Embed Size (px)
Citation preview
8/8/2019 Massimini PBR Coma Science 2009
http://slidepdf.com/reader/full/massimini-pbr-coma-science-2009 1/14
S. Laureys et al. (Eds.)Progress in Brain Research , Vol. 177ISSN 0079-6123Copyright r 2009 Elsevier B.V. All rights reserved
CHAPTER 14
A perturbational approach for evaluating the brain’scapacity for consciousness
Marcello Massimini 1, � , Melanie Boly 2 , Adenauer Casali 1 , Mario Rosanova 1 andGiulio Tononi 3
1Department of Clinical Sciences, University of Milan, Milan, Italy2Coma Science Group, Cyclotron Research Center and Neurology Department, University of Liege and
CHU Hospital, Belgium3Department of Psychiatry, University of Wisconsin, WI, USA
Abstract: How do we evaluate a brain’s capacity to sustain conscious experience if the subject does notmanifest purposeful behaviour and does not respond to questions and commands? What should wemeasure in this case? An emerging idea in theoretical neuroscience is that what really matters forconsciousness in the brain is not activity levels, access to sensory inputs or neural synchronization per se,but rather the ability of different areas of the thalamocortical system to interact causally with each otherto form an integrated whole. In particular, the information integration theory of consciousness (IITC)argues that consciousness is integrated information and that the brain should be able to generate
consciousness to the extent that it has a large repertoire of available states ( information ), yet it cannot bedecomposed into a collection of causally independent subsystems ( integration ). To evaluate the ability tointegrate information among distributed cortical regions, it may not be sufcient to observe the brain inaction. Instead, it is useful to employ a perturbational approach and examine to what extent differentregions of the thalamocortical system can interact causally ( integration ) and produce specic responses(information ). Thanks to a recently developed technique, transcranial magnetic stimulation and high-density electroencephalography (TMS/hd-EEG), one can record the immediate reaction of the entirethalamocortical system to controlled perturbations of different cortical areas. In this chapter, using sleepas a model of unconsciousness, we show that TMS/hd-EEG can detect clear-cut changes in the ability of the thalamocortical system to integrate information when the level of consciousness uctuates across thesleep–wake cycle. Based on these results, we discuss the potential applications of this novel technique toevaluate objectively the brain’s capacity for consciousness at the bedside of brain-injured patients.
Keywords: coma; consciousness; transcranial magnetic stimulation; electroencephalography; information;integration
Evaluating a subject’s level of consciousness
The bedside evaluation of patients affected by�Corresponding author.disorders of consciousness (DOC) relies onTel.: +39 33 39 92 57 91; Fax: +39 02 48002084;
E-mail: [email protected] repeated behavioural observation by trained
DOI: 10.1016/S0079-6123(09)17714-2 201

8/8/2019 Massimini PBR Coma Science 2009
http://slidepdf.com/reader/full/massimini-pbr-coma-science-2009 2/14
202
personnel. During the examination, spontaneousand elicited behaviour in response to multisensorystimulation is recorded in accordance with specicscales ( Giacino et al., 2004 ; Gill-Thwaites and Munday, 2004 ; Kalmar and Giacino, 2005 ; Shiel et al., 2000 ). Regardless of the scale employed,the examiner typically looks for (1) evidence of awareness of the self or of the environment, (2)evidence of sustained, reproducible, purposeful orvoluntary response to tactile, auditory or noxiousstimuli and (3) evidence of language comprehension and expression ( Laureys et al., 2004 ). If noneof these three dening behavioural features canbe detected during careful and repeated evaluations, the subject is considered unconscious
(Royal College of Physicians, 1994 ), whilepatients who show non-reexive behaviour butare unable to communicate their thoughts andfeelings are ascribed to a recently dened clinicalentity, the minimally conscious state ( Giacino et al., 2002 ). Thus, according to the clinicaldenition of consciousness, subjects are consciousif they can signal that this is the case. However,since in patients with severe brain injury motorresponsiveness is often impaired, it may alsohappen that a subject is aware but unable to
move or speak ( Schnakers et al., 2009 ). Therefore,while detecting the presence of voluntary behaviour at the bedside is sufcient to infer that asubject is aware, its absence does not necessarilyimply unconsciousness ( Boly et al., 2007 ; Laureys et al., 2004 ; Monti et al., 2009 ).
Recently, the development of new neuroimaging protocols has made it possible to probe forsigns of awareness even when subjects arecompletely unable to move ( Boly et al., 2007 ;Owen and Coleman, 2008 ). For example, in arecent study ( Owen and Coleman, 2008 ), aclinically vegetative, seemingly unresponsivepatient was put in the scanner and asked toimagine playing tennis or navigating through herown apartment. Remarkably, the patient showedfMRI patterns of brain activation that wereconsistent and specic for the requested cognitivetask, just like healthy subjects. This paradigmaticcase demonstrates that the patient’s ability towilfully enter specic neural states upon requestcan be used to detect the presence of awareness
even when motor outputs are absent. However,there still may be cases, such as in aphasia,akinetic mutism, catatonic depression or diffusedopaminergic lesions, where a patient, althoughaware, may not be able to understand or bewilling to respond ( Boly et al., 2007 ). Moreover,because of frequent movement artefacts andbecause of possible alterations of the normalcoupling of hemodynamics and neuronal ring(Rossini et al., 2004 ), acquiring and interpretingfMRI data is especially difcult in DOC patients(Giacino et al., 2006 ). Hence, the absence of volitional brain activity in the scanner, just like theabsence of purposeful movements during aclinical examination, does not necessarily imply
the absence of awareness.The behavioural approach and the neuroima
ging paradigm represent two different levels atwhich a communication can be established with aDOC patient ( Owen et al., 2005 ). If an overtbehaviour fails to signal consciousness, it is stillpossible to dig deeper by looking for purposefulneural activations. Both methods leave no doubtsin case of a positive result: if the subjects respond,they are actually aware. Instead, a negative resultleaves an open question.
Evaluating a brain’s capacity for consciousness
In this chapter, we propose an additional level atwhich consciousness can be studied even when nocommunication whatsoever (behavioural orneural) can be established with the subject. Thisparadigm does not aim at probing the subject inorder to elicit wilfull behaviours or neural activations; rather, it involves probing directly thesubject’s brain to gauge core properties that aretheoretically relevant for consciousness. Thisoption requires (1) starting from a theory thatsuggests which properties are fundamental for aphysical system to give rise to conscious experience and (2) identifying and implementing apractical measuring method to weigh up theseproperties in a real brain. Here, we start with theinformation integration theory of consciousness (IITC) ( Tononi, 2004, 2005, 2008 ), a theorythat argues that consciousness is integrated

8/8/2019 Massimini PBR Coma Science 2009
http://slidepdf.com/reader/full/massimini-pbr-coma-science-2009 3/14
203
information and that a physical system should beable to generate consciousness to the extent that itcan enter any of a large number of available states(information ), yet it cannot be decomposed into acollection of causally independent subsystems(integration ). Then, we devise a practical methodto gauge the brain’s capacity to integrate information. To do this we employ a combination of transcranial magnetic stimulation and electroencephalography (TMS/hd-EEG), a technique thatallows stimulating directly different subsets of cortical neurons and recording the immediatereaction of the rest of the brain. Based onmeasurements performed in sleeping subjects(Massimini et al., 2005, 2007 ), we argue that this
method represents an effective way to appreciate,at a general level, to what extent different regionsof the thalamocortical system can interact globally(integration ) to produce specic responses ( infor-mation ). Thus, instead of asking the subjects towilfully perform different motor or cognitivetasks, we directly ‘‘ask’’ (with TMS) their thalamocortical system to enter different neural statesand we assess (with hd-EEG) to what extent thesestates are integrated and specic. While thisapproach is not meant to tell whether a subject
is actually conscious or not, it may represent aprincipled way to objectively weigh a brain’scapacity for conscious experience.
Theoretical guidelines: the integrated informationtheory of consciousness
The IITC takes its start from phenomenology and,by making a critical use of thought experiments,argues that subjective experience is integratedinformation. Therefore, according to the IITC,any physical system will have subjective experience to the extent that it is capable of integratinginformation. In this view, experience, i.e. information integration, is a fundamental quantity that is,in principle, measurable, just as mass or energy is.Information and integration are, on the otherhand, the very essence of subjective experience.Classically, information is the reduction of uncertainty among alternatives: when a coin falls onone of its two sides, it provides 1 bit of
information, whereas a die falling on one of sixfaces provides B 2.6 bits. But then having anyconscious experience, even one of pure darkness,must be extraordinarily informative, because itrules out countless other experiences instead(think of all the frames of every possible movie).In other words, having any experience is likethrowing a die with a trillion faces and identifyingwhich number came up. On the other hand, everyexperience is an integrated whole that cannot besubdivided into independent components. Forexample, with an intact brain you cannot experience the left half of the visual eld independentlyof the right half, or visual shapes independently of their colour. In other words, the die of experience
is a single one; throwing multiple dice andcombining the numbers will not help.
If the capacity for consciousness corresponds tothe capacity to integrate information, then aphysical system should be able to generateconsciousness to the extent that it can discriminateamong a large number of available states ( infor-mation ), yet it cannot be decomposed into acollection of causally independent subsystems(integration ). How can one identify such anintegrated system, and how can one measure its
repertoire of available states? To measure therepertoire of different states that are available to asystem, one can use the entropy function, but thisway of measuring information is completelyinsensitive to whether the information is integrated. Thus, measuring entropy would not allowus to distinguish between one million photodiodeswith a repertoire of two states each, and a singleintegrated system with a repertoire of 2 1,000,000
states. To measure information integration, it isessential to know whether a set of elementsconstitutes a causally integrated system, or theycan be broken down into a number of independent or quasi-independent subsets among whichno information can be integrated.
Indeed, the theory claims that the level of consciousness of a physical system is related to therepertoire of different states ( information ) thatcan be discriminated by the system as a whole(integration ). Thus, a measure of integratedinformation, called phi ( F ), has been proposedin order to quantify the information generated

8/8/2019 Massimini PBR Coma Science 2009
http://slidepdf.com/reader/full/massimini-pbr-coma-science-2009 4/14
204
when a system discriminates one particular stateof its repertoire, above and beyond the information generated independently by its parts(Balduzzi and Tononi, 2008 ; Tononi, 2004 ).
As demonstrated through computer simulations, information integration is optimized ( F ishighest) if the elements of a complex areconnected in such a way that they are bothfunctionally specialized (connection patterns aredifferent for different elements) and functionallyintegrated (all elements can be reached from allother elements of the network). If functionalspecialization is lost by replacing the heterogeneous connectivity with a homogeneous one, or if functional integration is lost by rearranging the
connections to form small modules, the value of Fdecreases considerably ( Tononi and Sporns, 2003).
According to the IITC, this is exactly why,among many structures of the brain, the thalamocortical system is so special for consciousness: it isnaturally organized in a way that appears toemphasize at once both functional specializationand functional integration. Thus, it comprises alarge number of elements that are functionallyspecialized, becoming activated in different cir
cumstances ( Bartels and Zeki, 2005 ). This is trueat multiple spatial scales, from different corticalsystems dealing with vision, audition, etc., todifferent cortical areas dealing with shape, colour,motion, etc., to different groups of neuronsresponding to different directions of motion. Onthe other hand, the specialized elements of thethalamocortical system are integrated through anextended network of intra- and inter-areal connections that permit rapid and effective interactions within and between areas ( Engel et al., 2001).
But then, the theory also explicitly predicts thatthe fading of consciousness should be associatedwith either a reduction of integration withinthalamocortical circuits (e.g. they could breakdown into causally independent modules) or areduction in information (the repertoire of available states might shrink), or both. This specicprediction is however difcult to test in humans,since, in practice, F can only be measuredrigorously for small, simulated systems. In the
next section, we try to identify an empiricalmethod to approximate a measure of the capacityfor integrated information in a human brain.
Employing TMS/hd-EEG to evaluatethalamocortical integration and informationcapacity
Different methods have been proposed in order toinfer on a subject’s level of consciousness solelybased on brain activity. Some of these methods,such as spectral analysis ( Berthomier et al., 2007 )and the proprietary ‘‘bispectral index’’ ( Myles et al., 2004 ), seem to correlate empirically with
consciousness but have no clear theoreticalfoundation. Other measures, such as neuralcomplexity ( Tononi et al., 1994 ) and causaldensity ( Seth, 2005 ), are theoretically motivated(Seth et al., 2008 ) but have not yet been testedempirically. More or less explicitly, all thesemeasures attempt to capture the coexistence of functional integration and functional differentiation in spontaneous (mainly hd-EEG) brainsignals. Yet, to dependably appreciate the brain’scapacity for consciousness (dened as integrated
information), one should go beyond spontaneousactivity levels or patterns of temporal correlationamong distant neuronal groups (functional connectivity). First, this is because the repertoire of available states is, by denition, potential and,thus, not necessarily observable. Second, becauseit is difcult to say whether a system is actuallyintegrated or not by just observing the spontaneous activity it generates. For example, observing time-varying, complex correlations amongretinal neurons that are responding to a rich visualscene may lead one to the conclusion that theretina is both functionally specialized and functionally integrated. However, such complex spa-tial-temporal correlations do not imply that theretina per se has a capacity for consciousness. Infact, it is enough to perturb a few retinal elementsand to record from the rest of the cells to realizethat, to a large extent, the retina is actuallycomposed of segregated modules that do notinteract with each other. Indeed, the ability tointegrate information can only be demonstrated
8/8/2019 Massimini PBR Coma Science 2009
http://slidepdf.com/reader/full/massimini-pbr-coma-science-2009 5/14
205
from a causal perspective; one must employ aperturbational approach (effective connectivity)and examine to what extent subsets of neuronscan interact causally as a whole ( integration ) toproduce responses that are specic for thatparticular perturbation ( information ). Moreover,one should probe causal interactions by directlystimulating the cerebral cortex to avoid possiblesubcortical ltering or gating. Finally, since causalinteractions among thalamocortical neuronsdevelop on a sub-second time scale (just asphenomenal consciousness does), it is very important to record the neural effects of the perturbation with the appropriate temporal resolution.
Thus, in practice, one should nd a way to
stimulate different subsets of cortical neurons andmeasure, with good spatial-temporal resolution,the effects produced by these perturbations in therest of the thalamocortical system. Today, thismeasurement can be performed non-invasively in
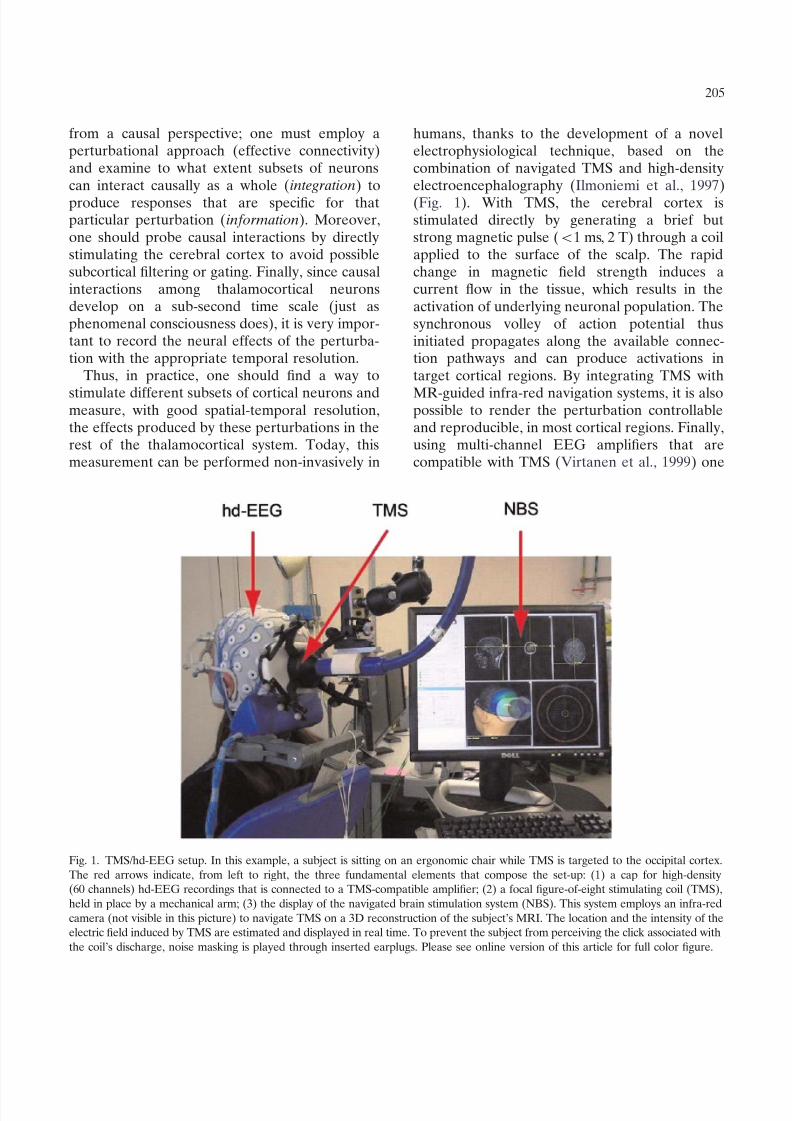
humans, thanks to the development of a novelelectrophysiological technique, based on thecombination of navigated TMS and high-densityelectroencephalography ( Ilmoniemi et al., 1997 )(Fig. 1). With TMS, the cerebral cortex isstimulated directly by generating a brief butstrong magnetic pulse ( o 1 ms, 2 T) through a coilapplied to the surface of the scalp. The rapidchange in magnetic eld strength induces acurrent ow in the tissue, which results in theactivation of underlying neuronal population. Thesynchronous volley of action potential thusinitiated propagates along the available connection pathways and can produce activations intarget cortical regions. By integrating TMS with
MR-guided infra-red navigation systems, it is alsopossible to render the perturbation controllableand reproducible, in most cortical regions. Finally,using multi-channel EEG ampliers that arecompatible with TMS ( Virtanen et al., 1999 ) one
Fig. 1. TMS/hd-EEG setup. In this example, a subject is sitting on an ergonomic chair while TMS is targeted to the occipital cortex.The red arrows indicate, from left to right, the three fundamental elements that compose the set-up: (1) a cap for high-density(60 channels) hd-EEG recordings that is connected to a TMS-compatible amplier; (2) a focal gure-of-eight stimulating coil (TMS),held in place by a mechanical arm; (3) the display of the navigated brain stimulation system (NBS). This system employs an infra-redcamera (not visible in this picture) to navigate TMS on a 3D reconstruction of the subject’s MRI. The location and the intensity of theelectric eld induced by TMS are estimated and displayed in real time. To prevent the subject from perceiving the click associated withthe coil’s discharge, noise masking is played through inserted earplugs. Please see online version of this article for full color gure.

8/8/2019 Massimini PBR Coma Science 2009
http://slidepdf.com/reader/full/massimini-pbr-coma-science-2009 6/14
206
can record, starting just a few milliseconds afterthe pulse, the impact of the perturbation on thestimulated target and in distant cortical areas.Indeed, the integrated use of neuro-navigationsystems, TMS and multichannel TMS-compatiblehd-EEG ampliers together constitute a newbrain scanning method in which stimulation isnavigated into any desired brain target and theconcurrently recorded scalp potentials are processed into source images of the TMS-evokedneuronal activation ( Komssi and Kahkonen, 2006).
It is worth highlighting some of the specicadvantages that TMS/hd-EEG may offer as a toolto probe the brain of DOC patients:
1. TMS-evoked activations are intrinsicallycausal ( Paus, 2005 ). Thus, unlike methodsbased on temporal correlations, TMS/hd-EEG immediately captures the fundamentalmechanism that underlies integration, i.e. theability of different elements of a system toaffect each other.
2. TMS/hd-EEG bypasses sensory pathwaysand subcortical structures to probe directlythe thalamocortical system. Therefore,
unlike peripherally evoked potentials andevoked motor activations, TMS/hd-EEGdoes not depend on the integrity of sensoryand motor systems and can access anypatient (deafferentated or paralysed). Moreover, with TMS one can stimulate mostcortical areas (including associative cortices)employing several different parameters(intensity, angle, current direction), thusprobing a vast repertoire of possibleresponses, above and beyond observableongoing brain states.
3. TMS-evoked potentials can be recorded withmillisecond resolution, a time scale that isadequate to capture effective synaptic interactions among neurons.
4. TMS/hd-EEG does not require the subjectto be involved in a task and the observedactivations are not affected either by thewillingness of the patient to participate or byhis effort and performance. Hence, thisapproach is well suited to assess the objective
capacity of thalamocortical circuits independently on behaviour.
5. TMS/hd-EEG can be made portable in orderto overcome the logistical and economichurdles that may separate severely brain-injured patients from advanced imagingfacilities.
Thus, at least in principle, TMS/hd-EEG mayrepresent an appropriate tool to approximate atheoretical measure of consciousness at thepatient’s bedside. However, the question whetherthis technique may actually detect changes in thebrain’s capacity to integrate information can onlybe answered experimentally. For example, one
should demonstrate that TMS-evoked activationsare widespread ( integration ) and specic ( infor-mation ) in a conscious brain but that they becomeeither local (revealing a loss of integration) orstereotypical (revealing a loss of information)when the same brain becomes unconscious. In thenext section, we describe the results of experiments where TMS/hd-EEG was used to understand what changes in human thalamocorticalcircuits when consciousness fades upon fallingasleep.
TMS/hd-EEG detects changes in the brain’scapacity for integrated information during sleep
Sleep is the only time when healthy humansregularly lose consciousness. Subjects awakenedduring slow-wave sleep early in the night mayreport short, thought-like fragments of experience, or often nothing at all ( Hobson et al., 2000 ).Sleep also exposes several interesting paradoxesabout the relationships between consciousnessand the brain. For instance, it was thought that thefading of consciousness during sleep was due tothe brain shutting down. However, while metabolic rates decrease in some cortical areas,thalamocortical neurons remain active duringslow-wave sleep also, with mean ring ratescomparable to those of quiet wakefulness(Steriade et al., 2001 ). It was also hypothesizedthat sensory inputs are blocked during sleep andthat they are necessary to sustain conscious

8/8/2019 Massimini PBR Coma Science 2009
http://slidepdf.com/reader/full/massimini-pbr-coma-science-2009 7/14
207
experience. However, we now know that, evenduring deep sleep, sensory signals continue toreach the cerebral cortex ( Kakigi et al., 2003 )where they are processed subconsciously ( Portas et al., 2000 ). Gamma activity and synchrony havebeen viewed as possible correlates of consciousness and they were found to be low in slow-wavesleep ( Cantero et al., 2004 ). However, they maybe equally low in REM sleep, when subjectiveexperience is usually vivid, and they can be high inanaesthesia ( Vanderwolf, 2000 ). On the otherhand, intracranial recordings show that gammaactivity ( Destexhe et al., 2007 ) and gamma-coherence ( Bullock et al., 1995 ) persist duringslow-wave sleep. Interestingly, similar paradoxes,
where neural activity levels, access to sensoryinformation and the degree of neural synchronydo not correlate with the level of consciousness,can be found in other conditions such asanaesthesia, epilepsy and DOC patients ( Tononi and Laureys, 2008 ). In this sense, sleep representsa general model to learn what really matters forconsciousness.
For this reason, in a series of recent experiments, we have employed TMS/hd-EEG tomeasure what changes in thalamocortical circuits
during the transition from wakefulness intodifferent stages of sleep ( Massimini et al., 2005, 2007). Figure 2A shows the response obtainedafter stimulation of rostral premotor cortex in onesubject during wakefulness. The black tracesrepresent the voltage recorded from all scalpelectrodes; the cortical currents associated withthe main peaks of activity are depicted below. Thecircles on the cortical surface indicate the site of stimulation, while the cross highlights the locationof maximal cortical activation. TMS, applied at anintensity corresponding to motor threshold, triggers, during wakefulness, a series of low-amplitude, high-frequency (25–30 Hz) waves of activityassociated with cortical activations that propagatealong long-range ipsilateral and transcallosalconnections. Remarkably, the exactly same stimulation, applied 15 min later, during sleepstages 3 and 4, results in a very different picture(Fig. 2B). In this case, TMS triggers a larger, low-frequency wave, associated with a strong initialcortical activation that does not propagate to
connected brain regions and dissipates rapidly.This nding is general and can be reproducedafter the stimulation of different cortical areas, aslong as the subjects are in slow-wave sleep stages3 and 4. Thus, the cortical area that is directlyengaged by TMS preserves its reactivity butbehaves as an isolated module; in this way,TMS/hd-EEG reveals a clear-cut reduction of cortico-cortical integration occurring during sleepearly in the night. Interestingly, during REM sleeplate in the night, when dreams become long andvivid and the level of consciousness returns tolevels close to wakefulness (despite the subjectbeing almost paralysed), thalamocortical integration partially recovers and TMS triggers a more
widespread and differentiated pattern of activation ( Fig. 2C).
TMS/hd-EEG measurements not only indicatethat during slow-wave sleep the thalamocorticalsystem tends to break down into isolated modules(loss of integration), but also show that the abilityof thalamocortical circuits to produce differentiated responses (information) is impaired. InFig. 3, the responses to two different TMSperturbations (one applied to premotor cortexand the other one applied to visual cortex) are
compared during wakefulness and slow-wavesleep. For each condition, the signicant currentsevoked by TMS are cumulated over the entirepost-stimulus interval and are plotted on thecortical surface; on the right side of each corticalsurface, the time course of the currents recordedfrom three selected areas are depicted. Thisexample, as the one reported in the previousgure, conrms a clear-cut loss of integrationduring slow-wave sleep by showing that distantcortical areas cease to be causally affected by theinitial perturbation. On the other hand, it alsoreveals a clear loss of response specicity. Thus,while during wakefulness the premotor and thevisual cortex react to the stimulus with a patternof activation which has a characteristic shape andfrequency content ( Rosanova et al., 2009 ), thisdistinction is clearly obliterated during sleep; thelocal response to TMS becomes, in both cases, asimple positive–negative wave.
Indeed, if the reactivity of the sleeping brain issystematically tested by applying TMS at different

8/8/2019 Massimini PBR Coma Science 2009
http://slidepdf.com/reader/full/massimini-pbr-coma-science-2009 8/14
Fig. 2. Cortical responses to TMS across the sleep–wake cycle. hd-EEG voltages and current densities are shown from arepresentative subject in whom the premotor cortex was stimulated with transcranial magnetic stimulation (TMS) (black arrow). (A)During waking, stimulation evokes hd-EEG responses rst near the stimulation site (circle; the cross is the site of maximum evokedcurrent) and then, in sequence, at other cortical locations, producing a long-range pattern of activation. (B) During slow-wave sleep,the stimulus-evoked response remains local, indicating a loss of cortical integration. At the same time, the response recorded fromthe electrode located under the stimulator (thick red trace) becomes a positive wave followed by a negative rebound. (C) DuringREM sleep, effective connectivity among distant cortical areas recovers, indicating a signicant resurgence of cortical integration(adapted with permission from Massimini et al., 2007 ). Please see online version of this article for full color gure.

8/8/2019 Massimini PBR Coma Science 2009
http://slidepdf.com/reader/full/massimini-pbr-coma-science-2009 9/14
209
Fig. 3. Loss of cortical integration and differentiation during slow-wave sleep. TMS is applied to premotor cortex (A) and to visualcortex (B) during wakefulness (left panels) and during slow-wave sleep (right panels). After source modelling, non-parametricstatistics is performed to detect the signicant currents induced by TMS. For each condition, the signicant currents recorded duringthe entire post-stimulus interval are plotted on the cortical surface; on the right side of each cortical surface, the time series of thecurrents recorded from three selected areas (Brodmann areas (BA) 8, 6 and 19) are depicted (the time of stimulation is marked by ared line). With the transition from wakefulness to slow-wave sleep, distant cortical areas cease to be causally affected by the initialperturbation, indicating a break-down of cortical integration. At the same time, cortical responses to TMS become stereotypical,indicating a loss of cortical differentiation. Please see online version of this article for full color gure.
intensities and in different cortical areas ( Massimini et al., 2007 ), one invariably obtains astereotypical response: a positive wave followedby a negative rebound ( Fig. 3). Interestingly, thispositive–negative component develops towards afull-edged sleep slow wave when TMS isdelivered at increasing intensities in a scalp regionaround the vertex ( Massimini et al., 2007 ). Theprominent negative component of TMS-evokedslow waves is very likely to be associated with awidespread hyperpolarization in a large population of cortical neurons, as is the case forspontaneous sleep slow waves ( Cash et al., 2009 ;Massimini et al., 2004 ). Thus, it appears that theonly way the sleeping brain can react to a directcortical perturbation is by producing a slow wave
that is either local ( Fig. 2B) or global and nonspecic ( Fig. 4B).
What prevents the emergence of a differentiated long-range pattern of activation duringsleep? It is likely that the mechanism underlyingthe impaired capacity of the sleeping brain forintegrated information is the same mechanism thatunderlies the occurrence of spontaneous sleepslow-waves, that is bistability in thalamocorticalcircuits ( Tononi and Massimini, 2008 ). Uponfalling asleep, brainstem activating systems reducetheir ring rates, thus increasing the inuence of depolarization-dependent potassium currents inthalamic and cortical neurons ( McCormick et al., 1993). Due to these currents, cortical neuronsbecome bistable and inevitably tend to fall into a

8/8/2019 Massimini PBR Coma Science 2009
http://slidepdf.com/reader/full/massimini-pbr-coma-science-2009 10/14
210
Fig. 4. The sleeping brain reacts to TMS by producing stereotypical responses that resemble spontaneous sleep slow-waves. (A)TMS is delivered at four midline sites along the posterior–anterior axis of the cortex (posterior parietal, sensorimotor, supplementarymotor, rostral premotor). The brain response to TMS is probed, at each site, at two intensities (MO is maximum stimulator output).The average responses to 15 TMS trials recorded from all channels (referenced to the mastoid) are shown for each intensity and eachcortical site. At all cortical sites, TMS evokes a positive component followed by a negative rebound that develops towards a full-edged sleep slow-wave when stimulation is delivered at increasing intensities in a scalp region closer to the sensory-motor cortex.(B) In this region, TMS triggers a large negative deection associated with long-lasting currents that spread like an oil-spot to thesurrounding cortex, starting from a xed local maximum. In this particular case, the brain’s reaction to TMS becomes global butremains stereotypical and non-specic (adapted with permission from Massimini et al., 2007 ).
silent, hyperpolarized state (down-state) after a occurring spontaneously or induced by a stimulusperiod of activation (up-state). This bistability (like TMS), eventually triggers a stereotypicalprovides the mechanism for the slow oscillations of down-state that, in turn, prevents the emergencesleep where large populations of cortical neurons of specic, long-range patterns of activation.spontaneously alternate between up- and down- Altogether, TMS/hd-EEG measurements sugstates ( Hill and Tononi, 2005 ). At the same time, gest that, during slow-wave sleep, the thalamodue to bistability, any local activation, whether cortical system, despite being active and reactive,

8/8/2019 Massimini PBR Coma Science 2009
http://slidepdf.com/reader/full/massimini-pbr-coma-science-2009 11/14
211
either breaks down in causally independentmodules (producing a local down-state) or burstsinto an explosive and non-specic response(producing a global down-state and a full-edgedhd-EEG slow-wave). In no case, during slow-wave sleep, does TMS result in a balanced, long-range, differentiated pattern of activation. TheTMS/hd-EEG perturbational approach also suggests that intrinsic bistability in thalamocorticalnetworks, the key mechanism responsible for theoccurrence of the spontaneous slow oscillationsof sleep, may be the reason why informationintegration is impaired in early NREM sleep(Massimini et al., 2009 ). While sleep and theassociated bistability are physiological and rever
sible processes, pathological processes may similarly result in a modication of the brain’s abilityto integrate information and this modication maybe similarly detected by TMS/hd-EEG. In thenext section, we discuss the possible applicationsof TMS/hd-EEG at the bedside of DOC patients.
TMS/EEG in DOC patients: some predictions
Given the variety of brain lesions and conditions
that are associated to DOC ( Laureys et al., 2004, 2009), it is very difcult to predict what kind of results TMS/hd-EEG might give in individualDOC patients. However, an informed guess canbe adopted at least in some specic cases. Forinstance, it is conceivable that TMS-evokedactivations similar to the ones described duringslow-wave sleep may also be found in patients thatare in a coma caused by a lesion in the ascendingreticular activating system. In these cases, onecould predict that, due to bistability, TMS shouldtrigger a stereotypically local, or global, slowwave, provided that thalamocortical circuits arefundamentally intact. Similarly, due to pathological bistability in cortical circuits ( Hahn and Durand, 2001 ), large and stereotypical responseswould be expected in patients that are in a statusepilepticus. On the other hand, TMS shouldresults in mostly local responses in cases whereconnectivity is generally impaired, such as inpatients with diffuse axonal injury ( Graham et al., 2005). What would happen, instead, when a coma
patient opens her/his eyes, shows only reexivebehaviour ( Schiff et al., 1999 ) and enters thevegetative state ( Laureys and Boly, 2008 )? Inprinciple, the recovery of arousal, if not paralleledby recovery of awareness, should not be associated with signicant changes in the ability of thalamocortical circuits to integrate information.In this sense, TMS-evoked activation is notexpected to show relevant changes during thetransition from coma to the vegetative state. Verydifferent is the condition of locked-in patients(Plum and Posner, 1972 ) who awaken from theircoma fully conscious ( Schnakers et al., 2008 ) butcompletely paralysed, except for the ability togaze upward; in this case, TMS should trigger
more widespread and differentiated patterns of activation, just as it does during normal wakefulness or at most upon entering REM sleep, whensubjects are conscious but almost paralysed.
The most important challenge for any objectivemeasure of consciousness is proving itself capableof detecting a potential for residual cognition whenno communication whatsoever can be establishedwith the patient. This task is difcult by denition,since there is no behavioural reference to assessthe subject’s actual level of consciousness. Never
theless, some strategies could be adopted topractically validate TMS/hd-EEG measures as adependable marker of the brain’s capacity forconsciousness. First, one should demonstrate thatusing TMS/hd-EEG it is possible to identifysignicant differences between vegetative andminimally conscious patients concerning theirbrain’s capacity for integrated information. Apositive result in such a population study wouldindicate that TMS/hd-EEG is sensitive enough toobjectify minimal changes in the brain’s capacityfor awareness. Second, one should demonstratethat the longitudinal TMS/hd-EEG measurementscan predict the individual patient’s outcome. Forinstance, it would be relevant to observe TMS-evoked cortical responses that progressivelybecome more global and specic in the brain of intensive care patients shortly before they regainconsciousness at the clinical level. Then, TMS/hd-EEG may be employed as a diagnostic/prognostic tool to evaluate covert consciousnessand to foster evidence-based neuro-rehabilitation.

8/8/2019 Massimini PBR Coma Science 2009
http://slidepdf.com/reader/full/massimini-pbr-coma-science-2009 12/14
212
Future perspectives
We attempted at identifying an objective markerof consciousness that is theoretically groundedand practically measurable. The core message of this chapter is that using by TMS/hd-EEG it ispossible to detect clear-cut changes in the capacityof human thalamocortical circuits to integrateinformation, a theoretical requirement to generate conscious experience, when the level of consciousness uctuates across the sleep–wakecycle. The implication of this nding is that TMS/hd-EEG may be similarly employed to evaluatethe brain’s capacity for consciousness at thebedside of non-communicative patients. Clearly,
before applying this technique to DOC patients,further steps need to be taken.First, TMS/hd-EEG normative data have to be
dened. Thus, several cortical areas must besystematically perturbed in healthy subjects inorder to determine the specicity and the reproducibility of cortical responses to TMS. A similarassessment has been recently performed on alimited set of cortical areas (superior occipitallobule, precuneus and premotor) and has revealedpatterns of TMS-evoked cortical activation thatare specic for the stimulated site and reproducible across subjects ( Rosanova et al., 2009 ). Thisdatabase needs to be further extended includingmore cortical areas and subjects.
Second, a standard analysis procedure mustbe developed in order to extract from TMS/hd-EEG data synthetic indices that capture thebrain’s capacity for integration and differentiation. In fact, the results presented in this chapterare suggestive, but only qualitative. Differentalgorithms can be devised in order to quantifyTMS/hd-EEG data in a way that is theoreticallyrelevant. For instance, the extent of the brain areathat is signicantly engaged by TMS ( Fig. 3)provides a simple measure of integration. Indeed,since TMS-evoked activations are intrinsicallycausal ( Paus, 2005 ), it is warranted that theelements within this area are interacting effectively with each other and that the observedpatterns of activations are not random. At thispoint, one could simply use measures relatedto entropy, or to algorithmic complexity, to
summarize in one number the spatial–temporaldifferentiation of the deterministic activationproduced by this integrated network. This numberwill be low for modular network, because, in thiscase, activity remains local, and will be equallylow for networks with widespread homogeneousconnectivity, because, all elements will respond inthe same way. Only networks that are integratedand differentiated at the same time are likely toreact to TMS with a response characterized by ahigh complexity value.
Third, the technique and the appropriateanalysis procedure must be tested in conditionswhere consciousness is graded and abolished ina controlled fashion, such as during anaesthesia
(Alkire et al., 2008 ). Specically, it would beimportant to apply TMS/hd-EEG measures of integrated information while consciousness isaltered using different anaesthetics (such asmidazolam, propofol or ketamine) that actthrough diverse mechanisms and that are associated with variable patterns of spontaneous EEGactivity. Certainly, a reliable marker should onlycorrelate with the level of consciousness, whetherthis has been altered by physiological sleep,by one anaesthetic or another, or by a patholo
gical process.
Acknowledgements
This work was supported by European grantSTREP LSHM-CT-2205-51818 to Marcello Massimini. Melanie Boly is Research Fellow at theBelgian National Fund for Scientic Research(FNRS). We thank Andrea Soddu, Silvia Casarotto and Fabio Ferrarelli for their help andcomments.
References
Alkire, M. T., Hudetz, A. G., & Tononi, G. (2008).Consciousness and anesthesia. Science , 322, 876–880.
Balduzzi, D., & Tononi, G. (2008). Integrated information indiscrete dynamical systems: Motivation and theoreticalframework. PLoS Computational Biology , 4, e1000091.
Bartels, A., & Zeki, S. (2005). The chronoarchitecture of thecerebral cortex. Philosophical Transactions of the Royal

8/8/2019 Massimini PBR Coma Science 2009
http://slidepdf.com/reader/full/massimini-pbr-coma-science-2009 13/14
213
Society of London. Series B, Biological Sciences , 360,733–750.
Berthomier, C., Drouot, X., Herman-Stoı ¨ ca, M., Berthomier,P., Prado, J., Bokar-Thire, D., et al. (2007). Automatic
analysis of single-channel sleep EEG: Validation in healthyindividuals. Sleep , 30, 1587–1595.Boly, M., Coleman, M. R., Davis, M. H., Hampshire, A., Bor,
D., Moonen, G., et al. (2007). When thoughts become action:An fMRI paradigm to study volitional brain activity innon-communicative brain injured patients. Neuroimage , 36,979–992.
Bullock, T. H., McClune, M. C., Achimowicz, J. Z., Iragui-Madoz, V. J., Duckrow, R. B., & Spencer, S. S. (1995).Temporal uctuations in coherence of brain waves. Proceed-ings of the National Academy of Sciences of the United Statesof America , 92, 11568–11572.
Cantero, J. L., Atienza, M., Madsen, J. R., & Stickgold, R.(2004). Gamma EEG dynamics in neocortex and hippocam
pus during human wakefulness and sleep. Neuroimage , 22,1271–1280.
Cash, S. S., Halgren, E., Dehghani, N., Rossetti, A. O., Thesen,T., Wang, C., et al. (2009). The human K-complex representsan isolated cortical down-state. Science , 324, 1084–1087.
Destexhe, A., Hughes, S. W., Rudolph, M., & Crunelli, V.(2007). Are corticothalamic ‘up’ states fragments of wakefulness? Trends in Neurosciences , 30, 334–342.
Engel, A. K., Fries, P., & Singer, W. (2001). Dynamicpredictions: Oscillations and synchrony in top-down processing. Nature Review, Neurosciences , 2, 704–716.
Giacino, J. T., Ashwal, S., Childs, N., Cranford, R., Jennett, B.,Katz, D. I., et al. (2002). The minimally conscious state:Denition and diagnostic criteria. Neurology , 58, 349–353.
Giacino, J. T., Kalmar, K., & Whyte, J. (2004). The JFK comarecovery scale-revised: Measurement characteristics anddiagnostic utility. Archives of Physical Medicine andRehabilitation , 85, 2020–2029.
Giacino, J. T., Hirsch, J., Schiff, N., & Laureys, S. (2006).Functional neuroimaging applications for assessment andrehabilitation planning in patients with disorders of consciousness. Archives of Physical Medicine and Rehabilitation ,87 , S67–S76.
Gill-Thwaites, H., & Munday, R. (2004). The Sensory ModalityAssessment and Rehabilitation Technique (SMART):A valid and reliable assessment for vegetative stateand minimally conscious state patients. Brain Injury , 18,
1255–1269.Graham, D. I., Adams, J. H., Murray, L. S., & Jennett, B.(2005). Neuropathology of the vegetative state after headinjury. Neuropsychological Rehabilitation , 15, 198–213.
Hahn, P. J., & Durand, D. M. (2001). Bistability dynamics insimulations of neural activity in high-extracellular-potassiumconditions. Journal of Computational Neuroscience , 11 , 5–18.
Hill, S., & Tononi, G. (2005). Modeling sleep and wakefulnessin the thalamocortical system. Journal of Neurophysiology ,93, 1671–1698.
Hobson, J. A., Pace-Schott, E. F., & Stickgold, R. (2000).Dreaming and the brain: Toward a cognitive neuroscience
of conscious states. The Behavioral and Brain Sciences , 23,793–842. discussion 904–1121
Ilmoniemi, R. J., Virtanen, J., Ruohonen, J., Karhu, J.,Aronen, H. J., Na ¨ a ¨ ta ¨ nen, R., et al. (1997). Neuronal
responses to magnetic stimulation reveal cortical reactivityand connectivity. Neuroreport , 8, 3537–3540.Kakigi, R., Naka, D., Okusa, T., Wang, X., Inui, K., Qiu, Y., et al.
(2003). Sensory perception during sleep in humans: Amagnetoencephalograhic study. Sleep Medicine , 4, 493–507.
Kalmar, K., & Giacino, J. T. (2005). The JFK coma recoveryscale - revised. Neuropsychological Rehabilitation , 15, 454–460.
Komssi, S., & Kahkonen, S. (2006). The novelty value of thecombined use of electroencephalography and transcranialmagnetic stimulation for neuroscience research. BrainResearch Reviews , 52, 183–192.
Laureys, S., & Boly, M. (2008). The changing spectrum of coma. Nature Clinical Practice Neurology , 4, 544–546.
Laureys, S., Owen, A. M., & Schiff, N. D. (2004). Brain
function in coma, vegetative state, and related disorders.Lancet Neurology , 3, 537–546.
Laureys, S., Boly, M., Moonen, G., & Maquet, P. (2009).Coma. In L. Squire (Ed.), Encyclopedia of neuroscienceVol. 2, (pp. 1133–1142). Amsterdam: Elsevier.
Massimini, M., Huber, R., Ferrarelli, F., Hill, S., & Tononi, G.(2004). The sleep slow oscillation as a traveling wave.The Journal of Neuroscience , 24, 6862–6870.
Massimini, M., Ferrarelli, F., Huber, R., Esser, S. K., Singh, H., &Tononi, G. (2005). Breakdown of cortical effective connectivity during sleep. Science , 309, 2228–2232.
Massimini, M., Ferrarelli, F., Esser, S. K., Riedner, B. A.,Huber, R., Murphy, M., et al. (2007). Triggering sleep slowwaves by transcranial magnetic stimulation. Proceedingsof the National Academy of Sciences of the United States of America , 104, 8496–8501.
Massimini, M., Tononi, G., & Huber, R. (2009). Slow waves,synaptic plasticity and information processing: Insights fromtranscranial magnetic stimulation and high-density EEGexperiments. The European Journal of Neuroscience , 29,1761–1770.
McCormick, D. A., Wang, Z., & Huguenard, J. (1993).Neurotransmitter control of neocortical neuronal activityand excitability. Cerebral Cortex , 3, 387–398.
Monti, M. M., Coleman, M. R., & Owen, A. M. (2009).Neuroimaging and the vegetative state: Resolving thebehavioral assessment dilemma? Annals of New York
Academy of Sciences , 1157 , 81–89.Myles, P. S., Leslie, K., McNeil, J., Forbes, A., & Chan, M. T.(2004). Bispectral index monitoring to prevent awarenessduring anaesthesia: The B-Aware randomised controlledtrial. Lancet , 363, 1757–1763.
Owen, A. M., Coleman, M. R., Boly, M., Davis, M. H.,Laureys, S., & Pickard, J. D. (2008). Detecting awareness inthe vegetative state. Annals of New York Academy of Sciences , 1129 , 130–138.
Owen, A. M., Coleman, M. R., Menon, D. K., Berry, E. L.,Johnsrude, I. S., Rodd, J. M., Davis, M. H., et al. (2005).Using a hierarchical approach to investigate residual

8/8/2019 Massimini PBR Coma Science 2009
http://slidepdf.com/reader/full/massimini-pbr-coma-science-2009 14/14
214
auditory cognition in persistent vegetative state. Progress inBrain Research , 150, 457–471.
Paus, T. (2005). Inferring causality in brain images: Aperturbation approach. Philosophical Transactions of the
Royal Society of London: Series B, Biological Sciences , 360,1109–1114.Plum, F., & Posner, J. B. (1972). The diagnosis of stupor and
coma. Contemporary Neurology Series , 10, 1–286.Portas, C. M., Krakow, K., Allen, P., Josephs, O., Armony, J.
L., & Frith, C. D. (2000). Auditory processing across thesleep-wake cycle: Simultaneous EEG and fMRI monitoringin humans. Neuron , 28, 991–999.
Rosanova, M., Casali, A., Bellina, V., Resta, F., Mariotti, M., &Massimini, M. (2009). Natural frequencies of humancorticothalamic circuits. Journal of Neuroscience , 29(24),7679–7685.
Rossini, P. M., Altamura, C., Ferretti, A., Vernieri, F.,Zappasodi, F., Caulo, M., et al. (2004). Does cerebrovascular
disease affect the coupling between neuronal activity andlocal haemodynamics? Brain , 127 , 99–110.
Royal College of Physicians. (1994). Medical aspects of the persistent vegetative state (1). The multi-society taskforce on PVS. The New England Journal Medicine , 330,1499–1508.
Schiff, N., Ribary, U., Plum, F., & Llina ´ s, R. (1999). Wordswithout mind. Journal Cognitive Neuroscience , 11 , 650–656.
Schnakers, C., Majerus, S., Goldman, S., Boly, M., VanEeckhout, P., Gay, S., et al. (2008). Cognitive function inthe locked-in syndrome. Journal of Neurology , 255, 323–330.
Schnakers, C., Perrin, F., Schabus, M., Hustinx, R., Majerus, S.,Moonen, G., et al. (2009). Detecting consciousness in atotal locked-in syndrome: An active event-related paradigm.Neurocase , 1–7.
Seth, A. K. (2005). Causal connectivity of evolved neuralnetworks during behavior. Network , 16, 35–54.
Seth, A. K., Dienes, Z., Cleeremans, A., Overgaard, M., &Pessoa, L. (2008). Measuring consciousness: Relating
behavioural and neurophysiological approaches. Trends inCognitive Sciences , 12, 314–321.
Shiel, A., Horn, S. A., Wilson, B. A., Watson, M. J., Campbell,M. J., & McLellan, D. L. (2000). The Wessex Head Injury
Matrix (WHIM) main scale: A preliminary report on a scaleto assess and monitor patient recovery after severe headinjury. Clinical Rehabilitation , 14, 408–416.
Steriade, M., Timodeev, I., & Grenier, F. (2001). Naturalwaking and sleep states: A view from inside neocorticalneurons. Journal of Neurophysiology , 85, 1969–1985.
Tononi, G. (2004). An information integration theory of consciousness. BMC Neuroscience , 5, 42.
Tononi, G. (2005). Consciousness, information integration, andthe brain. Progress in Brain Research , 150, 109–126.
Tononi, G. (2008). Consciousness as integrated information:A provisional manifesto. The Biological Bulletin , 215,216–242.
Tononi, G., & Laureys, S. (2008). The neurology of conscious
ness: An overview. In S. Laureys and G. Tononi (Eds.),The Neurology of Consciousness (pp. 375–411). Amsterdam:Elsevier.
Tononi, G., & Massimini, M. (2008). Why does consciousnessfade in early sleep? Annals of New York Academy of Sciences , 1129 , 330–334.
Tononi, G., & Sporns, O. (2003). Measuring informationintegration. BMC Neuroscience , 4, 31.
Tononi, G., Sporns, O., & Edelman, G. M. (1994). A measurefor brain complexity: Relating functional segregation andintegration in the nervous system. Proceedings of theNational Academy of Science of the United States of America ,91, 5033–5037.
Vanderwolf, C. H. (2000). Are neocortical gamma wavesrelated to consciousness? Brain Research , 855, 217–224.
Virtanen, J., Ruohonen, J., Na ¨ a ¨ ta ¨ nen, R., & Ilmoniemi, R. J.(1999). Instrumentation for the measurement of electricbrain responses to transcranial magnetic stimulation. Med-ical & Biological Engineering & Computing , 37 , 322–326.