Embed Size (px)
Citation preview
Andi Marmor, MD, MSEdAssociate Professor, PediatricsUniversity of California, San Francisco
Febrile seizures: Who need further workup? Afebrile seizures: Who needs imaging? Status epilepticus: Most effective treatments
Febrile seizures: Who need further workup? Afebrile seizures: Who needs imaging? Status epilepticus: Most effective treatments
Tesla is a previously healthy 16 mo girlBIB ambulance after she “had a seizure” Fell to the ground while playing and became stiff and non‐responsive, eyes rolled back, for 30 seconds – 911 called
No apnea or focal movements noted Sleepy but responsive in the ambulance, T = 37.9

Febrile to 39.0, VS otherwise WNL Neuro: Moving all extremities, fussy but consolable by father
Initially sleepy but becoming more and more alert as you observe her
No source for fever is apparent on history/PE
A. Obtain blood, urine and CSF culturesB. Admit for neurologic evaluationC. Obtain a head CT or MRID. Obtain a stat EEGE. Discharge when at neurologic baseline
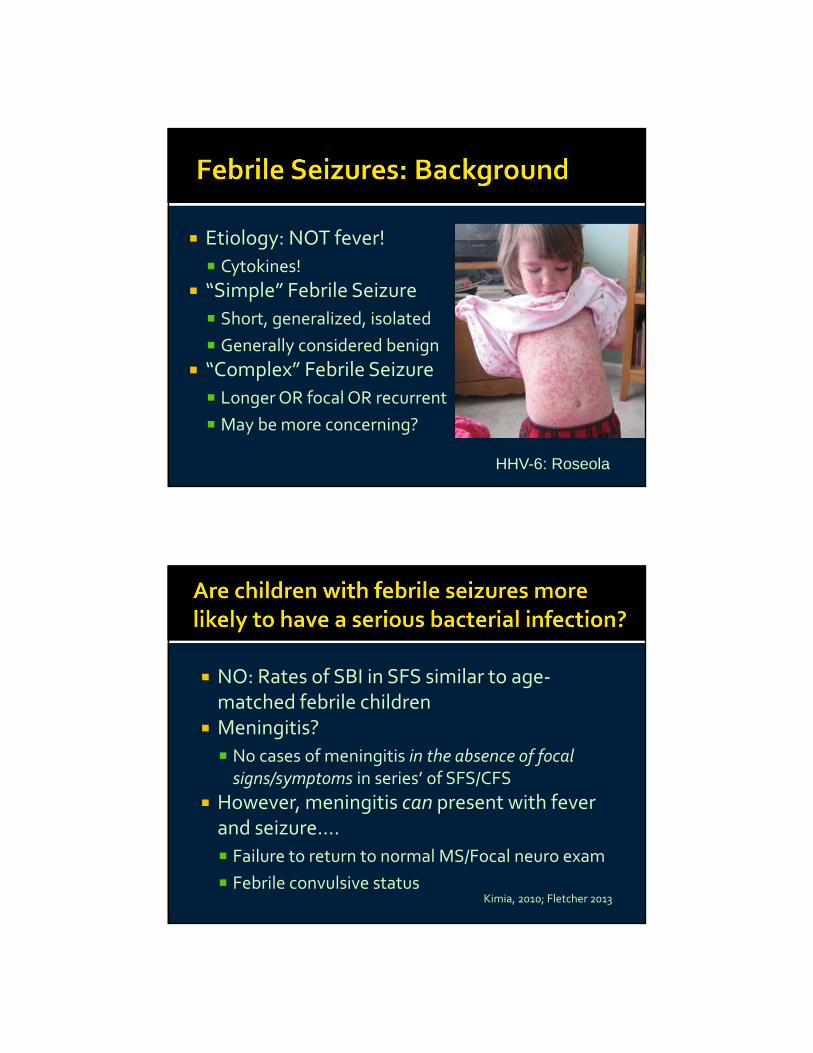
Etiology: NOT fever!
Cytokines!
“Simple” Febrile Seizure
Short, generalized, isolated
Generally considered benign
“Complex” Febrile Seizure
Longer OR focal OR recurrent
May be more concerning?
HHV-6: Roseola
NO: Rates of SBI in SFS similar to age‐matched febrile children
Meningitis?
No cases of meningitis in the absence of focal signs/symptoms in series’ of SFS/CFS
However, meningitis can present with fever and seizure….
Failure to return to normal MS/Focal neuro exam
Febrile convulsive statusKimia, 2010; Fletcher 2013
Your patient comes back within 24 hours with another short, generalized seizure
Now what would you do? Even children with CFS are at very low risk for SBI/meningitis
LP can be done in select children with concerning features
Febrile status, focal/abnormal neuro exam, recent antibiotics
Kimia, 2010; Fletcher 2013
EEG: Not useful in predicting recurrence or epilepsy, even in complex febrile seizures
Anticonvulsants/antipyretics : do not alter course
Confirm child has no neurologic abnormality Identify and treat source for fever, by age Further workup based on H and P
LP for convulsive status, abnormal neuro exam
Consider LP for
Recent antibiotics, several days of fever before sz
Consider referral to neuro for
Focal seizure or recurrent complex seizure
DC when back at neurologic baseline Educate on recurrence: 10‐50%
Younger age, family history, complex seizure, lower temperature
Treat fevers appropriately for comfort only
Leaf is a 2 yo boy BIB ambulance after a generalized, tonic clonic seizure
Given rectal diazepam seizure has ceased
No prior seizures, developmentally normal
Deny trauma, recent illness, travel, change in diet.
He is afebrile, sleepy but arousable
Pushes you away purposefully and symmetrically, and knows his name and age
A. Head CT B. Head MRIC. Complete H and PD. CBC and electrolytesE. Lumbar puncture
Yield of imaging in children with a first‐time afebrile seizure is very low
8% in one study (Sharma, 2003), with < 1% requiring immediate management
Findings requiring intervention can be predicted by
Predisposing factors (trauma, bleeding disorder)
Age < 6 months
Persistent neurologic abnormality
Neuroimaging, screening labs and/or lumbar puncture should not be routinely performed
Consider imaging in the ED (CT or MRI) if
History concerning for IC abnormality
Persistent neurologic abnormality
< 6 mo of age
Schedule pediatric/neurology follow up
May include EEG, MRI if indicated (eg: focal seizure, < 3 years of age)
Hirtz, 2000
Your resident calls you back in because Leaf has started to seize again
The seizure is generalized, and he is breathing on his own
VS: HR 150, RR 30, BP 110/75 You are concerned that Leaf is now in status epilepticus
The RN mentions that the IV is not flushing
A. IV lorazepamB. IM lorazepamC. IM midazolamD. Rectal diazepamE. Buccal midazolam
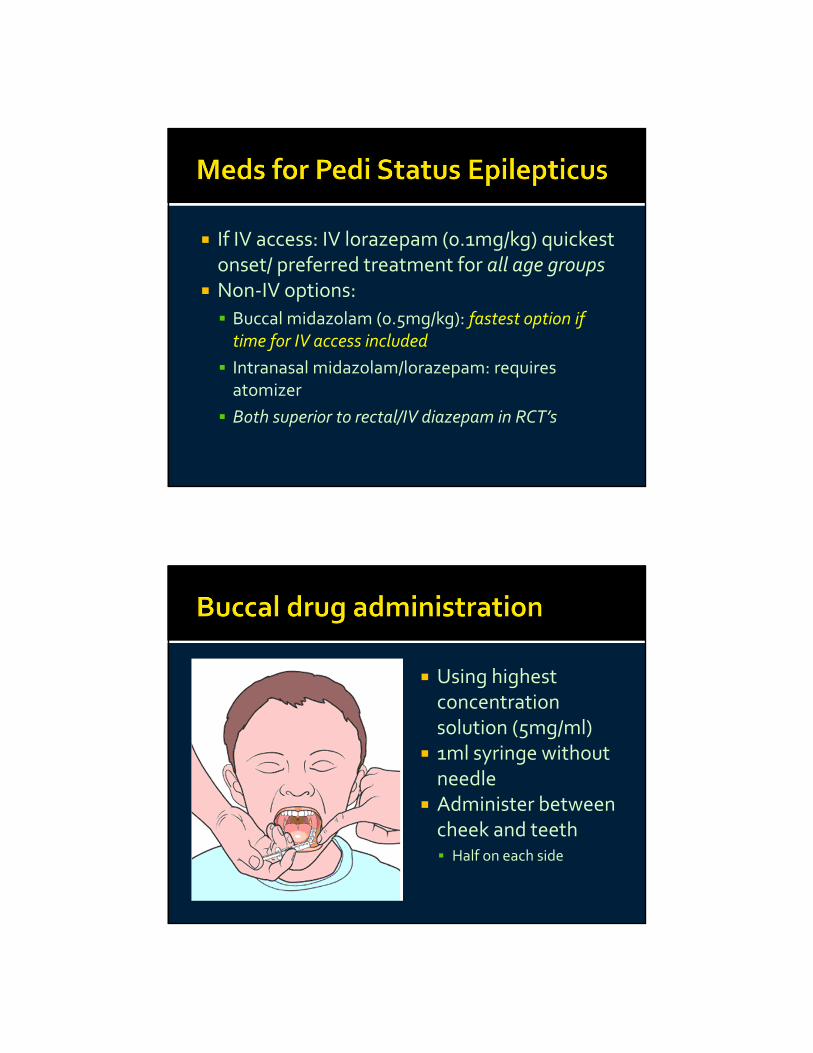
If IV access: IV lorazepam (0.1mg/kg) quickest onset/ preferred treatment for all age groups
Non‐IV options:
Buccal midazolam (0.5mg/kg): fastest option if time for IV access included
Intranasal midazolam/lorazepam: requires atomizer
Both superior to rectal/IV diazepam in RCT’s
Using highest concentration solution (5mg/ml)
1ml syringe without needle
Administer between cheek and teeth Half on each side
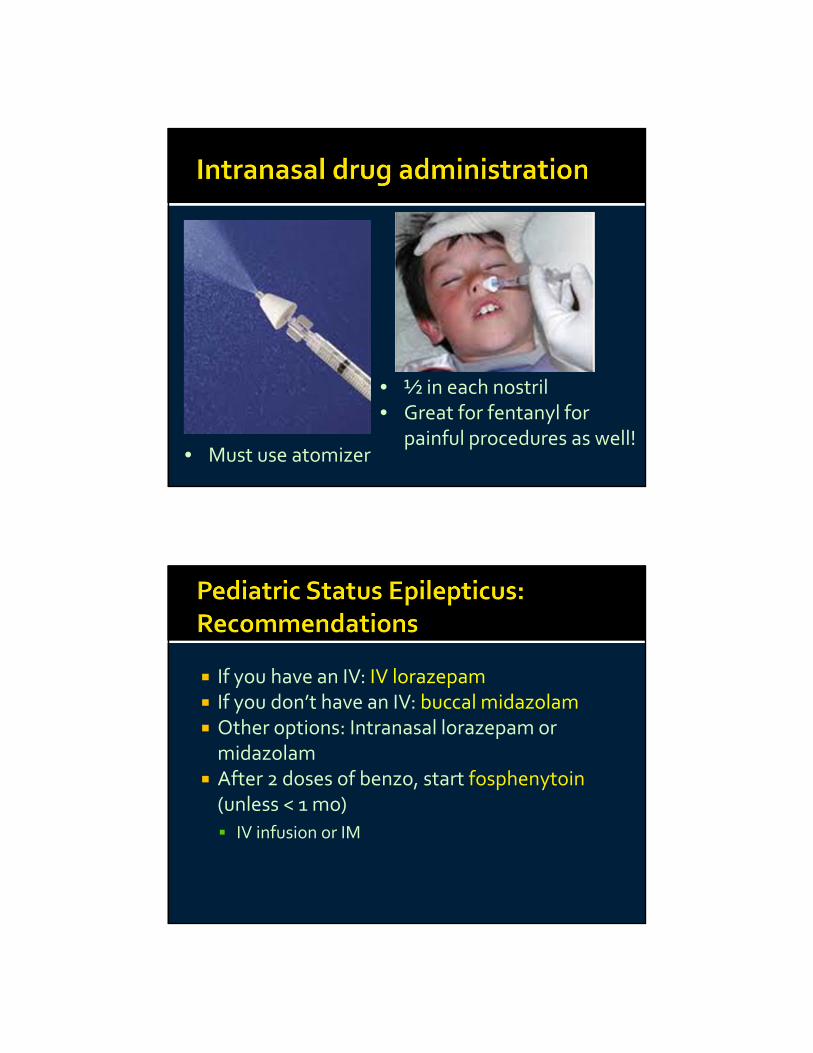
• ½ in each nostril• Great for fentanyl for
painful procedures as well!• Must use atomizer
If you have an IV: IV lorazepam If you don’t have an IV: buccal midazolam Other options: Intranasal lorazepam or midazolam
After 2 doses of benzo, start fosphenytoin(unless < 1 mo)
IV infusion or IM
Febrile Seizures: No additional studies needed for SFS or CFS if neuroexam improving at 30 min and normal at 1 hour
Consider LP if: < 12 moAND previous antibiotic treatment, seizure late in illness
Afebrile Seizures: Imaging rarely indicated, if normal exam and no predisposing factors
Treat pediatric status epilepticus with IV lorazepam or buccal midazolam x2
Then fosphenytoin
Andrea Marmor, MD UCSF High Risk Emergency Medicine May, 2014
1
Pediatric Seizures Andi Marmor, MD ([email protected])
▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪
FEBRILE SEIZURES ▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪ Question: What evaluation is indicated after a febrile seizure? Background
Definition: A seizure occurring in an otherwise well child 6 mo to 5 years of age without a seizure disorder or underlying neurologic disease, who is febrile or becomes febrile within 30 min of the seizure
Febrile seizures are generally considered a benign condition of childhood, and do not carry any significant risk of neurologic sequelae
Simple febrile seizures (SFS) are short (<15min), generalized, non‐recurring in 24 hours
Complex febrile seizures (CFS) may be prolonged, focal or recurring
The most controversial question that arises for children with a febrile seizure is whether LP is indicated Epidemiology:
Febrile seizures account for about 80% of first time pediatric seizures o Occur in 2‐5% of all children, with no geographic, racial or ethnic differences in incidence o Family history in 25‐40% of cases
About 80% are “simple febrile seizures” o Complex febrile seizures (CFS) cause a higher degree of concern, and are associated with higher rates of
status epilepticus, recurrence and epilepsy
Viral infections are the most common associated finding (especially HHV‐6); also recent vaccination with DTaP Etiology:
Mounting evidence suggests that the etiology for febrile seizures is inflammatory cytokine elevations, rather than elevated body temperature (Straussberg, 2001)
HHV‐6 and HHV‐7 infection seems to be a major viral cause of febrile seizures o 13‐36% of kids with HHV‐6 have febrile seizures, and up to 7% of those with HHV‐7 (Oluwabusi, 2012) o Implicated in up to 1/3 of first‐time febrile seizures (Oluwabusi, 2012)
Of note, fever may not be detectable at the time of seizure, but may present up to 30 minutes after the seizure
Febrile seizures typically occur at the onset of a febrile illness o Seizures occurring in children who have been febrile for several days, or those who have been pre‐treated
with antibiotics, should be managed more conservatively
SFS accompanying a febrile illness does not indicate more severe infection: o Rates of serious bacterial infection (particularly acute bacterial meningitis ‐ ABM) in infants/children with
SFS are no higher than febrile children without seizures. o Several recent studies have established that even CFS is rarely the sole presenting sign of meningitis
Prognosis:
No increased risk of mortality, hemiplegia or mental retardation in children with SFS
Risk of epilepsy slightly higher with SFS than in general population o Risk of epilepsy higher with complex features: recurrent or focal seizures, or febrile status epilepticus
Recurrence of febrile seizures occurs in about 10‐50%, depending on risk factors o Age < 12 mo, +family hx, lower temperature or complex seizure all increase risk of recurrence
Evaluation:
Simple febrile seizure: Most guidelines recommend no testing or imaging in addition to that indicated for evaluation of the fever itself
o AAP Practice Parameter 2011: Recommends against routine blood, CSF, EEG, or imaging studies Targeted evaluation only, as determined by age‐appropriate guidelines for febrile illnesses LP is “optional” in children 6‐12 mo: consider if unimmunized, or pre‐treated with abx
o Recent studies add support to evidence that rates of SBI (including meningitis) in children with SFS are similar to those among age‐matched febrile children without seizures (Trainor, Shah, Green).
o There have been no documented cases of bacterial meningitis presenting with SFS alone (Hampers 2011, Oluwabusi 2012, Hom 2011)
o Routine labs/EEG (electrolytes, glucose, CBC) are of no benefit in the evaluation of the child with 1st SFS.
Andrea Marmor, MD UCSF High Risk Emergency Medicine May, 2014
2
o Multiple studies have established that treatment with anti‐convulsants or antipyretics does not alter recurrence or prognosis (Strengell, 2009)
Complex febrile seizure: Evaluation after CFS is less well‐established – concern is higher for a serious bacterial infection, but multiple studies show rates of SBI remain low in otherwise well‐appearing children with CFS
o Certain features of CFS (such as focality, status epilepticus) may carry more risk than others (Kimia, 2010) o While up to 25% of children with acute bacterial meningitis (ABM) present with seizures, ABM is extremely
rare in children presenting ONLY with CFS (Hampers, 2011) Kimia (2010): retro review of 526 children with CFS, 65% had LP
14 pts had CSF pleocytosis, 2 pts had ABM (both with S. pneumo: 0.9% of those with LP)
Both pts with ABM were ill‐appearing and had focal neuro signs before/after seizure Fletcher (2013): retro review of 193 pts with first CFS, 70% had LP
Those with focality, status epilepticus or needing intubation more likely to get LP
14 pts had pleocytosis, no pts had confirmed ABM (1 was treated empirically) o Routine EEG has no utility in predicting recurrence development of epilepsy in children with CFS
Recommendations
1. In any child 6 mo ‐5 years of age presenting with a febrile seizure (simple or complex): Confirm that the child has no known brain abnormality or previous neurologic insult Verify that neurologic exam steadily improves after brief post‐ictal period, and is at baseline within 1 hour
of seizure Identify and treat the source for their fever, in an age‐appropriate manner
If no source is found, proceed to evaluate for fever without a source (FWS) as indicated, taking into account age, appearance and immunization status (may include testing for UTI)
2. Simple Febrile Seizure: No additional studies are recommended after a simple febrile seizure in a well‐appearing child with a
normal neuro exam 3. Complex Febrile Seizure:
If child is previously well and returns to neurologic baseline after seizure, no additional studies are needed Additional targeted evaluation recommended if
Febrile convulsive status epilepticus Intubation Failure to return to baseline after seizure
Consider evaluation for metabolic, infectious or neurologic causes more strongly if: Infant <6 mo of age Focal characteristics of seizure
4. Additional studies for special situations: Lumbar puncture
Recommended in child with meningeal signs/symptoms, or who fails to return to neurologic baseline Consider in the child who has received recent abx, or who has been febrile for several days prior to seizure Neuroimaging before lumbar puncture only recommended if focal neurologic findings are present If LP is performed, CSF pleocytosis (WBC > 20x106) should not be attributed to seizure alone, and should
prompt further evaluation and treatment for bacterial or viral meningitis Electrolytes, glucose, CBC
Only as specifically indicated by the child’s history or PE EEG
Usually not recommended in ED for febrile seizures May be performed as an outpatient for complex or focal seizures
Neuroimaging Consider for focal seizure with persistent focal neuro exam, concern for child abuse, history of trauma
5. Discharge and follow‐up: Routine use of antipyretics/anticonvulsants is NOT recommended for prevention of recurrence or epilepsy Education and reassurance of parents/guardians and arrange primary care follow up Further neurologic workup (usually outpatient) may be indicated for children with complex or focal
seizures, or with recurrent febrile seizures arousing parental concern
Andrea Marmor, MD UCSF High Risk Emergency Medicine May, 2014
3
Update on Pediatric MeningitisTrends in Incidence and Microbiology
Overall, meningitis has declined significantly in the last 10 years, especially in the 2‐23 month age group
Thigpen (2011) reported trends in incidence and microbiology of meningitis from 1998 ‐2007. o Incidences declined significantly for all age groups except for < 2 mo (increase by 10%, 95% CI = 1‐20)
Decrease in incidence primarily due to S. pneumo decreases Incidence remains highest for patients under 2 mo of age
o The decline was greatest in the 2‐23 mo age group, resulting in an increase in median age (from 30 to 40) o Ethnic disparities remain, with incidence highest in black patients of any age o No change in case fatality rate overall (7%, highest for S pneumo) o All pathogens decreased significantly overall, except for GBS
S. pneumo decreased by 26% , N mening by 58%, H flu by 35% PCV‐7 serotypes decreased 92% overall, but ABM from non‐PCV7 serotypes increased by 61%
Risk of meningitis in different age groups
1. Neonates:
Despite decreases in SBI in neonates, rates of meningitis in infants < 2 mo have not declined (Thigpen, 2011) 2. Infants 1‐3 mo of age
Overall, meningitis is extremely rare in this age group, especially in infants meeting low‐risk criteria (well‐appearing, with negative UA, and normal inflammatory markers)
3. Infants 3 mo to 2 years
In the post‐PCV era, occult meningitis is extremely rare in this age group and LP is not recommended if well‐appearing
Management: Steroids:
A large body of evidence now exists to support the use of steroids prior to antibiotics as an adjunct to the treatment of bacterial meningitis in children.
o Overall, corticosteroids are associated with lower mortality, hearing loss and long‐term neurologic sequelae in both children and adults, for both H. influenza and pneumococcal meningitis
Timing: No benefits have been shown when corticosteroids are administered after antibiotics
Duration of therapy: Most trials studied 4 days of therapy at doses of 0.6‐1 mg/kg/day. No randomized trials have directly compared 2‐day to 4‐day therapy.
Recommendations:
1. Perform Lumbar puncture and start empiric antibiotics in Any febrile infant/child who is toxic appearing or has focal neurologic signs, of any age
2. Strongly consider LP if giving empiric antibiotics for Suspected SBI in infants < 3 mo (eg: for elevated inflammatory markers) or A young, febrile infant in whom clinical assessment is limited (eg: pre‐treated with antibiotics)
3. Steroids Recommended in infants/children >6 weeks of age: as an adjunct to antibiotics in suspected or proven S.
pneumo or H. influenza meningitis Initiate steroid therapy as soon as possible in infants/children >6 weeks of age with suspected or proven S.
pneumo or H. influenza meningitis o Only shown to be effective when given prior to antibiotics
Whenever possible, obtain blood and CSF cultures prior to initiating antibiotics, but do not delay treatment in cases of suspected meningitis
Dosing: dexamethasone 0.15mg/kg every 6 hours Continue steroid therapy for 4 days, in patients with proven or suspected S. pneumo or H. influenza
Discontinue steroids in patients with a completely negative CSF cell count
Andrea Marmor, MD UCSF High Risk Emergency Medicine May, 2014
4
▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪ NON‐FEBRILE SEIZURES
▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪ Question: When is neuroimaging needed for a first‐time non‐febrile seizure? Background
While seizures represent ~2% of pediatric ER visits, only ~20% of these are non‐febrile seizures
Guidelines for imaging in adult patients are based on a high rate of abnormal imaging, with a high proportion of structural lesions requiring immediate therapy.
Evidence
A 2000 practice parameter by the American Academy of Neurology (Hirtz, 2000) concluded that there was insufficient evidence to support a recommendation to routinely perform a lumbar puncture, laboratory studies, or routine neuroimaging in a child >6 months of age after a first unprovoked, nonfebrile seizure.
More recent studies support this selective approach to imaging/diagnostic testing: o Maytal (2000): retrospective study of 63 kids with new‐onset seizures: those with clinically significant
findings on CT were all predicted by history/physical findings o Sharma, 2003 ‐ Retrospective review of 500 1st time afebrile seizures at Boston Children’s ‐ 8% had
clinically significant imaging abnormality (<1% required immediate mgmt). Risk fx for clinically significant abnormalities: 1) predisposing condition 2) focal seizure and < 33 mo
Studies show similar clinical variables predicting those at “high risk” for abnormal imaging: o Predisposing factors for IC abnormality (bleeding D/O, closed head inj, malignancy, HIV, sickle cell dz, etc) o Focal seizure in child <3 yrs (although findings not of immediate therapeutic significance) o Persistent neurologic abnormality (altered consciousness, focal deficits)
Children without these risk factors are very unlikely (1% or less) to have an imaging abnormality requiring ED intervention
Choice of imaging: CT vs MRI o CT has traditionally been used in ED setting for its rapid availability and lack of sedation needed. o MRI is a better study for subtle abnormalities, but unlikely to be of significance in the ED setting. o As MRI is becoming faster and more available, it may be a viable radiation‐free option for pediatric
neuroimaging in the ED Recommendations
1. Every child who has a first, afebrile, non‐provoked seizure should have a complete history and physical to ascertain any provoking events or conditions (trauma, toxins, illness, etc) or neurologic deficits
2. Emergent neuroimaging (CT scan) is not indicated in the ED if: > 6 months of age Normal neuro exam No risk factors/predisposing factors for treatable cause for seizure (eg: bleeding disorder, trauma) Reliable follow up
3. MRI may be used in place of CT if imaging is indicated in the ED and MRI is easily available 4. Screening blood work and/or lumbar puncture should be performed only if specific etiology suspected by H and P 5. Initiating treatment with anti‐epileptics after a first seizure is not recommended 6. Educate parents about the significance and implications of the seizure, and schedule follow up with the child’s
pediatrician or a neurologic consultation within a week. Outpatient workup may include: EEG – potentially helpful in classifying seizure, guiding therapy/prognosis MRI ‐ may be indicated especially in those < 3 with focal seizures.
▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪
PEDIATRIC STATUS EPILEPTICUS ▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪ Question: What are the best drugs for pediatric convulsive status epilepticus (SE)? Background
Delays in treatment of pediatric SE are common, and dosing errors (high or low) are widely reported (Abend, 2010)
Rapid treatment is important, as delay is associated with increased risk of prolonged status, medication failure, and worse outcomes (Abend, 2010, Sofou 2009)
In general, seizure control prior to 30 minutes is the goal
Andrea Marmor, MD UCSF High Risk Emergency Medicine May, 2014
5
Lack of IV access may slow the administration of preferred drugs Evidence:
IV lorazepam (0.1mg/kg, max 4mg) o The safest and most effective initial drug for acute pediatric seizures/SE in all age groups (Appleton, 2010)
Non‐IV options: o Buccal midazolam* (0.5mg/kg, max 10mg):
Superior to rectal diazepam (Appleton, 2010) with seizure control rate of 70% (Sofou 2009) *Most concentrated IV solution should be used: 5mg/ml recommended
o Intranasal* midazolam (0.2mg/kg) or IM midazolam (0.2 mg/kg): Faster than IV diazepam (Sofou, 2009; Silbergleit 2012)
o Intranasal* lorazepam (0.1mg/kg, max 4mg) Superior to IM paraldehyde in an RCT in Africa, longer acting than midazolam
*Intranasal administration requires a nasal atomizer
Fosphenytoin, if available, is superior to phenytoin in safety, and recommended as first‐line for established SE o Dosing in “phenytoin equivalents” = PE o Can be administered more quickly than phenytoin, and IM as well
Recommendations (see Figure 1 in appendix):
1. Initiate treatment promptly, and progress through treatment options quickly A protocol for pediatric status epilepticus may improve speed, consistency and efficacy of treatment
2. The preferred initial treatment for pediatric seizures is IV lorazepam, up to 2 doses If IV access is unavailable, alternatives in order of preference, include:
o Buccal midazolam (0.5mg/kg, max 10 mg) o IM midazolam (0.2mg/kg, max 10 mg) o Intranasal lorazepam (0.1mg/kg, max 4 mg) – consider if suspected ongoing sz focus (eg; CNS infection)
3. Established SE (fails to stop within 5 min of 2nd dose of benzodiazepine): Start infusion of fosphenytoin (preferred) or phenytoin Fosphenytoin (30 PE/kg) IV over 10 min (or IM); or phenytoin 25 mg/kg over 20 minutes For child < 1 mo, skip this step and use phenobarbital, 20 mg/kg IV over 10 minutes
4. Refractory SE (fails to respond to fosphenytoin infusion) Children < 2 years: IV phenobarbital (20 mg/kg IV over 10 min) Children > 2 years: IV valproate (20 mg/kg IV over 4 min)
Andrea Marmor, MD UCSF High Risk Emergency Medicine May, 2014
6
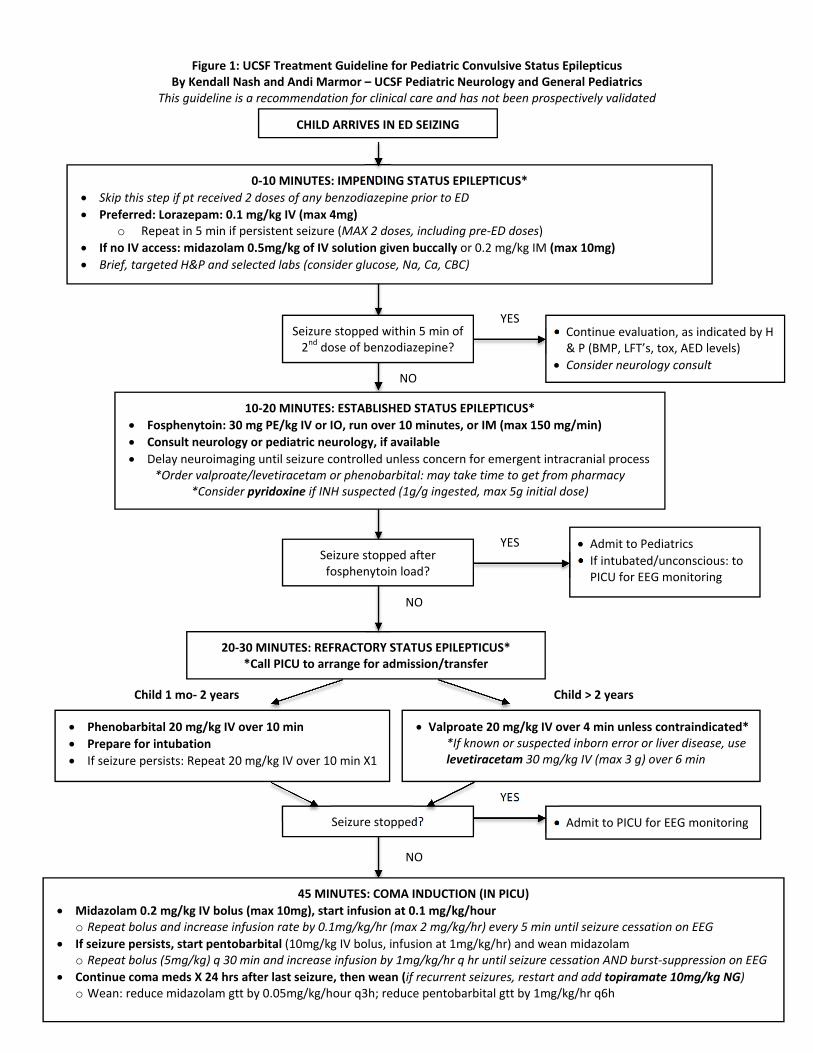
Figure 1: UCSF Treatment Guideline for Pediatric Convulsive Status Epilepticus By Kendall Nash and Andi Marmor – UCSF Pediatric Neurology and General Pediatrics
This guideline is a recommendation for clinical care and has not been prospectively validated
YES
0‐10 MINUTES: IMPENDING STATUS EPILEPTICUS*
Skip this step if pt received 2 doses of any benzodiazepine prior to ED
Preferred: Lorazepam: 0.1 mg/kg IV (max 4mg) o Repeat in 5 min if persistent seizure (MAX 2 doses, including pre‐ED doses)
If no IV access: midazolam 0.5mg/kg of IV solution given buccally or 0.2 mg/kg IM (max 10mg)
Brief, targeted H&P and selected labs (consider glucose, Na, Ca, CBC)
10‐20 MINUTES: ESTABLISHED STATUS EPILEPTICUS*
Fosphenytoin: 30 mg PE/kg IV or IO, run over 10 minutes, or IM (max 150 mg/min)
Consult neurology or pediatric neurology, if available
Delay neuroimaging until seizure controlled unless concern for emergent intracranial process *Order valproate/levetiracetam or phenobarbital: may take time to get from pharmacy
*Consider pyridoxine if INH suspected (1g/g ingested, max 5g initial dose)
Continue evaluation, as indicated by H & P (BMP, LFT’s, tox, AED levels)
Consider neurology consult
Admit to Pediatrics
If intubated/unconscious: to PICU for EEG monitoring
YES
NO
NO
YES
20‐30 MINUTES: REFRACTORY STATUS EPILEPTICUS**Call PICU to arrange for admission/transfer
45 MINUTES: COMA INDUCTION (IN PICU)
Midazolam 0.2 mg/kg IV bolus (max 10mg), start infusion at 0.1 mg/kg/hour o Repeat bolus and increase infusion rate by 0.1mg/kg/hr (max 2 mg/kg/hr) every 5 min until seizure cessation on EEG
If seizure persists, start pentobarbital (10mg/kg IV bolus, infusion at 1mg/kg/hr) and wean midazolam o Repeat bolus (5mg/kg) q 30 min and increase infusion by 1mg/kg/hr q hr until seizure cessation AND burst‐suppression on EEG
Continue coma meds X 24 hrs after last seizure, then wean (if recurrent seizures, restart and add topiramate 10mg/kg NG) o Wean: reduce midazolam gtt by 0.05mg/kg/hour q3h; reduce pentobarbital gtt by 1mg/kg/hr q6h
Child > 2 years
NO
Admit to PICU for EEG monitoring
CHILD ARRIVES IN ED SEIZING
Child 1 mo‐ 2 years
Seizure stopped?
Valproate 20 mg/kg IV over 4 min unless contraindicated* *If known or suspected inborn error or liver disease, use levetiracetam 30 mg/kg IV (max 3 g) over 6 min
Phenobarbital 20 mg/kg IV over 10 min
Prepare for intubation
If seizure persists: Repeat 20 mg/kg IV over 10 min X1
Seizure stopped after fosphenytoin load?
Seizure stopped within 5 min of 2nd dose of benzodiazepine?
Andrea Marmor, MD UCSF High Risk Emergency Medicine May, 2014
7
▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪ REFERENCES
▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪▪ 1. Abend NS, et al. Medical treatment of pediatric status epilepticus. Semin Pediatr Neur 2010; 17: 169‐175 2. American Academy of Pediatrics, Subcommittee on Febrile Seizures Clinical Practice Guideline – Febrile Seizures:
Guideline for the Neurodiagnostic Evaluation of the Child With a Simple Febrile Seizure. Pediatrics 2011; 127:389 – 394
3. Appleton R, et al. Drug management for acute tonic‐clonic convulsions including convulsive status epilepticus in children. Cochrane Database Syst Rev 2008; 16(3): CD001905
4. Arditi M, Mason EO, Bradley JS, et al. Three‐year multi‐center surveillance of pneumococcal meningitis in children: clinical characteristics and outcome related to penicillin susceptibility and dexamethasone use. Pediatrics 1998; 102: 1987‐97
5. Batra P, Gupta S, Gomber S, Saha A. Predictors of meningitis in children presenting with first febrile seizures. Pediatr Neurol 2011; 44: 35 – 39.
6. Boyle DA, Sturm JJ. Clinical factors associated with invasive testing and imaging in patients with complex febrile seizures. Pediatr Emerg Care 2013; 29(4): 430‐4
7. Chaudhuri A. Adjunctive dexamethasone treatment in acute bacterial meningitis. The Lancet Neurology Jan 2004; 3(1): 54‐62
8. Chen C‐Y, et al. New‐onset seizures in pediatric emergency. Pediatr Neonatal 2010; 51(2): 103‐111 9. Fletcher EM, Sharieff G. Necessity of lumbar puncture in patients presenting with new onset complex febrile
seizures. West J Emerg Med 2013; 14 (3): 206‐11 10. Freedman SB, Powell EC. Pediatric seizures and their management in the emergency department. Clin Ped Emerg
Med Sept 2003; 4(3): 195‐206 11. Freeman JM. Less testing is needed in the emergency room after a first afebrile seizure (letter). Pediatrics Jan 2003;
111(1): 194‐196 12. Gaillard WD, et al. Guidelines for imaging infants and children with recent‐onset epilepsy. Epilepsia 2009; 50(9):
2147‐2153 13. Green SM, Rothrock SG, Clem KJ. Can seizures be the sole manifestation of meningitis in febrile children? Pediatrics
1993;92:527‐34 14. Haeusler GM, et al. Question 1. Do febrile convulsions cause CSF pleocytosis? Arch Dis Child 2012; 97(2): 172‐5 15. Hampers LC, Spina LA. Evaluation and management of pediatric febrile seizures in the emergency department.
Emerg Med Clin North Am 2011;29: 83 – 93. 16. Hirtz D, Berg A, Bettis D, Camfield C, Camfield P, Crumrine P, et al. Practice parameter: treatment of the child with a
first unprovoked seizure: report of the Quality Standards Subcommittee of the American Academy of Neurology and the Practice Committee of the Child Neurology Society. Neurology 2003;60: 166–75
17. Hom J, et al. The low rate of bacterial meningitis in children, ages 6 to 18 months, with simple febrile seizures. Acad Emerg Med 2011; 18(11): 1114‐20
18. Hsieh DT et al. New‐onset afebrile seizures in infants: role of neuroimaging. Neurology 2010; 74(2): 150‐6 19. Hubert P, et al. Management of convulsive status epilepticus in infants and children. Rev Neurol 2009; 165(4): 390‐7 20. Kimia AA, Capraro AJ, Hummel D, et al. Utility of lumbar puncture for first simple febrile seizure among children 6 to
18 months of age. Pediatrics. 2009; 123: 6 – 12. 21. Kimia A, Ben‐Joseph EP, Rudloe T, et al. Yield of lumbar puncture among children who present with their first
complex febrile seizure. Pediatrics 2010; 126: 62 – 69 22. Maytal J, et al. The role of brain computed tomography in evaluating children with new onset of seizures in the
emergency department. Epilepsia 2000;41: 950‐4 23. McIntyre PB, Berkey CS, et al. Dexamethasone as adjunctive therapy in bacterial meningitis: meta‐analysis of
randomized clinical trails since 1988. JAMA 1997; 278: 925‐31 24. McMullan J, et al. Midazolam versus diazepam for the treatment of status epilepticus in children and young adults:
as meta‐analysis. Acad Emerg Med 2010; 17(6): 575‐82 25. Millar JA. Evaluation and treatment of the child with febrile seizure. Am Fam Physician May 2006; 73(10): 1761‐4 26. Molyneux EM, Walsh AL, Forsyth H, et al. Dexamethasone treatment in childhood bacterial meningitis in Malawi: a
randomised controlled trial. Lancet 2002; 360: 211‐8 27. Nigrovic LE, et al. Children with bacterial meningitis presenting to the emergency department during the
pneumococcal conjugate vaccine era. Acad Emerg Med 2008; 15:522‐528 28. Oluwabusi T, et al. Update on the management of simple febrile seizures: emphasis on minimal intervention. Curr
Opin Pediatr 2012; 24(2): 259‐265
Andrea Marmor, MD UCSF High Risk Emergency Medicine May, 2014
8
29. Seltz LB, et al. Risk of bacterial or herpes simplex virus meningitis/encephalitis in children with complex febrile seizures. Pediatr Emerg Care 2008; 25(8): 494‐497
30. Shah SS, Alpern ER, Zwerling L, Reid JR, McGowan KL, Bell LM. Low risk of bacteremia in children with febrile seizures. Arch Pediatr Adolesc Med 2002; 156: 469–72
31. Sharma S, et al. The role of emergent neuroimaging in children with new‐onset afebrile seizures. Pediarics 2003; 111: 1‐5
32. Silbergleit R, et al. Intramuscular versus intravenous therapy for prehospital status epilepticus. NEJM 2012; 366: 591‐600
33. Sofou K, et al. Management of prolonged seizures and status epilepticus in childhood: a systematic review. J Child Neurol 2009; 24(8): 918‐26
34. Straussberg R. Pro‐ and anti‐inflammatory cytokines in children with febrile convulsions. Pediatr Neurol Jan 2001; 24(1): 49‐53
35. Strengell T, Uhari M, Tarkka R, et al. Antipyretic agents for preventing recurrences of febrile seizures: randomized controlled trial. Arch Pediatr Adolesc Med 2009;163: 799 – 804.
36. Thigpen MC, et al. Bacterial meningitis in the United States, 1998–2007. N Engl J Med 2011; 364:2016–2025. 37. Trainor JL, et al. Children with first‐time simple febrile seizures are at low risk of serious bacterial illness. Acad
Emerg Med 2001; 8:781‐7 38. Van de Beek D, deGans J, McIntyre P, Prasad K. Corticosteroids for acute bacterial meningitis. Cochrane Database
Review Jan 2007 (1): CD004405 39. Warden CR, Zibulewsky J, Mace S, Gold C, Gausche‐Hill M. Evaluation and management of febrile seizures in the out‐
of‐hospital and emergency department settings. Ann Emerg Med 2003;41: 215–22.