Embed Size (px)
Citation preview

MAPPING
OF PARTNERS’ PROCUREMENT AND
SUPPLY MANAGEMENT SYSTEMS
FOR MEDICAL PRODUCTS
Federal Ministry of Health

© 2010 Federal Ministry of Health, Nigeria
All rights reserved. No part of this publication may be reproduced, stored in retrievalsystem or transmitted in any form or by any means, electronic, mechanical,photocopying, recording and/or otherwise, without prior written permission of theFederal Ministry of Health, Nigeria.
ISBN 978-978-49531-0-8
For all enquiries or comments, write to the publishers:
The Honourable Minister,Federal Ministry of Health,Federal Secretariat Complex,Shehu Shagari Way,P.M.B. 080 Garki,Abuja,Nigeria
Printed in Nigeria

TABLE OF CONTENTS
TABLE OF CONTENTS................................................................................................ii
LIST OFABBREVIATIONS ........................................................................................iii
ACKNOWLEDGMENTS ............................................................................................iv
EXECUTIVE SUMMARY ............................................................................................1
Partners' procurement policies.....................................................................................1
RECOMMENDATIONS................................................................................................3
OBJECTIVES ................................................................................................................5
METHODOLOGY.........................................................................................................5
RESULTS.......................................................................................................................6
How to read the map ....................................................................................................6
Details of Partners .......................................................................................................8
Categories of products supported ................................................................................9
Sources of funds ........................................................................................................10
Selection of products .................................................................................................10
Quantification of needs..............................................................................................11
Criteria considered for procurement of medicines and medical supplies ....................11
Working group for procurement.................................................................................11
Agency responsible for procurement .........................................................................12
Partners' procurement policies...................................................................................13
Ordering....................................................................................................................13
Monitoring performance of suppliers ........................................................................13
Quality assurance ......................................................................................................13
Stock management ....................................................................................................14
Storage of products....................................................................................................14
Distribution...............................................................................................................15
Budget allocation on activities...................................................................................15
First point of distribution ...........................................................................................17
DISCUSSION ..............................................................................................................18
RECOMMENDATIONS..............................................................................................19
Procurement and Supply Management ........................................................................1
Observations ...............................................................................................................2
INTRODUCTION..........................................................................................................4
ii

LIST OF ABBREVIATIONS
ARV Antiretroviral
CDC Centre for Disease ControlCHAN Christian Health Association of Nigeria
CIDA Canadian International Development AgencyCMS Central Medical Stores
DFID Department for International DevelopmentFMOH Federal Ministry of Health
FMS Federal Medical StoresGDF Global Drug Facility
GF Gede foundationGFATM Global Fund for Aids, Tuberculosis and Malaria
GHAIN Global Aids Initiative NigeriaHCP Health Commodities ProjectHF Health facility
IDA International Dispensary AssociationJICA Japan International Cooperation Agency
JSI John Snow IncorporatedLGA Local Government AreaMDG Millenium Development GoalsMSF Medicins Sans Frontieres
NACA National Agency for Control of AIDSNAFDAC National Agency for Food and Drug Administration and Control
NASCP National Aids and STD Control ProgramNDP National Drug Policy
NGO Non governmental organisationOIs Opportunistic Infections
PATHS Nigeria Partnership For Transforming Health SystemPEPFAR President's Emergency Plan for AIDS Relief
PSM Procurement Supply ManagementRBM Roll Back Malaria
SCMS Supply Chain Management SystemSFH Society for Family Health
SMS State Medical StoresSOP Standard Operating ProceduresTBLCP Tuberculosis and Leprosy Control ProgramUNFPA United Nation Fund for Population ActivitiesUNICEF United Nation Children’s Fund
USAID United State Agency for International DevelopmentUSFDA United States Food and Drug Agency
USG United States GovernmentWB World Bank
WHO World Health OrganizationZMS Zonal Medical Stores
iii

ACKNOWLEDGEMENTS
The Federal Ministry of Health is grateful to Prof. Babatunde Osotimehin, the Honorable Minister of
Health and , the Acting Head, Food and Drug Services Department for their
contribution to the project.
The Ministry also appreciates the continued support of the World Health Organization in Nigeria in
the pharmaceutical sector. We are particularly grateful to Dr. Peter Eriki, the WHO Representative in
Nigeria, Mrs. Helen Tata, Technical Officer, WHO, Geneva, Dr. Ogori Taylor, the Essential Drugs
and Medicine Policy (EDM) Advisor WHO, Nigeria and Dr. Olaokun Soyinka, the Health
PromotionAdvisor, WHO, Nigeria for their commitment to the realisation of the project. We wish to
thank the European Commission for their financial contribution to the project.
The contributions of the consultants, Mrs. Eno Ubok-Udom and Dr. Kazeem Babatunde Yusuff are
also acknowledged. Mr. J. E. B. Adagadzu who coordinated the implementation of the activities is
appreciated.
Mr. J. E. B. Adagadzu
iv

EXECUTIVE SUMMARY
Partners' procurement policies
Procurement and supply management
The Federal Government of Nigeria has continued to put in resources to enhance access to health for
her population. To achieve this aim, several partners such as multilateral and bilateral agencies, as
well as non governmental organisations support the government with funds, donations as well as
technical expertise in improving access to essential medicines.
The objective of this survey is to map the support provided by these partners in medicines
procurement and distribution. These include the financial flows, policies and mechanisms put in
place to manage the procurement and supply management of products.
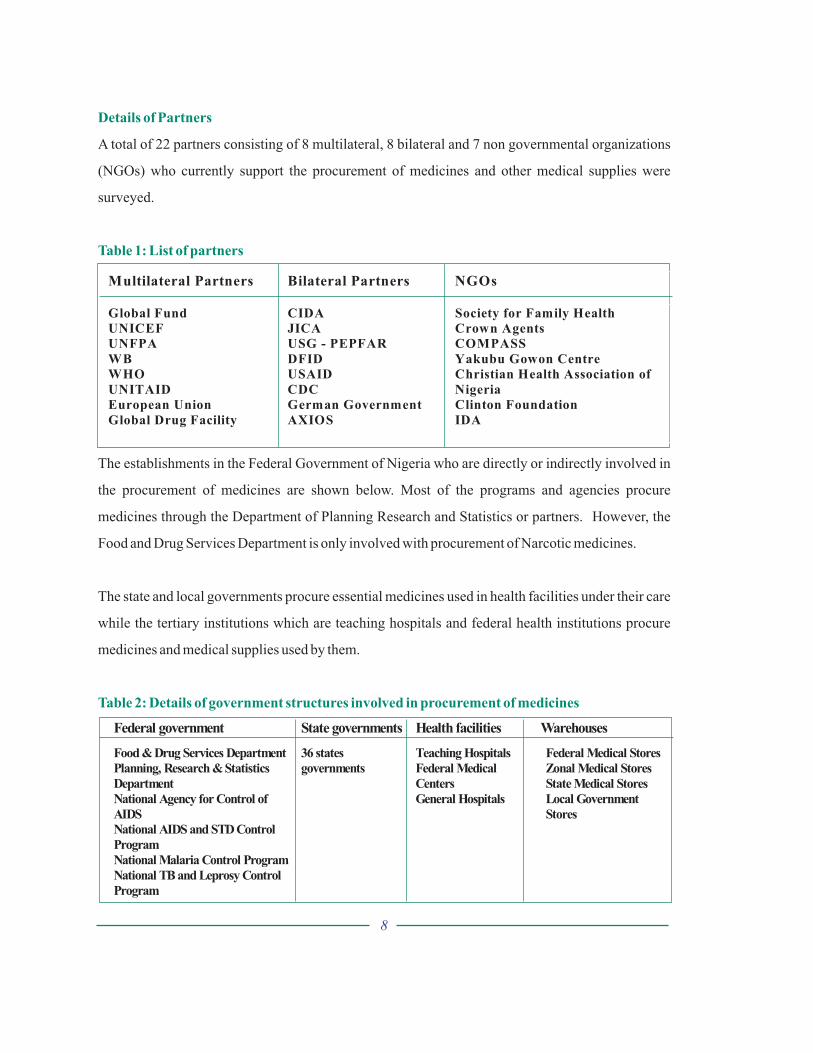
A total of 22 partners consisting of 8 multilateral, 8 bilateral and 7 non- governmental organizations
(NGOs) who currently support the procurement of medicines and other pharmaceutical supplies
were surveyed. There was unwillingness by partners to fully disclose their financial contributions to
the procurement and supply of medicines and medical products, making complete analysis of
situation impossible.
Most of the partners (85%) have specific policies for the procurement of products which do not take
into consideration the National Medicine Policy. These policies give priority to products registered
in the importing country (35%) or country of origin (30%) or WHO pre-qualification (25%).
The studies showed that only about half of the procurements are based on a procurement plan and
only 11% were based on the Essential Medicines List of the country. Only about 33% of partners
belong to a working group under the leadership of the Federal Ministry of Health. Of the
procurements carried out in 2006, only about 13% were executed by local suppliers.
Although most partners claimed to monitor suppliers' performance, only one partner provided a copy
of standard operating procedures (SOP) for procurement. Only about 69% of partners claimed to
1

systematically collect samples to send for quality control analysis. Of these, 78% use national
laboratories and all indicated relying on the regulatory authorities’registration to ascertain quality of
procured medicines
Most of the medicines purchased by partners were reported to be stored with private agents
contracted by them. However, all vaccines procured by partners are stored in government stores.
Most medicines and medical products are distributed by privately contracted agents and donors and
only 23% of procurements by partners are distributed by national programs. The FMS whose
statutory role is to manage medicines does not participate in distribution.
Only 29% of the products procured by partners were channelled through the Federal Medical Stores
as the first point of distribution while the others were either sent through private warehouses or sent
directly to health facilities.
The study demonstrates that procurement and supply of medicines in Nigeria is uncoordinated,
fragmented and unplanned. This results in duplication of efforts, wastage of resources and inability
of the government to optimize the support of the partners in a way to best benefit the country.
This situation may be attributed to inadequate political commitment in the medicines area and
absence of a procurement supply management plan to articulate the needs of the country and to guide
partners who wish to lend a helping hand to the government. Improvements to this situation will
require a health systems approach to ensure that the government addresses all issues about the
supply system in a coordinated, holistic and sustainable manner.
Observations
2

RECOMMENDATIONS
The government needs to take leadership in issues of procurement and supply management
of all medicines and pharmaceutical supplies by establishing a functional working group to
plan and implement PSM activities
APSM plan needs to be developed to ensure that all requirements of the country are detailed
and partners are thus required to participate in implementation of the plan
The National Policy on procurement of medicines and pharmaceutical
supplies should be developed and disseminated to all partners to ensure conformity of
current and future support to the country
To ensure conformity to the National Medicine Policy requiring flow of
medicines through the Federal Medical Stores, the warehouse should be refurbished into a
modern warehouse which provides appropriate management and security of products. Zonal
stores could also be developed to facilitate access to health facilities. However, all users of
the stores should be required to contribute to its maintenance.
Arobust medicines and supplies management information system should be established
using modern information technology to ensure flow of information to all stakeholders to
support planning and implementation of the PSM system.
3

INTRODUCTION
Access to optimal health care is recognized by governments all over the world as a fundamental right
for all people irrespective of setting or socio-economic status. Sustainable and uninterrupted supply
of efficacious, high quality and affordable essential medicines is an important component of a
functional health care system. Geographic and economic access to essential medicines is the most
critical success factor for achievement of optimal health care; and a sine qua non for making health
care services accessible particularly to the vulnerable and underserved in a developing and resource-
limited setting like Nigeria [1]. Indeed, one of the major targets of the MDG is to "… provide access
to affordable essential medicines in developing countries" and the indicator for monitoring
achievement of this target is "the proportion of population with access to affordable essential
medicines on a sustainable basis".
The role of the government is to put in place a viable national medicines supply system in Nigeria.
Indeed, this is a key objective of the National Drug Policy (NDP) which was launched in 1990 [2]
and reviewed in 2005. The goal of the National Drug Policy for Nigeria is to make available at all
times to the Nigerian populace adequate supplies of efficacious medicines that are affordable, safe
and of good quality. An important specific objective of the NDP is to also establish an effective and
efficient administrative framework for the financing, selection, quantification, procurement,
storage, distribution, sales and use of medicines in both public and private sectors.
This goal of ensuring an interrupted supply of essential medicines at public health facilities is being
complemented by support from development partners. They usually provide assistance to improve
access to essential medicines particularly for priority health diseases such as HIV /AIDS,
Tuberculosis, malaria, vaccine-preventable diseases etc. [3]. There are currently no comprehensive
data on contributions of development partners to financing of medicines and other medical supplies
in Nigeria despite the increase in the number of development partners providing financial,
infrastructural and / or technical support to health programs in Nigeria.
The objective of this report is to map out the current procurement and supply management systems of
essential medicines as practiced in Nigeria.
4

OBJECTIVES
METHODOLOGY
To carry out mapping of financing / financial flows of medicines and other medical supplies
by development partners in Nigeria
To identify roles played by development partners and non-governmental organisations in
the procurement and supply management systems
To identify the gaps in financing and management of essential medicines and medical
supplies in Nigeria
To identify available coordination mechanisms used in the country
To make recommendations on improvement of the procurement supply management
system to optimize access to essential medicines in the country
All development partners, faith based organisations, disease programs established in the Federal
Ministry of Health who are currently involved in financing, procurement and distribution of
medicines and medical supplies in Nigeria were invited for a meeting. The objectives of the survey
were explained to them and the tools were discussed.
The tools consist of a structured questionnaire (annex 1) which was administered to partners to elicit
information on the structures available and the processes employed in the management cycle -
selection, quantification, procurement, ordering, storage distribution, quality control, financing, and
human resources. Electronic copies of the questionnaires were either mailed or provided on compact
discs to the various partners who completed them. They were subsequently retrieved and additional
information or clarification was requested as necessary.
The data was analyzed to examine the distribution and involvement of the various partners in the
support of healthcare delivery programs and services and interpreted to form this report.Aschematic
representation of the product and financial flows was.
The limitation to the study was the fact that information was not always completely provided for
some of the items on the questionnaire. There was a lot of reluctance to provide details of financial
5

figures and funding flows in particular. Furthermore, it was not easy to determine the actual value of
in-kind donations as many invoices declare value for customs purposes that do not reflect the true
value of the donation.
1. The first row of boxes correspond to categories of medicines surveyed and are indicated by
specific colour codes.
2. The next row of boxes describe the four main groups of funding sources (government,
bilateral and multilateral donors, NGOs or the private sector). They are also represented by
specific colour codes.
3. Each product is linked to the funding source(s) by arrows. The product is represented by the
colour code of the product category.
4. The Agents who procure products on behalf of financing partners are represented on the
third row.
5. The succeeding 3 rows indicate the points of warehousing after procurement by agents.
6. The last box which is depicted by the pink colour shows the final beneficiary of the products
which is the patient.
RESULTS
How to read the map
6

7
Federal government State governments Health facilities Warehouses
Food &Drug Services Department
Planning, Research &Statistics
Department
National Agency for Control of
AIDS
National AIDS and STD Control
Program
National Malaria Control Program
National TB and Leprosy Control
Program
36 states
governments
Teaching Hospitals
Federal Medical
Centers
General Hospitals
Federal Medical Stores
Zonal Medical Stores
State Medical Stores
Local Government
Stores
Details of Partners
Table 1: List of partners
Table 2: Details of government structures involved in procurement of medicines
A total of 22 partners consisting of 8 multilateral, 8 bilateral and 7 non governmental organizations
(NGOs) who currently support the procurement of medicines and other medical supplies were
surveyed.
The establishments in the Federal Government of Nigeria who are directly or indirectly involved in
the procurement of medicines are shown below. Most of the programs and agencies procure
medicines through the Department of Planning Research and Statistics or partners. However, the
Food and Drug Services Department is only involved with procurement of Narcotic medicines.
The state and local governments procure essential medicines used in health facilities under their care
while the tertiary institutions which are teaching hospitals and federal health institutions procure
medicines and medical supplies used by them.
Multilateral Partners Bilateral Partners NGOs
Global Fund
UNICEF
UNFPA
WB
WHO
UNITAID
European Union
Global Drug Facility
CIDA
JICA
USG - PEPFAR
DFID
USAID
CDC
German Government
AXIOS
Society for Family Health
Crown Agents
COMPASS
Yakubu Gowon Centre
Christian Health Association of
Nigeria
Clinton Foundation
IDA
8

Categories of products supported
Table 4:Amount spent in 2006 and budgeted in 2007
Table 3: Categories of medicines supported
The contribution of the Federal Government of Nigeria, the State Governments and the Local
Governments are not included in the table below. Thus, the products are only those provided by
partners.
Categories Partners’
Support
[number]
Duration of
support
Type of support Type of financial
support
HIV / AIDS 5 1999-2010 Financial & Technical Grants & Donations
Anti-malaria 5 1979-2009 Financial & Technical Grants & Donations
TB medicines 1 1979- Financial Grants & Donations
Medicines for OIs 4 1999-2010 Financial & Technical Grants
Pediatric HIV/ AIDS 1 2005-2009 Financial & Technical Grant
Vaccines 1 2003- Financial & Technical Donation
Contraceptives 3 1999-2011 Financial & Technical Grants & Donations
Condom 2 1999-2008 Financial & Technical Grants & Donations
Medical supplies 4 1979-2010 Financial & Technical Grants & Donations
Reagents & HIV test
kits
5 1999-2010 Financial & Technical Grants & Donations
Product Amount spent in 2006 Amount budgeted for 2007
HIV/AIDS 4,687,000 7,312,644
Antimalarials 22,966,500 21,781,397
TB medicines 0 0
Medicines for OIs 1,000,000 5,012,500
Paediatric HIV/AIDS 1,000,000 1,500,000
Vaccines 773,901 1,007,350
Contraceptives 3,164,850 5,422,365
Condoms 46,666,458 50,488,704
Medical supplies 8970 2720
Reagents 988,700 9,587,890
TOTAL 81,256,379 102,115,570
9

Sources of funds
Selection of products
Table 5: Body responsible for the selection of products financed by donors
It was not possible to analyse the sources of funds for pharmaceuticals in the country as this
information was not provided by the government. The government does not earmark funds for
procurement of medicines as it provides funds in a decentralized manner to the facilities under its
jurisdiction to manage the health facilities. Thus, each facility determines the proportion of the
budget to be used for procurement of medicines and other medical supplies.
Also, the inability to capture the value of medicines donated by partners such as GDF, PEPFAR
makes it very difficult to estimate the value of partner's contribution to the pharmaceutical sector.
Consequently, it was not possible to indicate the actual amount spent by both the government of
Nigeria and the various development partners supporting the country in the medicines supplies
Selection of medicines and supplies financed by partners is done mainly within their organisations or
by their contracted agents. About half of partners (47%) surveyed involve the various programs in
the Federal Ministry of Health during their selection exercise.
The various agencies or programs of the Federal Ministry of Health such as NACA, NASCP, RBM,
TBLand Family Health select medicines and supplies financed by the government of Nigeria. This is
usually according to the respective clinical guidelines developed to manage the relevant diseases.
These guidelines are usually adopted into the National Essential Medicines List whenever there is a
review.
Body Selection
National program/FMOH 47%
FMS 0%
Donor 35%
Privately contracted agent 18%
Working groups 0%
10

Quantification of needs
Table 6: Body responsible for quantification of needs
Criteria considered for procurement of medicines and medical supplies
Working group for procurement
Quantification of medicines and supplies is mainly handled by partners or their agents.About 44% of
partners involve programmes in FMOH in the quantification process. It is worthy of note that a
working group does quantification in only 12% of donor-supported procurement (Table 3).
Quantification of HIV/AIDS medicines and supplies needs is currently being handled by JSI-
Deliver (Partner) and NASCP. Quantification is made using consumption data from treatment sites.
The main tool employed in the quantification process is Quantimed software. There is no evidence of
systematic quantification of anti-malarial medicines, contraceptives/condoms and TB medicines
and supplies.
Most (58%) of the procurements made by partners are based on a plan. Only 11% of the
procurements are based on the EML.
Only 38% of partners belong to a working group in which procurement activities are coordinated;
and of these, only 33% are under the leadership of the Ministry of Health. All the other working
groups are under the led by partners (UNICEF, UNFPA or World Bank). Most (60%) of the working
groups meet monthly while the rest meet quarterly and bi-annually.
Body Quantification
National program/FMOH 44%
FMS 0%
Donor 38%
Privately contracted agent 6%
Working groups 12%
11

Agency responsible for procurement
Table 7: Responsible for procurement of donor funded supplies
Table 8: Suppliers of products procured by partners in 2006
Most of the procurements were executed by either the donor or their contracted agents (87%) while
the Federal government managed the procurement of only 13% of supplies. The supplies of virtually
all the products (93%) were executed by international suppliers and manufacturers leaving only
7.2% of the products sourced within the country by both local suppliers and manufacturers (table 8).
Body Procurement
National program/FMOH 13%
FMS 0%
Donor 50%
Privately contracted agent 37%
Working groups 0%
PRODUCT Amount
spent in
2006
International
suppliers
International
Manufacturers
Local
distributors
Local
manufacturer
HIV/AIDS 4,687,000 - 2,004,000 81,000 119,6
Antimalarials 22,966,500 7,985,700 10,080,000 4,900,800
TB medicines 0 0
Medicines for
OIs
1,000,000 0
Paediatric
HIV/AIDS
1,000,000 0
Vaccines 773,901 773,901
Contraceptives 3,164,850 3,164,850
Condoms 46,666,458 46,666,458
Medical supplies 8970 8970
Reagents 988,700 313,360 44,640
Total 81,256,379 58,913,239 12,084,000 5,026,440 119,6
%age 100% 77% 16% 7% 0.2
12

Partners' procurement policies
Ordering
Table 9: Responsible for ordering medicines
Monitoring performance of suppliers
Quality assurance
Most of the partners (85%) have a specific policy for the procurement of products; and these policies
have more consideration for product registration in the importing country (35%) or country of origin
(30%) than WHO pre-qualification (25%).
Procurements by the Global Fund have specific laid out principles based on WHO prequalification
criteria or other stringent regulatory authority such as the USFDA. The USG follows the applicable
policies laid out by the United States government which does not necessarily correspond to those of
the country's.
Orders are usually made by the partner (64%) or their contracted agent (22%) and the national
program in the Federal Ministry of Health is rarely involved when they are deciding what to order.
Although most partners claimed to monitor suppliers' performance using indicators such as
conformity of orders, respect of delivery dates, appropriate transportation conditions, and quality of
after sales service. Only one partner provided a copy of SOPfor procurement.
Most of the partners (69%) claimed to systematically sample products which are sent to the
NAFDAC laboratory (78%) and laboratory in donor country by some partners for analysis. All
partners also relied on registration of medicines by NAFDAC in Nigeria as a key criterion for quality
assurance.
Ordering
National program/FMOH 14%
FMS 0%
Donor 64%
Privately contracted agent 22%
Working groups 0%
13

Stock management
Storage of products
Table 10:Analysis of first point of storage of procured medicines
Centralized first storage points for medicines and medical supplies
Stock management TB medicines, ARV medicines, reagents for blood safety and HIV test kits
procured by partners is done by private agents. Stock outs, procurements of medicines with less than
80% shelf life and expiration of products appeared to be a major problem. The main causes of stock
outs include error in quantification and forecasts of medicines and supplies, delay in delivery and
insufficient transport facilities.
Most of the medicines purchased by partners were reported to be stored mostly with private agents
contracted by partners. While all vaccines were stored in government stores, only some Global Fund
procured medicines and medical supplies are stored in the Federal Medical Stores (FMS).
The FMS has enough storage capacity to manage procurement and supplies of medicines especially
those procured by the Federal Government of Nigeria. There is evidence that there has been very
little work done to upgrade and refurbish the warehousing facilities at the FMS. Thus ceilings,
flooring of some stores, shelving, cooling systems, temperature monitors, information technology
Medicine Categories FMS Private Agents
HIV/AIDS 100%
Anti-malaria 40% 60%
TB medicines 100%
Medicines for OI’s 100%
Paediatric HIV/AIDS 100%
Vaccines 100%
Contraceptives 100%
Condoms 50% 50%
Medical Supplies 33% 67%
Reagents & HIV test kits 100%
14

equipment, lighting, warehousing equipment etc need to be provided for the stores for efficient
storage of medicines and supplies.
As other activities, most medicines and medical supplies are distributed by privately contracted
agents and donors. The national program is involved in the distribution of only 23% of procurements
by partners. The FMS whose statutory role is to manage medicines does not contribute to
distribution.
Distribution
Table 11: Responsible for Distribution of procured medicines
Budget allocation on activities
Figure 1: Resource allocation
Body Distribution
National program/FMOH 23%
FMS 0%
Donor 31%
Privately contracted agent 46%
Working groups 0%
Allocation of resources for activities
7682
18
76
6571
0
10
20
30
40
50
60
70
80
90
Dis
trib
ution
Ware
housin
g
and
sto
rage
Rem
unera
tion
for
ware
housin
g
sta
ff
Sta
fftr
ain
ing
Com
pute
rization
of
invento
ry
contr
ol
Qualit
yC
ontr
ol
Perc
en
tag
e
15

While most of the partners allocate funds for most of the activities shown on the chart above, only 3
out of 17 of them remunerate warehousing staff. However, only 6 out of 17 partners supplied the
actual funds budgeted for the listed activities. One partner indicated allocating $5.14 million dollars
for all the activities listed. The amount budgeted varies from organization to the other while
distribution and warehousing and storage are allocated the most funds. On the other hand, quality
control was allocated the least amount.
Table 12: Details of fund allocation by some partners
Activity area P 1 P 2 P 3 P 4 P 5 P 6 Total Avera
Medicines &
medical supplies
distribution
120,000 281,122 401,122 200,5
Warehousing
and storage
200,000 416,251 3,000 66,100 685,351 171,3
Remuneration
for warehousing
staff
120,000 10,000 4,000 134,000 44,6
Staff training for
supply chain
management
10,000 110,000 200,000 10,000 3,000 40,000 373,000 62,1
Computerization
of inventory
control
10,000 50,000 5,000 44,600 109,600 27,4
Quality Control 25,000 0 25,000 25,0
16

First point of distribution
Figure 2: % adherence to the National Drug Policy stipulation for product flow into the
country
Table 13: Details of warehousing
Only 29% of the products procured by partners was distributed through the government facilities.
One of the partners sends products directly to the health facility after procurement. Most of them
have established private structures at the central, zonal and state levels for the distribution of
products.
First point of Distribution
Government
29%
Private
71%
First point Second point Third point Fourth
point
Number of
products
% of produc
HF 1
FMS HF 3
CMS Private HF 3
FMS ZMS HF 2
FMS SMS LGA 1
Private HF 16 4
Private ZMS HF 6 1
Private ZMS SMS HF 1
Privatecentralwarehouse
Private zonalwarehouse
Private statewarehouse
HF 1
17

DISCUSSION
Conformity to National Policies
Government leadership
The objective of a procurement and supply system is to select the most cost-effective medicines; to
quantify the needs; to pre-select potential suppliers; to manage procurement and delivery; to ensure
good product quality; and to monitor the performance of suppliers and the procurement system. The
failure of any of these leads to either poor access to essential medicines or inefficiency in the system.
Inefficiency ultimately translates to wastage of scarce resources.
This study shows that international agencies, bilateral donors and development banks who finance
medicine procurement are operating with conflicting policies and these do not concord with the
national laws. For example, the National Drug Policy requires that all medicines meant for the
country must flow through the Federal Medical Stores but the study shows distribution of products
either through private warehouses or even directly to the health facility. This raises the question of the
quality of medicines procured as there is no systematic national evaluation of products and
monitoring of suppliers performance as shown in the results. Again, the National Drug Policy also
requires supply to facilities through expressed needs for the product which presumes that any
supplied product is preceded by appropriate quantification of needs. The results showed that some
partners planned their procurement internally and only sent products to the recipients. The country
also has regulations which require products supplied to the public sector to conform to the National
Essential Drugs List but the study also shows that some partners used their own criteria to choose
medicines.
The study shows that the government is only involved in the procurement supply management with
about one third of partners who are in the working group led by the government. This results in
duplication of efforts, wastage of resources and inability of the government to determine its needs
and optimize the support of partners in a way to best benefit the country.
The partners usually devise their own processes and systems due to the weakness of government
structures and consequently contract or build parallel systems. Most partners cite the weakness of the
18

Federal Medical Stores which fails to provide appropriate management and security of products.
Nevertheless, this practice does not lend the support which the government requires to reinforce
good pharmaceutical procurement and management practices and aim at sustainability. Rather, such
practices undermine or delay the development of good procurement and supply management
systems. Harnessing all efforts into one system in a coordinated manner would support the
government and ensure that a good system evolves to take charge of procurements in the immediate
and long term.
The government needs to take leadership in issues of procurement and supply management
of all medicines and medical supplies by establishing a functional working group to plan and
implement PSM activities
A PSM plan for all categories of medicines needs to be developed to ensure that all
requirements of the country are detailed and partners are thus required to partake in
implementation of the plan
The study demonstrates that procurement and supply of medicines in Nigeria is uncoordinated,
fragmented and unplanned. This situation may be attributed to the absence of strong national
leadership and absence of a procurement supply management plan to articulate the needs of the
country and guide partners who wish to lend a helping hand to the government. Improvements to this
situation will require the adoption of the health systems approach to ensure that the government
addresses all issues about health in a coordinated and sustainable manner. Thus, resources will be
appropriately harnessed and optimized when issues of procurement and management of medicines
and other medical supplies are addressed in a holistic manner and systems are built to sustain the
appropriate cost effective procurement of good quality medicines which are accessible to patients for
the health needs.
RECOMMENDATIONS
19

The National Policy on procurement of medicines and medical supplies should be
developed and disseminated to all partners to ensure conformity of current and future
supports to the country
To ensure conformity to the National Drug Policy requiring flow of medicines through the
Federal Medical Stores, the warehouse should be refurbished into a modern warehouse
which provides appropriate management and security of products. All users of the FMS
should be required to contribute to its maintenance.
A robust medicines and supplies management information system should be established
using modern information technology to ensure the flow of information to all stakeholders
to aid planning and implementation of the PSM system.
20

APPENDIX
List of Partners interviewed
1. GlobalAids Initiative Nigeria (GHAIN-AXIOS)
2. Society For Family Health (SFH)
3. Supply Chain Management System (SCMS)
4. United StateAgency for International Development (USAID)
5. Health Commodity Project (HCP)-CrownAgents
6. Nigeria Partnership For Transforming Health System (PATH)
7. Japan International CooperationAgency (JICA)
8. Medicins Sans Frontieres (MSF)
9. Canadian International DevelopmentAgency (CIDA)
10. United Nation Children's Fund (UNICEF)
11. United Nation Fund for PopulationActivities (UNFPA)
12. Gede Foundation
13. Yakubu Gowon Centre
14. Christian HealthAssociation of Nigeria (CHAN)
15. Christian HealthAssociation of Nigeria-Medipharm (CHAN-MEDIPHARM)
16. World Health Organization (WHO)
21