Embed Size (px)
Citation preview
APC
CTNNB1
EGFR
IDH1
KRAS
NOTCH1
PIK3CA
PTEN
Rapid Tumor Genotyping in Solid Tumors
AKT1
BRAF
KIT
MAP2K1
TP53
NRAS

Growth Factor
Receptortyrosine kinase
RAS
MAP2K1(MEK1)
RAF
ERK
Proliferation Survival
PI3K
AKT
mTOR PTEN
P P
Mitogen Activated Protein Kinase (MAPK) Pathway
Tumor Genotyping
www.genpathdiagnostics.com/oncology/OnkoMatch
Personalized Medicine Requires Personalized DiagnosticsBiological discoveries utilizing advanced sequencing techniques are unraveling the key drivers of cancer. These discoveries are now entering the clinic by personalizing treatment based on molecular profile. For example, conventional testing in lung cancer relies on 1 or 2 mutational events (EGFR
and ALK) but research groups such as the Lung Cancer Consortium1 are profiling patients across several oncogenes implicated in oncogenesis. This multidimensional view of cancer is taking hold in various solid tumors.
1. The Lung Cancer Mutation Consortium (LCMC) is an NCI sponsored initiative made up of 14 leading cancer centers across the country.
Major pathways have been identified in cancer proliferation including:
Mitogen Activated Protein Kinase (MAPK) signaling: EGFR, BRAF, KRAS, NRAS, MAP2K1, KIT
mTOR: PIK3CA, AKT, PTEN
Tumor Suppressor and DNA Repair: TP53, PTEN, APC
Cell Signaling: NOTCH1, CTNNB1
The molecular profiling of cancer patients is becoming the standard for disease management in top medical centers.
www.genpathdiagnostics.com/oncology/OnkoMatch
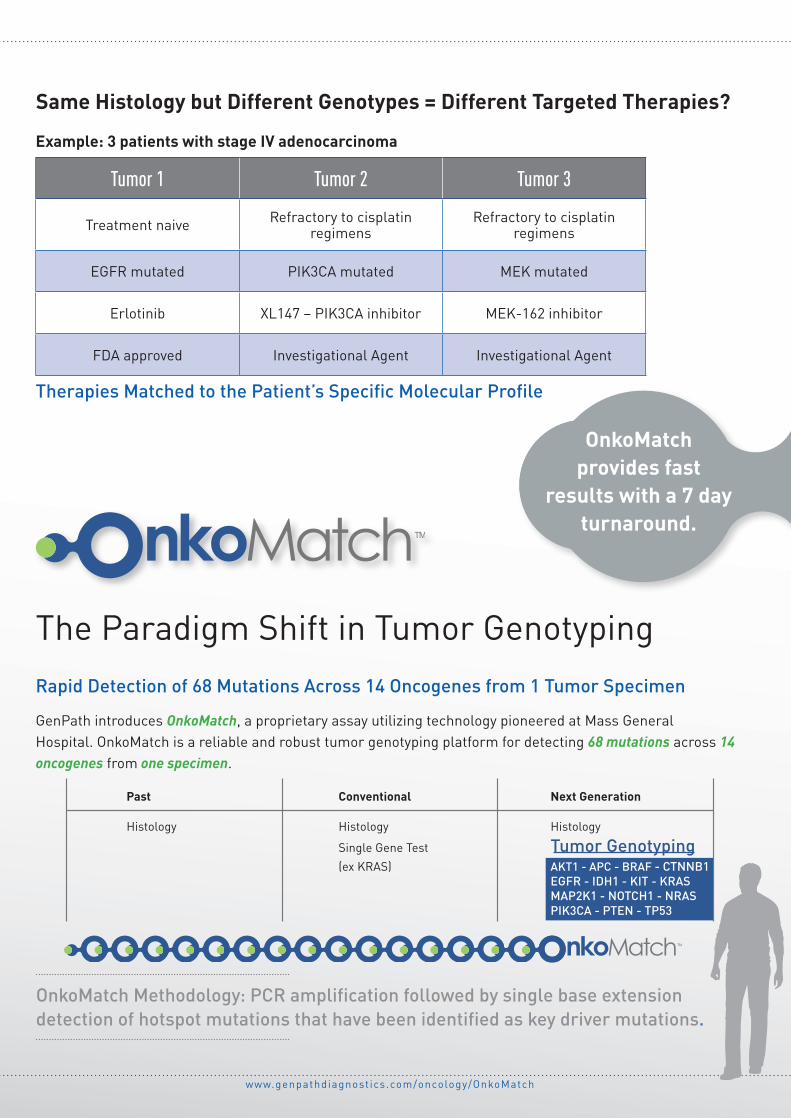
Same Histology but Different Genotypes = Different Targeted Therapies?
The Paradigm Shift in Tumor GenotypingRapid Detection of 68 Mutations Across 14 Oncogenes from 1 Tumor Specimen
GenPath introduces OnkoMatch, a proprietary assay utilizing technology pioneered at Mass General Hospital. OnkoMatch is a reliable and robust tumor genotyping platform for detecting 68 mutations across 14 oncogenes from one specimen.
Tumor 1 Tumor 2 Tumor 3
Treatment naive Refractory to cisplatin regimens
Refractory to cisplatin regimens
EGFR mutated PIK3CA mutated MEK mutated
Erlotinib XL147 – PIK3CA inhibitor MEK-162 inhibitor
FDA approved Investigational Agent Investigational Agent
Example: 3 patients with stage IV adenocarcinoma
Therapies Matched to the Patient’s Specific Molecular Profile
OnkoMatch Methodology: PCR amplification followed by single base extension detection of hotspot mutations that have been identified as key driver mutations.
Past Conventional Next Generation
Histology Histology Histology
Single Gene Test Tumor Genotyping (ex KRAS) AKT1 - APC - BRAF - CTNNB1 EGFR - IDH1 - KIT - KRAS MAP2K1 - NOTCH1 - NRAS PIK3CA - PTEN - TP53
OnkoMatch provides fast
results with a 7 day turnaround.
APCCTNNB1
EGFR
IDH1
KRAS
NOTCH1 PIK3CA
PTEN
BRAF
MAP2K1
TP53
NRAS
AKT1 KIT
Tumor Genotyping
EGFR
KRAS
Single Gene Test
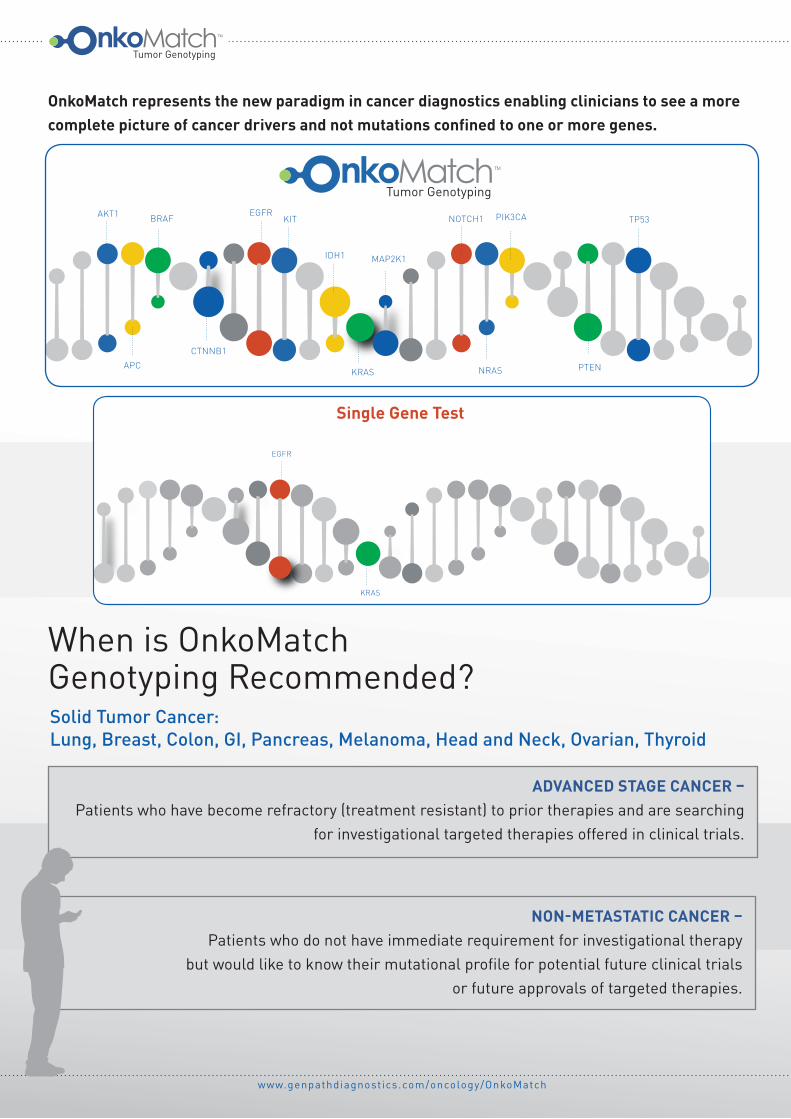
OnkoMatch represents the new paradigm in cancer diagnostics enabling clinicians to see a more complete picture of cancer drivers and not mutations confined to one or more genes.
Tumor Genotyping
www.genpathdiagnostics.com/oncology/OnkoMatch
Solid Tumor Cancer: Lung, Breast, Colon, GI, Pancreas, Melanoma, Head and Neck, Ovarian, Thyroid
ADVANCED STAGE CANCER – Patients who have become refractory (treatment resistant) to prior therapies and are searching
for investigational targeted therapies offered in clinical trials.
NON-METASTATIC CANCER – Patients who do not have immediate requirement for investigational therapy
but would like to know their mutational profile for potential future clinical trials or future approvals of targeted therapies.
When is OnkoMatch Genotyping Recommended?
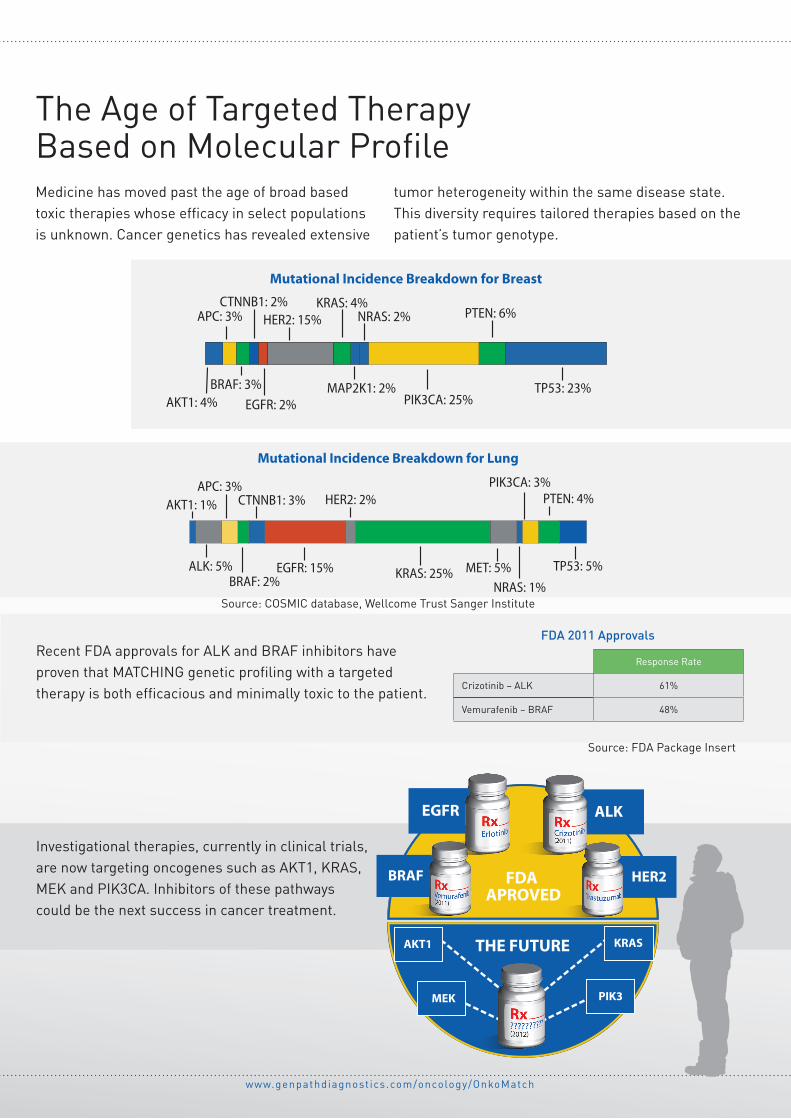
Mutational Incidence Breakdown for Lung
TP53: 5%
PTEN: 4%PIK3CA: 3%
NRAS: 1%MET: 5%KRAS: 25%
HER2: 2%
EGFR: 15%
CTNNB1: 3%
BRAF: 2%
APC: 3%
ALK: 5%
AKT1: 1%
BRAF HER2
EGFR ALK
MEK PIK3
KRASAKT1
FDA APROVED
THE FUTURE
HER2: 15%CTNNB1: 2%
EGFR: 2%AKT1: 4%
APC: 3%
BRAF: 3%
KRAS: 4%
MAP2K1: 2%
NRAS: 2%
PIK3CA: 25%
PTEN: 6%
TP53: 23%
Mutational Incidence Breakdown for Breast
www.genpathdiagnostics.com/oncology/OnkoMatch
The Age of Targeted Therapy Based on Molecular ProfileMedicine has moved past the age of broad based toxic therapies whose efficacy in select populations is unknown. Cancer genetics has revealed extensive
tumor heterogeneity within the same disease state. This diversity requires tailored therapies based on the patient’s tumor genotype.
Response Rate
Crizotinib – ALK 61%
Vemurafenib – BRAF 48%
FDA 2011 ApprovalsRecent FDA approvals for ALK and BRAF inhibitors have proven that MATCHING genetic profiling with a targeted therapy is both efficacious and minimally toxic to the patient.
Investigational therapies, currently in clinical trials, are now targeting oncogenes such as AKT1, KRAS, MEK and PIK3CA. Inhibitors of these pathways could be the next success in cancer treatment.
Source: COSMIC database, Wellcome Trust Sanger Institute
Source: FDA Package Insert
Tumor Genotyping
www.genpathdiagnostics.com/oncology/OnkoMatch
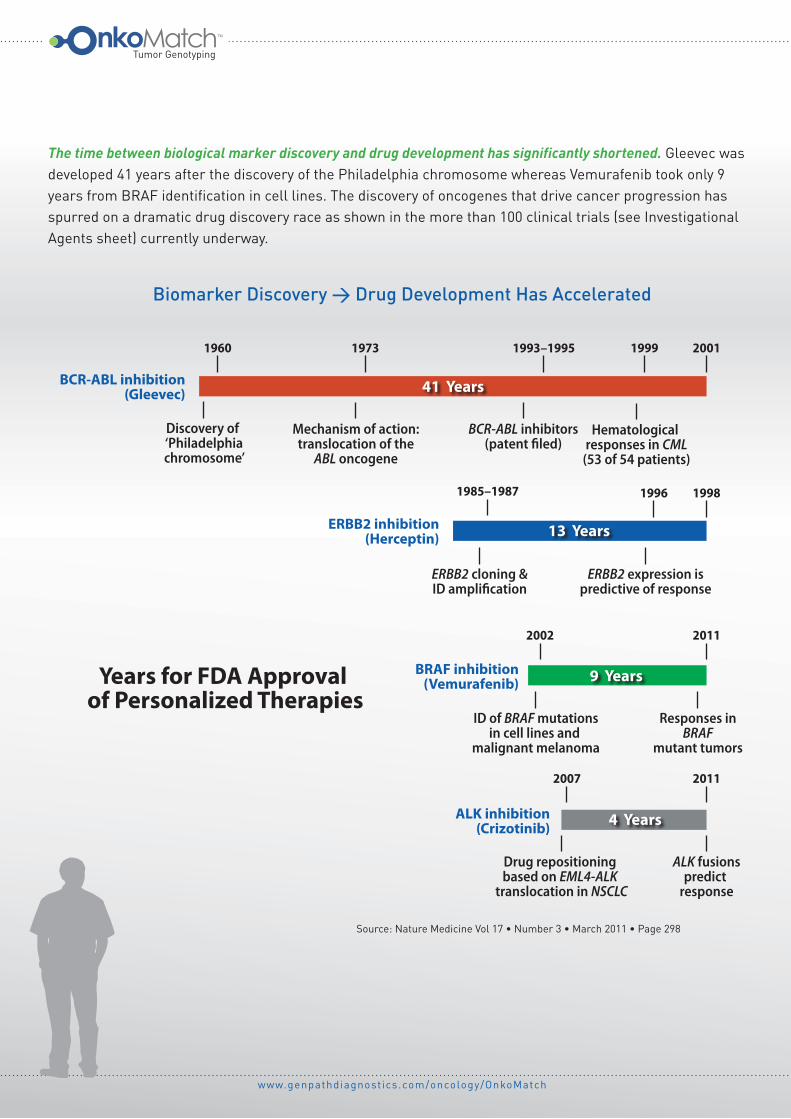
Source: Nature Medicine Vol 17 • Number 3 • March 2011 • Page 298
Biomarker Discovery → Drug Development Has Accelerated
41 Years
13 Years
9 Years
4 Years
1960 1973 1999
1996
2002 2011
2007 2011
1998
20011993–1995
1985–1987
Discovery of ‘Philadelphiachromosome’
Mechanism of action:translocation of the
ABL oncogene
BCR-ABL inhibitors(patent �led)
Hematological responses in CML
(53 of 54 patients)
ERBB2 cloning &ID ampli�cation
ERBB2 expression ispredictive of response
ID of BRAF mutationsin cell lines and
malignant melanoma
Responses in BRAF
mutant tumors
ALK fusionspredict
response
Drug repositioning based on EML4-ALK
translocation in NSCLC
BCR-ABL inhibition(Gleevec)
ERBB2 inhibition(Herceptin)
BRAF inhibition(Vemurafenib)
ALK inhibition(Crizotinib)
Years for FDA Approval of Personalized Therapies
The time between biological marker discovery and drug development has significantly shortened. Gleevec was developed 41 years after the discovery of the Philadelphia chromosome whereas Vemurafenib took only 9 years from BRAF identification in cell lines. The discovery of oncogenes that drive cancer progression has spurred on a dramatic drug discovery race as shown in the more than 100 clinical trials (see Investigational Agents sheet) currently underway.
www.genpathdiagnostics.com/oncology/OnkoMatch
Tumor Genotyping from MGH to your practice Technology used routinely at Mass General Hospital is now available nationally in community oncology practices.
OnkoMatch tumor genotyping technology has been licensed exclusively from Massachusetts General Hospital’s (MGH) Division of Translational Medicine.1 Dr. John Iafrate, MD, PhD (Director of Molecular Diagnostics at MGH and Associate Professor of Pathology, Harvard Medical School) and his team at MGH designed a multiplex genotyping assay for solid tumors based on SNaPshot2 technology. GenPath leveraged MGH’s sophisticated DNA extraction method and mutational analysis for detecting multiple mutations across several oncogenes in one test.
Tumor genotyping of solid tumors such as lung are part of MGH’s normal protocol for patient management. “Analysis by SNaPshot Multiplex System is now part of the routine pathological assessment of lung cancers at Mass General Hospital”3, John Iafrate, MD, PhD.
Patients at MGH with detected mutations may be placed in appropriate clinical trials that target the oncogenic pathway. More than 1,500 genotypes have been reported into MGH’s medical records reflecting the wide diversity of tumor profiles.
Annals of Oncology 22: 2616–2624, 2011
doi:10.1093/annonc/mdr489
Published online 9 November 2011original article
Implementing multiplexed genotyping of non-small-celllung cancers into routine clinical practice
L. V. Sequist1,2*, R. S. Heist1,2, A. T. Shaw1,2, P. Fidias1,2, R. Rosovsky1,2,3, J. S. Temel1,2,I. T. Lennes1,2, S. Digumarthy2,4, B. A. Waltman2, E. Bast1, S. Tammireddy1, L. Morrissey1,A. Muzikansky2,5, S. B. Goldberg1,2, J. Gainor2,6, C. L. Channick2,7, J. C. Wain2,8,H. Gaissert2,8, D. M. Donahue2,8, A. Muniappan2,8, C. Wright2,8, H. Willers2,9,D. J. Mathisen2,8, N. C. Choi2,9, J. Baselga1,2, T. J. Lynch10, L. W. Ellisen1,2, M. Mino-Kenudson2,11,M. Lanuti2,8, D. R. Borger1,2, A. J. Iafrate2,11, J. A. Engelman1,2 & D. Dias-Santagata2,11
1Massachusetts General Hospital Cancer Center, Boston; 2Harvard Medical School, Boston; 3The Mass General/North Shore Cancer Center, Danvers; 4Department of
Radiology; 5Department of Biostatistics; 6Department of Medicine; 7Division of Pulmonary and Critical Care Medicine; 8Division of Thoracic Surgery; 9Department of
Radiation Oncology, Massachusetts General Hospital, Boston; 10Yale University School of Medicine and Yale Cancer Center, New Haven; 11Department of Pathology,
Massachusetts General Hospital, Boston, USA
Received 14 August 2011; revised 17 September 2011; accepted 26 September 2011
Background: Personalizing non-small-cell lung cancer (NSCLC) therapy toward oncogene addicted pathway
inhibition is effective. Hence, the ability to determine a more comprehensive genotype for each case is becoming
essential to optimal cancer care.
Methods: We developed a multiplexed PCR-based assay (SNaPshot) to simultaneously identify >50 mutations in several
key NSCLC genes. SNaPshot and FISH for ALK translocations were integrated into routine practice as Clinical Laboratory
Improvement Amendments-certified tests. Here, we present analyses of the first 589 patients referred for genotyping.
Results: Pathologic prescreening identified 552 (95%) tumors with sufficient tissue for SNaPshot; 51% had ‡1mutation identified, most commonly in KRAS (24%), EGFR (13%), PIK3CA (4%) and translocations involving ALK (5%).
Unanticipated mutations were observed at lower frequencies in IDH and b-catenin. We observed several associations
between genotypes and clinical characteristics, including increased PIK3CA mutations in squamous cell cancers.
Genotyping distinguished multiple primary cancers from metastatic disease and steered 78 (22%) of the 353 patients
with advanced disease toward a genotype-directed targeted therapy.
Conclusions: Broad genotyping can be efficiently incorporated into an NSCLC clinic and has great utility in
influencing treatment decisions and directing patients toward relevant clinical trials. As more targeted therapies are
developed, such multiplexed molecular testing will become a standard part of practice.
Key words: carcinoma, non-small cell, genotype, molecular targeted therapy
introduction
Certain genetically defined cancers are ‘oncogene addicted’ toactivated kinases and are thereby highly sensitive to drugs thatselectively inhibit the corresponding kinase. Employinggenotype-based therapy has been highly successful in chronicmyelogenous leukemia, gastrointestinal stromal tumors, non-small-cell lung cancer (NSCLC) and melanoma, and in manyinstances, the targeted agent is far more effective thantraditional chemotherapy [1–9]. This shifting paradigm hasdramatically impacted lung cancer treatments. Until recently,therapeutic options for advanced NSCLC were limited to
chemotherapies that were ‘personalized’ only by considering
the side-effect profiles of a number of similar modestly effective
regimens. Response rates were typically 20%–30% and
progression-free survival (PFS) was 3–5 months [10–13]. But
now, we know that determining NSCLC genotype can inform
the most effective personalized therapies. Patients with
mutations in the epidermal growth factor receptor (EGFR) gene
benefit from EGFR tyrosine kinase inhibitors (TKIs) with
a response rate of �75%, PFS of 9–13 months and improved
quality of life compared with chemotherapy [8, 14–16].
Similarly, patients with EML4-ALK translocations have a 60%
response rate, 9-month PFS and a low degree of toxicity when
treated with crizotinib, an ALK TKI [6].Although these landmark studies have focused on a single or
small number of genetic mutations, there is an increasing
motivation to develop technologies that can simultaneously
determine the mutational status of many genes. Responding to
original
article
*Correspondence to: Dr L. V. Sequist, Massachusetts General Hospital Cancer Center,
55 Fruit Street, Professional Office Building room 212, Boston, MA 02114, USA. Tel: +1-617-726-7812; Fax: +1-617-724-3166; E-mail: [email protected] and Dr Dora
Dias-Santagata, Translational Research Laboratory, Massachusetts General Hospital,
55 Fruit Street, Jackson 1028, Boston, MA 02114, USA. Tel: +1-617-724-1261; Fax:+1-617-726-6974; E-mail: [email protected]
ª The Author 2011. Published by Oxford University Press on behalf of the European Society for Medical Oncology.
All rights reserved. For permissions, please email: [email protected]
at New
York M
edical College H
ealth Sciences Library on Novem
ber 29, 2011http://annonc.oxfordjournals.org/
Dow
nloaded from
Annals of Oncology 22: 2616–2624, 2011
doi:10.1093/annonc/mdr489
Published online 9 November 2011original article
Implementing multiplexed genotyping of non-small-celllung cancers into routine clinical practice
L. V. Sequist1,2*, R. S. Heist1,2, A. T. Shaw1,2, P. Fidias1,2, R. Rosovsky1,2,3, J. S. Temel1,2,I. T. Lennes1,2, S. Digumarthy2,4, B. A. Waltman2, E. Bast1, S. Tammireddy1, L. Morrissey1,A. Muzikansky2,5, S. B. Goldberg1,2, J. Gainor2,6, C. L. Channick2,7, J. C. Wain2,8,H. Gaissert2,8, D. M. Donahue2,8, A. Muniappan2,8, C. Wright2,8, H. Willers2,9,D. J. Mathisen2,8, N. C. Choi2,9, J. Baselga1,2, T. J. Lynch10, L. W. Ellisen1,2, M. Mino-Kenudson2,11,M. Lanuti2,8, D. R. Borger1,2, A. J. Iafrate2,11, J. A. Engelman1,2 & D. Dias-Santagata2,11
1Massachusetts General Hospital Cancer Center, Boston; 2Harvard Medical School, Boston; 3The Mass General/North Shore Cancer Center, Danvers; 4Department of
Radiology; 5Department of Biostatistics; 6Department of Medicine; 7Division of Pulmonary and Critical Care Medicine; 8Division of Thoracic Surgery; 9Department of
Radiation Oncology, Massachusetts General Hospital, Boston; 10Yale University School of Medicine and Yale Cancer Center, New Haven; 11Department of Pathology,
Massachusetts General Hospital, Boston, USA
Received 14 August 2011; revised 17 September 2011; accepted 26 September 2011
Background: Personalizing non-small-cell lung cancer (NSCLC) therapy toward oncogene addicted pathway
inhibition is effective. Hence, the ability to determine a more comprehensive genotype for each case is becoming
essential to optimal cancer care.
Methods: We developed a multiplexed PCR-based assay (SNaPshot) to simultaneously identify >50 mutations in several
key NSCLC genes. SNaPshot and FISH for ALK translocations were integrated into routine practice as Clinical Laboratory
Improvement Amendments-certified tests. Here, we present analyses of the first 589 patients referred for genotyping.
Results: Pathologic prescreening identified 552 (95%) tumors with sufficient tissue for SNaPshot; 51% had ‡1mutation identified, most commonly in KRAS (24%), EGFR (13%), PIK3CA (4%) and translocations involving ALK (5%).
Unanticipated mutations were observed at lower frequencies in IDH and b-catenin. We observed several associations
between genotypes and clinical characteristics, including increased PIK3CA mutations in squamous cell cancers.
Genotyping distinguished multiple primary cancers from metastatic disease and steered 78 (22%) of the 353 patients
with advanced disease toward a genotype-directed targeted therapy.
Conclusions: Broad genotyping can be efficiently incorporated into an NSCLC clinic and has great utility in
influencing treatment decisions and directing patients toward relevant clinical trials. As more targeted therapies are
developed, such multiplexed molecular testing will become a standard part of practice.
Key words: carcinoma, non-small cell, genotype, molecular targeted therapy
introduction
Certain genetically defined cancers are ‘oncogene addicted’ toactivated kinases and are thereby highly sensitive to drugs thatselectively inhibit the corresponding kinase. Employinggenotype-based therapy has been highly successful in chronicmyelogenous leukemia, gastrointestinal stromal tumors, non-small-cell lung cancer (NSCLC) and melanoma, and in manyinstances, the targeted agent is far more effective thantraditional chemotherapy [1–9]. This shifting paradigm hasdramatically impacted lung cancer treatments. Until recently,therapeutic options for advanced NSCLC were limited to
chemotherapies that were ‘personalized’ only by considering
the side-effect profiles of a number of similar modestly effective
regimens. Response rates were typically 20%–30% and
progression-free survival (PFS) was 3–5 months [10–13]. But
now, we know that determining NSCLC genotype can inform
the most effective personalized therapies. Patients with
mutations in the epidermal growth factor receptor (EGFR) gene
benefit from EGFR tyrosine kinase inhibitors (TKIs) with
a response rate of �75%, PFS of 9–13 months and improved
quality of life compared with chemotherapy [8, 14–16].
Similarly, patients with EML4-ALK translocations have a 60%
response rate, 9-month PFS and a low degree of toxicity when
treated with crizotinib, an ALK TKI [6].Although these landmark studies have focused on a single or
small number of genetic mutations, there is an increasing
motivation to develop technologies that can simultaneously
determine the mutational status of many genes. Responding to
original
article
*Correspondence to: Dr L. V. Sequist, Massachusetts General Hospital Cancer Center,
55 Fruit Street, Professional Office Building room 212, Boston, MA 02114, USA. Tel: +1-617-726-7812; Fax: +1-617-724-3166; E-mail: [email protected] and Dr Dora
Dias-Santagata, Translational Research Laboratory, Massachusetts General Hospital,
55 Fruit Street, Jackson 1028, Boston, MA 02114, USA. Tel: +1-617-724-1261; Fax:+1-617-726-6974; E-mail: [email protected]
ª The Author 2011. Published by Oxford University Press on behalf of the European Society for Medical Oncology.
All rights reserved. For permissions, please email: [email protected]
at New
York M
edical College H
ealth Sciences Library on Novem
ber 29, 2011http://annonc.oxfordjournals.org/
Dow
nloaded from
Annals of Oncology 22: 2616–2624, 2011doi:10.1093/annonc/mdr489Published online 9 November 2011
B Y E R I K A C H E C K H A Y D E N
After Van VanderMeer was diagnosed
with advanced lung cancer, the results
of a genetic test offered some hope. Last
year, the 64-year-old lawyer learned that his
cancer featured a genetic rearrangement that
might render it vulnerable to a drug being tested
in clinical trials. But because the experimental
drug, crizotinib, was being given only to patients
who had failed chemotherapy, VanderMeer had
to wait for more than a year to gain access to the
drug. Even though VanderMeer’s tumours had
by then spread to both of his lungs, crizotinib
vaporized them within two weeks.
VanderMeer is now doing well and hoping to
continue beating the disease: more than half of
patients who take the drug, made by Pfizer of
New York, seem to have a better prognosis than
do those who didn’t receive treatment. But what
if VanderMeer had started taking it sooner?
Now oncologists, pathologists and geneti-
cists are hoping to answer that question with
a study that will test whether genetically tar-
geted treatments, applied soon enough, can
cure patients of lung cancer rather than buying
them a few extra months of life.
Targeted therapies have now been approved
for many cancers, and it has become routine
for major cancer centres to genotype patients’
tumours to determine whether they might
benefit from targeted drugs, in case standard
treatments fail. But the clinical trial, which
will be conducted by the Alliance for Clinical
Trials in Oncology, a nationwide group
funded by the US National Cancer Institute in
Bethesda, Maryland, will test whether using
targeted treatments earlier can prevent patients
with lung cancer from ever reaching that point.
In the trial, tumours will be genotyped after
surgery to determine whether mutations are
present in a gene encoding epidermal growth
factor receptor (EGFR). Mutations in this gene
are targeted by many molecular therapies,
including erlotinib and gefitinib, which are
approved for the treatment of advanced lung
cancer. Some of the patients who have EGFR
mutations will begin taking erlotinib after sur-
gery, instead of waiting to see whether their
cancer recurs.
Although similar approaches have been
tested in smaller trials, yielding mixed results,
organizers say that a larger, better-defined
study is needed to provide a clear answer.
“We have never tested these drugs in the
right population,” says oncologist Ramaswamy
Govindan of Washington University in St Louis,
leader of the trial. “We have never tested a group
of patients who have mutations in EGFR and
then asked the question, ‘could these patients
be cured by gefitinib or erlotinib?’”
He hopes to expand the analysis to include
crizotinib, which targets a different genetic
rearrangement and was approved by the US
Food and Drug Administration in August.
Other targeted therapies are in the pipeline.
In a 9 November paper, for instance, a con-
sortium of researchers from Massachusetts
General Hospital and Harvard Medical
School, both in Boston, and Yale University in
New Haven, Connecticut, describe the results
of a study that tested more than 500 patients
with non-small cell lung cancer (L. V. Sequist
et al. Ann. Oncol. http://dx.doi.org/10.1093/
annonc/mdr489; 2011). The authors examined
mutations in several genes relevant to therapies
that have been approved or are in development
(see ‘Identifying targets’). Of the 353 patients
with the most advanced lung cancers, 22%
were matched to clinical trials appropriate for
their cancer type.
The Alliance trial will be logistically diffi-
cult. Only 10–20% of patients with non-small
cell lung cancer have mutations in the EGFR
gene; only 20% of patients are diagnosed early
enough to benefit from surgery; and only a
fraction of patients with the appropriate muta-
tions will actually gain any advantage from
targeted treatments. To reach their target of
400 participants, Govindan and his colleagues
may need to screen as many as 1,500 people.
VanderMeer, for one, hopes that the efforts
pay off — and spare other patients from what
he calls the “blunderbuss” of chemo therapy.
“I’d hate for anyone to have to go through
the blunderbuss before they get to the stiletto,”
he says. ■
M E D I C I N E
Targeted treatment tested
as potential cancer cure
Trial will deploy genetically targeted therapy early, rather than as last resort.
MORE ONLINE
E X P L A I N E R
The science
behind
Australia’s war
on tobacco
advertising
go.nature.com/
zjrfci
M O R E N E W S
● Sickle-cell mystery solved go.nature.
com/dxx61h ● Ancient adaptations to parasites
drove human genetic variation
go.nature.com/d4es4b
● Proof found for unifying quantum
principle go.nature.com/dt8syh
F R O M T H E B L O G
Japan
funds
Fukushima
clean-up
projects
go.nature.com/wdfscp
No mutation
49%
KRAS
24%EGFR
13%
TP53
5%CTTNB1
2%NRAS
1%
HER2 ~1%
IDH1 ~1% or less
ALK
5%
PIK3CA
4%BRAF
2%IDENTIFYING TARGETS
Genotyping of lung tumours from more than 500 patients revealed genetic changes
that could be targeted by drugs. Some patients had more than one mutation.
TEP
CO
AU
STR
ALI
AN
CA
NC
ER C
OU
NC
IL
SO
UR
CE:
L. V
. SEQ
UIS
T ET
AL.
AN
N. O
NC
OL.
(2011)
1 7 N O V E M B E R 2 0 1 1 | V O L 4 7 9 | N A T U R E | 2 8 1
IN FOCUS NEWS
© 2011 Macmillan Publishers Limited. All rights reserved
17 NOVEMBER 2011 | VOL 479 |NATURE
nature
MGH’s tumor genotyping test, SNaPshot, has recently been included in prestigious journals, explaining the assay’s novel findings.
1 MGH is a registered trademark of Massachusetts General Hospital 2 SNaPshot is a registered trademark of Applied Biosystems, Inc. 3 Shaw AT, Iafrate JA, et. al. Case 21-2011: A 31-Year-Old Man with ALK-Positive Adenocarcinoma of the Lung. NEJM 2011; 365:163.
481 Edward H Ross Drive · Elmwood Park, NJ 07407 ·1 800 627 1479 tel · 1 201 791 8760 fax · www.genpathdiagnostics.com GenPath is a business unit of BioReference Laboratories, Inc. © 2012 BioReference Laboratories, Inc. All rights reserved. 91031 1/12
Tumor Genotyping
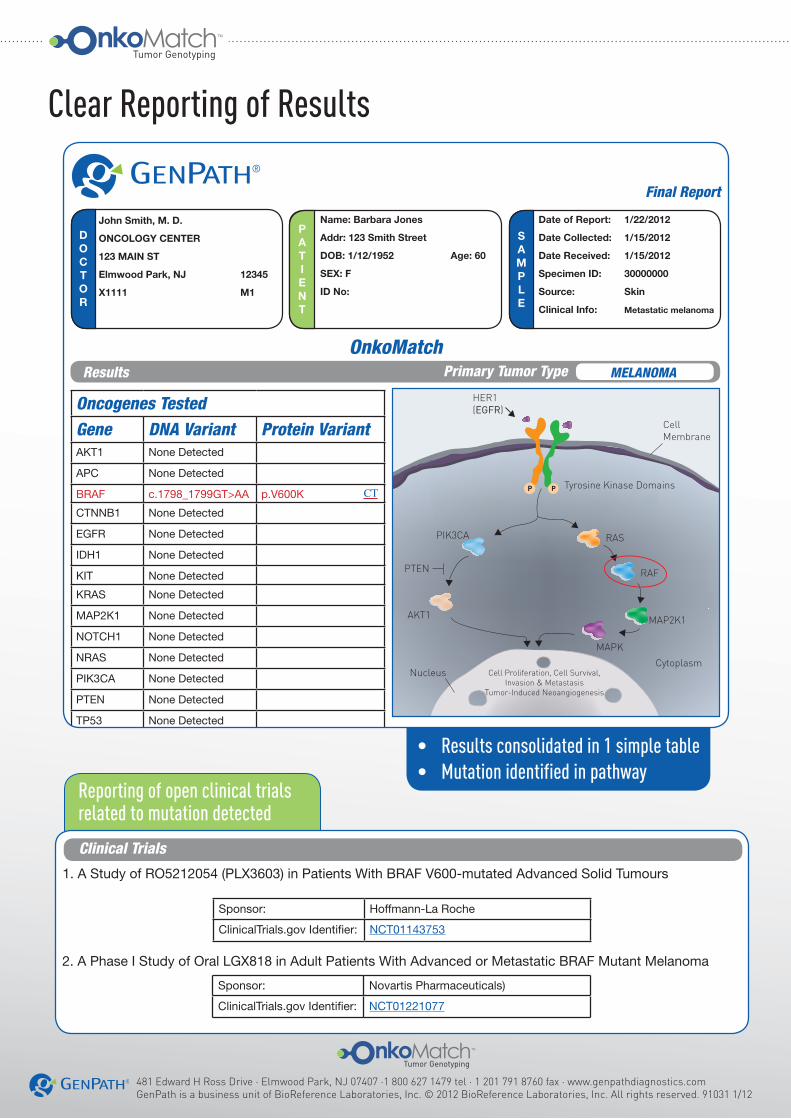
Reporting of open clinical trials related to mutation detected
• Results consolidated in 1 simple table• Mutation identified in pathway
Tumor Genotyping
Oncogenes TestedGene DNA Variant Protein VariantAKT1 None Detected
APC None Detected
BRAF c.1798_1799GT>AA p.V600K
CTNNB1 None Detected
EGFR None Detected
IDH1 None Detected
KIT None Detected
KRAS None Detected
MAP2K1 None Detected
NOTCH1 None Detected
NRAS None Detected
PIK3CA None Detected
PTEN None Detected
TP53 None Detected
Additional MarkersEGFR exon 19 deletion Not Detected
Final Report
®
John Smith, M. D.
ONCOLOGY CENTER
123 MAIN ST
Elmwood Park, NJ 12345
X1111 M1
DOCTOR
PATIENT
SAMPLE
Name: Barbara Jones
Addr: 123 Smith Street
DOB: 1/12/1952 Age: 60
SEX: F
ID No:
Date of Report: 1/22/2012
Date Collected: 1/15/2012
Date Received: 1/15/2012
Specimen ID: 30000000
Source: Skin
Clinical Info: Metastatic melanoma
Genpath is a business unit of BioReference Laboratories Inc.481 Edward H. Ross DriveElmwood Park, NJ 07407(800)633-4522
James Weisberger, M.D.Laboratory Director
Page 1 of 3Created 1/23/12 9:57 AM
TP2011-202778295
BRAF c.1798_1799GT>AA,p.V600K
Variant Description:The BRAF V600K mutation arises from a complex nucleotide change (c.1798_1799GT>AA) and results in an amino acid substitution of the valine (V) at position 600 by a lysine (K).
Prognostic Relevance: In one study of a consecutive series of patients with metastatic melanoma, the presence of a BRAF muta-tion was associated with a more aggressive clinical course and shorter survival for patients that were not treated with a BRAF inhibitor. (Long, Menzies, 2011).
Therapeutic Relevance:A phase III clinical trial showed that vemurafenib (PLX4032), a potent and orally-available BRAF kinase inhibitor, improved the rates of overall and progression-free survival in patients with previously untreated metastatic
OnkoMatch
Interpretative Information
HER1(EGFR)
RAS
RAF
MAP2K1
MAPK
PIK3CA
AKT1
Cytoplasm
Cell Membrane
Nucleus Cell Proliferation, Cell Survival, Invasion & Metastasis
Tumor-Induced Neoangiogenesis
Tyrosine Kinase DomainsP P
PTEN
CT
See report section on open clinical trialsCT
Results Primary Tumor Type MELANOMA
Genpath is a business unit of BioReference Laboratories Inc.481 Edward H. Ross DriveElmwood Park, NJ 07407(800)633-4522
James Weisberger, M.D.Laboratory Director
Page 2 of 3Created 1/23/12 9:57 AM
TP2011-202778295
Methodology
Clinical Trials
Methodology text
Sponsor: Novartis Pharmaceuticals)
ClinicalTrials.gov Identifier: NCT01221077
1. A Study of RO5212054 (PLX3603) in Patients With BRAF V600-mutated Advanced Solid Tumours
2. A Phase I Study of Oral LGX818 in Adult Patients With Advanced or Metastatic BRAF Mutant Melanoma
melanoma with the BRAF V600E or V600K mutations, when compared to chemotherapy (dacarbazine) (Chapman, 2011). Preliminary results from early phase clinical studies using other targeted agents are encouraging and include the BRAF inhibitor GSK2118436, and the RAF kinase inhibitor XL281 (Shepherd, 2011). Multiple MEK inhibitors are currently being evaluated for the treatment of advanced melanoma and other solid tumors, and include AZD6244, PD0325901 and GSK1120212 (Flaherty, CurrOpinOnc 2010).
Interpretative Information (continued)
Failed Probes
Comments
EGFR, c.2156G>C (p.G719A)
Final Report
®
John Smith, M. D.
ONCOLOGY CENTER
123 MAIN ST
Elmwood Park, NJ 12345
X1111 M1
DOCTOR
PATIENT
SAMPLE
Name: Barbara Jones
Addr: 123 Smith Street
DOB: 1/12/1952 Age: 60
SEX: F
ID No:
Date of Report: 1/22/2012
Date Collected: 1/15/2012
Date Received: 1/15/2012
Specimen ID: 30000000
Source: Skin
Clinical Info: Metastatic melanoma
Sponsor: Hoffmann-La Roche
ClinicalTrials.gov Identifier: NCT01143753
Clear Reporting of Results









![AtKC1 and CIPK23 Synergistically Modulate AKT1-Mediated Low ... - Plant … · AtKC1 and CIPK23 Synergistically Modulate AKT1-Mediated Low-Potassium Stress Responses in Arabidopsis1[OPEN]](https://img.pdfslide.net/doc/110x75/5e8b4152af7e1c6f2c7f962e/atkc1-and-cipk23-synergistically-modulate-akt1-mediated-low-plant-atkc1-and.jpg)



















