Embed Size (px)
Citation preview

Postgraduate Medical Journal (1988) 64, 497-504
Some connective tissue disorders of the lungMargaret Turner-WarwickCardiothoracic Institute, University of London, Fulham Road, London SW3 6HP, UK.
Summary: Many connective tissue disorders involve the lungs. The same clinical syndrome maybe associated with several distinctive types of pathology in different patients. Fibrosing alveolitis is a
common feature of a number of different syndromes. An hypothesis is set out in schematic formwhich may help to account for some of these differences and emphasizes the potential importance ofthe pulmonary vasculature in pathogenesis.
Introduction
The tissues of the lung alone receive virtually theentire venous circulating blood volume comingfrom other organs of the body. It is not thereforesurprising that the lungs are affected in a widevariety of multisystem disorders. In particular it isnot suprising that an inflammatory response andfibrotic reaction in the lung is common to severaldifferent connective tissue syndromes including sys-temic lupus erythematosus (SLE), rheumatoid arth-ritis and systemic sclerosis as well as occurringoccasionally in a number of other conditions suchas primary biliary cirrhosis, chronic active hepatitis,ulcerative colitis, Sj6gren's syndrome, autoimmunethyroiditis and ill defined digital vasculitides. Acentral unresolved question is why lung involve-ment is very common in certain syndromes such assystemic sclerosis and apparently very much lesscommon in others such as ulcerative colitis andperhaps chronic hepatic disease. Another unex-plained fact is that a number of different types ofpathology may be found in the lungs of differentpatients with the same connective tissue syndrome(Table I). For example, in rheumatoid arthritis,
Table I The overlap of pulmonary pathology in variousdifferent connective tissue disorders
Systemic RheumatoidSLE sclerosis arthritis
Pulmonary haemorrhage + - -Acute alveolitis + - +Pleural effusions + + - +Fibrosing alveolitis + + + + ++Necrobiotic nodules - - +Obliterative
bronchiolitis - - +
necrotic nodules, pleural effusions, alveolitis or
rarely pulmonary hypertension may each be thepredominating lesion in different patients.Another current unresolved argument centres on
whether 'cryptogenic' fibrosing alveolitis (CFA)occurring in association with connective tissue dis-orders differs from 'lone' CFA (i.e. that conditionapparently affecting the lungs only) either in itsnatural history or in its response to treatment.The question has been considered in a large
retrospective series of 139 patients with 'lone' CFA,comparing them to 66 patients with associatedconnective tissue diseases and followed during treat-ment over a similar period of time.1 The clinicalfeatures at presentation were found to be verysimilar although there was a trend towards a
greater male predominance in those with 'lone'CFA. In particular, the severity of symptoms was
notably similar. From this series about two thirdsof each group was selected on clinical grounds fortreatment with corticosteroids and a similar propor-tion showed a subjective improvement whenassessed after 4 to 8 weeks, although there was a
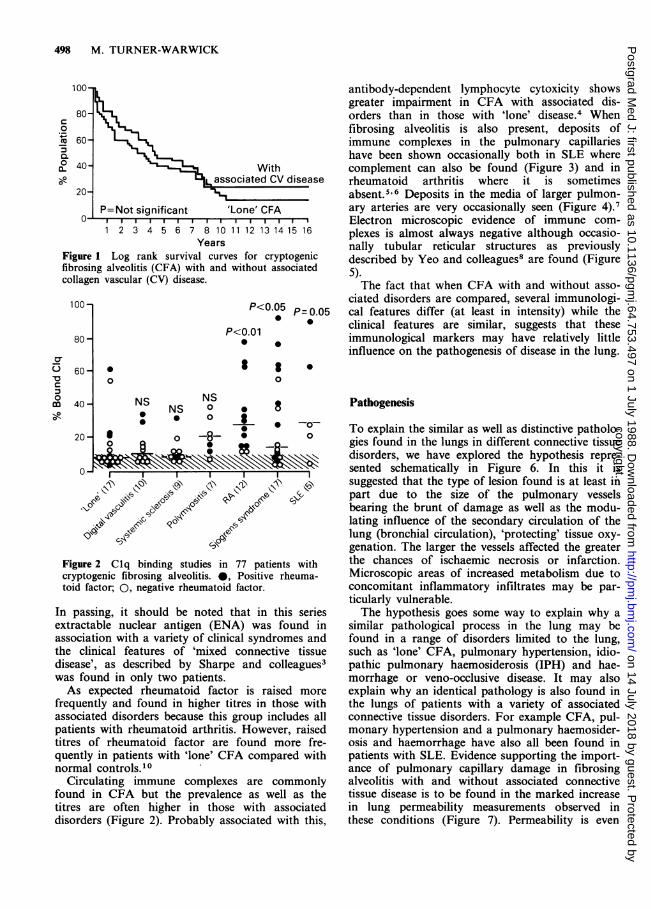
trend towards a better response in those withassociated disease. Overall, however, the survivalcurves were almost superimposable even in thosepatients who had been followed for up to 15 years(Figure 1).
In spite of the many clinical similarities shownbetween CFA with and without associated dis-orders, some of the immunological characteristicsdiffer. Circulating non-organ specific autoantibodiesare increased in both groups but the frequency ishigher in those with associated disease. Some differ-ences are also found in the type of nuclear anti-bodies demonstrated. For example Chapman andcolleagues2 showed that extractable anti-ribonuclearprotein antibody was found in only 4% of 689patients with 'lone' CFA but in 12 (22%) of 54patients with associated connective tissue disorders.
© The Fellowship of Postgraduate Medicine, 1988
Correspondence: Professor M. Turner-Warwick, Ph.D.,D.Sc.(Hon), D.M., F.R.C.P., F.R.A.C.P., F.A.C.P.(Hon).
copyright. on 14 July 2018 by guest. P
rotected byhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.64.753.497 on 1 July 1988. Dow
nloaded from
498 M. TURNER-WARWICK
100-
80-C0
° 60
0.4040- With
-00- associated CV disease20-
0 P=Not significant 'Lone' CFA0 ~ 1 1 1 i
1 2 3 4 5 6 7 8 10 11 12 13 14 15 16Years
Figure 1 Log rank survival curves for cryptogenicfibrosing alveolitis (CFA) with and without associatedcollagen vascular (CV) disease.
100- P<005=.05
P<0.0180
-
60- 0 * 00 0
c
C 40 NS NS-0 NS
20 0 -8- 00~~~~
0-I~~~~~~I
,( C>,
C3A
Figure 2 Clq binding studies in 77 patients withcryptogenic fibrosing alveolitis. 0, Positive rheuma-toid factor; 0, negative rheumatoid factor.
In passing, it should be noted that in this seriesextractable nuclear antigen (ENA) was found inassociation with a variety of clinical syndromes andthe clinical features of 'mixed connective tissuedisease', as described by Sharpe and colleagues3was found in only two patients.As expected rheumatoid factor is raised more
frequently and found in higher titres in those withassociated disorders because this group includes allpatients with rheumatoid arthritis. However, raisedtitres of rheumatoid factor are found more fre-quently in patients with 'lone' CFA compared withnormal controls.I0
Circulating immune complexes are commonlyfound in CFA but the prevalence as well as thetitres are often higher in those with associateddisorders (Figure 2). Probably associated with this,
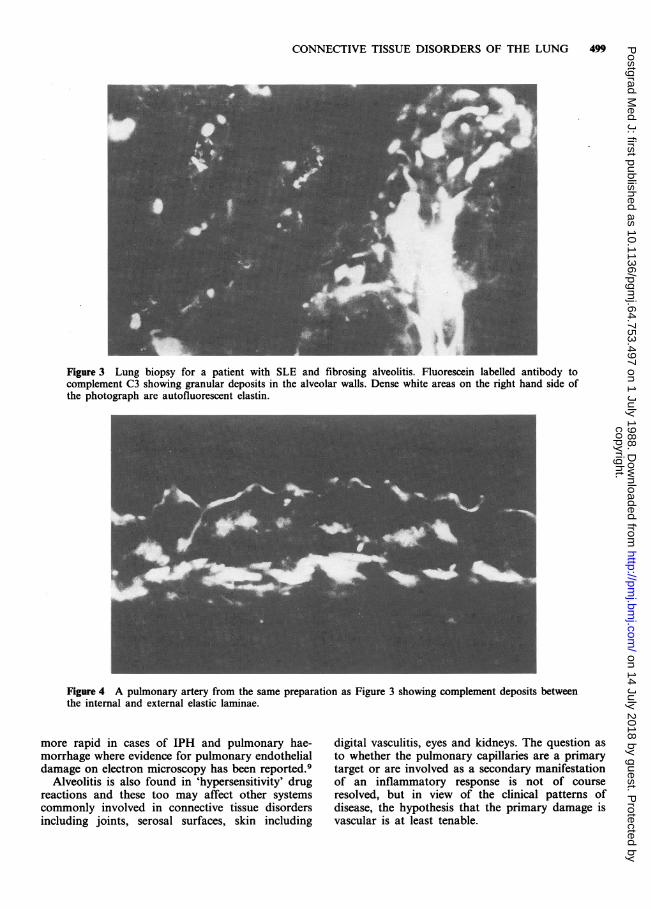
antibody-dependent lymphocyte cytoxicity showsgreater impairment in CFA with associated dis-orders than in those with 'lone' disease. Whenfibrosing alveolitis is also present, deposits ofimmune complexes in the pulmonary capillarieshave been shown occasionally both in SLE wherecomplement can also be found (Figure 3) and inrheumatoid arthritis where it is sometimesabsent.5 6 Deposits in the media of larger pulmon-ary arteries are very occasionally seen (Figure 4).7Electron microscopic evidence of immune com-plexes is almost always negative although occasio-nally tubular reticular structures as previouslydescribed by Yeo and colleagues8 are found (Figure5).The fact that when CFA with and without asso-
ciated disorders are compared, several immunologi-cal features differ (at least in intensity) while theclinical features are similar, suggests that theseimmunological markers may have relatively littleinfluence on the pathogenesis of disease in the lung.
Pathogenesis
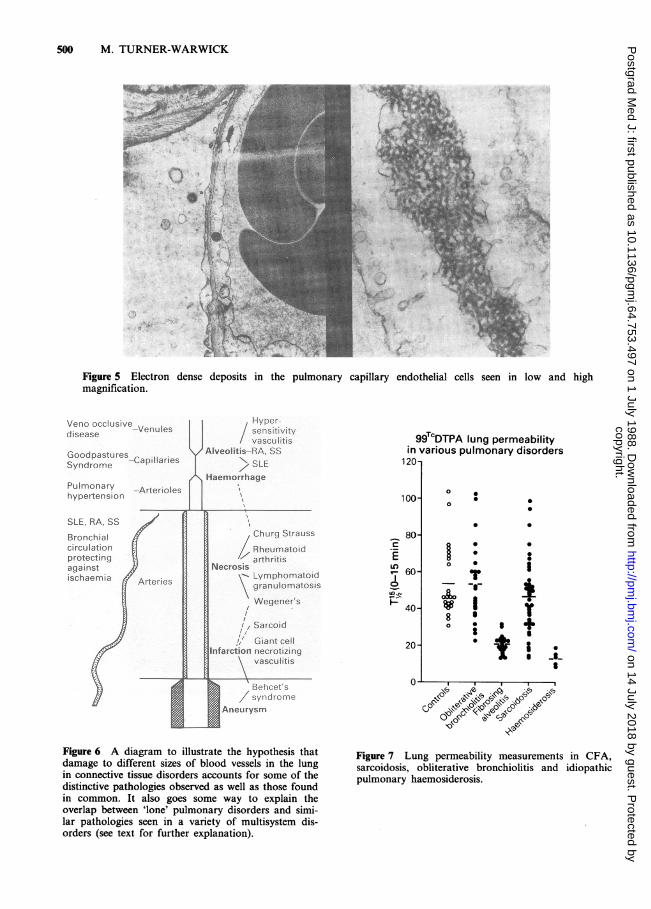
To explain the similar as well as distinctive patholo-gies found in the lungs in different connective tissuedisorders, we have explored the hypothesis repre-sented schematically in Figure 6. In this it issuggested that the type of lesion found is at least inpart due to the size of the pulmonary vesselsbearing the brunt of damage as well as the modu-lating influence of the secondary circulation of thelung (bronchial circulation), 'protecting' tissue oxy-genation. The larger the vessels affected the greaterthe chances of ischaemic necrosis or infarction.Microscopic areas of increased metabolism due toconcomitant inflammatory infiltrates may be par-ticularly vulnerable.The hypothesis goes some way to explain why a
similar pathological process in the lung may befound in a range of disorders limited to the lung,such as 'lone' CFA, pulmonary hypertension, idio-pathic pulmonary haemosiderosis (IPH) and hae-morrhage or veno-occlusive disease. It may alsoexplain why an identical pathology is also found inthe lungs of patients with a variety of associatedconnective tissue disorders. For example CFA, pul-monary hypertension and a pulmonary haemosider-osis and haemorrhage have also all been found inpatients with SLE. Evidence supporting the import-ance of pulmonary capillary damage in fibrosingalveolitis with and without associated connectivetissue disease is to be found in the marked increasein lung permeability measurements observed inthese conditions (Figure 7). Permeability is even
copyright. on 14 July 2018 by guest. P
rotected byhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.64.753.497 on 1 July 1988. Dow
nloaded from
CONNECTIVE TISSUE DISORDERS OF THE LUNG
Figure 3 Lung biopsy for a patient with SLE and fibrosing alveolitis. Fluorescein labelled antibody tocomplement C3 showing granular deposits in the alveolar walls. Dense white areas on the right hand side ofthe photograph are autofluorescent elastin.
Figure 4 A pulmonary artery from the same preparation as Figure 3 showing complement deposits betweenthe internal and external elastic laminae.
more rapid in cases of IPH and pulmonary hae-morrhage where evidence for pulmonary endothelialdamage on electron microscopy has been reported.9
Alveolitis is also found in 'hypersensitivity' drugreactions and these too may affect other systemscommonly involved in connective tissue disordersincluding joints, serosal surfaces, skin including
digital vasculitis, eyes and kidneys. The question asto whether the pulmonary capillaries are a primarytarget or are involved as a secondary manifestationof an inflammatory response is not of courseresolved, but in view of the clinical patterns ofdisease, the hypothesis that the primary damage isvascular is at least tenable.
499
copyright. on 14 July 2018 by guest. P
rotected byhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.64.753.497 on 1 July 1988. Dow
nloaded from
500 M. TURNER-WARWICK
40
~~~~~~~~~I~~~~~~~~~~~~~~~~~~~~~~~J.~~~~~~~~~~~~~g
-Aso.,/
Figure 5 Electron dense deposits in the pulmonary capillary endothelial cells seen in low and highmagnification.
Veno occlusive | senrvitydisease Ienul vascunitis
Goodpastures Aivnlltb-RA, SS-CapillariesSyndrome > SLEHaemorrhage
Pulmonary -Arterioleshypertension
SLE, RA, SS iBronchial { } Churg Strausscirculation Rheurnatoidprotecting -artvtisagainst rischaemia {Arteries
granulonwtotisWegeners
Sarcoid. Giant cell
a9'e;t.o necrotizingz~~~~~~--a. it
Behcet's/ syndrome
Aneurysm
Figure 6 A diagram to illustrate the hypothesis thatdamage to different sizes of blood vessels in the lungin connective tissue disorders accounts for some of thedistinctive pathologies observed as well as those foundin common. It also goes some way to explain theoverlap between 'lone' pulmonary disorders and simi-lar pathologies seen in a variety of multisystem dis-orders (see text for further explanation).
99TcDTPA lung permeabilityin various pulmonary disorders
120
0100
* c_ 80
E60 0
40 V 1o is +
2 *
20-
O~~~~~~~~0*Go l0d
Oc~O~,kFigure 7 Lung permeability measurements in CFA,sarcoidosis, obliterative bronchiolitis and idiopathicpulmonary haemosiderosis.
copyright. on 14 July 2018 by guest. P
rotected byhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.64.753.497 on 1 July 1988. Dow
nloaded from
CONNECTIVE TISSUE DISORDERS OF THE LUNG 501
Where larger vessels are affected or where largerareas of inflammation are not associated with acorresponding angiogenesis and cannot be reachedfor anatomical reasons by the bronchial circulation,ischaemic necrosis may develop. Such a hypothesiscould contribute to explain the necrotic lesions seenin rheumatoid arthritis, Wegener's granuloma, andthe rare syndrome of necrotizing sarcoidosis - in allof which there is good evidence of an associatedvasculitis of vessels larger than capillaries. Whereeven larger vessels are involved infarction may befound as in Behret's disease10 and some patientswith SLE.
Evidence of host susceptibility to lung involvementin connective tissue disorders
An explanation must be sought for the fact thatonly a small proportion of patients with certainconnective tissue disorders develop any type of lunginvolvement. Many years ago, Tomasi and collea-gues1 suggested that those patients with especiallyhigh titres of rheumatoid factor were more likely todevelop fibrosing alveolitis. An early study of ourpatients with rheumatoid arthritis with and withoutfibrosing alveolitis showed that the distribution ofrheumatoid factor was in fact very similar.l2 Indir-ect evidence suggestive of some susceptibility is,however, indicated by the finding that over 70% ofa series of 39 patients with fibrosing alveolitis andrheumatoid arthritis developed lung involvementwithin 4 years of the onset of joint symptoms.Conversely, of those rare cases where the lungswere involved first, the joints were affected within 3years.l3 Thus CFA seems to appear as a relativelyearly manifestation of rheumatoid disease in apredisposed sub-group of patients. The markers forthis susceptibility towards lung involvement havenot yet been identified.
Perhaps the most clear-cut evidence of an identi-fiable susceptibility is provided by the marker,histidyl t-RNA synthetase (anti-Jo-1 antibody) inpolymyositis. Bernstein and colleagues14 haverecently shown that this antibody was present inless than 5% of patients with polymyositis or CFAalone, but was observed in 77% of patients withthe combined syndrome. This finding suggests thatanalogous markers might be sought in other con-ditions. Such markers might then be used to estab-lish whether a genetic predisposition is important inthe development of lung disease. This in turn mightalso give us more insight into the nature of CFAwhen it occurs in the 'lone' form.
The severity and type of fibrosing alveolitisobserved
It is often stated that alveolitis when it occurs inconnective tissue disorders is mild and relatively
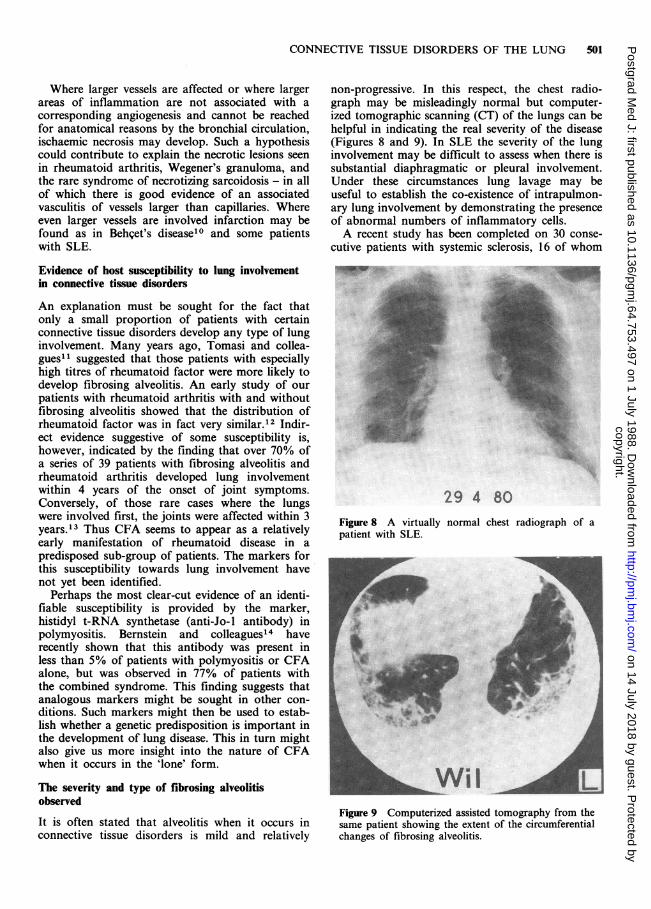
non-progressive. In this respect, the chest radio-graph may be misleadingly normal but computer-ized tomographic scanning (CT) of the lungs can behelpful in indicating the real severity of the disease(Figures 8 and 9). In SLE the severity of the lunginvolvement may be difficult to assess when there issubstantial diaphragmatic or pleural involvement.Under these circumstances lung lavage may beuseful to establish the co-existence of intrapulmon-ary lung involvement by demonstrating the presenceof abnormal numbers of inflammatory cells.A recent study has been completed on 30 conse-
cutive patients with systemic sclerosis, 16 of whom
29 4 80Figure 8 A virtually normal chest radiograph of apatient with SLE.
Figure 9 Computerized assisted tomography from thesame patient showing the extent of the circumferentialchanges of fibrosing alveolitis.
copyright. on 14 July 2018 by guest. P
rotected byhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.64.753.497 on 1 July 1988. Dow
nloaded from
502 M. TURNER-WARWICK
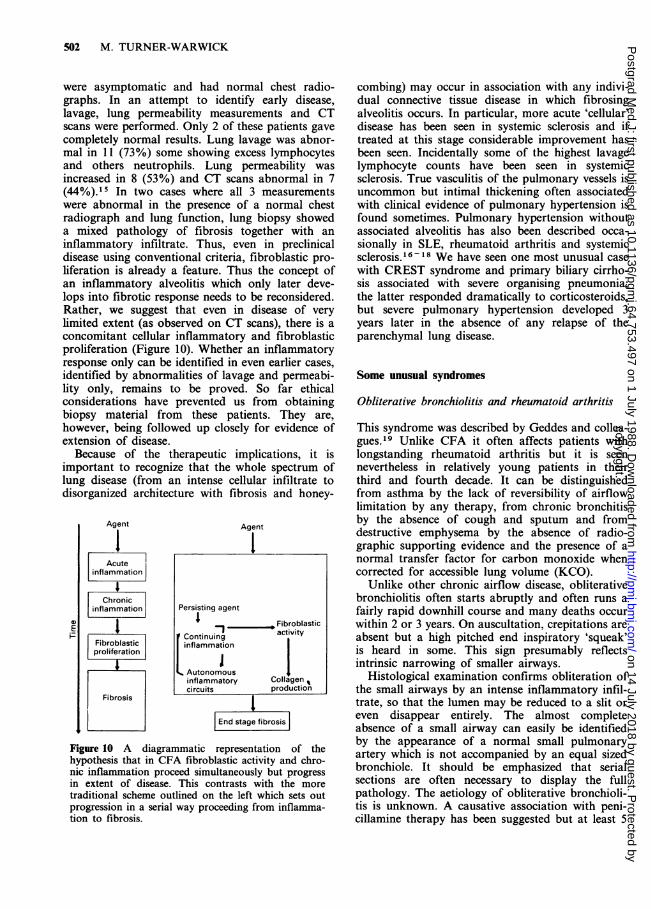
were asymptomatic and had normal chest radio-graphs. In an attempt to identify early disease,lavage, lung permeability measurements and CTscans were performed. Only 2 of these patients gavecompletely normal results. Lung lavage was abnor-mal in 11 (73%) some showing excess lymphocytesand others neutrophils. Lung permeability wasincreased in 8 (53%) and CT scans abnormal in 7(44%).15 In two cases where all 3 measurementswere abnormal in the presence of a normal chestradiograph and lung function, lung biopsy showeda mixed pathology of fibrosis together with aninflammatory infiltrate. Thus, even in preclinicaldisease using conventional criteria, fibroblastic pro-liferation is already a feature. Thus the concept ofan inflammatory alveolitis which only later deve-lops into fibrotic response needs to be reconsidered.Rather, we suggest that even in disease of verylimited extent (as observed on CT scans), there is aconcomitant cellular inflammatory and fibroblasticproliferation (Figure 10). Whether an inflammatoryresponse only can be identified in even earlier cases,identified by abnormalities of lavage and permeabi-lity only, remains to be proved. So far ethicalconsiderations have prevented us from obtainingbiopsy material from these patients. They are,however, being followed up closely for evidence ofextension of disease.
Because of the therapeutic implications, it isimportant to recognize that the whole spectrum oflung disease (from an intense cellular infiltrate todisorganized architecture with fibrosis and honey-
Agent
Acuteinflammation
Chronicinflammation
1Fibroblasticproliferation
Fibrosis
Agent
1
Persisting agent- Fibroblastic
activityIContinuinginflammation
Autonomousinflammatory Collagencircuits production
End stage fibrosis
Figure 10 A diagrammatic representation of thehypothesis that in CFA fibroblastic activity and chro-nic inflammation proceed simultaneously but progressin extent of disease. This contrasts with the moretraditional scheme outlined on the left which sets outprogression in a serial way proceeding from inflamma-tion to fibrosis.
combing) may occur in association with any indivi-dual connective tissue disease in which fibrosingalveolitis occurs. In particular, more acute 'cellular'disease has been seen in systemic sclerosis and iftreated at this stage considerable improvement hasbeen seen. Incidentally some of the highest lavagelymphocyte counts have been seen in systemicsclerosis. True vasculitis of the pulmonary vessels isuncommon but intimal thickening often associatedwith clinical evidence of pulmonary hypertension isfound sometimes. Pulmonary hypertension withoutassociated alveolitis has also been described occa-sionally in SLE, rheumatoid arthritis and systemicsclerosis.16-18 We have seen one most unusual casewith CREST syndrome and primary biliary cirrho-sis associated with severe organising pneumonia;the latter responded dramatically to corticosteroids,but severe pulmonary hypertension developed 3years later in the absence of any relapse of theparenchymal lung disease.
Some unusual syndromesObliterative bronchiolitis and rheumatoid arthritis
This syndrome was described by Geddes and collea-gues.19 Unlike CFA it often affects patients withlongstanding rheumatoid arthritis but it is seennevertheless in relatively young patients in theirthird and fourth decade. It can be distinguishedfrom asthma by the lack of reversibility of airflowlimitation by any therapy, from chronic bronchitisby the absence of cough and sputum and fromdestructive emphysema by the absence of radio-graphic supporting evidence and the presence of anormal transfer factor for carbon monoxide whencorrected for accessible lung volume (KCO).
Unlike other chronic airflow disease, obliterativebronchiolitis often starts abruptly and often runs afairly rapid downhill course and many deaths occurwithin 2 or 3 years. On auscultation, crepitations areabsent but a high pitched end inspiratory 'squeak'is heard in some. This sign presumably reflectsintrinsic narrowing of smaller airways.
Histological examination confirms obliteration ofthe small airways by an intense inflammatory infil-trate, so that the lumen may be reduced to a slit oreven disappear entirely. The almost completeabsence of a small airway can easily be identifiedby the appearance of a normal small pulmonaryartery which is not accompanied by an equal sizedbronchiole. It should be emphasized that serialsections are often necessary to display the fullpathology. The aetiology of obliterative bronchioli-tis is unknown. A causative association with peni-cillamine therapy has been suggested but at least 5
0E
copyright. on 14 July 2018 by guest. P
rotected byhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.64.753.497 on 1 July 1988. Dow
nloaded from
CONNECTIVE TISSUE DISORDERS OF THE LUNG 503
of the 20 cases recently reviewed never received thisdrug (Sweatman, unpublished). Whether penicilla-mine has some facilitating role in other cases isunclear, but this possibility is currently being exa-mined in a case control study.
Digital vasculitis and lung disease
Occasionally patients are seen who develop severedigital vasculitis with necrosis of the finger tips inassociation with fibrosing alveolitis in the lung.20Digital vasculitis of this type is well described insystemic sclerosis and rheumatoid arthritis. Theseassociated conditions were present in 5 of 12recently described cases. Two other cases werefound in association with polymyositis and fibros-ing alveolitis. However, of particular interest were 3cases developing florid digital vasculitis in whichthe only other clinical manifestation was CFA.Circulating immune complexes were infrequent butIgM was often raised in both patients with andwithout arthritis. Corticosteroids did not improvethe vasculitis in any of the 10 cases in which it wasused and, in fact, vasculitis occurred during steroidtreatment of the lung condition in 6. On the otherhand, treatment with immunosuppressant drugs(cyclophosphamide or azathioprine) improved thedigital vasculitis in 4 of 6 patients and penicillamineimproved the fingers in 4 of 5 patients so treated.While corticosteroids uniformly failed to controlthe digital features they frequently improved thelung disease. Thus distinct pathologies occurringsimultaneously in the fingers and lung respondeddifferentially to treatments; a fact that must beaccounted for when attempting to form hypothesesabout pathogenesis.
Lung disease associated with anti-mitochondrialantibodyAt least six distinct lung pathologies have been seenin association with a high titre anti-mitochondrialantibody. These include acute transient 'pneumoni-tis', fibrosing alveolitis, relapsing organising pneu-monia, sarcoid-like granulomas, pleural effusionsand radiographic evidence of small pulmonaryvenous arterial shunts (pulmonary 'spiders').
Sarcoid-like granulomata of the lung associatedwith mitochondrial antibody are of special interestbecause they present a number of features whichare atypical for either sarcoidosis or primary biliarycirrhosis.21 Our cases presented with pulmonarysymptoms and a chest radiograph showing wides-pread nodular shadows which, on biopsy, revealedtypical sarcoid-like granulomata. Enlargement ofthe liver was an incidental finding but the patho-logy of this was variable. In some, there were
granulomata without evidence of inflammatorychanges in the portal tracts and normal biliaryducts; in others there was some evidence of biliarytract involvement. Irrespective of the liver histo-logy, the alkaline phosphatase was considerablyraised in all, as were cytoplasmic liver enzymes. Onthe other hand the serum angiotensin convertingenzyme was normal in one and raised in two casestested before treatment. Treatment with corticoster-oids cleared the lung lesions dramatically but serialstudies on the liver have shown a trend towardsincreasing features of primary biliary cirrhosis withestablished cirrhosis in two. These cases wouldseem to occupy an analogous position to the duckbilled platypus in the evolution of species in that,while extremely rare, they appear to occupy acrucial linking position between a multiorgan sar-coid-like response and immunological and somepathological features of primary biliary cirrhosis.When the pathogenesis of these two conditionseventually becomes clear, the explanation for theserare 'overlap' cases should become apparent.
Another, perhaps uniquely rare, case has beenseen which showed features of CREST syndrome,histologically proven primary biliary cirrhosis andlung pathology of relapsing organising pneumonia.The lung lesions cleared dramatically on corticos-teroids, but relapsed, involving a new site in thelung after 3 years, when the dose of prednisone hadbeen reduced to 5mg on alternate days. This lesiontoo, improved when the dose of steroids wasincreased and later still, severe pulmonary hyperten-sion developed in the absence of relapse of paren-chymal lung disease.That granulomatous lesions and organising pneu-
monia occurring in association with high titre anti-mitochondrial antibody in the same patient are notchance findings is supported by a recent case. Thepatient presented with severe breathlessness andwidespread confluent shadows on the chest radio-graph. These partially cleared spontaneously, butsome nodular lesions persisted. Lung biopsyshowed typical sarcoid-like granulomas in someareas but an organising pneumonia with intra-alveolar fibroblastic proliferation, in others. Hightitre anti-mitochondrial antibody was present andhistology of the liver showed some infiltration ofinflammatory cells in the portal tracts. When thepathogenesis of primary biliary cirrhosis and sarcoi-dosis is eventually established it seems likely thatideas relevant to understanding the pathogenesis ofcryptogenic organising pneumonia may also becomeapparent.
Conclusions
One of the most challenging features of connective
B
copyright. on 14 July 2018 by guest. P
rotected byhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.64.753.497 on 1 July 1988. Dow
nloaded from
504 M. TURNER-WARWICK
tissue disorders affecting the lung is the dichoto-mous situation where on the one hand many dis-tinct pulmonary disorders are found in differentpatients with the same systemic syndrome, but onthe other hand, the same pulmonary pathology(notably fibrosing alveolitis) is found in patientswith clinically distinctive connective tissuesyndromes.The precise pathological features of fibrosing
alveolitis found in an individual patient will alsodepend upon the stage of disease. This ranges froma predominant chronic inflammation response togross fibrotic lung destruction. Recognition ofdifferent stages of disease is of great therapeuticimportance because early active disease (even whenasymptomatic) is more likely to respond to treat-ment than late disease, where destruction of lungarchitecture will deny the opportunity for improve-ment by any form of medication. Thus the aspectsof pathology described here relating to staging are
of more practical importance to clinicians than thelargely academic, semantic exercise of attachingdiagnostic labels to individual patients having theserare, complex, fascinating and often unique combi-nations of features which defy any simple groupingas described in standard textbooks.
AcknowledgementsSome of the ideas propounded in this review wereincluded in the Konrad Hiller Lecture delivered to theRoyal Australasian College of Physicians.
I would like to acknowledge my many colleaguesthroughout the UK who have referred patients withfascinating and rare syndromes which have allowed me todevelop some of the hypotheses proposed in this review.As ever I am also grateful to my junior staff for theirpatience, Dr Pat Haslam for running the laboratory for somany years and Professor Corrin for his collaboration onthe weekly clinical/pathology ward rounds continued formore than a decade.
References
1. Turner-Warwick, M. Interstitial pulmonary fibrosiswith and without associated collagen vascular disease.Am Rev Respir Dis 1981, 123: 73.
2. Chapman, J.R., Charles, P.P.J., Venables, P.J.W. etal. Definition and clinical relevance of antibodies tonuclear ribonuclear protein and other nuclear antigensin patients with cryptogenic fibrosing alveolitis. AmRev Resp Dis 1984, 130: 439-443.
3. Sharp, G.C., Irvin, W.S., Tan, E.M., Gould, R.G. &Hollman, H.R. Mixed connective tissue disease - anapparent distinct rheumatic disease syndromeassociated with a specific antibody to an extractablenuclear antigen (ENA). Am J Med 1972, 52: 148-159.
4. Haslam, P.L., Allan, F., Watling, A.F., Barrett, C.,Morris, L. & Turner-Warwick, M. Impaired antibody-dependent cell-mediated cytotoxicity in cryptogenicfibrosing alveolitis. Clin Exp Immunol 1982, 49: 59-66.
5. de Horatius, R.J.J., Abruzzo, J.L. & Williams, R.C.Immunofluorescent and immunological studies inrheumatoid lung. Arch Int Med 1972. 129: 441-446.
6. Turner-Stokes, L. & Turner-Warwick, M.Intrathoracic manifestations of SLE. Clin Rheum Dis1982, 8: 229-242.
7. Eisenberg, H., Simmons, D.H. & Barnett, E.V.Diffuse pulmonary interstitial disease - animmunohistory study. Chest 1979, 75 (suppl 2):262-264.
8. Yeo, P.P.B. & Sinnian, R. Lupus cor pulmonale withelectron miscroscope and immunofluorescent antibodystudies. Ann Rheum Dis 1975, 34: 457-460.
9. Turner-Warwick, M. & Dewar, A. Pulmonaryhaemorrhage and idiopathic haemosiderosis. ClinRadiol 1982, 33: 361-370.
10. Efthimiou, J., Johnson, C., Spiro, S.G. & Turner-Warwick, M. Pulmonary disease in Behcets syndrome.Q J Med 1986, 58: 259-280.
11. Tomasi, T.B., Fudenberg, H.H. & Finby, N. Possiblerelationship of rheumatoid factors and pulmonarydisease. Am J Med 1962, 33, 243-248.
12. Turner-Warwick, M. & Doniach, D. Autoantibodystudies in interstitial pulmonary fibrosis. Br Med J1965, 1: 886-891.
13. Turner-Warwick, M. & Courtenay-Evans, R.Pulmonary manifestations of rheumatoid disease. ClinRheum Dis 1977, 3: 549-564.
14. Bernstein, R.M., Morgan, S.H., Chapman, J. et al.Anti Jo-1 antibody: a marker for myositis withinterstitial lung disease. Br Med J 1984, 289: 151-152.
15. Glanville, A.R., Harrison, N.K., Miller, A. et al. Theassessment of pulmonary involvement in systemicsclerosis (SS). (in press).
16. Nair, S.S., Askeri, A.D., Popelka, C.G. &Kleinerman, J.F. Pulmonary hypertension in systemiclupus erythematosus. Arch Int Med 1980, 140:109-111.
17. Gardner, D.L., Duthie, J.J.R., McLeod, J. & Allan,W.S.A. Pulmonary hypertension in rheumatoidarthritis. Report of a case with intimal sclerosis of thepulmonary and digital arteries. Scott Med J 1957, 2,183-188.
18. Young, R.H. & Mark, G.J. Pulmonary vascularchanges in scleroderma. Am J Med 1978, 64,998-1004.
19. Geddes, D.M., Corrin, B., Brewerton, D.A., Davies,R.J. & Turner-Warwick, M. Progressive airways andobliteration in adults and its association withrheumatoid diseases. Q J Med 1977, 184: 427-444.
20. Hodson, M.E., Haslam, P.L., Spiro, S.G. & Turner-Warwick, M. Digital vasculitis in patients withcryptogenic fibrosing alveolitis. Br J Dis Chest 1984,78: 140-148.
21. Fagan, E.A., Moore-Gillon, J.C. & Turner-Warwick,M. Multiorgan granulomas and mitochondrialantibodies. N Engl J Med 1983, 308: 572-575.
22. Davison, A.G. & Epstein, O. Relapsing organizingpneumonitis in a man with primary biliary cirrhosis,CREST syndrome and chronic pancreatitius. Thorax1983, 38: 316-317.
copyright. on 14 July 2018 by guest. P
rotected byhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.64.753.497 on 1 July 1988. Dow
nloaded from





























