed, and patients should be advised of the importanceof proper skin and nail care.17 Topical antifungal agents, topical
steroids and skin lubricants may be warranted in patients withtinea pedis, eczema and dry, cracked skin, respectively.24,100,118
Any oedema related to venous or lymphatic insufficiency shouldbe addressed, e.g. with an Unna boot or compression stocking. Inrare cases of recurrent or recalcitrant infections, long-term anti-microbial prophylaxis or intermittent patient-initiated therapy maybe needed.17,100 In such cases, the benefits of prophylaxis need to beweighed against the potential for the development of resistance.
Close follow-up is necessary during and following therapy. A visitto the physician should take place at the end of antimicrobial therapy.Follow-up of the patient may be conducted by telephone 1 week later,but an outpatient visit may be necessary for less compliant patients.Patients should be given a brief information sheet on how to preventrecurrence, and what signs or symptoms should prompt a telephonecall or return visit to the physician or hospital. With a combination ofearly, aggressive treatment, and with elimination of underlyingcauses, most cases of SSTI can be effectively treated, and the potentialfor relapse or recurrence can be minimized.
Acknowledgements
The panel members thank Glenn Hodding, PharmD, for providingpharmacokinetic and pharmacodynamic information, and IanLeighton, PhD, for editorial assistance. This document is the finalproduct of a series of faculty meetings that began in San Francisco inJuly 2002 with a preliminary approach to the subject and concludedin Miami in February 2003 with the preparation of the guidelines intheir final form.
Faculty disclosures
L. Eron is on the Speaker’s Bureau of Bayer, Pfizer, Pharmacia,Roche Laboratories and Wyeth-Ayerst and has received a researchgrant from Roche Laboratories. B. Lipsky’s pharmaceutical contacts(research support, advisory board, honoraria) include Pfizer, Ortho-McNeil, Wyeth-Ayerst, Cubist, Merck, F. Hoffmann-La Roche Ltdand Bristol-Myers-Squibb. D. Low has received research supportfrom Hoffmann La-Roche Ltd, Bayer Inc., Pfizer Canada, AbbottLaboratories and Aventis Pharma, honoraria for medical continuingeducation from Hoffmann La-Roche Ltd, Bayer Inc., Pfizer Canada,GlaxoSmithKline and Bristol-Myers Squibb, and has served onAdvisory Boards for Aventis Pharma and GlaxoSmithKline. D.Nathwani is on the advisory boards of Bayer, MSD and Pfizer.A. Tice has received research funding from Roche, Merck, Elan,Wyeth, Cubist, Pfizer and Becton-Dickinson, has served on advisoryboards for Merck and Bayer, and received honoraria from Roche,Merck, Pfizer and Cubist. G. Volturo has received research supportfrom Roche Laboratories, honoraria from Roche Laboratories, Pfizerand Aventis, and has been a consultant for Scios.
Table 9. Factors suggesting the need for more prolonged antimicrobial therapy
Probable endocarditis or metastatic spread to organs (e.g. spleen, kidney, liver)Accompanying tissue necrosisOrganism that is difficult to eradicate (i.e. relatively resistant to available antimicrobial agents)Compromised immunityAdverse local factors (e.g. lymphoedema, ischaemia)
Dow
nloaded from https://academ
ic.oup.com/jac/article/52/suppl_1/i3/2473489 by guest on 11 January 2022

Managing skin and soft tissue infections
i15
References
1. Swartz, M. N. (2000). Cellulitis and subcutaneous tissue infec-tions. In Principles and Practice of Infectious Diseases, 5th edn (Mandell,G. L., Bennett, J. E. & Dolin, R., Eds), pp. 1042–57. Churchill Livingstone,Philadelphia, PA, USA.
2. Tice, A. D., Poretz, D., Cook, F. et al. (1998). Medicare coverageof outpatient ambulatory intravenous antibiotic therapy: a program thatpays for itself. Clinical Infectious Diseases 27, 1415–21.
3. Nathwani, D. (2001). The management of skin and soft tissueinfections: outpatient parenteral antibiotic therapy in the United Kingdom.Chemotherapy 47, Suppl. 1, 17–23.
4. Tice, A. (1998). Outpatient parenteral antimicrobial therapy as analternative to hospitalization. International Journal of Clinical PracticeSupplement 95, 4–8.
5. Nathwani, D. & Zambrowski, J. J. on behalf of the AdHOC Work-shop. (2000). Advisory group on Home-based and Outpatient Care(AdHOC): an international consensus statement on non-inpatientparenteral therapy. Clinical Microbiology and Infection 6, 464–76.
6. Gottlieb, T., Atkins, B. L. & Shaw, D. R. (2002). Soft tissue, boneand joint infections. Medical Journal of Australia 176, 609–15.
7. Carrasco, D. A. & Trying, S. (2002). Skin and soft tissue infections.In Antibiotics and Chemotherapy (Finch, R., Greenwood. D., Norbby,S. R. et al., Eds), pp. 692–707. Churchill Livingstone.
8. Anonymous. (2002). Dilemmas when managing cellulitis. Drugsand Therapeutics Bulletin 41, 43–6.
9. Eron, L. J. (2000). Infections of skin and soft tissue: outcomes of aclassification scheme. Clinical Infectious Diseases 31, 287 (A432).
10. Eron, L. J. & Passos, S. (2001). Early discharge of infectedpatients through appropriate antibiotic use. Archives of Internal Medicine161, 61–5.
11. Fine, M. J., Stone, R. A., Singer, D. E. et al. (1999). Processes andoutcomes of care for patients with community-acquired pneumonia:results from the Pneumonia Patient Outcomes Research Team (PORT)cohort study. Archives of Internal Medicine 159, 970–80.
12. Tice, A. D. (2000). Pharmacoeconomic considerations in theambulatory use of parenteral cephalosporins. Drugs 59, Suppl. 3, 29–35.
13. Bowler, P. G., Duerden, B. I. & Armstrong, D. G. (2001). Woundmicrobiology and associated approaches to wound management. ClinicalMicrobiological Reviews 14, 244–69.
14. Ratner, H. (1987). Vibrio vulnificus. Infection Control 8, 430–3.15. Sharkawy, A., Low, D. E., Saginur, R. et al. (2002). Severe group A
streptococcal soft tissue infections in Ontario: 1992–1996. Clinical Infec-tious Diseases 34, 454–60.
16. Nathwani, D., Moitra, S., Dunbar, J. et al. (1998). Skin and softtissue infections: development of a collaborative management planbetween community and hospital care. International Journal of ClinicalPractice 52, 456–60.
17. Baddour, L. M. (2000). Cellulitis syndromes: an update. Interna-tional Journal of Antimicrobial Agents 14, 113–6.
18. Fine, M. J., Auble, T. E., Yealy, D. M. et al. (1997). A predictionrule to identify low-risk patients with community-acquired pneumonia.New England Journal of Medicine 336, 243–50.
19. Carratala, J., Roson, B., Fernandez-Sabe, N. et al. (2003). Factorsassociated with complications and mortality in adult patients hospitalizedfor infectious cellulitis. European Journal of Clinical Microbiology andInfectious Diseases 22, 151–7.
20. Wallace, R. J., Brown, B. A. & Onyi G. O. (1992). Skin, soft tissue,and bone infections due to Mycobacterium chelonae: importance of priorcorticosteroid therapy, frequency of disseminated infections, and resist-ance to oral antimicrobials other than clarithromycin. Journal of InfectiousDiseases 166, 405–12.
21. Keane, J., Gershon, S., Wise, R. P. et al. (2001). Tuberculosisassociated with infliximab, a tumor necrosis factor alpha-neutralizingagent. New England Journal of Medicine 345, 1098–104.
22. Mikuls, T. R. & Moreland, L. W. (2003). Benefit–risk assessment ofinfliximab in the treatment of rheumatoid arthritis. Drug Safety 26, 23–32.
23. Bisno, A. L., Cockerill, F. R., III & Bermudez, C. T. (2000). The ini-tial outpatient-physician encounter in group A streptococcal necrotizingfasciitis. Clinical Infectious Diseases 31, 607–8.
24. Simonart, T., Simonart, J.-M., Derdelinckx, I. et al. (2001). Value ofstandard laboratory tests for the early recognition of group A β-hemolyticstreptococcal necrotizing fasciitis. Clinical Infectious Diseases 32, E9–12.
25. Wall, D. B., Klein, S. R., Black, S. et al. (2000). A simple model tohelp distinguish necrotizing fasciitis from nonnecrotizing soft tissue infec-tion. Journal of the American College of Surgeons 191, 227–31.
26. Wall, D. B., de Virgilio, C., Black, S. et al. (2000). Objective criteriamay assist in distinguishing necrotizing fasciitis from nonnecrotizing softtissue infection. American Journal of Surgery 179, 17–21.
27. Eady, E. A. & Cove, J. H. (2003). Staphylococcal resistance revis-ited: community-acquired methicillin resistant Staphylococcus aureus –an emerging problem for the management of skin and soft tissue infections.Current Opinions in Infectious Diseases 16, 103–24.
28. Cookson, B. D. (2000). Methicillin-resistant Staphylococcus aureusin the community: new batttlefronts, or are the battles lost? Infection Controland Hospital Epidemiology 21, 398–403.
29. Lee, P.-C., Turnidge, J. & McDonald, P. J. (1985). Fine-needleaspiration biopsy in diagnosis of soft tissue infections. Journal of ClinicalMicrobiology 22, 80–3.
30. Aly, A. A., Roberts, N. M., Seipol, K. S. et al. (1996). Case surveyof management of cellulitis in a tertiary teaching hospital. Medical Journalof Australia 165, 553–6.
31. Dong, S. L., Kelly, K. D., Oland, R. C. et al. (2001). ED manage-ment of cellulitis: a review of five urban centers. American Journal ofEmergency Medicine 19, 535–40.
32. Perl, B., Gottehrer, N. P., Raveh, D. et al. (1999). Cost-effective-ness of blood cultures for adult patients with cellulitis. Clinical InfectiousDiseases 29, 483–8.
33. Martinez, E., Reilly, B. M., Evans, A. T. et al. (2001). The obser-vation unit: a new interface between inpatient and outpatient care. Ameri-can Journal of Medicine 110, 274–7.
34. Roberts, R. (2001). Management of patients with infectious dis-ease in an emergency department observation unit. Emergency Medi-cine Clinics of North America 19, 187–207.
35. Hostetler, B., Leikin, J. B., Timmons, J. A. et al. (2002). Patterns ofuse of an emergency department-based observation unit. AmericanJournal of Therapeutics 9, 499–502.
36. Apelqvist, J. (1998). Wound healing in diabetes. Outcome andcosts. Clinics in Podiatric Medicine and Surgery 15, 21–39.
37. Gerding, D. N. (1995). Foot infections in diabetic patients: the roleof anaerobes. Clinical Infectious Diseases 20, Suppl. 2, S283–8.
38. Meehan, T. P., Fine, M. J., Krumholz, H. M. et al. (1997). Qualityof care, process, and outcomes in elderly patients with pneumonia. Journalof the American Medical Association 278, 2080–4.
39. Battleman, D. S., Callahan, M. & Thaler, H. T. (2002). Rapid anti-biotic delivery and appropriate antibiotic selection reduce length of hospitalstay of patients with community-acquired pneumonia: link between qualityof care and resource utilization. Archives of Internal Medicine 162, 682–8.
40. Fraschini, F., Braga, P. C., Scarpazza, G. et al. (1986). Humanpharmacokinetics and distribution in various tissues of ceftriaxone.Chemotherapy 32, 192–9.
41. Dong, Y., Zhao, X., Domagala, J. et al. (1999). Effect of fluoro-quinolone concentration on selection of resistant mutants of Mycobac-terium bovis BCG and Staphylococcus aureus. Antimicrobial Agents andChemotherapy 43, 1756–8.
42. Thomas, J. K., Forrest, A., Bhavnani, S. et al. (1998). Pharmaco-dynamic evaluation of factors associated with the development of bacterialresistance in acutely ill patients during therapy. Antimicrobial Agents andChemotherapy 42, 521–7.
43. Zhao, X. & Drlica, K. (2001). Restricting the selection of antibiotic-resistant mutants: a general strategy derived from fluoroquinolone studies.Clinical Infectious Diseases 3, Suppl. 3, S147–6.
Dow
nloaded from https://academ
ic.oup.com/jac/article/52/suppl_1/i3/2473489 by guest on 11 January 2022

L. J. Eron et al.
i16
44. Hollenstein, U. M., Brunner, M., Schmid, R. et al. (2001). Softtissue concentrations of ciprofloxcain in obese and lean subjects followingweight-adjusted dosing. International Journal of Obesity 25, 354–8.
45. Gee, T., Ellis, R., Marshall, G. et al. (2001). Pharmacokinetics andtissue penetration of linezolid following multiple oral doses. AntimicrobialAgents and Chemotherapy 45, 1843–6.
46. Child, J., Mortiboy, D., Andrews, J. M. et al. (1995). Open-labelcrossover study to determine pharmacokinetics and penetration of twodose regimens of levofloxacin into inflammatory fluid. AntimicrobialAgents and Chemotherapy 39, 2749–51.
47. Wise, R., Andrews, J. M., Ashby, J. P. et al. (1999). A study todetermine the pharmacokinetics and inflammatory fluid penetration ofgatifloxacin following a single oral dose. Journal of Antimicrobial Chemo-therapy 44, 701–4.
48. Muller, M., Stab, H., Brunner, M. et al. (1999). Penetration of moxi-floxacin into peripheral compartments in humans. Antimicrobial Agentsand Chemotherapy 43, 2345–9.
49. Mohlenbeck, F. (1976). The geriatric pharmacology of cefazolin,cefradin and sulfisomidine. Arzneimittelforschung 26, 1377–82.
50. Howard, G. W., Begg, E. J., Chambers, S. T. et al. (2002). Freeand total cefazolin plasma and interstitial fluid concentrations at steadystate during continuous infusion. Journal of Antimicrobial Chemotherapy50, 429–32.
51. Cadorniga, R., Barrios, S., Segura, J. et al. (1979). Penetration ofantibiotic into interstitial tissue fluid following parenteral administration oflysine cephalexin. Arzneimittel-Forschung 29, 1547–9.
52. Scaglione, F., Demartini, G., Arcidiacono, M. M. et al. (1997).Serum protein binding and extravascular diffusion of cefodizime andceftriaxone – an in vivo study. Clinical Drug Investigation 14, 211–6.
53. Vaillant, L., Machet, L., Taburet, A. M. et al. (1992). Levels offusidic acid in skin blister fluid and serum after repeated administration oftwo dosages (250 and 500 mg). British Journal of Dermatology 126, 591–5.
54. Klimowicz, A., Nowak, A. & Bielecka-Grzela, S. (1996). Plasmaand skin blister fluid concentrations of metronidazole and its hydroxyme-tabolite after oral administration. Polish Journal of Pharmacology 48,47–52.
55. Vaillant, L., Le Guellec, C., Jehl, F. et al. (2000). Comparativediffusion of fusidic acid, oxacillin, and pristinamycin in interstitial dermalfluid after repeated oral administration. Annales de Dermatologie et deVenereologie 127, 33–9.
56. McNulty, C. A. M., Garden, G. M. F., Wise, R. et al. (1985). Thepharmacokinetics and tissue penetration of teicoplanin. Journal of Anti-microbial Chemotherapy 16, 743–9.
57. Solberg, C. O., Halstensen, A., Digranes, A. et al. (1983). Penetra-tion of antibiotics into human leukocytes and dermal suction blisters.Reviews of Infectious Diseases 5, Suppl. 3, S468–73.
58. Nowak, A., Kadykow, M. & Klimowicz, A. (1983). Penetration oftrimethoprim and sulfamethoxazole into skin blister fluid. EuropeanJournal of Clinical Pharmacology 25, 825–7.
59. Lebel, M., Gregoire, S., Caron, M. et al. (1985). Difference in blis-ter fluid penetration after single and multiple doses of ceftriaxone. Anti-microbial Agents and Chemotherapy 28, 123–7.
60. Raymakers, J. T., Houben, A. J., van der Heyden, J. J. et al.(2002). The effect of diabetes and severe ischaemia on the penetrationof ceftazidime into tissues of the limb. Diabetic Medicine 18, 229–34.
61. Tice, A. D. (1991). Once-daily ceftriaxone outpatient therapy inadults with infections. Chemotherapy 37, Suppl. 3, 7–10.
62. Brown, G., Chamberlain, R., Goulding, J. et al. (1996). Ceftriaxoneversus cefazolin with probenecid for severe skin and soft tissue infec-tions. Journal of Emergency Medicine 14, 547–51.
63. Goldstein, E. J., Citron, D. M., Merriam, C. V. et al. (2002). Generalmicrobiology and in vitro susceptibility of anaerobes isolated from compli-cated skin and skin-structure infections in patients enrolled in a compar-ative trial of ertapenem versus piperacillin–tazobactam. Clinical InfectiousDiseases 35, Suppl. 1, S119–25.
64. Grayson, M. L., McDonald, M., Gibson, K. et al. (2002). Once-dailyintravenous cefazolin plus oral probenecid is equivalent to once-daily
intravenous ceftriaxone plus oral placebo for the treatment of moderate-to-severe cellulitis in adults. Clinical Infectious Diseases 34, 1440–8.
65. Craig, W. A. (1995). Kinetics of antibiotics in relation to effectiveand convenient outpatient parenteral therapy. International Journal ofAntimicrobial Agents 5, 19–22.
66. Stevens, D. L., Herr, D., Lampiris, H. et al. (2002). Linezolid versusvancomycin for the treatment of methicillin-resistant Staphylococcusaureus infections. Clinical Infectious Diseases 34, 1481–90.
67. Lipsky, B. A., Armstrong, D., Acin, F. et al. (2002). Treating diabeticfoot infections with linezolid vs. aminopenicillins: a randomized interna-tional multicenter trial. In Abstracts of the Fortieth Annual Meeting of theIDSA, Chicago, IL, 2002. Abstract 189, p.78. Infectious Diseases Societyof America, Alexandria, VA, USA.
68. Gerson, S. L., Kaplan, S. L., Bruss, J. B. et al. (2002). Hematologiceffects of linezolid: summary of clinical experience. Antimicrobial Agentsand Chemotherapy 46, 2723–6.
69. Waldrep, T. W. & Skiest, D. J. (2002). Linezolid-induced anemiaand thrombocytopenia. Pharmacotherapy 22, 109–12.
70. Heffelfinger, J. D., Dowell, S. F., Jorgensen, J. H. et al. (2000).Management of community-acquired pneumonia in the era of pneumo-coccal resistance. Archives of Internal Medicine 160, 1399–408.
71. Stevens, D. L. (1996). Invasive group A streptococcal disease.Infectious Agents and Disease 5, 157–66.
72. van Dissel, J. T., Kullberg, B. J. & van der Meer, J. W. (1999).Toxic shock-like syndrome caused by streptococci. Nederlands tijdschriftvoor geneeskunde 143, 1452–5.
73. Kaul, R., McGeer, A., Norrby-Teglund, A. et al. (1999). Intrave-nous immunoglobulin therapy for streptococcal toxic shock syndrome—acomparative observational study. The Canadian Streptococcal StudyGroup. Clinical Infectious Diseases 28, 800–7.
74. Ely, E. W., Bernard, G. R. & Vincent, J. L. (2002). Activatedprotein C for severe sepsis. New England Journal of Medicine 347,1035–6.
75. Fielden, M. P., Martinovic, E. & Ells, A. L. (2002). Hyperbaricoxygen therapy in the treatment of orbital gas gangrene. Journal ofAAPOS 6, 252–4.
76. Wunderlich, R. P., Peters, E. J. G. & Lavery, L. A. (2000). Sys-temic hyperbaric oxygen therapy: lower-extremity wound healing and thediabetic foot. Diabetes Care 23, 1551–5.
77. Donaldson, M. C. (2000). Chronic venous insufficiency. CurrentTreatment Options in Cardiovascular Medicine 2, 265–72.
78. Fry, D. E., Marek, J. M. & Langsfeld, M. (1998). Infection in theischemic lower extremity. Surgical Clinics of North America 78, 465–79.
79. Bergkvist, P. I. & Sjöbeck, K. (1997). Antibiotic and prednisolonetherapy of erysipelas: a randomized, double blind, placebo-controlledstudy. Scandinavian Journal of Infectious Diseases 29, 377–82.
80. Bergkvist, P. I. & Sjöbeck, K. (1998). Relapse of erysipelas followingtreatment with prednisolone or placebo in addition to antibiotics: a 1-yearfollow-up. Scandinavian Journal of Infectious Diseases 30, 206–7.
81. De Lalla, F., Pellizzer, G., Strazzabosco, M. et al. (2001). Ran-domized prospective controlled trial of recombinant granulocyte colony-stimulating factor as adjunctive therapy for limb-threatening diabetic footinfection. Antimicrobial Agents and Chemotherapy 45, 1094–8.
82. Gough, A., Clapperton, M., Rolando, N. et al. (1997). Randomisedplacebo-controlled trial of granulocyte-colony stimulating factor in diabeticfoot infection. Lancet 350, 855–9.
83. Jones, R. N. (1996). The emergent needs for basic research,education, and surveillance of antimicrobial resistance. Problems facingthe report from the American Society for Microbiology Task Force onAntibiotic Resistance. Diagnostic Microbiology and Infectious Disease25, 153–61.
84. Gould, I. M., Mackenzie, F. M., Lopez-Lozano, J. M. et al. (2002).Temporal relationship between prevalence of methicillin-resistantStaphylococcus aureus (MRSA) in one hospital and prevalence of MRSAin the surrounding community: a time series analysis. In Abstracts of theForty-second Interscience Conference on Antimicrobial Agents and
Dow
nloaded from https://academ
ic.oup.com/jac/article/52/suppl_1/i3/2473489 by guest on 11 January 2022

Managing skin and soft tissue infections
i17
Chemotherapy, San Diego, CA, 2002. Abstract K-103, p. 304. AmericanSociety for Microbiology, Washington, DC, USA.
85. Kataja, J., Huovinnen, P. & Seppälä, H. (2000). Erythromycinresistance genes in group A streptococci of different geographicalorigins. Journal of Antimicrobial Chemotherapy 46, 789–92.
86. Murdoch, D. R. & Reller, L. B. (2001). Antimicrobial susceptibilitiesof group B streptococci isolated from patients with invasive disease:10-year perspective. Antimicrobial Agents and Chemotherapy 45, 3623–4.
87. Karlowsky, J. A., Jones, M. E., Mayfield, D. C. et al. (2002). Ceftri-axone activity against Gram-positive and Gram-negative pathogensisolated in US clinical microbiology laboratories from 1996 to 2000:results from The Surveillance Network® (TSN®) Database—USA. Inter-national Journal of Antimicrobial Agents 19, 413–26.
88. Jones, R. N., Cormican, M. G. & Wanger, A. (1996). Clindamycinresistance among erythromycin-resistant Streptococcus pneumoniae.Diagnostic Microbiology and Infectious Disease 25, 201–4.
89. Hyde, T. B., Gay, K. & Stephens, D. S. (2001). Macrolide resistanceamong invasive Streptococcus pneumoniae isolates. Journal of theAmerican Medical Association 286, 1857–62.
90. Panagea, S., Perry, J. D. & Gould, F. K. (1999). Should clindamycinbe used as treatment of patients with infections caused by erythromycin-resistant staphylococci? Journal of Antimicrobial Chemotherapy 44,581–2.
91. Nathwani, D. (1998). Non-inpatient use of teicoplanin. InternationalJournal of Clinical Practice 52, 577–81.
92. Klein, N. C. & Cunha, B. A. (2001). New uses of older antibiotics.Medical Clinics of North America 85, 125–32.
93. Yelandi, V., Strodtman, R. & Lention, J. R. (1988). In-vitro and in-vivostudies of trimethroprim–sulphamethoxazole against multiple resistantStaphylococcus aureus. Journal of Antimicrobial Chemotherapy 22,873–80.
94. Yuk, J. H., Dignani, M. C., Harris, R. L. et al. (1991). Minocyclineas an alternative antistaphylococcal agent. Reviews of InfectiousDiseases 13, 1023–4.
95. Clumeck, N., Marcelis, L, Amiri-Lamraski, M. H. et al. (1984).Treatment of severe staphylococcal infections with a rifampicin–minocy-cline association. Journal of Antimicrobial Chemotherapy 13, Suppl. C,17–22.
96. Lipsky, B. A., Pecoraro, R. E., Larson, S. A. et al. (1990). Out-patient management of uncomplicated lower-extremity infections in diabeticpatients. Archives of Internal Medicine 150, 790–7.
97. Lipsky, B. A. (1999). Evidence-based antibiotic therapy of diabeticfoot infections. FEMS Immunology and Medical Microbiology 26, 267–76.
98. Bisno, A. L. & Stevens, D. L. (1996). Streptococcal infections ofskin and soft tissues. New England Journal of Medicine 334, 240–5.
99. Raz, R., Miron, D., Colodner, R. et al. (1996). A 1-year trial of nasalmupirocin in the prevention of recurrent staphylococcal nasal colonizationand skin infection. Archives of Internal Medicine 156, 1109–12.100. Kremer, M., Zuckerman, R., Avraham, Z. et al. (1991). Long-term
antimicrobial therapy in the prevention of recurrent soft-tissue infections.Journal of Infection 22, 37–40.101. Robinson, J. L., Hameed, T. & Carr, S. (2002). Practical aspects of
choosing an antibiotic for patients with a reported allergy to an antibiotic.Clinical Infectious Diseases 35, 26–31.102. Kelkar, P. S. & Li, J. T. (2001). Cephalosporin allergy. New England
Journal of Medicine 345, 804–9.
103. Saxson, A., Beall, G. N., Rohr, A. S. et al. (1987). Immediatehypersensitivity reactions to beta-lactam antibiotics. Annals of InternalMedicine 107, 204–15.104. Nathwani, D. & Tice, A. (2002). Ambulatory antimicrobial use: the
values of an outcomes registry. Journal of Antimicrobial Chemotherapy49, 149–54.105. Tice, A. D., Seibold, G. L. & Martinelli, L. P. (2002). Adverse
effects from intravenous antibiotics with OPAT. In Abstracts of the For-tieth Annual Meeting of the IDSA, Chicago, IL, 2002. Abstract 59, p. 55.Infectious Diseases Society of America, Alexandria, VA, USA.106. Caplan, G. A., Ward, J. A., Brennan, N. J. et al. (1999). Hospital in
the home: a randomised controlled trial. Medical Journal of Australia 170,156–60.107. Stevens, D. L., Smith, L. G., Bruss, J. B. et al. (2000). Randomized
comparison of linezolid (PNU-100766) versus oxacillin–dicloxacillin fortreatment of complicated skin and soft tissue infections. AntimicrobialAgents and Chemotherapy 44, 3408–13.108. Ahkee, S., Smith, S., Newman, D. et al. (1997). Early switch from
intravenous to oral antibiotics in hospitalized patients with infections: a6-month prospective study. Pharmacotherapy 17, 569–75.109. Cox, N. H., Colver, G. B. & Paterson, W. D. (1998). Management
and morbidity of cellulitis of the leg. Journal of the Royal Society ofMedicine 91, 634–7.110. Madaras-Kelly, K. J., Arbogast, R. & Jue, S. (2000). Increased
therapeutic failure for cephalexin versus comparator antibiotics in thetreatment of uncomplicated outpatient cellulitis. Pharmacotherapy 20,199–205.111. Dunn, A. S., Peterson, K. L., Schechter, C. B. et al. (1999). The
utility of an in-hospital observation period after discontinuing intravenousantibiotics. American Journal of Medicine 106, 6–10.112. Boyter, A. C., Stephen, J., Fegan, P. G. et al. (1997). Why do
patients with infection remain in hospital once changed to oral anti-biotics? Journal of Antimicrobial Chemotherapy 39, 286–8.113. Cacares, V. M., Strange, K. C., Kikano, G. E. et al. (1994). The
clinical utility of a day of observation after switching from intravenous tooral antibiotic therapy in the treatment of pyelonephritis. Journal ofFamily Practice 39, 337–9.114. Guay, D. R. (2000). Short-course antimicrobial therapy for upper
respiratory tract infections. Clinical Therapy 22, 673–84.115. Michael, M., Hodson, E. M., Craig, J. C. et al. (2002). Short
compared with standard duration of antibiotic treatment for urinary tractinfection: a systematic review of randomised controlled trials. Archives ofDisease in Childhood 87, 118–23.116. Cohen, R., Navel, M., Grunberg, J. et al. (1999). One dose ceftri-
axone vs. ten days of amoxicillin/clavulanate therapy for acute otitismedia: clinical efficacy and change in nasopharyngeal flora. PediatricInfectious Disease Journal 18, 403–9.117. Sanchez, M., Collvinent, B., Miro, O. et al. (2002). Short-term
effectiveness of ceftriaxone single dose in the initial treatment of acuteuncomplicated pyelonephritis in women. A randomised controlled trial.Emergency Medicine Journal 19, 19–22.118. Koutkia, P., Mylonakis, E. & Boyce, J. (1999). Cellulitis: evaluation
of possible predisposing factors in hospitalised patients. DiagnosticMicrobiology and Infectious Disease 34, 325–7.119. Ichiyama, S., Hirai, S., Minami, T. et al. (1998). Campylobacter
fetus subspecies fetus cellulitis associated with bacteremia in debilitatedhosts. Clinical Infectious Diseases 27, 252–5.
Dow
nloaded from https://academ
ic.oup.com/jac/article/52/suppl_1/i3/2473489 by guest on 11 January 2022