Embed Size (px)
Citation preview

2012/3/23
1
Mantle Cell Lymphoma (MCL):
Focused On Treatment
Bor-Sheng Ko, M.D., Ph.D.
Attending Physician and Assistant ProfessorDepartment of Internal Medicine
National Taiwan University Hospital, Taiwan2012-Mar-17
The incidences of MCL is changing.
US: Annual adjusted incidence ~ 0.6/100,000
Stage IV disease is increasing
Cancer 2008;113:791

2012/3/23
2
The classification of MCL is also changing:
• Diagnostic hallmark:
– CD5+CD23- mature B-cell neoplasm
– CCND1 gene/cyclin D1 protein overexpression;
t(11;14)(q13;q32)
• WHO classification:
– Classic: Sox11 nuclear over-expression
– Blastoid (pleomorphic)
– Marginal-zone like
– Small cell
Small-cell MCL represents a CLL-like clinical
phenotype:
• Still CCND-1/cyclin D1 overepxression
• Still CD5+CD23-
• Low Ki-67 index
• Low proliferation signature in
microarray
• Low Sox11 expression
• Good survival
Cancer Sci 2011;102:1734

2012/3/23
3
I am MCL !?
MCL is a disease with poor prognosis.
Take dis-advantages of both:
• Low-grade NHL: No cure
• High-grade NHL: Rapid progression
Overall survival
Overall survival
Blood 2000;95:2253

2012/3/23
4
Prognostic index for MCL
Simplified score:
LR: 0-3
IR: 4-5
HR: 6-11
IPI MIPI
Blood 2008;111: 558
Treatment scheme of MCL
InductionInduction ConsolidationConsolidation MaintenanceMaintenance
Proper induction Proper induction
regimens?regimens?
Role of AutoRole of Auto--HSCT?HSCT?
Role of Role of AlloAllo--HSCT?HSCT?Role of Role of
RituximabRituximab??
Roles of novel Roles of novel
agents?agents?
Risk
Stratification

2012/3/23
5
Choices of Induction Regimens..
Stepping from CHOP:
Rituximab improved response, but6666
TTF: All patients
encountered
PFS: CR+PR
encountered
P=0.013 P=NS
• German Low Grade Lymphoma
Study Group (GLSG)
• R-CHOP vs CHOP, N=62 vs 60
• Advanced MCL
• Prospective randomized trial
J Clin Oncol 2005;23:1984

2012/3/23
6
Evolving for intensive chemotherapy:
MDACC concepts with dose-intensive C/T
• Hyper-CVAD/MA regimen
Later changed to
16.7 mg/m2 x 3d
J Clin Oncol 1998;16:3803
MDACC cohort:
Hyper-CVAD+HSCT improved MCL outcome.
• Phase II study, age<65 y/o
• 55 cases with Stage II/IV MCL,
25 untreated
• 38% CR and 55.5% PR
• All responding cases go to
HSCT: 26 auto- and 8 allo-
• All them went to CR after
HSCT
• Overall 3-yr PFS 42% and 3-yr
OS 56%
• Allo- better than Auto-
• Untreated better than relapsed
J Clin Oncol 1998;16:3803
Historical control
Previously untreated cohort

2012/3/23
7
MDACC cohort:
Long-term results for Hyper-CVAD+auto-HSCT
Cancer 2003;98:2630
• N=33
• TBI+Cy for conditioning
• B2-microglobin and Anderson tumor score(TS) are with prognostic
significance
Upgrading MDACC cohort:
R-Hyper-CVAD/R-MA further improved outcome. (1)
Overall survival• Phase II trial, N=97
• 6-8 cycles
• Subtype: blastoid 18%,
nodular 16%
• CR rate 87%, response rate
97%P=0.047
J Clin Oncol 2005;23:7013

2012/3/23
8
Upgrading MDACC cohort:
R-Hyper-CVAD/R-MA further improved outcome. (2)
High b2m and elder age indicated
worse PFS
Progression-free survival
J Clin Oncol 2005;23:7013
Upgrading MDACC cohort:
R-Hyper-CVAD/R-MA further improved outcome. (3)
• 10-year follow-up
Br J Haematol 2010;150:200

2012/3/23
9
Problems in R-hyper-CVAD/R-MA
• Outside MDACC: inferior outcome6.
• Higher toxicity:
– 8% treatment-related death
– Increased 2nd malignancies:
Urological cancers,
AML/MDS
Eu J Haematol 2010;85:371
In J Haematol 2010;92:25
Ann Oncol 2002;12:318
N=154,
A.D.1994-2000 for Hyper-CVAD/MA
Omitting HDMTX may reduce toxicity.
• CALGB phase II trial, N=78, 2001-2004
• High M-IPI: 12%
• R-maxiCHOP6.R-EA6..CBV/autoHSCT6.R-maintenance
• 2 treatment-related death
J Clin Oncol 2009;27: 6101
2012/3/23
10
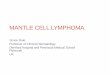
Early treatment of MCL may not result in better
outcome6.
• N=31 (observation) vs 66 (early treatment)
• Higher M-IPI in early treatment
J Clin Oncol 2009;27: 1209
Does upfront auto-HSCT work??

2012/3/23
11
Upfront auto-HSCT improved PFS.
• European MCL network
• Phase III randomized control trial
PFS OS
Blood 2005;105: 2677
Those who has CR before auto-HSCT benefited
the most.
CR before auto-HSCT PR before auto-HSCT
Blood 2005;105: 2677

2012/3/23
12
MDACC cohort6again:
Upfront auto-HSCT+R provided survival plateau6
but delayed auto-HSCT+/-R not!
Blood 2009; 113:4144
• Auto-HSC mobilization frequently failed after 6 cycles of R-HyperCVAD/R-MA
Nordic Group:
Impacts of rituximab and Ara-C on MCL treatment
Blood 2008;112: 2687

2012/3/23
13
Who is the candidate for allo-HSCT??
Still MDACC cohort6.:
G-V-L effects documented in NST
• Myeloablative protocol (TBI+Cy/BEAM) resulted in high TRM (38%)
and 55% 3-yr OS in advanced MCL.
• NST by FCR conditioning
• N=18, relapsed and refractory MCL after C/T and/or auto-HSCT
• 89% in chemo-sensitive relapse
J Clin Oncol 2003;21: 4407
Ann Oncol 1999;10: 1293

2012/3/23
14
Blood 2009; 113:4144
Leuk Lymphoma 2009;50:1239
Allo-HSCT provided the last chance to be cured
in relapse/refractory MCL.
FHCRC experiences of NST in MCL:
•NST with TBI (2Gy)+F
• MUD (n=17) and sibling donors (n=16) for relapsed/refractory MCL
• Most chemo-resistant
Blood 2004;104: 3535

2012/3/23
15
Is rituximab maintenance required?
Rituximab maintenance prolonged PFS in MCL.
• GLSG study, Phase III randimized control trial
• Induction with R-FCM
• N=29 (observation) vs 28 (maintenance)
• R maintenance: 4 times weekly on 3rd and 9th month
P=0.049
Blood 2006;108: 4003

2012/3/23
16
MDACC cohort:
Auto-HSCT or rituximab maintenance may be
equally effective.
• Retrospective analysis,
2005-2009
• RHCVAD alone (n=16) vs
autoHSCT (n=17) vs
R maintenance (n=11)
• R: q6m for 2 yr
Bone Marrow Transplant 2011 Nov 14, doi:10.1038/bmt.2011.218
Summary
InductionInduction
ConsolidationConsolidation
MaintenanceMaintenance
•• Intensive regimen Intensive regimen
requiredrequired
•• RituximabRituximab requiredrequired
•• RR--HyperCVADHyperCVAD/R/R--MA is MA is
good, but can be better.good, but can be better.
•• Upfront autoUpfront auto--HSCT is HSCT is
required if no R.required if no R.
•• If R added, autoIf R added, auto--HSCT? HSCT?
may still be required.may still be required.
•• AlloAllo--HSCT is the only HSCT is the only
way to cure way to cure
relapse/refractory MCLrelapse/refractory MCL
•• R R maintmaint. can . can
improve outcome if improve outcome if
no no autoHSCTautoHSCT..
•• But after autoBut after auto--
HSCT?HSCT?
•• Maybe preMaybe pre--emptive emptive
strategystrategy

2012/3/23
17
Novel Agents
Cyclin D1 over-expression is the key factor of
MCL pathogenesis.
Blood 2011;117: 26

2012/3/23
18
Classification of novel drugs:
Semin Cancer Biol 2011;21: 335
Novel targeted drugs for MCL
• Proteasome inhibitors
• mTOR inhibitors
• Other chemotherapeutic agents
• Radio-immunotherapy
• Other monoclonal antibodies (anti-CD22, etc)
• Serine/threonine or tyrosine kinase inhibitors
• HiDAC inhibitors
• PI3K/Akt inhibitors
• IMiDs

2012/3/23
19
Bortezomib is effective in relapsed/refractory MCL.
• Bortezomib single agent for relapsed/refractory MCL
• N=155
• Response rate 32%, with 8% CR/CRu
Ann Oncol 2009;20: 525
VcR-HyperCVAD is effective for induction in MCL.
• Phase II study, multi-center in USA
• N=27, 80% M-IPI intermediate to high
• Median age = 61 y/o
• Overall response 90%, CR/CRu rate 77%
• No TRM
• 9 with Gr3/4 polyneuropathy
PFSOS
Br J Haematol 2011;155: 190

2012/3/23
20
Temsirolimus is also effective in relapsed/refractory
MCL.
• Phase III randomized double-blinded trial, multi-nation
• N=54 for each, with 8% blastoid
• OR: 22% vs 6% vs 2%, CR rate: 2% vs 0% vs 2%
• ~60% experienced Gr 3/4 thrombocytopenia in 175/75 group.
Ann Oncol 2009;20: 525
Bedamustine is also effective in treating MCL.
• DNA Alkylators with durable effects..
Anti-metabolite effects
• Single agent for phase II trial in Japan:
ORR =100%, CR/Cru rate 73% (n=11)
• B+R: phase II trial in USA
n=12
ORR 92%, CR/CRu rate 59%
Cancer Sci 2010;101: 2059
J Clin Oncol 2008;26: 4473

2012/3/23
21
Radioimmunotherapy (RIT)
• 90Y-ibritumomab tiuxetan (Zevalin)131I-tositumomab (Bexxar)
• Zevalin: 30% ORR and 6m EFS in relapsed/refractory MCL
• Frontline therapy with zevalin: increased CR rate (55% vs 13%) and 31m EFS
• Bexxar: combined in auto-HSCT conditioning in FHCRC for relapsed/refractory MCL
3-yr PFS 61% and 3-yr OS 93%
Blood 2007;110: 389
Clin Oncol 2009;27: 5213
J Clin Oncol 2007;25: 1396
Thanks for Your AttentionThanks for Your AttentionThanks for Your AttentionThanks for Your Attention


![Impact of Mantle Cell Lymphoma Contamination of Autologous … · 2021. 5. 23. · MCL patients ultimately relapses, then facing a poor prognosis [2,3]. As lymphoma con-tamination](https://img.pdfslide.net/doc/110x75/61313cf11ecc515869449bfa/impact-of-mantle-cell-lymphoma-contamination-of-autologous-2021-5-23-mcl-patients.jpg)