Embed Size (px)
Citation preview

MASSIVE PYELOINTERSTITIAL EXTRAVASATION OF CONTRAST MATERIAL
By EVERETT ANDERSON, M.D., and OLIVER E. COBS, M.D.
From the Department of Surgery, Division of Urology, Peter Bent Brigham Hospital and Harvard Medical School, Boston, Massachusetts
OVERDISTENSION of the renal pelvis by ureteral obstruction, ureteral reflux, or retrograde pyelography may result in pyelovenous, pyelolymphatic, pyelotubular (pyelointerstitial), or peripelvic extravasation of urine (Hinman, 1963). Kohler (1953) found that a pressure of 80
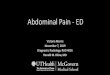
FIG. 1 FIG. 2
Fig. 1.-lleogram demonstrating free ureteral reflux with massive pyelointerstitial backflow extending into subcapsular space.
Fig 2.-lleogram demonstrating free ureteral reflux with absence of pyelointerstitial backflow.
to 100 mm. Hg is necessary to initiate backflow in a clinically normal kidney, but much lower pressures can sustain backflow once hydronephrosis has developed. Inflammation of the renal pelvis enhances all types of pelvirenal backflow. Recently we have had the opportunity to study an unusual instance of transient ureteral obstruction, pyelonephritis, and massive pyelo- interstitial backflow in a solitary kidney. A clinical and radiographic cure was obtained by conservative management.
410

M A S S I V E P Y E L O I N T E R S T I T T A L E X T R A V A S A T I O N O F C O N T R A S T M A T E R I A L 41 I
Case Report.-D. H. (PBBH No. 49551) a Caucasian male, aged 28 years, was admitted to the hospital with a 6 days' history of right flank pain, nausea, vomiting, hzmaturia, pyuria, chills, fever, and progressive diminution of urinary volume. He had undergone repair of ineningoniyelocele at age 2, and bilateral cutaneous ureterosignioid- ostomies had been performed at age 4 for fzcal and urinary incontinence. At age 20 he underwent left nephroureterectomy for a nonfunctioning left kidney and perinephric abscess; and ileal loop urinary diversion was performed at age 22 for persistent attacks of right pyelonephritis. The oral temperature was 102"F, and marked right costovertebral angle tenderness was present. The ileostomy stoma admitted a catheter, No. 20 French in size, with ease, and no residual urine was present in the conduit. Urinalysis revealed a microscopic sediment containing many erythrocytes and leucocytes, and the urine culture demonstrated Profrus vulgaris. Blood urea nitrogen was 116 mg./100 ml., sodium=124, potassium=3.6, chloride=91, and bicarbonate-10 mEq/l. KUB showed good psoas shadows and renal outline with absence of scoliosis and urinary calculi. Initial retro- grade instillation of radiopaque media into the ileal conduit showed no reflux up the right ureter.
Admission diagnoses were dehydration, acute right pyelonephritis, and progressive ureteroileal obstruction. Nephrostomy was considered, but follow- ing conservative treatment with intravenous saline, mannitol, and chloramphenicol, a diuresis occurred. A repeat ileogram under cine control (Fig. I ) on the fifth hospital day demonstrated free reflux up the right ureter with massive pyelointerstitial backflow from the superior and middle calyces extending into the subcapsular space. The fever and costovertebral angle tenderness had resolved on the eighth hospital day, and the blood urea nitrogen was 21 mg./l00 ml. on the fifteenth hospital day. The patient was asymptomatic at time of discharge from the hospital, and a cine ileogram (Fig. 2) three months later showed minimal pyelocaliectasis and dilatation of the urogran, demonstrating normal upper ureter with absence of interstitial extravasation. There was active peristalsis of the ureter and ileum with good emptying and no evidence of obstruction. An intravenous urogram (Fig. 3) demonstrated a normal upper urinary tract.
FIG. 3
urinary tract.
DISCUSSION
In this patient the combined effect of severe pyelotubular inflammation and progressive ureteral obstruction resulted in massive pyelo-interstitial extravasation of media. The exact cause of the ureteral obstruction.was never determined, although it was presumed that a blood clot or mucoid plug in the distal ureter had temporarily impeded the flow of urine. Conservative management with parenteral fluids, mannitol, and chemotherapy effected a clinical and radio- graphic cure.
REFERENCES
HINMAN, F. (1963). In : " Urology," edited by M. F. Campbell. Philadelphia and London :
KOHLER, R. (1953). Acta radio/., Stockh., Suppl. 99. W. B. Saunders Co.