Embed Size (px)
Citation preview

MASTERS IN CRITICAL CARE MEDICINE PAKISTAN INSTITUTE OF MEDICAL SCIENCES
TRAINER’S GUIDE AND COBATRICE SYLLABUS

THE MASTERS IN CRITICAL CARE MEDICINE Introduction Severe infections, asthma attacks, complicated deliveries, road traffic accidents and so many other conditions can lead to death within a few hours in previously healthy persons. Critical Care Medicine consists in supporting the failing organs until the condition of the patient stabilizes, through medical treatment or emergency surgery. Treatment and level of organ support need minute by minute adjustments because both insufficient and excessive support may be harmful for the patient. Critical Care Medicine in Pakistan is challenging. In developing / transitional countries, patient admitted in Intensive Care Units (ICUs) are much younger than in developed countries and they are suffering from reversible conditions. Therefore a critically ill patient is more likely, if he is managed quickly after an acute severe aggression, to recover and go back to a socially and economically active status. Death of a patient with reversible conditions such as tetanus or a road traffic accident should not be accepted. Provision of quality services to the critically ill is one of the basic requirements of tertiary care institutions. ICUs are mushrooming all over the country, especially after the earthquake of 8th October 2005 when a lot of equipment like cardiac monitors, ventilators and dialysis machines were donated to hospitals. Institutions in the private sector have invested in costly equipments to provide services to their critically ill patients. However, apart from a few prestigious institutions, very little effort has been made to train doctors and offer them career perspectives and structure. PIMS is having a unique set-up regarding critical care in Pakistan with 7 units (Surgical ICU, Cardiac surgery ICU, Medical ICU, Burn Unit ICU, Coronary care Unit, pediatric ICU, neonatal ICU) for a total of 75 beds, which represents a great field for training. A Department of Critical Care Medicine has been created at PIMS putting under the same umbrella the Surgical ICU (under the care of anesthesiologists) and the Medical ICU (under the care of physicians). The department of Critical Care Medicine is therefore a multidisciplinary professorial unit. There is a traditional approach which separates medical and surgical patients. This is mostly justified by the necessity to accommodate more patients in units of reasonable size. However the physiology and the management of the critically ill are very similar in medical and surgical patients and critical care medicine addresses both. The critically ill patient is challenging by his complexity and therefore benefits a lot from a multidisciplinary approach.

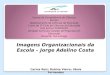
The Masters in Critical Care Medicine is for doctors with either a background of anesthesia or a background in medical specialties who want to gain theoretical and practical skills to manage the critically ill. Significant experience is necessary before enrolling in the proper Critical Care Medicine training, because critically ill patients need doctors with broad based knowledge and experience. The Masters in Critical Care Medicine is a competency-based course. Practical and formal teaching is aimed at acquiring those competencies. Faculty members Faculty members will include existing medical staff from Professor to Assistant Professor in the Critical care Medicine Department. Being a new specialty in Pakistan, the number of faculty members for teaching modules is scanty. That is why the Medical and Surgical ICUs at PIMS have been collaborating for the past 8 years with the Critical Care Medicine Department at Saint Antoine Hospital, Paris. Support by French visiting faculty members is presently under discussion with Embassy of France which has agreed in principle. The input from faculty members of recognized institutions in Pakistan will be requested. CoBaTrICE competencies CoBaTrICE is an international Competency Based Training program in Intensive Care Medicine for Europe and other world regions. It is the result of the consensus built between 536 critical care physicians from 57 countries (including Turkey, India, Malaysia and Indonesia) through a Delphi process. The CoBaTrICE competencies define the minimum standard of knowledge, skills and attitudes required for a doctor to be identified as a specialist in intensive care medicine / critical care medicine. They have been developed with the intention of being internationally applicable but able to accommodate national practices and local constraints. CoBaTrICE syllabus comprises 102 competence statements grouped into 12 domains:
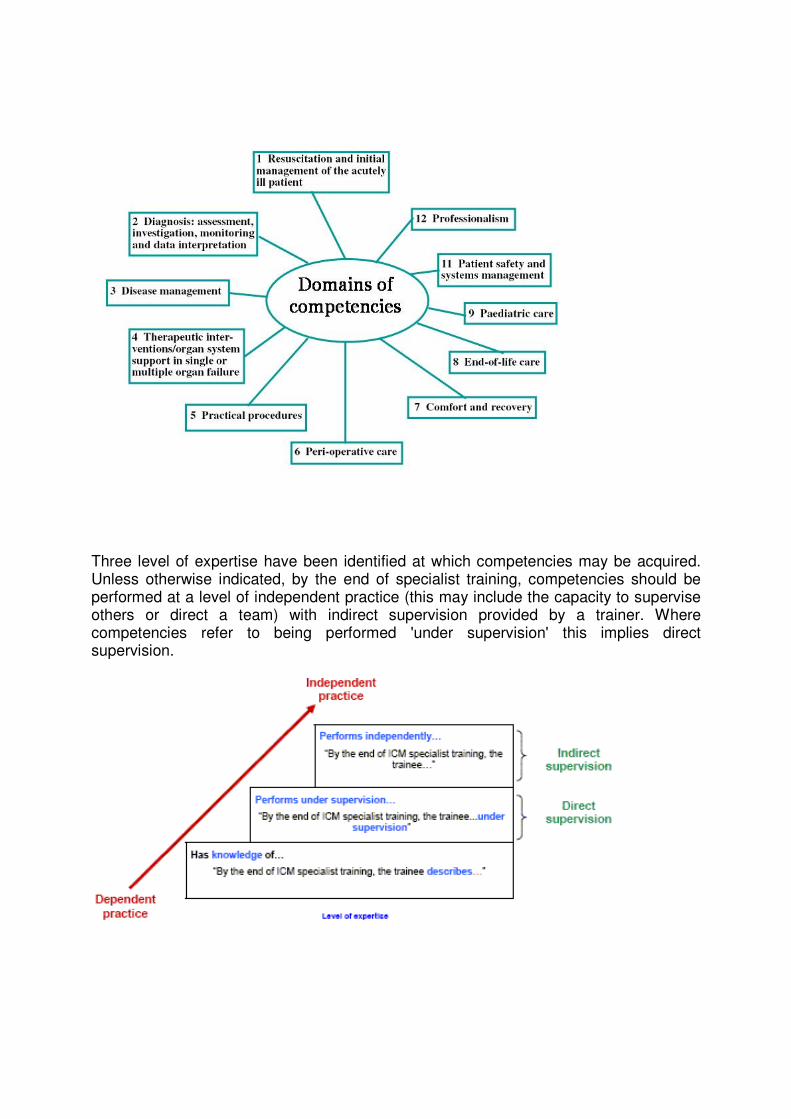
Three level of expertise have been identified at which competencies may be acquired. Unless otherwise indicated, by the end of specialist training, competencies should be performed at a level of independent practice (this may include the capacity to supervise others or direct a team) with indirect supervision provided by a trainer. Where competencies refer to being performed 'under supervision' this implies direct supervision.

Teaching modules Because of the nature of the practice of critical care medicine, formal classroom teaching is difficult to organize during the shift duties on a weekly basis. That is why teaching activities have been grouped in modules (2 days session) of 8 hours of classroom teaching being held every 2 months. This will also allow bringing together lectures in thematic sessions (like circulation, respiration…). Each of these modules will be coordinated by one of the faculty members with learning objectives linked to the above mentioned competencies. Each module is composed of:
1. Personal study of learning material by the student, 2. Attendance to 8 hours lectures given by the faculty, 3. Theoretical/simulation approach of procedures which will be performed under
supervision during the practical, 4. Validation through a short assessment paper. 5. Oral presentation related to one of the teaching module by the student once per
semester. The 12 teaching modules will be scheduled so that the students can complete their learning process within 2 years (3 modules / semester). Teaching modules are not supposed to cover comprehensively the required knowledge, but to address the main topics. Further personal reading of the relevant literature will be required according to the references provided by the faculty members. Here is the schedule of the modules: 1. General concepts
Day 1
2-3 PM 1.1 Historical perspective Dr Rubina Aman
3-4 PM 1.2 Minimal requirements of an ICU Dr Rubina Aman
4-5 PM 1.3 Organisation of care in the ICU Dr Vincent Ioos
5-6 PM 1.4 Triage, admission / discharge criteria Dr Vincent Ioos
Day 2
2-3 PM 1.5 ICU scoring systems Dr Vincent Ioos
3-4 PM 1.6 Patient safety Dr Rubina Aman
4-5 PM 1.7 Learning resources Dr Vincent Ioos
5-6 PM 1.8 Communicating with families Dr Rubina Aman

2. Circulation
Day 1
2-3 PM 2.1 Oxygen transport and delivery, regulation of blood presure and blood volume Dr Rubina Aman
3-4 PM 2.2 Cardiac arrest Dr Kamal Naseer
4-5 PM 2.3 Procedures: defibrillation, pacing, ballon counterpulsion Dr Shahid Malik
5-6 PM 2.4 Acute coronary syndrome Pr Iqbal Saifullah
Day 2
2-3 PM 2.5 Overview of shock and hemodynamic monitoring French faculty
3-4 PM 2.6 Cardiogenic shock French faculty
4-5 PM 2.7 Volume therapy French faculty
5-6 PM 2.8 Massive pulmonary embolism French faculty
3. Respiration
Day 1
2-3 PM 3.1 Ventilation, perfusion and gas exchange in the critically ill Dr Rubina Aman
3-4 PM 3.2 The difficult airway Dr Badar-Us-Samad
4-5 PM 3.3 Pleural diseases in the ICU Col Aslam Khan
5-6 PM 3.4 Severe acute asthma and COPD exacerbation Dr Aftab Akhtar
Day 2
2-3 PM 3.5 Mechanical ventilation (including NIV) French faculty
3-4 PM 3.6 Weaning from mechanical ventilation French faculty
4-5 PM 3.4 Acute lung injury and ARDS French faculty
5-6 PM 3.2 Severe community and hospital acquired pneumonia French faculty
4. Metabolic disturbances…
Day 1
2-3 PM 4.1 Renal physiology Pr Sami J Khan
3-4 PM 4.1 Regulation of acid-base balance Dr Hameed Ullah
4-5 PM 4.2 Water and sodium imbalances Dr Rubina Aman
5-6 PM 4.8 Endocrinologic emergencies Prof Nigat Bilal
Day 2
2-3 PM 4.5 Acute renal failure French faculty
3-4 PM 4.3 Potassium and calcium disturbances French faculty
4-5 PM 4.6 Renal repacement therapy in the critically ill French faculty
5-6 PM 4.7 Metabolic complications of diabetese mellitus French faculty
5. Neurology
Day 1
2-3 PM 5.1 Electrophysiology for the critically ill Dr Mazar Badshah
3-4 PM 5.2 Neuro-imaging for the critically ill Dr Shazia Khan
4-5 PM 5.3 Guillain Barre syndrome and myathenia gravis Prof Muhammad Tariq
5-6 PM 5.4 Rational for early mobilisation of patients in ICU Dr Rubina Aman
Day 2
2-3 PM 5.5 Neurophysiology French faculty
3-4 PM 5.6 Central nervous system infections French faculty
4-5 PM 5.7 Stroke French faculty
5-6 PM 5.8 Subarrachnoidal haemorrhage French faculty
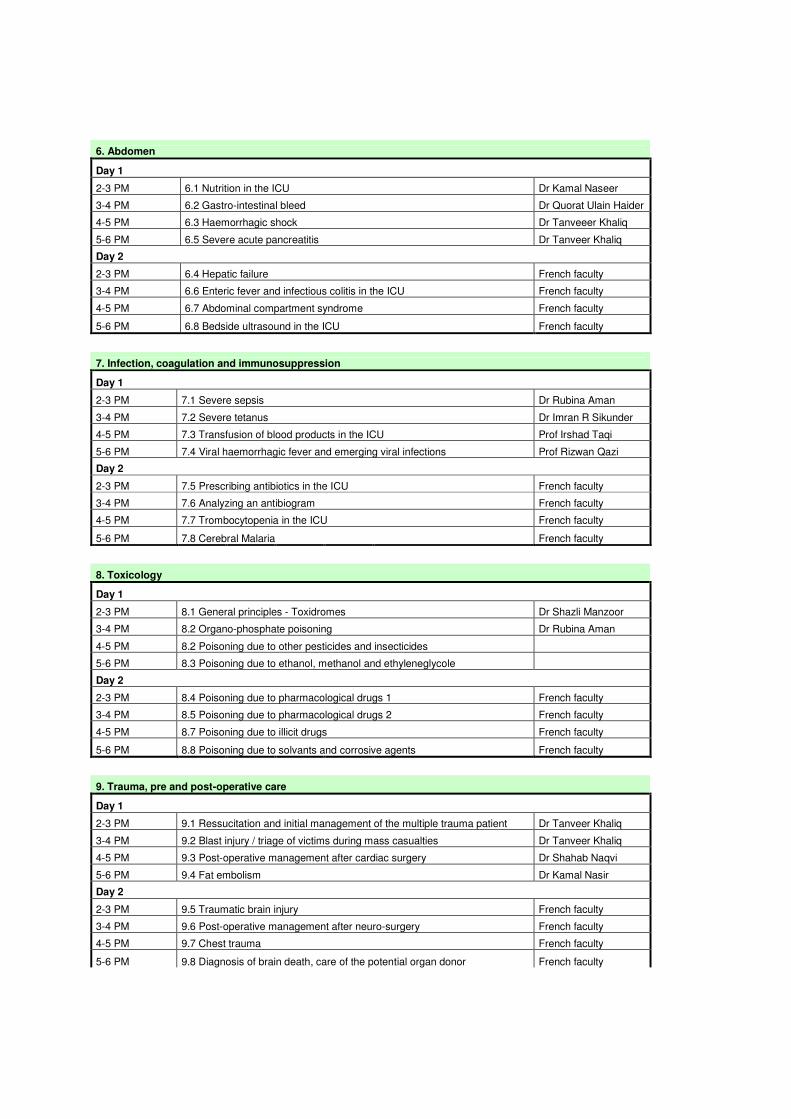
6. Abdomen
Day 1
2-3 PM 6.1 Nutrition in the ICU Dr Kamal Naseer
3-4 PM 6.2 Gastro-intestinal bleed Dr Quorat Ulain Haider
4-5 PM 6.3 Haemorrhagic shock Dr Tanveeer Khaliq
5-6 PM 6.5 Severe acute pancreatitis Dr Tanveer Khaliq
Day 2
2-3 PM 6.4 Hepatic failure French faculty
3-4 PM 6.6 Enteric fever and infectious colitis in the ICU French faculty
4-5 PM 6.7 Abdominal compartment syndrome French faculty
5-6 PM 6.8 Bedside ultrasound in the ICU French faculty
7. Infection, coagulation and immunosuppression
Day 1
2-3 PM 7.1 Severe sepsis Dr Rubina Aman
3-4 PM 7.2 Severe tetanus Dr Imran R Sikunder
4-5 PM 7.3 Transfusion of blood products in the ICU Prof Irshad Taqi
5-6 PM 7.4 Viral haemorrhagic fever and emerging viral infections Prof Rizwan Qazi
Day 2
2-3 PM 7.5 Prescribing antibiotics in the ICU French faculty
3-4 PM 7.6 Analyzing an antibiogram French faculty
4-5 PM 7.7 Trombocytopenia in the ICU French faculty
5-6 PM 7.8 Cerebral Malaria French faculty
8. Toxicology
Day 1
2-3 PM 8.1 General principles - Toxidromes Dr Shazli Manzoor
3-4 PM 8.2 Organo-phosphate poisoning Dr Rubina Aman
4-5 PM 8.2 Poisoning due to other pesticides and insecticides
5-6 PM 8.3 Poisoning due to ethanol, methanol and ethyleneglycole
Day 2
2-3 PM 8.4 Poisoning due to pharmacological drugs 1 French faculty
3-4 PM 8.5 Poisoning due to pharmacological drugs 2 French faculty
4-5 PM 8.7 Poisoning due to illicit drugs French faculty
5-6 PM 8.8 Poisoning due to solvants and corrosive agents French faculty
9. Trauma, pre and post-operative care
Day 1
2-3 PM 9.1 Ressucitation and initial management of the multiple trauma patient Dr Tanveer Khaliq
3-4 PM 9.2 Blast injury / triage of victims during mass casualties Dr Tanveer Khaliq
4-5 PM 9.3 Post-operative management after cardiac surgery Dr Shahab Naqvi
5-6 PM 9.4 Fat embolism Dr Kamal Nasir
Day 2
2-3 PM 9.5 Traumatic brain injury French faculty
3-4 PM 9.6 Post-operative management after neuro-surgery French faculty
4-5 PM 9.7 Chest trauma French faculty
5-6 PM 9.8 Diagnosis of brain death, care of the potential organ donor French faculty

10. Emergencies
Day 1
2-3 PM 10.1 Burns management 1 Dr Tariq Iqbal
3-4 PM 10.2 Burns management 2 Dr Tariq Iqbal
4-5 PM 10.3 Snake bite Dr Rubina Aman
5-6 PM 10.4 Disaster management Prof Shakila Zaman
Day 2
2-3 PM 10.5 Carbon monoxyde and cyanide poisoning, smoke inhalation injury French faculty
3-4 PM 10.6 Heat stroke, accidental hypothermia, malignant hyperthermia French faculty
4-5 PM 10.7 Drowning and hanging French faculty
5-6 PM 10.8 Medical evacuation French faculty
11. Pregnancy
Day 1
2-3 PM 11.1 Physiologic changes associated with pregnancy Dr Shohaib
3-4 PM 11.2 Epidemiology of maternal mortality Dr Farhat
4-5 PM 11.3 Post-partum haemorrhage Pr Ghazala Mehmood
5-6 PM 11.4 Septic abortion Dr Rubina Aman
Day 2
2-3 PM 11.5 Eclampsia and HELLP syndrome French faculty
3-4 PM 11.6 Chronic diseases, acute hepatic and renal failure in pregnancy French faculty
4-5 PM 11.7 Cerebral vein thrombosis in the post-partum French faculty
5-6 PM 11.8 Pulmonary embolism in pregnancy and amniotic fluid embolism French faculty
12. Paediatrics
Day 1
2-3 PM 12.1 Specificity of the physiology of the paediatric patient Prof Memood Jamal
3-4 PM 12.2 Venous access and intubation of the paediatric patient Dr Naeem
4-5 PM 12.3 Severe dehydration Dr Jai Kirshan
5-6 PM 12.4 Respiratory distress in the neonate Dr Nusrat
Day 2
2-3 PM 12.5 Sepsis in the neonate French faculty
3-4 PM 12.6 Central nervous system infections in the paediatric patient French faculty
4-5 PM 12.7 Acute respiratory tract infections in the paediatric patient French faculty
5-6 PM 12.8 Foreign body inhalation French faculty

Critical care medicine grand round Critical care medicine grand round is every Thursday morning from 8am to 9am. The attendance by the students of the Masters in critical Care Medicine is compulsory and should be documented (see the Logbook). The schedule is as follow: Week 1: Clinical case discussion Week 2: Presentation by one or two students Week 3: Journal Club Week 4: Morbi-mortality review. Practical Mandatory and elective rotations will be performed according to the table below. Each student is allocated a rotation track that he chooses according to his position on the merit list of the entry test. The following responsibilities and learning opportunities will be given to the post-graduate student in critical care medicine:
1. Assessment, management and medical prescription with precise allocation of beds, under supervision.
2. Performance of invasive procedures under supervision. 3. Interaction with the patient’s attendants. 4. Documentation: activity and severity scoring, ICU stay summary, infection control,
patient safety. 5. Supervision of house officers and post-graduate students on rotation from other
specialties. 6. Study the relevant literature through personal reading and journal clubs

Rotation plan Masters in Critical Care Medicine
Semesters 07-09 to 12-09 01-10 to 06-10 07-10 to 12-10 01-11 to 06-11 07-11 to 12-11 01-12 to 06-12
track PG 1.1 MICU 1 / OT MICU 2 SPEC. ICUs SICU 1
track PG 1.2 MICU 1 / OT MICU 2 SPEC. ICUs SICU 1
track PG 1.3 MICU 1 / OT MICU 2 SPEC. ICUs SICU 1
track PG 1.4 SICU 1 / OT SICU 2 MICU 1 SPEC. ICUs
track PG 1.5 SICU 1 / OT SICU 2 MICU 1 SPEC. ICUs
track PG 1.6 SICU1 / OT SICU 2 MICU 1 SPEC. ICUs
track PG 2.1 MICU 1 / OT MICU 2 SPEC. ICUs SICU 1
track PG 2.2 MICU 1 / OT MICU 2 SPEC. ICUs SICU 1
track PG 2.3 MICU 1 / OT MICU 2 SPEC. ICUs PICU
track PG 2.4 SICU 1 / OT SICU 2 MICU 1 SPEC. ICUs
track PG 2.5 SICU 1 / OT SICU 2 MICU 1 SPEC. ICUs
track PG 2.6 SICU1 / OT SICU 2 MICU 1 SPEC. ICUs
track PG 3.1 MICU 1 / OT MICU 2
track PG 3.2 MICU 1 / OT MICU 2
track PG 3.3 MICU 1 / OT MICU 2
track PG 3.4 SICU 1 / OT SICU 2
track PG 3.5 SICU 1 / OT SICU 2
track PG 3.6 SICU1 / OT SICU 2
During the first rotation, PG students should be rotated for 2 months in the OT to reach quickly profiency in airway management (PG with anesthesia background are not subjected to this compulsary rotation).
MICU: Medical ICU, 9 beds. Supervision: Dr Rubina Aman.
SICU: Surgical ICU, 13 beds. Supervision: Dr Kamal Naseer.
SPECIALIZED ICUs:
BICU: Burn unit ICU, 12 beds. Supervision: Prof Iqbal Memon / Dr Shohaib (2 months)
CSICU: Cardiac Surgery ICU, 4 beds. Supervision Dr Badar-us-Saman / Dr Rana Imran (2 months)
PICU: Paediatric ICU, 8 beds. Prof Iqbal Memon / Dr Naeem (2 months)

Credits distribution semester wise
On-job assignments (practical) are the main component of the credit distribution. Students of the MCCM will be recruited as Post Graduate trainees in the department of Critical Care Medicine. Students will be following the regular shift duties (morning 6 hours, evening 6 hours, night 12 hours). It is considered that 2/3 of the time of shift duties are dedicated to the learning process and skills development at the bedside under supervision resulting in a total of 11 credit hours per semester (48 hours of practical equivalent to one credit). The formal classroom teaching is the second component of credit distribution with 12 modules. Each teaching module is divided in 8 teaching hours corresponding to 0.5 credits (16 hours of formal teaching equivalent to one credit). Dissertation is the third component of credit distribution, based on a clinical research work or a review of the literature based on case reports. The dissertation is done under the supervision and guidance of one of the faculties of the Critical Care Medicine Department. Dissertation topic is selected at the end of the second semester, research and writing work will be performed during the 3rd and 4th semester.
1st semester 2nd semester 3rd semester 4th semester
Practical 11 credits 11 credits 11 credits 11 credits
Teaching modules 1.5 credits 1.5 credits 1.5 credits 1.5 credits
Dissertation 5 credits 5 credits
Total / semester 12.5 credits 12.5 credits 17.5 credits 17.5 credits
Total Master 60 credits
Learning resources
1. Textbook and medical journals � Mitchell P. Fink, Edward Abraham, Jean-Louis Vincent, Patrick Kodrank.
Textbook of Critical Care Medicine 5th edition 2005. Elsevier edition. Available at PIMS library
� Journal Intensive Care Medicine. Online edition available on Springerlink edition database trough HEC digital library accessible at PIMS library and in Medical / Surgical ICU
� Journal Critical Care Medicine. Online edition available in Medical ICU.
� New England Journal of Medicine (videos on procedures, articles relevant to critical care medicine). Free access for Pakistan.
� Chest Journal � Journal of Pakistan Medical Association � Annals of PIMS � Journal of the College of Physicians and Surgeons of Pakistan � Anesthesia, Pain and intensive Care Journal
2. Web based learning resources
� Learning resources classified according to competency domains at www.cobatrice.org (free access)
� Latest state of the art reviews and references at www.uptodate.com (access trough Medical ICU)
� PACT program: available with the membership of the European Society of Intensive Care Medicine (www.esicm.org )
� Wikispace Assessment
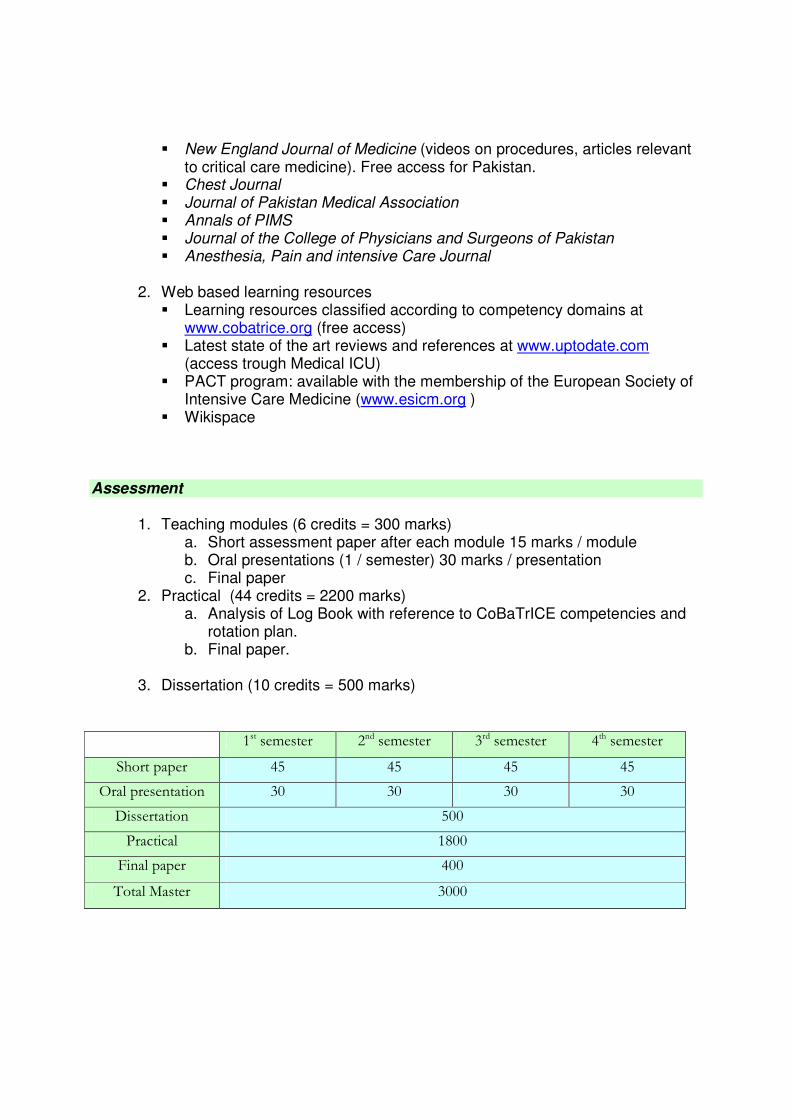
1. Teaching modules (6 credits = 300 marks) a. Short assessment paper after each module 15 marks / module b. Oral presentations (1 / semester) 30 marks / presentation c. Final paper
2. Practical (44 credits = 2200 marks) a. Analysis of Log Book with reference to CoBaTrICE competencies and
rotation plan. b. Final paper.
3. Dissertation (10 credits = 500 marks)
1st semester 2nd semester 3rd semester 4th semester
Short paper 45 45 45 45
Oral presentation 30 30 30 30
Dissertation 500
Practical 1800
Final paper 400
Total Master 3000
The final evaluation of the students will be as per the university terms and regulation. External examiners will be nominated by the Quaid-e-Azam University from its approved list. The minimum passing marks will be 50% for the practical, the dissertation and the final paper. The cumulative minimum marks required for passing the MCCM will be 60%. Terms of reference for the trainers
1. Each teaching hour is divided in 45mn of lecture and 15mn for
questions/answers
2. Lecture should be prepared with reference to the CoBaTrICE curriculum and the competencies relevant to each module. The detailed syllabus provided with this guide should be used to adjust the contents of the lectures.
3. For each teaching hour 5 MCQs should be prepared for the short assessment at the
end of the module. 4. Faculty should provide a list of reference relevant to the topic they are covering
within 2 months before the concerned module (in addition to the references already provided in the trainee’s guide)
5. After lecture delivery, faculty should provide the soft copy of their presentation for
display on the Wikispace designed for trainer/trainee’s interaction.

REFERENCES
Here are references proposed to the students to prepare their teaching modules. They are indicative and non exhaustive. In addition to these, the trainers will give a list of references which are relevant for the concerned module.
MCCM 01 General concepts 1. Kollef MH; Schuster DP. Predicting intensive care unit outcome with scoring systems. Underlying
concepts and principles. Crit Care Clin 1994 Jan; 10(1):1-18.
2. Carson SS; Stocking C; Podsadecki T; Christenson J; Pohlman A; MacRae S; Jordan J; Humphrey H; Siegler M; Hall J. Effects of organizational change in the medical intensive care unit of a teaching hospital: a comparison of 'open' and 'closed' formats. JAMA 1996 Jul 24-31;276(4):322-8.
3. Pronovost PJ; Angus DC; Dorman T; Robinson KA; Dremsizov TT; Young TL. Physician staffing patterns and clinical outcomes in critically ill patients: a systematic review. JAMA 2002 Nov 6; 288(17):2151-62.
4. Cantor MD; Braddock CH 3rd; Derse AR; Edwards DM; Logue GL; Nelson W; Prudhomme AM;
Pearlman RA; Reagan JE; Wlody GS; Fox E. Do-not-resuscitate orders and medical futility. Arch Intern Med 2003 Dec 8-22; 163(22):2689-94.
5. Duke GJ; Green JV; Briedis JH. Night-shift discharge from intensive care unit increases the mortality-
risk of ICU survivors. Anaesth Intensive Care 2004 Oct; 32(5):697-701. 6. Bernat JL. Medical futility: definition, determination, and disputes in critical care. Neurocrit Care.
2005;2(2):198-205. 7. Zimmerman JE; Kramer AA; McNair DS; Malila FM. Acute Physiology and Chronic Health Evaluation
(APACHE) IV: Hospital mortality assessment for today's critically ill patients. Crit Care Med. 2006 May; 34(5):1297-310.
8. Lautrette A; Darmon M; Megarbane B; Joly LM; Chevret S; Adrie C; Barnoud D; Bleichner G; Bruel C;
Choukroun G; Curtis JR; Fieux F; Galliot R; Garrouste-Orgeas M; Georges H; Goldgran-Toledano D; Jourdain M; Loubert G; Reignier J; Saidi F; Souweine B; Vincent F; Barnes NK; Pochard F; Schlemmer B; Azoulay E. A communication strategy and brochure for relatives of patients dying in the ICU. N Engl J Med. 2007 Feb 1; 356(5):469-78.
9. Wall RJ; Engelberg RA; Gries CJ; Glavan B; Curtis JR. Spiritual care of families in the intensive care
unit. Crit Care Med. 2007 Apr; 35(4):1084-90. 10. Wall RJ; Curtis JR; Cooke CR; Engelberg RA. Family Satisfaction in the ICU: Differences between
Families of Survivors and Non survivors. Chest. 2007 Nov; 132(5):1425-33.

MCCM 02 Circulation 1. Kontoyannis DA; Nanas JN; Kontoyannis SA; Stamatelopoulos SF; Moulopoulos SD. Mechanical
ventilation in conjunction with the intra-aortic balloon pump improves the outcome of patients in profound cardiogenic shock. Intensive Care Med 1999 Aug; 25(8):835-8.
2. Merce J; Sagrista-Sauleda J; Permanyer-Miralda G; Evangelista A; Soler-Soler J. Correlation between clinical and Doppler echocardiographic findings in patients with moderate and large pericardial effusion: implications for the diagnosis of cardiac tamponade. Am Heart J 1999 Oct; 138(4 Pt 1):759-64.
3. Guidelines 2000 for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. Part 3: adult basic life support. The American Heart Association in collaboration with the International Liaison Committee on Resuscitation. Circulation 2000; 102:I22.
4. Guidelines 2000 for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. Part 6:
advanced cardiovascular life support: section 1: Introduction to ACLS 2000: overview of recommended changes in ACLS from the guidelines 2000 conference. The American Heart Association in collaboration with the International Liaison Committee on Resuscitation. Circulation 2000; 102:I86.
5. Dorian P; Cass D; Schwartz B; Cooper R; Gelaznikas R; Barr A. Amiodarone as compared with
lidocaine for shock-resistant ventricular fibrillation. N Engl J Med 2002 Mar 21; 346(12):884-90. 6. Kucher N; Goldhaber SZ. Management of massive pulmonary embolism. Circulation 2005 Jul 12;
112(2):e28-32.
7. Babaev A; Frederick PD; Pasta DJ; Every N; Sichrovsky T; Hochman JS. Trends in management and outcomes of patients with acute myocardial infarction complicated by cardiogenic shock. JAMA 2005 Jul 27; 294(4):448-54.
8. Shah MR; Hasselblad V; Stevenson LW; Binanay C; O'Connor CM; Sopko G; Califf RM. Impact of the pulmonary artery catheter in critically ill patients: meta-analysis of randomized clinical trials. JAMA 2005 Oct 5; 294(13):1664-70.
9. Michard F; Teboul JL. Predicting fluid responsiveness in ICU patients: a critical analysis of the
evidence. Chest 2002 Jun; 121(6):2000-8. 10. Hochman JS; Sleeper LA; Webb JG; Dzavik V; Buller CE; Aylward P; Col J; White HD. Early
revascularization and long-term survival in cardiogenic shock complicating acute myocardial infarction. JAMA. 2006 Jun 7; 295(21):2511-5.
MCCM 03 Respiration
1. Pham LH, Brun-Buisson C, Legrand P, Rauss A, Verra F, Brochard L, Lemaire F. Diagnosis of
nosocomial pneumonia in mechanically ventilated patients. Comparison of a plugged telescoping catheter with the protected specimen brush. Am Rev Respir Dis 1991 May; 143(5 Pt 1): 1055-61.
2. Kollef MH; Bock KR; Richards RD; Hearns ML. The safety and diagnostic accuracy of minibronchoalveolar lavage in patients with suspected ventilator-associated pneumonia. Ann Intern Med 1995 May 15;122(10):743-8.
3. Fine MJ; Auble TE; Yealy DM; Hanusa BH; Weissfeld LA; Singer DE; Coley CM; Marrie TJ; Kapoor
WN. A prediction rule to identify low-risk patients with community-acquired pneumonia. N Engl J Med 1997 Jan 23;336(4):243-50.
4. The Acute Respiratory Distress Syndrome Network. Ventilation with lower tidal volumes as compared
with traditional tidal volumes for acute lung injury and the acute respiratory distress syndrome. N Engl J Med 2000 May 4;342(18):1301-8.
5. British Thoracic Society guidelines on diagnostic flexible bronchoscopy. Thorax 2001; 56 Suppl 1:i1.
6. Chastre J, Fagon JY. Ventilator-associated pneumonia. Am J Respir Crit Care Med 2002 Apr 1;
165(7): 867-903. 7. Gacouin A; Le Tulzo Y; Lavoue S; Camus C; Hoff J; Bassen R; Arvieux C; Heurtin C; Thomas R.
Severe pneumonia due to Legionella pneumophila: prognostic factors, impact of delayed appropriate antimicrobial therapy. Intensive Care Med 2002 Jun;28(6):686-91.
8. Leatherman JW; McArthur C; Shapiro RS. Effect of prolongation of expiratory time on dynamic
hyperinflation in mechanically ventilated patients with severe asthma. Crit Care Med 2004 Jul;32(7):1542-5.
9. Mandell LA; Wunderink RG; Anzueto A; Bartlett JG; Campbell GD; Dean NC; Dowell SF; File TM Jr;
Musher DM; Niederman MS; Torres A; Whitney CG. Infectious Diseases Society of America/American Thoracic Society consensus guidelines on the management of community-acquired pneumonia in adults. Clin Infect Dis. 2007 Mar 1;44 Suppl 2:S27-72.
10. Mercat A; Richard JC; Vielle B; Jaber S; Osman D; Diehl JL; Lefrant JY; Prat G; Richecoeur J;
Nieszkowska A; Gervais C; Baudot J; Bouadma L; Brochard L. Positive end-expiratory pressure setting in adults with acute lung injury and acute respiratory distress syndrome: a randomized controlled trial. JAMA. 2008 Feb 13;299(6):646-55.
MCCM 04 Metabolic disturbances and renal failure 1. Adrogue HJ; Madias NE. Management of life-threatening acid-base disorders. N Engl J Med 1998 Jan
1;338(1):26-34.
2. Gennari FJ. Hypokalemia. N Engl J Med 1998 Aug 13; 339(7):451-8.
3. Forni LG; McKinnon W; Hilton PJ. Unmeasured anions in metabolic acidosis: unraveling the mystery. Crit Care. 2006; 10(4):220.
4. Sterns RH; Silver SM. Brain volume regulation in response to hypo-osmolality and its correction. Am J
Med. 2006 Jul; 119(7 Suppl 1):S12-6. 5. Bellomo R. Do we know the optimal dose for renal replacement therapy in the intensive care unit ?
Kidney Int. 2006 Oct; 70(7):1202-4. 6. Vinsonneau C; Camus C; Combes A; Costa de Beauregard MA; Klouche K; Boulain T; Pallot JL;
Chiche JD; Taupin P; Landais P; Dhainaut JF. Continuous venovenous haemodiafiltration versus intermittent haemodialysis for acute renal failure in patients with multiple-organ dysfunction syndrome: a multicentre randomised trial. Lancet. 2006 Jul 29; 368(9533):379-85.
7. Liu KD; Himmelfarb J; Paganini E; Ikizler TA; Soroko SH; Mehta RL; Chertow GM. Timing of initiation of dialysis in critically ill patients with acute kidney injury. Clin J Am Soc Nephrol. 2006 Sep; 1(5):915-9.
8. Verbalis JG; Goldsmith SR; Greenberg A; Schrier RW; Sterns RH. Hyponatremia treatment guidelines
2007: expert panel recommendations. Am J Med. 2007 Nov; 120(11 Suppl 1):S1-21. 9. Montague BT; Ouellette JR; Buller GK. Retrospective review of the frequency of ECG changes in
hyperkalemia. Clin J Am Soc Nephrol. 2008 Mar; 3(2):324-30. 10. Brunkhorst FM; Engel C; Bloos F; Meier-Hellmann A; Ragaller M; Weiler N; Moerer O; Gruendling M;
Oppert M; Grond S; Olthoff D; Jaschinski U; John S; Rossaint R; Welte T; Schaefer M; Kern P; Kuhnt E; Kiehntopf M; Hartog C; Natanson C; Loeffler M; Reinhart K. Intensive insulin therapy and pentastarch resuscitation in severe sepsis. N Engl J Med. 2008 Jan 10; 358(2):125-39.
MCCM 05 Neurology 1. Gajdos P; Chevret S; Clair B; Tranchant C; Chastang C. Clinical trial of plasma exchange and high-
dose intravenous immunoglobulin in myasthenia gravis. Myasthenia Gravis Clinical Study Group. Ann Neurol 1997 Jun;41(6):789-96.
2. Raphael JC; Chevret S; Hughes RA; Annane D. Plasma exchange for Guillain-Barre syndrome. Cochrane Database Syst Rev 2002; (2):CD001798.
3. Stocchetti N; Maas AI; Chieregato A; van der Plas AA. Hyperventilation in head injury: a review. Chest 2005 May; 127(5):1812-27.
4. Edwards P; Arango M; Balica L; Cottingham R; El-Sayed H; Farrell B; Fernandes J; Gogichaisvili T;
Golden N; Hartzenberg B; Husain M; Ulloa MI; Jerbi Z; Khamis H; Komolafe E; Laloe V; Lomas G; Ludwig S; Mazairac G; Munoz Sanchez Mde L; Nasi L; Olldashi F; Plunkett P; Roberts I; Sandercock P; Shakur H; Soler C; Stocker R; Svoboda P; Trenkler S; Venkataramana NK; Wasserberg J; Yates D; Yutthakasemsunt S. Final results of MRC CRASH, a randomised placebo-controlled trial of intravenous corticosteroid in adults with head injury-outcomes at 6 months. Lancet 2005 Jun 21; 365(9475):1957-9.
5. Dondorp A; Nosten F; Stepniewska K; Day N; White N. Artesunate versus quinine for treatment of
severe falciparum malaria: a randomised trial. Lancet 2005 Aug 27-Sep 2; 366(9487):717-25. 6. Hughes RA; Raphael JC; Swan AV; van Doorn PA. Intravenous immunoglobulin for Guillain-Barre
syndrome. Cochrane Database Syst Rev. 2006 Jan 25;(1):CD002063. 7. Naval NS; Stevens RD; Mirski MA; Bhardwaj A. Controversies in the management of aneurysmal
subarachnoid hemorrhage. Crit Care Med. 2006 Feb;34(2):511-24. 8. Einhaupl K; Bousser MG; de Bruijn SF; Ferro JM; Martinelli I; Masuhr F; Stam J. EFNS guideline on
the treatment of cerebral venous and sinus thrombosis. Eur J Neurol. 2006 Jun;13(6):553-9. 9. Mai NT; Chau TT; Thwaites G; Chuong LV; Sinh DX; Nghia HD; Tuan PQ; Phong ND; Phu NH; Diep
TS; Chau NV; Duong NM; Campbell J; Schultsz C; Parry C; Torok ME; White N; Chinh NT; Hien TT; Stepniewska K; Farrar JJ. Dexamethasone in Vietnamese adolescents and adults with bacterial meningitis. N Engl J Med. 2007 Dec 13;357(24):2431-2440.

10. Rosenthal PJ. Artesunate for the treatment of severe falciparum malaria. N Engl J Med. 2008 Apr 24; 358(17):1829-36.
MCCM 06 Abdomen 1. Gianino S; St.John RE. Nutritional assessment of the patient in the intensive care unit. Crit Care Nurs
Clin North Am 1993 Mar; 5(1):1-16.
2. Heyland DK; Dhaliwal R; Drover JW; Gramlich L; Dodek P. Canadian clinical practice guidelines for nutrition support in mechanically ventilated, critically ill adult patients. JPEN J Parenter Enteral Nutr. 2003 Sep-Oct; 27(5):355-73.
3. Runyon BA. Management of adult patients with ascites due to cirrhosis. Hepatology 2004 Mar;
39(3):841-56. 4. Baradarian R; Ramdhaney S; Chapalamadugu R; Skoczylas L; Wang K; Rivilis S; Remus K; Mayer I;
Iswara K; Tenner S. Early intensive resuscitation of patients with upper gastrointestinal bleeding decreases mortality. Am J Gastroenterol 2004 Apr; 99(4):619-22.
5. Runzi M; Niebel W; Goebell H; Gerken G; Layer P. Severe acute pancreatitis: nonsurgical treatment
of infected necroses. Pancreas 2005 Apr; 30(3):195-9. 6. Polson J; Lee WM. AASLD position paper: the management of acute liver failure. Hepatology. 2005
May; 41(5):1179-97. 7. Lau JY; Leung WK; Wu JC; Chan FK; Wong VW; Chiu PW; Lee VW; Lee KK; Cheung FK; Siu P; Ng
EK; Sung JJ. Omeprazole before endoscopy in patients with gastrointestinal bleeding. N Engl J Med. 2007 Apr 19; 356(16):1631-40.
8. Forsmark CE; Baillie J. AGA Institute Technical Review on Acute Pancreatitis. Gastroenterology. 2007
May; 132(5):2022-44. 9. Garcia-Tsao G; Sanyal AJ; Grace ND; Carey W. Prevention and management of gastroesophageal
varices and variceal hemorrhage in cirrhosis. Hepatology. 2007 Sep; 46(3):922-38. 10. Zar FA; Bakkanagari SR; Moorthi KM; Davis MB. A comparison of vancomycin and metronidazole for
the treatment of Clostridium difficile-associated diarrhea, stratified by disease severity. Clin Infect Dis. 2007 Aug 1; 45(3):302-7. Epub 2007 Jun 19.
MCCM 07 Infections, coagulation and immunosuppression 1. Trujillo MH; Castillo A; Espana J; Manzo A; Zerpa R. Impact of intensive care management on the
prognosis of tetanus. Analysis of 641 cases. Chest. 1987 Jul; 92(1):63-5.
2. Jorgensen JH; Ferraro MJ. Antimicrobial susceptibility testing: general principles and contemporary practices. Clin Infect Dis 1998 Apr; 26(4):973-80.

3. Pittet D; Hugonnet S; Harbarth S; Mourouga P; Sauvan V; Touveneau S; Perneger TV. Effectiveness of a hospital-wide programme to improve compliance with hand hygiene. Infection Control Programme. Lancet 2000 Oct 14; 356(9238):1307-12.
4. Ryan M; Levy MM. Clinical review: fever in intensive care unit patients. Crit Care 2003 Jun; 7(3):221-
5.
5. Rutala WA; Weber DJ. Disinfection and sterilization in health care facilities: what clinicians need to know. Clin Infect Dis 2004 Sep 1; 39(5):702-9.
6. Walsh TS; Garrioch M; Maciver C; Lee RJ; MacKirdy F; McClelland DB; Kinsella J; Wallis C. Red cell
requirements for intensive care units adhering to evidence-based transfusion guidelines. Transfusion 2004 Oct; 44(10):1405-11.
7. Jacoby GA; Munoz-Price LS. The new beta-lactamases. N Engl J Med 2005 Jan 27; 352(4):380-91. 8. Levy MM; Abraham E; Zilberberg M; MacIntyre NR. A descriptive evaluation of transfusion practices in
patients receiving mechanical ventilation. Chest 2005 Mar; 127(3):928-35.
9. Thwaites CL; Yen LM; Loan HT; Thuy TT; Thwaites GE; Stepniewska K; Soni N; White NJ; Farrar JJ. Magnesium sulphate for treatment of severe tetanus: a randomised controlled trial. Lancet. 2006 Oct 21; 368(9545):1436-43.
10. Dellinger RP; Levy MM; Carlet JM; Bion J; Parker MM; Jaeschke R; Reinhart K; Angus DC; Brun-
Buisson C; Beale R; Calandra T; Dhainaut JF; Gerlach H; Harvey M; Marini JJ; Marshall J; Ranieri M; Ramsay G; Sevransky J; Thompson BT; Townsend S; Vender JS; Zimmerman JL; Vincent JL. Surviving Sepsis Campaign: International guidelines for management of severe sepsis and septic shock: 2008. Crit Care Med. 2008 Jan; 36(1):296-327.
MCCM 08 Toxicology 1. Chyka PA; Seger D. Position statement: single-dose activated charcoal. American Academy of
Clinical Toxicology; European Association of Poisons Centres and Clinical Toxicologists. J Toxicol Clin Toxicol 1997; 35(7):721-41.
2. Ernst A; Zibrak JD. Carbon monoxide poisoning. N Engl J Med 1998 Nov 26; 339(22):1603-8.
3. Brent J; McMartin K; Phillips S; Aaron C; Kulig K. Fomepizole for the treatment of methanol poisoning. N Engl J Med 2001 Feb 8; 344(6):424-9.
4. Mokhlesi B; Leiken J; Murray P; Corbridge T. Adult Toxicology in Critical Care. Part I. Chest 2003; 123(2):577-92.
5. Mokhlesi B; Leiken J; Murray P; Corbridge T. Adult Toxicology in Critical Care. Part II. Chest 2003; 123(3):897-922.
6. Eyer P. The role of oximes in the management of organophosphorus pesticide poisoning. Toxicol Rev
2003; 22(3):165-90. 7. Eddleston M; Phillips MR. Self poisoning with pesticides. BMJ 2004 Jan 3; 328(7430):42-4. 8. Vale JA; Kulig K. Position paper: gastric lavage. J Toxicol Clin Toxicol 2004; 42(7):933-43.

9. Pawar KS; Bhoite RR; Pillay CP; Chavan SC; Malshikare DS; Garad SG. Continuous pralidoxime infusion versus repeated bolus injection to treat organophosphorus pesticide poisoning: a randomised controlled trial. Lancet. 2006 Dec 16; 368(9553):2136-41.
10. Paasma R; Hovda KE; Tikkerberi A; Jacobsen D. Methanol mass poisoning in Estonia: outbreak in
154 patients. Clin Toxicol (Phila). 2007; 45(2):152-7.
MCCM 09 Trauma, pre and post-operative care 1. Marik PE; Varon J; Trask T. Management of head trauma. Chest 2002 Aug; 122(2):699-711.
2. Richards CF; Mayberry JC. Initial management of the trauma patient. Crit Care Clin 2004 Jan; 20(1):1-
11. 3. Wanek S; Mayberry JC. Blunt thoracic trauma: flail chest, pulmonary contusion, and blast injury. Crit
Care Clin 2004 Jan; 20(1):71-81.
4. Parr MJ; Alabdi T. Damage control surgery and intensive care. Injury 2004 Jul; 35(7):713-22. 5. Rose JS. Ultrasound in abdominal trauma. Emerg Med Clin North Am 2004 Aug; 22(3):581-99, vii. 6. Wood KE; Becker BN; McCartney JG; D'Alessandro AM; Coursin DB. Care of the potential organ
donor. N Engl J Med 2004 Dec 23; 351(26):2730-9. 7. DeLoughery TG. Coagulation defects in trauma patients: etiology, recognition, and therapy. Crit Care
Clin 2004 Jan; 20(1):13-24. 8. Edouard AR; Vanhille E; Le Moigno S; Benhamou D; Mazoit JX. Non-invasive assessment of cerebral
perfusion pressure in brain injured patients with moderate intracranial hypertension. Br J Anaesth 2005 Feb; 94(2):216-21.
9. Sugrue M. Abdominal compartment syndrome. Curr Opin Crit Care 2005 Aug; 11(4):333-8. 10. Schwartz D; Amir L; Dichter R; Figenberg Z. The use of a powered device for intraosseous drug and
fluid administration in a national EMS: a 4-year experience. J Trauma. 2008 Mar; 64(3):650-4; discussion 654-5.
MCCM 10 Emergencies
1. Bouchama A; Knochel JP. Heat stroke. N Engl J Med 2002 Jun 20; 346(25):1978-88.
2. Gold BS; Dart RC; Barish RA. Bites of venomous snakes. N Engl J Med 2002 Aug 1; 347(5):347-56.
3. Miller K; Chang A. Acute inhalation injury. Emerg Med Clin North Am 2003 May; 21(2):533-57. 4. Kempainen RR; Brunette DD. The evaluation and management of accidental hypothermia. Respir
Care 2004 Feb; 49(2):192-205.
5. Salomez F; Vincent JL. Drowning: a review of epidemiology, pathophysiology, treatment and prevention. Resuscitation 2004 Dec; 63(3):261-8.
6. Spies C; Trohman RG. Narrative review: Electrocution and life-threatening electrical injuries. Ann
Intern Med. 2006 Oct 3; 145(7):531-7. 7. Namias N. Advances in burn care. Curr Opin Crit Care. 2007 Aug; 13(4):405-10. 8. Mulvey JM; Awan SU; Qadri AA; Maqsood MA. Profile of injuries arising from the 2005 Kashmir
earthquake: the first 72 h. Injury 2008 May; 39(5):554-60. 9. Simpson ID. A study of the current knowledge base in treating snake bite amongst doctors in the high-
risk countries of India and Pakistan: does snake bite treatment training reflect local requirements? Trans R Soc Trop Med Hyg; 2008 Nov; 102(11):1108-14.
10. Crabtree J. Terrorist homicide bombings: a primer for preparation. J Burn Care Res 2006 Sep-Oct;
27(5):576-88.
MCCM 11 Pregnancy 1. Clark SL; Hankins GD; Dudley DA; Dildy GA; Porter TF. Amniotic fluid embolism: analysis of the
national registry. Am J Obstet Gynecol 1995 Apr; 172(4 Pt 1):1158-67; discussion 1167-9.
2. Usta IM; Sibai BM. Emergent management of puerperal eclampsia. Obstet Gynecol Clin North Am 1995 Jun; 22(2):315-35.
3. de Swiet M. Management of pulmonary embolus in pregnancy. Eur Heart J 1999 Oct; 20(19):1378-85. 4. Sciscione AC; Ivester T; Largoza M; Manley J; Shlossman P; Colmorgen GH. Acute pulmonary
edema in pregnancy. Obstet Gynecol 2003 Mar; 101(3):511-5. 5. Mousa HA; Alfirevic Z. Treatment for primary postpartum haemorrhage. Cochrane Database Syst Rev
2003; (1):CD003249. 6. Duley L; Henderson-Smart D. Magnesium sulphate versus diazepam for eclampsia. Cochrane
Database Syst Rev 2003; (4):CD000127. 7. Sibai BM. Diagnosis, controversies, and management of the syndrome of hemolysis, elevated liver
enzymes, and low platelet count. Obstet Gynecol 2004 May; 103(5 Pt 1):981-91. 8. Matchaba P; Moodley J. Corticosteroids for HELLP syndrome in pregnancy. Cochrane Database Syst
Rev 2004; (1): CD002076. 9. Selo-Ojeme DO; Omosaiye M; Battacharjee P; Kadir RA. Risk factors for obstetric admissions to the
intensive care unit in a tertiary hospital: a case-control study. Arch Gynecol Obstet. 2005 Sep; 272(3):207-10.
10. Burtelow M; Riley E; Druzin M; Fontaine M; Viele M; Goodnough LT. How we treat: management of
life-threatening primary postpartum hemorrhage with a standardized massive transfusion protocol. Transfusion. 2007 Sep;47(9):1564-72.
MCCM 12 Pediatrics
1. King BR; Baker MD; Braitman LE; Seidl-Friedman J; Schreiner MS. Endotracheal tube selection in children: a comparison of four methods. Ann Emerg Med. 1993 Mar;22(3):530-4.
2. Gagliardi L; Rusconi F. Respiratory rate and body mass in the first three years of life. The working party on respiratory rate. Arch Dis Child. 1997 Feb;76(2):151-4.
3. Werner HA. Status asthmaticus in children: a review. Chest. 2001 Jun;119(6):1913-29. 4. Walker RW. Management of the difficult airway in children. J R Soc Med. 2001 Jul;94(7):341-4. 5. Newth CJ; Rachman B; Patel N; Hammer J. The use of cuffed versus uncuffed endotracheal tubes in
pediatric intensive care. J Pediatr. 2004 Mar;144(3):333-7. 6. Holliday MA; Friedman AL; Segar WE; Chesney R; Finberg L. Acute hospital-induced hyponatremia in
children: a physiologic approach. J Pediatr 2004 Nov;145(5):584-7. 7. Jain L; Dudell GG. Respiratory transition in infants delivered by cesarean section. Semin Perinatol.
2006 Oct;30(5):296-304. 8. DuBois D; Baldwin S; King WD. Accuracy of weight estimation methods for children. Pediatr Emerg
Care. 2007 Apr;23(4):227-30. 9. Cherry JD. Clinical practice. Croup. N Engl J Med. 2008 Jan 24;358(4):384-91. 10. Friedman AL; Ray PE. Maintenance fluid therapy: what it is and what it is not. Pediatr Nephrol. 2008
May;23(5):677-680.
COMPETENCIES IN RELATION TO TEACHING MODULES Here are listed the competencies related to each teaching module. A competency is a combination of skills, knowledge and attitudes acquired both during teaching modules and ICU rotations. MCCM 01 General concepts ���� Resuscitation and initial management of the acutely ill patient
− Adopts a structured and timely approach to the recognition, assessment and stabilization of the acutely ill patient with disordered physiology
− Triages and prioritizes patients appropriately, including timely admission to ICU ���� Diagnosis: assessment, investigation, monitoring and data interpretation
− Obtains a history and performs an accurate clinical examination
− Undertakes timely and appropriate investigations
− Liaises with radiologists to organize and interpret clinical imaging
− Monitors and responds to trends in physiological variables
− Integrates clinical findings with laboratory investigations to form a differential diagnosis ���� Therapeutic interventions / organ system support in single or multiple organ failure
− Prescribes drugs and therapies safely ���� Comfort and recovery
− Manages the safe and timely discharge of patients from the ICU
− Identifies and attempts to minimize the physical and psychosocial consequences of critical illness for patients and families
− Manages the assessment, prevention and treatment of pain and delirium
− Communicates the continuing care requirements of patients at ICU discharge to health care professionals, patients and relatives
���� End of life care
− Manages the process of withholding or withdrawing treatment with the multidisciplinary team
− Discusses end of life care with patients and their families / surrogates
− Manages palliative care of the critically ill patient ���� Patient safety and health systems management
− Leads a daily multidisciplinary ward round
− Complies with local infection control measures
− Identifies environmental hazards and promotes safety for patients & staff
− Identifies and minimizes risk of critical incidents and adverse events, including complications of critical illness
− Critically appraises and applies guidelines, protocols and care bundles
− Organizes a case conference
− Critically appraises and applies guidelines, protocols and care bundles
− Describes commonly used scoring systems for assessment of severity of illness, case mix and workload
− Demonstrates an understanding of the managerial & administrative responsibilities of the ICM specialist

���� Professionalism
− Collaborates and consults; promotes team-working
− Ensures continuity of care through effective hand-over of clinical information
− Supports clinical staff outside the ICU to enable the delivery of effective care
− Appropriately supervises, and delegates to others, the delivery of patient care
− Takes responsibility for safe patient care
− Seeks learning opportunities and integrates new knowledge into clinical practice
− Communicates effectively with patients and relatives
− Communicates effectively with members of the health care team
− Maintains accurate and legible records / documentation
− Involves patients (or their surrogates if applicable) in decisions about care and treatment
− Demonstrates respect of cultural and religious beliefs and an awareness of their impact on decision making
− Respects privacy, dignity, confidentiality and legal constraints on the use of patient data
− Formulates clinical decisions with respect for ethical and legal principles
− Participates in multidisciplinary teaching
− Participates in research or audit under supervision
MCCM 02 Circulation ���� Resuscitation and initial management of the acutely ill patient
− Adopts a structured and timely approach to the recognition, assessment and stabilization of the acutely ill patient with disordered physiology
− Manages cardiopulmonary resuscitation
− Manages the patient post-resuscitation
���� Diagnosis: assessment, investigation, monitoring and data interpretation
− Obtains a history and performs an accurate clinical examination
− Undertakes timely and appropriate investigations
− Describes indications for echocardiography (transthoracic / transoesophageal)
− Performs electrocardiography (ECG / EKG) and interprets the results
− Obtains appropriate microbiological samples and interprets results
− Monitors and responds to trends in physiological variables
− Integrates clinical findings with laboratory investigations to form a differential diagnosis ���� Disease management
− Manages the care of the critically ill patient with specific acute medical conditions
− Identifies the implications of chronic and co-morbid disease in the acutely ill patient
− Recognizes and manages the patient with circulatory failure
− Recognizes and manages the septic patient ���� Therapeutic interventions / organ system support in single or multiple organ failure
− Prescribes drugs and therapies safely
− Manages antimicrobial drug therapy
− Administers blood and blood products safely
− Uses fluids and vasoactive / inotropic drugs to support the circulation
− Describes the use of mechanical assist devices to support the circulation ���� Practical procedures
− Performs peripheral venous catheterization
− Performs arterial catheterization

− Describes a method for surgical isolation of vein / artery
− Describes ultrasound techniques for vascular localization
− Performs central venous catheterization
− Performs defibrillation and cardio version
− Performs cardiac pacing (transvenous or transthoracic)
− Describes how to perform pericardiocentesis
− Demonstrates a method for measuring cardiac output and derived haemodynamic variables
���� Patient safety and health systems management
− Critically appraises and applies guidelines, protocols and care bundles
MCCM 03 Respiration ���� Resuscitation and initial management of the acutely ill patient
- Adopts a structured and timely approach to the recognition, assessment and stabilization of the acutely ill patient with disordered physiology
���� Diagnosis: assessment, investigation, monitoring and data interpretation - Obtains a history and performs an accurate clinical examination - Undertakes timely and appropriate investigations - Obtains appropriate microbiological samples and interprets results - Obtains and interprets the results from blood gas samples - Interprets chest x-rays - Monitors and responds to trends in physiological variables - Integrates clinical findings with laboratory investigations to form a differential diagnosis
���� Disease management - Manages the care of the critically ill patient with specific acute medical conditions - Identifies the implications of chronic and co-morbid disease in the acutely ill patient - Recognizes and manages the patient with acute lung injury syndromes (ALI / ARDS)
���� Therapeutic interventions / organ system support in single or multiple organ failure
- Prescribes drugs and therapies safely - Manages antimicrobial drug therapy - Initiates, manages, and weans patients from invasive and non-invasive ventilatory support
���� Practical procedures
- Administers oxygen using a variety of administration devices - Performs fibreoptic laryngoscopy under supervision - Performs emergency airway management - Performs difficult and failed airway management according to local protocols - Performs endotracheal suction - Performs fibreoptic bronchoscopy and BAL in the intubated patient under supervision - Performs percutaneous tracheostomy under supervision - Performs thoracocentesis via a chest drain
���� Comfort and recovery
- Manages sedation and neuromuscular blockade
���� Transport - Undertakes transport of the mechanically ventilated critically ill patient outside the ICU
���� Patient safety and health systems management
- Critically appraises and applies guidelines, protocols and care bundles
MCCM 04 Metabolic disturbances and renal failure ���� Resuscitation and initial management of the acutely ill patient
- Adopts a structured and timely approach to the recognition, assessment and stabilization of the acutely ill patient with disordered physiology
���� Diagnosis: assessment, investigation, monitoring and data interpretation
- Obtains a history and performs an accurate clinical examination - Undertakes timely and appropriate investigations - Performs electrocardiography (ECG / EKG) and interprets the results - Obtains and interprets the results from blood gas samples2.9 Monitors and responds to
trends in physiological variables ���� Disease management
- Manages the care of the critically ill patient with specific acute medical conditions ���� Therapeutic interventions / organ system support in single or multiple organ failure
- Initiates, manages and weans patients from renal replacement therapy - Recognizes and manages electrolyte, glucose and acid-base disturbances - Co-ordinates and provides nutritional assessment and support
���� Practical procedures
- Performs central venous catheterization - Performs urinary catheterization
MCCM 05 Neurology
���� Resuscitation and initial management of the acutely ill patient
- Adopts a structured and timely approach to the recognition, assessment and stabilization of the acutely ill patient with disordered physiology
���� Diagnosis: assessment, investigation, monitoring and data interpretation
- Obtains a history and performs an accurate clinical examination - Undertakes timely and appropriate investigations - Obtains appropriate microbiological samples and interprets results - Liaises with radiologists to organize and interpret clinical imaging - Monitors and responds to trends in physiological variables - Integrates clinical findings with laboratory investigations to form a differential diagnosis
���� Disease management
- Manages the care of the critically ill patient with specific acute medical conditions - Identifies the implications of chronic and co-morbid disease in the acutely ill patient - Recognizes and manages the patient with neurological impairment

���� Therapeutic interventions / organ system support in single or multiple organ failure
- Prescribes drugs and therapies safely - Manages antimicrobial drug therapy
���� Practical procedures
- Performs lumbar puncture (intramural / 'spinal') under supervision - Manages the administration of analgesia via an epidural catheter
���� Peri-operative care
- Manages the care of the patient following craniotomy under supervision ���� Comfort and recovery
- Manages the assessment, prevention and treatment of pain and delirium - Manages sedation and neuromuscular blockade
���� End of life care
- Performs brain-stem death testing - Manages the physiological support of the organ donor
���� Patient safety and health systems management
- Critically appraises and applies guidelines, protocols and care bundles
MCCM 06 Abdomen
���� Resuscitation and initial management of the acutely ill patient
- Adopts a structured and timely approach to the recognition, assessment and stabilisation of the acutely ill patient with disordered physiology
���� Diagnosis: assessment, investigation, monitoring and data interpretation
- Undertakes timely and appropriate investigations - Monitors and responds to trends in physiological variables
���� Disease management
- Manages the care of the critically ill patient with specific acute medical conditions - Identifies the implications of chronic and co-morbid disease in the acutely ill patient - Recognizes and manages the patient with, or at risk of, acute liver failure - Recognizes and manages the patient with acute gastrointestinal failure
���� Therapeutic interventions / organ system support in single or multiple organ failure
- Administers blood and blood products safely - Co-ordinates and provides nutritional assessment and support
���� Practical procedures
- Performs nasogastric tube placement - Performs abdominal paracentesis - Describes Sengstaken tube (or equivalent) placement - Describes indications for, and safe conduct of gastroscopy
���� Peri-operative care
- Manages the pre- and post-operative care of the high risk surgical patient

MCCM 07 Infections, coagulation and immunosuppression
���� Resuscitation and initial management of the acutely ill patient
- Adopts a structured and timely approach to the recognition, assessment and stabilization of the acutely ill patient with disordered physiology
���� Diagnosis: assessment, investigation, monitoring and data interpretation
- Obtains appropriate microbiological samples and interprets results - Monitors and responds to trends in physiological variables
���� Disease management
- Manages the care of the critically ill patient with specific acute medical conditions - Recognizes and manages the patient with circulatory failure - Recognizes and manages the septic patient
���� Therapeutic interventions / organ system support in single or multiple organ failure
- Manages antimicrobial drug therapy - Uses fluids and vasoactive / inotropic drugs to support the circulation
���� Practical procedures
- Performs arterial catheterization - Describes ultrasound techniques for vascular localisation - Performs central venous catheterization - Performs lumbar puncture (intradural / 'spinal') under supervision
���� Patient safety and health systems management
- Complies with local infection control measures - Identifies environmental hazards and promotes safety for patients & staff - Critically appraises and applies guidelines, protocols and care bundles
MCCM 08 Toxicology
���� Resuscitation and initial management of the acutely ill patient
- Adopts a structured and timely approach to the recognition, assessment and stabilization of the acutely ill patient with disordered physiology
���� Diagnosis: assessment, investigation, monitoring and data interpretation
- Undertakes timely and appropriate investigations - Monitors and responds to trends in physiological variables
���� Disease management
- Manages the care of the critically ill patient with specific acute medical conditions - Recognizes and manages the patient with circulatory failure - Recognizes and manages the patient with, or at risk of, acute renal failure - Recognizes and manages the patient with, or at risk of, acute liver failure - Recognizes and manages the patient with neurological impairment - Recognizes and manages the patient with acute lung injury syndromes (ALI / ARDS) - Recognizes and manages the patient following intoxication with drugs or environmental
toxins

���� Therapeutic interventions / organ system support in single or multiple organ failure - Prescribes drugs and therapies safely - Describes the use of mechanical assist devices to support the circulation - Initiates, manages and weans patients from renal replacement therapy
���� Comfort and recovery
- Identifies and attempts to minimize the physical and psychosocial consequences of critical illness for patients and families
���� Professionalism
- Communicates effectively with patients and relatives
MCCM 09 Trauma, pre and post-operative care
���� Resuscitation and initial management of the acutely ill patient
- Adopts a structured and timely approach to the recognition, assessment and stabilization of the acutely ill patient with disordered physiology
- Assesses and provides initial management of the trauma patient ���� Diagnosis: assessment, investigation, monitoring and data interpretation
- Undertakes timely and appropriate investigations - Liaises with radiologists to organize and interpret clinical imaging - Monitors and responds to trends in physiological variables
���� Disease management - Recognizes and manages the patient with circulatory failure
���� Therapeutic interventions / organ system support in single or multiple organ failure
- Administers blood and blood products safely - Uses fluids and vasoactive / inotropic drugs to support the circulation
���� Practical procedures
- Performs difficult and failed airway management according to local protocols - Describes how to perform pericardiocentesis - Manages the administration of analgesia via an epidural catheter
���� Peri-operative care
- Manages the pre- and post-operative care of the high risk surgical patient - Manages the care of the patient following cardiac surgery under supervision - Manages the care of the patient following craniotomy under supervision - Manages the care of the patient following solid organ transplantation under supervision - Manages the pre- and post-operative care of the trauma patient under supervision
���� Comfort and recovery
- Manages the assessment, prevention and treatment of pain and delirium ���� End of life
- Performs brain-stem death testing - Manages the physiological support of the organ donor

����Transport - Undertakes transport of the mechanically ventilated critically ill patient outside the ICU
MCCM 10 Emergencies
���� Resuscitation and initial management of the acutely ill patient
- Adopts a structured and timely approach to the recognition, assessment and stabilisation of the acutely ill patient with disordered physiology
- Manages cardiopulmonary resuscitation - Manages the patient post-resuscitation - Triages and prioritises patients appropriately, including timely admission to ICU - Describes the management of mass casualties - Assesses and provides initial management of the patient with burns
���� Diagnosis: assessment, investigation, monitoring and data interpretation
- Monitors and responds to trends in physiological variables ���� Disease management
- Manages the care of the critically ill patient with specific acute medical conditions
���� Transport
- Undertakes transport of the mechanically ventilated critically ill patient outside the ICU
MCCM 11 Pregnancy
���� Resuscitation and initial management of the acutely ill patient
- Adopts a structured and timely approach to the recognition, assessment and stabilization of the acutely ill patient with disordered physiology
���� Diagnosis: assessment, investigation, monitoring and data interpretation
- Monitors and responds to trends in physiological variables ���� Disease management
- Manages the care of the critically ill patient with specific acute medical conditions - Recognizes life-threatening maternal peripartum complications and manages care under
supervision ���� Therapeutic interventions / organ system support in single or multiple organ failure
- Prescribes drugs and therapies safely ���� Practical procedures
- Performs emergency airway management - Performs difficult and failed airway management according to local protocols - Manages the administration of analgesia via an epidural catheter
MCCM 12 Pediatrics ���� Resuscitation and initial management of the acutely ill patient
- Adopts a structured and timely approach to the recognition, assessment and stabilisation of the acutely ill patient with disordered physiology
���� Diagnosis: assessment, investigation, monitoring and data interpretation
- Obtains a history and performs an accurate clinical examination - Undertakes timely and appropriate investigations - Monitors and responds to trends in physiological variables - Integrates clinical findings with laboratory investigations to form a differential diagnosis
���� Disease management - Manages the care of the critically ill patient with specific acute medical conditions
���� Therapeutic interventions / organ system support in single or multiple organ failure
- Prescribes drugs and therapies safely - Co-ordinates and provides nutritional assessment and support
���� Pediatric care
- Describes the recognition of the acutely ill child and initial management of paediatric emergencies
- Describes national legislation and guidelines relating to child protection and their relevance to critical care
���� Professionalism
- Communicates effectively with patients and relatives
GUIDELINES FOR DISSERTATION These guidelines have been customized from those proposed by the Intercollegiate Board for Training in Intensive Care Medicine, UK. The dissertation topic must be discussed first with a dissertation supervisor selected among the faculty of Critical Care Medicine. The dissertation must be written by the candidate. Whilst the candidate is expected to seek advice and help, the final dissertation must be the work of the candidate and the dissertation must be single author. The intention of the synopsis is to provide the examiners with an opportunity to ensure that the dissertation is in an appropriate subject area and of adequate depth and breadth for the examination. To do this the examiners need adequate information to make an assessment of what the candidate is intending to produce. In general terms the dissertation may be:
− Review - it does not need to be a 'systematic review' but if it is described as such it should conform to that definition.
− Research paper - it must be of adequate substance and quality to be publishable, with a full and appropriate discussion. In particular, as the research may be limited in nature, the discussion should encompass the general area within which the research is relevant so it constitutes a review of the subject matter.
− Audit - if an audit is to be used it must provide a full introduction and full discussion of the subject matter being audited, as with a research based paper.
���� The synopsis The synopsis must not exceed 700 words – It should be structured as follows: First page:
− Title of dissertation
− Candidate’s name
− Name of supervisor
− Name of department and university Second page:
− Define the dissertation topic.
− Outline the limits of the subject to be addressed. In apparently narrow topics this may require emphasis on the scope of the topic while in massive topics it may require demonstration of the specific area that will be focused upon.

− Technique that will be used to research the literature on the topic. This may but does not necessarily include some of the following:
o Literature search methodology; Electronic Search use, e.g. Medline, Biomed Central and Web of Knowledge. Limits of that search (for example English language articles).
o Specific subtitles that demonstrate the main areas to be covered through the dissertation.
o You may wish to point out areas of exclusion for example specific populations such as adults or children.
− In research based dissertations following a publication style (Introduction, Methods, Results and Discussion) may be more appropriate but there should be an adequate introduction as well as a critical discussion. As in other dissertations, a reasonable standard would be one that is commensurate with publication.
− Conclusions or recommendations that will be sought. The synopsis should be submitted during the 2nd semester of the masters.
Responses to the synopsis The nature of any synopsis is that it only provides an indication of the form of the dissertation. Three outcomes may arise: 1. The examiners may be satisfied with the dissertation and the candidate will proceed. 2. The examiners may overall be satisfied with the synopsis and the candidate may proceed but some of the examiners may have raised questions from their reading of the synopsis that to them suggest areas of potential weakness in the final dissertation. It will provide an opportunity for the candidate and supervisor to modify the plan of the dissertation if they feel it necessary. These comments are intended to be helpful, arise only from the dissertation summary and may or may not be relevant in the full dissertation and that is for the candidate and their supervisor to determine. 3. The final outcome is if the topic or the synopsis suggests the dissertation will not be suitable for this examination. It is important to emphasize that this examination is in Critical Care Medicine and while this is a very broad topic it does not encompass the entirety of medical practice.
���� The dissertation
• Title page
− Title of dissertation
− Candidate’s name
− Name of supervisor
− Name of department and university
• Abstract page For clinical/laboratory investigations:
1. Objective 2. Design

3. Patients/subjects 4. Interventions 5. Measurements and Main Results 6. Conclusions
For review or audit papers: 1. Objective 2. Data Sources 3. Study Selection 4. Data Extraction 5. Data Synthesis 6. Conclusions
• Introduction
• Materials and Methods
• Results
• Discussion This section of the text should interpret the results without unnecessary repetition. References to related studies should be included in this section.
• Acknowledgements
• References Should be cited in sequential order in the text and typed on a separate sheet. Identify references in the text, legends or tables by Arabic numerals in parentheses. Titles of journals should be set in italics and stated in full. Use inclusive page numbers (e.g. pp 1-10) for all references. For guidance on the format, refer to the 6 January 1996 (pp. 41-43) issue of the British Medical Journal (No. 7022, volume 312).
• Tables The tables should be typed single-spaced on a separate page. Each table should have an Arabic number and a descriptive title. Tables must be referenced in sequential order in the text.
• Abbreviations The abbreviations should be identified in a footnote to the table. Footnoted information should be referenced using italicized, superscript, lower case letters, i.e. a,b.
• Figures Figures must be referenced sequentially in the text.

In General
- Manuscripts should be typewritten on white A4 plain paper (21cm x 29.5cm). Typing should be double-spaced with margins of 2.5cm on all sides.
- All pages should be consecutively numbered, beginning with the title page. - All photocopies (including figures, tables and computer print-outs where
appropriate) should be clearly legible. - Avoid the use of abbreviations, except clinically used abbreviations such as acute
respiratory distress syndrome (ARDS), mean arterial pressure (MAP), blood pressure (BP) and heart rate (HR).
- Use SI units where appropriate. Blood pressure should be given in mmHg and ventilation pressures in cmH2O.
Manufacturers Provide in parentheses the model number, name of manufacturer, their city and country, for all equipment used in the paper. Only generic drug names should be used.
Copyright Permission Any submitted material that is to be reproduced (or adapted) from publications protected by copyright must be accompanied by a letter of permission both from the author and the copyright holder.
Guidelines for preparation of the dissertation
1. Candidates are each required to present a dissertation of 4,000 to 6,000 words
(references not included). The aim of the dissertation is to show that the candidate has studied a topic in depth, and has developed skills in analysis, synthesis and evaluation.
2. The standard for a review or research topic should be that which would be found
acceptable, with appropriate editing, for publication in an indexed journal.
3. Dissertations should have a clear structure, specifying the nature of the topic, the reasons for its choice, the areas to be explored and the methods used. The dissertation should be focused, and not be of too general a nature: the intention is that the Candidate presents a small topic at reasonable depth rather than a superficial review of a broad topic, which might be over ambitious.
4. For a review, the methods by which reviewed publications were identified should
be stated. The references should be up to date.

5. For a research paper, the reasons for choosing the topic should be stated, and the key questions that are to be addressed must be stated unambiguously. The research method must be outlined and critiqued. Results must be clearly stated with appropriate statistical analysis. The results must be analyzed in the manner of the discussion of a paper in a peer reviewed journal. The relevance and significance of the research must be discussed.
Authorship: The dissertation should be largely the work of the individual submitting the dissertation. It is accepted that with many pieces of work particularly in research and audit several individuals may be involved and indeed the dissertation may be based on that joint work, but the written dissertation itself should be the work of the individual sitting the examination. If others have been involved it should be acknowledged and their permission sought to use their work in the dissertation. It may be appropriate to include material from other work in the dissertation, but any use of other authors’ work must be acknowledged by clear references in all cases.
Objectives for the dissertation are to enable the candidate to perform
1. Review a. Define a question for review
• What is the area of study? Why has this been chosen?
• How are you going to approach your study?
• Will this be a systematic review? b. Access relevant and up to date resources in the particular area of
study
• Have you found out what you need to know?
• Have you explained why you chose the data sources you used?
• Is the text clearly and appropriately referenced?
c. Appraise the current status of the field of study
• Have you described the issues and drawn out the various conclusions from the literature?
• Mentioned the key factors?
• Have you questioned or supported relevant opinions?
2. Research or audit a. Define a question for original research or audit
• What is the area of study?
• Why has this been chosen?
• Have you thoroughly researched the background information? b. Design and conduct a study to address the question identified
• How are you going to approach your study?

• Have you explained why you chose the methods you used?
• Is the text clearly and appropriately referenced? c. Present the results to confirm or refute the hypothesis
• Have you described the key findings?
• Correctly analyzed and supported the reliability of the data? d. Draw own pertinent conclusions from the results of the review or
study
• Have you demonstrated a logical and sequential argument that shows analysis and synthesis of available data?
• Have you evaluated your findings to construct an answer to your original question?
e. Appraise the limitations of the review or study undertaken, and indicate possible future directions in the field of study
• Is the available data sufficient to draw a conclusion?
• Is there consistency and agreement in the data?
• Where are the gaps in our knowledge? f. Demonstrate written communication skills
• Present the work at a level consistent with submission of a critical review for publication in a peer review journal, or to a national grant awarding body.