Embed Size (px)
Citation preview
Managing the Complex Parenteral Nutrition (PN) PatientCarol J. Rollins, MS, RD, PharmD, CNSC, BCNSP
Coordinator, Nutrition Support Team, The University of Arizona Medical CenterAssociate Professor, The University of Arizona College of Pharmacy
Tucson, Arizona
CE Credit in Four Easy Steps!
3/27/2013 2
1. Scan your badge as you enter each session.
2. Carry your Evaluation Packet to every session so you can add session evaluation forms to it.
3. Track your hours on the “Statement of Session Attendance Form” as you go.
4. At your last session, total the hours and sign both pages of your Statement of Session Attendance Form.
Keep the PINK copy for your records.
Put the YELLOW and WHITE copies in your CE Envelope.
Make sure an Evaluation Form is in your CE Envelope for each session you attended. Miss one? Extras are in a file near Registration.
Fill out the information on the outside of the CE Packet envelope, seal it, and drop it in the box near Registration.
Applying for Pharmacy CPE? If you have not yet registered for an NABP e-Profile ID, please visit www.MyCPEmonitor.net to do so before submitting your packet. You must enter your NABP e-Profile ID in order to receive CE credit this year!
Speaker Disclosures
• Carol J. Rollins has no conflicts of interest or potential financial conflicts to disclose. • Clinical trials and off‐label/ investigational uses will not be discussed during this presentation.
3
Objectives1. Discuss options for management of macronutrient
intolerance, including hyperglycemia and hypertriglyceridemia.
2. Discuss the inter‐relationship of potassium, magnesium and phosphorus when managing a parenteral nutrition patient.
3. Assess the likelihood of an acid‐base imbalance developing based on a patient's clinical presentation and recommend appropriate interventions.
4
Self‐Assessment Question 1The GIR for a 50 kg patient (BMI 16 kg/m2) who receives 400 g dextrose (1360 kcal; 27 kcal/kg) daily in PN is generally considered to be:A. Below the maximum that can be oxidizedB. Within an appropriate range for weight gainC. The maximum that does not cause fatty liverD. Excessive for a patient with metabolic stress
5
Self‐Assessment Question 2For a patient with PN‐associated hyperglycemia, which type of insulin is most likely to be appropriate for use in a sliding scale regimen?A. LisproB. Regular C. NPHD. Glargine
6
Self‐Assessment Question 3Which nutrient source is the most appropriate for increasing calories in a patient with hyperglycemia (FSBG 220 – 300 mg/dL) and hypertriglyceridemia (TG 250 mg/dL)?A. DextroseB. GlycerolC. Fat emulsionD. Protein
7
Hyperglycemia ‐ Assessment• New vs known• Range of glucose concentrations• Pattern or timing of abnormal glucose • Treatment administered, if any, and response • Confirmation of abnormal glucose• Confounding factors
8
Hyperglycemia – Potential Causes• Disease related – DM, pancreatic dz• Medication related ٭ Glucocorticoids, octreotide
• Imbalance of nutritional substrates – GIR • Other ٭ Infection٭ Metabolic stress, inflammatory response٭ Chromium deficiency
9
Balance of Nutritional Substrates• Glucose infusion rate (GIR)٭ Calculate as mg/kg/minute٭ Maximum glucose oxidized
• Stressed adult, 3 – 5 mg/kg/min (4.3 – 7.2 g/kg/day)
• IVFE as a caloric source٭ Minimum vs maximum
• Protein as a caloric source٭ Requires energy for conversion
10
Treatment of Hyperglycemia• Insulin٭ Type based on duration of action٭ Route
• Admixed in PN• Separate from PN – SQ, IV
٭ Schedule• Routine – once daily, twice daily, multiple daily doses• Sliding scale
• Other
11
Hyperglycemia – Case of C.C.• 67 y.o. F with enterocutaneous fistula x2• NPO except meds (not to exceed 360 mL/day)• Weight for PN calculations: 60 kg • Home PN 2400 mL/day over 18 hr, 1 hr 1 hr • PN order/day: Dextrose 240 g, AA 100 g, Fat 60 g • Insulin: PN 20 units regular; SQ 8 units glargine• FSBG (mg/dL) range from 75 to 292
12
Hyperglycemia – C.C.How should C.C.’s hyperglycemia be treated?A. Use ultra short acting insulin analog (Lispro)
in sliding scale coverageB. Split glargine dose with 60% an hour before
PN is started, 40% in amC. Increase taper up time to 2 hrD. Reduce dextrose in PN
13
Other Information Needed for C.C. • Adherence to NPO • GIR = 2.77 mg/kg/min (4 g/kg/day)
٭ [(240 g/d x 1000 mg/g) / 60 kg] / 1440 min/d• Pattern of FSBG (range from 75 to 292 mg/dL)
٭ Off PN: 75 – 90 ٭ 2 hr after PN starts: 226 – 292٭ 15‐16 hr after PN starts: 90 – 134
• Stability considerations٭ Fat containing PN: minimum 10% Dextrose, 4% AA, 2% Fat [Driscoll]
Hyperglycemia – C.C.How should C.C.’s hyperglycemia be treated?A. Use ultra short acting insulin analog (Lispro)
in sliding scale coverageB. Split glargine dose with 60% an hour before
PN is started, 40% in amC. Increase taper up time to 2 hrD. Reduce dextrose in PN
15
Hyperglycemia – Case of M.H.• 69 y.o. M with SBO, G‐tube to drainage٭ Colostomy s/p hemicolectomy for colon cancer
• Weight for PN calculations: 73 kg• Home PN 2280 mL/day continuous infusion• PN order/day: Dextrose 420 g, AA 100 g, Fat 73 g • FSBG 120 – 150 mg/dL for 1st 20 days at home٭ No insulin added to PN
• FSBG 180‐265 mg/dL past 48 hr
16
Hyperglycemia – M.H.How should M.H.’s hyperglycemia be managed?A. Add regular insulin to PN B. Add a sliding scale insulin regimenC. Start long‐acting basal insulin and add a
sliding scale insulin regimenD. Re‐formulate PN for lower dextrose dose
17
Other Information Needed for M.H.• Has oral intake started recently?• Pattern of hyperglycemia• Vital signs – is pt stable? ٭ Temperature, heart rate
• Signs of infection?٭ CVL٭ Surgical site/ ostomy٭ Pneumonia
Hyperglycemia – M.H.How should M.H.’s hyperglycemia be managed?A. Add regular insulin to PN B. Add a sliding scale insulin regimenC. Start long‐acting basal insulin and add a
sliding scale insulin regimenD. Re‐formulate PN for lower dextrose dose
19
Hyperglycemia – Case of T.N.• 52 y.o. F with wound vac on complex surgical site• 10 weeks s/p repair of duodenal stricture• Weight for PN calculations: 40 kg (BMI 15.5)٭ Continued weight loss on PN x 3 months; stable x 3 wk
• Home PN 2000 mL over 16 hr, 1 hr 1hr• PN order: D15% AA5% and 500 mL 20% fats MWF• Insulin: PN 30 units regular; sliding scale regular• FSBG 145 – 266 mg/dL
20
Hyperglycemia – T.N. How should T.N.’s hyperglycemia be managed?A. Increase regular insulin in PN using sliding
scale amount as a guideB. Start long‐acting basal insulin and make
sliding scale dose more aggressiveC. Lower dextrose and increase fat caloriesD. Reduce dextrose and total calories
21
Other Information Needed for T.N.• Diet order and adherence to order NPO• Pattern of hyperglycemia• Units of insulin used for sliding scale coverage• Assess nutrient provision and requirements٭ Protein 100 g/day = 2.5 g/kg/d
• BUN 65 mg/dL
٭ Dextrose 300 g/day = GIR 5.2 mg/kg/min٭ Total calories = 1848 average/day (46.2kcal/kg/d)
22
Hyperglycemia – T.N. How should T.N.’s hyperglycemia be managed?A. Increase regular insulin in PN using sliding
scale amount as a guideB. Start long‐acting basal insulin and make
sliding scale dose more aggressiveC. Lower dextrose and increase fat caloriesD. Reduce dextrose and total calories
Supported by metabolic cart 23
Hyperglycemia – Case of K.S.• 46 y.o. F with multiple medical issues • Hx Roux‐en‐Y gastric bypass for obesity 6 yr ago, followed by reversal 2 yr ago
• Frequent hospital admissions for c/o N,V and severe retrosternal and epigastric pain
• Home PN since last hospital d/c 3 weeks ago • Pt’s care provider reports mental status changes• Lab yesterday: hyperglycemia, hypokalemia
24
Hyperglycemia – K.S.• Wt for PN calculations: 56.6kg (99% IBW)• Lab results: Na 135 K 2.9 Cl 106 Bicarb 20Ca 8.4 Mg 2.1 Phos 2.9BUN 9 SCr0.9 Glucose 544
• Home PN 1000 mL over 12 hr, 1 hr 1hr• PN order: D20% AA5% and 250 mL 20% fats M,Th• No insulin added to PN; no FSBG available
25
Hyperglycemia – K.S.• What other information do you want/need? ٭ How labs were drawn – peripheral stick vs CVL٭ K content of PN٭ Glycated Hgb (from recent hospitalization) 5.3%٭ From yesterday: WBC 4.9 Bands 2%٭ From 1 week ago: K 4.1Glucose 94٭ Other potential causes of mental status changeWhen PN cycle had ended relative to blood draw٭
26
Hyperglycemia – K.S.• Should hyperglycemia be treated in K.S?• Why or why not?٭ Question results that are inconsistent with previously stable results in stable patient
٭ Redraw labs before any treatment • May see euglycemia during off cycle despite hyperglycemia when PN infuses
٭ Labs likely reflect PN contamination
27
Hypertriglyceridemia – Assessment • New vs known• Treatment• Confirmation of abnormal triglyceride٭ Aim for TG < 200 mg/dL٭ Avoid 400 mg/dL or higher
• Confounding factors٭ Medications ٭ Hyperglycemia٭ Micronutrient alteration – Carnitine
28
Hypertriglyceridemia – Case of N.B.• 30 y.o. M s/p MUD HSCT, day + 35• GVHD of GI tract and liver, thrombocytopenia• Weight for PN calculations: 65 kg (95% IBW)• Day 6 Home PN 2400 mL/day at 100 mL/hr ٭ PN hung daily in clinic٭ Care provider issues; limited home RN visits
• PN order/day: Dextrose 150 g, AA 126 g, F 110 g• Triglyceride 290 mg/dL
Hypertriglyceridemia – N.B.How should hypertriglyceridemia be managed?A. Keep tight glucose control with current PN and
monitor TGB. Add immediate release nicotinic acid to
medication regimenC. Reduce fats and increase dextrose calories
provided by PN D. Maintain dextrose calories and reduce fat
provided by PN
Other Information Needed for N.B.• Medications ٭ Glucocorticoids (High dose methylprednisolone)٭ CSA
• Glucose over past 5 days: 180 – 250 mg/dL٭ 15 units regular insulin added to PN٭ No routine FSBG due to thrombocytopenia
• Previous Triglycerides٭ Baseline (day + 4 HSCT): 145 mg/dL٭ Day + 20 HSCT/ Day 4 PN: 250 mg/dL
Other Considerations for IVFE• Maximum dose for adults٭ 2.5 g/kg/day (rarely go above 2 g/kg/day and seldom above 1.5 g/kg/day)
٭ Not more than 60% of total calories from fat• Minimum to prevent EFAD٭ 1% – 2% of total calories as linoleic acid٭ Home PN: No EFAD with 500 mL 20% IVFE weekly
• Critical illness٭ No IVFE in sepsis; limit IVFE to 1 g/kg/day in ICU
32
Hypertriglyceridemia – N.B.How should hypertriglyceridemia be managed?A. Keep tight glucose control with current PN and
monitor TGB. Add immediate release nicotinic acid to
medication regimenC. Reduce fats and increase dextrose calories
provided by PND. Maintain dextrose calories and reduce fat
provided by PN
Self‐Assessment Question 1The GIR for a 50 kg patient (BMI 16 kg/m2) who receives 400 g dextrose (1360 kcal; 27 kcal/kg) daily in PN is generally considered to be:A. Below the maximum that can be oxidizedB. Within an appropriate range for weight gainC. The maximum that does not cause fatty liverD. Excessive for a patient with metabolic stress
34
Self‐Assessment Question 2For a patient with PN‐associated hyperglycemia, which type of insulin is most likely to be appropriate for use in a sliding scale regimen?A. LisproB. Regular C. NPHD. Glargine
35
Self‐Assessment Question 3Which nutrient source is the most appropriate for increasing calories in a patient with hyperglycemia (FSBG 220 – 300 mg/dL) and hypertriglyceridemia (TG 250 mg/dL)?A. DextroseB. GlycerolC. Fat emulsionD. Protein
36
Self‐Assessment Question 4In which clinical situation is bicarbonate loss from the GI tract likely to be highest?A. Nasogastric suctioningB. Aggressive diuresisC. Protracted vomitingD. Prolonged diarrhea
37
Self‐Assessment Question 5Which of the following serum electrolyte patterns is associated with metabolic alkalosis? A. Decreased chloride with sodium disproportionately
high compared to chlorideB. Elevated bicarbonate and chloride with sodium low
compared to chlorideC. Decreased chloride and proportionately low sodium D. Elevated chloride and proportionately high sodium
38
Self‐Assessment Question 6The primary mechanism for the acid‐base disorder associated with acute renal failure is:A. Inability to filter bicarbonate B. Lack of bicarbonate reabsorption in the distal
tubulesC. Retention of organic acids D. Loss of hydrogen ion when potassium is retained
39
40
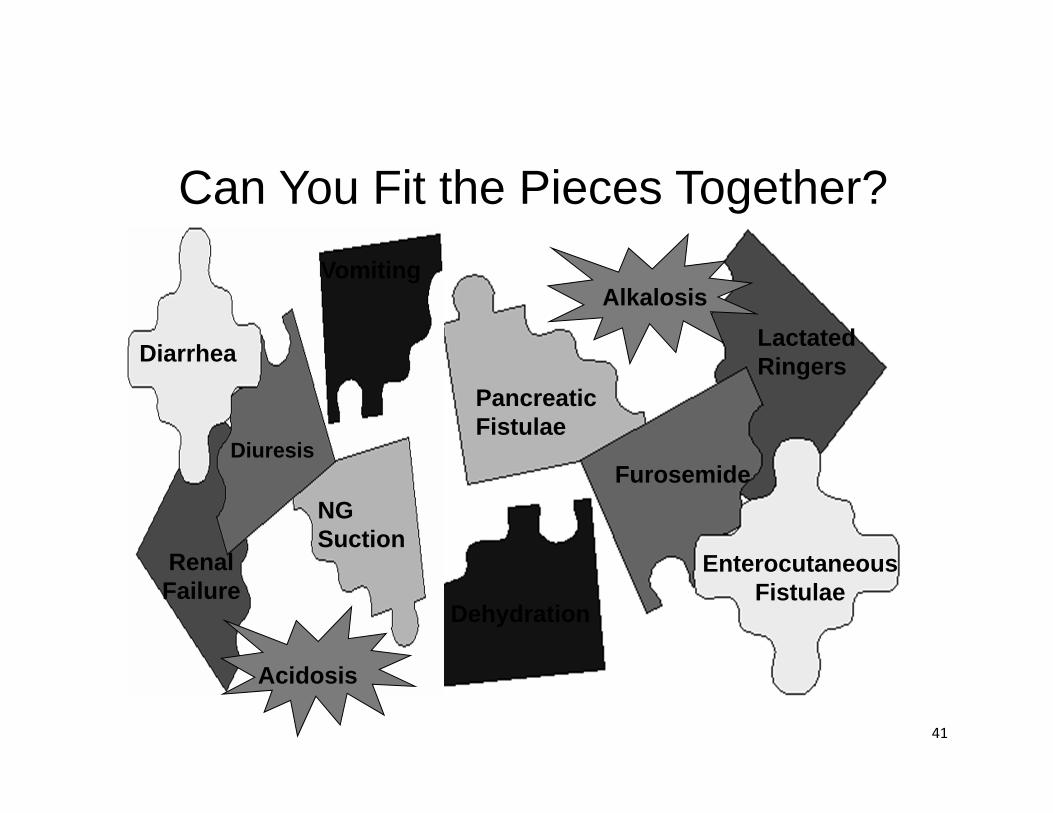
Assessing Acid‐Base Status• Many factors involved• ABG’s provide objective data• Must gather pieces of the puzzle and fit them together when there are no ABG’s– Many assumptions– Less accurate than ABG’s– A simplified interpretation
41
Can You Fit the Pieces Together?Vomiting
Diarrhea
NG Suction
EnterocutaneousFistulae
Dehydration
DiuresisFurosemide
PancreaticFistulae
Renal Failure
Lactated Ringers
Alkalosis
Acidosis
42
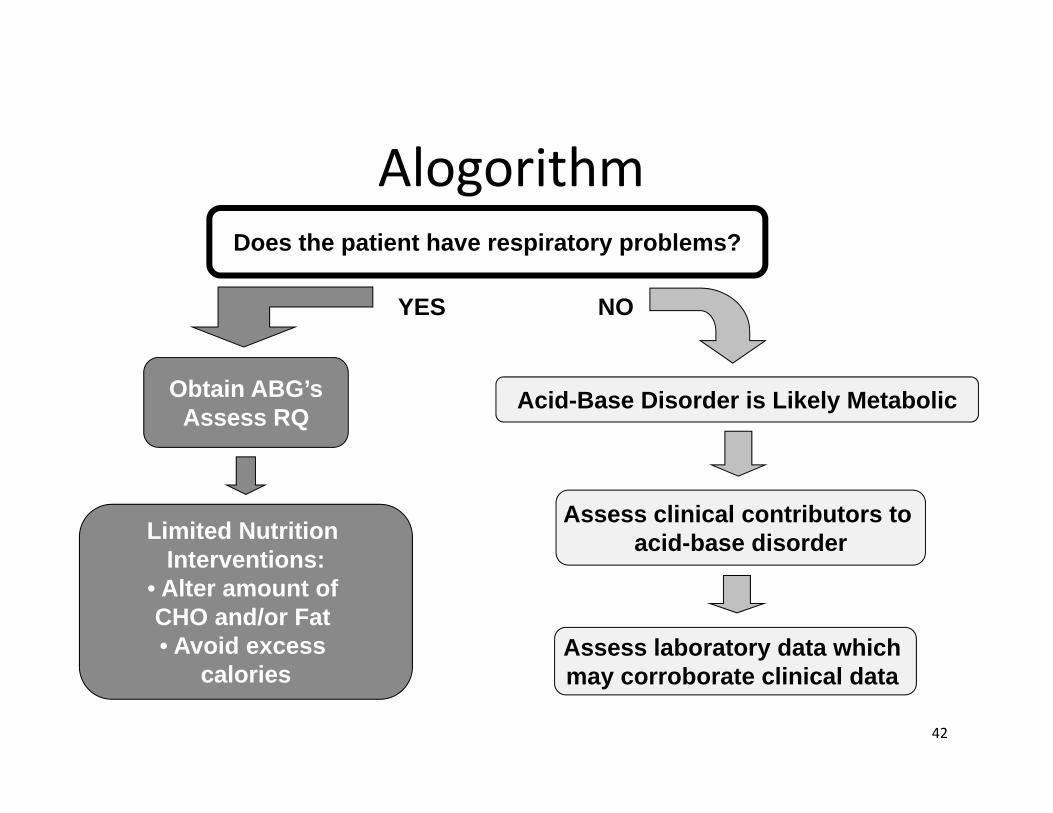
AlogorithmDoes the patient have respiratory problems?
Obtain ABG’sAssess RQ
YES NO
Acid-Base Disorder is Likely Metabolic
Limited Nutrition Interventions:
• Alter amount of CHO and/or Fat • Avoid excess
calories
Assess clinical contributors to acid-base disorder
Assess laboratory data which may corroborate clinical data
Metabolic Acid‐Base Disorder• Factors associated with acidosis٭ Gain of acid [↑ produc on or ↓ loss]٭ Loss of bicarbonate
• Factors associated with alkalosis٭ Loss of acid٭ Gain of bicarbonate
• Exogenous sources• Bicarb precursors
43
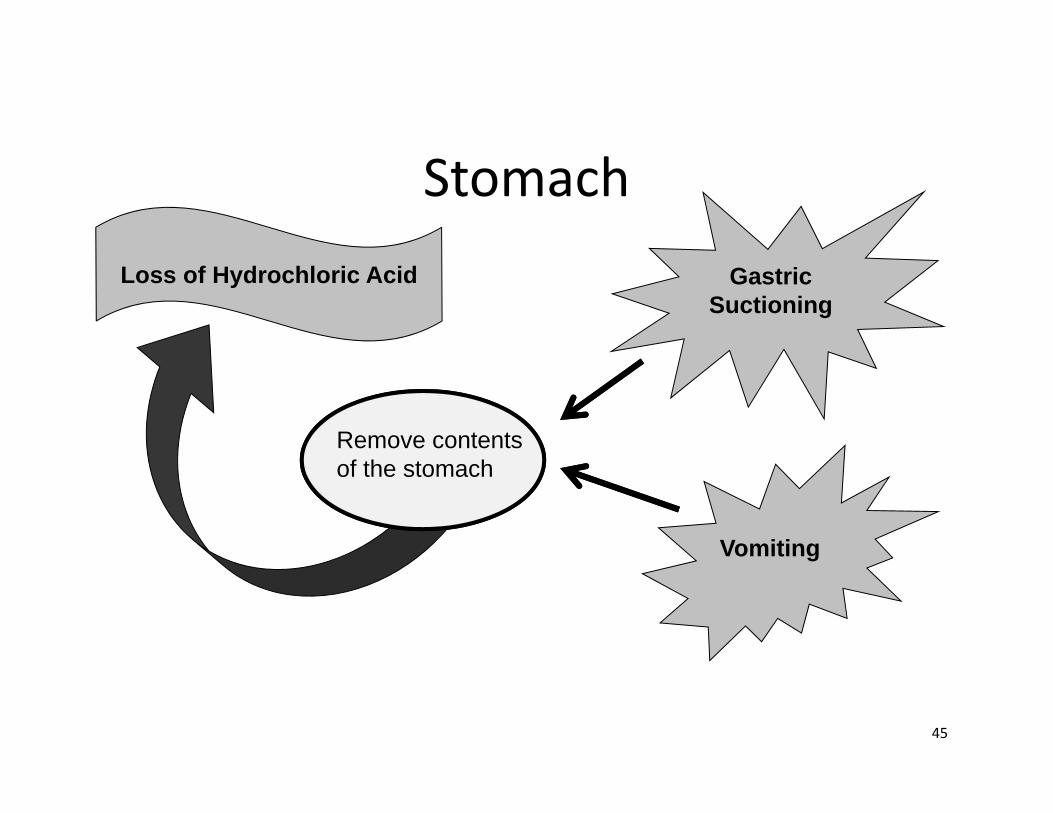
Consider Physiology• Stomach – Gastric acid production• Pancreas – Bicarbonate production• Renal tubules٭ Reabsorption of acid (H+)٭ Reabsorption NaHCO3
• About 400 g/day
44
45
StomachGastric
Suctioning
Vomiting
Loss of Hydrochloric Acid
Remove contents of the stomach
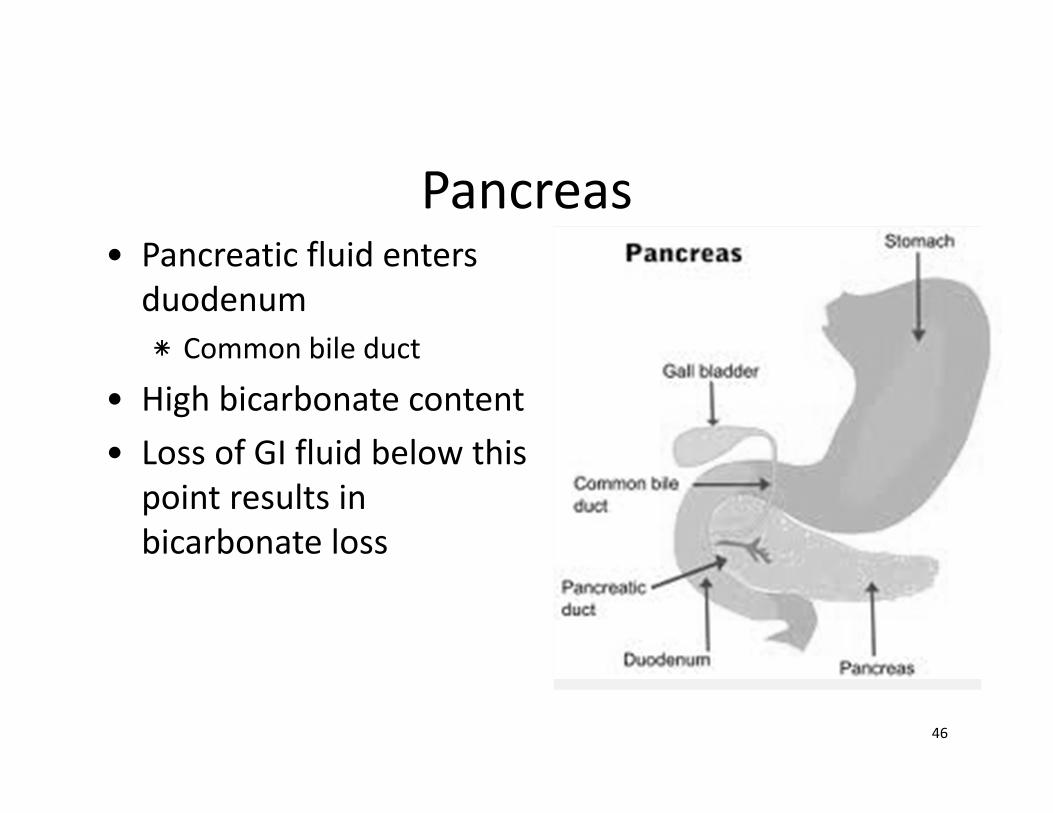
Pancreas• Pancreatic fluid enters duodenum ٭ Common bile duct
• High bicarbonate content• Loss of GI fluid below this point results in bicarbonate loss
46
Acid‐Base Disorder – Case of J.D.• 69 y.o. M admitted to the hospital ٭ Height 70 inches, weight 75 kg
• Chief Complaint: abdominal pain, nausea and vomiting starting one day PTA
• Diagnosis from the ER is SBO • PMH: Right hemicolectomy 9 months ago٭ Colon cancer٭ Otherwise healthy
47
Therapy for J.D.• Conservative therapy implemented ٭ NG suction and fluids
• NG tube output٭ 3200 ml removed immediately in ER٭ 3.5 to 4.5 liters daily after this
• MIV: 5%Dextrose‐0.45%NaCl + 20 mEq KCl/L٭ Rate of 200 mL/hr
• Consult for initiation of PN on day 6 ٭ SBO is not improving
48
49
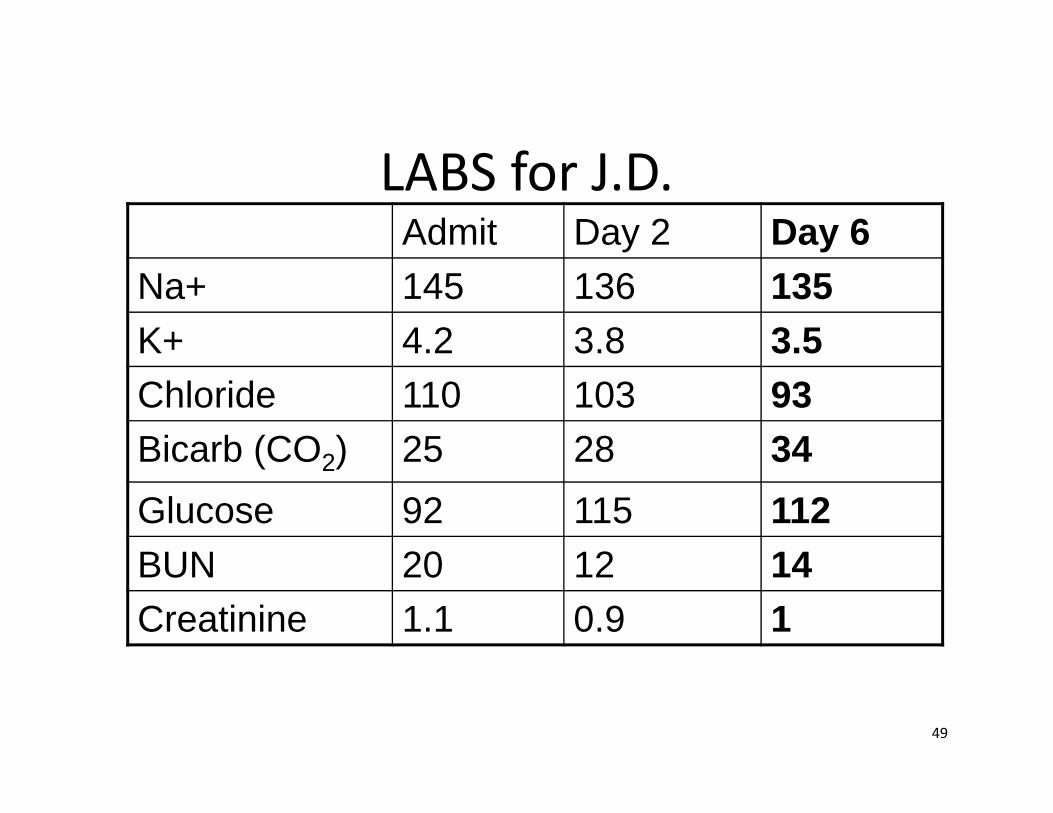
LABS for J.D.Admit Day 2 Day 6
Na+ 145 136 135K+ 4.2 3.8 3.5Chloride 110 103 93Bicarb (CO2) 25 28 34Glucose 92 115 112BUN 20 12 14Creatinine 1.1 0.9 1
Acid‐Base Assessment – J.D.Based on the history and the labs shown, how would you assess J.D. on day 6?A. NG output has resulted in hypovolemiaB. Labs are diluted by the MIV at 200 mL/hrC. Metabolic acidemia (acidosis)D. Metabolic alkalemia (alkalosis)
50
Acid‐Base Assessment – J.D.• What clinical features are important?٭ Vomiting٭ NG suction
• What laboratory values support the assessment?٭ High serum bicarb (34)٭ Low serum chloride (93) ٭ Chloride disproportionately low vs sodium (135)
51
Acid‐Base Assessment – J.D.Based on the history of vomiting/ high NG output, and labs shown (Na 135, Cl 93, HCO3 34), how would you assess J.D. on day 6?A. NG output has resulted in hypovolemiaB. Labs are diluted by the MIV at 200 mL/hrC. Metabolic acidemia (acidosis)D. Metabolic alkalemia (alkalosis)
52
Metabolic Alkalosis – Loss of H+
• Gastric fluid loss٭ Vomiting, NG suction, gastrostomy drainage
• Extracellular loss٭ Shift of H+ into cells٭ Hypokalemia, refeeding syndrome
• Renal loss٭ Diuretics, “contraction alkalosis”
53
Diuretic Actions • Increase sodium delivery to the distal segment of the distal tubule٭ Loop and thiazide diuretics
• Increased distal tubular sodium concentration stimulates aldosterone‐sensitive sodium pump ٭ Increase sodium reabsorption
• Sodium exchanged for H+ (and potassium)٭ Increased H+ [acid] loss to the urine
54
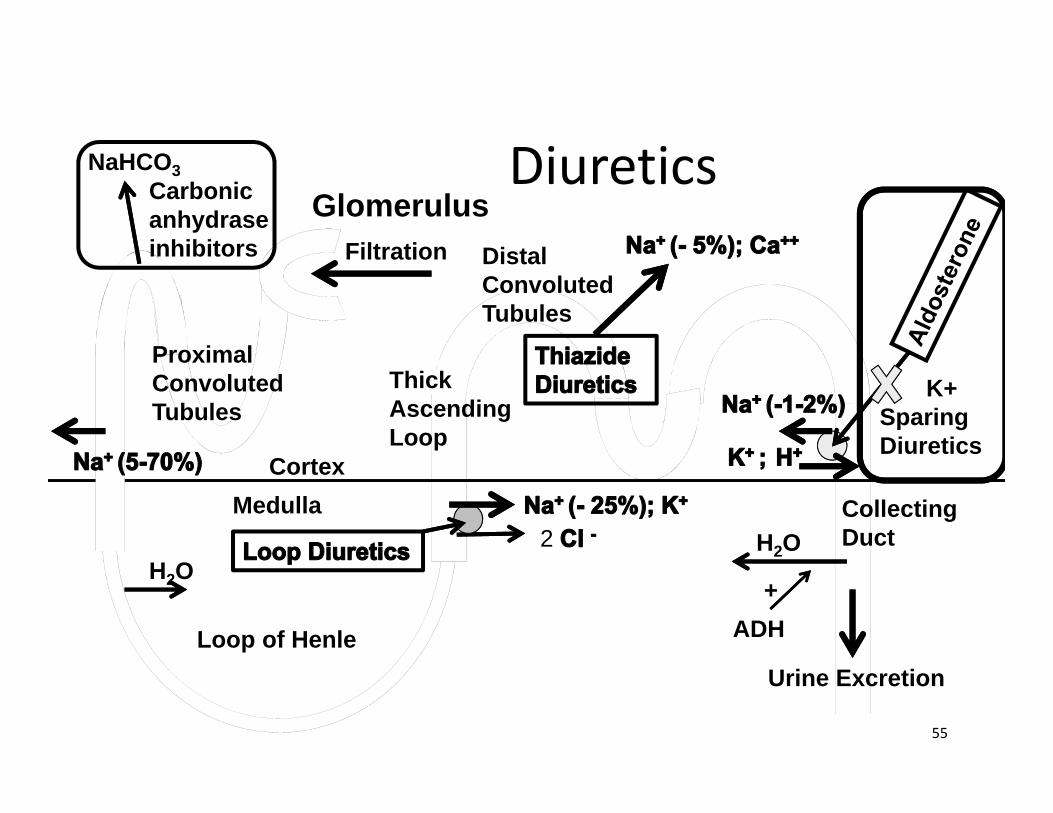
Diuretics
55
GlomerulusFiltration
Proximal Convoluted Tubules
NaHCO3Carbonic anhydrase inhibitors
Loop of Henle
H2O
Distal Convoluted Tubules
Thick Ascending Loop
H2OCollecting Duct
Urine Excretion
CortexMedulla
2
K+ Sparing Diuretics
ADH+
Metabolic Alkalosis – Gain of HCO3
• Exogenous bicarbonate• Exogenous bicarbonate precursors٭ Lactate, acetate, citrate
• Medications
56
Metabolic Alkalosis Management• Avoid bicarb or bicarb precursors٭ Chloride, not acetate, lactate or citrate in PN, fluids
• Provide adequate potassium (avoid hypokalemia)٭ Prevent dehydration with adequate fluid
• Consider total fluid – PN, MIV, medications• Consider total losses – excess GI loss, insensible loss
• Add an H2 antagonist to regimen (?)٭ Reduce acid production in the stomach٭ Reduce subsequent acid loss with NG suction
57
Case of J.D. – Part 2• Day 8: J.D. is taken to the OR ٭ Exploration due to ↑ abdominal distention ٭ Total colectomy with end ileostomy٭ Transferred to ICU post‐op
• Day 12: extubated, transferred to the floor ٭ PN transitioned to tube feeding post‐op ٭ Tube feeding at goal rate (80 mL/hr)
58
J.D.’s Progress Post‐Op• Day 13: Tube feeding continues (at goal) ٭ Clear liquid diet is started٭ Patient c/o nausea, takes only sips of clears
• Day 15 (POD 7): c/o ↑ N, abdominal pain ٭ Temperature to 38.8 C during the night ٭ Ileostomy output 5 liters over the past 24 hours (increased from 2 liters two days ago)
٭ Tube feeding is reduced to “trickle feeds” ٭ PN is to re‐start
59
Labs for J.D.
60
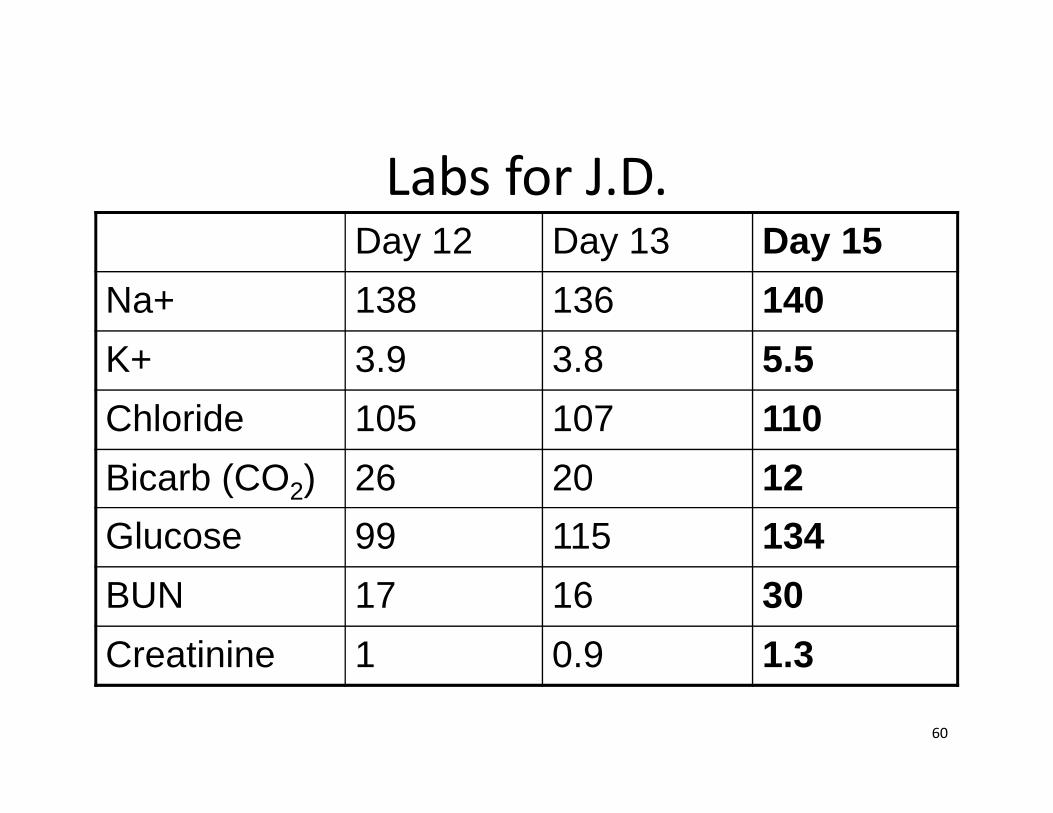
Day 12 Day 13 Day 15Na+ 138 136 140K+ 3.9 3.8 5.5Chloride 105 107 110Bicarb (CO2) 26 20 12Glucose 99 115 134BUN 17 16 30Creatinine 1 0.9 1.3
Acid‐Base Assessment – J.D. Based on the history and the labs shown, what is your assessment on day 15?A. Ileostomy output and high temperature have
resulted in hypovolemiaB. Renal failure has resulted in excessive fluid
retentionC. Metabolic acidemia (acidosis)D. Metabolic alkalemia (alkalosis)
61
Acid‐Base Assessment – J.D. • What clinical features are important in your assessment on day 15? ٭ High ileostomy output٭ Decreasing renal function. Acute renal failure ?
• Likely inadequate fluid replacement• May be reversible with adequate fluids/hydration• Increased ileostomy output?
٭ Infection• Increased temperature and increasing glucose
62
Acid‐Base Assessment – J.D. • What laboratory values are important in supporting the assessment?٭ Low serum bicarb (12)٭ High serum chloride (110) ٭ Disproportionately high chloride vs sodium (140)٭ High anion gap (18)
• Na – Cl – bicarb = anion gap; normal 12 +/‐ 5
٭ Potassium high normal • Potassium shifts out of cells with acidosis
63
Acid‐Base Assessment – J.D. Based on the history and the labs shown, what is your assessment on day 15?A. Ileostomy output and high temperature have
resulted in hypovolemiaB. Renal failure has resulted in excessive fluid
retentionC. Metabolic acidemia (acidosis)D. Metabolic alkalemia (alkalosis)
64
Metabolic Acidosis – Mechanisms • Loss of HCO3
٭ Loss from the GI tract (ileostomy)• Pancreas secretes bicarbonate into the GI tract• HCO3 loss if GI losses distal to pancreatic duct
• Gain of acid٭ Renal failure: retain unmeasured organic acids
• Ion shifts between intra‐ and extra‐cellular٭ Increased serum K –K shifts out, H+ in (acidosis)
• Reduced renal elimination
65
Metabolic Acidosis Management• Reduce chloride provision٭ Use bicarb precursors, chloride in PN, fluids٭ General rule: > 1 mEq acetate/kg/day for effect٭ Up to 2 – 2.5 mEq/kg/day of bicarbonate or bicarbprecursors likely needed with serum bicarb of 12
• Removal of organic acids ٭ Dialysis ٭ Improved renal function
66
Refractory Lactic Acidosis – Case of F.R.• 62 y.o. F with multiple EC fistulae ٭ Home PN for over 1 yr
• Shortage of adult MVI ٭ No IV vitamins for nearly 3 weeks٭ Oral vitamin ordered
• Patient doing poorly when seen by home RN٭ Labs drawn, results show bicarb 13٭ Patient seen in clinic and admitted to hospital
67
Refractory Lactic Acidosis – F.R. • Admitted then transferred to ICU٭ pH < 7.2٭ Lactate > 15٭ Bicarb drip started
• No improvement over next 3 days٭ Bicarb drip at 150 ml/hr x 3 days٭ 3 amps NaHCO3/L = 150 mEq Na+/L
68
Refractory Lactic Acidosis – F.R.
69
70
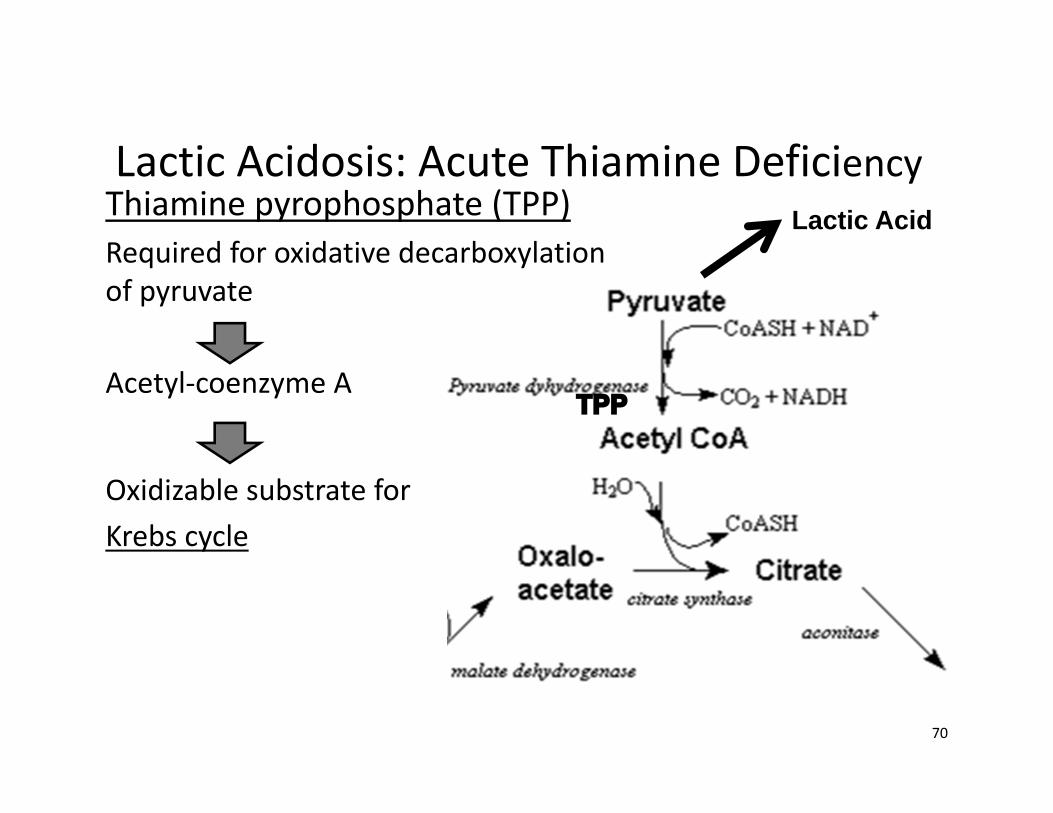
Lactic Acidosis: Acute Thiamine DeficiencyThiamine pyrophosphate (TPP) Required for oxidative decarboxylationof pyruvate
Acetyl‐coenzyme A
Oxidizable substrate for Krebs cycle
Lactic Acid
71
Can You Fit the Pieces Together?
Diarrhea
EnterocutaneousFistulae
PancreaticFistulae
Renal Failure
Alkalosis
Metabolic Acidosis
72
Do these Pieces Fit?
Vomiting
NG Suction
Dehydration
DiuresisFurosemide
Lactated Ringers
MetabolicAlkalosis
Acidosis
Self‐Assessment Question 4In which clinical situation is bicarbonate loss from the GI tract likely to be highest?A. Nasogastric suctioningB. Aggressive diuresisC. Protracted vomitingD. Prolonged diarrhea
73
Self‐Assessment Question 5Which of the following serum electrolyte patterns is associated with metabolic alkalosis? A. Decreased chloride with sodium disproportionately
high compared to chlorideB. Elevated bicarbonate and chloride with sodium low
compared to chlorideC. Decreased chloride and proportionately low sodium D. Elevated chloride and proportionately high sodium
74
Self‐Assessment Question 6The primary mechanism for the acid‐base disorder associated with acute renal failure is:A. Inability to filter bicarbonate B. Lack of bicarbonate reabsorption in the distal
tubulesC. Retention of organic acids D. Loss of hydrogen ion when potassium is retained
75
Self‐Assessment Question 7Which of the following electrolytes are primarily intracellular?A. Sodium, potassium, chlorideB. Phosphorus, potassium, magnesiumC. Phosphorus, sodium, magnesiumD. Chloride, calcium, phosphorus
76
Self‐Assessment Question 8Which of the following electrolytes tend to decrease significantly with initiation of PN in a severely malnourished patient? A. Sodium, potassium, chlorideB. Phosphorus, potassium, magnesiumC. Phosphorus, sodium, magnesiumD. Chloride, calcium, phosphorus
77
Electrolyte Inter‐Relationships• Sodium and water٭ Is there a sodium problem or a water problem?
• Potassium, magnesium and phosphorus٭ Intracellular electrolytes
• Serum concentration is low relative to body content• Shifts in and out of cells change serum concentration
٭ Renal elimination
78
Potassium, Magnesium, Phosphorus
• Affected by renal function• Cellular damage٭ Different concentrations in different types of cells ٭ Hemolysis RBC٭ Tumor lysisWBC (lymphocyte)٭ RhabdomyolysisMuscle
• Shifts between intracellular and extracellular
79
Refeeding Syndrome• Patients at risk٭ Severely malnourished٭ Significant weight loss, esp. over several weeks٭ Calorie/energy malnutrition ٭ Aggressive nutrition, esp. with CHO
• Shift intracellular electrolytes from serum back into the cell
• Risk of cardiac failure 80
Refeeding Syndrome• Serum electrolyte decreases drive by CHO٭ Phosphorus required to phosphorylate glucose٭ Phosphorus is part of ATP٭ Potassium follows glucose into cells
• Fluid٭ Heart failure
• Fat and protein٭ Can be more aggressive with minimal risk
81
Refeeding Syndrome• Not exclusive to PN occurs with po and EN• Start with low CHO٭ 10% dextrose in PN٭ 100 g CHO/day
• Above standard phosphorus, potassium, magnesium
• Average time to stabilize electolytes: 5‐7 days٭ Daily labs until stable
82
Self‐Assessment Question 7Which of the following electrolytes are primarily intracellular?A. Sodium, potassium, chlorideB. Phosphorus, potassium, magnesiumC. Phosphorus, sodium, magnesiumD. Chloride, calcium, phosphorus
83
Self‐Assessment Question 8Which of the following electrolytes tend to decrease significantly with initiation of PN in a severely malnourished patient? A. Sodium, potassium, chlorideB. Phosphorus, potassium, magnesiumC. Phosphorus, sodium, magnesiumD. Chloride, calcium, phosphorus
84
QUESTIONS
Carol J. Rollins, MS, RD, CNSC, PharmD, BCNSPCoordinator, Nutrition Support Team
The University of Arizona Medical Center, Main Campus
[email protected]‐694‐4618
85





















![Parenteral Nutrition[1]](https://img.pdfslide.net/doc/110x75/5469fe10af79593b558b4f0d/parenteral-nutrition1.jpg)







