Embed Size (px)
Citation preview
Máster en Medicina Cosmética, Estética y del Envejecimiento Fisiológico PRP In Facial Rejuvenation: An Extensive Study of the Aging Process and the Role of Platelet Rich Plasma in Facial Rejuvenation as an Anti-aging Treatment.
Dr. Shatha Rawashdeh Dr. Vanessa Torrico Sejas.
1
Index:
Number Subject Page 1 Summary 2 2 Introduction 3 3 Antecedents 4 4.1 Introduction into Skin Aging 5 4.2 The Aging Process 6-7 4.3 Intrinsic/Chronological Aging 8-9 4.4 Extrinsic Aging/Photoaging 10-15 4.5 Photoaging and the Importance of Sun Protection 16-17 4.6 Clinical and Histological Manifestation of Aged Skin 18-19 5.1 Platelet Rich Plasma (PRP):Platelets 20-23 5.2 Platelet Rich Plasma (PRP):Definition 24-27 5.3 Platelet Rich Plasma (PRP):Growth Factors 28-32 5.4 Platelet Rich Plasma (PRP):Mechanism of Action 33-37 5.5 Platelet Rich Plasma (PRP):Obtaining and Injection PRP 38-42 6 Objectives 43 7 Materials and Methods 43 8 Results 44 9 PRP in Facial Rejuvenation: Review and Evaluation of Clinical
Studies 45-51
10 PRP in Cell Therapy and Regenerative Medicine 51-52 11 Methods to Improve Patient Satisfaction 53 12 Complications of PRP 53-54 13 Contraindications to PRP 55-56 14 Advantages,limitations and Precautions 56 15 Discussion 57-58 16 Conclusion 59 References 60-67
2
1. Summary.
The human body has a remarkable capacity to heal itself. Regeneration of new tissue is accomplished by stem cells and is fostered by growth factors and hormones. Platelet-rich plasma (PRP) is an emerging treatment in a new health sector known as orthobiologics, which refer to growth factors and proteins that are naturally found in the human body.
In humans, PRP has been investigated and used as a clinical tool for several types of medical treatments, including nerve injury, tendonitis, osteoarthritis, cardiac muscle injury, bone repair and regeneration, plastic surgery, and oral surgery. It has received attention in the popular media because of its use in treating sports injuries in professional athletes.
Aging of the skin, dermal components, and cells means that the skin texture and appearance deteriorate and have been damaged. Aging affects the hands and soft tissue of the face, neck, and décolleté. This is characterized by sagging jowls, thinning of the skin, puffiness, age spots, and wrinkling.
In dermatology and cosmetic medicine, PRP has been used to treat acne, scarring, and alopecia. It is also effective for skin rejuvenation and tightening around the eyes (for thin crepe-like skin and fine lines) and in the following areas: cheeks and midface, thinning skin on the neck, jawline and submalar regions, back of hands, décolleté, and others (eg, knees, elbows, and upper arms, as well as for postpregnancy skin laxity).
This review shows platelet-rich-plasma (PRP) as an enhancer of the histological characteristics of the tissues with platelet-derived growth factor receptors. A review has been made of the literature on the platelet-rich plasma published in PubMed. This article describes the aging process, the cellular biology of PRP, the technique for obtaining it, its clinical applications and studies regarding PRP in facial rejuvenation and its role as an antiageing mechanism.
Keywords
Platelet rich plasma - skin aging - skin rejuvenation –skin wrinkles-biostimulation-photoaging –intrinsic aging - growth factors - cytokines- transforming growth factor-β - platelet-derived growth factor - vascular endothelial growth factor

3
2. Introduction.
Autologous Platelet-rich Plasma (PRP) has attracted attention for skin rejuvenation. PRP is derived from fresh whole blood, which contains a high concentration of platelets (1). Various GF, including platelet-derived growth factor (PDGF), transforming growth factor (TGF), vascular endothelial growth factor (VEGF), and insulin-like growth factor (IGF), are secreted from the α-granules of concentrated platelets activated by aggregation inducers(2). These factors are known to regulate processes including cell migration, attachment, proliferation and differentiation, and promote extracellular matrix (ECM) accumulation by binding to specific cell surface receptors (3), Although the optimal PRP platelet concentration is unclear, the current methods by which PRP is prepared is reported to involve 300~700% enrichment, with platelet concentrations consequently increasing to greater than 1,000,000 platelets/µl. (4)
Due to the presence of high concentrations of these growth factors, PRP has been used in a wide variety of surgical procedures and clinical treatments, including the treatment of problematic wounds(5)and maxillofacial bone defects, cosmetic surgeries(6), and gastrointestinal surgeries(7). Recently, PRP has attracted attention in the field of dermatology, specifically in the aesthetic field for skin rejuvenation.
The application of PRP stimulates the rejuvenation of photoaged facial skin, improving its clinical appearance and inducing new collagen synthesis. Since PRP secretes various growth factors with roles in skin regeneration, it may be hypothesized that PRP may induce the synthesis of collagen and other matrix components by stimulating the activation of fibroblasts, thus, rejuvenating the skin. Though PRP is widely used in clinical dermatology, experimental studies confirming the effects of PRP on aged fibroblasts are very limited (8).
4
3. Antecedents.
Plasma rich in growth factors (PRGF) is an endogenous therapeutic technology that is
gaining interest in regenerative medicine due to its potential to stimulate and accelerate
tissue healing and bone regeneration. This autologous biotechnology is designed for the
in situ delivery of multiple cellular modulators and the formation of a fibrin scaffold,
thereby providing different formulations that can be widely used in numerous medical
and scientific fields. It has been shown that the application of a Platelet Rich Plasma
(PRP) enhances early wound healing (9, 10), and improves healing in diabetic ulcers (11).
Since the 1990s, the application of platelet preparations for wound healing has
outpaced that of isolated, exogenous growth factors.
Autologous platelet rich plasma (PRP) injections were first used in 1987 in open heart
surgery (12). Apart from the wide use of PRP to accelerate wound healing, there is
substantial clinical evidence regarding its use in other medical fields. For example, cross-
linked PRP forms a gel which is widely used in orthopedics, sports medicine, as well as in
maxillofacial surgery (13, 14), cosmetic surgery (15) and tissue engineering among
others.
Following the successful use of Platelet Rich Plasma in the field of medical pathology, it
is now being used in the aesthetics area with many advantages such as: tissue
regeneration and rejuvenation, induction of cell differentiation, extracellular matrix
formation, recruitment of other cells to the site of injury, and an increase in collagen
production, which can increase skin thickness and overall skin health. In addition, PRP is
nonallergenic, is an autologous physiological product, eliminates donor transmissible
infections, and is biological glue for tissue adhesion, especially in skin flaps, bone grafts,
and trauma. (16)
5
4.1. Introduction into Skin Aging.
Skin – the largest organ of the body – protects all the other organs from the external environment. The skin is a complex organ with multiple structures and cell types and divided into three layers: epidermis, dermis, and the subcutaneous tissue. The epidermis is mainly composed of keratinocytes, pigment-producing melanocytes, and antigen-presenting Langerhans cells. A basement membrane separates the epidermis from the dermis, which primarily contains extracellular proteins produced by the fibroblasts below.
The vascular supply to the skin resides in the dermis. The subcutaneous tissue consists of fat cells that underline the connective tissue network. Type I collagen is the most abundant protein in the skin connective tissue. The other extracellular matrix proteins, which are a part of the skin connective tissue, are collagens (III, V, and VII), elastin, proteoglycans, fibronectin, etc. The newly synthesized type I procollagen is secreted into the dermal extracellular space where it undergoes enzymatic processing to arrange itself into a triple helix configuration. (17)
With age the skin’s natural rejuvenation process slows drastically and the Skinbecomes thinner, drier, and less elastic. (18)
Skin aging is particularly important because of its social impact. It is visible and also represents an ideal model organ for investigating the aging process (19). The “biological clock” affects both the skin and the internal organs in a similar way, causing irreversible degeneration (20, 21).
However, Nicholas Perricone, a prominent American dermatologist, begins his book with the words “Wrinkled, sagging skin is not the inevitable result of getting older. It’s a disease, and you can fight it” (22).

6
4.2. The Aging Process.
Aging represents a biologic attrition at the cellular level resulting in decreased reserve capacity and ability to perform normal functions occurs throughout an organisms’ life span increasing the likelihood of death. Aging is thus the result of a genetic program or a clock that is implanted in the genetic make-up of each species. One must also remember that cumulative damage to the genes and proteins derived thereof, result in compromised function and homeostatic failure. This leads the organism towards premature aging and death, which in turn shall depend on its repair systems.
The somatic cells have telomeres at the terminal portion of the eukaryotic chromosomes which consist of many hundreds of tandem short sequence repeats (TTAGGG) predetermining the number of times the cell can divide before it senesces. The enzyme DNA polymerase that replicates cellular chromosomes during mitosis cannot replicate the final base pairs of each chromosome, resulting in progressive telomere shortening with each cellular division. A critically short telomere will compromise gene transcription and signal cellular senescence which is otherwise better known as “apoptosis”. (23)
Human keratinocytes approach replicative senescence after 50–100 population doublings in culture and remain permanently arrested in the G1 phase of the cell cycle. The telomere is just one of the three molecules which were found to be crucial for replicative senescence. In addition, keratinocytes have an increased resistance to apoptosis, thus giving a time window for DNA and protein damage to accumulate. (24)

7
The skin, being the ultimate protective barrier between the internal organs and the environment, is exposed to ultraviolet (UV) irradiation and to a lesser extent to other DNA damaging agents such as cigarette smoke, automobile exhaust, and professional exposure. UV irradiation causes formation of pyrimidine dimers and the benzo[a]pyrene from cigarette smoke causes formation of guanine base pair adducts. All this moves hand-in-hand with damage from endogenous agents such as reactive oxygen and nitrogen species (ROS/RNS) generated by all aerobic cell species as part of their routine metabolic processes. (25)
Amino acid racemization and interaction of amino acid groups with reducing sugars (Maillard reaction) result in an altered or total loss of protein functions which does the dermal collagen proteins.
Skin aging is influenced by several factors including genetics, environmental exposure (UV radiation, xenobiotics, and mechanical stress), hormonal changes and metabolic processes (generation of reactive chemical compounds such as activated oxygen species, sugars and aldehydes). All factors together act on the alterations of skin structure, function, and appearance. Yet solar UV radiation unquestionably is the single major factor responsible for skin aging. (26)
8
4.3. Intrinsic /chronological Aging.
Intrinsic aging depends on time. The changes occur partially as the result of cumulative endogenous damage due to the continuous formation of reactive oxygen species (ROS), which are generated by oxidative cellular metabolism. Despite a strong antioxidant defense system, damage generated by ROS affects cellular constituents such as membranes, enzymes, and DNA. (27, 28)
It has a genetic background, but is also due to decreased sex hormone levels. The telomere, a terminal portion of the eukaryotic chromosome, plays an important role. With each cell division, the length of the human telomere shortens. Even in fibroblasts of quiescent skin more than 30% of the telomere length is lost during adulthood. (29) The enzyme telomerase is responsible for its maintenance. It seems that telomeres are responsible for longevity. (30) The progressive erosion of the telomere sequence (50–100 bp per mitosis) through successive cycles of replication eventually precludes protection of the ends of the chromosomes, thus preventing end-to-end fusions, which is incompatible with normal cell function.
The majority of cells have the capacity for about 60 to 70 postnatal doublings during their lifecycles, and thereafter they reach senescence, remaining viable but incapable of proliferation. This event facilitates end-to-end chromosomal fusions resulting in karyotype disarray with subsequent apoptosis, thus serving as the “biological clock”. (31)
9
Skin aging is affected by growth factor modifications and hormone activity that declines with age. The best-known decline is that of sex steroids such estrogen, testosterone, dehydroepiandrosterone (DHEA), and its sulfate ester (DHEAS). Other hormones such as melatonin, insulin, cortisol, thyroxine, and growth hormone decline too. At the same time, induced levels of certain signaling molecules such as cytokines and chemokine’s decline as well, leading to the deterioration of several skin functions (32). Also, the levels of their receptors decline as well (33).
At the same time, some signaling molecules increase with age. One of these is a cytokine called transforming growth factorbeta1, which induces fibroblast senescence. Cellular senescence is a result of molecular alterations in the cellular milieu as well as in DNA and proteins within the cell. All of these changes gradually lead to aberrant cellular response to environmental factors, which can decrease viability and lead to cell death. (34)

10
4.4. Extrinsic Aging/Photoaging. Extrinsic aging develops due to several factors: ionizing radiation, severe physical and psychological stress, alcohol intake, poor nutrition, overeating, environmental pollution, and exposure to UV radiation. Among all these environmental factors UV radiation contributes up to 80%. It is the most important factor in skin aging, especially in premature aging. Both UVB (290–320 nm), and UVA (320–400 nm) are responsible, and the skin Alterations caused by UV radiation depend upon the phenotype of photoexposed skin (27, 35). UVB induces alterations mainly at the epidermal level, where the bulk of UVB is absorbed. It damages the DNA in keratinocytes and melanocytes, and induces production of the soluble epidermal factor (ESF) and proteolytic enzymes, which can be found in the dermis after UV exposure. UVB is responsible for appearance of thymidine dimers, which are also called “UV fingerprints.” That is, after UVB exposure, a strong covalent bond between two thymidines occurs. With aging, this bond cannot be dissolved quickly, and accumulation of mutations occurs. Affected cells appear as sunburn cells 8 to 12 hours after exposure. Reduced production of DNA can be observed during the next 12 hours. Actinic keratoses, lentigines, carcinomas, and melanomas represent delayed effects. A mnemonic for UVB is B as in burn or bad. UVA penetrates more deeply into the dermis and damages both the epidermis and dermis. The amount of UVA in ambient light exceeds the UVB by 10 to 100 times, but UVB has biological effects 1,000 times stronger than UVA. It is accepted that UVA radiation plays an important role in the pathogenesis of photoaging, so the mnemonic for UVA is A as in aging (35).

11
The exact mechanism of how UV radiation causes skin aging is not clear. The dermal extracellular matrix consists of type I and III collagens, elastin, proteoglycans, and fibronectin, and collagen fibrils strengthen the skin. Photoaged skin is characterized by alterations in dermal connective tissue. The amount and structure of this tissue seems to be responsible for wrinkle formation. In photoaged skin, collagen fibrils are disorganized and elastin-containing material accumulates (36). Levels of precursors as well as cross-links between type I and III collagens are reduced, whereas elastin is increased (37, 38). UV radiation increases the production of collagen-degrading enzymes, matrix metalloproteinases (MMPs), and the xerodermapigmentosum factor (XPF), which can also be found in the epidermis. XPF induces epidermal-dermal invagination, representing the beginning of wrinkle formation. At the base of wrinkles, less type IV and VII collagen is found. This instability deepens the wrinkles. Each MMP degrades a different dermal matrix protein; for example, MMP-1 cleaves collagen types I, II, and III, and MMP-9 (gelatinase) degrades type IV and V and gelatin. Under normal conditions, MMPs are part of a coordinated network and are regulated by their endogenous inhibitors (TIMPs). The imbalance between activation and inhibition can lead to proteolysis (39). The activation of MMPs can be triggered by UVA and UVB, but molecular mechanisms differ depending upon the type of radiation. UVA radiation can generate ROS that affect lipid peroxidation and generate DNA strand breaks (40). On the other hand, within minutes after exposure UVB radiation causes MMP activity and DNA damage. These effects can be observed after exposing human skin to one-tenth of the minimal erythema dose. The degree of skin damage following long-lasting UV irradiation also depends on the skin phototype according to Fitzpatrick. In lighter complexes (types I and II) more serious degenerative changes are elicited than in types III and IV, in which melanosomes in the upper epidermal layer serve as relatively good UVA and UVB protection. (41)
12
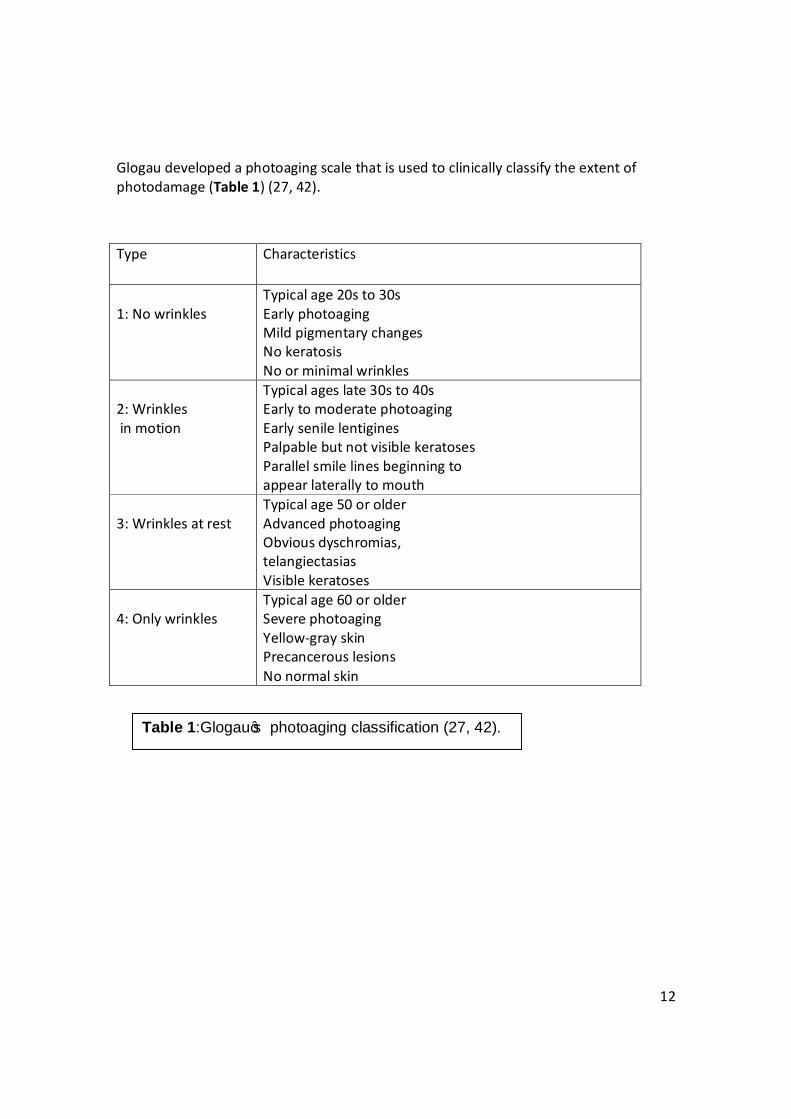
Glogau developed a photoaging scale that is used to clinically classify the extent of photodamage (Table 1) (27, 42).
Type Characteristics
1: No wrinkles
Typical age 20s to 30s Early photoaging Mild pigmentary changes No keratosis No or minimal wrinkles
2: Wrinkles in motion
Typical ages late 30s to 40s Early to moderate photoaging Early senile lentigines Palpable but not visible keratoses Parallel smile lines beginning to appear laterally to mouth
3: Wrinkles at rest
Typical age 50 or older Advanced photoaging Obvious dyschromias, telangiectasias Visible keratoses
4: Only wrinkles
Typical age 60 or older Severe photoaging Yellow-gray skin Precancerous lesions No normal skin
Table 1:Glogau’s photoaging classification (27, 42).

13
Another environmental factor contributing to premature aging is smoking. “Smoker’s face” or “cigarette skin” is characteristic; implying increased facial wrinkling and an ashen and gray skin appearance (43, 44). A prematurely old appearance is a symptom of long-term smokers. Yellow and irregularly thickened skin is result of elastic tissue breakdown due to smoking (45) or to UV. Premature facial wrinkling is not reduced in women on hormone replacement therapy (46). Genetic predisposition may also influence the development of facial wrinkling (47). It seems that cigarette smoking induces the activation of MMPs in the same mode as in persons with significant sun exposure (48). Smoking also reduces facial stratum corneum moisture as well as vitamin A level, which is important in reducing the extent of collagen damage (27). The photochemical activity of smog is due to the reduction of air pollutants such as nitrogen oxides and volatile organic compounds created from fossil fuel combustion in the presence of sunlight. Emission from factories and motor vehicle exhaust are primary sources of these compounds. The major targets of ozone in the skin are the superficial epidermal layers; this results in the depletion of antioxidants such as alpha-tocopherol (vitamin E) and ascorbic acid (vitamin C) in the superficial epidermal layers (49). As stochastic damage is explained, the damage is initiated by random cosmic radiation and triggered by free radicals during cell metabolism, which damages cell lipid compounds, especially membrane structures. The free radical theory is one of the most widely accepted theories to explain the cause of skin aging. These compounds are formed when oxygen molecules combine with other molecules, yielding an odd number of electrons. That is, an oxygen molecule with paired electrons is stable, but one with an unpaired electron is very reactive and it takes electrons from other vital components. As result, cell death or mutation appears (27).
14
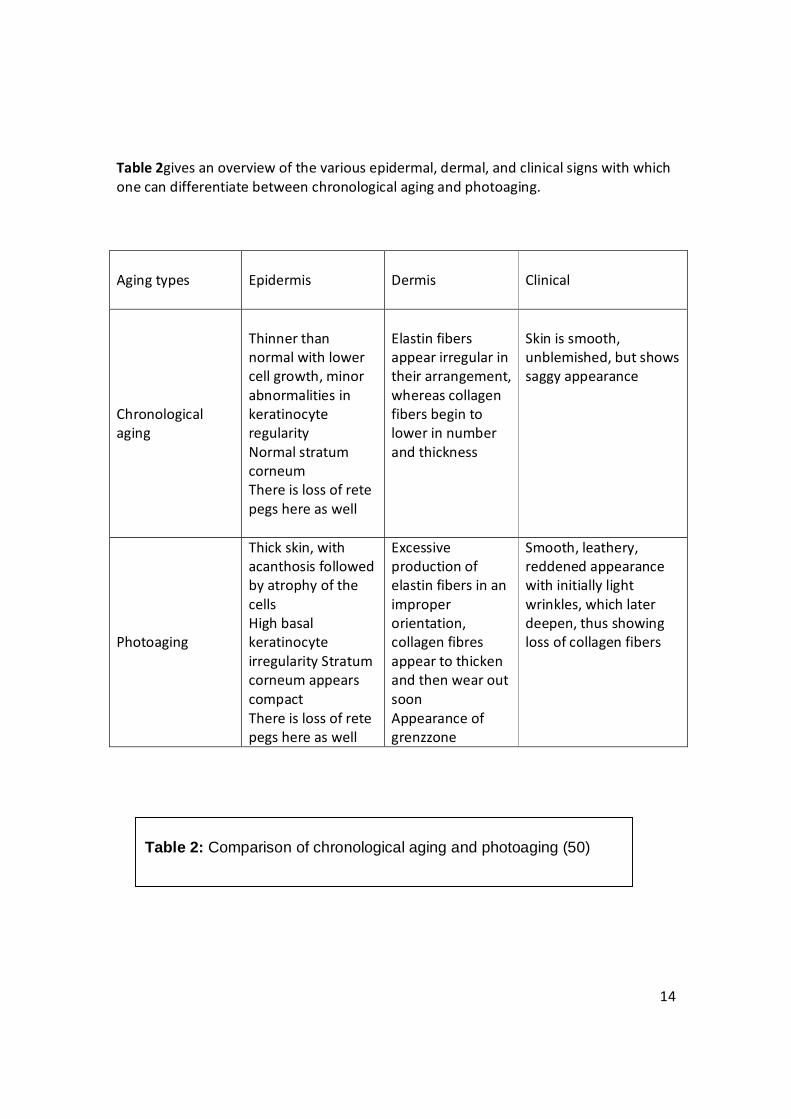
Table 2gives an overview of the various epidermal, dermal, and clinical signs with which one can differentiate between chronological aging and photoaging.
Aging types
Epidermis
Dermis
Clinical
Chronological aging
Thinner than normal with lower cell growth, minor abnormalities in keratinocyte regularity Normal stratum corneum There is loss of rete pegs here as well
Elastin fibers appear irregular in their arrangement, whereas collagen fibers begin to lower in number and thickness
Skin is smooth, unblemished, but shows saggy appearance
Photoaging
Thick skin, with acanthosis followed by atrophy of the cells High basal keratinocyte irregularity Stratum corneum appears compact There is loss of rete pegs here as well
Excessive production of elastin fibers in an improper orientation, collagen fibres appear to thicken and then wear out soon Appearance of grenzzone
Smooth, leathery, reddened appearance with initially light wrinkles, which later deepen, thus showing loss of collagen fibers
Table 2: Comparison of chronological aging and photoaging (50)

15
The picture below (Picture 2) is for a 69-year-old man presented with a 25-year history of gradual, asymptomatic thickening and wrinkling of the skin on the left side of his face. The physical examination showed hyperkeratosis with accentuated ridging, multiple open comedones, and areas of nodular elastosis. Histopathological analysis showed an accumulation of elastolytic material in the dermis and the formation of milia within the vellus hair follicles. Findings were consistent with the Favre–Racouchot syndrome of photodamaged skin, known as dermatoheliosis. The patient reported that he had driven a delivery truck for 28 years. Ultraviolet A (UVA) rays transmit through window glass, penetrating the epidermis and upper layers of dermis. Chronic UVA exposure can result in thickening of the epidermis and stratum corneum, as well as destruction of elastic fibers. This photoaging effect of UVA is contrasted with photocarcinogenesis. Although exposure to ultraviolet B (UVB) rays is linked to a higher rate of photocarcinogenesis, UVA has also been shown to induce substantial DNA mutations and direct toxicity, leading to the formation of skin cancer. The use of sun protection and topical retinoids and periodic monitoring for skin cancer were recommended for the patient. (51)
Picture 2: A 69 year old man presented with a 25-year history of gradual, asymptomatic thickening and wrinkling of the skin on the left side of his face. (51)
16
4.5. Photoaging and the Importance of Sun Protection. This part was included in this review based on the fact that exposure to sun is responsible of 80% of photodamaged skin. So it should be emphasized that sun protection in daily life is a must to maintain a healthy youthful skin. The skin is equipped with two photoprotective mechanisms: the melanin in the lower layer of epidermis, and the urocanic acid barrier of the stratum corneum, Which reflects and absorbs a significant amount of UVB radiation. The thickness of the stratum corneum appears to be highly significant for photoprotection (53). Antioxidants provide protection against UVB-induced oxidative stress, especially in stratum corneum lipids. Even systemically applied antioxidants accumulate in the stratum corneum and play an important role against UV-induced skin damage (54) The body has developed further defense mechanisms that protect against UV radiation and dangerous free radicals. Antioxidants naturally occurring in the skin are superoxide dismutase, catalase, alpha-tocopherol, ascorbic acid, ubiquinone, and glutathione. Many of them are inhibited by UV and visible light. The antioxidant program consists of a diet containing large amounts of vitamins A, E, and C, grape-seed extracts, coenzyme Q10, and alpha-lipoic acid (55). The most highly recommended foods include: avocados, berries, dark green leafy vegetables, orange-colored vegetables and fruits, pineapples,salmon, and tomatoes. The mainstay in the prevention of skin aging is photoprotection. UV filters are now present in cosmetic products for daily use, such as makeup, creams, lotions, and hair sprays.
17
The general requirements are that modern sunscreens should protect against UVA and UVB rays and be photo-stable and water resistant Chemical UV filters have the capacity to absorb shortwavelength UV and transform photons into heat-emitting long-wavelength (infrared) radiation. Most of them absorb a small wavelength range. They can be divided into three groups. The first group consists of molecules that primarily absorb the UVB spectrum (p-aminobenzoic acid derivatives and zincacid esters), and second of molecules that primarily absorb the UVA spectrum (butyl-methoxydibenzoylmethane). The third group consists of molecules that absorb UVA and UVB photons (benzophenone). A combination of different filters in the same product renders the whole filter system photo-unstable that means that UV exposure causes photochemical reactions that generate ROS with subsequent phototoxic and photoallergic reactions. Great efforts have been made to stabilize molecules in UV filters, which have improved the efficacy of photoprotection with chemical UV filters. Today there is a growing need for standardization and evaluation of UVA photoprotection, while for UVB there is already consensus on the international level (56). The use of physical filters is encouraged. The most frequently used of these are microparticles of zinc oxide and titanium dioxide with diameters in the range of 10 to 100 nm. They are capable of reflecting a broad spectrum of UVA and UVB rays. They do not penetrate into the skin and thus have low potential for developing toxic or allergic effects. Today they are increasingly being used in combination with chemical filters. One disadvantage of the inorganic micropigments is that they reflect visible light, creating a “ghost” effect. This is one reason such sunscreens are often rejected by consumers (57, 58)
18
4.6. Clinical and Histological Manifestations of Aged Skin. Xerosis, laxity, wrinkles, slackness, and the occurrence of benign neoplasms such as seborrheickeratoses and cherry angiomas. There are histological features that accompany these changes. In the epidermis, there is no alteration in the stratum corneum and epidermal thickness, keratinocyte shape, and their adhesion, but a decreased number of melanocytes and Langerhans cells is evident (23). The most obvious changes are at the epidermaldermal junction: flattening of the rete ridges with reduced surface contact of the epidermis and dermis. This results in a reduced exchange of nutrients and metabolites between these two parts. In the dermis several fibroblasts may be seen, as well as a loss of dermal volume (23, 52). A decrease in blood supply due to a reduced number of blood vessels also occurs. There is also a depressed sensory and autonomic innervation of epidermis and dermis. Cutaneous appendages are affected as well. Terminal hair converts to vellus hair. As melanocytes from the bulb are lost, hairs begin to gray. Further reasons for graying are decreased tyrosinase activity, less efficient melanosomal transfer and migration, and melanocyte proliferation (59). Factors that contribute to wrinkling include changes in muscles, the loss of subcutaneous fat tissue, gravitational forces, and the loss of substance of facial bonesand cartilage. Expression lines appear as result of repeated tractions caused by facial muscles that lead to formation of deep creases over the forehead and between eyebrows, and in nasolabial folds and periorbital areas. Repeated folding of the skin during sleeping in the same position on the side of the face contributes to appearance of “sleeping lines.”
19
Histologically, thick connective tissue strands containing muscle cells are present beneath the wrinkle (24). In the muscles and accumulation of lipofuscin (the “age pigment”), a marker of cellular damage, appears. The deterioration of neuromuscular control contributes to wrinkle formation (26). The constant gravitational force also acts on the facial skin, resulting in an altered distribution of fat and sagging. Skin becomes lax and soft tissue support is diminished. Gravitational effects with advanced years play an important role and contribute to advanced sagging. This factor is particularly prominent in the upper and lower eyelids, on the cheeks, and in the neck region. Fat depletion and accumulation at unusual sites contributes to the altered appearance of the face (26). It affects the forehead, periorbital, and buccal areas, the inner line of nasolabial folds, and the temporal and perioral regions. At the same time it accumulates submentally, around the jaws, at outer lines of nasolabial folds and at lateral malar areas. In contrast to the young, in whom fat tissue is diffusely distributed, in aged skin fat tends to accumulate in pockets, which droop and sag due to the force of gravity (26, 27). The mass of facial bones and skeletal bones reduces with age. Resorption affects the mandible, maxilla, and frontal bones. This loss of bone enhances facial sagging and wrinkling with obliteration of the demarcation between the jaw and neck that is so distinct in young persons (28).
20
5.1. Platelet Rich Plasma (PRP):Platelets.
Platelets are the first element to arrive at the site of tissue injury and are particularly
active in the early inflammatory phases of the healing process (60).
They play a role in aggregation, clot formation, homeostasis through cell membrane
adherence, and release of substances that promote tissue repair and that influence the
reactivity of blood vessels and blood cell types involved in angiogenesis, regeneration,
and inflammation (61).
Platelet secretory granules contain growth factors (GFs), signaling molecules, cytokines,
integrins, coagulation proteins, adhesion molecules, and some other molecules, which
are synthesized in megakaryocytes and packaged into the granules through vesicle
trafficking processes (62). Three major storage compartments in platelets are alpha
granules, dense granules, and lysosomes (62).
Platelets mediate these effects through degranulation, in which platelet-derived GF
(PDGF), insulin-like GF (IGF1), transforming GF-beta 1 (TGF-β1), vascular endothelial GF
(VEGF), basic fibroblastic GF (bFGF), and epidermal GF (EGF) are released from alpha
granules (63). In fact, the majority of the platelet substances are contained in alpha
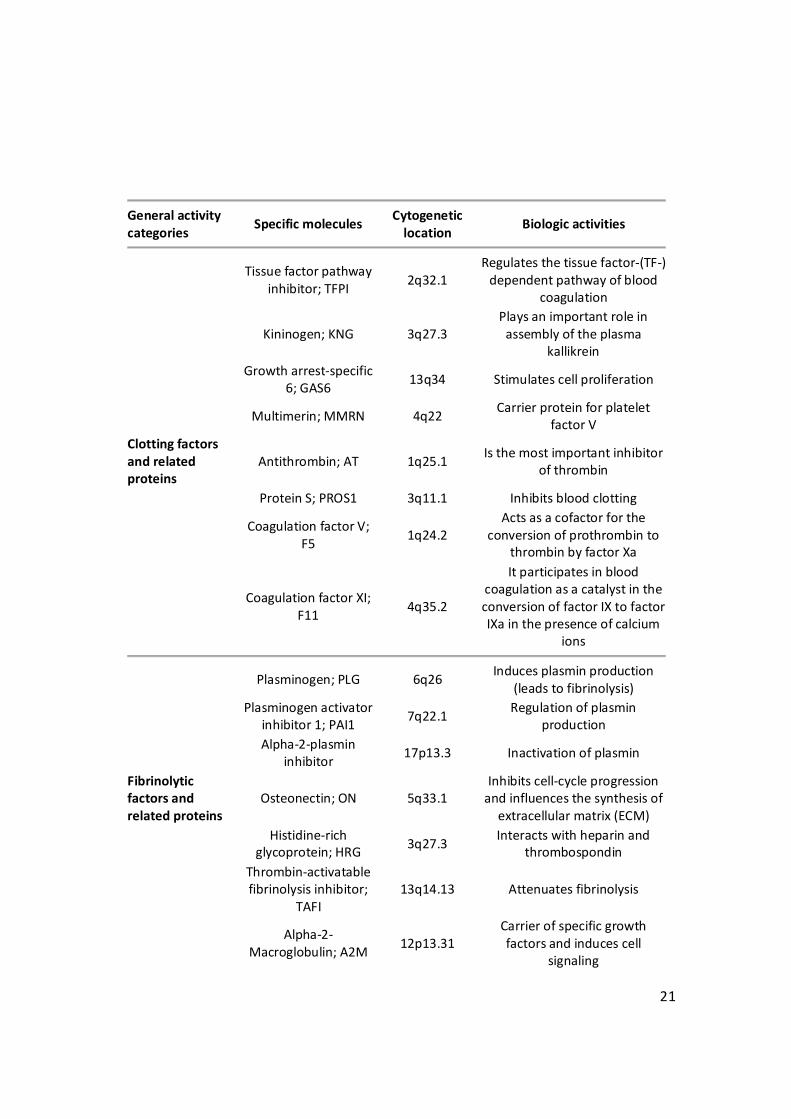
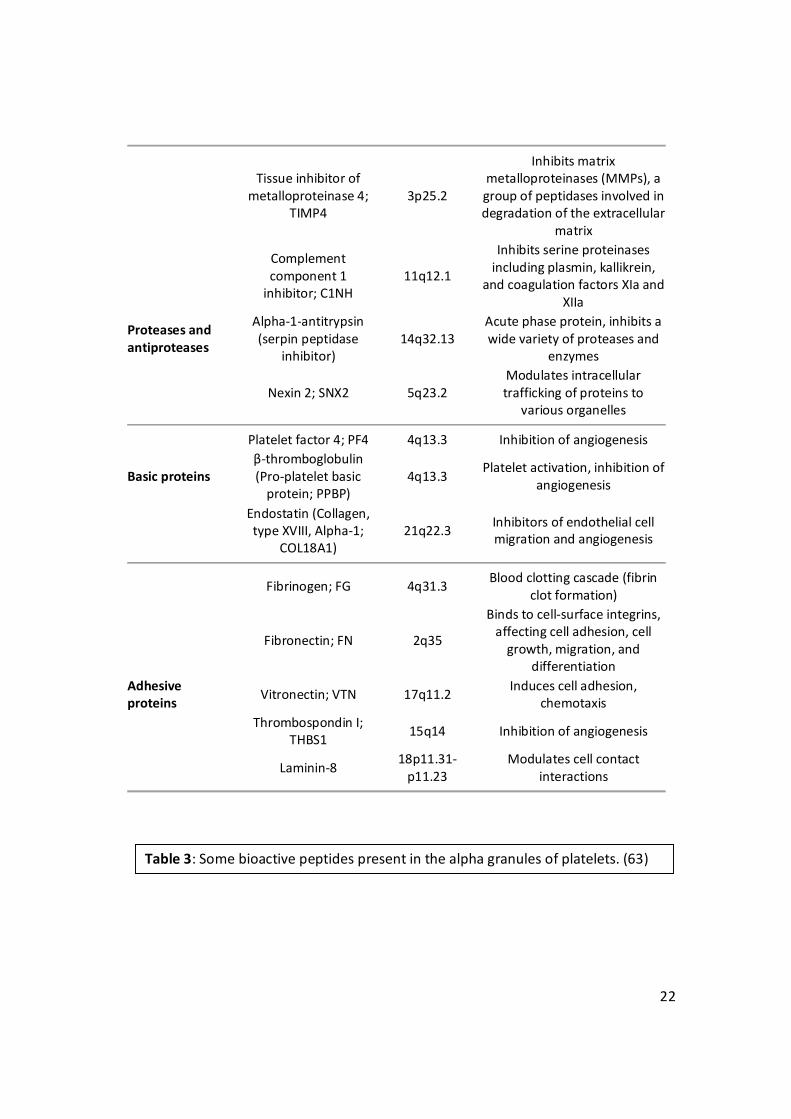
granules (see Table 3) (63).
When platelets are activated, they exocytose the granules; this process is mediated by
molecular mechanisms homologous to other secretory cells, uniquely coupled to cell
activation by intracellular signaling events (64).
21
General activity categories Specific molecules Cytogenetic
location Biologic activities
Tissue factor pathway
inhibitor; TFPI 2q32.1 Regulates the tissue factor-(TF-)
dependent pathway of blood coagulation
Kininogen; KNG 3q27.3 Plays an important role in
assembly of the plasma kallikrein
Growth arrest-specific
6; GAS6 13q34 Stimulates cell proliferation
Multimerin; MMRN 4q22 Carrier protein for platelet factor V
Clotting factors and related proteins
Antithrombin; AT 1q25.1 Is the most important inhibitor of thrombin
Protein S; PROS1 3q11.1 Inhibits blood clotting
Coagulation factor V;
F5 1q24.2 Acts as a cofactor for the
conversion of prothrombin to thrombin by factor Xa
Coagulation factor XI;
F11 4q35.2
It participates in blood coagulation as a catalyst in the conversion of factor IX to factor IXa in the presence of calcium
ions
Plasminogen; PLG 6q26 Induces plasmin production (leads to fibrinolysis)
Plasminogen activator
inhibitor 1; PAI1 7q22.1 Regulation of plasmin production
Alpha-2-plasmin
inhibitor 17p13.3 Inactivation of plasmin
Fibrinolytic factors and related proteins
Osteonectin; ON 5q33.1 Inhibits cell-cycle progression
and influences the synthesis of extracellular matrix (ECM)
Histidine-rich
glycoprotein; HRG 3q27.3 Interacts with heparin and thrombospondin
Thrombin-activatable fibrinolysis inhibitor;
TAFI 13q14.13 Attenuates fibrinolysis
Alpha-2-
Macroglobulin; A2M 12p13.31 Carrier of specific growth factors and induces cell
signaling
22
Tissue inhibitor of metalloproteinase 4;
TIMP4 3p25.2
Inhibits matrix metalloproteinases (MMPs), a group of peptidases involved in degradation of the extracellular
matrix
Complement component 1
inhibitor; C1NH 11q12.1
Inhibits serine proteinases including plasmin, kallikrein,
and coagulation factors XIa and XIIa
Proteases and antiproteases
Alpha-1-antitrypsin (serpin peptidase
inhibitor) 14q32.13
Acute phase protein, inhibits a wide variety of proteases and
enzymes
Nexin 2; SNX2 5q23.2 Modulates intracellular trafficking of proteins to
various organelles
Platelet factor 4; PF4 4q13.3 Inhibition of angiogenesis
Basic proteins β-thromboglobulin (Pro-platelet basic
protein; PPBP) 4q13.3 Platelet activation, inhibition of
angiogenesis
Endostatin (Collagen, type XVIII, Alpha-1;
COL18A1) 21q22.3 Inhibitors of endothelial cell
migration and angiogenesis
Fibrinogen; FG 4q31.3 Blood clotting cascade (fibrin clot formation)
Fibronectin; FN 2q35
Binds to cell-surface integrins, affecting cell adhesion, cell
growth, migration, and differentiation
Adhesive proteins Vitronectin; VTN 17q11.2 Induces cell adhesion,
chemotaxis
Thrombospondin I;
THBS1 15q14 Inhibition of angiogenesis
Laminin-8 18p11.31-p11.23
Modulates cell contact interactions
Table 3: Some bioactive peptides present in the alpha granules of platelets. (63)

23
Among bioactive molecules stored and released from platelets dense granules are
catecholamines, histamine, serotonin, ADP, ATP, calcium ions, and dopamine, which are
active in vasoconstriction, increased capillary permeability, attract and activate
macrophages, tissue modulation and regeneration. These non-GF molecules have
fundamental effects on the biologic aspects of wound healing (65).
For their numerous functions, platelets have developed a set of platelet receptors that
are the contact between platelets and their surroundings; they determine the reactivity
of platelets with a wide range of agonists and adhesive proteins. Some of these
receptors are expressed only on activated platelets (60). Certain biological mechanisms
present in the platelets are shared with other cells, and therefore they contain some
common cytoplasmic enzymes, signal transduction molecules, and cytoskeletal
components (62).
The platelet lifespan is approximately 7 to 9 days, which they spend circulating in the
blood in their resting form. When adhered to exposed endothelium or activated by
agonists, they change their shape and secrete the contents of the granules (including
ADP, fibrinogen, and serotonin), which is followed by platelet aggregation (66). Initiation
of the signaling event within the platelet leads to the reorganization of the platelet
cytoskeleton, which is visible as an extremely rapid shape change (67).
24
5.2. Platelet Rich Plasma (PRP): Definition.
PRP has been used clinically in humans since the 1970s for its healing properties attributed of autologous GF and secretory proteins that may enhance the healing process on a cellular level (68). Furthermore, PRP enhances the recruitment, proliferation, and differentiation of cells involved in tissue regeneration (69). PRP-related products, also known as platelet-rich concentrate, platelet gel, preparation rich in growth factors (PRGF), and platelet releasate, have been studied with in vitro and in vivo experiments in the fields of surgical sciences mainly (70).
Platelets are activated either by adhesion to the molecules that are exposed on an injured endothelium, such as von Willebrand Factor (vWF), collagen, fibronectin, and laminin, or by physiologic agonists such as thrombin, ADP, collagen, thromboxane A2, epinephrine, and platelet-activating factors (71). Depending on the device and technique used, PRP can contain variable amounts of plasma, erythrocytes, white blood cells, and platelets. The platelet concentration should be increased above baseline or whole blood concentration. It is generally agreed upon that PRP should have a minimum of 5 times the number of platelets compared to baseline values for whole blood to be considered “platelet rich” (72). This conclusion is supported by in vitro work showing a positive dose-response relationship between platelet concentration and proliferation of human mesenchymal stem cells, proliferation of fibroblasts, and production of type I collagen (73). This suggests that the application of autologous PRP can enhance wound healing, as has been demonstrated in controlled animal studies for both soft and hard tissues (74, 75).
25
Autologous PRP represents an efficacious treatment for its use in wound healing like chronic diabetic foot ulceration due to multiple growth factors, is safe for its autologous nature, and is produced as needed from patient blood. Like we said, key for self-regeneration (76). Upon activation, platelets release their granular contents into the surrounding environment. The platelet alpha granules are abundant and contain many of the GFs responsible for the initiation and maintenance of the healing response (62). These GFs have been shown to play an important role in all phases of healing. The active secretion of these proteins by platelets begins within 10 minutes after clotting, with more than 95% of the presynthesized GFs secreted within 1 hour. After this initial burst, the platelets synthesize and secrete additional proteins for the balance of their life (5–10 days) (77). The fibrin matrix formed following platelet activation also has a stimulatory effect on wound healing. The fibrin matrix forms by polymerization of plasma fibrinogen following either external activation with calcium or thrombin or internal activation with endogenous tissue thromboplastin(73). This matrix traps platelets allowing a slow release of a natural combination of GF while providing a provisional matrix that provides a physical framework for wound stem cells and fibroblast migration and presentation of other biological mediators such as adhesive glycoproteins (78, 79) PRP with a platelet concentration of at least 1 000 000 platelets/μL in 5 mL of plasma is associated with the enhancement of healing (80). PRP can potentially enhance healing by the delivery of various GF and cytokines from the alpha granules contained in platelets and has an 8-fold increase in GF concentrations compared with that of whole blood (81).
26
The use of PRP to enhance bone regeneration and soft tissue maturation has increased dramatically in the fields of orthopedics, periodontics, maxillofacial surgery, urology, and plastic surgery over the last years. However, controversies exist in the literature regarding the added benefit of this procedure. While some authors have reported significant increases in bone formation and maturation rates (70), others did not observe any improvement (82). The wound-healing process is a complex mechanism characterized by four distinct, but overlapping, phases: hemostasis, inflammation, proliferation, and remodeling (83). The proliferative phase includes blood vessel formation by endothelial cells and bone synthesis by osteoblasts. All these events are coordinated by cell-cell interactions and by soluble GF released by various cell types. Recent reviews have emphasized the need for additional research aiming to characterize PRP in terms of GF content and their physiological roles in wound healing (84-86) Thrombin represents a strong inducer of platelet activation leading to GF release (87). It is also known that particulate grafts, when combined with calcium and thrombin treated PRP, possess better handling characteristics and higher GF content (82). Typically, thrombin concentrations used in clinical applications vary between 100 and 200 units per mL (70), while platelet aggregation is maximum in the range of 0.5 to 4 units per mL (88). The basic cytokines identified in platelets play important roles in cell proliferation, chemotaxis, cell differentiation, regeneration, and angiogenesis (79).A particular value of PRP is that these native cytokines are all present in “normal” biologic ratios. The platelets in PRP are delivered in a clot, which contains several cell adhesion molecules including fibronectin, fibrin, and vitronectin. These cell adhesion molecules play a role in cell migration and thus also add to the potential biologic activity of PRP. The clot itself can also play a role in wound healing by acting as conductive matrix or “scaffold” upon which cells can adhere and begin the wound-healing process (79).
27
PRP can only be made from anticoagulated blood. Preparation of PRP begins by addition of citrate to whole blood to bind the ionized calcium and inhibit the clotting cascade (63). This is followed by one or two centrifugation steps. The first centrifugation step separates the red and white blood cells from plasma and platelets. The second centrifugation step further concentrates the platelets, producing the PRP separate from platelet-poor plasma (68). An important point is that clotting leads to platelet activation, resulting in release of the GF from the alpha granules, otherwise known as degranulation. Approximately 70% of the stored GFs are released within 10 minutes, and nearly 100% of the GFs are released within 1 hour. Small amounts of GF may continue to be produced by the platelet during the rest of its lifespan (1 week) (70). A method to delay the release of GF is possible by addition of calcium chloride (CaCl2) to initiate the formation of autogenous thrombin from prothrombin. The CaCl2 is added during the second centrifugation step and results in formation of a dense fibrin matrix. Intact platelets are subsequently trapped in the fibrin matrix and release GF slowly over a 7-day period. The fibrin matrix itself may also contribute to healing by providing a conductive scaffold for cell migration and new matrix formation (78).
28
5.3. Platelet Rich Plasma (PRP): Growth Factors.
Platelets are known to contain high concentrations of different GF and are extremely
important in regenerative process; activation of the platelet by endothelial injury
initiates the wound-healing process (89). When platelets are activated, their alpha
granules are released, resulting in an increased concentration of GF in the wound milieu
(90).
There is increasing evidence that the platelet cell membranes themselves also play a
crucial role in wound healing through their GF receptor sites (77). GFs are found in a
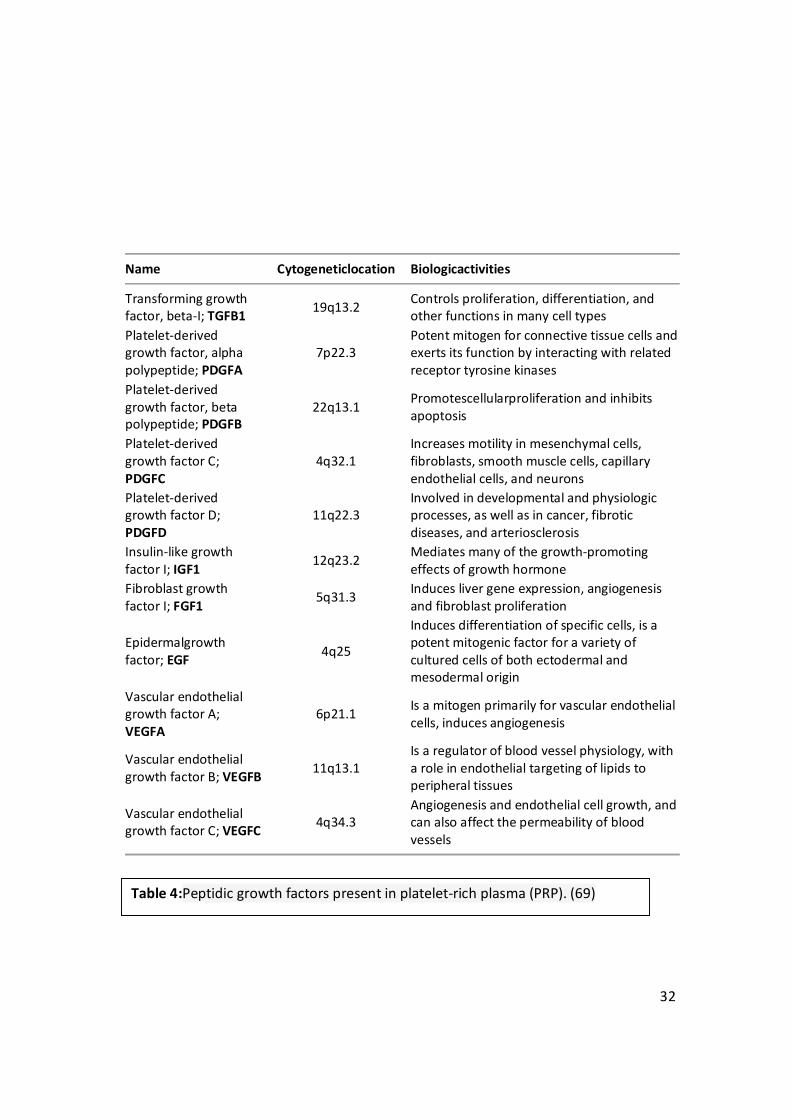
wide array of cells and in platelet alpha granules (68). Table 4 gives an overview of some
of the more extensively studied GFs and their involvement in wound healing. There are
many more, both discovered and undiscovered, GFs. The platelet is an extremely
important cell in wound healing because it initiates and plays a major role in the wound
regenerative process (69).
The first discovered GF was EGF in 1962 by Cohen (70). It was not until 1989 before
clinical trials with EGF were attempted to demonstrate enhanced wound healing.
Studies did demonstrate that EGF can accelerate epidermal regeneration and enhance
healing of chronic wounds (72).

29
PDGF was discovered in 1974 and is ubiquitous in the body. It is known to be released
by platelet alpha granules during wound healing and stimulate the proliferation of many
cells, including connective tissue cells. In fact, thus far, high-affinity cell-surface
receptors specific for PDGF have only been demonstrated on connective tissue cells.
When released, PDGF is chemotactic for monocytes, neutrophils, and fibroblasts. These
cells release their own PDGF, thus creating a positive autocrine feedback loop (73).
Other functions of PDGF include effects on cell growth, cellular migration, metabolic
effects, and modulation of cell membrane receptors (74).
PDGFs were first identified as products of platelets which stimulated the proliferation in
vitro of connective tissue cell types such as fibroblasts (75).
The PDGF system, comprising four isoforms (PDGF-A, -B, -C, and -D) and two receptor
chains (PDGFR-alpha and -beta), plays important roles in wound healing,
atherosclerosis, fibrosis, and malignancy. Components of the system are expressed
constitutively or inducibly in most renal cells (74). They regulate a multitude of
pathophysiologic events, ranging from cell proliferation and migration to extracellular
matrix accumulation, production of pro- and anti-inflammatory mediators, tissue
permeability, and regulation of hemodynamics (75).
Inactivation of PDGF-B and PDGF beta receptor (PDGFRb) genes by homologous
recombination in embryonic stem cells shows cardiovascular, hematological, and renal
defects. The latter is particularly interesting since it consists of a specific cellular defect:
the complete loss of kidney glomerular mesangial cells and the absence of urine
collection in the urinary bladder (75).
30
PDGF-C and PDGFR-alpha contribute to the formation of the renal cortical interstitium.
Almost all experimental and human renal diseases are characterized by altered
expression of components of the PDGF system. Infusion or systemic overexpression of
PDGF-B or -D induces prominent mesangioproliferative changes and renal fibrosis.
Intervention studies identified PDGF-C as a mediator of renal interstitial fibrosis and
PDGF-B and -D as key factors involved in mesangioproliferative disease and renal
interstitial fibrosis (75, 76).
Fréchette et al., demonstrated that the release of PDGF-B, TGF-beta1, bFGF, and VEGF is
significantly regulated by the amount of calcium and thrombin added to the PRP and
that PRP supernatants are more mitogenic for endothelial cells than whole-blood
supernatants (91). Other GFs such as epidermal growth factor (EGF), transforming
growth factor-alpha (TGF-alpha), insulin-like growth factor-1 (IGF-1), angiopoietin-2
(Ang-2), and interleukin-1beta (IL-1beta) are also known to play important roles in the
wound-healing process (77).

31
In 2008, Wahlström et al., demonstrated that growth factors released from platelets
had potent effects on fracture and wound healing. The acidic tide of wound healing,
that is, the pH within wounds and fractures, changes from acidic pH to neutral and
alkaline pH as the healing process progresses (76). They investigated the influence of pH
on lysed platelet concentrates regarding the release of growth factors. The platelet
concentrates free of leukocyte components were lysed and incubated in buffers with pH
between 4.3 and 8.6. Bone morphogenetic protein-2 (BMP-2), platelet-derived growth
factor (PDGF), transforming growth factor-beta (TGF-beta), and vascular endothelial
growth factor (VEGF) were measured by quantitative enzyme-linked immunosorbent
assays. BMP-2 was only detected in the most acidic preparation (pH 4.3), which is
interesting since BMP-2 has been reported to be an endogenous mediator of fracture
repair and to be responsible for the initiation of fracture healing. These findings indicate
that platelets release substantial amounts of BMP-2 only under conditions of low pH,
the milieu associated with the critical initial stage of fracture healing (76).
Recently, Bir et al., demonstrated stromal cell-derived factor 1-α (SDF-1α) PRP from
diabetic mice. The concentration (pg/mL) of different growth factors was significantly
higher in the PRP group than in the platelet-poor plasma (PPP) group. The
concentrations (pg/mL) of SDF-1α (10,790 ± 196 versus 810 ± 39), PDGF-BB (45,352 ±
2,698 versus 958 ± 251), VEGF (53 ± 6 versus 30 ± 2), bFGF (29 ± 5 versus 9 ± 5), and IGF-
1 (20,628 ± 1,180 versus 1,214 ± 36) were significantly higher in the PRP group than in
the PPP group, respectively (79).
32
Name Cytogeneticlocation Biologicactivities
Transforming growth factor, beta-I; TGFB1 19q13.2 Controls proliferation, differentiation, and
other functions in many cell types Platelet-derived growth factor, alpha polypeptide; PDGFA
7p22.3 Potent mitogen for connective tissue cells and exerts its function by interacting with related receptor tyrosine kinases
Platelet-derived growth factor, beta polypeptide; PDGFB
22q13.1 Promotescellularproliferation and inhibits apoptosis
Platelet-derived growth factor C; PDGFC
4q32.1 Increases motility in mesenchymal cells, fibroblasts, smooth muscle cells, capillary endothelial cells, and neurons
Platelet-derived growth factor D; PDGFD
11q22.3 Involved in developmental and physiologic processes, as well as in cancer, fibrotic diseases, and arteriosclerosis
Insulin-like growth factor I; IGF1 12q23.2 Mediates many of the growth-promoting
effects of growth hormone Fibroblast growth factor I; FGF1 5q31.3 Induces liver gene expression, angiogenesis
and fibroblast proliferation
Epidermalgrowth factor; EGF 4q25
Induces differentiation of specific cells, is a potent mitogenic factor for a variety of cultured cells of both ectodermal and mesodermal origin
Vascular endothelial growth factor A; VEGFA
6p21.1 Is a mitogen primarily for vascular endothelial cells, induces angiogenesis
Vascular endothelial growth factor B; VEGFB 11q13.1
Is a regulator of blood vessel physiology, with a role in endothelial targeting of lipids to peripheral tissues
Vascular endothelial growth factor C; VEGFC 4q34.3
Angiogenesis and endothelial cell growth, and can also affect the permeability of blood vessels
Table 4:Peptidic growth factors present in platelet-rich plasma (PRP). (69)

33
5.4. Platelet Rich Plasma (PRP): Mechanism of Action.
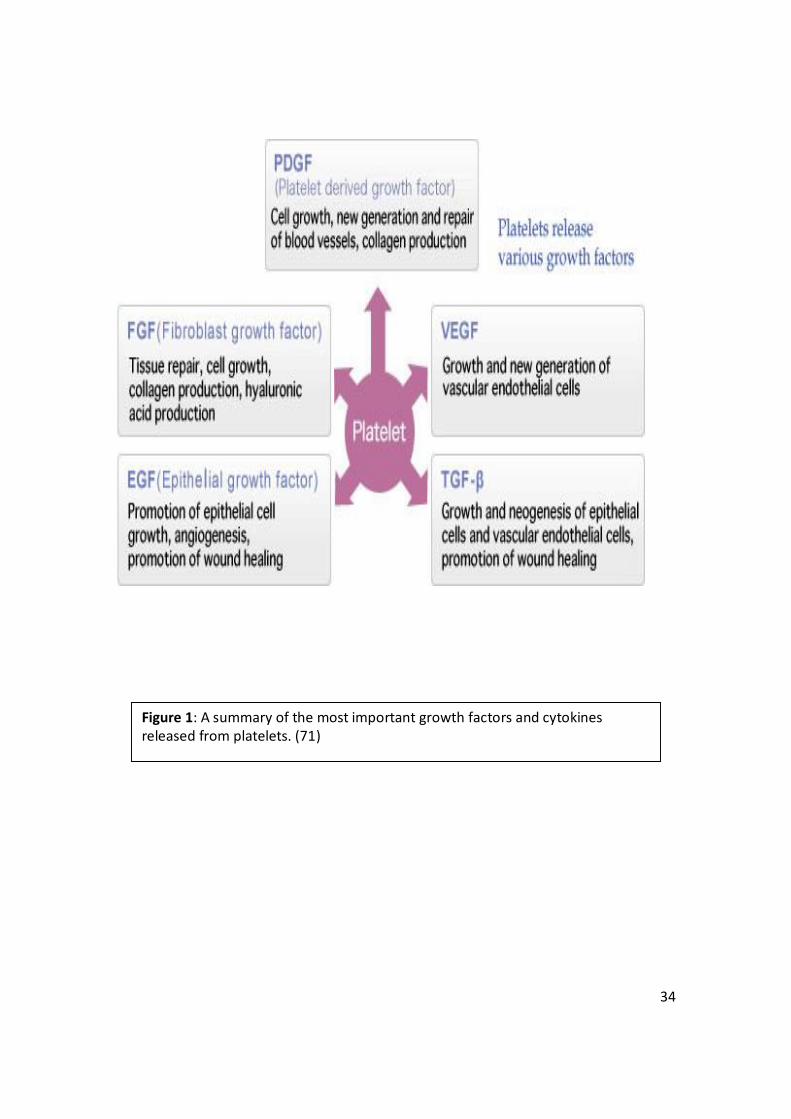
PRP can potentially enhance healing process of musculoskeletal tissue by the delivery of
various growth factors and cytokines from the α-granules contained in platelets figure
1(71).
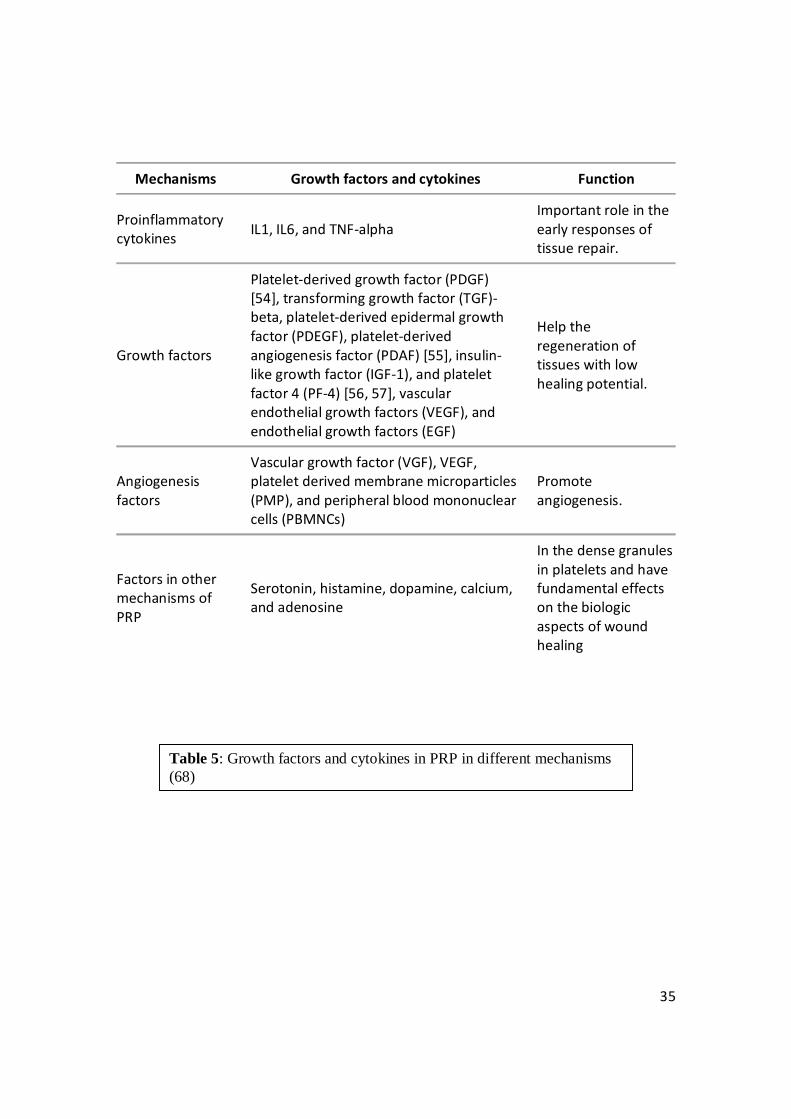
The basic cytokines,Table 5, which identified platelets, play important roles in cell
proliferation, chemotaxis, cell differentiation, and angiogenesis. Bioactive factors are
also contained in the dense granules in platelets. The dense granules contain serotonin,
histamine, dopamine, calcium, and adenosine (68). These nongrowth factors have
fundamental effects on the biologic aspects of wound healing.
34
Figure 1: A summary of the most important growth factors and cytokines released from platelets. (71)
35
Mechanisms Growth factors and cytokines Function
Proinflammatory cytokines IL1, IL6, and TNF-alpha
Important role in the early responses of tissue repair.
Growth factors
Platelet-derived growth factor (PDGF) [54], transforming growth factor (TGF)-beta, platelet-derived epidermal growth factor (PDEGF), platelet-derived angiogenesis factor (PDAF) [55], insulin-like growth factor (IGF-1), and platelet factor 4 (PF-4) [56, 57], vascular endothelial growth factors (VEGF), and endothelial growth factors (EGF)
Help the regeneration of tissues with low healing potential.
Angiogenesis factors
Vascular growth factor (VGF), VEGF, platelet derived membrane microparticles (PMP), and peripheral blood mononuclear cells (PBMNCs)
Promote angiogenesis.
Factors in other mechanisms of PRP
Serotonin, histamine, dopamine, calcium, and adenosine
In the dense granules in platelets and have fundamental effects on the biologic aspects of wound healing
Table 5: Growth factors and cytokines in PRP in different mechanisms (68)
36
Platelet concentration is a rich source of various cytokines and growth factors, which are activated after its injection into the target tissue. Platelets are activated endogenously by coagulation factors (in some methods of preparing PRP, the activated PRP is injected to the tissue). Following their attachment to special receptors on the cell surfaces, some intracellular processes are activated, that facilitate extracellular matrix (ECM) accumulation and improve cell proliferation and differentiation. Tissue regeneration is resulted from cell proliferation, angiogenesis and cell migration (92, 93). Matrix metaloproteinas proteins (MMP) are involved in aging process by degradation of collagen and other extracellular matrix (ECM) proteins (94), this characteristic can be used to benefit rejuvenation. They can help regeneration of dermis through omission of collagen fragments that are harmful to the dermal connective tissue, and so, provide an appropriate foundation for new collagen deposition (94). In some studies aPRP (activated PRP) increases the expression of MMP-1 and MMP-3 protein. Thus, aPRP may cause ECM remodeling through stimulating the removal of photo-damaged ECM components and inducing the synthesis of new collagen by fibroblasts, which are in turn proliferated by their stimulation (95). Another study showed that high concentration of PRP increased type I collagen, MMP-1 and MMP-2 expression in human skin fibroblasts (96). In addition to above mechanisms, improving aging skin through PRP which is a dose–response relationship has been recognized between concentrated platelet and mesenchymal stem cell proliferation (97).
37
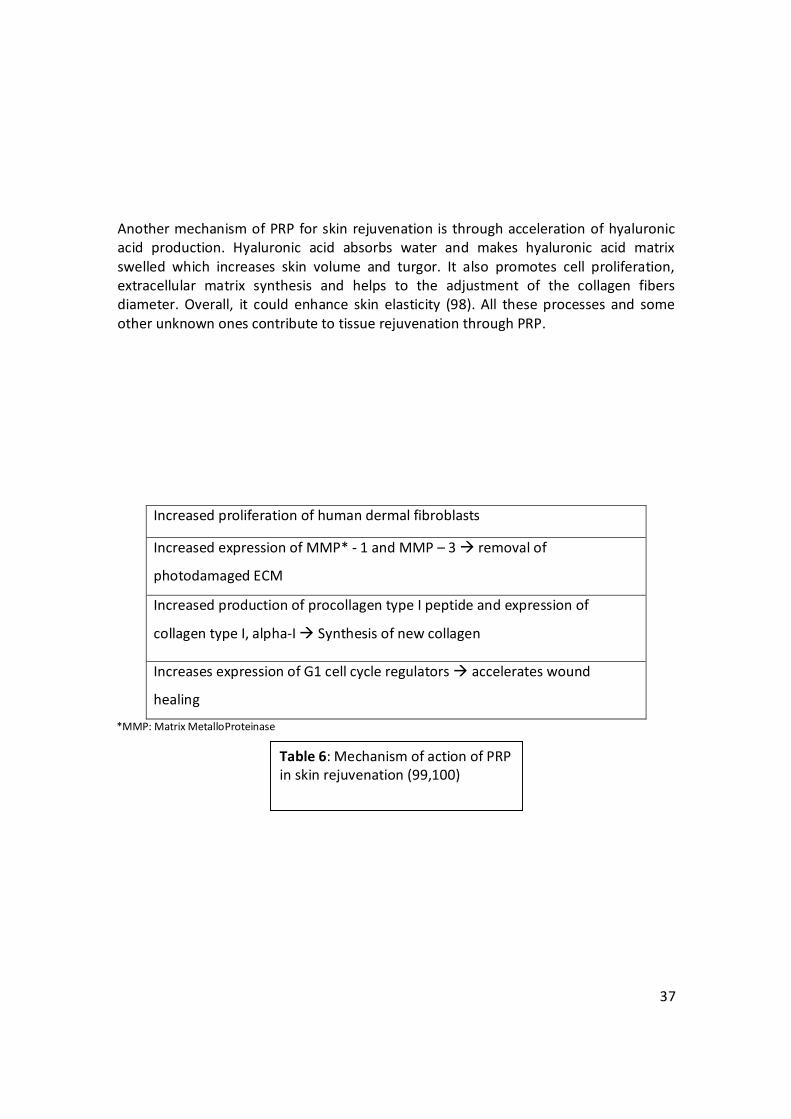
Another mechanism of PRP for skin rejuvenation is through acceleration of hyaluronic acid production. Hyaluronic acid absorbs water and makes hyaluronic acid matrix swelled which increases skin volume and turgor. It also promotes cell proliferation, extracellular matrix synthesis and helps to the adjustment of the collagen fibers diameter. Overall, it could enhance skin elasticity (98). All these processes and some other unknown ones contribute to tissue rejuvenation through PRP.
*MMP: Matrix MetalloProteinase
Increased proliferation of human dermal fibroblasts
Increased expression of MMP* - 1 and MMP – 3 à removal of
photodamaged ECM
Increased production of procollagen type I peptide and expression of
collagen type I, alpha-I à Synthesis of new collagen
Increases expression of G1 cell cycle regulators à accelerates wound
healing
Table 6: Mechanism of action of PRP in skin rejuvenation (99,100)

38
5.4. Platelet Rich Plasma (PRP): Obtaining and Injection PRP.
BLOOD COLLECTION
As your own (autologous) blood is used, it is first collected
by venesection, the same procedure used in blood tests or
blood donations.
The site of the venesection is usually a large vein in your
elbow. Up to 20 ml of blood may be collected. (4 tubes of
5ml)
39
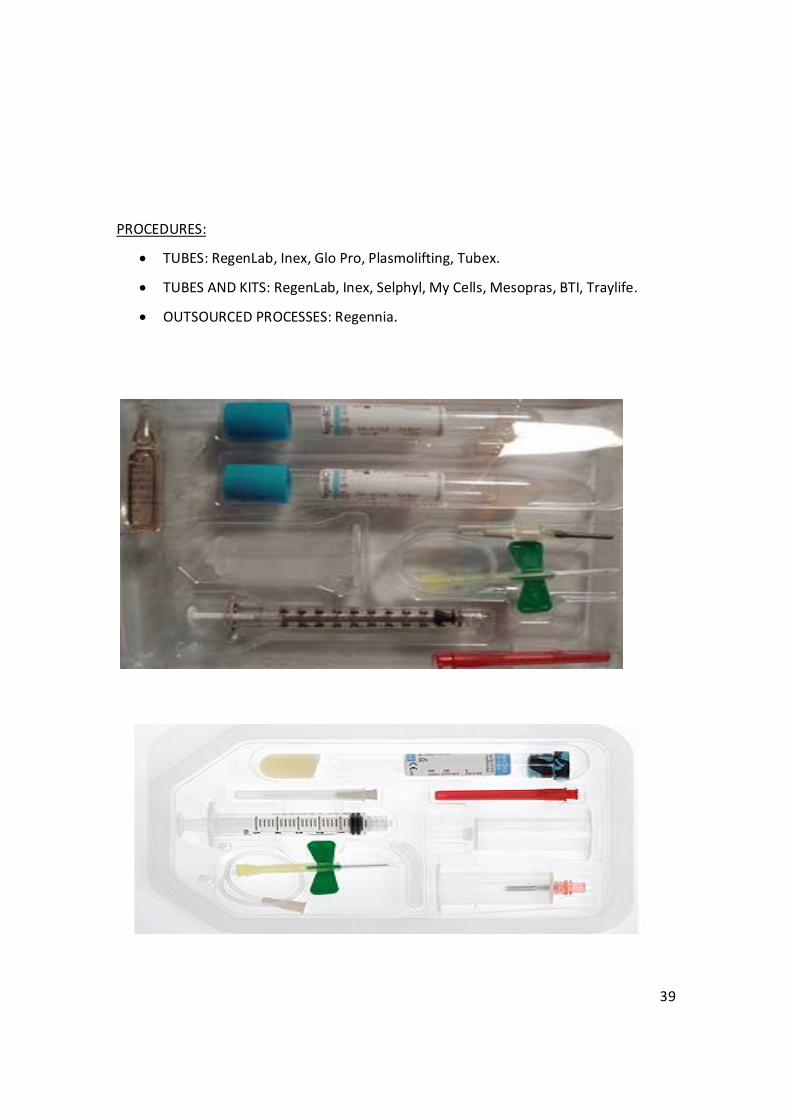
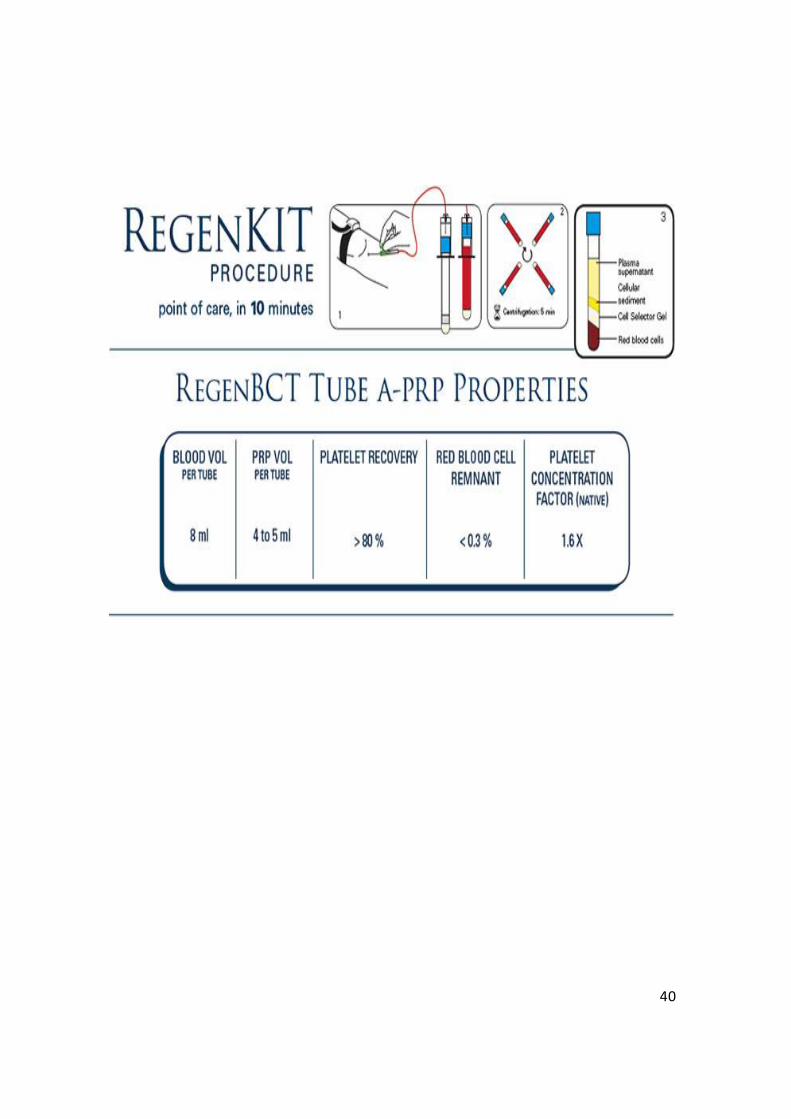
PROCEDURES:
• TUBES: RegenLab, Inex, Glo Pro, Plasmolifting, Tubex.
• TUBES AND KITS: RegenLab, Inex, Selphyl, My Cells, Mesopras, BTI, Traylife.
• OUTSOURCED PROCESSES: Regennia.
40
41
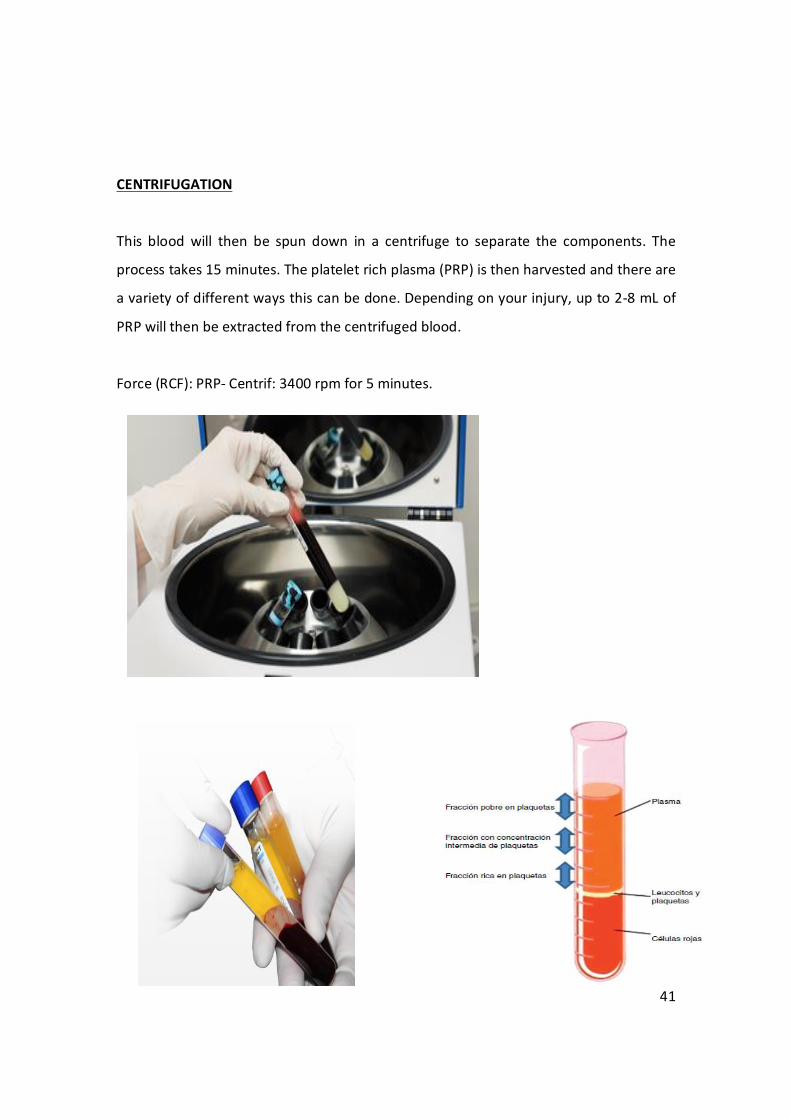
CENTRIFUGATION
This blood will then be spun down in a centrifuge to separate the components. The
process takes 15 minutes. The platelet rich plasma (PRP) is then harvested and there are
a variety of different ways this can be done. Depending on your injury, up to 2-8 mL of
PRP will then be extracted from the centrifuged blood.
Force (RCF): PRP- Centrif: 3400 rpm for 5 minutes.
42
In the centrifugation tube 4 levels are obtained:
I. Deeper, sediment area, rich in erythrocytes and leukocytes. Should be discarded.
II. Zone platelet rich plasma (PRP)
III. Zone normal platelet in plasma. Should be discarded.
IV. Zone platelet poor plasma rich in fibrin
THE INJECTION
1) The patient is placed in an appropriate and comfortable position that allows for
sterility and access to the site of injection.
2) All necessary materials for the injection (PRP, additives, 4X4s, needles, US gel) should
have been planned and placed on a sterile table adjacent and easily accessible to the
physician.
3) The patient’s skin is cleansed appropriately and towels or drapes may be used to
create an aseptic field.
4) If local anesthetic will be used, it is to be applied with aseptic technique for 30 minutes before the procedure.
5) Injection is done with nappage technique, same as in mesotherapy.
43
6. Objectives.
To understand the process of aging, its causes and to emphasis on the role of
photoaging/extrinsic aging in wrinkled aged looking skin.
Toinvestigate the evidence concerning the management and use of PRP as an antiaging
mechanism in facial rejuvenation.
To Research the benefits of using PRP in Aesthetic Medicine.
To establish therapeutic uses and effects of PRP in skin rejuvenation, skin aging and
decrease wrinkles, fine lines and over all skin appearance.
7. Materials and Methods.
Articles and publications have been selected and revised. These have been mainly chosen from PubMed, Medical journals like the New England Journal of Medicine.
High-impact articles, literature, meta-analysis, medical reviews and randomized case-
control studies with standardized measures and statistically significant results that were
currently in place were included.
The revised articles mainly have been chosen from the year 2002 up to this current year.
Articles that were not in English or Spanish were excluded for the review of the uses of
PRP in skin rejuvenation.
44
8. Results.
The use of PRP in dermatology has taken on new meaning over the past few years,
research on. All studies on this topic vary in their methodology in one way or another;
however, the similarity lies in the results. All show the beneficial effects of PRP on
wound repair, differentiation and proliferation of adipose precursor cells, and
angiogenesis
Applications of PRP such as acne scars, fat grafting, wound healing, wrinkling around the
eyes, facial rejuvenation and hair regrowth have plenty of publications to boost about.
Newer combinations therapies such as PRP with carbon dioxide fractional lasers for acne
scars or microneedling for skin tightening effect.
Despite these abundant studies in various reviewed journals, we await evidence-based
data regarding the exact concentration and dosing parameters. All the studies are
conducted with different methodology. Questions such as, when to inject PRP? Will PRP
work better if injected weekly, daily, or monthly? For how long post procedure? Still
boggle the mind. For now, all we have are arbitrary guidelines. Instead of being helpful
and encouraging, these studies can often be confusing and misguiding to a doctor
planning to inculcate PRP in his daily practice. These unanswered questions, plus the
time and cost of equipment setup, are obstacles to widespread implementation of PRP.
It is undoubtable that the use of platelet-based formulations in cutaneous medicine will
continue to evolve. Hence to use PRP to the fullest extent, the principles, procedure and
indications need to be understood, standardized and simplified; only then, we can trust
this procedure completely and give maximum benefit to our patients.
45
9. PRPin Facial Rejuvenation: Review and Evaluation of Clinical Studies.
EVIDENCE TO SUPPORT ITS USE
Monthly intradermal injections of PRP in 3 sessions have shown satisfactory results in
face and neck rejuvenation and scar attenuation. (101)Shin et al.,(102) showed that a
combination of fractional non-ablative (erbium glass) laser therapy with topical
application of PRP, resulted in objective improvement in skin elasticity, a lower
erythema index and an increase in collagen density as well. Histological examination
showed an increase in length of dermoepidermal junction, amount of collagen and
fibroblasts in the treated skin.
PRP in combination with fractional ablative lasers (carbon dioxide) for deep wrinkles and
severe photodamaged skin, has also been shown to reduce commonly encountered,
transient adverse effects and decrease the downtime.(103)In a split face blinded trial,
PRP injections given monthly for 3 months, have shown good results for infraorbital
rejuvenation as well, without any obvious side effects.(104)
As varied number of products are available nowadays for skin rejuvenation like
mesotherapy solutions, adipose derived stem cells etc., whether PRP can be used in
combination with them to boost the aesthetic results, needs further clinical trials. Also,
comparative studies are lacking to contrast PRP with other treatments like topical
cosmeceutical preparations of growth factors, to be used after fractional laser
resurfacing.
46
SCARS AND CONTOUR DEFECTS
PRP has become a promising modality among soft tissue augmentation techniques.
PRFM has been used as a filler to correct deep nasolabial folds without any adverse
effects. (105)
As an adjuvant, it has been studied with autologous fat transfer procedures. An in
vitro pilot study, revealed that fat grafts when mixed with PRP resulted in greater
vascularity, fewer cysts and vacuoles, less fibrosis and overall improved survival and
quality of fat grafts as compared to saline.(106)This novel regimen was found to
maintain fat graft survival in a patient with facial contour defect for upto 2
years.(107)Data suggests that fat grafts can be admixed with PRP in treating traumatic
scars, and further can be followed by fractional laser resurfacing to give best
results.(108)
PRP injections in combination with fractional carbon dioxide resurfacing have shown
good results in acne scar resurfacing also, apart from skin rejuvenation. (109)
47
Role of Growth factors in skin healing
1. IN VITRO STUDIES
Knowledge of GF and their function is far from complete. Many of the known functions
were learned through in vitro study. Although many GFs are associated with wound
healing, PDGF and TGF-β1 appear to be two of the more integral modulators (110).
PDGF has activity in early wound healing (during the acid tide). In vitro studies have
shown that at lower pH (5.0), platelet concentrate lysate has increased concentrations
of PDGF, with an increased capacity to stimulate fibroblast proliferation (73). TGF-β
increases the production of collagen from fibroblasts (110)its release in vitro is
enhanced by neutral or alkaline pH, which correspond to the later phases of healing
(77).
Through modulation of interleukin-1 production by macrophages, PRP may inhibit
excessive early inflammation that could lead to dense scar tissue formation (111).
Insulin-like GF-I (IGF-1) has also been extensively studied for its ability to induce
proliferation, differentiation, and hypertrophy of multiple cell lines. Separate analyses of
GF in PRP have shown significant increases in PDGF, VEGF, TGF-β1, and EGF, compared
with their concentrations in whole blood (63,112)

48
IGF-1 has two important functions: chemotaxis for vascular endothelial cells into the
wound which results in angiogenesis and promoting differentiation of several cell lines
including chondroblasts, myoblasts, osteoblasts, and hematopoietic cells .(113)
TGF-β is a member of the newest family of proteins discovered. Two major sources of
this protein are the platelet and macrophage. TGF-β causes chemotactic attraction and
activation of monocytes, macrophages, and fibroblasts. The activated fibroblasts
enhance the formation of extracellular matrix and collagen and also stimulate the cells
ability to contract the provisional wound matrix (114). Macrophages infiltration
promotes TGF-β that induces extracellular matrix such as collagen and fibronectin;
however alpha-mangostin prevents the increase in this molecule in rats with Cisplatin-
induced nephrotoxicity (115).
2. IN VIVO STUDIES
In vivo study is much more complex due to the inability to control the environment. A
further complexing matter is the fact that the same GF, depending on the presence or
absence of other peptides, may display either stimulatory or inhibitory activity within
the same cell. Also, a particular GF can alter the binding affinity of another GF receptor
(116).
49
Release of PDGF can have a chemotactic effect on monocytes, neutrophils, fibroblasts,
stem cells, and osteoblasts. This peptide is a potent mitogen for mesenchymal cells
including fibroblasts, smooth muscle cells and glial cells (117) and is involved in all three
phases of wound healing, including angiogenesis, formation of fibrous tissue, and
reepithelialization.
TGF beta released from platelet alpha granules is a mitogen for fibroblasts, smooth
muscle cells, and osteoblasts. In addition, it promotes angiogenesis and extracellular
matrix production [59]. VEGF promotes angiogenesis and can promote healing of
chronic wounds and aid in endochondral ossification. EGF, another platelet-contained
GF, is a mitogen for fibroblasts, endothelial cells, and keratinocytes and also is useful in
healing chronic wounds (118).
IGF, another platelet-contained GF regulates bone maintenance and is also an important
modulator of cell apoptosis, and, in combination with PDGF, can promote bone
regeneration (119).
However, there are conflicting results with regard to IGF-1, where the majority of
studies reported no increase in IGF-1 in PRP, compared with whole blood. There are also
conflicting results regarding the correlation between the GF content and platelet counts
in PRP (120).The basis of these contradictions is not fully understood and may be related
to variability in patient age, health status, or platelet count.
50
Alternatively, differences in GF content and platelet count may be due to the various
methods of processing, handling, and storing of samples, in addition to the type of assay
performed. The diversity of PRP products should be taken into account when
interpreting and comparing results and methods for generating PRP (77).
VEGF, discovered 25 years ago, was initially referred to as vascular permeability factor
(121). In mammals, there are at least four members of the VEGF family: VEGF-A, VEGF-
B, and the VEGF-C/VEGF-D pair, which has a common receptor, VEGF receptor 3 (VEGF-
R3) (122). VEGF-A is a proangiogenic cytokine during embryogenesis and contributes to
vascular integrity: selective knockout of VEGF-A in endothelial cells increases apoptosis,
which compromises the integrity of the junctions between endothelial cells (123,124)
VEGF-B, which can form heterodimers with VEGF-A, occurs predominantly in brown fat,
myocardium, and skeletal muscle (125).VEGF-C and VEGF-D seem to regulate
lymphangiogenesis.
The expression of VEGF-R3 in adults is restricted to the lymphatics and fenestrated
endothelium (126). Neuropilin 1 and neuropilin 2 are receptors that bind specific VEGF
family members and are important in neuronal development and embryonic
vasculogenesis (127).
51
Megakaryocytes and platelets contain the three major isoforms of VEGF-A; after
exposure to thrombin in vitro, they release VEGF-A (128-131) VEGF-A alters the
endothelial-cell phenotype by markedly increasing vascular permeability, upregulating
expression of urokinase, tissue plasminogen activator, connexin, osteopontin, and the
vascular-cell adhesion molecule (132).
10. PRP in Cell Therapy and Regenerative Medicine.
PRP can be combined with cell-based therapies such as adipose-derived stem cells,
regenerative cell therapy, and transfer factors therapy (133).While this is a relatively
new concept, the strategy is appealing as the regenerative matrix graft delivers a potent
trilogy of regenerative cells, fibrin matrix, and GF (63) The applications are similar to
those for PRP alone with the added benefit of regenerative cell enrichment.
Verrier et al., demonstrated that cultures of human mesenchymal stem cell (MSC)
supplemented with platelet-released supernatant (PRS) had differentiation towards an
osteoblastic phenotype in vitro possibly mediated by bone morphogenetic protein-2
(BMP-2). PRS showed an osteoinductive effect on MSC, as shown by an increased
expression of typical osteoblastic marker genes such as collagen I, bone sialoprotein II,
BMP-2, and matrix metalloproteinase-13 (MMP-13), as well as by increased Ca++
incorporation (134)

52
Furthermore, the role of platelets in hemostasis may be influenced by alteration of the
platelet redox state, the presence of endogenous or exogenous antioxidants, and the
formation of reactive oxygen and nitrogen species (135). As discussed by Sobotková et
al., (135), trolox and resveratrol inhibit aggregation of washed platelets and PRP
activated by ADP, collagen, and thrombin receptor-activating peptide.
Antioxidants, apart from nonspecific redox or radical-quenching mechanisms, inhibit
platelet activation also by specific interaction with target proteins. In this context,
powerful natural antioxidants, like nordihydroguaiaretic acid (NDGA) extracted from
Larreatridentata (136), S-allylcysteine (SAC), the most abundant organosulfur compound
in aged garlic extract (AG) (137), sulforaphane (SFN), an isothiocyanate produced by the
enzymatic action of myrosinase on glucoraphanin, a glucosinolate contained in
cruciferous vegetables (138), and acetonic and methanolic extracts of
Heterothecainuloides, can be administered with ample safety margin in patients treated
with PRP (139).
53
11. Methods to Improve Patient Satisfaction. The evaluation is essentially subjective. 95% of patients are satisfied with the
improvements in the appearance, texture, softness, touch, tone, brightness, etc. The
results can be objectified to measure and compare the parameters, such as
corneometry, hygrometry or sebometria.
PRP can be combined with other skin rejuvenating procedures such as: mesotherapy,
microneedling, fillers, botulinum toxin injections, various peeling, fractionated laser
therapy and radiofrequency biostimulation. (140)
12. Complications of PRP.
After the procedure there will be some pain, mild swelling or redness, of the skin
following injection of the platelet rich plasma - PRP. Bruising is also a possibility as the
needle is used to place the PRP into the skin. This may take a week or so to resolve.
There can be side effects. Here are the most common: (141)
Pain in the Injured Area: Some people who’ve undergone PRP therapy complain about an acute ache or soreness in the spot of the injection. Sometimes this pain is even felt deep inside the area, whether in the muscle or bone.
54
Infection: As with any injection-based treatment, infection is a slight possibility regardless of thorough sterilization procedures.While a tremendous amount of precaution is taken when injecting a patient with a PRP serum–intense sterilization procedures are, in fact, followed closely for each treatment–sometimes an infection can break out in the injured area. No Improvement in Injured Area: While this is not necessarily a side-effect, we still
need to mention that not all athletes respond to a PRP injection. (Of course, this
particular type of sports medicine is undergoing more studies so we can understand
exactly why. Sometimes the original pain and soreness of the injury remains (it may even get worse), even after an extended rest period after the PRP therapy. Allergic Reaction: Some patients’ body will reject their own serum and react negatively to the treatment. This is rare, but it does happen. Again, more studies need to be done to understand why. Blood Clot: Normally, a blood clot forms when there is damage to the lining of a blood vessel, like with a cut. Because a PRP injection uses a needle (guided by a sonogram) there is a chance that a artery or vein could be damaged. If that happens a blood clot occurs and is treated like any normal clot. Skin Discoloration: Sometimes the color around the skin of a PRP injection will appear bruised. This could be normal, based upon your history of bruising.
55
13. CONTRAINDICATIONS TO PRP
Treatment with autologous PRP is generally considered safe in appropriately selected
patients. Potential candidates for treatment with PRP should undergo a pre-treatment
hematologic evaluation to rule out potential coagulopathies and disorders of platelet
function. (142)
Patients who are anemic and those with thrombocytopenia may be unsuitable
candidates for treatment whit PRP.
Other potential contraindications include hemodynamic instability, severe hypovolemia,
unstable angina, sepsis, and anticoagulant or fibrinolytic drug therapy. (143)
Absolute Contraindications:
• Platelet dysfunction syndrome
• Critical thrombocytopenia
• Hemodynamic instability
• Septicemia
• Local infection at the site of the procedure
• Patient unwilling to accept risks
56
Relative Contraindications:
• Consistent use of NSAIDs within 48 hours of procedure
• Corticosteroid injection at treatment site within 1 month
• Systemic use of coriticosteroids within 2 weeks
• Tobacco use
• Recent fever or illness
• Cancer- especially hematopoetic or of bone
• HGB < 10 g/dl
• Platelet count < 105/ul
14. Advantages, Limitations and Precautions.
PRP as autologous procedure eliminates secondary effects and unnecessary risks for
chemically processed strange molecules, is a natural reserve of various growth factors
that can be collected autologously, and is cost effective (144,145)
Thus for clinical use, no special considerations concerning antibody formation and
infection risk are needed. The key of our health and our own regeneration resides in our
own body. Nevertheless this treatment is not the panacea; it is only the beginning in this
new age of the regenerative medicine. Some clinical devices automatically prepare PRPs
are available at present.
57
15. Discussion. The problem of skin ageing has captured public attention and has an important social impact. Different therapeutic approaches have been developed to treat cutaneous ageing and to diminish or prevent the negative effects of UVR.
The primary factor that causes human skin aging is its direct contact with the environment; therefore, skin aging can be considered as a consequence of environmental damage. The most important environmental factor involved in human skin aging is ultraviolet (UV) irradiation from the sun. This sun-induced skin aging (photo-aging) depends primarily on the degree of sun exposure and skin pigment. Individuals who have outdoor lifestyles and those who are lightly pigmented will experience the greatest degree of photo-aging (127).
The deleterious effects of solar radiation on the skin impact primarily on the dermal connective tissue with accelerated breakdown and synthesis of collagen, and enhanced inflammatory processes. These processes are directly responsible for the clinical appearance of photo-aged skin: wrinkling, telangiectasia, laxity, pigment changes, coarseness, dehydration, and loss of tensile strength (128)
Intradermal injection of growth factors produced remarkable clinical changes on aging skin: restores skin vitality, increases the thickness of the skin, restores elastic consistency, improves vascular flow, stimulates secretions and improves the smoothness and appearance of the skin .The Growth factors regulate the remodeling of the epidermis and dermis, and have a great influence on the appearance and texture of the skin.

58
The PRP treatments can be used on all skin types and tones. Minimal swelling, bruising, and redness for the initial 12 to 24 hours are expected. A bruise at the needlestick site may be visible for 2 to 3 days up to a week. Swelling from the fluid is what the patient will notice first. During several weeks, the platelets stimulate growth factors, which assist in more collagen stimulation. Treatment results vary but last up to 18 months in most patients. Biannual touch-up treatments will maintain the results. As an initial treatment strategy, up to 4 sessions may be given. These are usually performed 2 to 4 weeks apart.
PRP is effective particularly for fine wrinkles under the eyes that are difficult to treat by conventional rejuvenation therapy. It is also effective for treating periorbital dark circles, wrinkles on the face and neck, acne scars, saggy skin, eye bags, and nasolabial folds.
59
16. CONCLUSION
Compared with other skin rejuvenation therapies, the clinical experience using Platelet
Rich Plasma (PRP) has demonstrated it to be a useful primary or adjunctive therapy for
the tissue rejuvenation.
Both superficial and deep dermal applications can result in skin rejuvenation and global
facial volumisation. PRP is a form of biostimulation that is safe and creates an
immediate, long lasting volumetric effect with natural looking results. The technique is
easy to perform and has virtually no side-effects.
Platelet rich plasma (prp) skin rejuvenation therapy utilizes the potential of your own body to improve the overall texture and tone of your skin, naturally. It reduces wrinkles and blemishes such as acne scars and may be used as part of your health and beauty regimes to improve the overall condition of the skin, improving tone and texture. Platelet Rich Plasma Skin Rejuvenation Therapy is a natural approach to improving the condition of your skin, and you are using your own unique tissue growth factors and healing properties to revitalize the skin by improving blood supply and stimulating collagen formation, the results of which improves and increases over time with evidence suggesting that the results of PRP Skin Rejuvenation Therapy lasts longer than chemical treatments. PRP Skin Rejuvenation Therapy is specifically designed for you, by you!
60
References (1)mermann R, Jakubietz R, Jakubietz M, Strasser E, Schlegel A, Wiltfang J, et al. Different preparation
methods to obtain platelet components as a source of growth factors for local
application.Transfusion. 2001;41:1217–24. doi: 10.1046/j.1537-2995.2001.41101217.x.
(2) Marx RE. Platelet-rich plasma: evidence to support its use. J Oral Maxillofac Surg. 2004;62:489–96. doi:
10.1016/j.joms.2003.12.003.
(3) Freymiller EG. Platelet-rich plasma: evidence to support its use. J Oral Maxillofac Surg. 2004;62:1046–,
author reply 1047-8. doi: 10.1016/j.joms.2004.05.205.
(4) landesberg R, Roy M, Glickman RS. Quantification of growth factor levels using a simplified method of
plateletrich plasma gel preparation. J Oral MaxillofacSurg 2000;58:297–300
(5)Margolis DJ, Kantor J, Santanna J, Strom BL, Berlin JA. Effectiveness of platelet releasate for the
treatment of diabetic neuropathic foot ulcers. Diabetes Care 2001;24:483–488
(6) Man D, Plosker H, Winland-Brown JE. The use of autologous platelet-rich plasma (platelet gel) and
autologous plateletpoor plasma (fibrin glue) in cosmetic surgery.PlastReconstrSurg 2001;107:229–237
(7) Yol S, Tekin A, Yilmaz H, Küçükkartallar T, Esen H, Caglayan O, et al. Effects of platelet rich plasma on
colonic anastomosis. J Surg Res 2008;146:190–194
(8) Kim DH, Je YJ, Kim CD, Lee YH, Seo YJ, Lee JH, et al. Can Platelet-rich Plasma Be Used for Skin
Rejuvenation? Evaluation of Effects of Platelet-rich Plasma on Human Dermal Fibroblast. Ann
Dermatol.2011;23:424–31. (9) HOM D.B., LINZIE B.M., HUANG T.C. The healing effects of autologous platelet gel on acute skin wounds. Arch. Facial Plast. Surg. 2007; 9: 174-183. (10) KIM J.H., PARK C., PARK H.M. Curative effect of autologous plateletrich plasma on a large cutaneous lesion in a dog. Vet. Dermatol.2009 Jan 21. (11) DOUGHERTY E.J. An evidence-based model comparing the cost-effectiveness of platelet-rich plasma gel to alternative therapies for patients with non-healing diabetic foot ulcers. Adv. Skin Wound Care. 2008 Dec; 21(12):568-75. (12) Rai B, Oest ME, Dupont KM, Ho KH, Teoh SH, Guldberg RE. Combination of platelet-rich plasma withpolycaprolactone-tricalciumphosphatescaffoldsforsegmentalbonedefectrepair. J Biomed Mater Res A. 2007; 81(4):888-899. (13)MARX R.E., CARLSON E.R., EICHSTAEDT R.M. SCHIMMELE S.R., STRAUSS J.E., GEORGEFF K.R. Platelet-rich plasma: Growth factor enhancement for bone grafts. Oral Surg. Oral Med. Oral Pathol.Oral Radiol.Endod. 1998;85:638-646 (14)Marx RE. Platelet-rich plasma: evidence to support its use. J Oral MaxillofacSurg 2004;62:489–496. (15).Man D, Plosker H, Winland-Brown JE. The use of autologous platelet-rich plasma (platelet gel) and autologous plateletpoor plasma (fibrin glue) in cosmetic surgery.PlastReconstrSurg 2001;107:229–237.
(16) Pierce GF, Tarpley JE, Yanagihara D, Mustoe TA, Fox GM, Thomason A. Platelet-derived growth factor
(BB homodimer), transforming growth factor-beta 1, and basic fibroblast growth factor in dermal wound
healing: neovessel and matrix formation and cessation of repair. Am J Pathol. 1992;140(6):1375-1388.
61
(17)Rittié L, Fisher G. UV-light-induced signal cascades and skin aging. Aging Res Rev.2002;1:705–20. (18)Ramos-E-Silva M, Hexsel DM, Rutowitsch MS, et al. Hydroxy acids and retinoids in cosmetics.ClinDermatol. 2001;19:460–6. (19)Gilchrest BA, Krutmann J. Skin aging. Heidelberg: Springer; 2006. 198 p. (20) Berneburg M, Plettenberg H, Krutmann J. Photoaging of human skin. PhotodermatolPhotoimmunolPhotomed. 2000;16:239–44. (21)Dewberry C, Norman RA.Skin cancer in elderly patients.DermatolClin. 2004;22:93–6. (22)Perricone N. The wrinkle cure. New York: Warner Books; 2001. 207 p (23)Yaar M, Gilchrest BA. Skin Aging: Postulated mechanisms and consequent changes in structure and function.ClinGer Med. 2001;17:617–30 (24)Rheinwald JG, Hahn WC, Ramsey MR, et al. A two-stage p16 (INK4A) and p53–dependent keratinocyte senescence mechanism that limits replicative potential independent telomere status. Mol Cell Bio. 2002;22:5157–72 (25)Yaar M, Gilchrest BA. Skin Aging: Postulated mechanisms and consequent changes in structure and function.ClinGer Med. 2001;17:617–30 (26)Rittié L, Fisher G. UV-light-induced signal cascades and skin aging. Aging Res Rev. 2002;1:705–20. (27)Baumann L. Cosmetic dermatology. New York: McGraw-Hill; 2002. 226 p. (28)Yaar M, Gilchrest BA. Aging of skin. In: Freedberg IM, Eisen AZ, Wolf K, Austen KF, Goldsmith LA, Katz SI, editors. Fitzpatrick’s dermatology in general medicine, vol 2. New York: McGraw-Hill; 2003. p. 1386–98. (29)Allsopp RC, Vaziri H, Patterson C, Goldstein S, Younglai EV, Futcher AB, Greider CW, Harley CB.Telomere length predicts replicative capacity of human fibroblasts. ProcNatlAcadSci USA.1992;89:10114–8. (30)Cooper GM, Hausman RE. Stanica: molekularnipristup. [Translation of The cell, 3rd ed.] Zagreb: Medicinskanaklada; 2004. 713 p. (31)Glogau RG. Systemic evaluation of the aging face. In: Bolognia JL, Jorizzo JL, Rapini RP, editors.Dermatology. Edinburgh: Mosby; 2003. p. 2357–60. (32)Swift ME, Burns AL, Gray KL, DiPietro LA. Age-related alterations in inflammatory response to dermal injury. J Invest Dermatol. 2001;117:1027–35. (33)Avrat E, Broglio F, Ghigo E. Insulin-like growth factor I: implications in aging. Drugs Aging. 2000;16:29–40. (34)Frippiat C, Chen QM, Zdanov S, Magalhaes JP, Remacle J, Toussaint O. Subcytotoxic H2O2 stress triggers a release of transforming growth factor-beta a, which induces biomarkers of cellular senescence of human diploid fibroblasts. J Biol Chem. 2001;276:2531–7. (35)Ferguson J, Dover JS.Photodermatology. London: Manson Publishing; 2006. 160 (36)Scharffetter-Kochanek K, Brenneisen P, Wenk J, et al. Photoaging of the skin: From phenotype to mechanisms. ExpGerontol. 2000;35:307–16. (37)Braverman IM, Fonferko E. Studies in cutaneous aging I. The elastic fibre network. J Invest Dermatol. 1982;78:434–43. (38)Talwar HS, Griffiths CE, Fisher GJ, Hamilton TA, Voorhees JJ. Reduced type I and type III procollagens in photodamaged adult human skin. J Invest Dermatol. 1995;105:285–90. (39)Fisher GJ, Talwar HS, Lin J, et al. Retinoic acid inhibits induction of c-jun protein by ultraviolet radiation that occurs subsequent to activation of mitogen-activated protein kinase pathways in human skin in vivo. J Clin Invest. 1998;101:1432–40. (40)Sams M Jr. Sun-induced aging.Clinical and laboratory observations in man.DermatolClin 1986;4:509–16. (41)Fisher G, Data s, Wang Z, Li X, Quan T, Chung J, Kang S, Voorhees J. c-Jun dependent inhibition of cutaneusprocollagen transcription following ultraviolet irradiation is reversed by all-trans retinoid acid. J Clin Invest. 2000;106:661–8. (42)Glogau RG. Chemical peeling and aging skin.J GeriatrDermatol. 1994;2:31–5. (43)Boyd S, Stasko T, King LE Jr, Cameron GS, Pearse AD, Gaskell SA. Cigarette smoking-associated elastotic changes in the skin. J Am AcadDermatol. 1999;41:23–6. (44)Smith JB, Fenske NA. Cutaneous manifestations and consequence of smoking. J Am Acad Dermatol.1996;34:717–32.
62
(45)Demierre MF, Brooks D, Koh H, Geller AC. Public knowledge, awareness and perception of the association between skin aging and smoking. J Am AcadDermatol. 1999;41:27–30. (46)Castelo-Branco C, Figueras F, Martinez de Osaba MJ, Vanrell JA.Facial wrinkling in postmenopausal women.Effects of smoking status and hormone replacement therapy.Maturitas. 1998;29:75–86. (47)O’Hare PM, Fleischer AB Jr, D’Agostino RB Jr, Feldman SR, Hinds MA, Rassette SA et al. Tobacco smoking contributes little to facial wrinkling. J EurAcadDermatolVenereol. 1999;12:133–9. (48)Lahman C, Bergemann J, Harrison G, Young A. Matrix metalloproteinase-I and skin aging in smokers. Lancet. 2001;357:935–6. (49)Wenk J, Brenneisen P, Meewes C, Wlaschek M, Peters T, Blaudschun R, Ma W, Kuhr I, Schneider L, Scharffetter-Kochanek K. UV-induced oxidative stress and photoaging. CurrProblDermatol. 2001;29:83–94. (50)ClinInterv Aging. 2006 December; 1(4): 327–348. (51)Jennifer R.S. Gordon, M.D., and Joaquin C. Brieva, M.D.N Engl J , Unilateral DermatoheliosisMed 2012; 366:e25April 19, 2012DOI: 10.1056/NEJMicm1104059 (52)Lavker RM, Zheng PS, Dong G. Aged skin: a study by light, transmission electron, and scanning electron microscopy. J Invest Dermatol. 1987;88:44s–51s. (53)Griffiths CEM. Dowling Oration delivered at the Royal College of Physicians, London, Retinoids: renaissance and reformation. ClinExpDermatol. 1998;24:329–35. (54)Kircik LH, Dahl A, Yatskayer M, Raab S, Oresajo C.Safety and efficacy of two anti-acne/anti-aging treatments in subjects with photodamaged skin and mild to moderate acne vulgaris.J Drugs Dermatol. 2012 Jun;11(6):737-40. (55)Oda RM, Shimizu RW, Sabatine SC, et al. Effects of structural changes on retinoid cytotoxity in the CHO clonal assay.In vitro. Toxicol. 1996;9:173–81. (56)Torras H. Retinoids in aging. ClinDermatol. 1996;74:207–15.
(57)Kim BH, Lee YS, Kang KS.The mechanism of retinol-induced irritation and its application to anti-irritant development. ToxicolLett. 2003;146:65–73.
(58)Torras H. Retinoids in aging. ClinDermatol. 1996;74:207–15.
(59)Tobin DJ, Paus R. Graying: geronobiology of the hair follicle pigmentary unit. ExpGerontol. 2001;36:29–54 (60) R. L. Nachman and S. Rafii, “Platelets, petechiae, and preservation of the vascular wall,” The New England Journal of Medicine, vol. 359, no. 12, pp. 1261–1270, 2008. (61)N. Borregaard and J. B. Cowland, “Granules of the human neutrophilicpolymorphonuclearleukocyte,”Blood, vol. 89, no. 10, pp. 3503–3521, 1997 (62) F. Rendu and B. Brohard-Bohn, “The platelet release reaction: granules' constituents, secretion and functions,” Platelets, vol. 12, no. 5, pp. 261–273, 2001. (63) E. Anitua, I. Andia, B. Ardanza, P. Nurden, and A. T. Nurden, “Autologous platelets as a source of proteins for healing and tissue regeneration,” Thrombosis and Haemostasis, vol. 91, no. 1, pp. 4–15, 2004. (64) A. Garcia, N. Zitzmann, and S. P. Watson, “Analyzing the platelet proteome,” Seminars in Thrombosis and Hemostasis, vol. 30, no. 4, pp. 485–489, 2004. (65) A. H. Qureshi, V. Chaoji, D. Maiguel et al., “Proteomic and phospho-proteomic profile of human platelets in basal, resting state: insights into integrin signaling,” PLoS One, vol. 4, no. 10, Article ID e7627, 2009. (66) K. Jurk and B. E. Kehrel, “Platelets: physiology and biochemistry,” SeminThrombHemost, vol. 31, pp. 381–392, 2005. (67) A. I. Mininkova, “Platelet structure and functions (a review of literature). Part 1,” KlinichescheskayaLaboratornayaDiagnostika, no. 11, pp. 21–26, 2010
63
(68)O. Mei-Dan, L. Laver, M. Nyska, and G. Mann, “Platelet rich plasma—a new biotechnology for treatment of sports injuries,” Harefuah, vol. 150, no. 5, pp. 453–457, 2011. (69)A. T. Nurden, “Platelets, inflammation and tissue regeneration,” Thrombosis and Haemostasis, vol. 105 suppl 1, pp. S13–S33, 2011. (70) R. E. Marx, E. R. Carlson, R. M. Eichstaedt, S. R. Schimmele, J. E. Strauss, and K. R. Georgeff, “Platelet-rich plasma: growth factor enhancement for bone grafts,” Oral Surgery, Oral Medicine, Oral Pathology, Oral Radiology, and Endodontics, vol. 85, no. 6, pp. 638–646, 1998. (71) A. I. Mininkova, “Investigation of platelets by the flow cytofluorometric technique (a review of literature). Part 2,” KlinichescheskayaLaboratornayaDiagnostika, no. 4, pp. 25–30, 2011. (72) L. Brass, “Understanding and evaluating platelet function,” Hematology / the Education Program of the American Society of Hematology Education Program, vol. 2010, pp. 387–396, 2010. (73) Y. Liu, A. Kalen, O. Risto, and O. Wahlström, “Fibroblast proliferation due to exposure to a platelet concentrate in vitro is pH dependent,” Wound Repair and Regeneration, vol. 10, no. 5, pp. 336–340, 2002 (74) C. A. Carter, D. G. Jolly, C. E. Worden, D. G. Hendren, and C. J. M. Kane, “Platelet-rich plasma gel promotes differentiation and regeneration during equine wound healing,” Experimental and Molecular Pathology, vol. 74, no. 3, pp. 244–255, 2003. (75) B. L. Eppley, W. S. Pietrzak, and M. Blanton, “Platelet-rich plasma: a review of biology and applications in plastic surgery,” Plastic and Reconstructive Surgery, vol. 118, no. 6, pp. 147e–159e, 2006. (76) K. M. Lacci and A. Dardik, “Platelet-rich plasma: support for its use in wound healing,” Yale Journal of Biology and Medicine, vol. 83, no. 1, pp. 1–9, 2010. (77) B. Cole and S. Seroyer, “Platelet-rich plasma: where are we now and where are we going?” Sports Health, vol. 2, no. 3, pp. 203–210, 2010. (78) T. E. Foster, B. L. Puskas, B. R. Mandelbaum, M. B. Gerhardt, and S. A. Rodeo, “Platelet-rich plasma: from basic science to clinical applications,” American Journal of Sports Medicine, vol. 37, no. 11, pp. 2259–2272, 2009. (79) S. Werner and R. Grose, “Regulation of wound healing by growth factors and cytokines,” Physiological Reviews, vol. 83, no. 3, pp. 835–870, 2003. (80) R. E. Marx, “Platelet-rich plasma (PRP): what is PRP and what is not PRP?” Implant Dentistry, vol. 10, no. 4, pp. 225–228, 2001. (81)B. L. Eppley, J. E. Woodell, and J. Higgins, “Platelet quantification and growth factor analysis from platelet-rich plasma: implications for wound healing,” Plastic and Reconstructive Surgery, vol. 114, no. 6, pp. 1502–1508, 2004. (82) S. J. Froum, S. S. Wallace, D. P. Tarnow, and S. C. Cho, “Effect of platelet-rich plasma on bone growth and osseointegration in human maxillary sinus grafts: three bilateral case reports,” International Journal of Periodontics and Restorative Dentistry, vol. 22, no. 1, pp. 45–53, 2002. (83) A. Mishra, J. Velotta, T. J. Brinton et al., “RevaTen platelet-rich plasma improves cardiac function after myocardial injury,” Cardiovascular Revascularization Medicine, vol. 12, no. 3, pp. 158–163, 2011. (84)A. R. Sanchez, P. J. Sheridan, and L. I. Kupp, “Is platelet-rich plasma the perfect enhancement factor? A current review,” International Journal of Oral and Maxillofacial Implants, vol. 18, no. 1, pp. 93–103, 2003. (85) T. F. Tozum and B. Demiralp, “Platelet-rich plasma: a promising innovation in dentistry,” Journal Canadian Dental Association, vol. 69, no. 10, p. 664, 2003. (86) E. G. Freymiller and T. L. Aghaloo, “Platelet-rich plasma: ready or not?” Journal of Oral and Maxillofacial Surgery, vol. 62, no. 4, pp. 484–488, 2004. (87) M. I. Furman, L. Liu, S. E. Benoit, R. C. Becker, M. R. Barnard, and A. D. Michelson, “The cleaved peptide of the thrombin receptor is a strong platelet agonist,” Proceedings of the National Academy of Sciences of the United States of America, vol. 95, no. 6, pp. 3082–3087, 1998.
64
(88)J. P. Maloney, C. C. Silliman, D. R. Ambruso, J. Wang, R. M. Tuder, and N. F. Voelkel, “In vitro release of vascular endothelial growth factor during platelet aggregation,” American Journal of Physiology, vol. 275, no. 3, pp. H1054–H1061, 1998. (89)A. Kocaoemer, S. Kern, H. Klüter, and K. Bieback, “Human AB serum and thrombin-activated platelet-rich plasma are suitable alternatives to fetal calf serum for the expansion of mesenchymal stem cells from adipose tissue,” Stem Cells, vol. 25, no. 5, pp. 1270–1278, 2007 (90) Wrotniak M, Bielecki T, Gaździk TS. Current opinion about using the platelet-rich gel in orthopaedics and trauma surgery.OrtopTraumatolRehabil 2007;9:227–238. (91) Marx R, Garg A. Dental and craniofacialapplications of platelet- rich plasma. Carol Stream: Quintessence Publishing Co, Inc.; 2005. (92) Graziani F, Ivanovski S, Cei S, et al. The in vitro effect of different PRP concentrations on osteoblasts
and fibroblasts.Clin Oral Implants Res. 2006;17:212-219.
(93)Karimipour DJ, Rittié L, Hammerberg C, et al. Molecular analysis of aggressive microdermabrasion in
photoaged skin.Arch Dermatol.2009;145:1114-1122.
(94) Quan T, Qin Z, Xia W, Shao Y, et al. Matrix-degrading metalloproteinases in photoaging. J
InvestigDermatolSymp Proc. 2009;14:20-24.
(95)Kim DH, Je YJ, Kim CD, et al. Can Platelet-rich Plasma Be Used for Skin Rejuvenation? Evaluation of
Effects of Platelet-rich Plasma on Human Dermal Fibroblast.Ann Dermatol. 2011;23:424-431
(96)Redaelli A, Romano D, Marcianó A. Face and neck revitalization with platelet-rich plasma (PRP):
clinical outcome in a series of 23 consecutively treated patients. J Drugs Dermatol. 2010;9:466-472.
(97) Cho JW, Kim SA, Lee KS. Platelet-rich plasma induces increased expression of G1 cell cycle regulators,
type I collagen, and matrix metalloproteinase-1 in human skin fibroblasts. Int J Mol Med. 2012;29:32-36.
(98)Kakudo N, Minakata T, Mitsui T, et al. Proliferation-promoting effect of platelet-rich plasma on human adipose-derived stem cells and human dermal fibroblasts.PlastReconstr Surg. 2008;122:1352–1360.
(99)Cho JW, Kim SA, Lee KS. Platelet-rich plasma induces increased expression of G1 cell cycle regulators, type I collagen, and matrix metalloproteinase-1 in human skin fibroblasts. Int J Mol Med 2012;29:32-6.
(100) Kim DH, Je YJ, Kim CD, Lee YH, Seo YJ, Lee JH, et al. Can platelet-rich plasma be used for skin rejuvenation? Evaluation of effects of platelet-rich plasma on human dermal fibroblast. Ann Dermatol 2011;23:424-31.
(101)Redaelli A, Romano D, Marcianó A. Face and neck revitalization with platelet-rich plasma
(PRP): Clinical outcome in a series of 23 consecutively treated patients. J Drugs Dermatol 2010;9:466-72.
(102)Shin MK, Lee JH, Lee SJ, Kim NI. Platelet-rich plasma combined with fractional laser therapy for skin rejuvenation. DermatolSurg 2012;38:623-30.
(103) Na JI, Choi JW, Choi HR, Jeong JB, Park KC, Youn SW, et al. Rapid healing and reduced erythema after ablative fractional carbon dioxide laser resurfacing combined with the application of autologous platelet-rich plasma. DermatolSurg 2011;37:463-8.
65
(104) Kang BK, Lee JH, Shin MK, Kim NI. Infraorbital rejuvenation using PRP (platelet-rich plasma): A prospective, randomized, split-face trial. J Am AcadDermatol 2013;68:SAB24.
(105) Sclafani AP. Platelet-rich fibrin matrix for improvement of deep nasolabial folds. J CosmetDermatol 2010;9:66-71.
(106) Oh DS, Cheon YW, Jeon YR, Lew DH. Activated platelet-rich plasma improves fat graft survival in nude mice: A pilot study. DermatolSurg 2011;37:619-25.
(107) Park KY, Kim IS, Kim BJ, Kim MN. Letter: Autologous fat grafting and platelet-rich plasma for treatment of facial contour defects. DermatolSurg 2012;38:1572-4.
(108) Cervelli V, Nicoli F, Spallone D, Verardi S, Sorge R, Nicoli M, et al. Treatment of traumatic scars using fat grafts mixed with platelet-rich plasma, and resurfacing of skin with the 1540 nm nonablative laser. ClinExpDermatol 2012;37:55-61.
(109)Lee JW, Kim BJ, Kim MN, Mun SK. The efficacy of autologous platelet rich plasma combined with ablative carbon dioxide fractional resurfacing for acne scars: A simultaneous split-face trial. DermatolSurg 2011;37:931-8. (110) S. C. Bir, J. Esaki, A. Marui et al., “Therapeutic treatment with sustained-release platelet-rich plasma restores blood perfusion by augmenting ischemia-induced angiogenesis and arteriogenesis in diabetic mice,” Journal of Vascular Research, vol. 48, no. 3, pp. 195–205, 2011. (111)S. C. Bir, J. Esaki, A. Marui et al., “Angiogenic properties of sustained release platelet-rich plasma: characterization in-vitro and in the ischemic hind limb of the mouse,” Journal of Vascular Surgery, vol. 50, no. 4, pp. 870–879, 2009. (112)A. Mishra and T. Pavelko, “Treatment of chronic elbow tendinosis with buffered platelet-rich plasma,”American Journal of Sports Medicine, vol. 34, no. 11, pp. 1774–1778, 2006. (113)G. Weibrich, W. K. Kleis, G. Hafner, and W. E. Hitzler, “Growth factor levels in platelet-rich plasma and correlations with donor age, sex, and platelet count,” Journal of Craniomaxillofacial Surgery, vol. 30, no. 2, pp. 97–102, 2002. (114)M. M. Rechler and S. P. Nissley, “Insulin-like growth factors,” in Handbook of Experimental Pharm: Peptide Growth Factors and Their Receptors, M. B. Sporn and A. B. Roberts, Eds., vol. 96, pp. 263–367, Springer, Berlin, Germany, 1990. (115)G. F. Pierce, T. A. Mustoe, J. Lingelbach, V. R. Masakowski, P. Gramates, and T. F. Deuel, “Transforming growth factor β reverses the glucocorticoid-induced wound healing deficit in rats. Possible regulation in macrophages by platelet-derived growth factor,” Proceedings of the National Academy of Sciences of the United States of America, vol. 86, no. 7, pp. 2229–2233, 1989. (116)J. M. Pérez-Rojas, C. Cruz, P. García-López et al., “Renoprotection byα-mangostin is related to the attenuation in renal oxidative/nitrosative stress induced by cisplatin nephrotoxicity,” Free Radical Research, vol. 43, no. 11, pp. 1122–1132, 2009. (117)M. G. Goldner, “The fate of the second leg in the diabetic amputee,” Diabetes, vol. 9, pp. 100–103, 1960. (118) J. Yu, C. Ustach, and H. R. Kim, “Platelet-derived growth factor signaling and human cancer,” Journal of Biochemistry and Molecular Biology, vol. 36, no. 1, pp. 49–59, 2003.
66
(119) S. P. Bennett, G. D. Griffiths, A. M. Schor, G. P. Leese, and S. L. Schor, “Growth factors in the treatment of diabetic foot ulcers,” British Journal of Surgery, vol. 90, no. 2, pp. 133–146, 2003. (120)E. M. Spencer, A. Tokunaga, and T. K. Hunt, “Insulin-like growth factor binding protein-3 is present in the α-granules of platelets,” Endocrinology, vol. 132, no. 3, pp. 996–1001, 1993. (121) T. McCarrel and L. Fortier, “Temporal growth factor release from platelet-rich plasma, trehalose lyophilized platelets, and bone marrow aspirate and their effect on tendon and ligament gene expression,” Journal of Orthopaedic Research, vol. 27, no. 8, pp. 1033–1042, 2009. (122) H. F. Dvorak, “Discovery of vascular permeability factor (VPF),” Experimental Cell Research, vol. 312, no. 5, pp. 522–526, 2006. (123) T. Tammela, B. Enholm, K. Alitalo, and K. Paavonen, “The biology of vascular endothelial growth factors,” Cardiovascular Research, vol. 65, no. 3, pp. 550–563, 2005. (124) S. Lee, T. T. Chen, C. L. Barber et al., “Autocrine VEGF signaling is required for vascular homeostasis,”Cell, vol. 130, no. 4, pp. 691–703, 2007. (125) P. Carmeliet, V. Ferreira, G. Breier et al., “Abnormal blood vessel development and lethality in embryos lacking a single VEGF allele,” Nature, vol. 380, no. 6573, pp. 435–439, 1996. (126) B. Olofsson, M. Jeltsch, U. Eriksson, and K. Alitalo, “Current biology of VEGF-B and VEGF-C,” Current Opinion in Biotechnology, vol. 10, no. 6, pp. 528–535, 1999. (127) T. A. Partanen, J. Arola, A. Saaristo et al., “VEGF-C and VEGF-D expression in neuroendocrine cells and their receptor, VEGFR-3, in fenestrated blood vessels in human tissues,” FASEB Journal, vol. 14, no. 13, pp. 2087–2096, 2000. (128) M. Klagsbrun, S. Takashima, and R. Mamluk, “The role of neuropilin in vascular and tumor biology,”Advances in Experimental Medicine and Biology, vol. 515, pp. 33–48, 2002. (129) R. J. Levine, S. E. Maynard, C. Qian et al., “Circulating angiogenic factors and the risk of preeclampsia,”The New England Journal of Medicine, vol. 350, no. 7, pp. 672–683, 2004. (130) J. Folkman, “Angiogenesis: an organizing principle for drug discovery?” Nature Reviews Drug Discovery, vol. 6, no. 4, pp. 273–286, 2007. (131) R. Möhle, D. Green, M. A. Moore, R. L. Nachman, and S. Rafii, “Constitutive production and thrombin-induced release of vascular endothelial growth factor by human megakaryocytes and platelets,”Proceedings of the National Academy of Sciences of the United States of America, vol. 94, no. 2, pp. 663–668, 1997 · (132) M. Lucerna, A. Zernecke, R. de Nooijer et al., “Vascular endothelial growth factor-A induces plaque expansion in ApoE knock-out mice by promoting de novo leukocyte recruitment,” Blood, vol. 109, no. 1, pp. 122–129, 2007. (133)D. J. Sánchez-González, C. A. Sosa-Luna, and I. Vásquez-Moctezuma, “Transfer factors in medical therapy,” MedicinaClinica, vol. 137, no. 6, pp. 273–277, 2011. (134) S. Verrier, T. R. Meury, L. Kupcsik, P. Heini, T. Stoll, and M. Alini, “Platelet-released supernatant induces osteoblastic differentiation of human mesenchymal stem cells: potential role of BMP-2,”European Cells & Materials, vol. 20, pp. 403–414, 2010.
67
(135)A. Sobotková, L. Másová-Chrastinová, J. Suttnar et al., “Antioxidants change platelet responses to various stimulating events,” Free Radical Biology and Medicine, vol. 47, no. 12, pp. 1707–1714, 2009. (136) E. Floriano-Sánchez, C. Villanueva, O. N. Medina-Campos et al., “Nordihydroguaiaretic acid is a potent in vitro scavenger of peroxynitrite, singlet oxygen, hydroxyl radical, superoxide anion and hypochlorous acid and prevents in vivo ozone-induced tyrosine nitration in lungs,” Free Radical Research, vol. 40, no. 5, pp. 523–533, 2006. (137) C. Cruz, R. Correa-Rotter, D. J. Sánchez-González et al., “Renoprotective and antihypertensive effects of S-allylcysteine in 5/6 nephrectomized rats,” American Journal of Physiology, vol. 293, no. 5, pp. F1691–F1698, 2007. (138) C. E. Guerrero-Beltrán, M. Calderón-Oliver, E. Tapia et al., “Sulforaphane protects against cisplatin-induced nephrotoxicity,” Toxicology Letters, vol. 192, no. 3, pp. 278–285, 2010. (139)E. Coballase-Urrutia, J. Pedraza-Chaverri, N. Cárdenas-Rodríguez et al., “Hepatoprotective effect of acetonic and methanolic extracts of Heterothecainuloides against CCl(4)-induced toxicity in rats,”Experimental and Toxicologic Pathology, vol. 63, no. 4, pp. 363–370, 2011.
(140) Dermatol Surg. 2012 Apr;38(4):623-30. doi: 10.1111/j.1524-4725.2011.02280.x. Epub
2012 Jan 30.Platelet-rich plasma combined with fractional laser therapy
for skin rejuvenation.Shin MK1, Lee JH, Lee SJ, Kim NI. (141) http://uscenterforsportsmedicine.com/
(142)Sampson S, Gerhardt M, Mandelbaum B. Platelet rich plasma injection grafts for musculoskeletal
injuries: a review. Curr Rev Musculoskelet Med. 2008 Dec;1(3-4):165-74.
(143) World Anti-Doping Agency [online]. Available from URL: http://www.wada-
ama.org/en/Resources/Q-and-A/2011-Prohibited-List/ [Accessed July 21, 2011]
(144) M. Sánchez, E. Anitua, J. Azofra, I. Andía, S. Padilla, and I. Mujika, “Comparison of surgically repaired achilles tendon tears using platelet-rich fibrin matrices,” American Journal of Sports Medicine, vol. 35, no. 2, pp. 245–251, 2007. (145)L. Savarino, E. Cenni, C. Tarabusi et al., “Evaluation of bone healing enhancement by lyophilized bone grafts supplemented with platelet gel: a standardized methodology in patients with tibial osteotomy for genu varus,” Journal of Biomedical Materials Research, vol. 76, no. 2, pp. 364–372, 2006.





























