-
7/22/2019 Materials Used in Pediatric Endodontics
1/122
1
Guided By:Dr. Binita Srivastava
Dr. Archana AggarwalDr. Nidhi GuptaDr. Rashi SinghDr. Neeti
Presented By:Dr. Parul Verma
Final yr PG Student
-
7/22/2019 Materials Used in Pediatric Endodontics
2/122
1. Introduction
2. History
3. Pulp Capping Agents- Calcium Hydroxide
Isobutyl Cyanoacrylate
Corticosteroids and antibiotics
Collagen fibers
4-Meta adhesive
Direct bondingDenatured albumin
Mineral trioxide aggregate(MTA)
Laser
BMP 2
CONTENTS:
-
7/22/2019 Materials Used in Pediatric Endodontics
3/122
4. Pulpotomy Agents- Formocresol Glutaraldehyde
Calcium hydroxide
ZnO eugenol
Ferric Sulphate
Bone Morphogenic proteins & Osteogenic proteins
Devitalizing paraformaldehyde paste
Beechwood creosote
Antibiotic paste
Enriched collagen solution
Collagen calcium phosphate gel
Dimethyl suberidement
Tetrandrine
Freeze Dried bone Tricalcium phosphate
Chondroitin sulphate
Denatured albumin
Sodium hyaluronate
3
-
7/22/2019 Materials Used in Pediatric Endodontics
4/122
5. Properties of an ideal root canal filling material
6. Pulpectomy Agents- Zinc oxide eugenolIodoform pastes- KRI ,
Walkhoff, Maisto
Endoflas
Calcium hydroxideVitapex
4
-
7/22/2019 Materials Used in Pediatric Endodontics
5/122
INTRODUCTION
Primary objective of Pulp treatment of an affected tooth is
to
maintain the integrity & health of oral tissue.
AAPD 1991, it is possible to stabilize pulp autolysis or
eliminate the pulp entirely without significantly
compromising
the function of the tooth.
Aimto treat reversible pulpal injures in both primary &
permanent teeth, maintaining pulp vitality & function.
5
-
7/22/2019 Materials Used in Pediatric Endodontics
6/122
HISTORY
6
-
7/22/2019 Materials Used in Pediatric Endodontics
7/122
1700S & Early 1800sMetal Foils
Mid 1800s to Early 1900sAsbestos fibers, cork,
beewax, pulverized glass, Calcium compounds &
other based on Eugenol
19th centuryhuman pulp had very little healing
power.
1874Nitzel : Tricresol- formalin tanning agent
7
-
7/22/2019 Materials Used in Pediatric Endodontics
8/122
1886Adolph WilzelMetal (Gold) Foil
1885LeptowskiFormalin
1898GysiParaformaldehyde
Triopaste
1904BuckleyFormocresol or Tricresol Formalin
1908Solid Formaldehyde
8
-
7/22/2019 Materials Used in Pediatric Endodontics
9/122
Boennecken40% Formalin, Thymol, Cocaine
1930HermannCalcium mixture Calxyl
1938Zender & TeuscherCalcium Hydroxide
1955Teuscher & Nybrong
1975S Gravenmade - Gluteraldehyde
9
-
7/22/2019 Materials Used in Pediatric Endodontics
10/122
1978Ranly & LazzariGulteraldehyde (Pulpotomy agent)
1979Wright & MidmerFormocresol causes
chronicinflammation
1983Reumping et al - Electrosurgery for Pulpotomy
1985Shoji et alCarbon dioxide laser in pulpotomy
1991NakashimaBone Morphogenic Proteins
1993Rutherford et alOsteogenic Proteins
10
-
7/22/2019 Materials Used in Pediatric Endodontics
11/122
11
INDIRECT PULP CAPPING:
It is defined as the application of amedicament over a thin
layer of remaining
carious dentin, after deep excavation, with no
exposure of the pulp.
The treatment objective is to avoid pulp
exposure by stimulating the pulp to generate
reparative dentin beneath the carious lesion.
-
7/22/2019 Materials Used in Pediatric Endodontics
12/122
12
This results in the arrest of caries
progression and preservation of the vitality ofnon exposed
pulp.
Next sitting involves re-entry after a 6 to 8-
week interval to remove any remaining carious
dentin and place the final restoration.
-
7/22/2019 Materials Used in Pediatric Endodontics
13/122
13
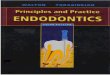
A) Medicament is placed against remaining caries.
B) Lasting temporary restoration.
Following repair, both materials are removed along with
softenedcaries, and final restorations are placed.
Ingle; Pediatric Endodontics
-
7/22/2019 Materials Used in Pediatric Endodontics
14/122
14
DIRECT PULP CAPPING:
Direct pulp capping involves the placement of abiocompatible
agent on healthy pulp tissue that
has been inadvertently exposed from caries
excavation or traumatic injury. The treatment objective is to
seal the pulp
against bacterial leakage, encourage the pulp to
wall off the exposure site by initiating a dentinbridge, and
maintain the vitality of the
underlying pulp tissue regions.
-
7/22/2019 Materials Used in Pediatric Endodontics
15/122
15
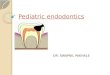
A) Capping material covers pulp exposure and the floor of the
cavity.
B) Protective base
C) Restoration.
-
7/22/2019 Materials Used in Pediatric Endodontics
16/122
16
PULP CAPPING AGENTS:
1. Zinc Oxide Eugenol- Before calcium hydroxide
came into common use, zinc-oxide eugenol was
used more often than any other pulp capping
agent.
2. Calcium Hydroxide- Herman (1930) introduced
calcium hydroxide for pulp capping. In 1938,
Teuscher and Zander introduced calcium
hydroxide in the united states.
-
7/22/2019 Materials Used in Pediatric Endodontics
17/122
17
When calcium hydroxide is applied directly to
pulp tissue reparative dentin bridge formation
occurs at the junction of necrotic tissue and
vital inflamed tissue.
-
7/22/2019 Materials Used in Pediatric Endodontics
18/122
18
Three main calcium hydroxide products are:
Pulpdent Paste contains 52.5% calcium
hydroxide in an aqueous methyl cellulose solution.Considered to
be most capable of stimulating
early bridge formation.
Hydrex- It is a two paste system, non-essential oil hard setting
compound that contains
calcium hydroxide, barium sulfate, titanium
dioxide and a selected resin.
Dycal
-
7/22/2019 Materials Used in Pediatric Endodontics
19/122
19
3. Isobutyl Cyanoacrylate- Introduced by
Berkman in 1971. It has been reported to be an
excellent pulp capping agent because of its
hemostatic and bacteriostatic properties.
It cannot be regarded as an adequate
therapeutic alternative to calcium hydroxide
since it does not produce a continuous barrier of
reparative dentin after application to the
exposed pulp
-
7/22/2019 Materials Used in Pediatric Endodontics
20/122
4. Corticosteroids and antibiotics- Introduced by
Brosch JW in 1966. These agents include neomycin and
hydrocortisone, ledermix (calcium hydroxide and
prednisolone), penicillin or vancomycin with calcium
hydroxide.
5. Collagen Fibers- Influences mineralization and are
less irritant than calcium hydroxide with dentin bridge
formation in 8 weeks.
6. 4-META adhesive- It can soak into the pulp,
polymerize there and form a hybrid layer with the pulp
providing adequate sealing. 20
-
7/22/2019 Materials Used in Pediatric Endodontics
21/122
7. Direct Bonding- A polygenic film can be layered over
an exposed site without displacing pulp tissue and onto
surrounding dentin where it penetrates the tubules. The
film acts as a barrier as composite resin is gently
spread over the pulp onto the surrounding dentin.
8. Denatured Albumin- This protein has calcium binding
properties. If applied over the exposed pulp it becomes
a matrix for calcification.
9. Laser- Introduced by Andreas Meritz in 1998. He
evaluated the effect of laser on DPC and reported a
success rate of 89%. 21
-
7/22/2019 Materials Used in Pediatric Endodontics
22/122
10. Mineral Trioxide Aggregate (MTA)- Torabinejad
described the physical and chemical properties of MTA
in 1995. It is ash colored powder made up of fine
hydrophilic particles of tricalcium aluminate, tricalcium
silicate, silicate oxide, tricalcium oxide and bismuth
oxide.
Properties:
1. Biocompatible and sealing ability better than that of
amalgam and ZOE.
2. Initial ph is 10.2 and set ph is 12.5
3. Setting time of cement is 4 hours. 22
-
7/22/2019 Materials Used in Pediatric Endodontics
23/122
4. Compressive strength is 70 MPA, which is comparable
with that of IRM.
5. Presents minimal inflammation if extended beyond
the apex.
Mechanism of action:
1. Forms CH that releases calcium ions for cell
attachment and proliferation.
2. Creates an antibacterial environment by its alkaline
pH.
3. Encourages differentiation and migration of hard
tissue-producing cells 23
-
7/22/2019 Materials Used in Pediatric Endodontics
24/122
4. Forms hydroxyapatite on the MTA surface and
provides a biologic seal.11. Bone morphogenic protein-
Discovered by Urist in
1965. It has inductive properties and forms both bone
and dentin.
24
-
7/22/2019 Materials Used in Pediatric Endodontics
25/122
PULPOTOMY
25
-
7/22/2019 Materials Used in Pediatric Endodontics
26/122
Pulpotomy is defined as amputation of vital pulp from the
coronalchamber followed by placement of a medicament over the
radicular pulp stumps to stimulate repair, fixation or
mummificationof the remaining vital radicular pulp. (Braham &
Morris 1985)
Removalofthe coronal portion of the pulp & the treatment of
the
remaining radicular pulp in an attempt to maintain the tooth
& its
supporting structure in a state of health. (Heillig 1984)
Procedures involving removal of vital, partially inflamed
coronalpulp tissue & placing a dressing over the amputed pulp
stumps &
placing the final restoration. (Kennedy 1986)
26
-
7/22/2019 Materials Used in Pediatric Endodontics
27/122
Procedure in which the entire coronal pulp is removed, with
the
aim of removing all the infected pulp tissue, the radicular pulp
is
then treated in different ways, according to technique
employed.
(Andlaw & Rock 1993)
Complete removal of the coronal portion of dental pulp,
followed
by placement of a suitable dressing or medicament that will
promote healing & preserve the vitality of the tooth.
(Finn)
27
-
7/22/2019 Materials Used in Pediatric Endodontics
28/122
MEDICAMENTS
28
-
7/22/2019 Materials Used in Pediatric Endodontics
29/122
29
Formocresol
Glutaraldehyde
Calcium hydroxide
ZnO eugenol
Ferric Sulphate
Bone Morphogenic proteins & Osteogenic proteins
Devitalizing paraformaldehyde paste
Beechwood creosote
Antibiotic paste
Enriched collagen solution
Collagen calcium phosphate gel
Tetrandrine
Freeze Dried bone
Tricalcium phosphate
Chondroitin sulphate
Denatured albumin
Sodium hyaluronate
-
7/22/2019 Materials Used in Pediatric Endodontics
30/122
Action of Formocresol on pulp tissue: Formaldehyde undoubtedly
fixes the pulp tissue
Alters blood flow by inducing thrombus formation
ischemia causes coagulation necrosis of tissue deprived ofits
normal nutrition.
Enzymatic hydrolysis of necrotic tissues replacement of it
by granulation tissue.
Slight resorption of dentinal walls in zone of replacement
&
deposition of osteodentin as a repair tissue.
30
FORMOCRESOL Introduced by Buckleys 1904
-
7/22/2019 Materials Used in Pediatric Endodontics
31/122
31
-
7/22/2019 Materials Used in Pediatric Endodontics
32/122
Buckleys FormocresolFormalin (37%) : 19%
Tricresol : 35%Glycerin : 15%
Water
Achieve 1:5 concentration of original Buckleys formocresolDilute
3 parts glycerine with 1 part of distilled sterile water.
Add 1 part formocresol to 4 part diluent
90ml glycerine
30ml water Loos et al
30ml formocresol
32
-
7/22/2019 Materials Used in Pediatric Endodontics
33/122
Emmerson : determined significant formocresol action
within 1st five minutes.
Braham & Morris : Linear calcification may have
adverseinfluence on resorption process.
Histological Observation:
Massler M & Mansukhani N : surface of pulp
immediately under formocresol became fibrous &
acidophilic
within few minutes after application of formocresol.
33
-
7/22/2019 Materials Used in Pediatric Endodontics
34/122
3 distinct Zones:
Acidophilic zone of fixation
Zone of atrophy
Zone of inflammatory cells
No reparative dentin formation.
Berger - histologic findings:
3 weeks postoperative:
1. Nuclei, cytoplasm & intercellular ground
substancemost
Coronal region, all dark stain
2. Odontoblast & other cellular elements well outlined
&
distended blood vessels with well preserved erythrocytes
34
-
7/22/2019 Materials Used in Pediatric Endodontics
35/122
Middle 3rd:
1. Stain of tissue decreased
2. Cellular details less distinct
Apical 3rd:
1. Absence of cellular details
2. Blood vessels containing decomposed erythrocytes which
appeared to lose structural integrity
7weeks post operative:
1. Dark stained coronal zone, light stained middle zone &
Cellular
apical zone
2. CT originating from periodontal ligament
3. Richly vascular & contained lymphocytes, PMN,
macrophages,
proliferating fibroblasts & granulation tissue
35
-
7/22/2019 Materials Used in Pediatric Endodontics
36/122
Connective tissue undergoing castration due to decreased
number of mature fibroblasts & increase of fibrous
intracellular elements.
Coagulation necrosis in middle 3rd, delineated apically by a
zone of necrotic tissue
Braham & Morris - these zones are obvious in1 month
&
established in 3months although pulpal fixation did not extend
to
the apex
36
T i it
-
7/22/2019 Materials Used in Pediatric Endodontics
37/122
Toxicity Post operative systemic transport
Possible effects on the enamel of succedaneous teeth
Reversible fixation leading to autoantibody formation
Mutagenicity & Carcinogenicity
Destruction of cellular integrity due to cresol factor
Irreversible connective tissue changes
Irritation & necrosis
Leukoplakia & lesions resembling carcinoma in situ
37
-
7/22/2019 Materials Used in Pediatric Endodontics
38/122
Local Toxicity
PruhsAll permanent teeth showed enamel defectsbecause:
Formocresol which damages the permanent tooth germs
Inflammation which was in the primary tooth which causes
the defects in the permanent tooth germs.
38
-
7/22/2019 Materials Used in Pediatric Endodontics
39/122
39
Human studies not done.
Kettley & Mejare in animals
Formaldehyde labeled with radioactive carbon which was
apparently distributed among the muscles, liver, kidney,
heart,spleen & lungs. 1% of total administered dose was
absorbed.
Myers et al & Pashley et al concluded that 5-10%
formaldehyde is absorbed systemically from pulpotomy
sites.
-
7/22/2019 Materials Used in Pediatric Endodontics
40/122
Mutagenicity & Carcinogenicity
Most common type of DNA damageClastogenic lesions,
micronuclei & chromosomal aberration & deletions.
Ribeiro et al not produce detectable DNA damage & not
considered genotoxic.
40
-
7/22/2019 Materials Used in Pediatric Endodontics
41/122
Advantages Commonly available medicament
Stable at room temperature Long shelf life
Disadvantages: Reaction reversible
Very caustic medication
High dose toxic
Systemic absorption & distribution throughout the body
Has mutagenic & cariogenic potential
41
-
7/22/2019 Materials Used in Pediatric Endodontics
42/122
Internal resorption of the root adjacent to the area where
the
formocresol was applied.
Radiolucency may develop in the bifurcation or
trifurcationarea.
Furcal lesions may contain granulomatous tissue having the
potential for cyst formation.
42
Area showing root resorption following formocresol
pulpotomy.
-
7/22/2019 Materials Used in Pediatric Endodontics
43/122
43
GLUTERALDEHYDE
Known for its high degree of cross linking & limited
diffusability.
By S Gravenmade
Denkertminimum diffusion through apices.
Martin J. Davis, Myers & M.D.Switkes- more active in
fixing surface tissue & more rapidly limited depth
ofpenetration through tissues.
-
7/22/2019 Materials Used in Pediatric Endodontics
44/122
44
Martin J. Davis et al : Glutaraldehyde & Formocresol - does
not
perfuse through the apex & shows no systemic distribution
& other
extra dental phenomena.
Franklin Gracia Godoy et al : ZnO as vehicle for
Glutaraldehyde
2% glutaraldehyde incorporated in ZnO not effective as when
applied for 5min.
Hue- Wen- Jeng et al : compared cytotoxicity & found human
pulp
fibroblastformaldehyde is more toxic & 2.5% glutaraldehyde
is
15-20times less toxic
Hermandez Pereyra et al : 2% glutaraldehyde &
FormocresolR/G
success of 80% & 90% with glutaraldehyde after 6months &
2yrs.
-
7/22/2019 Materials Used in Pediatric Endodontics
45/122
45
Prakash C. et al : formocresol showed 90% success whereas
Glutaraldehyde 100% success. Glutaraldehyde better fixative
& less
toxic.
Histology
-
7/22/2019 Materials Used in Pediatric Endodontics
46/122
46
Histology
Martin J. Davis, Myers & Switkase -5% buffered
glutaraldehyde, pH= 8.5After 1week:
Coronal third: radicular tissue fixed & found to be non
vital. Cells
compressed & darkly stained
Middle 1/3rd: radicular tissue vital with good cellular details
& moderate
inflammation
Apical 3rd: vital with scattered inflammatory cells.
After 4 weeks:
Coronal 3rd: same
Middle portion: clear cellular details, unchanged degree of
inflammation.
Limited dystrophic calcification apparent on lateral wall of
canal.
Apical 3rd: apparently vital with occasionally observed
inflammatory cells.
Aft 8 k
-
7/22/2019 Materials Used in Pediatric Endodontics
47/122
47
After 8weeks:
Coronal 3rdno change
Middle 3rd: dystrophic calcification apparent
Apical 3rd: vital & demonstrated good cellular details with
scattered inflammatory
cells.
Appearance of multinucleated giant cells & fibroblasts.
Indicative of replacement
repair
Deep red cellular zone adjacent to amputation surface & few
lymphocytes &
plasma cells. Blood vessels dilated. Remaining pulp free of
inflammatory cells &
root canal lined with layer of reparative dentin.
After 3months:
Coronal region: stained redPulp tissue: no layering or signs of
inflammation. Macrophages visible in &
adjacent to red zone.
No pathosis noted.
-
7/22/2019 Materials Used in Pediatric Endodontics
48/122
48
Kopel concluded:
2% glutaraldehyde accepted as dressing medicament for
maintaining
vitality of remaining pulp.
Histologically, pulp tissue in root does not resemble pulp
tissue subjectedto formocresol
Initial zone of fixation adjacent to dressing does not proceed
apically.
The tissue which adjoins fixed zone has cellular details &
is vital.
Fixed zone replaced through macrophagic action with dense
collagenoustissue.
Established biochemical properties & effect on vital pulpuse
of 2%
glutaraldehyde as pulpotomy agent.
Anna B. Fuks - contraindicate use of Glutaraldehyde
Kopel & Gracia Godoyrecommend use of 2% Gluteraldehyde for 1
or
3min
-
7/22/2019 Materials Used in Pediatric Endodontics
49/122
49
Advantages:
Reaction with pulp irrevisible Molecules do not diffuse out of
apical foramen
Fixes tissue instantly
Not known to be cytotoxic, mutagenic & cariogenic
No systemic toxic effect.
Disadvantages:
Short shelf life
Freshly prepared
Buffered solution to be refrigerated.
Glutaraldehyde Vs Formocresol
-
7/22/2019 Materials Used in Pediatric Endodontics
50/122
50
Glutaraldehyde Vs Formocresol
Advantages of Glutaraldehyde over Formocresol:
Is better bactericidal
Not diffuse apically or laterally from the canals Not known to
be cariogenic
Not induce toxic effect
Less systemic distribution immediately after application
Fixes tissue instantly
Not known to be caustic
Better fixation at lower conc.
-
7/22/2019 Materials Used in Pediatric Endodontics
51/122
51
FERRIC SULFATE
15.5% solutionFei et al 1991
Used: coagulative & haemostatic retraction agent for crown
& bridgeimpression & slightly acidic
MOA- agglutination of blood proteins results from reaction of
blood with
both ferric & sulfate ions.
Schroedercontrolling hemorrhage might minimize chance
ofinflammation & internal resorption clot formation.
Ranlymetal protein clot may act as barrier to irritative
components ofsub-base & function in passive manner.
Landaw & Johnson - 1st to study pulpal response from ferric
sulfate inmonkey teeth.
Ferric Sulfate Vs Formocresol
-
7/22/2019 Materials Used in Pediatric Endodontics
52/122
52
Ferric Sulfate Vs FormocresolAuthor C/L & R/G
success respc. of
formocresol
C/L & R/G
success respc. of
ferric Sulfate
Duration
Fei et al 1991 96% & 91% 100% & 97% 12mths
Fuks et al 1997 84% & 80% 93% & 93% 34mths
Aktoren & Gencay2000
88% & 80% 88% & 84% After 24mths
Papagiannoulis
2002
97% & 78% 90% & 74%
Ibrevic & Al Jame
2003
96% & 92% 42mths
Huth et al 2005 96% & 90% 100% & 86% 24mths
Morkovic et al
2005
89% & 82% 18mths
ZINC OXIDE EUGENOL (ZOE)
-
7/22/2019 Materials Used in Pediatric Endodontics
53/122
53
ZINC OXIDE EUGENOL (ZOE)
Considered as therapeutic or obtundent.
Used as non toxicve control but, applied directly todental pulp,
nerve tissue , this medicamenttoxic
Flagg 1875clove oil + zinc oxide plastic mass
Used as: base, temporary dressing, endodontic root
filling paste, impression material, PD packs & asPulpotomy
medicament.
Composition
-
7/22/2019 Materials Used in Pediatric Endodontics
54/122
54
Composition
Various formulations & uses of ZOE restorative material:
Type 1: temporary cementation
Type 2: permanent cementation of restoration
Type 3: temporary filling material, thermal insulating
base
Type 4: cavity liners
Composition:
Powder Liquid
Zinc oxide: 69%
White resin: 29.3%
Zinc sterate : 1%
Zinc acetate: 0.7%
Eugenol: 85%
Olive oil: 15%
Histology
-
7/22/2019 Materials Used in Pediatric Endodontics
55/122
55
HistologyJames E. Berger : active inflammatory reactions which
varied
from simple chronic to acute suppurative pulpitis.
Boller RJ : calcific deposition associated with dentinal debris
&
bridge formation.
R.L. Glass & H.A. Zander: inflammation, abscess formation
&liquefaction necrosis.
24hrs after:
underlying tissue contain mass of red blood cells & PMN
leukocytes
Hemorrhage mass demarcated by Zone of fibrin & inflammatory
cells
2weeks after:
Degeneration of pulp & chronic inflammation extends into
apicalportion of pulp lymphocytes, plasma cells & PMNs
leukocytes
Failed to stimulate osteogenesis.
6 months: 1 tooth showed acute inflammation involving entire
-
7/22/2019 Materials Used in Pediatric Endodontics
56/122
56
6 months: 1 toothshowed acute inflammation involving entire
pulp
12 months: microscopic appearance of acute inflammation
18months: all teeth showed chronically inflamed pulp &
absenceof fibrous tissue.
Doyle et al 92%histologic success, 92% R/G & 100%
clinical
Success.
Ranly : lowclinical success rate (80 to 82%)
-
7/22/2019 Materials Used in Pediatric Endodontics
57/122
57
Zinc Oxide preparationsVarious preparations used as pulpotomy
medicament:
Zinc oxide/Eugenol & Paraformaldehyde
Zinc oxide/Liquid Paraffin & Paraformaldehyde
Zinc oxide/ Liquid paraffin
-
7/22/2019 Materials Used in Pediatric Endodontics
58/122
58
CALCIUM HYDROXIDE
Foreman & Barnes
Hermann & Zander - introduced for Pulpotomy &
foundsuccess rate of 70%
Granath :Apexification following trauma
Kaiser & Frank : use for apexification
Pure form- high pH & dental use ability to stimulate
mineralization & antibacterial properties.
-
7/22/2019 Materials Used in Pediatric Endodontics
59/122
MECHANISM OF ACTION:
Antimicrobial activity of calcium hydroxide isrelated to the
release of hydroxyl ions in aqueous
environment.
Hydroxyl ions are highly oxidant, free radicals
that show extreme reactivity.
Their lethal effects on the bacterial cells are
probably due to the following mechanisms:
59
-
7/22/2019 Materials Used in Pediatric Endodontics
60/122
Damage to the bacterial cytoplasmic
membrane:
Hydroxyl ions induce lipid oxidation destruction
of phospholipids.
Hydroxyl ions generates free lipid radical.
This free radical reacts with oxygen formation ofa lipidic
peroxidase radical.
Thus, peroxidases act as free radicals resulting in
extensive tissue damage.
60
-
7/22/2019 Materials Used in Pediatric Endodontics
61/122
Proteindenaturation:
The alkalinization provided by calcium hydroxide
breakdown of the ionic bonds that maintain the
tertiary structures of proteins.
Loss of biological activity of the enzyme anddisruption of the
cellular metabolism.
Structure may also be damaged by hydroxyl ions.
61
-
7/22/2019 Materials Used in Pediatric Endodontics
62/122
Damage to the DNA:
Hydroxyl ions react with the bacterial DNA and
induce the splitting of the strands.
Genes are then lost. Consequently DNA
replication is inhibited and the cellular activity is
disarranged.
62
Composition & Chemistry
-
7/22/2019 Materials Used in Pediatric Endodontics
63/122
63
Composition & Chemistry
De Freitas & Rosser : cements set by acid base reaction,
the
phenolic group in alkyl salicylate ester acting as acid.Once
set, therapeutic activity depends upon release of calcium &
hydroxyl ion which occur if cement water soluble.
Plasticizer imparts solubility.
Milosevic - calcium hydroxide reaction with salicylate ester
chelating agent in presence of toloudine sulphonamide
plasticizer.
Hydrophilic & Soluble.
Ca hydroxide powder + distilled water creamy paste with high
-
7/22/2019 Materials Used in Pediatric Endodontics
64/122
64
Ca hydroxide powder + distilled water creamy paste with high
alkalinity
3 main products:
Pulpdent- 52.5% calcium hydroxide suspended in aqueousmethyl
cellulose solution
Dycalby L.D. Caulk.
Available in 2 pastes- Base & Catalyst
Base: Titanium dioxide in glycol salicylate
Catalyst: Calcium hydroxide & ZnO in ethyl toluene
sulfonamide.
Hydrex: 2 paste; non essential oilcontain calcium hydroxide,
barium sulphate, titanium dioxide & selected resin.
Hydrex- hydrophobic paraffin oil methacrylate.
-
7/22/2019 Materials Used in Pediatric Endodontics
65/122
65
Hydrex hydrophobic paraffin oil methacrylate.
1. Relatively insoluble (Prosser )
2. Poor antibacterial properties (Fisher & Mc Cabe ; Fisher
&Shortal )
3. Hydroxyline resistant to acid etching (Milosevic)
4. Linn & Mc Cabe reaction between calcium & Zn ions
& a
salicylate chelating agent is accelerated by presence of
water.
Histology
-
7/22/2019 Materials Used in Pediatric Endodontics
66/122
66
HistologyTeuscher & Zander -
Superficial layernecrotized, accompanied by acute
inflammatory
changes. Demarcated by new, deeply staining zone
comprisingbasophilic elements of Ca Hydroxide dressing
Proteinate zone present
New area of fibrous tissue linked to primitive type of bone.
After 4weeks:
Acute inflammation subsides new odontoblastic layer bridge
of
dentin
Pulp tissue beneath calcific bridgevital & free of
inflammatory cells.
Calcium hydroxide appears to stimulate resorption.
Andersen External root resorption of avulsed teeth when
-
7/22/2019 Materials Used in Pediatric Endodontics
67/122
67
p
repositioned with cal hydroxide
Law 49% success in 1yr
Doyle et alhistological success of 50% & R/G 64% &
clinicalsuccess 71%
Schroder67% clinical success after 1yr; 38-59% after 2yr in
33
pulpotomized primary teeth.
Hellig et al rapid decrease in hemorrhage & better R/G.
Internal Resorption:
Occurs near junction of coronal & radicular pulp (Hannah
& Rowe )
Inflammation- inflammatory cells attract osteoclastic cells
&
initiate internal resorption
Vascularity of apical region increased
Osteoclastic activity predispose to External Resorption when
an
irritant (CaOH)2 is placed on the pulp.
Via69% failure (internal resorption)
L 54% f il
-
7/22/2019 Materials Used in Pediatric Endodontics
68/122
68
Law54% failure
Magunsson80% failure
Comparing CALCIUM HYDROXIDE with FORMOCRESOL:
Author Clinical & R/Gsuccess of Ca
hydroxide
Clinical & R/Gsuccess of
Formocresol
Duration
Waterhouse et al 77% 84% 22mths
Huth et al 87% 96% 24mths
Markovic et al 82% & 76% 91% & 85% 18mths
BONE MORPHOGENIC PROTEINS
-
7/22/2019 Materials Used in Pediatric Endodontics
69/122
69
BONE MORPHOGENIC PROTEINS
& OSTEOGENIC PROTEINS
Proteins evaluated from osteogenic potential
Pulp responsesdetermined in dogs & primary teeth
Role in healing bone & pulp
BMP 4epithelial/ mesenchymal interaction during early
tooth development (Ranly DM)
BMP Function
-
7/22/2019 Materials Used in Pediatric Endodontics
70/122
70
BMP 1 It is a metalloprotease that acts on procollagen I,II,III.
Involved
in cartilage development
BMP 2 Acts as a disulfide linked homodimer & induce bone
& cartilage
formation. Plays role in osteoblast differentiation.
BMP 3 Induce bone formation
BMP 4 Regulates the formation of teeth, limbs & bone from
mesoderm.
Role in fracture repair also
BMP 5 Function in cartilage development
BMP 6 Role in joint integrity in adults
BMP 7 Key role in Osteoblast differentiation. Role in renal
development
BMP 8a Involved in bone & cartilage development
BMP 8b Expressed in hippocampus
BMP 10 Role in trabeculation of embryonic heart
BMP 12 Potential repair of alveolar bone defects
BMP 15 Role in oocyte & follicular development
FREEZE DRIED BONE
-
7/22/2019 Materials Used in Pediatric Endodontics
71/122
71
FREEZE DRIED BONE Used in Orthopedic & Oral surgery.
Pulp & dentinMesodermal tissuesFreeze dried boneserve as
inducer of calcific barrier at amputation site.
Mc Lean & Urist 1968
Interaction of mesodermal cells & mesodermal
derivativesduring bone resorption that induce differenation.
Alternative for Formocresol
Fadavi et al 1996
COLLAGEN
-
7/22/2019 Materials Used in Pediatric Endodontics
72/122
72
COLLAGEN
Bimstein E, Shoshan S.Enriched Collagen Solution.
Anna B. Fuks, Y. Michaeli et al 80% teeth vital pulp &
73% of teeth dentin bridge present & cells proliferating
through incomplete dentin bridge.
Nevins et alused CollagenCalcium Phosphate gel
paste.
TETRANDRINE
-
7/22/2019 Materials Used in Pediatric Endodontics
73/122
73
TETRANDRINE
Noval Anti Inflammatory Agent.
Composition:
98% buffered saline dissolved in Phosphate &
20% 0.1N HCl with pH 7.2
Tetrandrine pulpotomies Showed significantly less
inflammatory changes as compared to formocresol.
FERACRYLUM
-
7/22/2019 Materials Used in Pediatric Endodontics
74/122
74
FERACRYLUM Incomplete iron salt of Polyacrylic acid0.05-0.5%
iron
MOA: binds with plasma proteins & form clot
Properties:
Bacteriocidal property
Devoid of Systemic toxicity
Used for various medical surgeries
Neetu T. Prabhu & A.K. Munshi : clinical success 100%
Histological Examination after 1month: 4 zones-
Eosinophillic zone Zone of Ghost cells
Inflammatory zone
Normal radicular pulpal tissue
CALCIUM PHOSPHATE CEMENT
-
7/22/2019 Materials Used in Pediatric Endodontics
75/122
75
CALCIUM PHOSPHATE CEMENT
Clinical applicationOrthopedic & Dentistry
Composition:
Powdercalcium & Phosphorous ingredients
Liquidaqueous solution of phosphates
Cement undergoesthermal setting & gets
converted into hydroxyapatite.
TETRACALCIUM PHOSPHATE
-
7/22/2019 Materials Used in Pediatric Endodontics
76/122
76
TETRACALCIUM PHOSPHATE
CEMENT (4CP)
Calcium phosphate ceramics tricalcium phosphate
- bone substitute
tricalcium phosphate
- Dental cement
Yoshimine Y 1993: 4CP effective as bone cement.
Yoshimine Y 1995: 4CP as a Direct pulp capping agent. No finding
of necrosis
Biocompatible
MINERAL TRIOXIDE AGGREGATE
-
7/22/2019 Materials Used in Pediatric Endodontics
77/122
77
MINERAL TRIOXIDE AGGREGATE
Lee & colleagues 1993 : 1st to get MTA
in dental literature.
Used : Root end filling, DPC, perforation repairs in
root,furcation & apexification.
Ideal to use against bone.
Allow for overgrowth of cementum & formation of bone
& facilitate regeneration of PDL.
C iti Ph i l & Ch i l
-
7/22/2019 Materials Used in Pediatric Endodontics
78/122
Composition, Physical & ChemicalProperties
Mixture of refined Portland cement & bismuth oxide
Portland cement: Dicalcium silicate,Tricalcium silicate,
Tricalcium aluminate, gypsum & Tetrcalcium alumino
ferrite.
Trace Elements: SiO2, CaO, MgO,
Gypsum : Setting time
Aluminum species: longer working time
Powder : Liquid3:1
78
Hydration: MTA forms Colloidal gel solidifies to hard tissue3
4h
-
7/22/2019 Materials Used in Pediatric Endodontics
79/122
79
3-4hrs.
Initial pH10.2 which rises to 12.5 three hrs after mixing.
Compressive Strength: increase in presence of moisture for
upto21days.
Microhardness & hydration behavior adversely affected
Upto 2002 : GREY colored powder MTA.(GMTA)
WHITE MTA (WMTA) : Pro Root MTA (Dentsply Endo. Tulsa)
Mineralization:
Induce hard tissue formation in pulpal tissue
Histologic evaluation: stimulate Reparative dentin formation
withthick dentinal bridging, minimal inflammation & normal
hypermia.
-
7/22/2019 Materials Used in Pediatric Endodontics
80/122
80
WMTAfound to have 54.9% less Al2O3, 56.5% less MgO &
90.8% less FeO.
FeO cause color change
WMTA smaller particle size.
WMTA : is significantly less soluble, exhibit greater
hardness
& more radiopaque.
MTA as Pulpotomy dressing
-
7/22/2019 Materials Used in Pediatric Endodontics
81/122
81
MTA as Pulpotomy dressing
Eidelman E : pulp obliteration seen at higher frequency in
GMTA
Cuisia et al : 93% clinical &77% radiographic success with
formocresol
& 97% Clinical & 93% radiographic success with MTA
Jabbarifar et al : 94% success with MTA
Agamy : GMTA>WMTA=Formocresol- 12mths
Farsi N : non failure with WMTA whereas 13% radiographic failure
&2% clinical failure with formocresol- 24mths
Holan et al : 83% success- formocresol & 97% with MTA-
74mths
Nark & Hegde : 100% success with MTA in 6mths
-
7/22/2019 Materials Used in Pediatric Endodontics
82/122
82
Maroto M: GMTA 100% clinical success & 50% radiographic
success
WMTAradiographically 69% pulp canal signs of stenosis
11.5% - dentin bridge & 1 canal exhibited early signs
ofinternal resorption
No statistical significance in rate of stenosis, but GMTA showed
significant
more dentine bridge.
Pinto LM : 2 failure with MTA & 6 failure with Calcium
hydroxide in 12mths.
Barreshi Nusairk: after 24mths 79% - +ve results.
64% had hard tissue bridge formation while 7 teeth displayed R/G
signs ofcontinued root development.
Chacko V : WMTA induced more homogenous & continued dentin
bridge with
less pulpal inflammation than Calcium hydroxide.
-
7/22/2019 Materials Used in Pediatric Endodontics
83/122
83
Ideal Requirements of Root filling
-
7/22/2019 Materials Used in Pediatric Endodontics
84/122
84
q gMaterials-
The material should resorb as the primary tooth root
resorbs. Not irritate the periapical tissues nor coagulate
any
organic remnants in the canal. Have a stable disinfecting power.
Any surplus material passed beyond the apex should
be resorbed easily. Inserted easily into the root canal and also
removed
easily if necessary. Not be soluble in water. Not discolor the
tooth.
Radio opaque. Harmless to the adjacent tooth germ. Adhere to the
walls of the canal & should not shrink Not set as a hard mass,
which could deflect erupting
successor
(Catagnola 1952, Rifkin 1980, Woods 1984)
Zinc Oxide Eugenol ( ZOE)
-
7/22/2019 Materials Used in Pediatric Endodontics
85/122
85
Zinc Oxide Eugenol ( ZOE)
To fill root canals of primary teeth was first described bySweet
1930
Roths Sealer
Powder
Zinc oxide reagent- 42 parts
Stabelite resin 27 parts Bismuth subcarbonate 15 parts
Barium sulphate 15 parts
Sodium borate, anhydrous 1part
Liquid
Eugenol
Properties
-
7/22/2019 Materials Used in Pediatric Endodontics
86/122
86
Properties
Extended working time- but set faster in mouth due toincreased
temperature & humidity.
Good sealing potential because of small volumetric changes
on
setting
Eg Tubliseal, Wachs Cement, Nogenol
-
7/22/2019 Materials Used in Pediatric Endodontics
87/122
87
Gould
First proposed single visit pulpectomy
39 molars were filled with ZOE after a follow up of 16
months
35 out of 39 were successful.
E i & M b l
-
7/22/2019 Materials Used in Pediatric Endodontics
88/122
88
Erausquin & Muruzabal
Used ZOE in 141 rats followed from 1-90 days
ZOE irritated the periapical tissues and caused necrosis of
bone & cementum.
Extruded ZOE developed fibrous capsule that prevented
resorption
Coll
-
7/22/2019 Materials Used in Pediatric Endodontics
89/122
89
Coll
Retained ZOE after loss of pulpectomized tooth
27.3% after a mean of 40.2 months after loss of treated
tooth
Retained
Short filled ( 1mm or more short of apex) retained ZOE less
often than beyond fills
Size of particles of most retained ZOE filler decreased over
time
Antibacterial Activity
-
7/22/2019 Materials Used in Pediatric Endodontics
90/122
90
Antibacterial Activity
ZOE could not inhibit Echerichia coli, S. aureus,
Streptococcus viridans
Inhibited- S.aureus & S.viridans
Inclusion of zinc acetate allowed to inhibit all three
Cox et al
-
7/22/2019 Materials Used in Pediatric Endodontics
91/122
91
Iodoform Pastes-
Rifkin 1980, 1982.
-
7/22/2019 Materials Used in Pediatric Endodontics
92/122
92
KRI
Walkhoff 1928Parachlorophenol, Camphor, Menthol Iodoform
Paste
2.025%- Parachlorophenol
4.86%- Camphor
1.215%- Menthol 80.8%- Iodoform
Rifkin - It meets all criteria required from an ideal root
canalfilling material
Advantages
-
7/22/2019 Materials Used in Pediatric Endodontics
93/122
93
Advantages
Disinfectant to treat osteitis after extractions Remains in
paste form and never sets to a hard mass.
Smooth, viscous material, can be spun in with lentulo-spiral
orinjected with pressure syringe
Resorbable so if inadvertantly expressed into periapical
granulomatous tissue is rapidly removed and replaced byhealthy
connective tissue ( Castagnola , Woods )
Resorbs in synchrony with roots.
Easily inserted and removed
Resorbs from apical tissues in one or two weeks.
Holan Anna Fuks -
-
7/22/2019 Materials Used in Pediatric Endodontics
94/122
94
Holan Anna Fuks
Compared the ZOE and KRI
Success rate of both was similar if underfilled
Slightly higher when KRI flushed to the apex
Maistos Paste
-
7/22/2019 Materials Used in Pediatric Endodontics
95/122
95
Maisto s Paste
Maisto 1967
Zinc oxide- 14g
Iodoform42g
Thymol- 2g
Chlorphenol camphor-3cc
Lanolin- 0.50g
Eliyahu Mass
-
7/22/2019 Materials Used in Pediatric Endodontics
96/122
96
y
Maisto was successful in treating infected molars.
Iodoform containing pastes are easily resorbed from the
periradicular region.
These cause no foreign body reaction like Zinc Oxide Eugenol
Over filling and resorption of iodoform containing had no
effect on success of treatment rather had positive healing
effect.
Reddy VV, Fernandes .
http://www.ncbi.nlm.nih.gov/sites/entrez?Db=pubmed&Cmd=Search&Term=%22Reddy%20VV%22%5BAuthor%5D&itool=EntrezSystem2.PEntrez.Pubmed.Pubmed_ResultsPanel.Pubmed_DiscoveryPanel.Pubmed_RVAbstractPlushttp://www.ncbi.nlm.nih.gov/sites/entrez?Db=pubmed&Cmd=Search&Term=%22Fernandes%22%5BAuthor%5D&itool=EntrezSystem2.PEntrez.Pubmed.Pubmed_ResultsPanel.Pubmed_DiscoveryPanel.Pubmed_RVAbstractPlushttp://www.ncbi.nlm.nih.gov/sites/entrez?Db=pubmed&Cmd=Search&Term=%22Fernandes%22%5BAuthor%5D&itool=EntrezSystem2.PEntrez.Pubmed.Pubmed_ResultsPanel.Pubmed_DiscoveryPanel.Pubmed_RVAbstractPlushttp://www.ncbi.nlm.nih.gov/sites/entrez?Db=pubmed&Cmd=Search&Term=%22Reddy%20VV%22%5BAuthor%5D&itool=EntrezSystem2.PEntrez.Pubmed.Pubmed_ResultsPanel.Pubmed_DiscoveryPanel.Pubmed_RVAbstractPlus
-
7/22/2019 Materials Used in Pediatric Endodontics
97/122
97
Reddy VV, Fernandes .
On clinical evaluation, teeth obturated with Maisto's paste
showed 100% success. Five teeth that were overfilled with
Maisto's paste showedcomplete resorption of excess material within
3 months
while the two teeth overfilled with zinc oxide-eugenol
showedincomplete resorption of the excess material even after 9
months. Zinc oxide-eugenol treated cases showed only 26.7%
bone
regeneration while in case of Maisto's paste, it was 93%.
Complete healing of the inter-radicular pathology was seenwith
Maisto's paste.
However, the pathology was present in 40% of the zinc
oxide-eugenol treated teeth even after 9 months.
Maisto's paste was thus seen to be superior to zinc
oxide-eugenol.
Endoflas
http://www.ncbi.nlm.nih.gov/sites/entrez?Db=pubmed&Cmd=Search&Term=%22Reddy%20VV%22%5BAuthor%5D&itool=EntrezSystem2.PEntrez.Pubmed.Pubmed_ResultsPanel.Pubmed_DiscoveryPanel.Pubmed_RVAbstractPlushttp://www.ncbi.nlm.nih.gov/sites/entrez?Db=pubmed&Cmd=Search&Term=%22Fernandes%22%5BAuthor%5D&itool=EntrezSystem2.PEntrez.Pubmed.Pubmed_ResultsPanel.Pubmed_DiscoveryPanel.Pubmed_RVAbstractPlushttp://www.ncbi.nlm.nih.gov/sites/entrez?Db=pubmed&Cmd=Search&Term=%22Fernandes%22%5BAuthor%5D&itool=EntrezSystem2.PEntrez.Pubmed.Pubmed_ResultsPanel.Pubmed_DiscoveryPanel.Pubmed_RVAbstractPlushttp://www.ncbi.nlm.nih.gov/sites/entrez?Db=pubmed&Cmd=Search&Term=%22Reddy%20VV%22%5BAuthor%5D&itool=EntrezSystem2.PEntrez.Pubmed.Pubmed_ResultsPanel.Pubmed_DiscoveryPanel.Pubmed_RVAbstractPlus
-
7/22/2019 Materials Used in Pediatric Endodontics
98/122
98
Endoflas
Resorbable paste produced in South America Similar to Vitapex
contains Zinc oxide and eugenol
Paste-
Tri-iodomethane , Iodine dibutilorthocresol- 40.6%
Zinc oxide- 56.5% Calcium Hydroxide1.07%
Barium sulfate 1.63%
Liquid-
Eugenol Paramonochlorophenol
-
7/22/2019 Materials Used in Pediatric Endodontics
99/122
99
Hydrophilic material- can be used in humid canals
Firmly adheres to the surface to provide good seal
Disinfects dentinal tubules & hard to reach accessory
canals
Broad spectrum antibacterial effect
It resorbs when extruded extra radicularly but does not wash
-
7/22/2019 Materials Used in Pediatric Endodontics
100/122
100
It resorbs when extruded extra-radicularly but does not wash
out intra-radicularly.
( Fuks) Eugenol causes periapical irritation ( Erausquin)
Calcium Hydroxide
-
7/22/2019 Materials Used in Pediatric Endodontics
101/122
101
Calcium Hydroxide
Antiseptic
Osteoinductive properties(Hendry , Stevens 1983, Sjogren ).
Gets depleted from the canals earlier than the physiological
resorption.( Pitts )
Lentulo spiral has been reported to be the most effective in
carrying calcium hydroxide paste to working length- highest
quality filling.
-
7/22/2019 Materials Used in Pediatric Endodontics
102/122
102
Resorbs within 1-2 weeks when extruded(Ranly)
Causes no damage to permanent tooth (Reyes)
Can be removed easily
Eg. Sealapex.- 92.3% success (Sari )
-
7/22/2019 Materials Used in Pediatric Endodontics
103/122
103
Rehman
Determined the amount of duration of diffusion of calcium
ionfrom both calcium hydroxide containing root canal sealer and
an intracanal medicament
Calcium ion diffusion was more in non setting group.
-
7/22/2019 Materials Used in Pediatric Endodontics
104/122
104
Nadkarni, Damle SG
Compared ZOE and Calcium hydroxide on 70 molars for
ninemonths
94.28% success with Calcium Hydroxide.
-
7/22/2019 Materials Used in Pediatric Endodontics
105/122
105
Chawla HS et al
Mixture of Zinc oxide powder 15 gms, Calcium hydroxidepaste (
1cm) , and distilled water as root canal filling material
for 12 months
The material remained upto the apex till the beginning of
physiologic root resorption Material resorbed at the same rate
as the teeth in one case.
-
7/22/2019 Materials Used in Pediatric Endodontics
106/122
106
Vitapex- Kawakami 1979
Contains calcium hydroxide & Iodoform
Iodoform- 40.4%
Calcium hydroxide- 30.3%
Silicone- 22.4%
-
7/22/2019 Materials Used in Pediatric Endodontics
107/122
107
Bone regeneration clinically & Histologically (Dominguez
,Block )
Do not set hard so retrieval is easy
Harmless to permanent tooth germs
It is radiopaque (Garcia Godoy )
Bacteriostatic
Rate of resorption faster than phsiological resorption of
tooth
Resorbs without ill effects (Garcia Godoy).
-
7/22/2019 Materials Used in Pediatric Endodontics
108/122
108
Allergic reactions to iodine in some individuals(
Castognala)
Discoloration of teeth (Rotstein)
Iodoform irritating to the periapical tissue can cause
cemental
necrosis( Erausquin)
-
7/22/2019 Materials Used in Pediatric Endodontics
109/122
109
Kawakami T
Used Vitapex to find the fate of calcium hydroxide componentin
root canal filling paste.
Water based pastes caused necrosis because of high
alkalinity
of calcium hydroxide while silicone based paste (VITAPEX)
shows no necrotizing effect.
Comparison of zinc oxide and eugenol,and Vitapex for root canal
treatment of
-
7/22/2019 Materials Used in Pediatric Endodontics
110/122
pnecrotic primary teeth.
Mortazavi M, Mesbahi M Both ZOE and Vitapex gave encouraging
results.
overall success rates of Vitapex and ZOE were 100% and
78.5%, respectively
110
Evaluation of various root canal fillingmaterials in primary
molar pulpectomies:
http://www.ncbi.nlm.nih.gov/sites/entrez?Db=pubmed&Cmd=Search&Term=%22Mortazavi%20M%22[Author]&itool=EntrezSystem2.PEntrez.Pubmed.Pubmed_ResultsPanel.Pubmed_DiscoveryPanel.Pubmed_RVAbstractPlushttp://www.ncbi.nlm.nih.gov/sites/entrez?Db=pubmed&Cmd=Search&Term=%22Mesbahi%20M%22[Author]&itool=EntrezSystem2.PEntrez.Pubmed.Pubmed_ResultsPanel.Pubmed_DiscoveryPanel.Pubmed_RVAbstractPlushttp://www.ncbi.nlm.nih.gov/sites/entrez?Db=pubmed&Cmd=Search&Term=%22Mesbahi%20M%22[Author]&itool=EntrezSystem2.PEntrez.Pubmed.Pubmed_ResultsPanel.Pubmed_DiscoveryPanel.Pubmed_RVAbstractPlushttp://www.ncbi.nlm.nih.gov/sites/entrez?Db=pubmed&Cmd=Search&Term=%22Mesbahi%20M%22[Author]&itool=EntrezSystem2.PEntrez.Pubmed.Pubmed_ResultsPanel.Pubmed_DiscoveryPanel.Pubmed_RVAbstractPlushttp://www.ncbi.nlm.nih.gov/sites/entrez?Db=pubmed&Cmd=Search&Term=%22Mesbahi%20M%22[Author]&itool=EntrezSystem2.PEntrez.Pubmed.Pubmed_ResultsPanel.Pubmed_DiscoveryPanel.Pubmed_RVAbstractPlushttp://www.ncbi.nlm.nih.gov/sites/entrez?Db=pubmed&Cmd=Search&Term=%22Mortazavi%20M%22[Author]&itool=EntrezSystem2.PEntrez.Pubmed.Pubmed_ResultsPanel.Pubmed_DiscoveryPanel.Pubmed_RVAbstractPlushttp://www.ncbi.nlm.nih.gov/sites/entrez?Db=pubmed&Cmd=Search&Term=%22Mortazavi%20M%22[Author]&itool=EntrezSystem2.PEntrez.Pubmed.Pubmed_ResultsPanel.Pubmed_DiscoveryPanel.Pubmed_RVAbstractPlushttp://www.ncbi.nlm.nih.gov/sites/entrez?Db=pubmed&Cmd=Search&Term=%22Mortazavi%20M%22[Author]&itool=EntrezSystem2.PEntrez.Pubmed.Pubmed_ResultsPanel.Pubmed_DiscoveryPanel.Pubmed_RVAbstractPlus
-
7/22/2019 Materials Used in Pediatric Endodontics
111/122
111
materials in primary molar pulpectomies:an in vivo study.
Ozalp N, Sarolu I, Snmez H.
In the ZOE group, all pulpectomies were successful.
In the Sealapex group, two pulpectomies
Calcicur group, four pulpectomies showed complete resorption
of the material in the root canal.
Vitapex group, although six pulpectomies showed resorption
of the filling material within the canals, this had no effect
on
the clinical and radiographical success of the treatment.
Report of success rates in root filling in
http://www.ncbi.nlm.nih.gov/sites/entrez?Db=pubmed&Cmd=Search&Term=%22Ozalp%20N%22%5BAuthor%5D&itool=EntrezSystem2.PEntrez.Pubmed.Pubmed_ResultsPanel.Pubmed_DiscoveryPanel.Pubmed_RVAbstractPlushttp://www.ncbi.nlm.nih.gov/sites/entrez?Db=pubmed&Cmd=Search&Term=%22Saro%C4%9Flu%20I%22%5BAuthor%5D&itool=EntrezSystem2.PEntrez.Pubmed.Pubmed_ResultsPanel.Pubmed_DiscoveryPanel.Pubmed_RVAbstractPlushttp://www.ncbi.nlm.nih.gov/sites/entrez?Db=pubmed&Cmd=Search&Term=%22Saro%C4%9Flu%20I%22%5BAuthor%5D&itool=EntrezSystem2.PEntrez.Pubmed.Pubmed_ResultsPanel.Pubmed_DiscoveryPanel.Pubmed_RVAbstractPlushttp://www.ncbi.nlm.nih.gov/sites/entrez?Db=pubmed&Cmd=Search&Term=%22S%C3%B6nmez%20H%22%5BAuthor%5D&itool=EntrezSystem2.PEntrez.Pubmed.Pubmed_ResultsPanel.Pubmed_DiscoveryPanel.Pubmed_RVAbstractPlushttp://www.ncbi.nlm.nih.gov/sites/entrez?Db=pubmed&Cmd=Search&Term=%22S%C3%B6nmez%20H%22%5BAuthor%5D&itool=EntrezSystem2.PEntrez.Pubmed.Pubmed_ResultsPanel.Pubmed_DiscoveryPanel.Pubmed_RVAbstractPlushttp://www.ncbi.nlm.nih.gov/sites/entrez?Db=pubmed&Cmd=Search&Term=%22S%C3%B6nmez%20H%22%5BAuthor%5D&itool=EntrezSystem2.PEntrez.Pubmed.Pubmed_ResultsPanel.Pubmed_DiscoveryPanel.Pubmed_RVAbstractPlushttp://www.ncbi.nlm.nih.gov/sites/entrez?Db=pubmed&Cmd=Search&Term=%22S%C3%B6nmez%20H%22%5BAuthor%5D&itool=EntrezSystem2.PEntrez.Pubmed.Pubmed_ResultsPanel.Pubmed_DiscoveryPanel.Pubmed_RVAbstractPlushttp://www.ncbi.nlm.nih.gov/sites/entrez?Db=pubmed&Cmd=Search&Term=%22Saro%C4%9Flu%20I%22%5BAuthor%5D&itool=EntrezSystem2.PEntrez.Pubmed.Pubmed_ResultsPanel.Pubmed_DiscoveryPanel.Pubmed_RVAbstractPlushttp://www.ncbi.nlm.nih.gov/sites/entrez?Db=pubmed&Cmd=Search&Term=%22Saro%C4%9Flu%20I%22%5BAuthor%5D&itool=EntrezSystem2.PEntrez.Pubmed.Pubmed_ResultsPanel.Pubmed_DiscoveryPanel.Pubmed_RVAbstractPlushttp://www.ncbi.nlm.nih.gov/sites/entrez?Db=pubmed&Cmd=Search&Term=%22Saro%C4%9Flu%20I%22%5BAuthor%5D&itool=EntrezSystem2.PEntrez.Pubmed.Pubmed_ResultsPanel.Pubmed_DiscoveryPanel.Pubmed_RVAbstractPlushttp://www.ncbi.nlm.nih.gov/sites/entrez?Db=pubmed&Cmd=Search&Term=%22Ozalp%20N%22%5BAuthor%5D&itool=EntrezSystem2.PEntrez.Pubmed.Pubmed_ResultsPanel.Pubmed_DiscoveryPanel.Pubmed_RVAbstractPlushttp://www.ncbi.nlm.nih.gov/sites/entrez?Db=pubmed&Cmd=Search&Term=%22Ozalp%20N%22%5BAuthor%5D&itool=EntrezSystem2.PEntrez.Pubmed.Pubmed_ResultsPanel.Pubmed_DiscoveryPanel.Pubmed_RVAbstractPlushttp://www.ncbi.nlm.nih.gov/sites/entrez?Db=pubmed&Cmd=Search&Term=%22Ozalp%20N%22%5BAuthor%5D&itool=EntrezSystem2.PEntrez.Pubmed.Pubmed_ResultsPanel.Pubmed_DiscoveryPanel.Pubmed_RVAbstractPlus
-
7/22/2019 Materials Used in Pediatric Endodontics
112/122
112
p gprimary molars
Invest igator Fol lowupMonths
No.of teethexamined
Fi l l ingMaterial
Success Rate%
Gould 7-26 29 ZOE 68.7
Rifkin 12 26 KRI 89.0
Coll 6-36 33 ZOE 80.5
Coll 60-82 29 ZOE 86.1
Garcia
Godoy
6-24 55 KRI 95.6
Reyes 6-24 53 KRI+FC+
Ca(OH)2
100
Barr 12-74 62 ZOE+
FC
82.3
Success of pulpectomy with zinc oxide-e genol s calci m h d o
ide/iodofo m
-
7/22/2019 Materials Used in Pediatric Endodontics
113/122
113
eugenol vs calcium hydroxide/iodoformpaste in primary
molars.
Trairatvorakul C, Chunlasikaiwan S.
At 6 and 12 months, the ZOE success rates were 48% and
85%, respectively, and the Vitapex success rates were 78%and
89%
Vitapex appeared to resolve furcation pathology at a faster
rate
than zinc oxide-eugenol at 6 months, while at 12 months,
both
materials yielded similar results.
Conclusion
http://www.ncbi.nlm.nih.gov/sites/entrez?Db=pubmed&Cmd=Search&Term=%22Trairatvorakul%20C%22%5BAuthor%5D&itool=EntrezSystem2.PEntrez.Pubmed.Pubmed_ResultsPanel.Pubmed_DiscoveryPanel.Pubmed_RVAbstractPlushttp://www.ncbi.nlm.nih.gov/sites/entrez?Db=pubmed&Cmd=Search&Term=%22Chunlasikaiwan%20S%22%5BAuthor%5D&itool=EntrezSystem2.PEntrez.Pubmed.Pubmed_ResultsPanel.Pubmed_DiscoveryPanel.Pubmed_RVAbstractPlushttp://www.ncbi.nlm.nih.gov/sites/entrez?Db=pubmed&Cmd=Search&Term=%22Chunlasikaiwan%20S%22%5BAuthor%5D&itool=EntrezSystem2.PEntrez.Pubmed.Pubmed_ResultsPanel.Pubmed_DiscoveryPanel.Pubmed_RVAbstractPlushttp://www.ncbi.nlm.nih.gov/sites/entrez?Db=pubmed&Cmd=Search&Term=%22Chunlasikaiwan%20S%22%5BAuthor%5D&itool=EntrezSystem2.PEntrez.Pubmed.Pubmed_ResultsPanel.Pubmed_DiscoveryPanel.Pubmed_RVAbstractPlushttp://www.ncbi.nlm.nih.gov/sites/entrez?Db=pubmed&Cmd=Search&Term=%22Chunlasikaiwan%20S%22%5BAuthor%5D&itool=EntrezSystem2.PEntrez.Pubmed.Pubmed_ResultsPanel.Pubmed_DiscoveryPanel.Pubmed_RVAbstractPlushttp://www.ncbi.nlm.nih.gov/sites/entrez?Db=pubmed&Cmd=Search&Term=%22Trairatvorakul%20C%22%5BAuthor%5D&itool=EntrezSystem2.PEntrez.Pubmed.Pubmed_ResultsPanel.Pubmed_DiscoveryPanel.Pubmed_RVAbstractPlushttp://www.ncbi.nlm.nih.gov/sites/entrez?Db=pubmed&Cmd=Search&Term=%22Trairatvorakul%20C%22%5BAuthor%5D&itool=EntrezSystem2.PEntrez.Pubmed.Pubmed_ResultsPanel.Pubmed_DiscoveryPanel.Pubmed_RVAbstractPlushttp://www.ncbi.nlm.nih.gov/sites/entrez?Db=pubmed&Cmd=Search&Term=%22Trairatvorakul%20C%22%5BAuthor%5D&itool=EntrezSystem2.PEntrez.Pubmed.Pubmed_ResultsPanel.Pubmed_DiscoveryPanel.Pubmed_RVAbstractPlus
-
7/22/2019 Materials Used in Pediatric Endodontics
114/122
114
Conclusion
REFERENCES
-
7/22/2019 Materials Used in Pediatric Endodontics
115/122
115
Don M. Ranly; Pulpotomy therapy in primary teeth: new modalities
for old
rationales; Pediatric dentistry; 16: 1994; 403-9
D.R. Llewelyn; The pulp treatment of the primary dentition;
International
Journal of Pediatric Dentistry; 2000; 10: 248-252
Cheng D.Fong, Martin J.Davis; Partial pulpotomy for immature
permanentteeth, its present & future; Pediatric Dentistry 24:
29-32, 2002
Scott A. Fishman, Richard D. Udin, David L.Good, Fairborz Rodef;
Success of
electrofulguration pulpotomies covered by zinc oxide &
eugenol or calcium
hydroxide: a clinical study; Pediatric Dentistry; 18: 385-90;
1996
Waterhouse PJ; Formocresol & alternative primary molar
pulpotomy
medicaments: a review; Endod Dent Traumatol 1995; 11:
157-162
V. Srinivasan, C. L. Patchett, P. J. Waterhouse; Is there life
after Buckleys
Formocresol? Part IA narrative review of alternative
interventions &
-
7/22/2019 Materials Used in Pediatric Endodontics
116/122
116
materials; International Journal of Pediatric Dentistry; 2006;
16: 117-127
V. Srinivasan, C. L. Patchett, P. J. Waterhouse; Is there life
after BuckleysFormocresol? Part IIDevelopment of a protocol for the
management of
extensive caries in the primary molar; International Journal of
Pediatric
Dentistry; 2006; 16: 199-206
Peter L. Judd, David J. Kenny; Formocresol Concern; J. Canad
Dent Assn,1987; no.5; 401-4
Bradley Lewis; Formaldehyde in dentistry: a review for the
millennium; The
Journal of Clinical Pediatric Dentistry; Vol. 22; No. 2/1998
Sharon D. Hill, N. Sue Seale, E. Matthew Quintero, BS Ingrid Y.
Guo; The
effect of glutaraldehyde pulpotomy treatment on pulpal enzymes;
Pediatric
Dentistry: Sep./Oct. 1993; vol. 15, no. 5; 337-42
Robert J. Feigal, harold H. Messer; A critical look at
gluteraldehyde;
Pediatric dentistry: April/ May, 1990; Vol. 12, No. 2; 69-71
-
7/22/2019 Materials Used in Pediatric Endodontics
117/122
117
D.M. Ranly, Franklin Garcia Gogoy, Diane Horn; Time,
concentration &
pH parameters for the use of gluteralhehyde as a pulpotomy
agent: an invitro study; Pediatric dentistry: sep. 1987/ vol. 9.
No.3; 199-203
Ay- Luen Fei, Richard d. Udin, Ronald Johnson; A clinical study
of ferric
sulfate as a pulpotomy agent in primary teeth; Pediatric
dentistry;
Nov./Dec. 1991; Vol.13; No.6; 327-32.
Nikki L Smith, N. Sue Seale, Martha E. Nunn; ferric sulfate
pulpotomy in
primary molars: A retrospective study; Pediatric Dentistry 2000;
22: 192-
199.
David M.Strange, N. Sue Seale, Martha E. Nunn, Malcolm
Strange;
Outcome of formocresol/ ZOE sub-base pulpotomies utilizing
alternative
radiographic success criteria; Pediatric Dentistry 2001; 23:
331-336
Derek Zurn, N. sue Seale; Light cured Calcium hydroxide
VsFormocresol in human primary molar pulpotomies: A
randomizedControlled trial; Pediatric dentistry 2008; 30: 34 31
-
7/22/2019 Materials Used in Pediatric Endodontics
118/122
118
Controlled trial; Pediatric dentistry 2008; 30: 34-31
A.B.S. Moretti et al, The effectiveness of MTA, calcium
hydroxide& formocresol for pulpotomies in primary teeth;
InternationalEndodontic Journal, 2008, 41, 547-555
Howard W. Robert, Jeffery M. Toth, David W. Berzins, David
G.
Charlton; MTA material use in endodontic treatment: A review
ofthe literature; Dental Materials; 24 (2008); 149-164
D. Tuna & A. Olmez; Clinical long term evaluation of MTA as
adirect pulp capping material in primary teeth; International
Endodontic Journal; 41; 2008; 273-278
Eliezer Eidelman, Dr. Odont, Gideon Holan, Anna B. Fuks; MTAVs
Formocresol in pulpotomized primary molars: a preliminaryreport;
Pediatric Dentistry-2001, 23:15-18
Richard S. Schwartz et al; MTA: a new material for Endodontics;
JADA1999; Vol.130, 967-975
-
7/22/2019 Materials Used in Pediatric Endodontics
119/122
119
Neeta T. Prabhu, A.K. Munshi; Clinical, radiographic &
histologicalobservation of the radicular pulp following Feracrylum
pulpotomy; J.
Clin Pediatr Dent; 1997, 21(2): 151-156
K. Iohara et al; Dentin regeneration by dental pulp stem cell
therapy withrecombinant Human Bone morphogenetic Protein2; Journal
of DentalResearch; 2004; 83(8): 590-595
Yoshito Yoshimine, Katsumasa Maeda, Fukuoka; Histologic
evaluation oftetracalcium phosphate based cement as a direct pulp
capping agent;OOOE; 1995; 79: 351-8
Manoj Komath, varma H.K.; Fully injectable calcium phosphate
cement- apromise to dentistry; Ind J Dent Res; 2004; 15(3):
89-95
Anna B. Fuks; Vital pulp therapy with new materials for primary
teeth:New direction & Treatment perspectives; Pediatr Dent
2008; 30: 211-9
Fuks AB; Pulp therapy for primary dentition. In Pediatric
Dentistry:infancy through adolescence; Pediatric Dentistry 2005
-
7/22/2019 Materials Used in Pediatric Endodontics
120/122
120
Fuks AB, Papaginnoulis L; Pulpotomy in primary teeth: review
of
literature; Eur Arch Pediatr Dent 2006;7; 64-71
David E. Witherspoon; Vital pulp tissue with new material:
Newdirection & treatment perspectives- Permanent teeth; Pediatr
dent2008; 30; 220-4
Alan R. Milnes; Is Formocresol Obsolete? A fresh look at
theevidence concerning safety Issues; Pediatr dent 2008; 30;
237-46
Paula Jane Waterhouse; New Age pulp therapy: Personal thoughtson
a hot debate; Pediatr dent 2008; 30; 247-52
D. B. Kennedy; Pulp therapy; Kennedys Pediatric
OperativeDentistry; Chapter 18,19; 4th edt.; 157-168
Shobha Tandon; Pediatric EndodonticsTreatment Modalities;
Textbook ofPedodontics; 2nd edt.; 404-410
-
7/22/2019 Materials Used in Pediatric Endodontics
121/122
121
Nikhil Marwah; Pediatric Endodontics; Comprehensive Pediatric
Dentistry;chapter 20 ;1st edt.; 183-189
John I. Ingle; Pediatric Endodontics; Endodontics; Chapter 17;
5th edt.; 875-889
Jimmy Pinkham; Pulp therapy of Primary dentition; Pediatric
dentistryInfancy through Adolescence; Chapter 22; Edt.4;
384-387
Mc Donald; Treatment of deep caries, Vital pulp exposure &
pulpless teeth;Dentistry for Child & Adolescent; chapter18; 8th
edt.; 397-399
Cohen, Pathways of pulp , Pediatric Endodontics.
THANK U
-
7/22/2019 Materials Used in Pediatric Endodontics
122/122