Embed Size (px)
Citation preview

strategies for revenue cycle success
by jeni williams
In an era of healthcare reform, excellence across all areas of revenue
cycle operations is critical to a hospital’s success. Here, winners of
HFMA’s MAP Award for High Performance in Revenue Cycle share
their strategies for performance excellence.

As healthcare reform leads to significant changes across the
industry, achieving optimal performance in revenue cycle opera-
tions has never been more important for hospitals.
“In an environment of healthcare reform, we’re going to need
to drive toward excellence,” Richard L. Clarke, DHA, FHFMA,
HFMA President and CEO, told attendees of HFMA’s ANI: The
Healthcare Finance Conference in June. HFMA announced its
MAP initiative and the 2010 MAP Award winners at ANI.
“The status quo and incremental change will not prepare us
for the drastic changes in patient access, insurance, and payment
coming our way,” Clarke says. “To thrive, we will need to provide
high-quality care and service at low cost. And we will need to
ensure that our revenue cycles are as efficient and productive
as possible.”
In 2009, HFMA created the MAP Award for High
Performance in Revenue Cycle to honor hospitals that achieve
revenue cycle excellence. MAP Award winners excel in
meeting key benchmarks for success, as established through
HFMA’s MAP initiative while adhering to the principles
outlined by HFMA’s PATIENT FRIENDLY BILLING® project.
The award is sponsored by 3M Health Information Systems.
Here, three MAP Award-winning hospitals share the
specific strategies and tactics that made their organizations
high performers—and what your organization can do
to enhance revenue cycle performance.
This award is an annual award recog-nizing healthcare organizations that achieve excellence in the revenue cycle. Applications for the third-annual award will be available in early 2011.
Map Keys are defining key indicators of revenue cycle performance. Using MAP Keys, healthcare finance professionals can improve business intelligence, strengthen revenue cycle management, and decide—based on industry-created metrics—where to focus for improvement.
The MAP App is a tool being piloted for tracking a provider’s performance throughout the revenue cycle and comparing performance with that of other organizations. The MAP App also offers tips on evolving best practices and includes a community discussion forum for airing common concerns. HFMA plans to roll out the tool for general use later this year.
The MAP Event will bring together the best ideas on how to improve revenue cycle performance. A MAP event will be held Nov. 7-9 in San Diego; more information is available at www.hfma.org/mapevent.
HFMA’s MAP initiative gives providers the tools they need to measure revenue cycle performance, apply evidence-based strategies for improve-ment, and perform to the highest standards of revenue cycle excellence. HFMA’s MAP initiative features the following.
For more information
about HFMA’s MAP initiative,
visit www.hfma.org/map.
HFMA’s MAP Initiative: Taking a Closer Look

Strategies for a More Collaborative Revenue CycleSeven years ago, Saint Francis Hospital in Tulsa, Okla., undertook an initiative to significantly overhaul its revenue cycle operations.
At that time, the hospital relied on four different IT systems for
revenue cycle management. The need for improved communication
between front-end and back-end revenue cycle staff at Saint Francis
had become increasingly clear, and the hospital’s days in accounts
receivable (A/R), which were in the mid-40s, were higher than the
organization would have liked. Additionally, Saint Francis sought to
implement new tools that would enhance insurance verification.
“We really imploded our revenue cycle operations to make
them more efficient and much more collaborative,” says Eric Schick,
vice president of finance for Saint Francis Hospital. “We studied our
revenue cycle from the front end to the back, and ran dry scenarios
to determine where areas of improvement existed. Through that
process, we determined that there were some processes that could
be shifted from the back end to the front end of the revenue cycle.
We also made the decision to create a centralized scheduling
department and prearrival department.”
One of the first challenges Saint Francis’ revenue cycle depart-
ment tackled was the need to increase collaboration between front-
end and back-end revenue cycle staff. “At that time, the front-end
staff really didn’t connect with the back-end staff; they were both
in separate worlds,” Schick says. He and Renee Edwards, director
of patient financial services, began to hold meetings with staff from
both areas to show them how their work is connected and the ways
in which their efforts are integral to the performance of the depart-
ment as a whole. “They began to understand that they are one
team—that they succeed together and that they fail together.”
When Saint Francis implemented new software and tools for
revenue cycle management, the hospital trained its front-end
revenue cycle staff in back-end processes, and vice versa. “This
helps front-end and back-end staff understand each other’s worlds.
It also increases collaboration among the revenue cycle team,”
Schick says. Saint Francis also hired two full-time and one part-time
trainer for the department, with training programs held monthly
for new staff and quarterly for staff who desire or need increased
education in a particular area.
Saint Francis measures performance against metrics such as
days in A/R; aged A/R as a percentage of billed A/R by payer,
which enables the health system to monitor its partnership with man-
aged care payers; days in discharged not final billed (DNFB), with
a DNFB goal of four days or less; point-of-service cash collections;
insurance verification rate; and service authorization rate. When
performance falls below expectations, revenue cycle leaders discuss
the issues with the directors of specific areas or with individual
employees, when appropriate, and develop plans for improvement.
And when a claim is rejected, the claim is sent back to the staff
person who originally made the error to be corrected. “This helps
the person who made the error to learn from it,” Edwards says.
“We’re a very productivity driven system,” Schick says. “For
example, we count transaction codes on the back end and look
at the number of claims that are processed to make sure staff are
meeting their monthly targets. Over the past year and a half, we’ve
also paid increased attention to the intricate role that our medical
records department plays in revenue cycle performance, and have
worked with medical records staff and physicians to ensure that
charts are completed in a timely manner. It’s important for physicians
and medical records staff to recognize that when DNFB spikes from
three days to seven days for a period of 60 days, then 60 days from
now, our organization is going to have trouble meeting our cash
goals, because that increase in DNFB days will have a domino effect
throughout the revenue cycle.”
The hospital’s focus on tightening its revenue cycle operations
has paid off. Saint Francis has dramatically reduced its days in A/R,
from the low 40s in late 2008 to the mid-20s today, and its days
in total DNFB measured just 3.42 in February 2010, when the
hospital’s MAP Award application was submitted. Now, the hospital
is working with managed care payers on issues that have caused
delays in processing claims. Ultimately, Saint Francis’ efforts in this
area will lead to claims being paid more quickly.
“Our efforts to improve revenue cycle operations have really
given us the capacity to move our performance to the next level,”
Schick says.

Using Data to Drive Revenue Cycle PerformanceAt Riverside Methodist Hospital in Columbus, Ohio, one of five OhioHealth facilities, an atmosphere of teamwork among the health system’s revenue cycle departments has helped to propel the hospital’s revenue cycle performance.
Several years ago, OhioHealth began to consolidate its business
office operations as a new IT system was introduced. The health
system also brought its patient access, health information manage-
ment, and central business office operations under the leadership
of the health system’s vice president of revenue cycle, who reports
to OhioHealth’s corporate CFO.
Weekly, OhioHealth’s revenue cycle leadership team meets
to discuss challenges, results, projects, training, and resources.
Monthly, OhioHealth’s revenue cycle leaders, hospital CFOs, and
other key finance representatives meet to review results and discuss
action plans. Cross-departmental revenue cycle teams meet at least
monthly, and targeted revenue cycle improvement teams meet as
frequently as needed. Additionally, OhioHealth hired IT personnel
who work solely with the revenue cycle team, as well as full-time
trainers who develop orientation and continuing education
sessions for staff.
This atmosphere of “systemness” among revenue cycle depart-
ments throughout the health system has enhanced OhioHealth’s
ability to effect significant improvements in its revenue cycle opera-
tions. At Riverside Methodist Hospital, aged A/R as a percentage
of billed A/R over 30 days is just 11.1 percent; over 60 days, 7.4
percent; and over 90 days, 4.5 percent. Days in total DNFB were
4.87 in February 2010, when the hospital’s MAP Award application
was submitted, and cash collection as a percentage of adjusted net
patient services revenue is 113.1 percent. And 80 percent of River-
side Methodist Hospital’s customers would recommend the hospital.
“One of the keys to our success in revenue cycle performance
is that all components of the revenue cycle report to finance,” says
Jane Berkebile, vice president, revenue cycle for OhioHealth. “It’s
very hard to achieve the same level of results in revenue cycle per-
formance if staff in health information management or patient ac-
cess don’t report to the same leaders as your billing staff. All revenue
cycle staff need to be on the same train, going in the same direction.
If you don’t have that level of systemness, when there are problems,
you’ll have people pointing fingers at each other rather than working
together toward a solution.”
OhioHealth also relies on data to measure and drive revenue
cycle performance at facilities such as Riverside Methodist Hospital.
The health system recently implemented an automated quality as-
surance system for registrars that monitors all registrations, includes
more than 200 real-time edits, returns errors to registrars to cor-
rect, and provides detailed error reporting and quality assurance
data down to the individual registrar. “Following implementation of
this system, our overall percentage of returned mail dropped from
2 percent to 1 percent, and our clean claim rate increased,”
Berkebile says.
Data from revenue cycle operations also are used to set goals
for revenue cycle staff and to measure progress; results are regularly
shared with staff. “Last year we had significant targets around patient
cash and around write-offs. They were stretch targets for us—and
we exceeded those targets,” Berkebile says. “Our point-of-service
[POS] collection goals are developed by facility and down to the
department level based upon the percentage of opportunity. We
provide feedback to individual registrars and financial counselors,
comparing their individual collections with the target goal.” The
increased focus on POS collections has paid off for OhioHealth
and Riverside Methodist. In the previous fiscal year, POS telephone
collections at time of preregistration averaged $180,000 per
month. With focused efforts and targets, this year, that average has
increased to $370,000 per month. “This is just one component of a
very successful POS program that increased POS collections year
over year by 21 percent,” Berkebile says.

One of the keys to our success in revenue cycle performance is that all components of the revenue cycle report to finance.” Jane Berkebile, vice president, revenue cycle, OhioHealth
surance system for registrars that monitors all registrations, includes
To nearly all patients receiving an electiveprocedure (75% or more of all elective procedures)
To some patients (below 75% of all patients)
At scheduling upon request
At registration upon request
At time of service upon request
To What Extent Do You ProvideEstimates of Patient’s Financial Obligations Prior to Rendering Services?
x
x
x x x
x x x
x x x
The Valley HospitalRidgewood, N.J.
Saint Francis HospitalTulsa, Okla.
Riverside Methodist HospitalColumbus, Ohio
Estimating Patient Financial Obligations Prior to Service
R
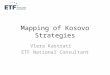
Net Days in A/R 23.2 36.8 35.2
Operating Margin 10.3% 6.0% 7.7%
Cash Collection as a Percentage ofAdjusted Net Patient Services Revenue
105.7% 100.5% 113.1%
Total Bad Debt Write-Off 4.1% 1.02% 1.4%
Total Charity Care Write-Off 3.7% 1.59% 4.29%
Days in Total Discharged Not Final Billed 3.42 5.6 4.87
Patient Would Recommend 82% 79% 80%
The Valley HospitalRidgewood, N.J.
Saint Francis HospitalTulsa, Okla.
Riverside Methodist HospitalColumbus, Ohio
A Snapshot of Award-winning Performance
*Exhibits reflect responses provided by the organizations in February 2010, when applications for MAP Award were submitted.
“

HFMA’s MAP Award for High Performance in Revenue Cycle, sponsored by 3M Health Information Systems, recognizes healthcare organizations that are distinctive, innovative, and effective in revenue cycle process improvements and patient satisfaction. In addition, it recognizes sustainable financial performance that serves the mission of the organization. For more information, visit www.hfma.org/mapaward.
About HFMA’s MAP Award
The following organizations received HFMA’s MAP Award for Revenue Cycle Excellence in 2010.
MAP Award Winners
• Denials Overturned by Appeal • Net Days Revenue in Credit Balance • Preregistration Rate • Insurance Verification Rate • Service Authorization Rate • Net Days in Accounts Receivable • Aged A/R as a Percentage of Billed A/R
The following 19 KPIs comprise the MAP Keys:• Aged A/R as a % of Billed A/R by Payer Group • Days in Final Billed Not Submitted to Payer • Days in Total Discharged Not Submitted to Payer • Late Charges as % of Total Charges • Initial Denial Rate—Zero Pay • Initial Denial Rate—Partial Pay
• Point-of-Service Cash Collections • Cost to Collect • Cash Collection as a Percentage of Adjusted Net Patient Services Revenue • Bad Debt • Charity Care • Days in Total Discharged Not Final Billed
HFMA recently developed a common set of revenue cycle key performance indicators (KPIs) known as MAP Keys in collaboration with multiple stakeholders. The MAP Keys promote the consistent reporting practices and peer-to-peer comparisons needed to achieve significant revenue cycle performance improvement. Embracing the MAP Keys for tracking revenue cycle performance can help hospitals identify revenue cycle performance trends and pro-actively prioritize and address areas in need of attention.
Key Performance Indicators for Tracking Performance
• Baylor Medical Center at Irving, part of Baylor Health Care System, Irving, Texas• CHRISTUS Schumpert Health System, part of CHRISTUS Health, Shreveport, La.• Hospital of the University of Pennsylvania, part of the University of Pennsylvania Health System, Philadelphia• Riverside Methodist Hospital, part of OhioHealth, Columbus, Ohio• Danbury Hospital, part of Danbury Health System, Danbury, Conn.• Saint Francis Hospital, part of Saint Francis Health System, Tulsa, Okla.• The Valley Hospital, part of Valley Health System, Ridgewood, N.J.• Princeton Medical Center, part of Baptist Health System, Birmingham, Ala.• Geisinger Medical Center, Danville, Pa.• Brookwood Medical Center, part of Tenet Health System, Birmingham, Ala.

The collaborative approach to revenue cycle performance
improvement has pushed revenue cycle performance to a higher
level at The Valley Hospital. Department by department, operating
margins have increased, from 2.1 percent in 2000 to 3.5 percent
in 2009. Managers’ yearly goals are tied in part to the hospital’s
financial performance, so that all hospital leaders have a stake in
the hospital’s revenue cycle performance. Monthly reports that
compare each department’s performance with its target goals keep
departments on track. Notably, the hospital’s patient satisfaction
scores, quality indicators, and employee satisfaction have demon-
strated improvement.
“I think the continual feedback we provide for managers and
employees throughout the hospital helps them to participate in
working toward the hospital’s revenue cycle goals,” Klutkowski says.
It’s important to take the time to sit down with individual departments
and talk with them regarding their concerns, because every depart-
ment is different. For example, what’s going on in radiation therapy?
What problems is the department experiencing with managed care
contracts? What are the concerns of leaders and key stakeholders
in the department? It’s also important to involve medical records in
these discussions, where appropriate, so you can really concentrate
on any coding issues that exist and help the department take steps
toward improvement.”
One of the keys to effecting change in individual departments
is to include all the appropriate stakeholders in discussions, not
just the department leaders. “Often, revenue cycle leaders choose
to meet with the department director when in fact a staff member
might have more influence in improving the department’s revenue
cycle performance,” Klutkowski says. “In some instances, including
an IT person in discussions with a department also can be key. Bring
payment records with you—most departments have no idea what
they actually get paid. Show the departments what they charged in
relation to what Medicare and insurance companies actually paid,
without saying, ‘You missed a charge.’ Information such as this will
be an eye-opener for leaders and staff and will help them to better
focus on the actions needed for improvement.”
We began to offer revenue cycle educa-tion to everyone throughout the hospital—specifics that really mattered to their department—and provided the support to helppeople improve performance as it relates to the revenue cycle.” Bill Klutkowski, CPA, assistant vice
president of finance, The Valley Hospital
Accelerating Revenue Cycle Improvement through a Change in CultureAt The Valley Hospital in Ridgewood, N.J., a change in the hospital’s culture and the mindset of staff have fueled significant improvements in revenue cycle performance.
We’ve always been strong in revenue cycle performance, but not
as strong as we are today,” says Bill Klutkowski, CPA, assistant vice
president of finance for the hospital. “We weren’t struggling for cash,
but we knew our revenue cycle performance could be even better.
The challenge for us was how to go from ‘good’ to ‘great.’”
The Valley Hospital began its quest toward excellence in
revenue cycle performance in 2000 by educating all employees
regarding their contributions to the hospital’s financial performance.
Everything changed with the introduction of Medicare’s ambula-
tory payment classification system. Edits and payments were all in
turmoil. We learned something new every day and realized quickly
that we couldn’t do it alone. We needed department head involve-
ment and accountability to the revenue cycle,” Klutkowski says.
“We began to offer revenue cycle education to everyone
throughout the hospital—specifics that really mattered to their
department—and provided the support to help people improve
performance as it relates to the revenue cycle. Our organization
also offers a leadership institute series for department leaders
three times a year, and we’ve given presentations to leaders that
address common budget issues, expense management, and various
aspects of the revenue cycle. When new managers join the
hospital, they meet with our director of budgets and reimbursement
staff to review their responsibilities. Each of these initiatives helps
to set targets and expectations related to revenue cycle
performance earlier.”
“
“
“
“

Lessons Learned
Build the morale of your staff. The Valley Hospital in Ridge-
wood, N.J., created a “finance morale committee” to discuss issues
that could affect employee satisfaction and ways to boost the spirits
of staff. Each quarter, representatives who are chosen by their peers
plan events for the staff (the group once held a carnival for revenue
cycle staff in the hospital parking lot) as well as community service
activities, such as contributing to a compassion fund set up to help
hospital employees who are experiencing financial hardship.
“Finance is a very stressful environment; we’re all expected to
do more with less. It’s good to invest in the morale of your staff,” says
Josette Melillo, director, patient financial administration, for The
Valley Hospital. In 2009, employee satisfaction scores ranked in the
91st percentile for revenue cycle staff, with a mean score of 85.7
percent, 12.6 percentage points higher than in 2000.
Invest in continuing education for revenue cycle staff. MAP Award winners have dedicated trainers for their
revenue cycle departments. At Brookwood Medical Center in Bir-
mingham, Ala., trainers provide reeducation for staff who are strug-
gling and conduct mandatory education refreshers for the revenue
cycle team. “We also encourage our staff to obtain certification,”
says Doug Carter, CFO. “Staff who achieve certification receive an
increase in pay, so there is an incentive for them to meet this goal.”
At Saint Francis Hospital in Tulsa, Okla., where front-end staff
have been trained in back-end revenue cycle processes, and vice
versa, “Staff realize that they are one team, and that they succeed
together,” says Eric Schick, vice president of finance.
Meet regularly with managed care payers to address issues that are delaying processing of claims. Such meetings
have enabled Saint Francis Hospital to address problems with con-
tract enforcement and claims processing that are delaying payments
Move your organization’s revenue cycle performance to the
next level at HFMA’s MAP Event. The event will feature revenue
cycle leaders from high-performing hospitals, who will discuss
proven tactics for achieving revenue cycle excellence.
Learn Strategies for Transforming Your Hospital’s Revenue Cycle Performance
HFMA’s MAP Event, to be held Nov. 7-9 at the Coronado Island
Marriott Resort and Spa in San Diego, will offer interactive op-
portunities for participants to learn best practices for revenue cycle
performance. Additionally, the event will feature a tour of MAP
Award-winning Sharp Grossmont hospital and insight from keynote
speaker Quint Studer, who will discuss the importance of evidence-
based leadership
For more information, or to register, visit
www.hfma.org/mapevent.
to the hospital. “Because our revenue cycle is as tight as it is,
we’re able to pay attention to details such as why some claims aren’t
being paid quickly, and to dial down into those issues and address
them with payers,” Shick says. “It takes diligence, perseverance, and
a lot of data to effect change, but it can be accomplished. There are
a lot of other providers in our market who are benefiting from our
efforts in this area.”
Maintain a dedicated IT staff for revenue cycle. “I have
my own IS team that works solely on revenue cycle projects,” says
Jane Berkebile, vice president, revenue cycle, for OhioHealth. “This
allows us to move very quickly to resolve any issues with technology
within the revenue cycle.”
Celebrate successes. OhioHealth keeps a treasure chest
full of dollar-store items in each of its revenue cycle departments to
reward employees who reach certain targets. This year, the health
system also held a “Right Choice Awards” program to honor individ-
uals and teams who contributed to the health system’s revenue cycle
success. Staff at Saint Francis Hospital are treated to an afternoon
at the zoo or the movies to celebrate the achievement of significant
goals. “It’s important to let your staff know that they are doing a great
job and that their efforts are appreciated,” Schick says.
Recognize the efforts of other departments in the organization that contribute to the organization’s revenue cycle success. At The Valley Hospital, revenue cycle staff recently
showed their appreciation to employees in other departments by
inviting them to a “sweets party,” complete with a chocolate fountain.
You have to develop a good relationship with other departments
that contribute to your organization’s revenue cycle success,” says
Bill Klutkowski, assistant vice president of finance.
“