Embed Size (px)
Citation preview

March 2006
Bromley PCT
Deployment of Connecting for Health PACS
A Programme Manager’s viewpoint
Geoff Broome
March 2006
Agenda
Context and rolesPACS: Why bother?Lessons and challenges– What was hard work– What would we do differently– What we could have been better at
Questions

March 2006
Projects in context – old world
Your project
Trust
SHA
Supplier
Requirements Responses and delivery
InformationAuthority
Support andstandards
Approval and performancemanagement
March 2006
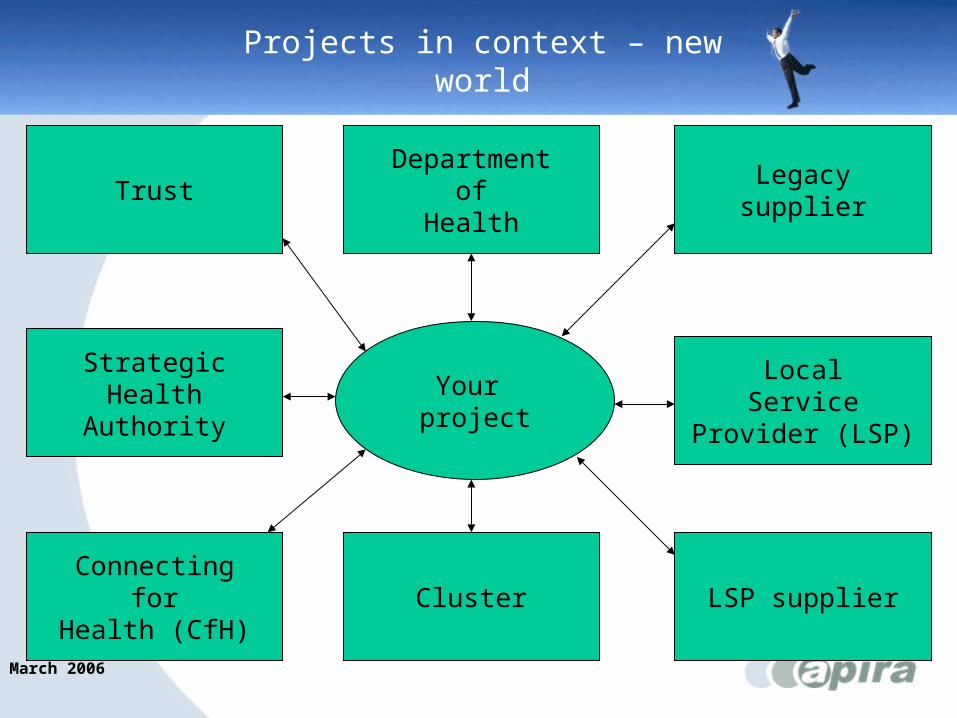
Projects in context – new world
Your project
Trust
Cluster
Legacysupplier
Connectingfor
Health (CfH)
Departmentof
Health
StrategicHealth
Authority
LocalService
Provider (LSP)
LSP supplier
March 2006
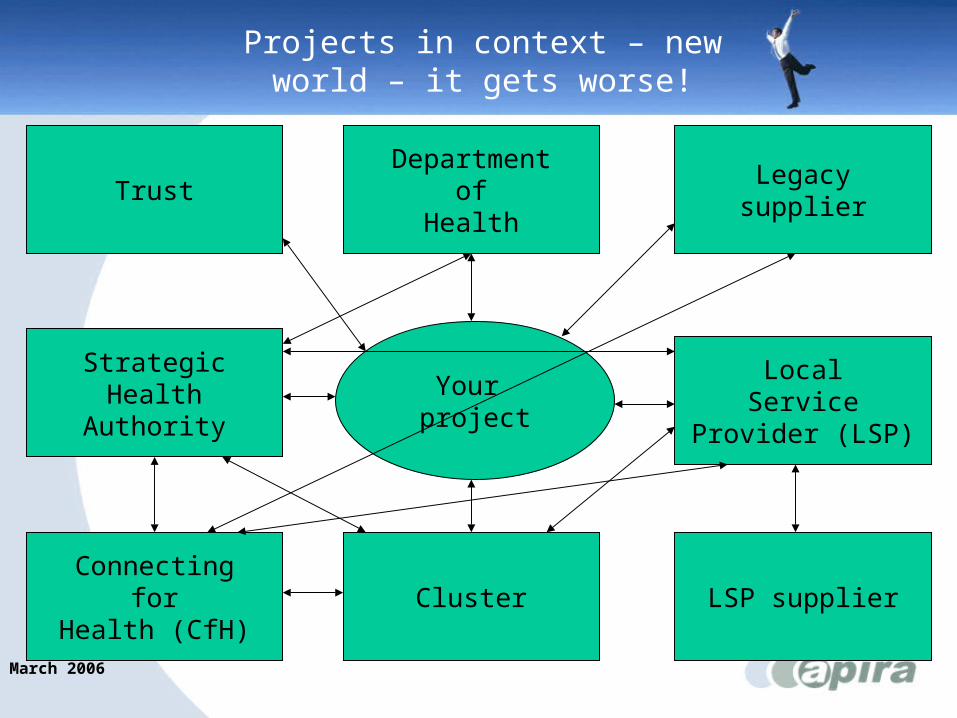
Projects in context – new world – it gets worse!
Your project
Trust
Cluster
Legacysupplier
Connectingfor
Health (CfH)
Departmentof
Health
StrategicHealth
Authority
LocalService
Provider (LSP)
LSP supplier

March 2006
Context and roles (1)
PACS was an afterthought in national programme– no Trust level input to negotiations– anything in “too hard/ risky” or “can’t assess”
column given to Trusts– Trusts categorised as S/M/L
CCA role– between supplier and Trust– contractual risk and margin management– had to sign off changes without knowledge of
context
March 2006
Context and roles (2)
Cluster role– was CCAs “client”– programme management with CfH interests
driving them
Trust role– bigger than anticipated – not always clear – negotiated by others
March 2006
Context and roles (3)
Philips role– supplier with hands tied behind back– forced to work through CCA– no direct contact with the Trust allowed
March 2006
PACS: Why bother? (1)
Strategic flexibility/ position – to grow, distribute diagnostic services– better (more multi-disciplinary) practice
• ease of getting others involved
– many risks held outside Trust level
Patients want (expect) it– may influence GPs referring behaviour
Clinicians wanted it– decision support system– better (flexible) working conditions for staff
(recruitment/ retention)
– Qudos

March 2006
PACS: Why bother? (2)
It is working and is free to air (albeit with large project costs)Will differentiate Trusts that have it as “forward thinking” for a while at leastUltimately will improve departmental efficiency with knock on effect in wider hospital– investigations/ radiology department employee– cancelled appointments/ repeat tests due to
mislaid images– Average Length of Stay (ALOS)

March 2006
PACS: Why bother? (3)
If you are not doing anything else you will learn about the programme
Some of the lessons are being learnt and should make later projects easier!

March 2006
What was hard work (1)
Agreeing plan (inc. technical details) and who owns it– roles, governance, configuration management
Getting through CCA/ cluster to the supplier– many more relationships to be managed
Educating CCA about the NHS– role of doctors and the need to listen to them– clinical risks and why we try and minimise
them

March 2006
What was hard work (2)
Educating CCA (in particular) about the need to get user acceptance for systems to workGetting past the “contractual” in order to deliver an acceptable local solutionStopping them “presumptively closing” re acceptance and moving on to new projects– managing the move to later phases– support in a business as usual world

March 2006
What was hard work (3)
Identifying all users and roles
Gaining respect for role of Project Board and ensuring that suppliers and cluster do not circumvent it

March 2006
What would we do differently (1)
Engage non-Radiology users earlierThink about partner relationships which may be impacted – especially if you are a supplier of diagnostic
services
Have better test plans and insist on themEngagement of operational management earlier and in more detail, especially re workflow design

March 2006
What would we do differently (2)
Engagement of information governance specialists earlier to ensure access policies and disaster recovery issues are tackledAgree business plans with clear funding sources and contingencies before the project starts– including backfill
Think about how junior doctor rotation should be managed vis a vis training

March 2006
What we could have been better at (1)
Analysing Trust side responsibilities and ensuring we had the funds and capability to deliverCommunications especially outside RadiologyAllocating dedicated training facilitiesWatching our audit trail and ensuring good configuration management on our side

March 2006
What we could have been better at (2)
External relationship building– differentiating the must win battles from nice
to haves– being prepared to help external parties
Getting specification nailed down, changes were difficult to agree, caused delays and were expensive
March 2006
Summary – take home messages (1)
Insist on role as customer but don’t try to fight on all fronts at once– try to understand and come to terms with the
supplier/ cluster/ SHA/ CfH side– use PRINCE2 to make sure that suppliers stay
focussed on your agenda and managerial attention on issues is sustained
• keep the focus on your Project
Make sure you manage your own side well, do not give them weapons– be persistent and be prepared to repeat yourself or
change audience– do not select purely “administrative” project
managers

March 2006
Summary – take home messages (2)
Pick strong and knowledgeable “Senior User(s)” or “Business Change Managers”– expose all external parties to vociferous but
articulate users– listen to them, but be willing to challenge
appropriately in right setting
It’s our programme let’s fix it

March 2006
Questions
?





























