Embed Size (px)
Citation preview

Mapping the Risk and Distribution of Epidemics in the WHO African Region
A Technical Report
May 2016

WHO/AFRO Library Cataloguing – in – Publication Data Mapping the Risk and Distribution of Epidemics in the WHO African Region: a technical report
1. Disease Outbreaks – statistics and numerical data
2. Epidemics – statistics and numerical data
3. Communicable Diseases – statistics and numerical data
4. Risk Assessment – supply and distribution – statistics and numerical data
5. Data collection – utilization
6. Africa
I. Work Health Organization. Regional Office for Africa II. Title
ISBN: 978-9290233084-4 (NLM Classification : WA 105)
© WHO Regional Office for Africa, 2016
Publications of the World Health Organization enjoy copyright protection in accordance with
the provisions of Protocol 2 of the Universal Copyright Convention. All rights reserved. Copies
of this publication may be obtained from the Library, WHO Regional Office for Africa, P.O. Box
6, Brazzaville, Republic of Congo (Tel: +47 241 39100; Fax: +47 241 39507; E-mail:
[email protected]). Requests for permission to reproduce or translate this publication –
whether for sale or for non-commercial distribution – should be sent to the same address.
The designations employed and the presentation of the material in this publication do not
imply the expression of any opinion whatsoever on the part of the World Health Organization
concerning the legal status of any country, territory, city or area or of its authorities, or
concerning the delimitation of its frontiers or boundaries. Dotted lines on maps represent
approximate border lines for which there may not yet be full agreement.
The mention of specific companies or of certain manufacturers’ products does not imply that
they are endorsed or recommended by the World Health Organization in preference to others
of a similar nature that are not mentioned. Errors and omissions excepted, the names of
proprietary products are distinguished by initial capital letters.
All reasonable precautions have been taken by the World Health Organization to verify the
information contained in this publication. However, the published material is being distributed
without warranty of any kind, either express or implied. The responsibility for the
interpretation and use of the material lies with the reader. On no account shall the World
Health Organization or its Regional Office for Africa be liable for damages arising from its use.

Contact Information Dr Ibrahima-Socé Fall, Director, Health Security and Emergencies Cluster WHO Regional Office for Africa, HSE Cluster, Attention: IDS BP 6, Cité du Djoué, Brazzaville, Congo Tel: (242) 241 39387/39412, (47) 241 38000 Fax: (47) 241 38005/6 Email: [email protected]
WHO AFRO Technical Team Dr Ibrahima-Socé FALL, Dr Nestor NDAYIMIRIJE Dr Zabulon YOTI Mr Etienne MINKOULOU Mrs Senait Tekeste FEKADU Dr Vincent Dossou SODJINOU Dr Soatiana RAJATONIRINA Dr Ali Ahmed YAHAYA Dr Magaran BAGAYOKO
WHO Technical Consultants Professor Abdisalan M Noor, FAAS, Visiting Professor, University of Oxford Director, Nairobi Programme KEMRI-Wellcome Trust Research Programme Second Floor, 197 Lenana Place, Lenana Road, PO Box 43640, 00100 Nairobi Kenya Email: [email protected]
Assisted by Mr Stephen Oloo, Mr Ezekiel Gogo, Mr Joseph Maina Assistant Research Officers, Geographic Information Systems KEMRI-Wellcome Trust Research Programme Second Floor, 197 Lenana Place, Lenana Road, PO Box 43640, 00100 Nairobi Kenya Email: [email protected]
Cover photo: Modified climatic ecological zones of Africa (source: http://www.fao.org/docrep/004/y1997e)
Acknowledgements The authors would like to thank Peter Macharia and Paul Ouma of the KEMRI/Wellcome Trust Research Programme for their help in data assemblies and mapping. The authors are grateful to Raymond Bruce J Aylward Sylvie Brand, Sandra Garnier, Olivier Ronveaux and Eric Gerard Georges Bertherat of WHO Geneva and Amadou Sall Institut Pasteur, Senegal, for comments on earlier drafts of this report.

Contents Executive Summary ................................................................................................................................. 1 1. Introduction ........................................................................................................................................ 3 2. Objectives............................................................................................................................................ 4
2.1 Specific objectives ......................................................................................................................... 4 3. Assembly of outbreak and epidemics data ........................................................................................... 4
3.1 Identification of sources and developing a unified database .......................................................... 4 3.2 Summary of epidemic data by country and PHEIC disease ............................................................. 6
4. Mapping ecological zones and district of occurrence of PHEIC and other diseases ............................. 10 4.1 Ebola ........................................................................................................................................... 12 4.2 Lassa fever virus .......................................................................................................................... 14 4.3 Crimean Congo Hemorrhagic Fever ............................................................................................. 16 4.4 Marburg ...................................................................................................................................... 18 4.5 Rift Valley Fever........................................................................................................................... 20 4.6 Dengue Fever .............................................................................................................................. 22 4.7 West Nile Virus ............................................................................................................................ 24 4.8 Chikungunya ................................................................................................................................ 26 4.9 Yellow Fever ................................................................................................................................ 28 4.10 Zika Virus ................................................................................................................................... 30 4.11 Cholera ...................................................................................................................................... 32 4.12 Plague ....................................................................................................................................... 34 4.13 Meningitis ................................................................................................................................. 36 4.14 Anthrax ..................................................................................................................................... 38 4.15 Malaria ...................................................................................................................................... 40
5. Correlates of outbreaks and epidemics .............................................................................................. 42 5.1 Population ................................................................................................................................... 42 5.2 Urban Population ........................................................................................................................ 43 5.3 Gross Domestic Product (GDP) per capita .................................................................................... 44 5.4 Percentage GDP expenditure on health ....................................................................................... 45 5.5 Human Development Index ......................................................................................................... 46 5.6 Under 5 Mortality Rate ................................................................................................................ 47 5.7 Global Hunger Index .................................................................................................................... 48 5.8 Conflicts ...................................................................................................................................... 49 5.9 El Nino occurrence....................................................................................................................... 50 5.10 Forest cover............................................................................................................................... 51
6. References ........................................................................................................................................ 52 Annex A: Districts maps of outbreaks and epidemics from 1970-2016 ................................................... 56 Annex B: Outbreaks and epidemics reported at national level only and not by district ........................... 59 Annex C: Summary of correlates used in the analysis of association with outbreaks and epidemics ....... 62 *See Accompanying MS PowerPoint file for district maps of outbreaks and epidemics by time period.

1
Executive Summary Disease epidemics result in substantial ill health and loss of lives and therefore pose a threat to global health security, undermine socio-economic lives and destabilize societies. Disease surveillance is a critical component in detecting and effectively responding to epidemics to minimize loss of live and their disruptive consequences. Carefully assembled surveillance data at the highest possible spatial resolutions also permit the understanding of the burden of epidemics, their co-occurrence and the key biological, ecological, economic, health system and governance determinants. It is for this purpose that the WHO-AFRO has commissioned this report. The overarching objective was to develop a comprehensive spatially defined database of outbreaks and epidemics and delineate the ecological zones of diseases that are classified as Public Health Emergency of International Concern (PHEIC) according the International Health Regulations (IHR) 2005 and malaria. The main tasks included the assembly of an inventory of all epidemics reported in Africa from 1970-2016 characterised by date of occurrence, length of epidemic and magnitude and district of occurrence; definition of ecological zones of PHEIC diseases and malaria; the assembly of data on important socio-economic, health systems and environmental correlate and an basic statistical analysis of their relationship with occurrence and frequency of epidemics and outbreaks. Through this study, several products have been developed including time series graphs of outbreak and epidemic occurrence by country, maps of the ecologies of the PHEIC diseases and epidemics, the distribution of these diseases by district. Overall, over 1730 outbreaks/epidemics have been reported in the WHO African region in the period 1970 to 2016. Because the outbreak/epidemic thresholds of the different diseases vary and the actual case data is incomplete, it is difficult to compare which diseases are most prevalent or pervasive. However, in terms of frequency of events, cholera, the arboviruses, measles and meningitis rank the highest. Of the nearly 5250 administrative 2 units analysed in this study, almost each one has reported some form of a disease outbreak in the period 1970-2016, with cholera being the most geographically widespread. The resulting databases are spatially defined and should serve as the basis of subnational inventory of disease outbreaks and epidemics in the region. Several challenges were encountered in the process of implementing this exercise:
There is limited information on the definitions and thresholds of outbreaks used over time and how this may have been affected by changing diagnostics and case definitions. This results in uncertainties in the temporal comparison of data.
There were inconsistencies between the major databases used in this report in terms of occurrence and magnitude of outbreaks. Agreement across more than two databases supported with literature review and consultation with the WHO AFRO and HQ teams helped with data verification.
Poor access to national surveillance bulletins, which are an important source of original outbreak and epidemics data, was a challenge to the data verification process and the development of online portals of national surveillance reports is critical.
There is limited data before 1980, most likely as a consequence of poor reporting or archiving of outbreak and epidemic data in libraries outside of Africa. In contrast, there is a greater frequency of reported outbreaks in the last 15 years as diagnosis and surveillance improved. For these reasons, extreme caution must be exercised when interpreting the trends in disease outbreaks and epidemics in Africa.

2
The description of the location of outbreak and epidemic events were variable. In some cases the name of village, town or district were reported. In others, the spatial definition of data was at regional or country levels. The aim of this project was to harmonize these data was to define events by district and where this was not possible, the data were reflected in the time series graphs but are not shown on the district maps.
Most of the potential correlates of epidemics, particularly those on socio-economic and health system development, are rarely available by district restricting the analysis to national level.
The databases and maps produced in this report should be considered as the foundation for tracking epidemics sub-nationally within the WHO African region. However, they require continuous verification, improvements in spatial resolution and regular updating. Finally, these data can also serve as the inputs for disease specific risk and vulnerability analysis. For example, the simple analysis in this report of the correlates shows that urbanization, gross domestic product (GDP) per capita, percentage GDP expenditure on health, human development index, global hunger index, conflicts, El Nino occurrence and forest cover seemed to correlate with patterns of epidemics. Combining such correlates with the detailed district level outbreak and epidemic data developed under this report could be the basis of further analysis of the assessment of risk of and vulnerability to the PHEICs.

3
1. Introduction There is an increasing recognition of the threat epidemics pose to global security, beyond its impact on human health [https://ghsagenda.org/; WHO 2015a; Sands et al. 2016]. Epidemics impact on human security through the catastrophic loss of life, the fear it creates in communities and the potential disruption of political and public order [Sands et al. 2016]. It also impacts on economic activity through the loss of labour and productivity and restrictions on travel and movement of goods. Low income countries, where the burden of infectious diseases are also generally high and the health systems are ill equipped to even respond to the basic health needs of the population, face greater vulnerabilities to the consequences of epidemics, setting back hard-earned health and socio-economic gains. Increased global connectivity and human population movement and economic interdependence mean that the risk and consequences of infectious diseases spreading across borders has grown dramatically and the threat to global security of an outbreak in a ‘distant’ corner of the world can no longer be ignored. The recent Ebola virus disease (EVD) outbreak in West Africa and its consequences is a poignant reminder of the global threat of epidemics [Moon et al 2015; Sands et al. 2016]. The outbreak began in Guinea in December 2013 and rapidly spread to Liberia in March 2014 and Sierra Leone May 2014 as a result of imported infections from Guinea [Moon et al 2015; WHO 2015b]. In all three countries, a full blown epidemic occurred and has only recently being brought under control. Small outbreaks also occurred in Nigeria and Mali and imported cases have been reported in Senegal, USA, the United Kingdom and other parts of the world. In the three main affected countries, over 28,000 people have become infected and 11,000 lives have been lost since [Moon et al 2015]. The economic losses as a result of the Ebola epidemic were estimated to be up to 2.2 billion US dollars in 2015 alone [World Bank 2016]. Although the epidemic has been largely controlled, cases have been reported in all countries in 2015. The rapid spread of the EVD and its catastrophic consequences were attributed to several national and international weaknesses [Moon et al 2015; Sands et al. 2016]. In February 2014, the Global Health Security Agenda (GHSA) was launched with a vision of ‘..a world safe and secure from the global health threats posed by infectious diseases…’ [https://ghsagenda.org/about.html]. By November 2015, 48 countries, including 10 from the WHO African region, had become members of the GHSA. Eleven action package areas (4 on prevention, 5 on detection and 3 on response) have been identified as part of the roadmap to implement the IHR (2005) [https://ghsagenda.org/packages.html]. Throughout the post-Ebola discussions, the existence of important surveillance gaps in several African countries was seen as a major obstacle to the prevention, preparedness, detection and response of future epidemics on the continent. The WHO African Regional Office (AFRO) has undertaken several activities including the critical assessment of country reading for International Health Regulations (IHR) 2005 requirements, the scale up and improvements of integrated disease surveillance and response (IDSR) systems and the strengthening of country laboratory capacity to detect diseases of international public health importance [WHO 2015c; CDC-IDSR 2015]. As part of this response, the WHO-AFRO has identified the need to develop a comprehensive, high resolution and spatially defined database of past outbreaks and epidemics to understand the disease specific epidemiological risks, the sub-national distribution of outbreaks and to support epidemic risk vulnerability analyses necessary for prioritizing country support. It for these reasons that this work was commissioned.

4
2. Objectives The occurrence of disease causing pathogens, host susceptibility, and environmental and contextual factors necessary for transmission are the key determinants of infectious outbreaks and epidemics [Janeway et al 2001]. Epidemics are likely to occur under conditions where there has been an increase in amount or virulence of the agent, introduction of the agent into a non-immune population, change in the host susceptibility, or pathogen susceptibility to drugs or enhanced transmission pathways increasing infection rates [Kelsey et al 1986]. The main objective of this project, therefore, was to develop a comprehensive spatially defined database of outbreaks and epidemics and delineate the ecological niche of diseases that are classified as Public Health Emergency of International Concern (PHEIC) according the International Health Regulations (IHR) 20051, and malaria, in the WHO African region. Under the IHR (2005), diseases classified as PHEIC were small pox, poliomyelitis due to wild-type poliovirus, human influenza caused by a new subtype and severe acute respiratory syndrome (SARS), pneumonic plague, yellow fever, viral hemorrhagic fevers, and West Nile fever and Zika virus.
2.1 Specific objectives
1) Develop an inventory of all epidemics reported in Africa from 1970-2016 and characterise data by date of occurrence, length of epidemic and magnitude.
2) Define the ecological zones of diseases that are classified as PHEIC and malaria.
3) Link the assembled data on outbreaks and epidemics to highest geographic resolution, preferably by district or equivalent
4) Identify and assemble data on important socio-economic, health systems and environmental factors
and implement a statistical analysis of their relationship with occurrence and frequency of epidemics
3. Assembly of outbreak and epidemics data
3.1 Identification of sources and developing a unified database A single complete reference database of epidemics in Africa does not exist. Therefore, the first step in developing such a database was to identify all potential sources of epidemic data, harmonize them and undertake additional searches of published and unpublished literature to develop a detailed database of epidemics. The key data sources used were Emergency Events Database (EM-DAT) of the Centre for Research on the Epidemiology of Disasters (CRED), the WHO/AFRO outbreaks database for the period 2007-2014, and the WHO-Disease Outbreak News (DON). Additional sources included the US Center for Disease Control and Prevention CDC) Morbidity and Mortality Weekly Reports (MMWR), the ProMED
1Global Health Security: International Health Regulations (IHR) http://www.cdc.gov/globalhealth/healthprotection/ghs/ihr/

5
(the Program for Monitoring Emerging Diseases) database, the Poliomyelitis Global Status database and other WHO disease specific databases. The EM-DAT epidemic data is compiled from sources such as UN agencies, non-governmental organizations, insurance companies, research institutes and press agencies who report epidemic events. The epidemic reports are then validated before they are entered into the EM-DAT database [Guha-Sapir et al 2015]. This data is available in the OFDA/CRED International Disaster Database and can be accessed through the EM-DAT website (www.emdat.be). Data was obtained through an official request and the data elements included were the actual location of the epidemic, origin of the epidemic and start and end dates of the epidemic. These database was received via email on 11th September, 2015. The EM-DAT epidemics data contained 778 epidemic events from 1970 to 2014. As part of the project, the WHO-AFRO Health Security and Emergencies Cluster team provided a database of disease outbreaks covering the period 2007-2015 in Africa. The database contained information on 22 epidemic and pandemic diseases. The WHO/AFRO 2007-2014 dataset contained 439 public health events across 22 different diseases, which was reduced to 18 after naming all influenza virus strains generally as “Influenza”. The WHO-DON databased is run from Geneva and is based on notifications of public health events caused by various infectious pathogens and other hazardous substances submitted to the WHO by member states as required under the IHR 2005 [WHO 2008]. Public health events that are unusual or associated with increased risk to humans are published weekly in the DON website (http://www.who.int/csr/don/en/). Data on these events due to infectious disease outbreaks was compiled from the reports published on the website from 1996 to 2015. The DON data reported 218 public health events. Data on several notifiable diseases, particularly on viral hemorrhagic fevers, such as Ebola, were also obtained from various outbreaks portals hosted on the US Centre for Disease Control and Prevention (CDC) website [www.cdc.gov]. Most of the databases included information on disease, time and location of outbreak. In some cases, data was reported on the various strains of the disease causing, but for purpose of mapping these strains were grouped together. For example, 30 Ebola outbreaks were reported from the CDC-Ebola dataset. The ProMED (the Program for Monitoring Emerging Diseases) database is an open source online reporting system established in 1994 by the Federation of American Scientists and SATELLIFE, to provide up-to-date information on outbreak of diseases and exposures to toxins that affect humans as well as animals and crops grown for food. The information disseminated by ProMED is collected through media reports, official reports, online summaries and by local observers, and later verified by a team of experts before it is posted on the ProMED website (www.promedmail.org) where it can be accessed freely. Epidemic data from each data source was counter-checked with data from other data sources. The various databases were compared on the basis of disease, location, start and end times, and magnitude in terms of infections and deaths. Where one epidemic was reported from different data sources, the record from the data source that had reported the disease causing the epidemic, the exact location of the epidemic, the exact start and end dates of the epidemic, the actual number of people affected by the epidemic, the number of deaths caused by the epidemic and the origin of the pathogen causing the epidemic was retained. There was no data source that contained all of these variables for all the epidemics reported, therefore the higher the number of these variables in a particular record, the higher

6
the rank of that record. Where the retained records had missing data elements available in other data sources, this information was transferred to final database. Where an epidemic was reported in only one data source, online searches of published literature, new articles and any online references to search epidemic was undertaken for verification. Unverified epidemic events were classified as being from a single source. A broad literature search was also undertaken to identify past and recent epidemics that were not captured in any of the established databases. Specifically, a systematic literature review carried out to identify malaria epidemics found 221 articles of which only 75 articles reported malaria epidemics. Malaria epidemic events was extracted from these articles and duplicate events removed resulting in 62 malaria epidemic events reported in Africa since 1970.
3.2 Summary of epidemic data by country and PHEIC disease Assembled epidemic data were summarized by country and year from the period 1970-2016. A 1970 starting point was selected simply for pragmatic reasons, however, there is limited data on epidemics before this period. Where a disease outbreak or epidemic started in one year and continued in consecutive years, this was considered to be one event unless there was evidence that they were totally independent epidemiologically. For example, the Ebola epidemic that started in Guinea in 2013 and continued through to 2015 was considered to be a single epidemic. Figure 1 A graph of all the outbreak and epidemic events by disease in the countries of the WHO African region

7
Figure 2 A bubble plot of outbreaks and epidemics of 39 diseases from 1970 to 2016 in the WHO African region.
Figure 3 A bubble plot of PHEIC diseases (Ebola , Lassa, Crimean Congo , Marburg , Rift Valley Fever, Dengue, West Nile virus, Chikungunya, Yellow Fever, Zika virus, Plague, Meningitis and Polio) from 1970 to 2016 in the WHO African region.

8
Figure 4 A bubble plot of viral hemorrhagic diseases (Crimean Congo, Dengue, Ebola, Lassa, Marburg, Rift Valley Fever, Yellow Fever and unknown or unspecified viral hemorrhagic fevers) from 1970 to 2016 in the WHO African region.
Figure 5 A graph of the number of unknown or unspecified viral hemorrhagic diseases by country from 1970 to 2016 in the WHO African region.

9
Table 1 Summary of outbreaks or epidemics reported in the WHO African region period 1970-2016 by
known disease (n=38) and unknown conditions (n=2)
No. Disease Frequency
1 Acute Flaccid Paralysis 1
2 Acute Jaundice Syndrome 1
3 Acute Neurological Syndrome 3
4 Acute Respiratory Syndrome/Infection 7
5 Aflatoxicosis 1
6 Anthrax 46
7 Chicken Pox 1
8 Chikungunya 13
9 Cholera 476
10 Crimean Congo 20
11 Dengue Fever 23
12 Diarrhoeal Disease 42
13 Ebola* 31
14 Fever with jaundice (Febrile Icterus) 1
15 Hepatitis (undefined) 1
16 Hepatitis A 1
17 Hepatitis B 2
18 Hepatitis E 8
19 Influenza 17
20 Lassa Fever 28
21 Leishmaniasis 2
22 Leptospirosis 1
23 Malaria 60
24 Marburg Disease 12
25 Measles 75
26 Meningococcal Disease 99
27 MERS-CoV** 3
28 Monkey Pox 16
29 Nodding 1
30 O'NyongNyong fever 2
31 Plague 47
32 Polio 439
33 Rift Valley fever 17
34 Schistosomiasis 1
35 Typhoid Fever 27
36 West Nile Fever 4
37 Yellow Fever 131
38 Zika Virus 1
39 Unknown Epidemic 96
40 Unknown Hemorrhagic Fever 22
Total 1779 * In Senegal one case was imported from Guinea; in South Africa one case imported from Gabon; in Cote d’Ivoire the case was a nosocomial infection (laboratory accident)] **Algeria –an imported case from Mecca in Saudi Arabia

10
4. Mapping ecological zones and district of occurrence of PHEIC and other diseases For the purpose of this analysis, the ecological zone of a disease is defined as any area within a country, where transmission of pathogens to humans can occur. A combination of country data on reported local cases, serological or genetic evidence of presence of pathogens in human hosts and the presence of transmitting vectors or zoonotic reservoirs have been used to define the ecological zones of the various PHEIC diseases. Although an entire country may be classified as belonging to the ecological zone of a specific disease, it is not uncommon that only a small area within the country has the ecological factors required for transmission, and the risk assigned to a country may be exaggerated. Therefore, it is important that reported cases are also described at the highest possible geographic resolution to reflect this heterogeneity. Here, the district geographic unit, or its equivalent, was used as the highest spatial resolution and epidemic data reported from a village, town and district were all assigned to the district (Annex A). In a few cases, data were reported at regional, provincial and state level and for such data, all districts in these geographic units were assumed to be affected by the epidemic. There were many reports of disease outbreaks that were provided with information on the country of occurrence. Although such data were used in country level ecological niche mapping, it was not possible to link them to any district and are summarized in Annex B. Almost all countries have undergone administrative boundary changes over time and these have affected the boundaries of districts. In some countries, the boundaries have change multiple times. As a first step, a decision was made to map the epidemic data at the current district extent to allow for future updating of the data. Consequently, a process of boundary digitization of district boundaries was undertaken in several countries using existing maps that are available online or other published sources. For Algeria, an updated district map was not available and the province boundaries was used. Across the 47 countries of the WHO African region, data were linked to a total of 5,249 district polygons or equivalent (Table 1). Overall the ecological zone maps can be used by global and regional partners for country risk assessment and prioritization while the district maps serve a useful purpose for local planning, risk factor analysis and sub-national surveillance prioritization.

11
Table 2 The number of district units or equivalent (n=5249) that were used to map the outbreak and epidemic data. For Algeria, the province level boundaries were used.
Country Number of administrative polygons
Algeria 48
Angola 161 Benin 34
Botswana 27
Burkina Faso 70
Burundi 46
Cameroon 180
Cape Verde Islands 23
Central Africa Republic 24 Chad 62
Comoros 3
Cote d'Ivoire 82
DRC 512
Equatorial Guinea 7
Eritrea 58
Ethiopia 731 Gabon 48
Gambia 7
Ghana 216
Guinea 38
Guinea-Bissau 89
Kenya 295
Lesotho 10
Liberia 90 Madagascar 112
Malawi 29
Mali 63
Mauritania 53
Mauritius 12
Mozambique 156
Namibia 34 Niger 42
Nigeria 775
Republic of Congo 39
Rwanda 30
Sao Tome and Principe 2
Senegal 76
Seychelles 1 Sierra Leone 14
South Africa 354
South Sudan 79
Swaziland 55
Tanzania 171
Togo 40
Uganda 112 Zambia 72
Zimbabwe 67

12
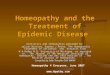
4.1 Ebola Figure 6: Ebola virus ecological zones mapped using a combination of reported cases and potential risk based on environment factors that may support the habitation by the African fruit bat.
Ebola hemorrhagic fever is a rare disease with a high fatality rate caused by infection with one of the five Ebola virus species [CDC-Ebola 2016]. There is no known natural reservoir host of the virus, however, the general consensus is that initial infection may be due to contact with to the fruit bats and some primates such as monkeys and chimpanzees followed by human-to-human transmission [Chowell et al 2014; CDC-Ebola 2016]. Transmission between humans is through direct contact with blood and other body fluids of infected persons. Ebola was first discovered in 1976 not far from the Ebola River in the Democratic Republic of Congo. In the same year, an outbreak was reported in Nzara district of South Sudan [CDC-Ebola 2016]. Since 1976, 31 outbreaks of the Ebola virus have occurred in the WHO African region. The most recent outbreak began in Guinea in December 2013 and has since spread extensively in Liberia and Sierra Leone with smaller outbreaks triggered by imported cases reported in Nigeria and Mali [Baize et al 2014; Bausch and Schwarz 2014; CDC-Ebola 2016]. In 2014, Ebola was recently declared a PHEIC by the World Health Organization [Funk and Piot 2014]. To define the ecological zones for Ebola virus transmission, data on reported local cases [CDC-Ebola 2016; WHO 2016a] were combined with information from an ecological niche model [Pigott et al 2014]
to classify countries into those where local cases (indigenous and introduced) were reported and those that can support transmission based on the ecological niche modelling. The ecological niche model used data on reported cases and fruit bat occurrence paired with environmental covariates to predict a zoonotic transmission niche in 22 countries across Central and West Africa. The environmental covariates used were vegetation, elevation, temperature, evapotranspiration [Pigott et al 2014].

13
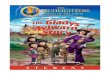
Figure 7: District map of reported Ebola virus disease cases reported from 1976 to 2015.

14
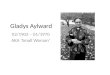
4.2 Lassa fever virus Figure 8: Lassa fever virus ecological zones mapped using a combination of reported cases and potential risk based on environment factors that support the habitation by the mouse Mastomys natalensis
Lassa fever is a viral haemorrhagic illness and occurs as outbreaks across West Africa. It is a zoonosis, with the primary reservoir species identified as the Natal multimammate mouse, Mastomys natalensis. The host is distributed across sub-Saharan Africa while the virus’ range appears to be restricted to West Africa. The majority of infections result from interactions between the animal reservoir and human populations, although secondary transmission between humans can occur, particularly in hospital settings [CDC-Lassa Fever, 2015]. Since its initial discovery, cases of Lassa fever have been reported in Sierra Leone, Liberia, Guinea, Nigeria, Niger, Mali, Ghana, Togo, Cameroun, Benin and Burkina Faso while serological evidence have been shown in Togo and Benin and in the rodent in Cameroon [Fichet-Calvert & Rogers 2009; Mylne et al 2015; CDC-Lassa Fever 2015]. Recent outbreaks of Lassa fever have been reported in Nigeria, Togo and Benin [WHO 2016]. The locations of confirmed human and animal infections with Lassa virus (LASV) were used to generate a probabilistic surface of zoonotic transmission potential across sub-Saharan Africa using species distribution models [Mylne et al 2015]. Lassa fever ecological zones were developed using the data on reported
cases and rodents and the predicted geographic extent of the Natal multimammate mouse.

15
Figure 9: District map of reported Lassa fever virus cases reported from 1989 to 2016. Some outbreaks have only being reported at national and could not be linked to a district (see Annex B)

16
4.3 Crimean Congo Hemorrhagic Fever Figure 10: Crimean Congo Hemorrhagic fever virus ecological zones mapped using a combination reported cases, serological evidence and potential risk of transmission based on tick vector
Crimean-Congo haemorrhagic fever (CCHF) is caused by a tick-borne virus, Nairovirus, of the Bunyaviridae family [CDC-CCHF 2014]. Some wild and domestic animals are asymptomatic carriers of the virus. The virus was first isolated in the Crimea in 1944 and later identified as a cause of illness in 1969 in the Congo, hence its name. The CCHF virus causes severe viral hemorrhagic fever outbreaks, with a case fatality rate of 10%–40% and is found in many parts Africa, the Balkans, the Middle East and Asian countries across the geographical limit of the principal tick vector [WHO 2013; Ergonul 2006]. Climatic factors that influence the presence of the tick, such as temperature, precipitation and moisture indices, have been found to be important drivers of CCHF infection [Wilson et al 1990; Vescio et al 2012; Messina et al 2015]. A combination of case reports, serological evidence of the virus in humans and the presence of the Hyalomma tick were used to develop probabilistic maps of CCHF virus risk [Messina et al 2015]. Country classification based on this map were updated using newly assembled. Countries with confirmed reported cases of CCHF or serological evidence in humans were classified as having complete presence of CCHF virus. Countries where the tick vector was present were classified as having moderate CCHF presence and the rest as indeterminable.

17
Figure 11: District map of reported Crimean Congo Hemorrhagic fever cases reported from 1996 to 2015. Some outbreaks have only being reported at national and could not be linked to a district (see Annex B).

18
4.4 Marburg Figure 12: Marburg virus ecological zones mapped using a combination reported cases and potential risk of transmission based on the presence of the Roussettus aegyptiacus vector.
Marburg virus disease (MVD) (formerly known as Marburg haemorrhagic fever) was first identified in 1967 during epidemics in Marburg and Frankfurt in Germany and Belgrade in the former Yugoslavia from importation of infected monkeys from Uganda [WHO n.d.(a); CDC-MVD 2014]. MVD is a zoonotic disease, with the African fruit bat (Rousettus aegyptiacus) identified as a reservoir host and affects both human and non-human primates. Infection is suspected to result from contact between this reservoir and human populations, with occasional secondary human-to-human transmission. In Africa, five countries have confirmed or suspected instances of animal-to-human zoonotic transmission of Marburg, namely Kenya, Uganda, Zimbabwe, Angola and the DRC [CDC-MVD 2014; Pigott et al 2015]. Countries in the WHO African region were classified into two Marburg ecological zones, those with reported MVD cases [CDC-MVD 2014], those without reported cases but with ecology that support the occurrence of Rousettus aegyptiacus [Pigott et al 2015] and those with no evidence of risk. However, there is limited data on both the distribution of the
disease and the zoonotic reservoir and this map may reflect the true extent of the likelihood of Marburg transmission.

19
Figure 13: District map of reported Marburg virus disease cases reported from 1975 to 2014. Some outbreaks have only being reported at national and could not be linked to a district (see Annex B).

20
4.5 Rift Valley Fever Figure 14: Rift Valley fever virus ecological zones mapped using a combination reported cases, serological evidence and potential risk of transmission based on the presence of the Aedes mosquito.
Rift Valley Fever (RVF) is viral zoonosis transmitted mainly by mosquitoes of the genus Aedes that primarily affects animals but also has the capacity to infect humans. Infection can cause severe disease in both animals and humans [Nanyingi et al 2015; CDC-RVF 2013]. The disease also results in significant economic losses due to death and abortion among RVF virus infected livestock. Since the first isolation of the virus in humans in the 1930s there have been multiple epizootics and epidemics of the RVF in sub-Saharan Africa [Muriithi et al 2011; Nanyingi et al 2015]. Outbreaks have been reported in many parts of sub-Saharan and North Africa. In 1997-98, a major outbreak occurred in Kenya, Somalia and Tanzania and in September 2000, RVF cases were confirmed in Saudi Arabia and Yemen, marking the first reported occurrence of the disease outside the African continent and raising concerns that it could extend to other parts of Asia and Europe [WHO 2010]. RVF virus outbreak was reported in 1987 in the lower Senegal River and was linked with flooding as a result of the Senegal River Project [CDC-RVF 2013]. Countries were classified into three RVF ecological zones: reported large outbreaks; reported periodic cases and/or serological evidence in humans; and only the presence of the Aedes mosquito was
reported.

21
Figure 15: District map of reported Rift Valley fever virus disease cases reported from 1997 to 2012. Some outbreaks have only being reported at national and could not be linked to a district (see Annex B).

22
4.6 Dengue Fever Figure 16: Dengue hemorrhagic fever virus ecological zones mapped using a combination reported cases, serological evidence and potential risk of transmission based on presence of the Aedes mosquito.
Dengue is a systemic viral infection transmitted between humans by Aedes mosquitoes, especially Ae. aegypti and Ae. albopictus [Simmons et al 2012; Kraemer et al 2015]. For some patients, dengue is a life-threatening illness [WHO and TDR 2009]. In Africa, dengue, like many other arboviruses, is considered to be under-reported [Brady et al 2012; Bhatt et al 2013] making its distribution uncertain despite the widespread presence of the transmitting vectors. The US CDC and HealthMap have developed a global dengue activity map based on data derived from the CDC Health Information for International Travel (or the YellowBook) and other data sources. These data on reported cases and serological evidence were used to classify countries into those with complete, moderate or intermediate presence of the dengue virus. These classification was further improved with an updated dataset.

23
Figure 17: District map of reported Dengue hemorrhagic fever virus disease cases reported from 1973 to 2015. Some outbreaks have only being reported at national and could not be linked to a district (see Annex B).

24
4.7 West Nile Virus Figure 18: West Nile virus ecological zones mapped using a combination reported cases and serological evidence in human or non-human hosts.
West Nile virus (WNV) is transmitted through female mosquitoes and was first isolated in 1937 from the blood of a febrile female patient who was examined in the context of a study of sleeping sickness in the West Nile district of Uganda [Smithburn et al 1940]. The largest outbreaks of WNV have been in Greece, Israel, Romania, Russia, and the USA. The outbreak of WNV in America was from 1999-2010 and since then has spread more widely across the world. This disease is seen as more of a threat to birds and horses, than the virus is to humans. Only 20% of the people infected with WNV show symptoms and less than 1% die from the virus. About 1 in 5 people who are infected will develop a fever with other symptoms. Less than 1% of infected people develop a serious, sometimes fatal, neurologic illness [CDC-WNV 2015]. This virus is currently, geographically, the most widely distributed arbovirus in the world, occurring on all continents except Antarctica [Ciota & Kramer, 2013].
The West Nile Virus (WNV) risk map was generated from the data presented by Cabre et al 2006 and the updated datasets collected for this report. The map show areas of high risk defined as countries that have reported frequent WNV outbreaks. Countries that have reported few sporadic WNV cases were considered to be of medium risk, while low risk class comprised countries that
have never reported any case of WNV but have serological evidence from either human or non-human host of the virus circulation. The grey regions are regions that have never reported or there is no data to indicate the presence of WNV transmission.

25
Figure 19: District map of reported West Nile fever virus disease cases reported from 2001 to 2014. Some outbreaks have only being reported at national and could not be linked to a district (see Annex B).

26
4.8 Chikungunya Figure 20: Chikungunya ecological zones mapped using a combination reported cases, serological evidence and the presence of the Aedes mosquito.
Chikungunya virus is transmitted to people by the Aedes mosquito. The most common symptoms of chikungunya virus infection are fever and joint pain. Other symptoms may include headache, muscle pain, joint swelling, or rash. Outbreaks have occurred in countries in Africa, Asia, Europe, and the Indian and Pacific Oceans. In late 2013, chikungunya virus was found for the first time in the Americas on islands in the Caribbean [CDC-CHIKV 2015]. Chikungunya is a mosquito-borne viral disease first described during an outbreak in southern Tanzania in 1952 [WHO 2015d]. The 2005 2007 outbreak was the most severe and one of the biggest eruptions caused by this virus [Jadav et al 2014]. Chikungunya fever has an epidemiological pattern with both sporadic and epidemics cases in West Africa, from Senegal to Cameroun, and in many other African countries including Democratic Republic of Congo, Nigeria, Angola, Uganda, Guinea, Malawi, Central African Republic, Burundi, and South Africa [Pialoux et al 2007; Jain et al 2008]. Ecological zones were based on reported cases and the presence of the Aedes mosquito.

27
Figure 21: District map of reported Chikungunya viral disease cases reported from 2005 to 2015. Some outbreaks have only being reported at national and could not be linked to a district (see Annex B).

28
4.9 Yellow Fever Figure 22: Yellow fever virus ecological zones mapped using a combination reported cases and potential risk of transmission based on serological evidence and the presence of the Aedes aegypti vector. Areas shaded grey are considered to be free of yellow fever transmission.
Yellow fever is an acute viral hemorrhagic disease transmitted by infected Aedes mosquitoes. The "yellow" in the name refers to the jaundice that affects some patients. The virus is endemic in tropical areas of Africa and Latin America [WHO 2014a]. The yellow fever ecological zones were defined according to the risk of infection. There are two transmission classes presented in this map. The first class is the moderate to high risk which includes the endemic and transitional zones [Jentes et al 2011]. These are areas which have a long history of reported enzootic yellow fever, both the vector and non-human host exist, and/or there were high numbers of reported human yellow fever cases before high coverage of the vaccine or there is serological evidence of high levels of yellow fever virus. Transitional zones are regions bordering the endemic area and include areas that experience the virus transmission during epidemic expansions. The second class is the low risk zone. This class covers the areas where yellow fever vectors and non-human host exist but no human or non-human yellow fever infection have been reported. The serological
evidence in this zone might also indicate low levels of yellow fever transmission in the past.
Figure 23: District map of reported Yellow fever virus disease cases reported from 1978 to 2016. Some outbreaks have only being reported at national and could not be linked to a district (see Annex B).

29

30
4.10 Zika Virus Figure 24: Zika virus ecological zones mapped using a combination of reported cases and potential risk of transmission based on serological evidence and the presence of the Aedes aegypti vector.
Zika viral disease is transmitted through the bite of an infected mosquito, primarily Aedes aegypti. The virus was first identified in 1947 in rhesus monkeys in the Zika forest of Uganda [Dick et al. 1952], and human disease was first identified in 1952 in Uganda and the United Republic of Tanzania. Zika virus disease outbreaks were reported for the first time from the Pacific in 2007 and 2013 in Yap and French Polynesia, respectively. The geographical spread of Zika virus has since been steadily increasing. Zika virus disease has similar clinical presentation as chikungunya and dengue, although it generally causes a milder illness. Symptoms of Zika virus disease include fever, skin rashes, conjunctivitis, muscle and joint pain, malaise, and headache, which normally last for 2 to 7 days. Neurological complications have been reported in Polynesia and in Brazil in 2014 and 2015 respectively. More recently increased number of microcephaly cases has been reported in Brazil since October 2015[WHO 2016b]. For many years, despite lack of systematic surveillance mechanism for Zika virus disease, sporadic human cases were detected in Africa. Since 2007 the spread of the virus has been confirmed in 8 Pacific islands, 25 countries and territories of the Americas, and a few Asian countries. In the African region, Cape Verde has reported outbreak with over 7000 cases from October 2015 to January 2016. However, the number of cases has been on the decline since December 2015
according to available data. The Zika virus transmission zone map was developed from data on reported cases, serological evidence of exposure in humans , confirmed transmission of dengue and/or chikungunya and confirmed presence of the Ae.aegypti and/or Ae albopictus. Evidence of infection in humans through local transmission was weighted highest followed by the serological data and reported transmission of dengue and chikungunya. Data on only the presence of the vector was given the lowest weight. The confirmed transmission of the two arboviruses was used as a proxy of sufficient vector density and/or efficiency. For more information please refer to the recent Zika virus risk assessment in the WHO African region [WHO-AFRO 2016].

31
Figure 25: District map of reported Zika virus disease cases reported from 2015 to 2016

32
4.11 Cholera Figure 26: Cholera ecological zones mapped using reported case data. Cholera outbreaks can occur in any country of the WHO African region but more prevalent in areas with poor sanitation and low access to clean water.
Cholera is an acute, diarrheal illness caused by infection of the intestine with the toxigenic bacterium Vibrio cholerae serogroup O1 or O139. Infection can be asymptomatic, mild, or severe. approximately 1 in 20 infected persons has severe disease characterized by profuse watery diarrhea, vomiting, and leg cramps. In these persons, rapid loss of body fluids leads to dehydration, electrolyte disturbances, and hypovolemic shock. Without treatment, death can occur within hours [Sack et al 2004].
Cholera, has largely been eliminated from the industrialized countries by water and sewage treatment, but still remains a significant cause of illness and death in many low income countries. Sub-Saharan Africa bears the brunt of the global cholera burden. The region is broadly affected by many cholera cases and outbreaks that can spread across countries [Gaffga et al 2007]. This reflects the lack of access to basic sanitation, clean water and health care [WHO 2012]. Cholera outbreaks have been reported across Africa and the ecological zones have broadly been defined on the basis case reporting. Countries have been classified into those that have reported local outbreaks and those that report imported cases only.

33
Figure 27: District map of reported cholera cases reported from 1970 to 2016. Some outbreaks have only being reported at national and could not be linked to a district (see Annex B).

34
4.12 Plague Figure 28: Plague ecological zones mapped using a combination of reported cases in humans and potential risk of transmission based on reported cases of plague in animals and countries with suitable ecology for transmission.
Plague is a bacterial disease, caused by Yersinia pestis, which primarily affects wild rodents. It is spread from one rodent to another by fleas. Humans bitten by an infected flea usually develop a bubonic form of plague, which is characterized by a bubo, i.e. a swelling of the lymph node draining the flea bite site. If the bacteria reach the lungs, the patient develops pneumonia (pneumonic plague), which is then transmissible from person to person through infected droplets spread by coughing. Initial symptoms of bubonic plague appear 7–10 days after infection. If diagnosed early, bubonic plague can be successfully treated with antibiotics. Pneumonic plague, on the other hand, is one of the most deadly infectious diseases; patients can die 24 hours after infection. The mortality rate depends on how soon treatment is started, but is always very high [WHO 2014b]. In Africa, plague cases generally occur in seasonal pulses, and show a geographically clearly discontinuous distribution in circumscribed foci that are assumed to be correlated with distributions of dominant vectors and rodent reservoirs and their ecology [Prentice & Rahalison 2007]. The plague occurrence data set consists of 45 unique locations from central (Democratic Republic of the Congo and Uganda), eastern (Tanzania, Malawi, and Mozambique), and southern Africa (Botswana, Lesotho, Namibia, South Africa,
Zambia, and Zimbabwe [Neerinckx et al 2008] and WHO Weekly Epidemiological Records. The plague foci are defined as areas where the bacteria is supposed to circulate in animal reservoirs and vectors and therefore are areas with potential human plague occurrence. The Plague foci were extracted from the WHO/PED map of global distribution of natural plague foci [WHO/PED Plague map – Personal Communication, Eric Gerard Georges Bertherat] and was constructed from through literature review and WHO collaborating centres.

35
Figure 29: District map of reported plague cases in humans from 1970 to 2015. Some outbreaks have only being reported at national and could not be linked to a district (see Annex B).

36
4.13 Meningitis Figure 30: Meningitis ecological zone map showing countries in the meningitis belt, those with part of their areas in the meningitis belt and countries outside the belt that have reported outbreaks or epidemics.
Neisseria meningitidis is found worldwide, but the highest incidence is in the “meningitis belt” of sub-Saharan Africa [WHO 2016c]. The meningitis belt, 10° and 15° of latitude North, was first defined by Lapeyssonnie in 1963 [Lapeyssonnie 1963] and covers 26 countries from the west to east of Africa. Meningococcal disease is hyperendemic in this region, and periodic epidemics during the dry season (December–June) reach up to 1,000 cases per 100,000 population. Meningococcal outbreaks have also been reported outside the meningitis belt. Since 2004, the enhanced surveillance network has been operational [WHO 2016c] Before the mass vaccination campaigns that began in 2010, the serogroup A accounted for over 80% of cases in the meningitis belt. Since 2010, over 220 million persons between 1-29 years of age have received the meningococcal A conjugate vaccine [WHO 2016c]. Three ecological zones have been developed and these are the meningitis belt, countries with parts in the meningitis belt and countries outside the belt
but have reported outbreaks.

37
Figure 31: District map of reported meningitis cases from 1970 to 2015. Some outbreaks have only being reported at national and could not be linked to a district (see Annex B).

38
4.14 Anthrax Figure 32: Anthrax ecological zones based on reported cases in humans and animals
Anthrax bacteria exist in the vegetative form and as a spore, making the bacteria more resistant to adverse environmental conditions thus ensuring its survival. Once the spore enters a conducive environment (inside a host), it germinates into a vegetative form, multiplying and rapidly colonizing the host. If untreated this infection can be fatal. In a case the host dies, the vegetative bacteria in the presence of oxygen sporulates. The spores are then shed from the dead carcass ready for uptake by another host. Anthrax disease mostly affect herbivores through transmission while grazing on contaminated grounds. Humans can get infected either through direct or indirect contact with infected animal, carcass or contaminated animal products. Infection in humans can occur in three ways that is a) cutaneous infection, which occurs when the bacteria enters the body through a cut or abrasion on the skin, b) pulmonary infection occurring when one inhales the spores, and c) gastrointestinal infection due ingestion of contaminated substance. All the three forms of infections are fatal with gastrointestinal and pulmonary infections having greater fatality rates. Cutaneous anthrax is the most common anthrax infection covering 95% or more of human reported cases [Turnbull 1998].
The World Health Organization Collaborating Center for Remote Sensing and Geographic Information Systems for Public Health mapped the risk of anthrax infections by country using data on reported cases [WHO n.d.(b)]. These was updated using recently assembled data.

39
Figure 33: District map of reported Anthrax cases from 1996 to 2016. Some outbreaks have only being reported at national and could not be linked to a district (see Annex B).

40
4.15 Malaria Figure 34: Map of malaria epidemicity developed from community P. falciparum parasite rate corrected to the age range 2-10 years of age (PfPR2-10) in 2000 and 2010.
Malaria is transmitted to humans through the bite of a female Anopheles mosquito that is infected with the plasmodium parasite. In Africa, the Plasmodium falciparum is the main parasite although other such as P. vivax, P. malariae and P. ovale have been reported. Malaria epidemics have been shown to occur among nonimmune populations in urban centres, highlands, arid and semi-arid areas [Najera et al 1998; Abeku et al 2003] as a consequence of extreme climatic anomalies, population displacements, uncontrolled large scale developments and/or failure of control interventions [Najera et al 1998; RBM 2001]. The WHO defines a malaria epidemic as a sudden increase in cases in an epidemic beyond what is considered normal [Najera et al 1998; Hook 2004]. There is an inverse relationship between levels of malaria endemicity and the likelihood of epidemics as modulated by the acquisition of immunity [Najera et al 1998]. Populations living in areas of stable transmission to malaria develop immunity early in life due to the high frequency of exposure to infections [Snow & Marsh 2002]. Therefore, in areas of stable transmission, the disease is concentrated among children under the age of five years and clinical episodes become rarer with age.
In areas of unstable transmission, normally defined as areas of hypoendemicity (≤10% parasite rate among children aged 2-10 years), populations are likely to be wholly susceptible or of partial immunity that is likely to be lost due to reduced exposure during a prolonged drought or under sustained control. It is among populations in unstable transmission, where majority of the infected people are likely to become clinically ill, that epidemics occur [Najera et al. 1998]. Using a map of malaria transmission intensity developed from community P. falciparum parasite rate corrected to the age range 2-10 years of age (PfPR2-10) for the years 2000 and 2010 [Noor et al 2014] within the stable limits of transmission [Snow et al 2012] at 1 x 1 km spatial resolution, the following malaria epidemic classification was developed (Figure 34): Malaria free area – This include areas which have declared malaria free such as the whole of Algeria and Western Sahara, parts of Zimbabwe and highland areas where low temperatures do not allow for the development of parasite [Snow et al 2012]; Naturally epidemic prone – These are areas where P. falciparum malaria transmission

41
was ≤10% (hypoendemic) and therefore at risk of epidemics naturally; Epidemic prone due to loss of immunity after control – These are areas where current (2010) P. falciparum transmission is ≤10% but where transmission in 2000 was >10%. Due to control, immunity in the population would have waned and if control is interrupted, an epidemic is likely to occur; Desert areas – where epidemics are rare but could occur near water sources; and stable transmission – where there is widespread parasite circulation and older children and adults are likely to have functional immunity and epidemics are unlikely. District level data on epidemics of malaria (Figure 35) were assembled from unpublished reports and systematic review of the published literature.
Figure 35: Map of malaria epidemics reported from 1970-2015. In Algeria and Mauritania, outbreaks were reported in specific villages and their location is shown on the map. The epidemic data were assembled through a systematic review of the published literature.

42
5. Correlates of outbreaks and epidemics Several contextual and environmental factors were assembled for the period 1995 to 2015 when data on epidemics and the correlates were sufficient for analysis. Data on several correlates were assembled (see Annex C for more details) and were classified into various categories based on their distribution and natural breaks in the data. Box plots of the various categories of the correlates and the total outbreak/epidemics events reported in the WHO African region since 1995 were developed to provide a simple statistical description of their relationships. These descriptions are limited to 10 correlates. Further analysis of these and other correlates and sophisticated modeling of the statistical relationships are beyond the scope of this report. However, the analysis serves as a basis to begin developing a conceptual framework for future epidemic risk and vulnerability assessments.
5.1 Population
Population data was obtained from the United Nations, Department of Economic and Social Affairs, Population Division [http://esa.un.org/unpd/wpp/DVD/]. The annual total population is estimated yearly and is consistent with previous census results and with estimates of subsequent trends in fertility, mortality and international migration. The estimates are then rounded to the nearest 1,000. For this study, World Population Prospects 2015, total population estimate for both sexes was downloaded [United Nations 2015]. Population estimates for African states from 1970 - 2015 were then extracted from the dataset.
Figure 36 A box plot of population size and the number of outbreaks and epidemic events reported in the period 1995-2016 in the WHO African region. The analysis shows increasing number of events in more densely populated countries

43
5.2 Urban Population
The percentage of population in each country living in areas defined as urban by national statistical offices was computed using the World Bank population estimates and urban ratios from the United Nation World Urbanization Prospects [World Bank 2015a]. This data was downloaded from the World Bank Open Data (http://data.worldbank.org/indicator/SP.URB.TOTL.IN.ZS). Percentage urban population growth for African states were then extracted from the dataset from 1970 to 2015. Figure 37 A box plot of percentage population in urban areas and the number of outbreaks and epidemic events reported in the period 1995-2016 in the WHO African region. The analysis suggest lower number of events with increasing urbanization.

44
5.3 Gross Domestic Product (GDP) per capita
The GDP data was downloaded from the World Bank Open Data website (http://data.worldbank.org/indicator/NY.GDP.MKTP.KD.ZG). GDP per capita is gross domestic product divided by midyear population. GDP is the sum of gross value added by all resident producers in the economy plus any product taxes and minus any subsidies not included in the value of the products. It is calculated without making deductions for depreciation of fabricated assets or for depletion and degradation of natural resources. Data for this study was obtained from the World Bank Open Data website (http://data.worldbank.org/indicator/NY.GDP.PCAP.CD) on 27, September, 2015. Where there were gaps in data, the estimated of the closest preceding or following for a country was used. Figure 38 A box plot of GDP per capita and the number of outbreaks and epidemic events reported in the period 1995-2016 in the WHO African region. A threshold of 600 USD was used based on distribution of the data and to allow for sufficient power between categories. The analysis shows a slight decrease in number of events with increasing GDP per capita.

45
5.4 Percentage GDP expenditure on health
These estimates were developed by the World Bank and used here as a broad indicator of health system strength. The indicator is computed from the total health expenditure as percentage of GDP for a given year. Total health expenditure is computed as the sum of public and private health expenditure and covers the provision of health services (preventive and curative), family planning activities, nutrition activities, and emergency aid designated for health but does not include provision of water and sanitation [http://data.worldbank.org/indicator/SH.XPD.TOTL.ZS]. Figure 39 A box plot of percentage GDP expenditure on health and the number of outbreaks and epidemic events reported in the period 1995-2016 in the WHO African region. As percentage GDP expenditure increases above 5 USD, there a slight decrease in outbreak or epidemic events but the difference is very small. This may be because across the WHO African region, investment in health remains very low and not sufficiently discriminative of epidemic risk.

46
5.5 Human Development Index The Human Development Index (HDI) is a composite index measuring average achievement in three basic dimensions of human development - long and healthy life, knowledge and a decent standard of living. The HDI is the geometric mean of normalized indices for each of the three dimensions. This data was available from 1980 to 2013 in the UNDP - Human Development Reports website - http://hdr.undp.org/en/content/table-2-human-development-index-trends-1980-2013 but not for all countries and years. For missing year data, the HDI from preceding or following nearest years in a country was used. South Sudan was dropped from analysis as no HDI data was available throughout the period 1995-2015. The HDI is subdivided into four categories;- Very High HDI (0.80-0.99), High HDI (0.70-0.79), Medium HDI (0.55-0.69) & Low HDI (0.00-0.54) - based on the Human Development report of 2014. In the WHO African region, only Algeria, Mauritius and Seychelles were classified as having high HDI in the period from 2009. Only 9 other countries were categories as medium HDI. For this reason, and to provide sufficient power category, a threshold 0.4 HDI was used. Figure 40 A box plot of HDI and the number of outbreaks and epidemic events reported in the period 1995-2016 in the WHO African region. The analysis shows fewer events in higher HDI countries. However, majority of countries in the WHO African region have low HDI.

47
5.6 Under 5 Mortality Rate
Under five child mortality dataset (U5MR) is seen as a strong measure of disease burden and health system strength. U5MR is also a strong proxy for impact of potential large scale epidemics. Data was obtained from the Child Mortality Estimate database, computed and maintained by the United Nation Inter-agency Group for Child Mortality Estimation (http://www.childmortality.org/index.php?r=site/index). The data included the minimum, median and maximum estimates for the U5MR per 1000 live births for all countries in the world from 1950 to 2013. The median estimates were categorized and categories for 2013 were maintained for subsequent years with missing data.
Figure 41 A box plot of under-five mortality rate and the number of outbreaks and epidemic events reported in the period 1995-2016 in the WHO African region. The analysis shows higher number of events in periods where under five mortality was ≥100 deaths per 1000 child birth. This suggests, as expected, a strong contribution of outbreak and epidemic events to child mortality.

48
5.7 Global Hunger Index Global Hunger Index is computed annually by the International Food Policy Research Institute (IFPRI). It is used to measure and track hunger globally, and by region and country. Undernourishment, child underweight and child mortality are the indicators used to calculate the index. A country's GHI score is calculated by averaging the percentage of the population that is undernourished, the percentage of children younger than five years old who are underweight, and the percentage of children dying before the age of five. This calculation results in a 100 point scale on which zero is the best score (no hunger) and 100 the worst. The data was reported between 1988-07 and 2009-13 [https://dataverse.harvard.edu/dataset.xhtml?persistentId=doi:10.7910/DVN/27557]. The GHIS classification is: Low < 5.0, Moderate 5.0 – 9.9, Serious 10.0 – 19.9, Alarming 20.0 – 29.9 & Extremely alarming 29.9< for each year [von Grebmer 2014]. For this report, low and moderate were combined and similarly alarming and very alarming.
Figure 42 A box plot of Global Hunger Index (GHI) and the number of outbreaks and epidemic events reported in the period 1995-2016 in the WHO African region. The analysis shows higher number of events with increasing level of hunger, with the alarming or very alarming levels of GHI associated with greater frequency of outbreak and epidemic events.

49
5.8 Conflicts Data was obtained from http://www.pcr.uu.se/research/ucdp/datasets/ucdp_prio_armed_conflict_dataset/, the website of the Peace Research Institute, Oslo and Uppsala Conflict Data Program (UCDP/PRIO) which documents armed conflicts. UCDP/PRIO collects conflict data from news articles and report the status of armed conflict on a yearly basis from 1946 to 2014. For this report, countries were classified into period of conflict or not and not necessarily the intensity or nature of conflict.
Figure 43 A box plot of conflicts and the number of outbreaks and epidemic events reported in the period 1995-2016 in the WHO African region. The analysis shows higher number of disease outbreak or epidemic events during conflicts.

50
5.9 El Nino occurrence According to National Oceanic and Atmospheric Administration (NOAA), an El Nino is a warm weather anomaly of the sea surface temperature (SST) in the Equatorial Pacific that might result in adverse weather patterns around the globe (http://www.pmel.noaa.gov/tao/elnino/el-nino-story.html). To identify an El Nino, NOAA computes five consecutive three month running mean of SST anomalies in the Equatorial Pacific (specifically the Nino 3.4 region which is between latitudes 50 N and 50 S, and longitudes 120 W and 170 W). This anomaly is known as Oceanic Nino Index (ONI). If the ONI exceed a specified threshold (in this case +0.50C) then an El Nino episode is experienced (https://www.ncdc.noaa.gov/teleconnections/enso/indicators/sst.php). El Nino years were obtained from the most recent computed values of ONI, as of 26th September, 2015, from NOAA (http://www.cpc.ncep.noaa.gov/products/analysis_monitoring/ensostuff/ensoyears.shtml).
Figure 44 A box plot of El Nino occurrence and the number of outbreaks and epidemic events reported in the period 1995-2016 in the WHO African region. There is no clear association between the occurrence of El Nino and frequency of epidemics, although there is marginally more epidemics reported during El Nino events. Analysis of specific vector borne diseases that have been reported to increase during El Nino, such as malaria, may reveal more interesting patterns.

51
5.10 Forest cover Several zoonotic disease that have eventually caused human epidemics have been shown to be associated with forest areas. The percentage forest cover data was downloaded from the Food and Agriculture Organization of the United Nations (FAO) website (http://www.fao.org/forest-resources-assessment/explore-data/en/). The data is generated from country forest reports and remote sensing1. The forest cover data show the percentage of land in a country that has natural or planted tress covering at least 5 meters in situ and exclude trees in agricultural production systems such as fruit plantation as well as trees in urban gardens. Figure 45 A box plot of percentage forest cover and the number of outbreaks and epidemic events reported in the period 1995-2016 in the WHO African region. There is no clear association between the percentage forest cover and frequency of epidemics. Analysis of specific zoonotic diseases that are spread by animal hosts found in forests may reveal more interesting patterns.

52
6. References 1. Abeku TA, van Oortmarssen GJ, Borsboom G, de Vlas SJ, Habbema JDF. Spatial and temporal variations of
malaria epidemic risk in Ethiopia: factors involved and implications. Acta Trop. 2003;87(3):331-340. 2. Baize, S., Pannetier, D., Oestereich, L., Rieger, T., Koivogui, L., Magassouba, N.F., Soropogui, B., Sow, M.S.,
Keïta, S., De Clerck, H. and Tiffany, A., 2014. Emergence of Zaire Ebola virus disease in Guinea. New England Journal of Medicine, 371(15), pp.1418-1425, doi:10.1056/NEJMoa1404505.
3. Bausch, D.G. and Schwarz, L 2014, ‘Outbreak of Ebola virus disease in Guinea: where ecology meets economy’, PLoS Negl Trop Dis, 8(7), p.e3056, doi:10.1371/journal.pntd.0003056.
4. Bhatt, S., Gething, P.W., Brady, O.J., Messina, J.P., Farlow, A.W., Moyes, C.L., Drake, J.M., Brownstein, J.S., Hoen, A.G., Sankoh, O. and Myers, M.F. 2013, ‘The global distribution and burden of dengue’, Nature, 496(7446), pp.504-507, doi:10.1038/nature12060.
5. Brady, O.J., Gething, P.W., Bhatt, S., Messina, J.P., Brownstein, J.S., Hoen, A.G., Moyes, C.L., Farlow, A.W., Scott, T.W. and Hay, S.I. 2012, ‘Refining the global spatial limits of dengue virus transmission by evidence-based consensus’, PLoS Negl Trop Dis, 6(8), p.e1760, doi:10.1371/journal.pntd.0001760.
6. Cabre, O., Grandadam, M., Marie, J.L., Gravier, P., Prange, A., Santinelli, Y., Rous, V., Bourry, O., Durand, J.P., Tolou, H. and Davoust, B. 2006, ‘West Nile Virus in Horses in sub-Saharan African’, Emerging infectious diseases, 12(12), p.1958.
7. CDC-CCHF 2014, Crimean-Congo Hemorrhagic Fever (CCHF), Viral Hemorrhagic Fevers, Centers for Disease Control and Prevention, viewed January 29, 2016,<http://www.cdc.gov/vhf/crimean-congo/>.
8. CDC-CHIKV 2015, Chikungunya Virus. Centers for Disease Control and Prevention, viewed January 29, 2016,<http://www.cdc.gov/chikungunya/>.
9. CDC-Ebola 2016, About Ebola Virus Disease, Viral Hemorrhagic Fevers, Centers for Disease Control and Prevention, viewed January 29, 2016, < http://www.cdc.gov/vhf/ebola/about.html>.
10. CDC-IDSR 2015, CDC Accomplishments in Integrated Disease Surveillance and Response (IDSR), Integrated Disease Surveillance and Response, Centers for Disease Control and Prevention viewed May 17, 2016. <http://www.cdc.gov/globalhealth/healthprotection/idsr/progress/accomplishment.html>.
11. CDC-Lassa Fever 2015, Lassa Fever, Viral Hemorrhagic Fevers, Centers for Disease Control and Prevention, viewed January 29, 2016, <http://www.cdc.gov/vhf/lassa/>.
12. CDC-MVD 2014, Marburg Hemorrhagic Fever (Marburg HF), Viral Hemorrhagic Fevers, Centers for Disease Control and Prevention, viewed May 17, 2016, <http://www.cdc.gov/vhf/marburg/>.
13. CDC-RVF 2013, Rift Valley Fever (RVF), Viral Hemorrhagic Fevers, Centers for Disease Control and Prevention, viewed January 28, 2016, <http://www.cdc.gov/vhf/rvf/>.
14. CDC-WNV 2015, West Nile virus, Centers for Disease Control and Prevention, viewed January 28, 2016 <http://www.cdc.gov/westnile/>.
15. Chowell, G. and Nishiura, H 2014, ‘Transmission dynamics and control of Ebola virus disease (EVD): a review’, BMC medicine, 12(1), p.196, doi:10.1186/s12916-014-0196-0.
16. Ciota, A.T. and Kramer, L.D., 2013, ‘Vector-virus interactions and transmission dynamics of West Nile virus’, Viruses, 5(12), pp.3021-3047, doi:10.3390/v5123021.
17. Dick, G.W.A., Kitchen, S.F. and Haddow, A.J. 1952, ‘Zika virus (I). Isolations and serological specificity’, Transactions of the Royal Society of Tropical Medicine and Hygiene, 46(5), pp.509-520.
18. Ergönül, Ö. 2006, ‘Crimean-Congo haemorrhagic fever’, The Lancet infectious diseases, 6(4), pp.203-214. 19. FAO 2015, The Forest Land Use Data Explorer, Global Forest Resources Assessments, Food and Agriculture
Organization of the United nations, retrieved January 27, 2016 <http://www.fao.org/forest-resources-assessment/explore-data/en/>.
20. Fichet-Calvet, E. and Rogers, D.J 2009, ‘Risk maps of Lassa fever in West Africa’, PLoS Negl Trop Dis, 3(3), p.e388, doi:10.1371/journal.pntd.0000388.
21. Funk, S. and Piot, P 2014, ‘Mapping Ebola in wild animals for better disease control’, Elife, 3, p.e04565. 22. Gaffga, N.H., Tauxe, R.V. and Mintz, E.D. 2007, ‘Cholera: a new homeland in Africa?’, The American journal of
tropical medicine and hygiene, 77(4), pp.705-713. 23. Guha-Sapir D, Below R, Hoyois P. EM-DAT: International Disaster Database – www.emdat.be – Université
Catholique de Louvain – Brussels – Belgium.

53
24. Hook, C., 2004, Field guide for malaria epidemic assessment and reporting: draft for field testing, World Health Organization, Geneva.
25. Human Development Report 2014, Sustaining Human Progress: Reducing Vulnerabilities and Building Resilience, United Nations Development Programme, New York.
26. Janeway CA Jr, Travers P, Walport M, et Al 2001, ‘Immunobiology: The Immune System in Health and Disease’, 5th Edition, Infectious Agents and How They Cause Disease, Garland Science, New York, Available from: <http://www.ncbi.nlm.nih.gov/books/NBK27114/>.
27. Jadav, S.S., Korupolu, P., Sinha, B.N. and Jayaprakash, V. 2014, ‘Chikungunya epidemiological survey and Current available inhibitors’, Journal of Pharmaceutical Chemistry, 1(3), pp.59-67, doi: 10.14805/jphchem.2014.art22.
28. Jain, M., Rai, S. and Chakravarti, A. 2008, ‘Chikungunya: a review’, Tropical doctor, 38(2), pp.70-72. 29. Jentes, E.S., Poumerol, G., Gershman, M.D., Hill, D.R., Lemarchand, J., Lewis, R.F., Staples, J.E., Tomori, O.,
Wilder-Smith, A. and Monath, T.P. 2011, ‘The revised global yellow fever risk map and recommendations for vaccination, 2010: consensus of the Informal WHO Working Group on Geographic Risk for Yellow Fever’, The Lancet infectious diseases, 11(8), pp.622-632.
30. Kelsey JL, Thompson WD, Evans AS 1986, ‘Methods in observational epidemiology’, New York, Oxford University Press, pp. 216.
31. Kraemer, M.U., Sinka, M.E., Duda, K.A., Mylne, A.Q., Shearer, F.M., Barker, C.M., Moore, C.G., Carvalho, R.G., Coelho, G.E., Van Bortel, W. and Hendrickx, G. 2015, ‘The global distribution of the arbovirus vectors Aedes aegypti and Ae. Albopictus’, Elife, 4, p.e08347.
32. Lapeyssonnie, L. 1963, ‘La méningite cérébro-spinale en Afrique’, Bulletin of the World Health Organization 28: 3–5.
33. RBM 2001, Specifications for Netting materials. WHO/CDS/RBM/2001.28 Geneva: World Health Organization. Available at: http://www. who. int/malaria/publications/atoz/who_cds_rbm_2001_28/en/Accessed on May 17, 2016.
34. Messina, J.P., Pigott, D.M., Golding, N., Duda, K.A., Brownstein, J.S., Weiss, D.J., Gibson, H., Robinson, T.P., Gilbert, M., Wint, G.W. and Nuttall, P.A. 2015, ‘The global distribution of Crimean-Congo hemorrhagic fever’, Transactions of The Royal Society of Tropical Medicine and Hygiene, 109(8), pp.503-513, doi: 10.1093/trstmh/trv050.
35. Moon S, Sridhar D, Pate MA, Jha AK, Clinton C, Delaunay S, Edwin V, Fallah M, Fidler DP, Garrett L, Goosby E, Gostin LO, Heymann DL, Lee K, Leung GM, Morrison JS, Saavedra J, Tanner M, Leigh JA, Hawkins B, Woskie LR, Piot P 2015, ‘Will Ebola change the game? Ten essential reforms before the next pandemic. The report of the Harvard-LSHTM Independent Panel on the Global Response to Ebola’. Lancet, 386:2204-21. doi: 10.1016/S0140-6736(15)00946-0.
36. Murithi, R.M., Munyua, P., Ithondeka, P.M., Macharia, J.M., Hightower, A., Luman, E.T., Breiman, R.F. and Njenga, M.K. 2011, ‘Rift Valley fever in Kenya: history of epizootics and identification of vulnerable districts’ Epidemiology and infection, 139(03), pp.372-380, doi: 10.1017/s0950268810001020.
37. Mylne, A.Q., Pigott, D.M., Longbottom, J., Shearer, F., Duda, K.A., Messina, J.P., Weiss, D.J., Moyes, C.L., Golding, N. and Hay, S.I 2015, ‘Mapping the zoonotic niche of Lassa fever in Africa’, Transactions of The Royal Society of Tropical Medicine and Hygiene, 109(8), pp.483-492, doi:10.1093/trstmh/trv047.
38. Nanyingi, M.O., Munyua, P., Kiama, S.G., Muchemi, G.M., Thumbi, S.M., Bitek, A.O., Bett, B., Muriithi, R.M. and Njenga, M.K. 2015, ‘A systematic review of Rift Valley Fever epidemiology 1931–2014’, Infection ecology & epidemiology, 5, doi: 10.3402/iee.v5.28024.
39. Nájera, J.A., Kouznetsov, R.L. and Delacollette, C., 1998, Malaria epidemics: detection and control, forecasting and prevention, Geneva: World Health Organization.
40. Neerinckx, S.B., Peterson, A.T., Gulinck, H., Deckers, J. and Leirs, H. 2008, ‘Geographic distribution and ecological niche of plague in sub-Saharan Africa’, International Journal of Health Geographics, 7(1), p.1.
41. NOAA 2015, Historical El Nino/ La Nina episodes (1950-present), National Weather Service,Climate Prediction Center, retrieved September 26, 2015, <http://www.cpc.ncep.noaa.gov/products/analysis_monitoring/ensostuff/ensoyears.shtml>
42. Noor, A.M., Kinyoki, D.K., Mundia, C.W., Kabaria, C.W., Mutua, J.W., Alegana, V.A., Fall, I.S. and Snow, R.W. 2014, ‘The changing risk of Plasmodium falciparum malaria infection in Africa: 2000–10: a spatial and temporal analysis of transmission intensity’, The Lancet, 383(9930), pp.1739-1747.

54
43. Pialoux, G., Gaüzère, B.A., Jauréguiberry, S. and Strobel, M. 2007, ‘Chikungunya, an epidemic arbovirosis’, The Lancet infectious diseases, 7(5), pp.319-327.
44. Pigott, D.M., Golding, N., Mylne, A., Huang, Z., Weiss, D.J., Brady, O.J., Kraemer, M.U. and Hay, S.I. 2015, ‘Mapping the zoonotic niche of Marburg virus disease in Africa’, Transactions of The Royal Society of Tropical Medicine and Hygiene, 109(6), pp.366-378, doi: 10.1093/trstmh/trv024.
45. Pigott, D.M., Golding, N., Mylne, A., Huang, Z., Henry, A.J., Weiss, D.J., Brady, O.J., Kraemer, M.U., Smith, D.L., Moyes, C.L. and Bhatt, S 2014, ‘Mapping the zoonotic niche of Ebola virus disease in Africa’, Elife, 3, p.e04395.
46. Prentice, M.B. and Rahalison, L. 2007, ‘Plague’, The Lancet, 369(9568), pp.1196-1207. 47. Sack D.A., Sack R.B., Nair G.B., Siddique A.K. 2004, Cholera. Lancet 363: 223–233 48. Sands, P., Mundaca-Shah, C. and Dzau, V.J., 2016. ‘The Neglected Dimension of Global Security—A Framework
for Countering Infectious-Disease Crises’. New England Journal of Medicine, vol 374, no.13, pp.1281-87. 49. Simmons, C.P., Farrar, J.J., van Vinh Chau, N. and Wills, B. 2012, ‘Dengue’, New England Journal of
Medicine, 366(15), pp.1423-1432. 50. Smithburn, K.C., Hughes, T.P., Burke, A.W. and Paul, J.H. 1940, ‘A neurotropic virus isolated from the blood of
a native of Uganda’, American Journal of Tropical Medicine, 20, pp.471-2. 51. Snow, R.W. and Marsh, K. 2002, ‘The consequences of reducing transmission of Plasmodium falciparum in
Africa’, Advances in parasitology,52, pp.235-264. 52. Snow, R.W., Amratia, P., Kabaria, C.W., Noor, A.M. and Marsh, K. 2012, ‘The changing limits and incidence of
malaria in Africa: 1939–2009’, Advances in parasitology, 78, p.169. 53. Turnbull, P.C.B. , R. Böhm , O. Cosivi , M. Doganay , M.E. Hugh-Jones , D.D. Joshi , M.K. Lalitha and V. de
Vos . 1998. Guidelines for the Surveillance and Control of Anthrax in Humans and Animals, 3rd ed. World Health Organization, Geneva.
54. Uppsala Conflict Data Program 2015, UCDP Conflict Encyclopedia: Armed Conflict dataset, Uppsala University retrieved August 10, 2015, <www.ucdp.uu.se/database>.
55. United Natoins, Department of Economic and Social Affairs, Population Division 2015, World Population Prospects: The 2015 Revision, DVD Edition, retrieved on September 24, 2015, <http://esa.un.org/unpd/wpp/DVD/>
56. United Nation Inter-agency Group for Child Mortality Estimation, Child Mortality Estimate, Estimates for under-five, retrieved August 9, 2015, <http://www.childmortality.org/index.php?r=site/index>.
57. Vescio, F.M., Busani, L., Mughini-Gras, L., Khoury, C., Avellis, L., Taseva, E., Rezza, G. and Christova, I 2012, ‘Environmental correlates of Crimean-Congo haemorrhagic fever incidence in Bulgaria’, BMC Public Health, 12(1), p.1.
58. von Grebmer, K., Saltzman, A., Birol, E., Wiesman, D., Prasai, N., Yin, S., Yohannes, Y., Menon, P., Thompson, J. and Sonntag, A. 2014, ‘2014 Global Hunger Index: The challenge of hidden hunger’, IFPRI books.
59. WHO-AFRO 2016, Zika Virus Risk Assessment in the WHO African region – a technical report. World Health Organization Regional Office for Africa, Brazaville.
60. WHO and TDR 2009, ‘Dengue: guidelines for diagnosis, treatment, prevention and control’, Geneva: WHO Library.
61. WHO n.d.(a), Marburg virus disease, viewed September 25, 2015, <http://www.who.int/csr/disease/marburg/en/>.
62. WHO n.d.(b), World Anthrax Data Site, World Health Organization Collaborating Center for Remote Sensing and Geographic Information Systems for Public Health, viewed 06 May 2016, < http://www.vetmed.lsu.edu/whocc/mp_world.htm>
63. WHO 2008, International Health Regulations 2005. World Health Organization, <http://apps.who.int/iris/bitstream/10665/43883/1/9789241580410_eng.pdf>.
64. WHO 2010, Rift Valley fever, Media centre, World Health Organization, viewed January 28, 2016, <http://www.who.int/mediacentre/factsheets/fs207/en/>.
65. WHO 2012, Cholera, 2011, Weekly Epidemiological Record, World Health Organization, Geneva, pp. 289–304. 66. WHO 2013, Crimean-Congo Haemorrhagic fever, Media centre, World Health Organization, viewed January 29,
2016, <http://www.who.int/mediacentre/factsheets/fs208/en/>. 67. WHO 2014a, Yellow fever, Media centre, World Health Organization, viewed January 27, 2016,
<http://www.who.int/mediacentre/factsheets/fs100/en/>.

55
68. WHO 2014b, Plague, Media centre, World Health Organization, viewed May 17, 2016, <http://www.who.int/mediacentre/factsheets/fs267/en/>.
69. WHO 2015a, Global tuberculosis report 2015, World Health Organization, Geneva. doi:WHO/HTM/TB/2015.08. 70. WHO 2015b, One year into the Ebola epidemic: a deadly, tenacious and unforgiving virus, World Health
Organization, <http://www.who.int/csr/disease/ebola/one-year-report/introduction/en/>. 71. WHO 2015c, Ebola Situation Report – 16 September 2015, World Health Organization,
<http://apps.who.int/iris/bitstream/10665/184623/1/ebolasitrep_16Sept2015_eng.pdf?ua=1>. 72. WHO 2015d, Chikungunya, Media centre, World Health Organization, viewed January 29, 2016,
<http://www.who.int/mediacentre/factsheets/fs327/en/>. 73. WHO 2016a, Ebola virus disease, Media centre, World Health Organization, viewed May 17, 2016
<http://www.who.int/mediacentre/factsheets/fs103/en/>. 74. WHO 2016b, Zika virus, Media centre, World Health Organization, viewed May 17, 2016,
<http://www.who.int/mediacentre/factsheets/zika/en/>. 75. WHO 2016c, Meningococcal meningitis, Media centre, World Health Organization, viewed January 27, 2016,
<http://www.who.int/mediacentre/factsheets/fs141/en/> 76. Wilson, M.L., LeGuenno, B., Guillaud, M., Desoutter, D., Gonzalez, J.P. and Camicas, J.L. 1990, ‘Distribution of
Crimean-Congo hemorrhagic fever viral antibody in Senegal: environmental and vectorial correlates’, Am J Trop Med Hyg, 43(5), pp.557-66.
77. World Bank 2015a, Urban Population, World Development Indicators, World Bank, viewed September 24, 2015, <http://data.worldbank.org/indicator/SP.URB.TOTL.IN.ZS>
78. World Bank 2015b, GDP per capita, World Development Indicators, World Bank, viewed September 24, 2015, <http://data.worldbank.org/indicator/NY.GDP.PCAP.CD>.
79. World Bank 2015c, Health expenditure, World Development Indicators, World Bank, viewed September 24, 2015, < http://data.worldbank.org/indicator/SH.XPD.TOTL.ZS>.
80. World Bank 2016, World Bank Group Ebola Response Fact Sheet, viewed May 17, 2016, <http://www.worldbank.org/en/topic/health/brief/world-bank-group-ebola-fact-sheet>.

56
Annex A: Districts maps of outbreaks and epidemics from 1970-2016

57

58

59
Annex B: Outbreaks and epidemics reported at national level only and not by district
Countries Chikunguny
a Cholera
Crimean Congo
Dengue Fever
Malaria Measles Meningiti
s Marb
urg Monkey Pox
Plague Polio RVF West Nile
Yellow Fever Typhoid Fever
Algeria 2012
Angola 2015 1995 1980-2006 and 2008
1988
Benin 2001 1976-2000, 2003, 2004, 2008 and 2009
1995, 1997, 1998, 2003 and 2004
Botswana 1988, 1993 and 1997
1997 1980-1989 and 1997
Burkina Faso 1991, 1998 and 2013 1997, 2012 and 2013
1980- 2004, 2008 and 2009
1983, 1984, 1985, 1996, 1999, 2002, 2006, 2007, 2009, 2010 and 2011
Burundi 1978 and 2015 2003 1998 1980-1996 and 1999
1995
Cameroon 1971, 1985 and 2015 1980-2005 and 2009
1980, 1984, 1994, 2003, 2006, 2012 and 2014
Cape Verde 1974, 1976, 1996 and 1998
1976-1988
Central Africa Republic
1996 2016 1980-2008, 2009 and 2011
2003, 2010, 2011 and 2013
Chad 1971 and 1991 2008 1983-2000, 2003, 2006, 2012 and 2013
2013
Comoros 2006 1975
1980, 1989, 1990, 1994, 2006, 2009, 2011 and 2012
1980 and 1983
Congo 2013 2015 1980-1988, 1999 and 2000
2012 and 2013
Cote d’Ivoire 1970, 1971, 1991, 1993, 1994, 1996, 2012 and 2015
1980-2009 and 2011
1982, 1997, 1999, 2012, 2013 and 2014
DRC
2004 1980-2000, 2006-2012
2001 2005

60
Eritrea 2011 and 2014
1994, 1995, 1997, 1999, 2000 and 2005
Ethiopia 1970, 1971 and 1985 2015 1981 2015 2009 1980-2010 2013 2009
Gabon 1980- 1996 and 2011
1994 and 2006
Gambia 1997 1980-1992, 1997 and 2000
2003 and 2012
Ghana 1970-1984, 1990-1996, 2012 and 2015
2011 and 2014
1980-2003 and 2008
1980, 1981, 1982, 1983, 1993, 1994, 1997 and 2006
Guinea 2007 2014 and 2015
1980- 1999, 2004, 2009 and 2011
1987, 2004, 2013 and 2014
Guinea Bissau
1971-1988, 1990 and 1997
1999
Kenya 2006 1997 and 1999 2003 1980-1999 1992, 1993, 1994 and 1995
Liberia
1973, 1980, 1981, 1995, 1998, 2001, 2004, 2006, 2007, 2008, 2009, 2010 and 2011
1980-1989, 1993-1999, 2009 and 2010
2002, 2003, 2005, 2006, 2010, 2012 and 2014
Madagascar 2012 2014
Malawi 1997 and 2000
Mali 2011 2009
Mauritania 1971, 1986, 1987, 1989, 1996 and 1997
1980-2001, 2009 and 2010
2003
Mauritius 2005
Mozambique
1980 and 2015 2014 and 2015
1980-2000 and 2011
2015
Namibia 2013 and 2014
1989, 1993-1999
Niger 1971, 1973, 1974, 1984, 1996, 1997 and 2015
2015 1995 1980-2011
Nigeria 1987 2015 1980-2005
1980, 1983, 1984, 1985, 1988, 1989, 1990, 1992, 1993, 1994, 1997, 2001 and 2011

61
Rwanda 1991-1993, 2000, 2004, 2007, 2009 and 2012
1980-1993, 1995, 1998 and 1999
2015
Senegal
1971, 1972, 1979, 1981,1984 - 1988, 1995, 1997, 2002 and 2012
2009 2010 1980-1998
1981, 2003, 2004, 2006, 2012 and 2013
Seychelles 2005 2015
Sierra Leone 1994 and 2007 1980- 2010
1995, 2000, 2005, 2006, 2009 and 2013
South Africa 1981, 1982, 1984, 1985, 1986 and 2005
1972, 1978, 1985, 1993, 1997, 1998, 1999 and 2001
1980-1999 2011
South Sudan 2015 2015 2013 2013 2011
Swaziland 1992 1980-1989
Tanzania 1991 1980-1998
Togo 1980-2009 1984, 1987, 2008 and 2012
Uganda 1971-1980, 1992, 1994, 1997, 2010 and 2015
2015 2015 2000 and 2008
1980-1998 2003
Zambia 2015 2007 1980-1999 and 2002
2001 2015
Zimbabwe 1992, 1993, 2000 and 2010
1992, 1996 and 2004
1980-1999

62
Annex C: Summary of correlates used in the analysis of association with outbreaks and epidemics
Data Data Source Link Date of data download
Population United Nations, Department of Economic and Social Affairs, Population Division http://esa.un.org/unpd/wpp/DVD/ 9/24/2015
Urban Population Growth World Bank http://data.worldbank.org/indicator/SP.URB.TOTL.IN.ZS
9/24/2015
GDP Growth World Bank http://data.worldbank.org/indicator/NY.GDP.MKTP.KD.ZG
7/24/2015
GDP Health Expenditure World Bank World Bank, http://data.worldbank.org/indicator/SH.XPD.PCAP
8/7/2015
Vaccine Coverage WHO http://www.who.int/immunization/monitoring_surveillance/
8/7/2015
Under 5 Mortality Rate United Nations Inter-agency Group for Child Mortality Estimation http://www.childmortality.org/index.php?r=site/index
8/9/2015
Corruption Perception Index Transparency International http://www.transparency.org/research/cpi
7/27/2015
Conflict Data UCDP/PRIO http://www.pcr.uu.se/research/ucdp/datasets/
8/10/2015
Fragile State Index Fund for Peace Organization http://fsi.fundforpeace.org/data 8/4/2015
Human Development Index UN http://hdr.undp.org/en/content/table-2-human-development-index-trends-1980-2013
8/11/2015
Drought and Floods EM-DAT www.emdat.be 8/13/2015
El Nino Year NOA http://www.cpc.ncep.noaa.gov/products/analysis_monitoring/ensostuff/ensoyears.shtml
9/26/2015
Global Hunger Index IFPRI https://dataverse.harvard.edu/dataset.xhtml?persistentId=doi:10.7910/DVN/27557
8/4/2015
Health System Strength WHO http://apps.who.int/gho/data/node.main.475?lang=en
8/20/2015
Percentage forest cover FAO FAO. "Global Forest Resources Assessments." Http://www.fao.org/forest-resources-assessment/explore-data/en/. FAO, n.d. Web. 11 Mar. 2016.
3/6/2016